Embed Size (px)
Citation preview
Anatomical basis of radical
hysterectomy
Denis Querleu
Institut Bergonié Cancer Center, Bordeaux, France
PART 1 : SURGICAL ANATOMY
• Classical spaces
• Non existing structures
• Less classical spaces
• Autonomic nerves anatomy
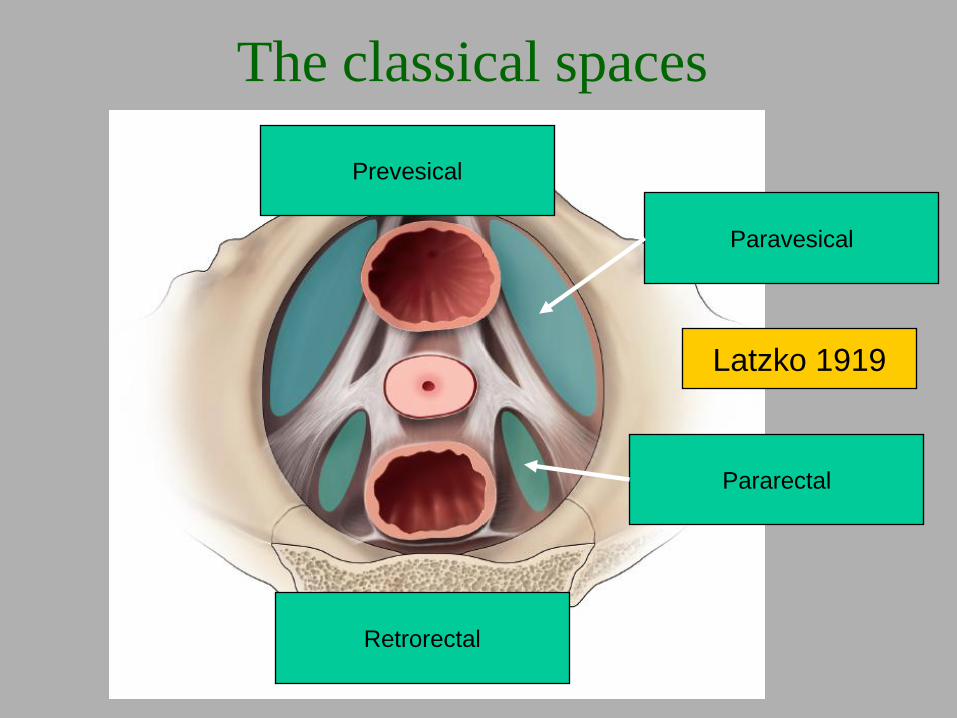
The classical spaces
Paravesical
Prevesical
Retrorectal
Pararectal
Latzko 1919
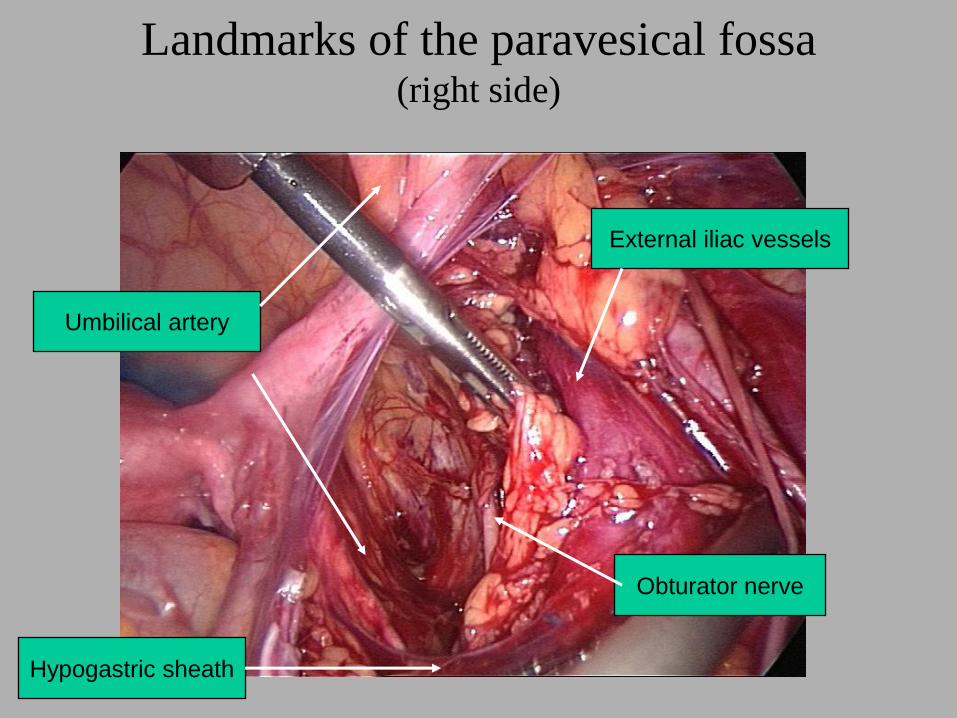
Landmarks of the paravesical fossa(right side)
Umbilical artery
External iliac vessels
Obturator nerve
Hypogastric sheath
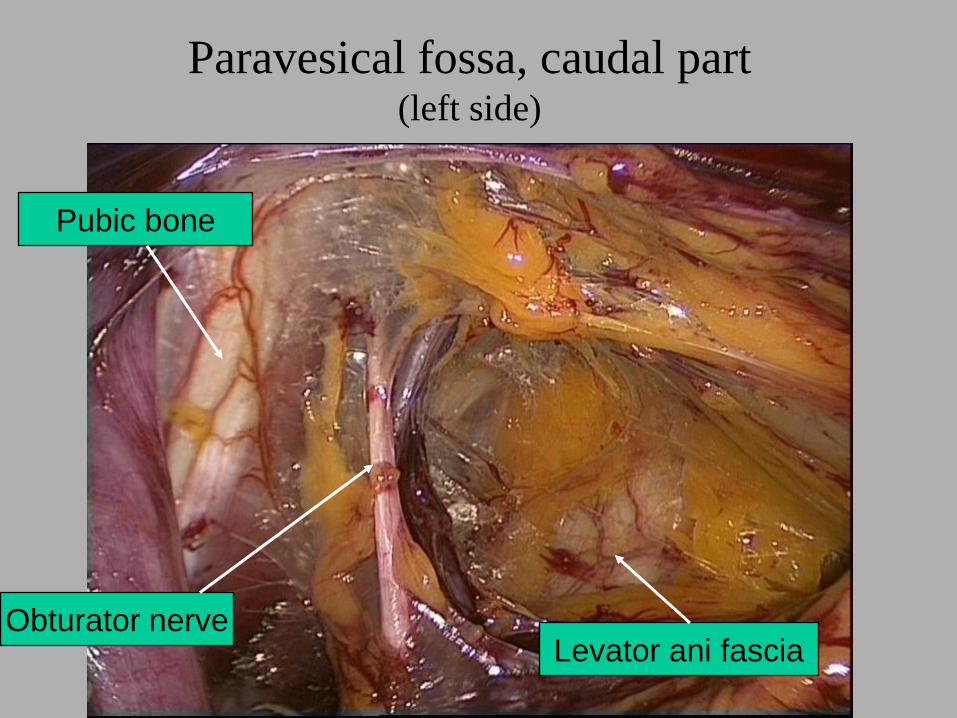
Paravesical fossa, caudal part(left side)
Obturator nerveLevator ani fascia
Pubic bone
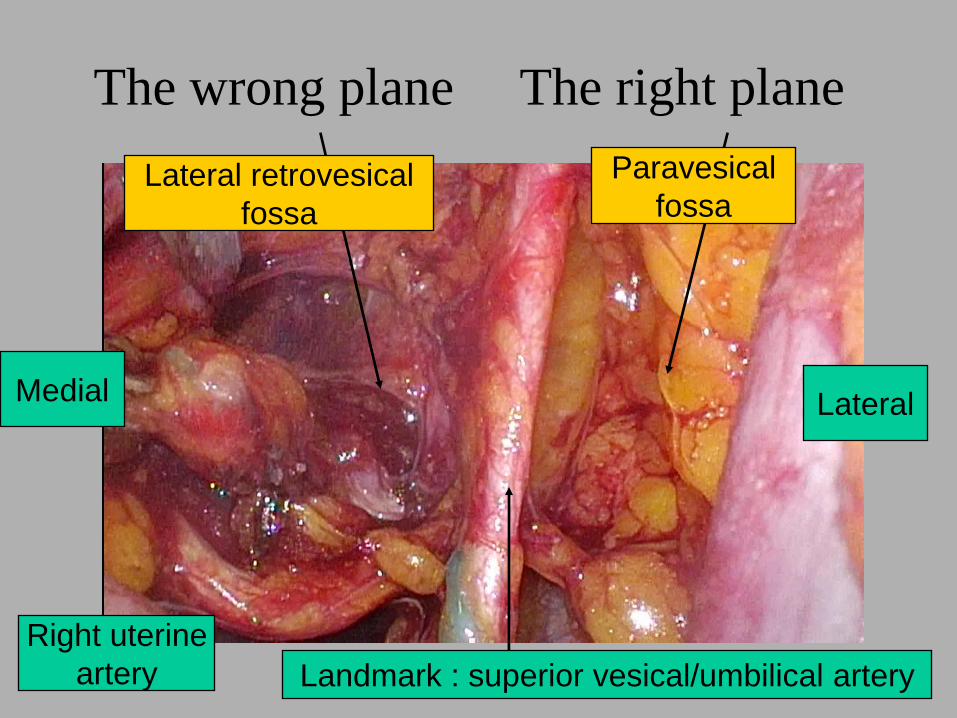
The wrong plane The right plane
Landmark : superior vesical/umbilical artery
Medial Lateral
Right uterine
artery
Lateral retrovesical
fossa
Paravesical
fossa
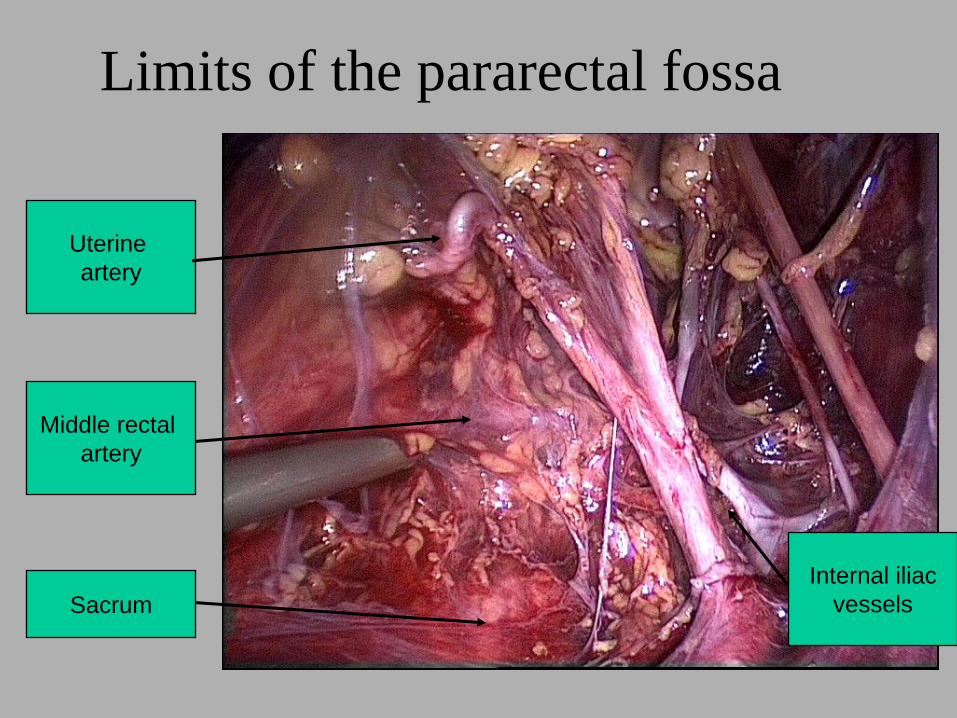
Limits of the pararectal fossa
Middle rectal
artery
Uterine
artery
Sacrum
Internal iliac
vessels
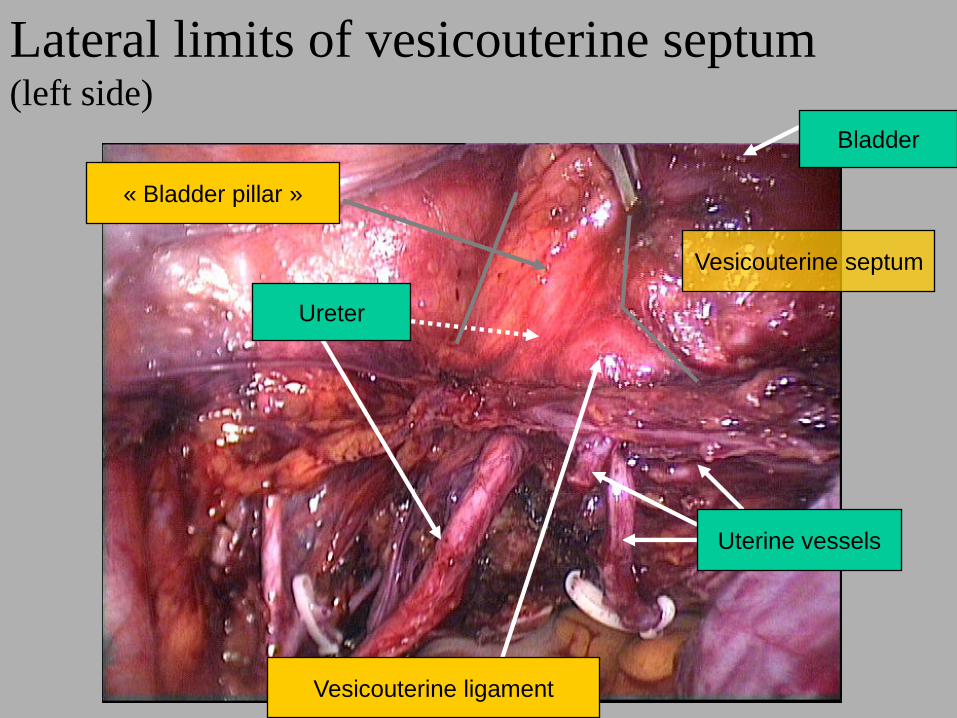
Lateral limits of vesicouterine septum(left side)
« Bladder pillar »
Vesicouterine septum
Bladder
Ureter
Uterine vessels
Vesicouterine ligament
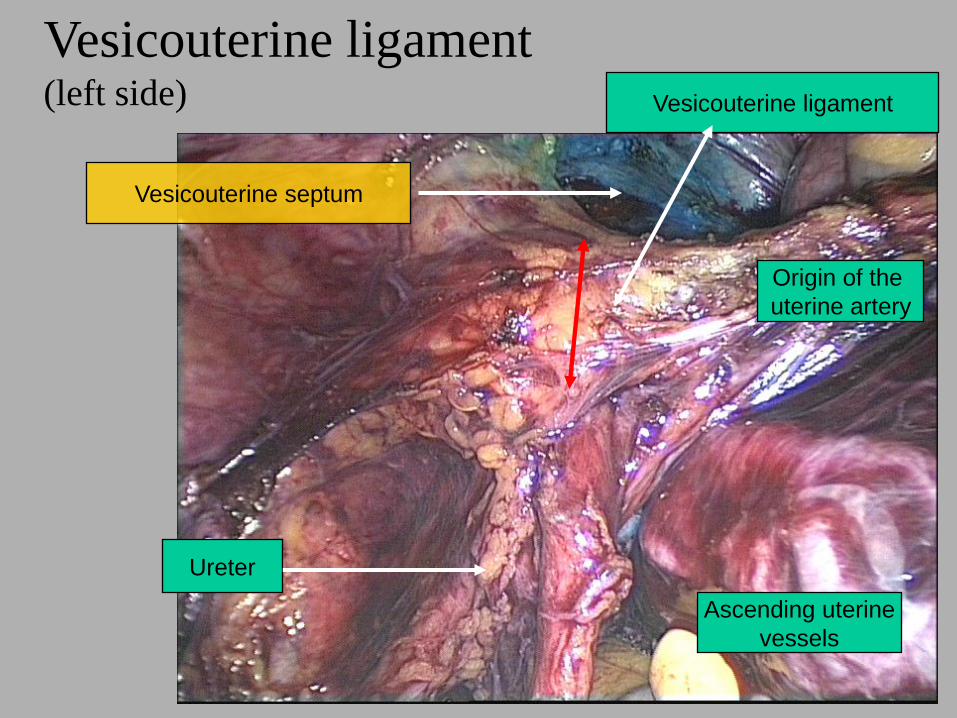
Vesicouterine ligament(left side) Vesicouterine ligament
Vesicouterine septum
Origin of the
uterine artery
Ureter
Ascending uterine
vessels
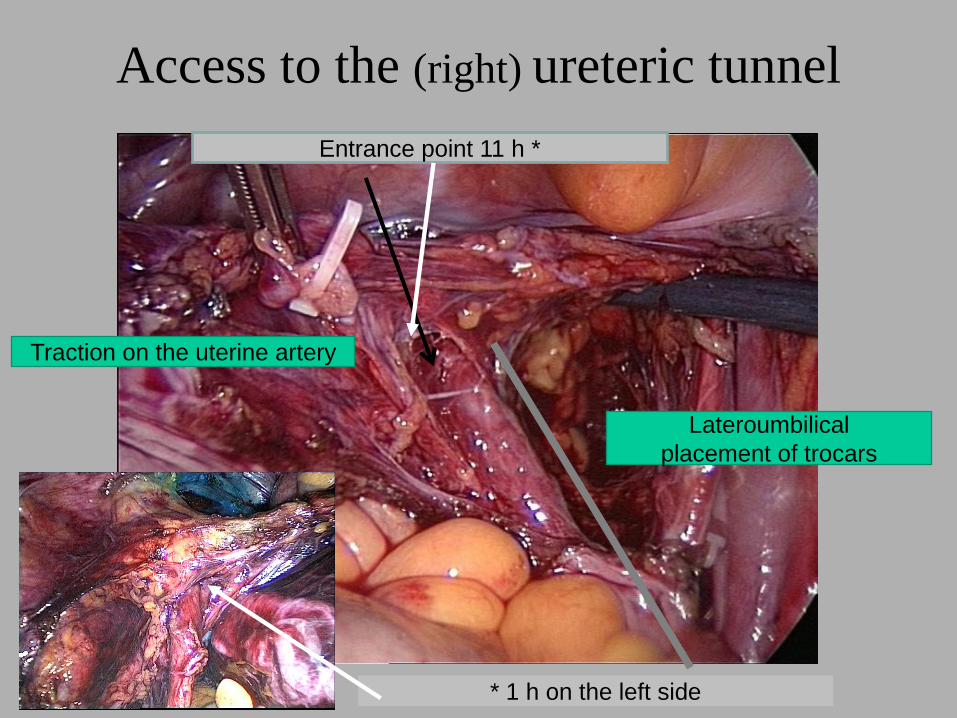
Access to the (right) ureteric tunnel
* 1 h on the left side
Entrance point 11 h *
Lateroumbilical
placement of trocars
Traction on the uterine artery
Ureter
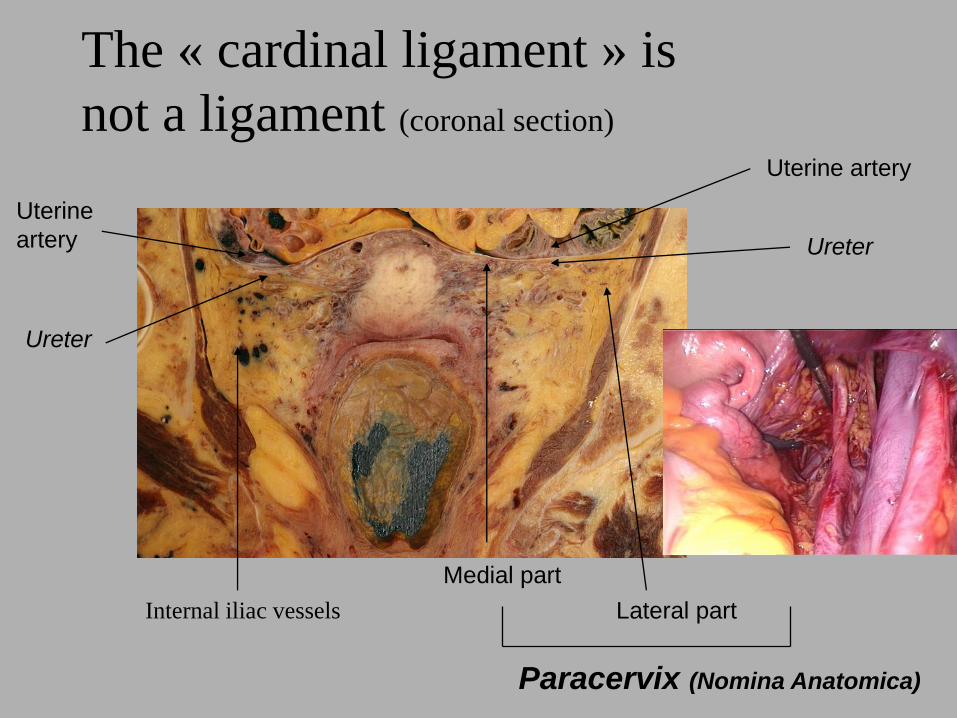
The « cardinal ligament » is
not a ligament (coronal section)
Medial part
Lateral partInternal iliac vessels
Paracervix (Nomina Anatomica)
Uterine artery
Uterine
artery
Ureter
Ureter
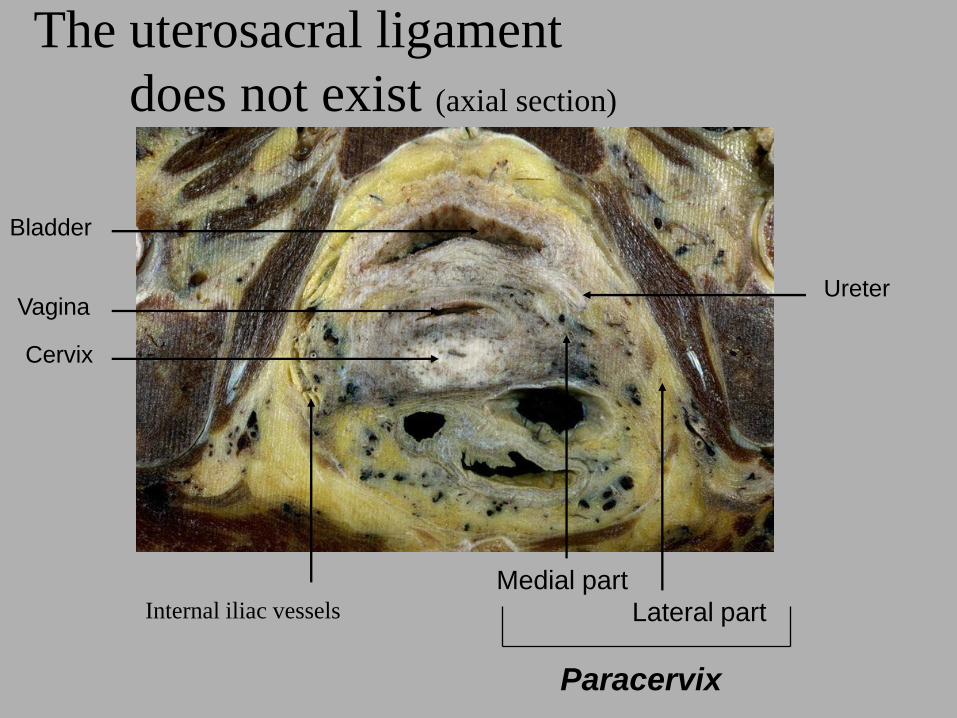
The uterosacral ligament
does not exist (axial section)
Bladder
Vagina
Cervix
Medial part
Lateral partInternal iliac vessels
Paracervix
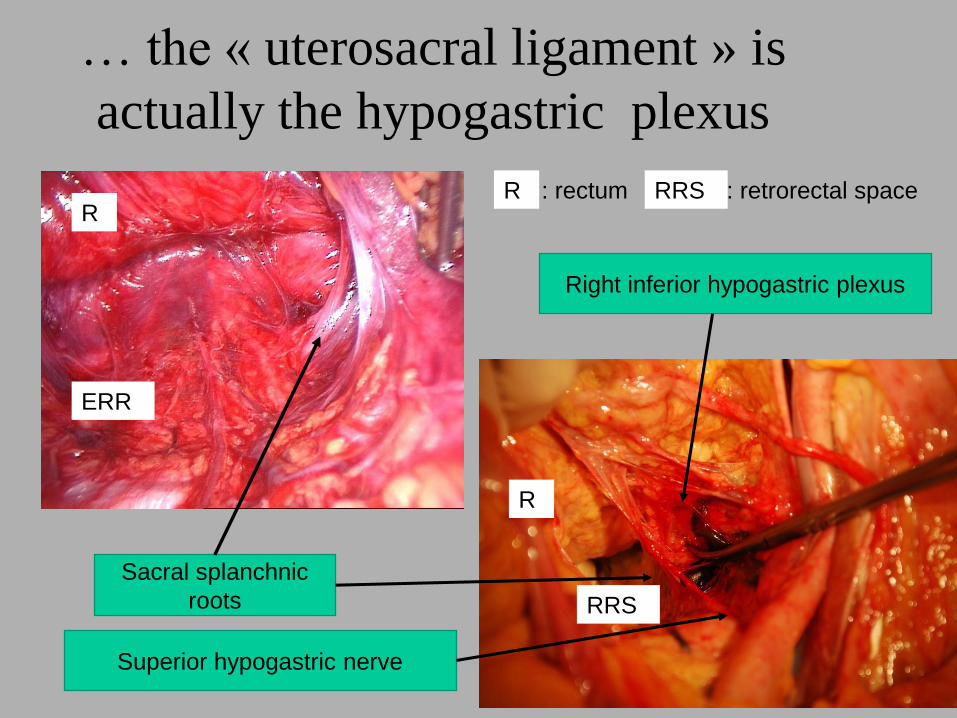
… the « uterosacral ligament » is
actually the hypogastric plexus
Sacral splanchnic
roots
Right inferior hypogastric plexus
Superior hypogastric nerve
R
R
R : rectum
ERR
RRS
RRS : retrorectal spaceR RRS
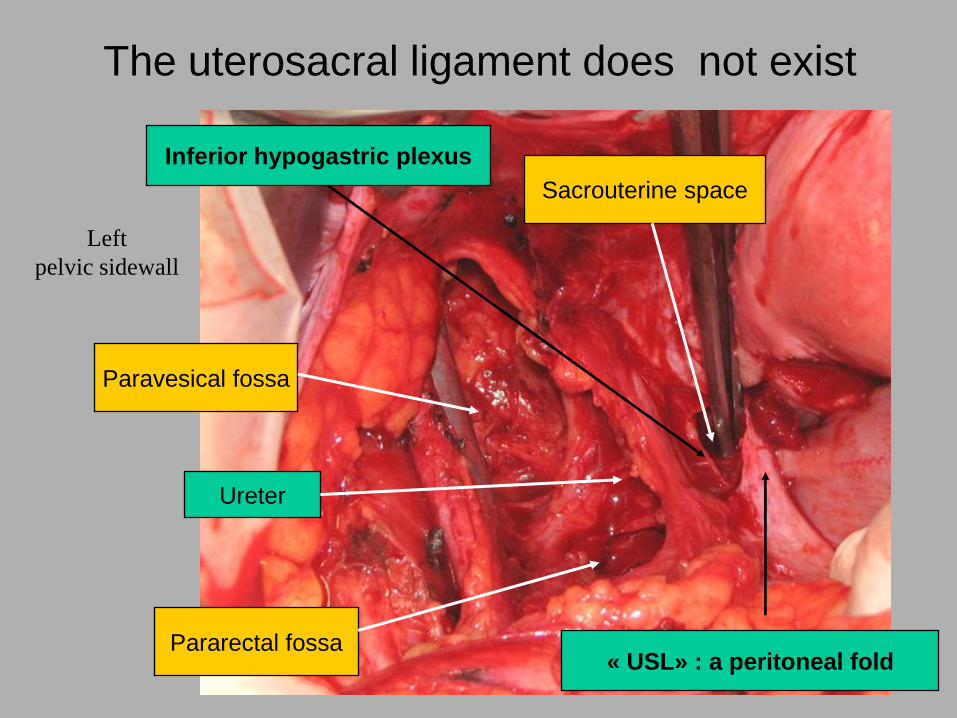
Left
pelvic sidewall
The uterosacral ligament does not exist
Inferior hypogastric plexus
Paravesical fossa
Ureter
Pararectal fossa« USL» : a peritoneal fold
Sacrouterine space

Other inexisting or misnamed
structures
• « Lateral parametrium » = paracervix
• « Anterior parametrium » = vesical lateral ligament = umbilical and superior vesical arteries
• « Posterior parametrium » = « uterosacral ligament » = nothing but a fibrous condensation close to the torus uterinus
• « Deep vesicouterine ligament » = vesicovaginal ligament
Less classical spaces
• The same spaces, from below
• « New spaces »
– Retrovesical spaces (lateral/medial)
– Sacrouterine space
• The pelvic sidewall layers
– vascular plane
– sacral nerves plane
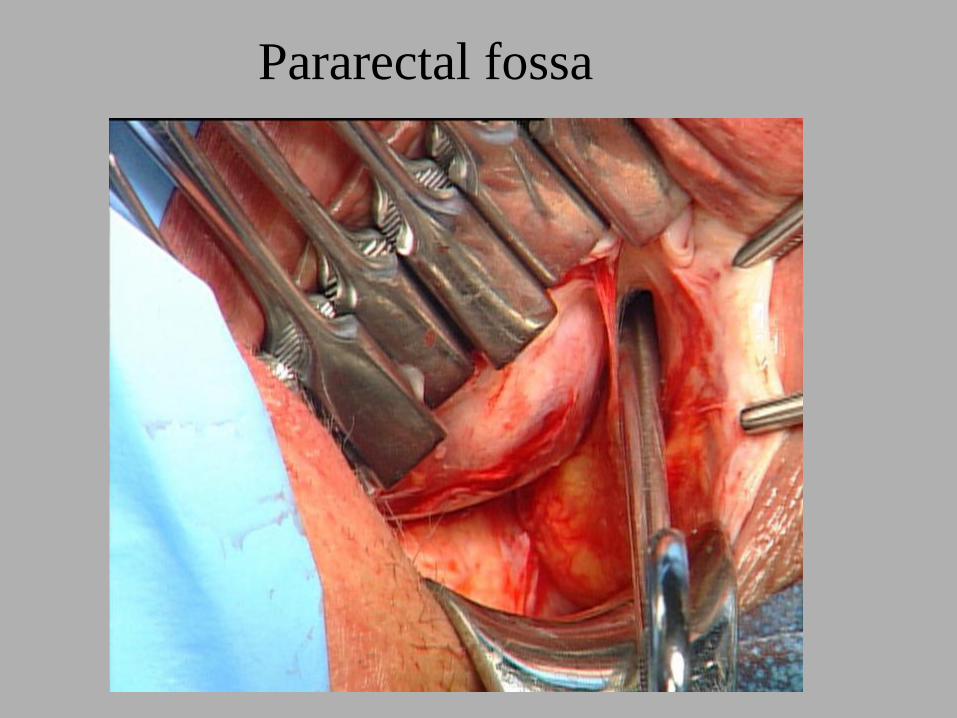
Pararectal fossa
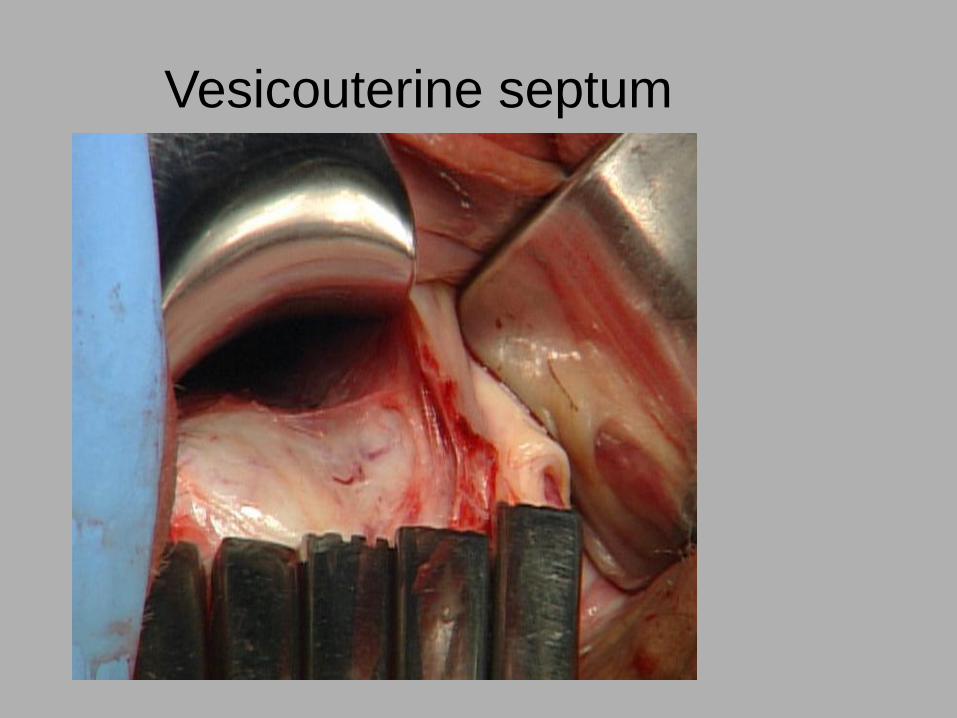
Vesicouterine septum

Paravesical fossa
Bladder pillar
Vesicouterine
septum
Paravesical fossa
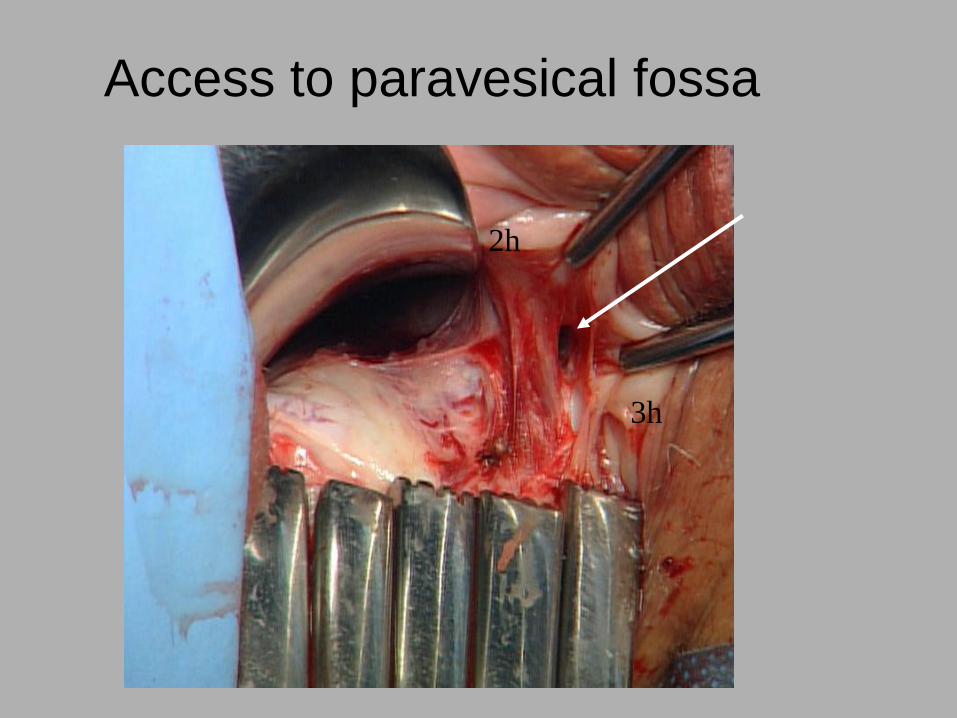
2h
Access to paravesical fossa
3h
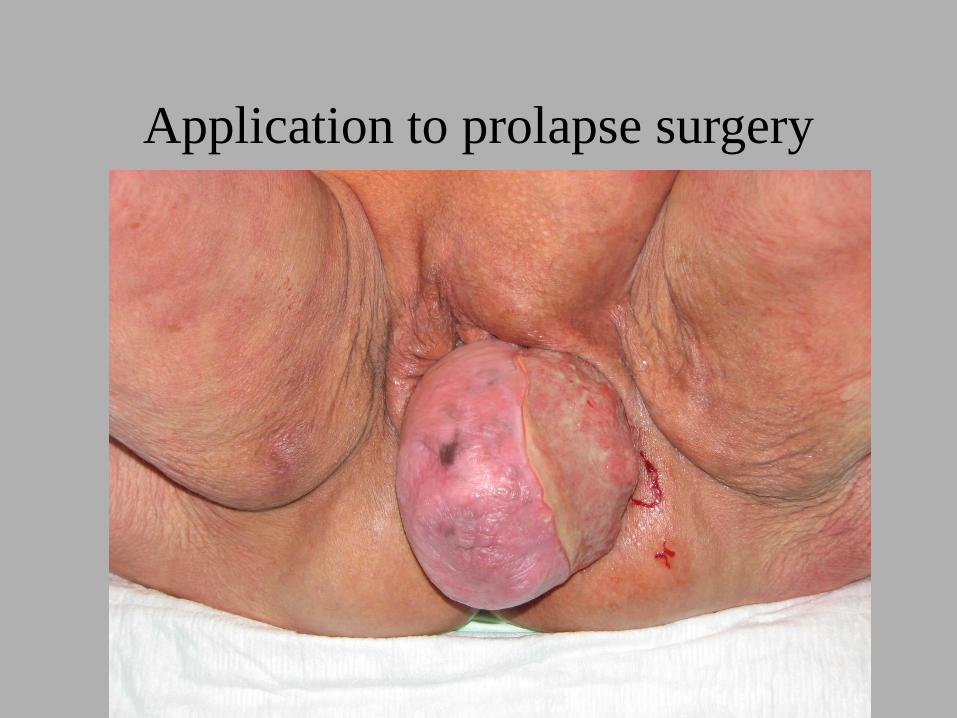
Application to prolapse surgery
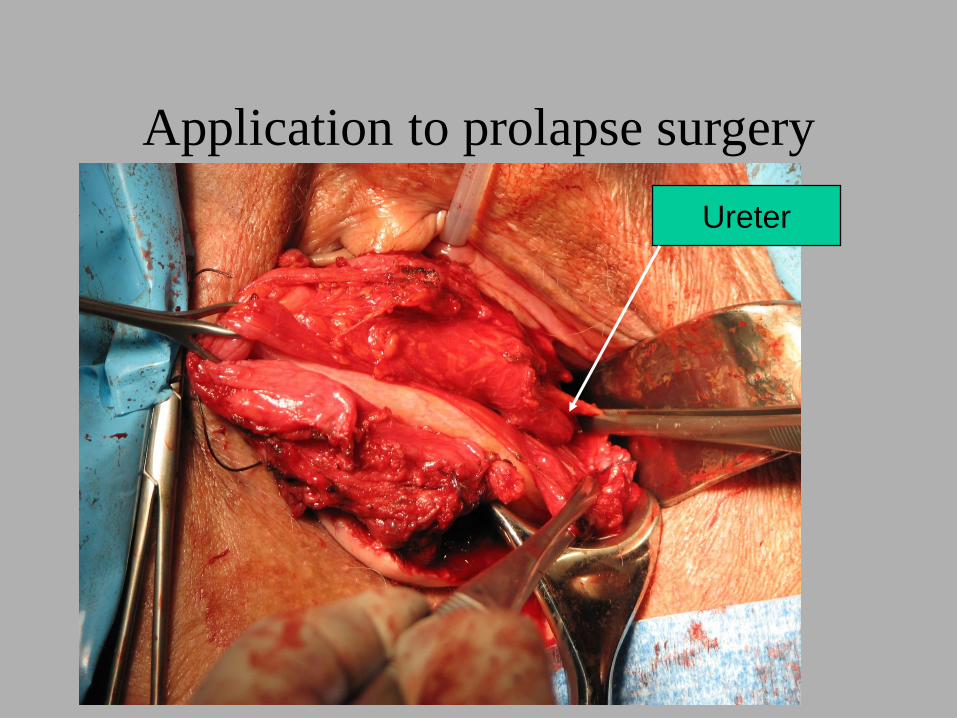
Application to prolapse surgery
Ureter
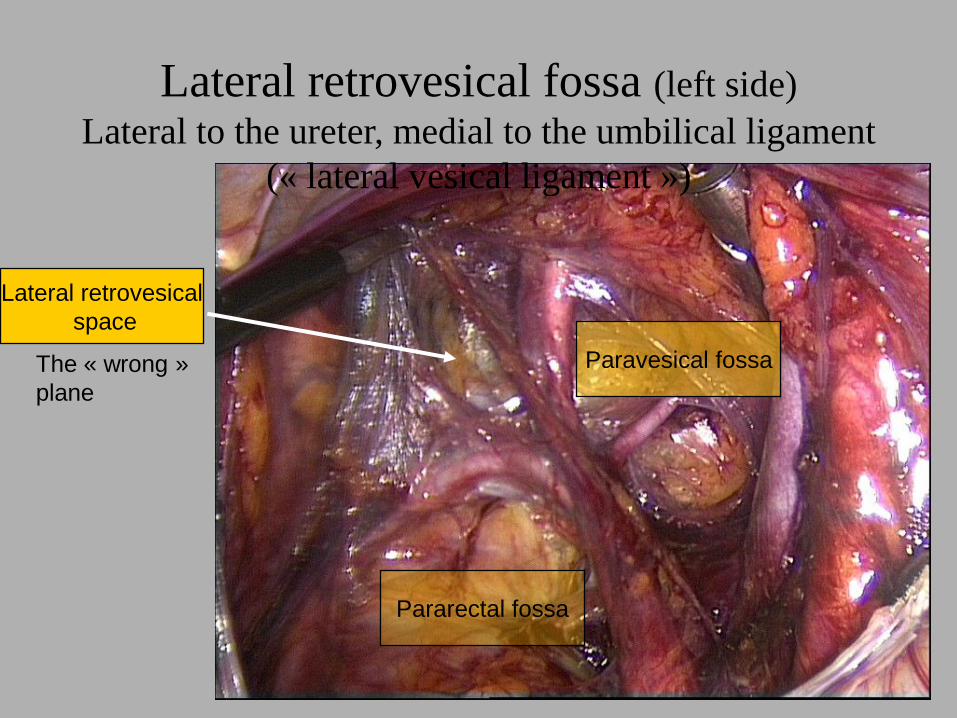
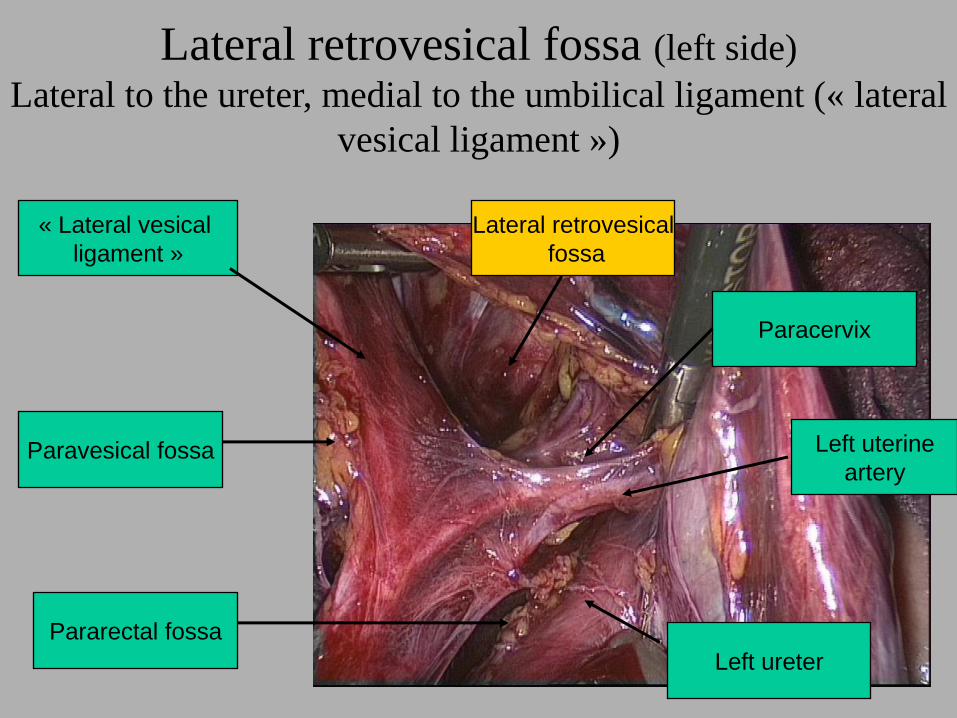
Lateral retrovesical fossa (left side)
Lateral to the ureter, medial to the umbilical ligament
(« lateral vesical ligament »)
Paravesical fossa
Pararectal fossa
The « wrong »
plane
Lateral retrovesical
space
Lateral retrovesical fossa (left side)
Lateral to the ureter, medial to the umbilical ligament (« lateral
vesical ligament »)
Paravesical fossa
Paracervix
Pararectal fossa
Left ureter
Left uterine
artery
« Lateral vesical
ligament »
Lateral retrovesical
fossa
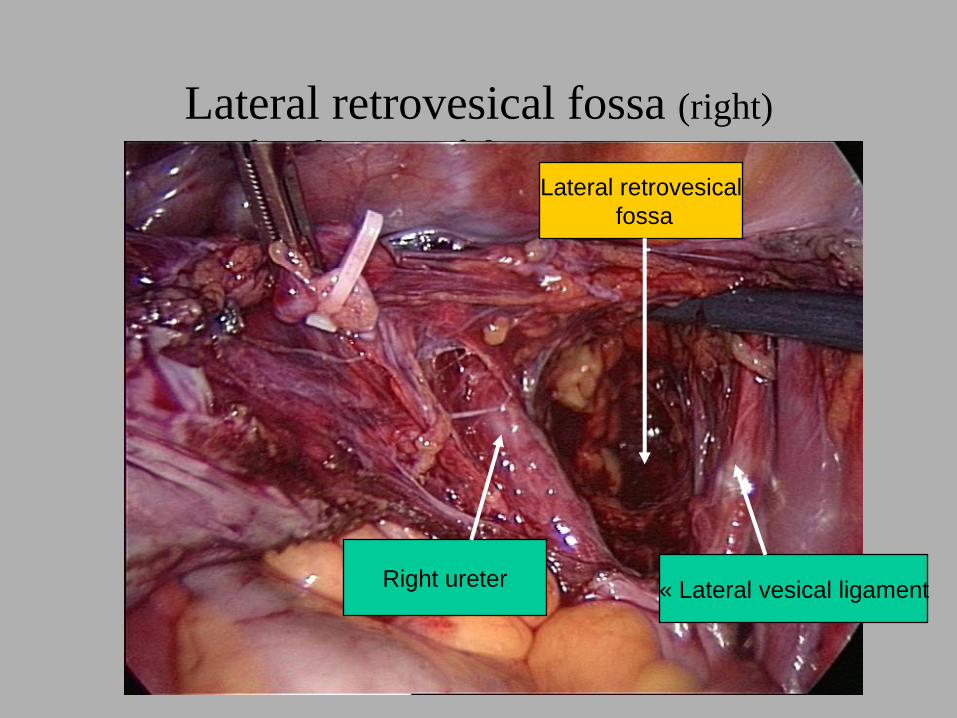
Lateral retrovesical fossa (right)
after division of the uterine arteryLateral retrovesical
fossa
« Lateral vesical ligamentRight ureter
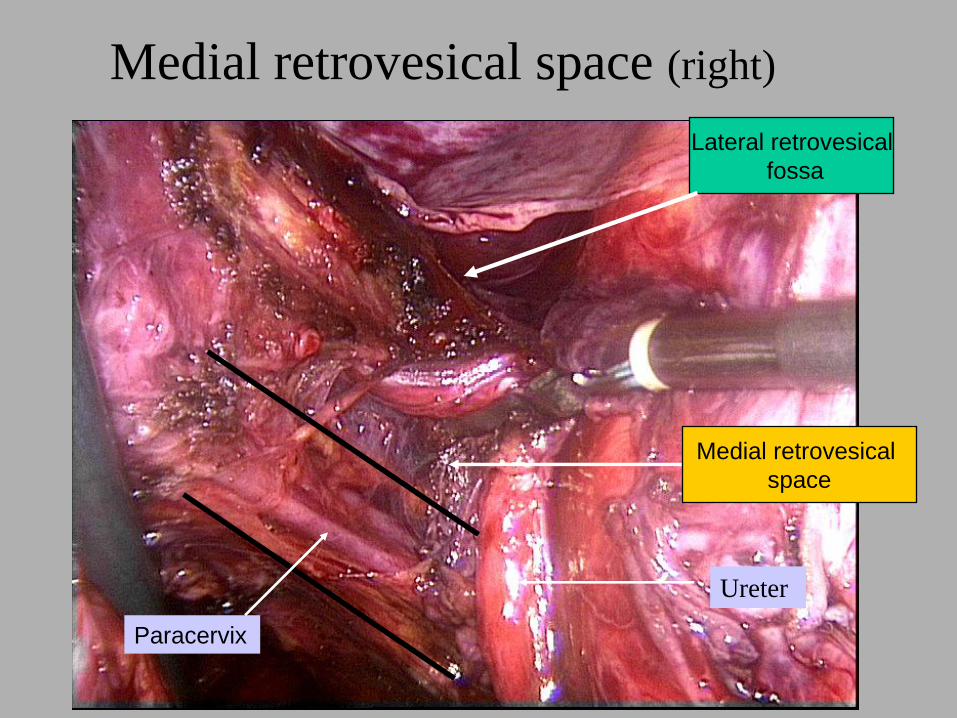
Medial retrovesical space (right)
Ureter
Lateral retrovesical
fossa
Medial retrovesical
space
Paracervix
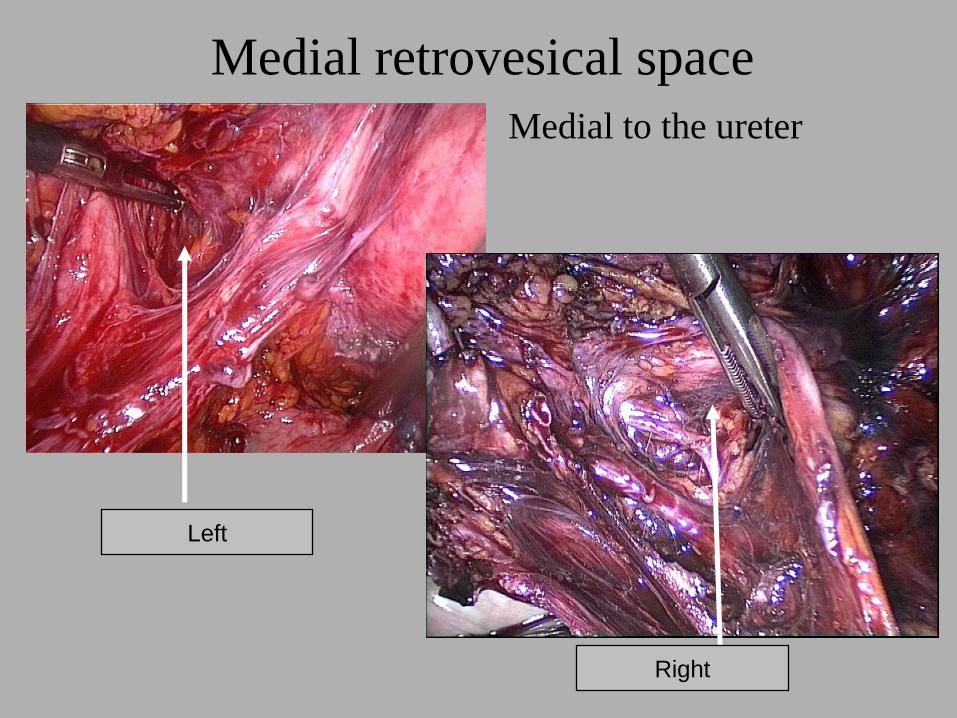
Medial retrovesical space
Medial to the ureter
Left
Right
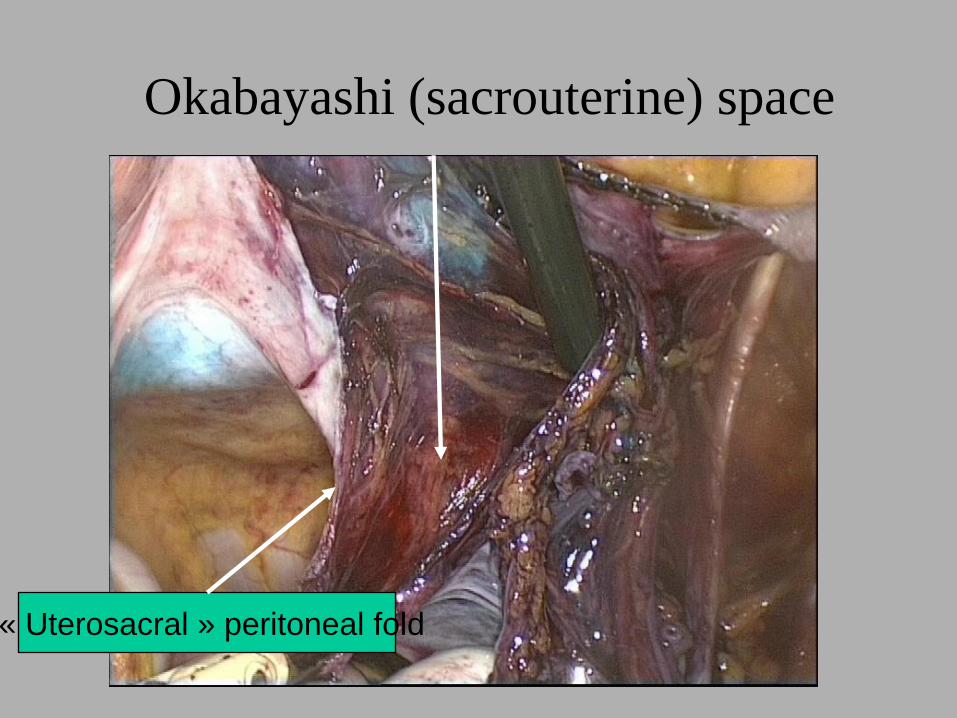
Okabayashi (sacrouterine) space
« Uterosacral » peritoneal fold
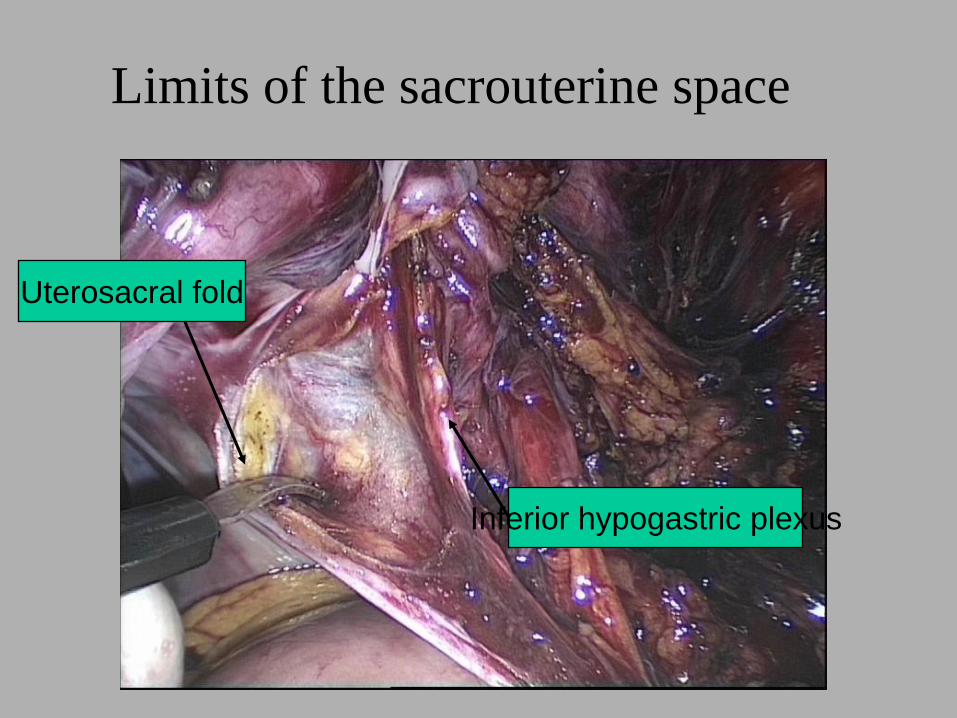
Limits of the sacrouterine space
Uterosacral fold
Inferior hypogastric plexus
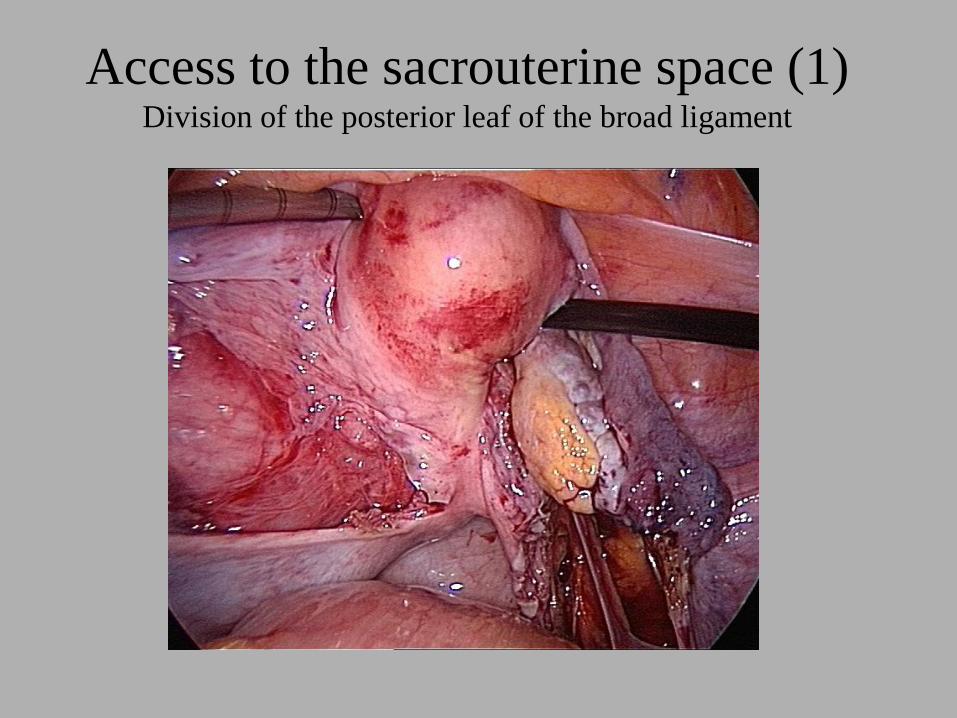
Access to the sacrouterine space (1)Division of the posterior leaf of the broad ligament
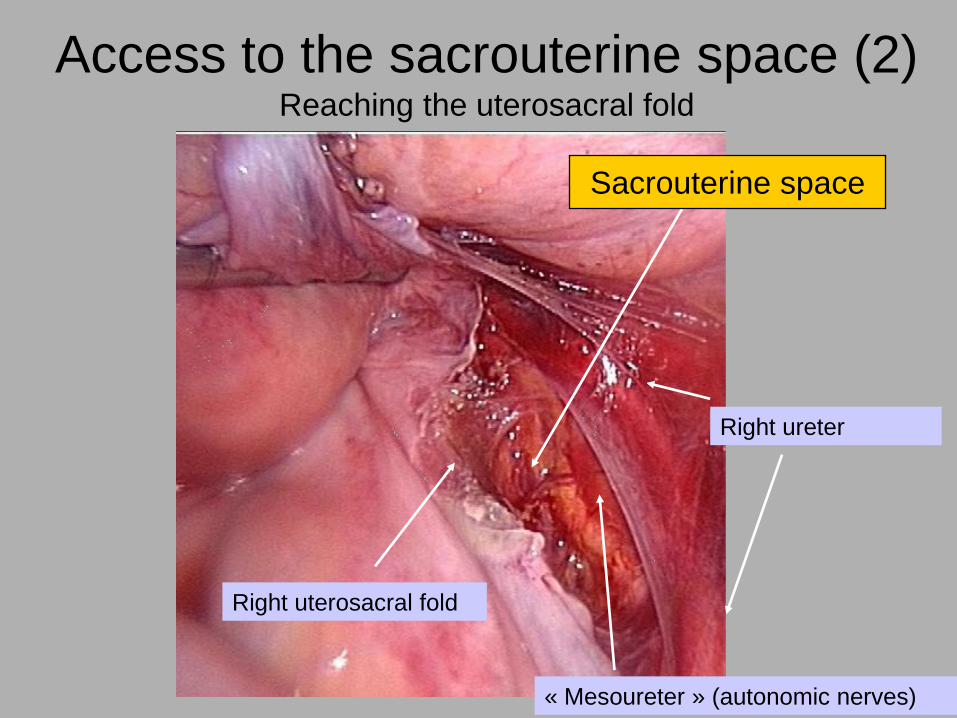
Right uterosacral fold
Right ureter
« Mesoureter » (autonomic nerves)
Access to the sacrouterine space (2)Reaching the uterosacral fold
Sacrouterine space
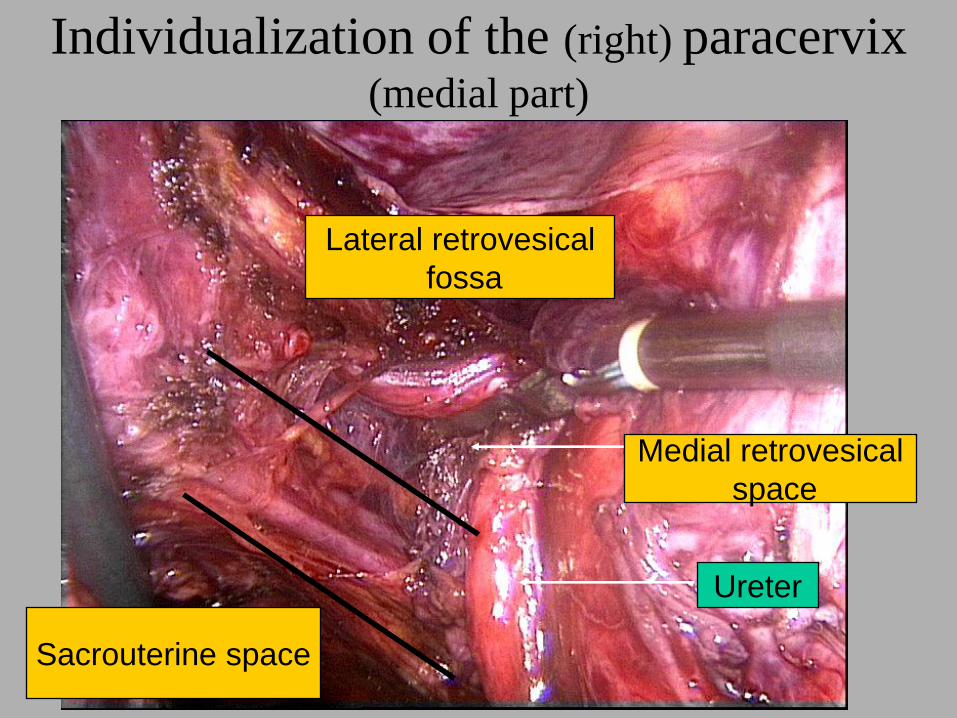
Individualization of the (right) paracervix (medial part)
Lateral retrovesical
fossa
Medial retrovesical
space
Sacrouterine space
Ureter
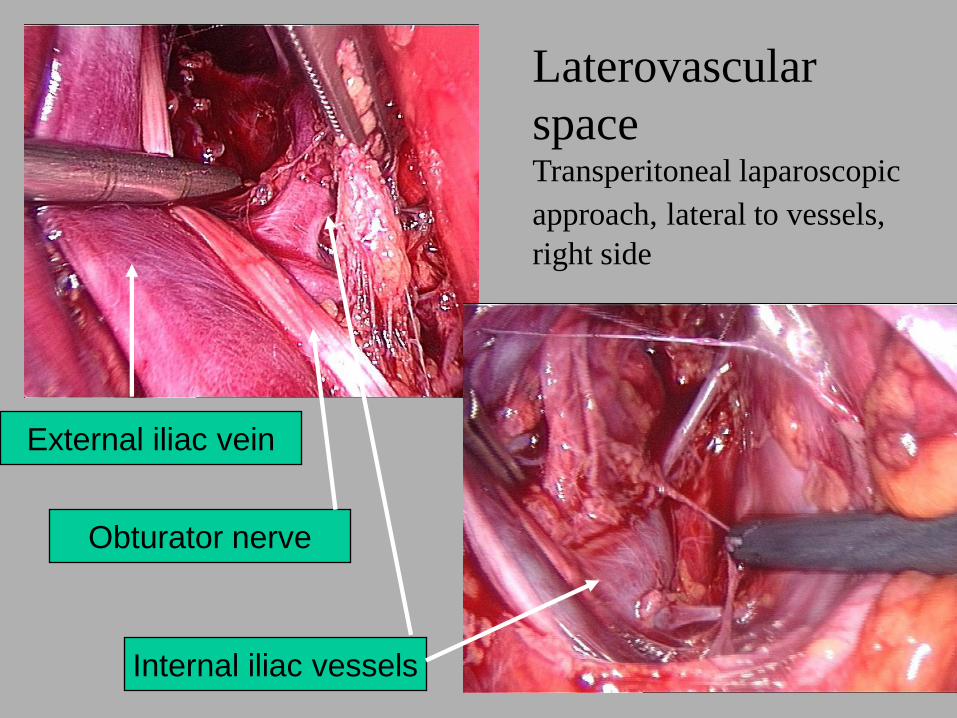
Laterovascular
spaceTransperitoneal laparoscopic
approach, lateral to vessels,
right side
External iliac vein
Obturator nerve
Internal iliac vessels
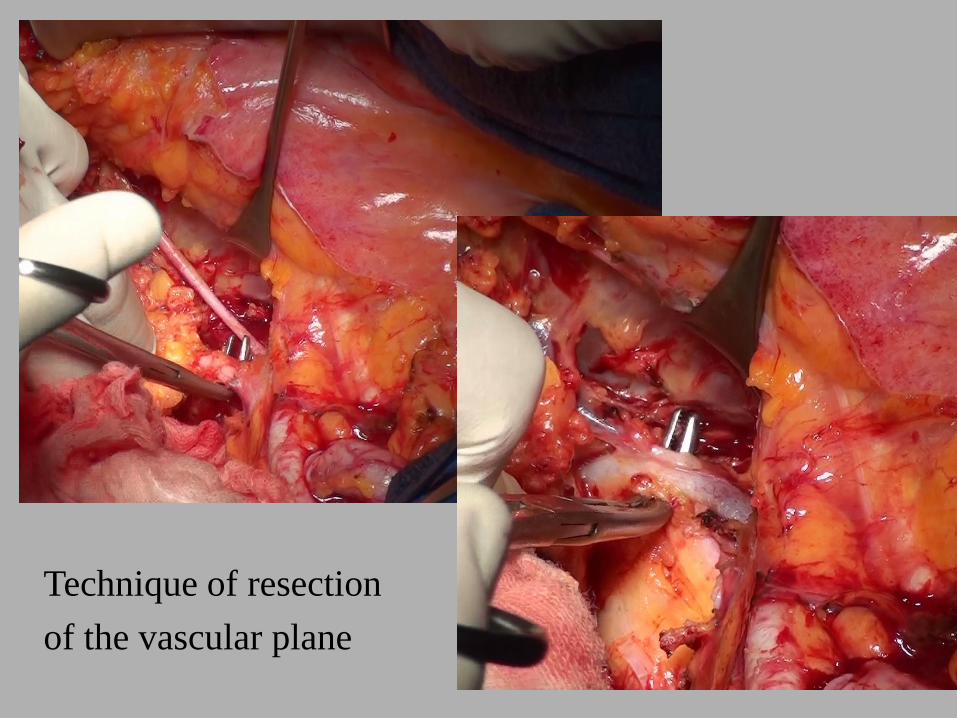
Technique of resection
of the vascular plane
(Mibayashi 1942)
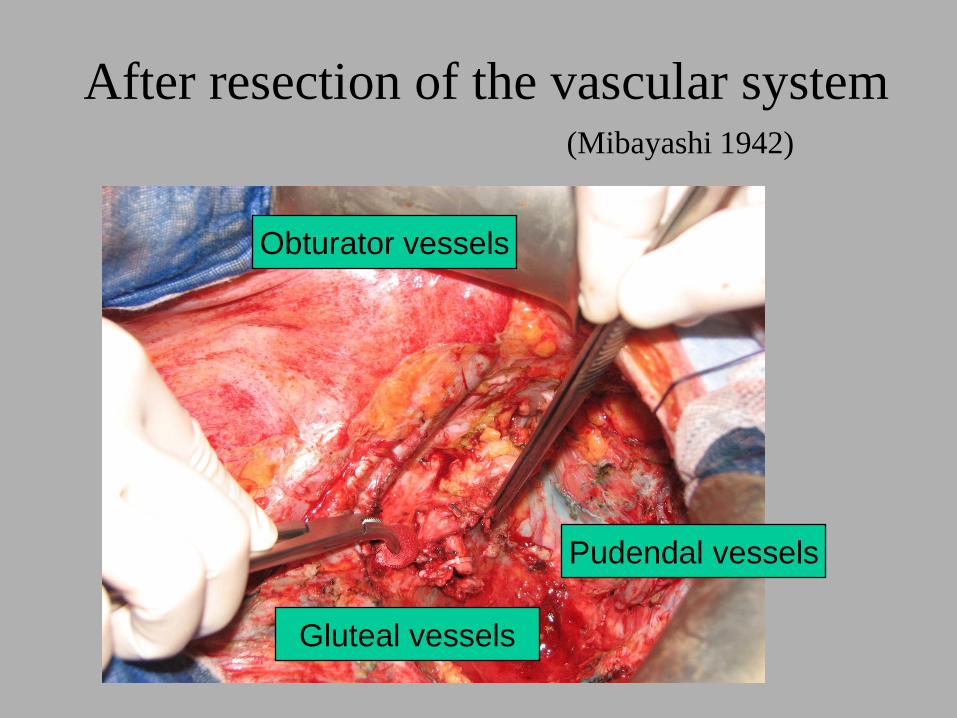
After resection of the vascular system
Obturator vessels
Pudendal vessels
Gluteal vessels
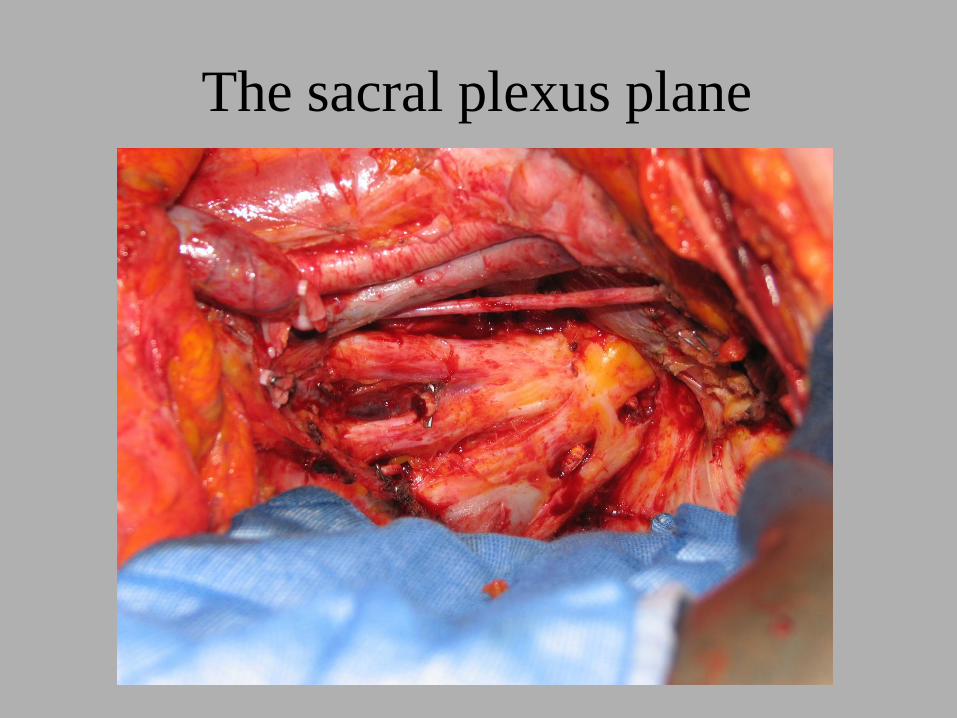
The sacral plexus plane
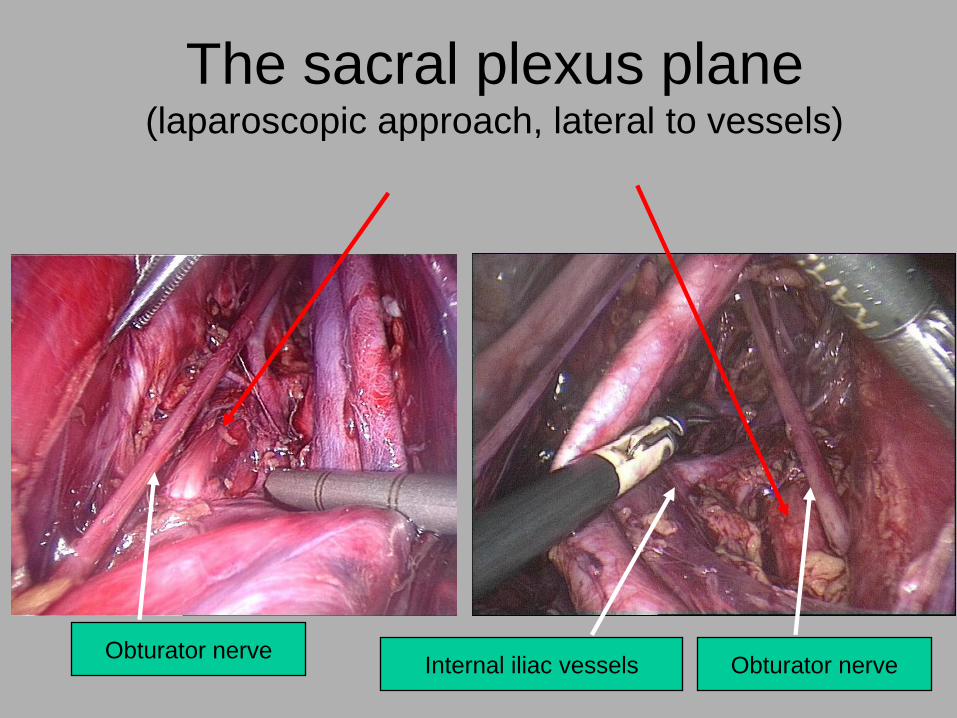
The sacral plexus plane(laparoscopic approach, lateral to vessels)
Obturator nerveObturator nerveInternal iliac vessels
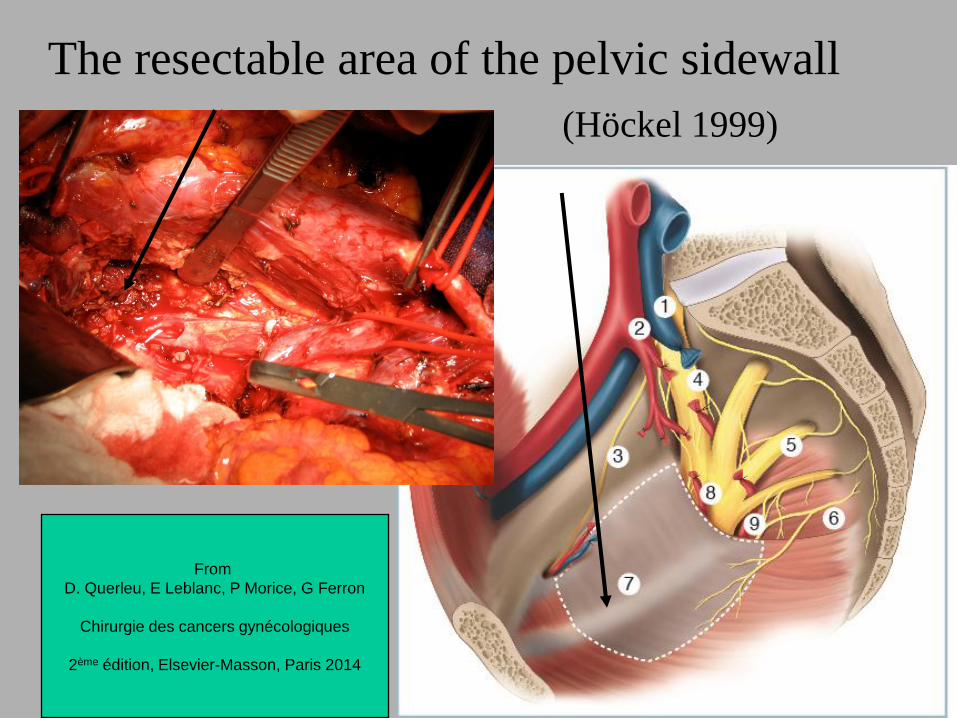
The resectable area of the pelvic sidewall
(Höckel 1999)
From
D. Querleu, E Leblanc, P Morice, G Ferron
Chirurgie des cancers gynécologiques
2ème édition, Elsevier-Masson, Paris 2014
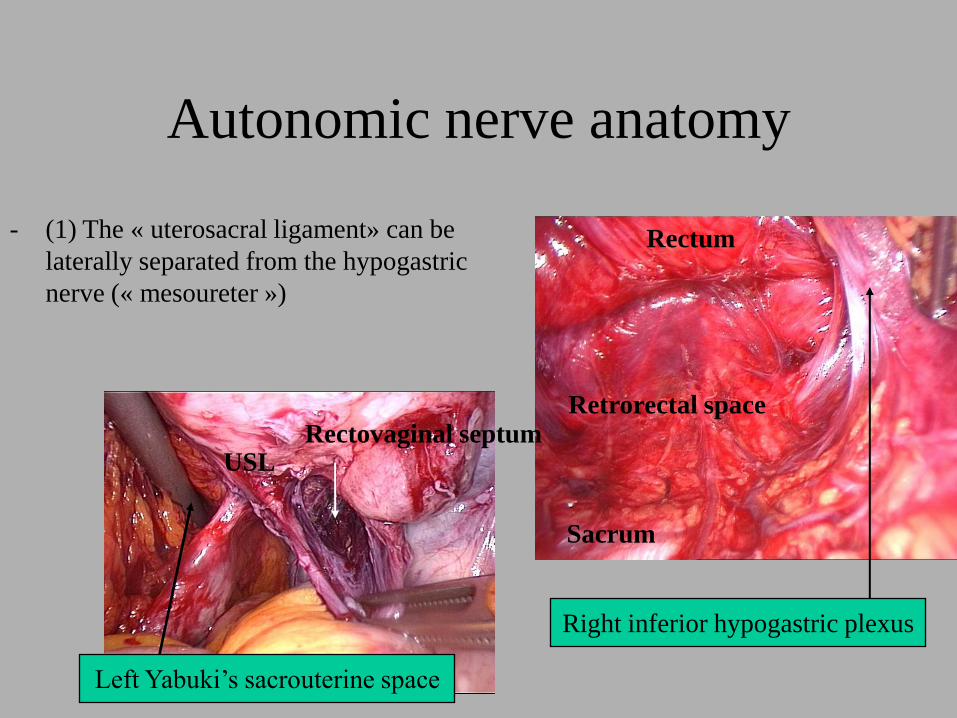
Autonomic nerve anatomy
- (1) The « uterosacral ligament» can be
laterally separated from the hypogastric
nerve (« mesoureter »)
Left Yabuki’s sacrouterine space
Right inferior hypogastric plexus
Rectovaginal septumUSL
Retrorectal space
Rectum
Sacrum
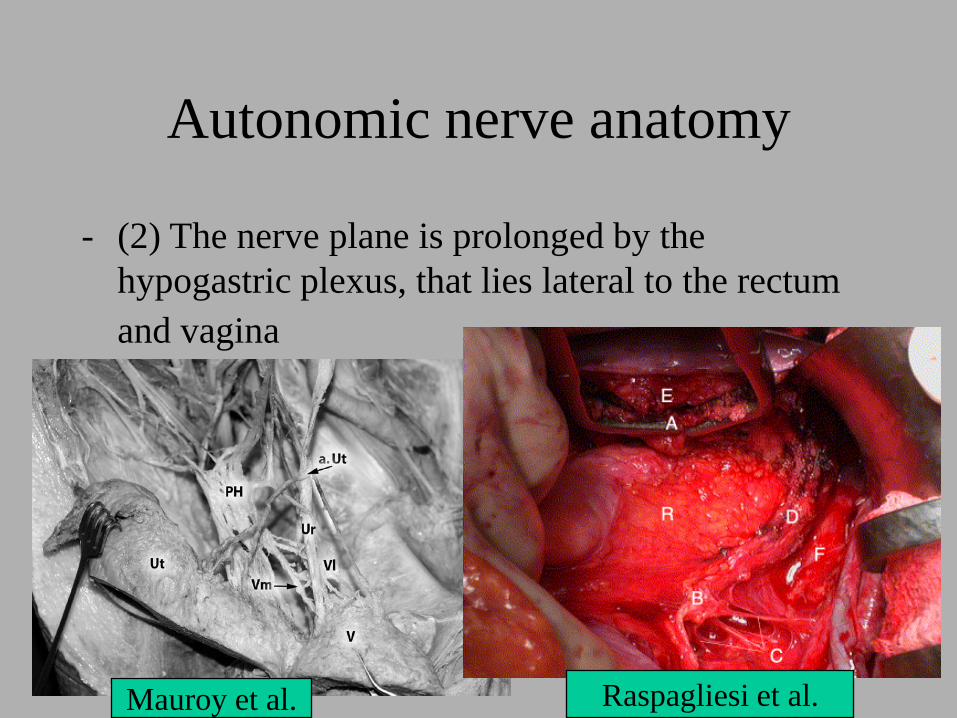
Autonomic nerve anatomy
- (2) The nerve plane is prolonged by the
hypogastric plexus, that lies lateral to the rectum
and vagina
Mauroy et al. Raspagliesi et al.
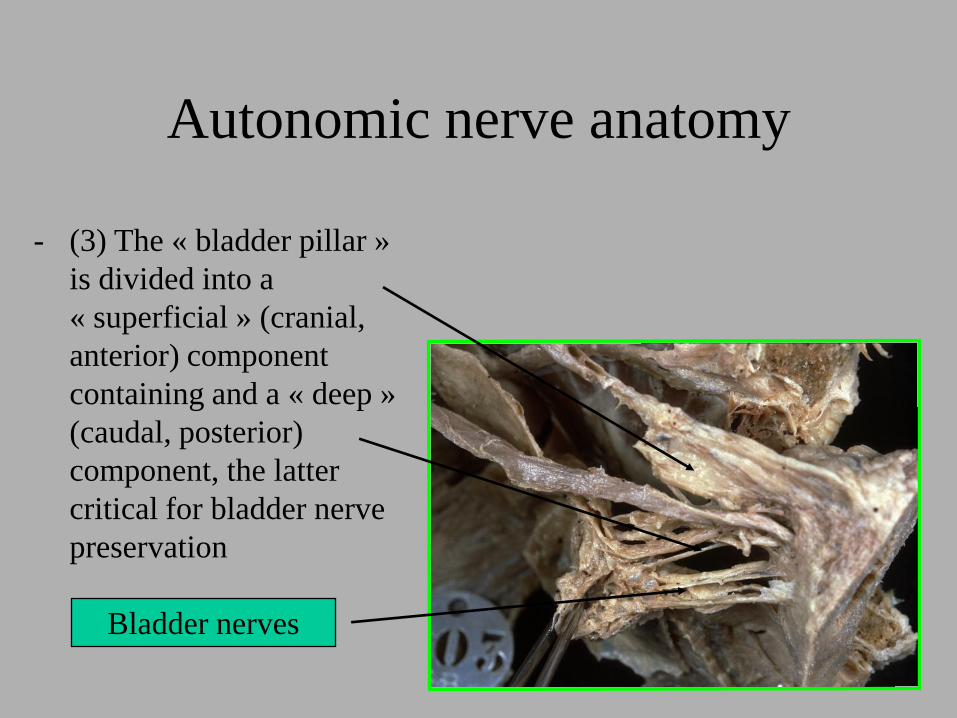
Autonomic nerve anatomy
- (3) The « bladder pillar »
is divided into a
« superficial » (cranial,
anterior) component
containing and a « deep »
(caudal, posterior)
component, the latter
critical for bladder nerve
preservation
Bladder nerves
PART 2 : A « NEW » WAY TO
MANAGE THE PARACERVIX
(« cardinal ligament ») :
PARACERVICAL
LYMPHADENECTOMY
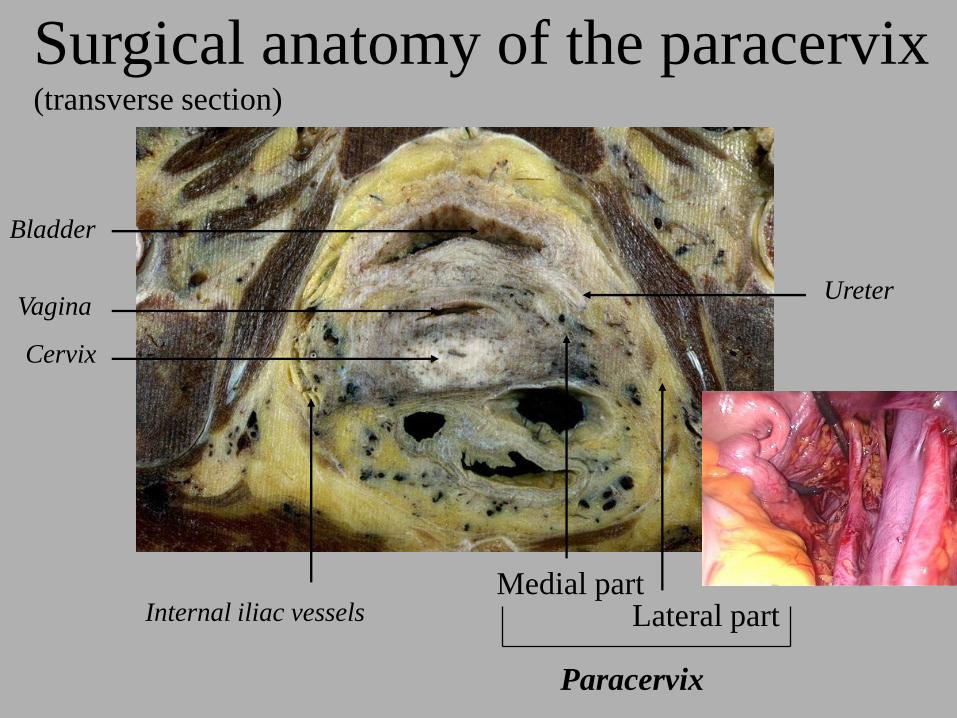
Ureter
Surgical anatomy of the paracervix(transverse section)
Bladder
Vagina
Cervix
Medial partLateral partInternal iliac vessels
Paracervix
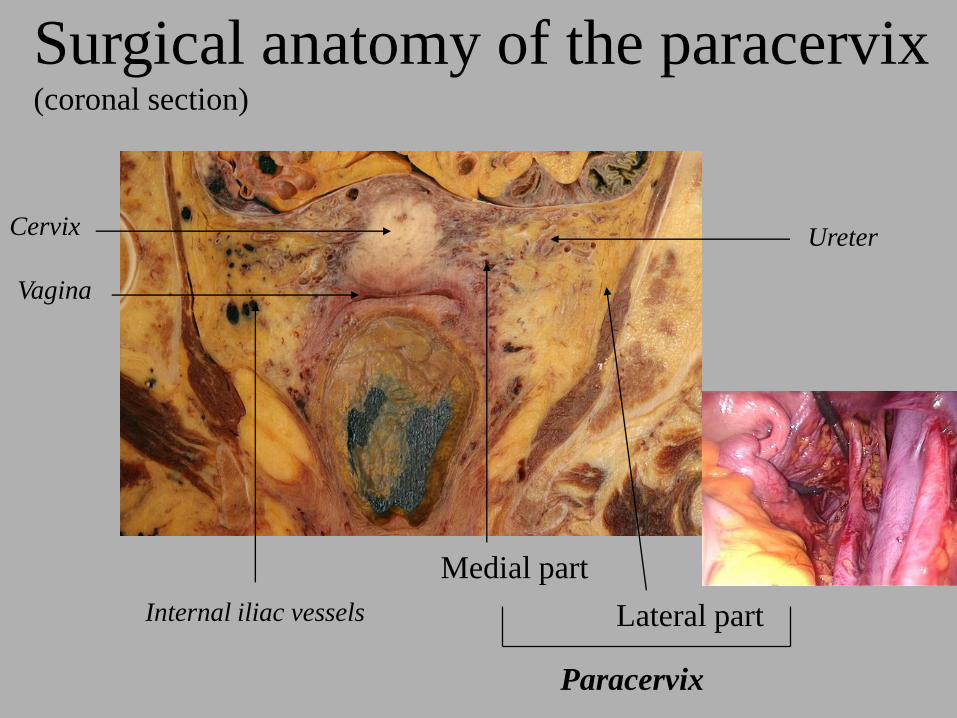
Ureter
Surgical anatomy of the paracervix(coronal section)
Vagina
Cervix
Medial part
Lateral partInternal iliac vessels
Paracervix
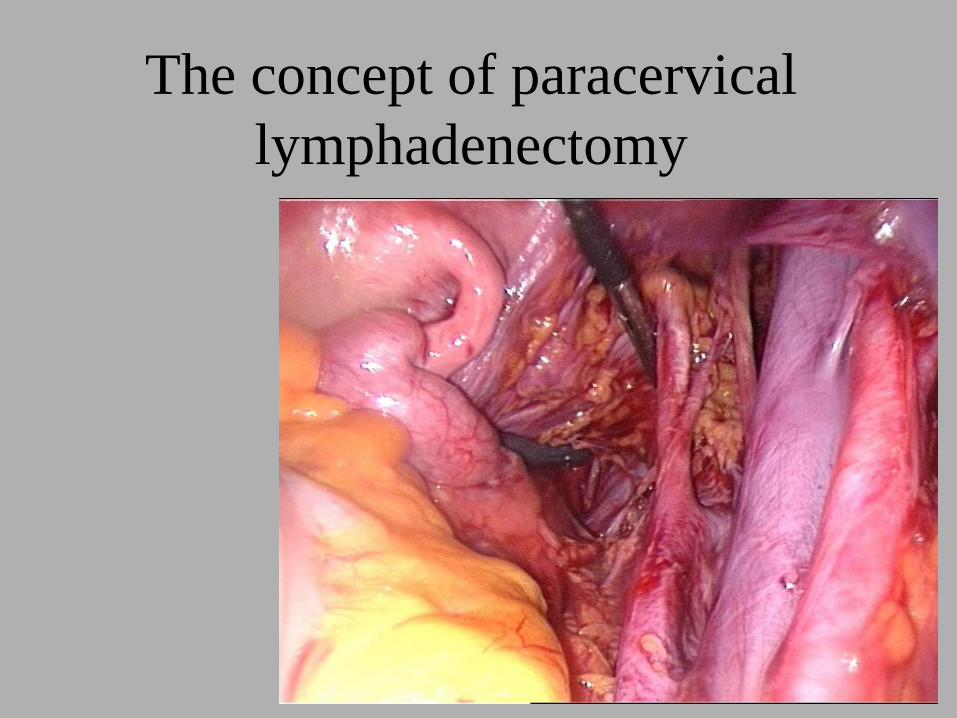
The concept of paracervical
lymphadenectomy
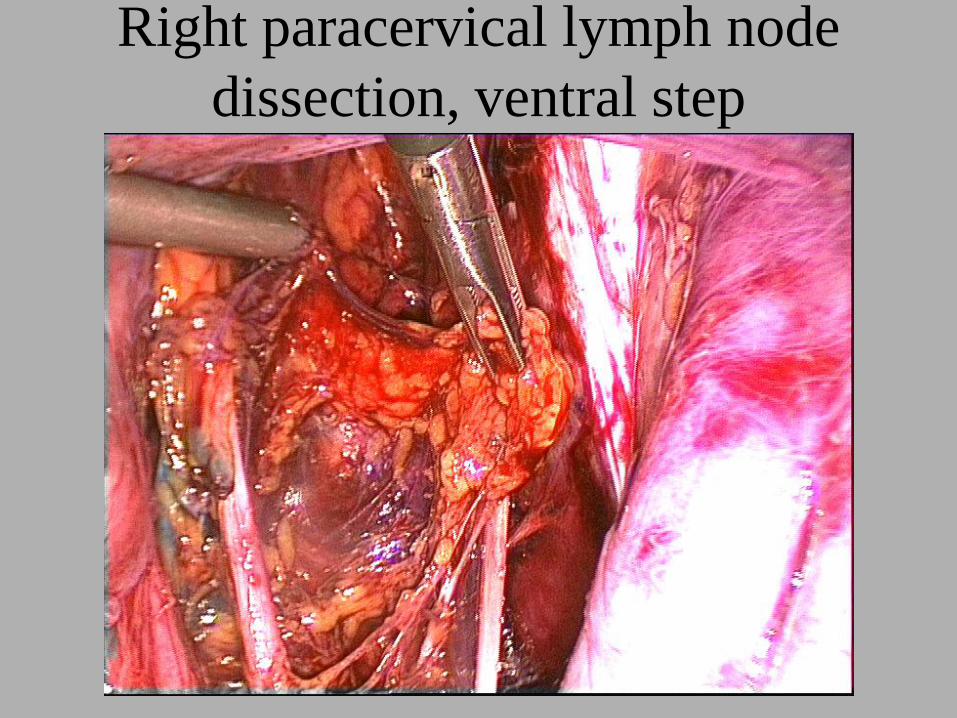
Right paracervical lymph node
dissection, ventral step
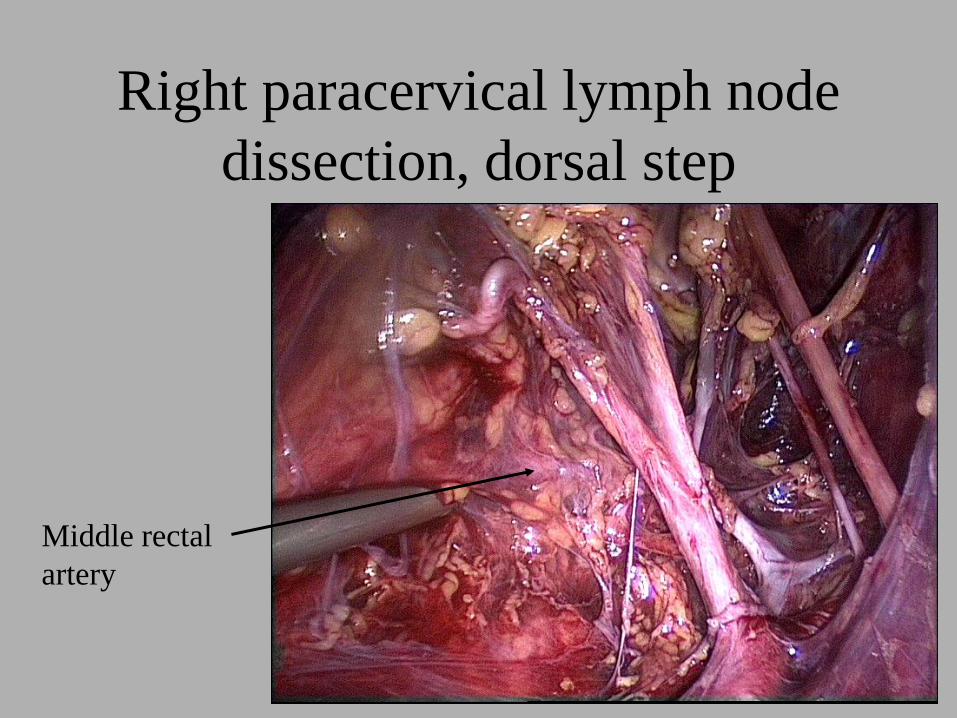
Right paracervical lymph node
dissection, dorsal step
Middle rectal
artery
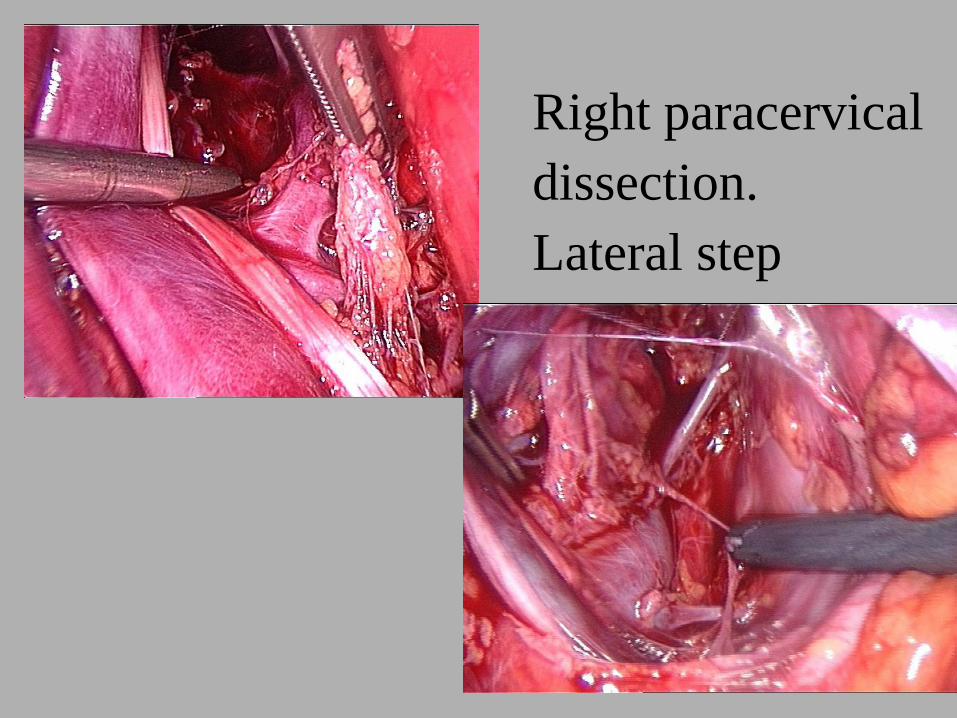
Right paracervical
dissection.
Lateral step
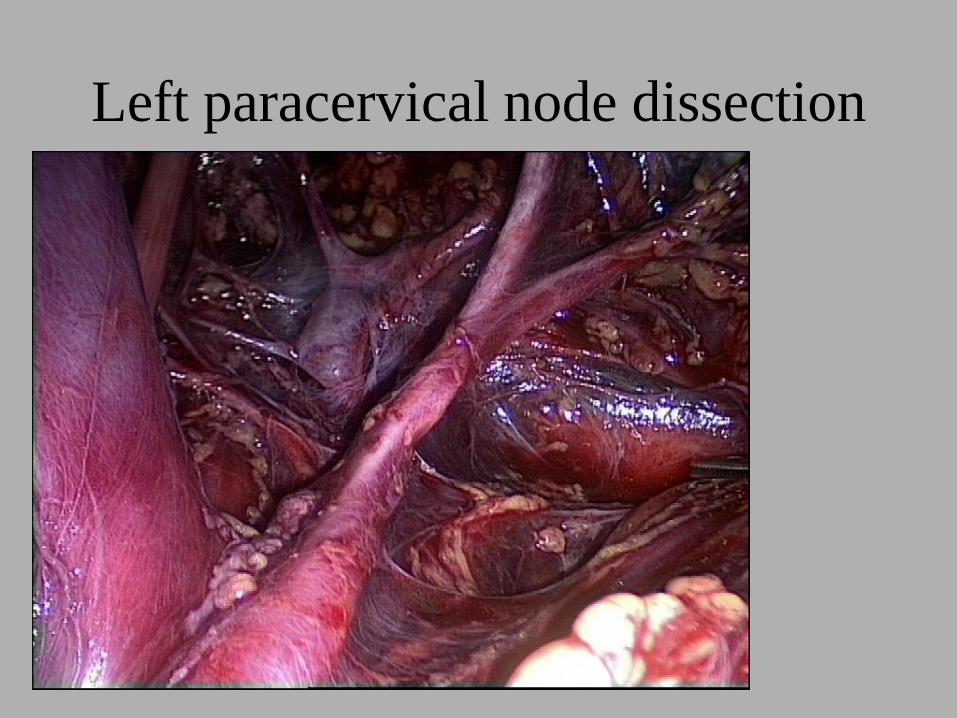
Left paracervical node dissection
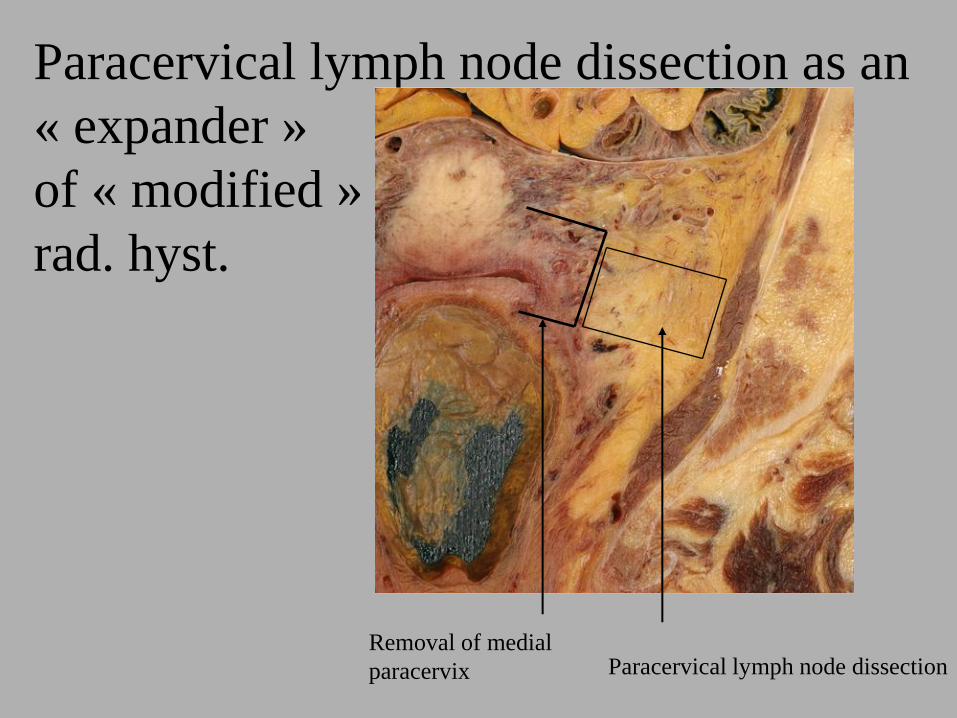
Paracervical lymph node dissection as an
« expander »
of « modified »
rad. hyst.
Removal of medial
paracervix Paracervical lymph node dissection
PART 3 : ANATOMICAL
CLASSIFICATION OF
RADICAL HYSTERECTOMIES
• Tailoring has become a major issue
in cancer surgery (adverse vs
curative effects)
• « Extended » or « radical »
hysterectomies encompass a variety
of different surgeries
• Eponyms are altered with time
Need for a new classification
• Piver/Rutledge/Smith
– Does not take into account Terminologia Anatomica
– Ignores nerve preservation techniques
– Applies to open surgery only
– Mixes lateral, dorsal, and vaginal extent
– Class I is not « radical » ; Class III and IV are not
clearly defined ; Class V is obsolete
– Templates are not clear

Need for a new classification
• Piver/Rutledge/Smith : unclear sketches
Need for standardization of
anatomical nomenclature
• (1) Spatial orientation in the pelvis according to the international anatomical nomenclature
– Medial / lateral
– Caudal / cranial
– Dorsal/ventral
• (2) Adopt a uniform name for the lateral attachments of the cervix and upper vagina : paracervix (Nomina Anatomica)
– Avoiding confusing terms as « cardinal ligament », « Mackenrodt’s ligament », « lateral parametrium »
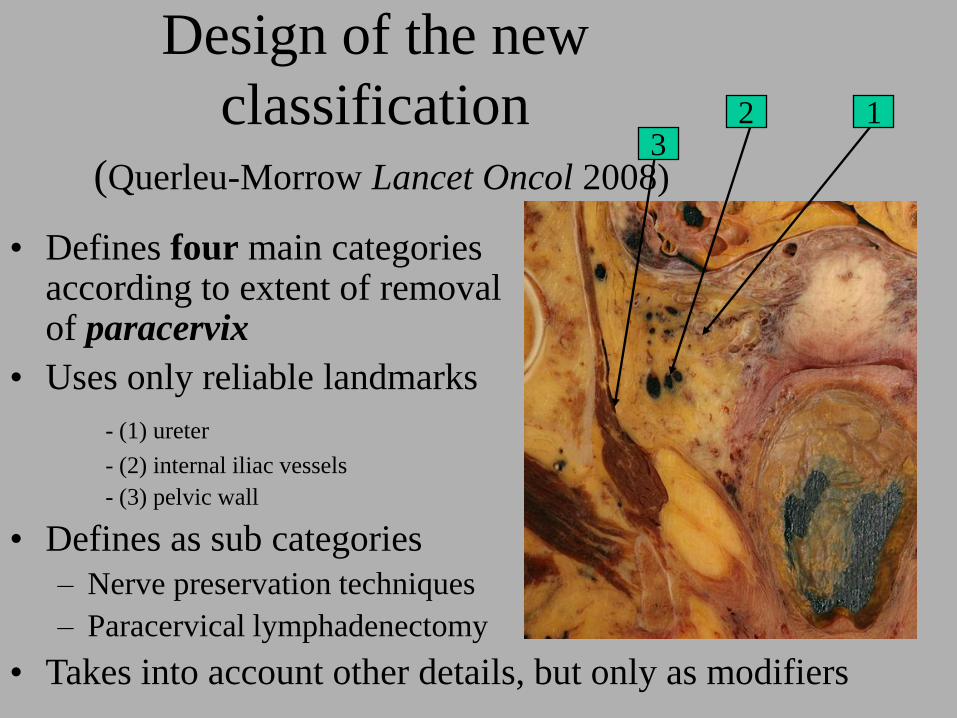
Design of the new
classification(Querleu-Morrow Lancet Oncol 2008)
• Defines four main categories according to extent of removal of paracervix
• Uses only reliable landmarks
- (1) ureter
- (2) internal iliac vessels
- (3) pelvic wall
• Defines as sub categories
– Nerve preservation techniques
– Paracervical lymphadenectomy
• Takes into account other details, but only as modifiers
123
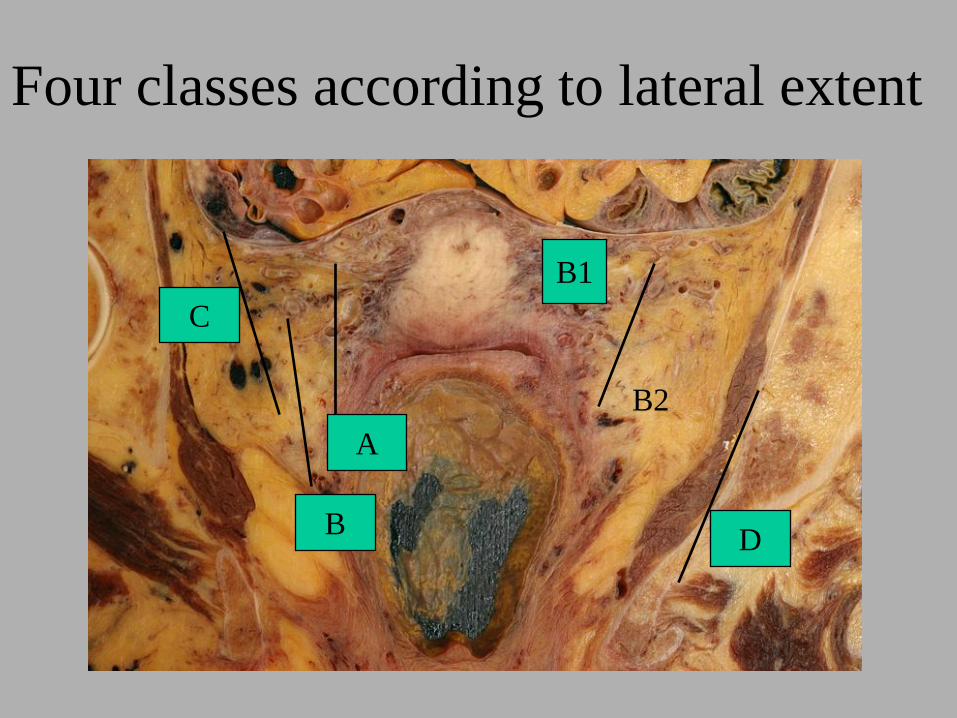
Four classes according to lateral extent
AC
B
D
C
B
A
B1
B2
D
The four categories
• Class A : minimal resection of paracervix cervix removed in toto
• Class B : resection of the paracervix at the ureter resection of the fibrous component
• Class C : resection of the paracervix at the pelvic sidewall resection of entire paracervix
• Class D : extension of resection to the anatomical structures of the pelvic sidewall exenterative procedures
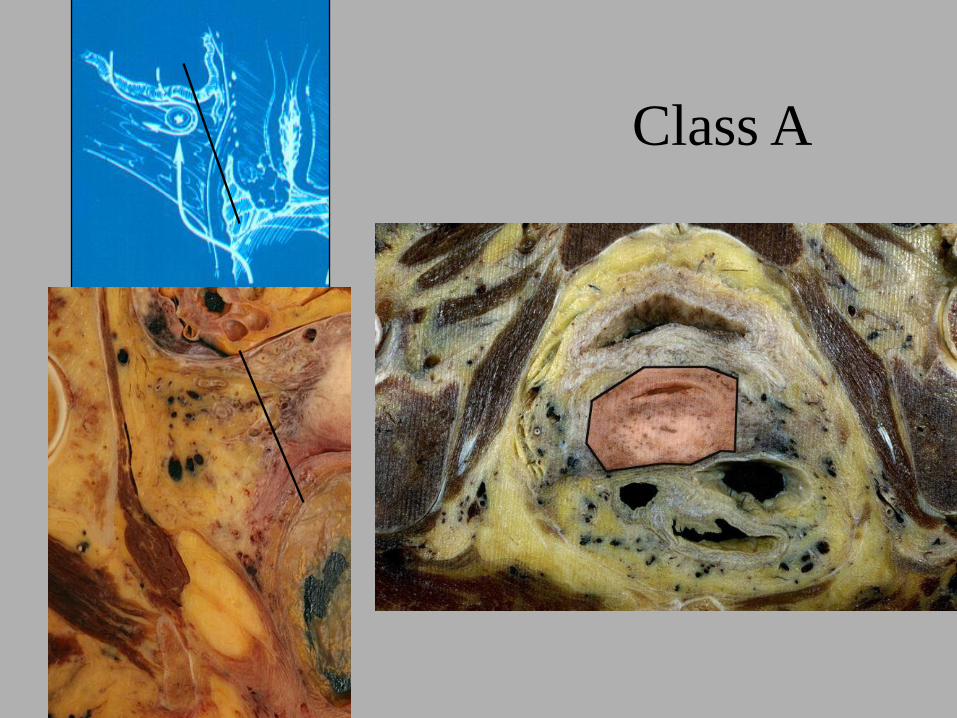
Class A : the paracervix is transected
medial to the ureter but lateral to the cervix
(half-way)
– Extrafascial hysterectomy in which the position of the
ureters is determined by palpation or direct vision (after
opening the ureteral tunnels) without freeing the ureters
from their beds
– The bladder and rectal pillar are not transected at a
distance from the uterus
• Goal : make sure that the cervix has been removed
in toto by a gynecologic oncologist
Class A
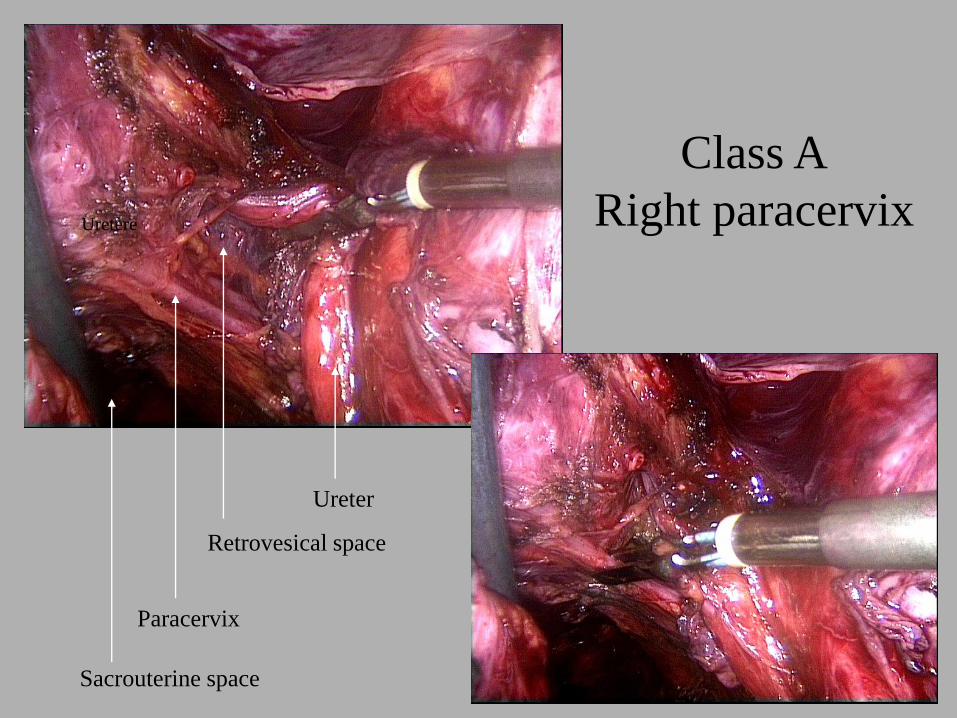
Class A
Right paracervix
Ureter
Uretère
Paracervix
Retrovesical space
Sacrouterine space
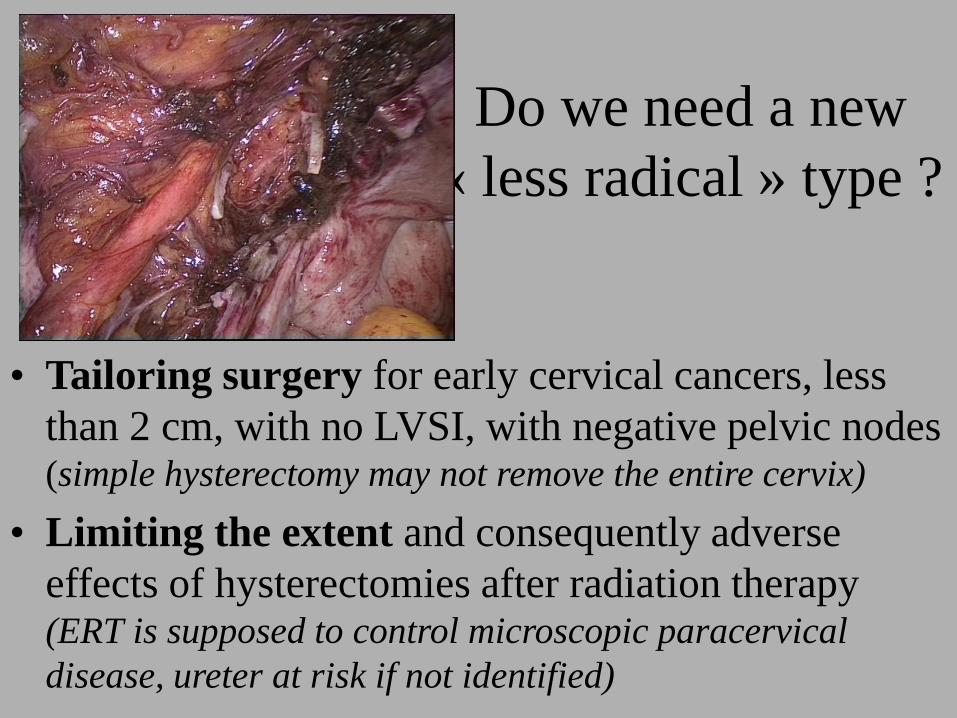
Do we need a new
« less radical » type ?
• Tailoring surgery for early cervical cancers, less
than 2 cm, with no LVSI, with negative pelvic nodes (simple hysterectomy may not remove the entire cervix)
• Limiting the extent and consequently adverse
effects of hysterectomies after radiation therapy (ERT is supposed to control microscopic paracervical
disease, ureter at risk if not identified)
Class B : the paracervix is divided at the
ureter
– The ureter is unroofed and rolled laterally permitting transection of the paracervix at the level of the ureteral tunnel
– The neural component of the paracervix is not transected
– The bladder and rectal pillars are resected at a distance from the uterus
– Subcategories : B1 : as described
B2 : with additional lateral paracervical lymph node dissection or liposuction.
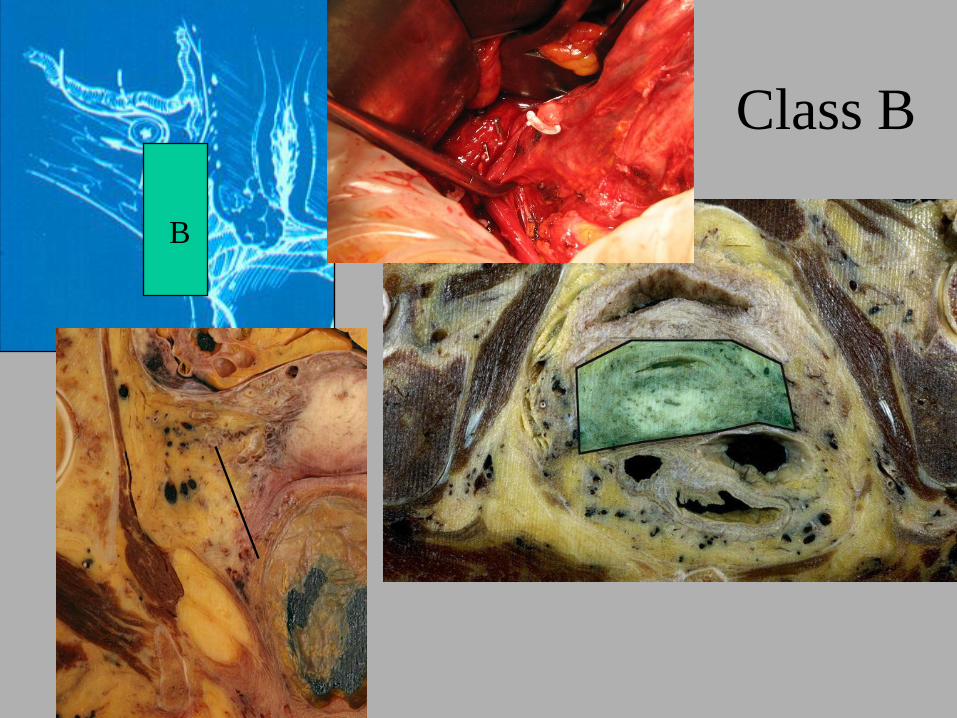
Class B
B

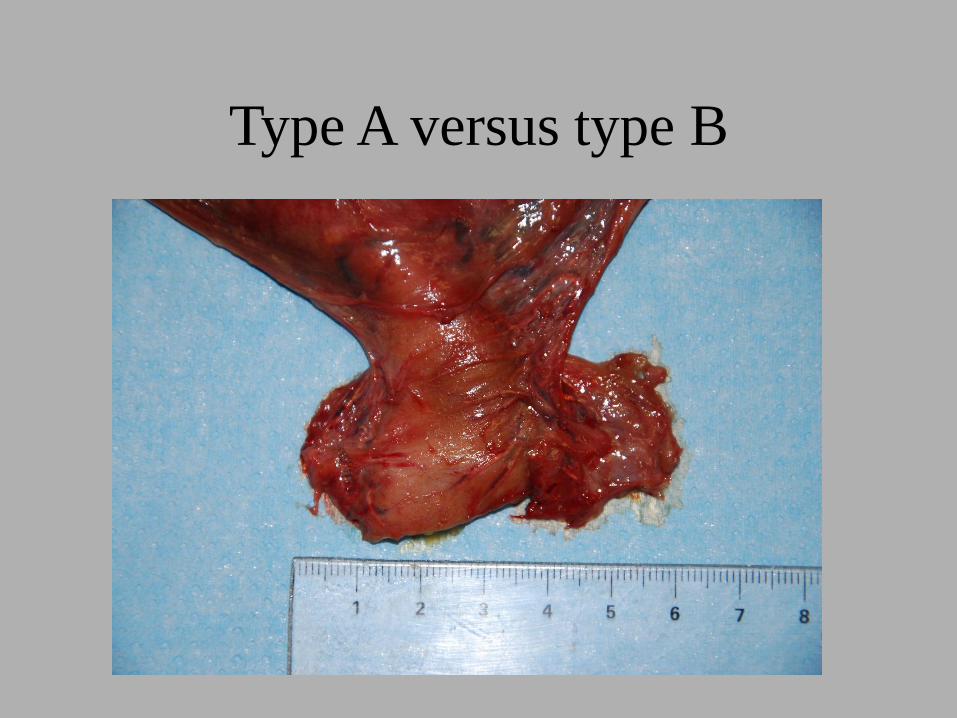
Type A versus type B
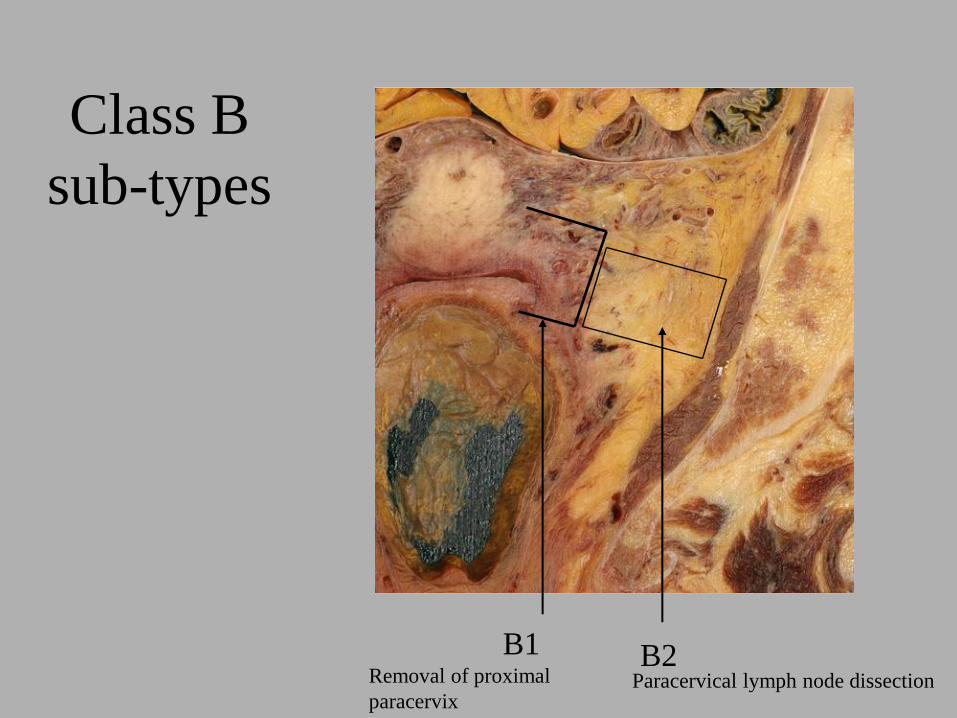
Class B
sub-types
B1 B2Removal of proximal
paracervixParacervical lymph node dissection
Class C : Resection of the
paracervix at the junction with
hypogastric vessels
- Resection of the rectal pillar at the rectum and
bladder pillar at the bladder
- The ureter is completely mobilized.
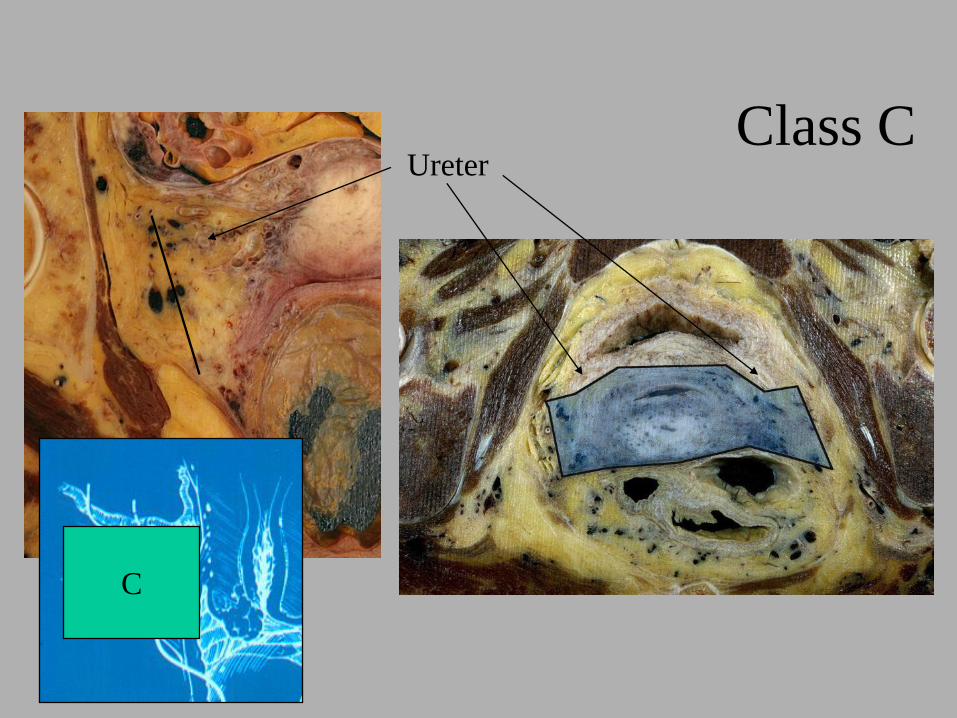
Class CUreter
C
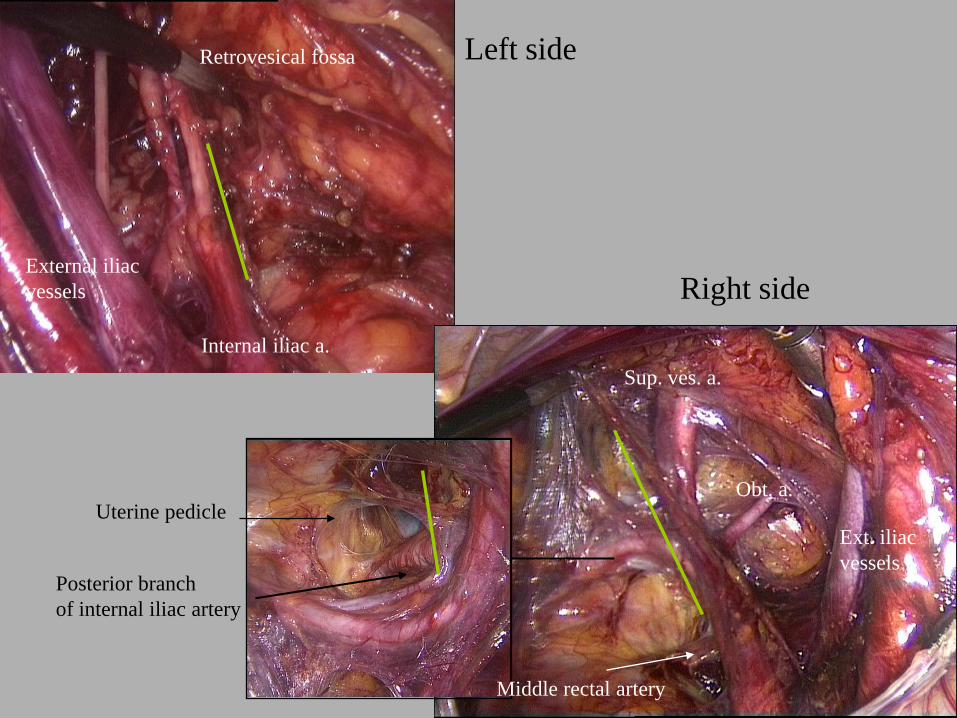
Left side
Right side
Posterior branch
of internal iliac artery
Middle rectal artery
Uterine pedicle
Sup. ves. a.
Obt. a.
Ext. iliac
vessels
External iliac
vessels
Retrovesical fossa
Internal iliac a.
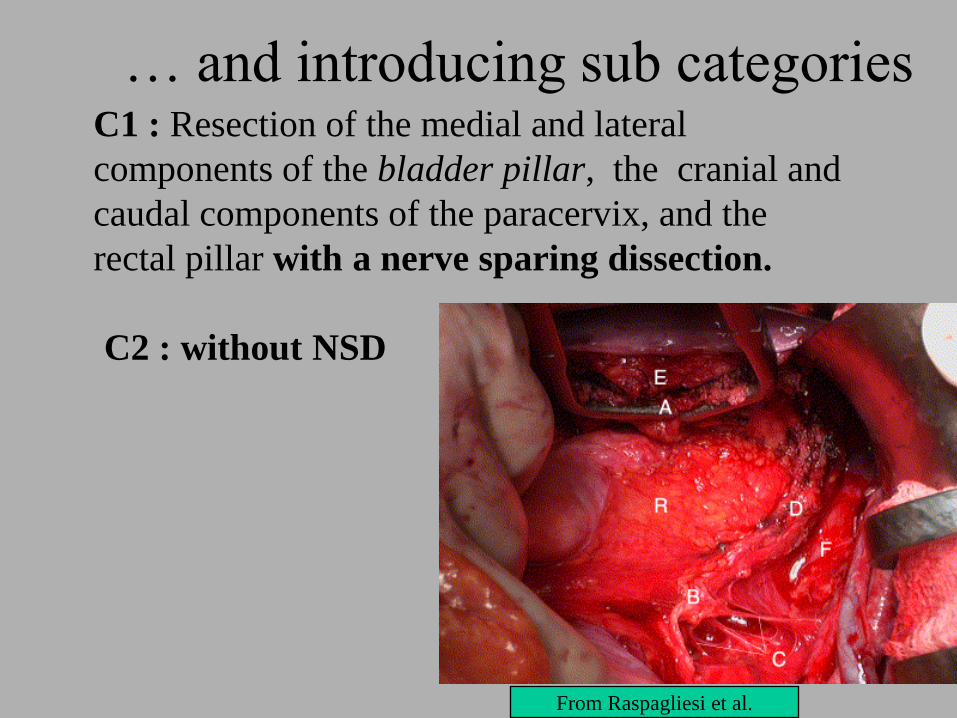
… and introducing sub categoriesC1 : Resection of the medial and lateral
components of the bladder pillar, the cranial and
caudal components of the paracervix, and the
rectal pillar with a nerve sparing dissection.
C2 : without NSD
From Raspagliesi et al.
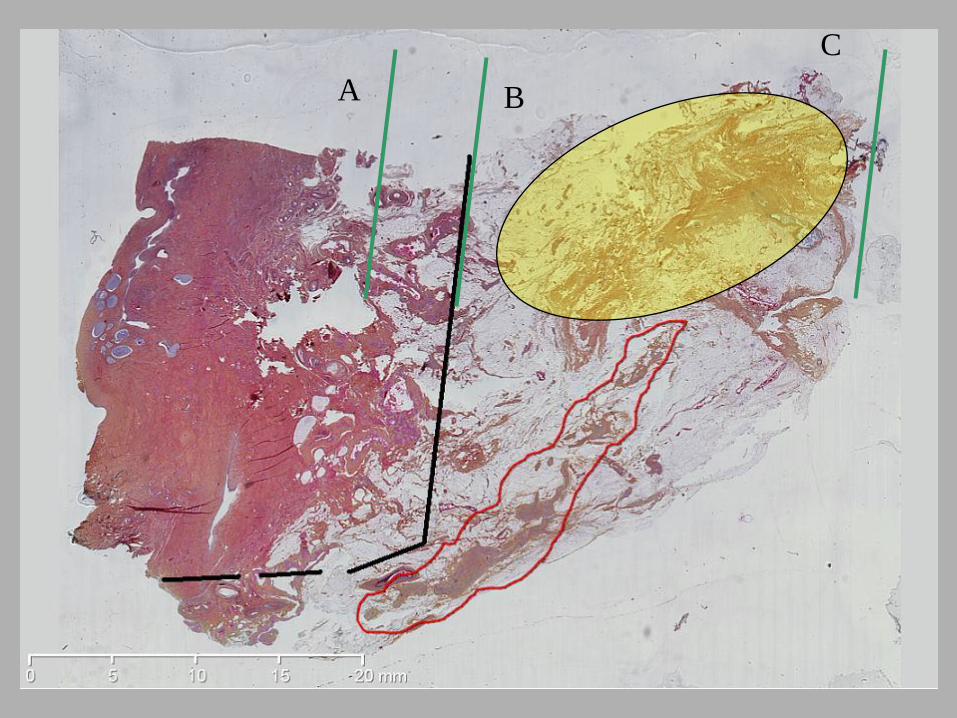
A B
C