Embed Size (px)
Citation preview
611
Chapter 22
THE POST ANESTHESIA CARE UNIT (PACU)
Susan Fossum RN, CPAN, Maria Pedersen RN, and George A Gregory, MD
Introduction
Within a year of anesthesia’s discovery, it was recognized that patients recovering from anesthesia develop problems that require care in a specialized unit. However, it took many years for this concept to spread to most of the developing world. It only did so when Beecher and Todd documented fewer deaths in hospitals that had PACUs.1 All hospitals in these countries now have a PACU staffed by nurses specially trained to care for patients recovering from anesthesia and surgery. This training is important because it is the PACU staff that provides the minute-to-minute postoperative care and must understand how patients recover from anesthesia. Even with this knowledge, in many parts of the world today, patients still recover from anesthesia in their bed on the ward, not in a post anesthesia care unit (PACU), with family providing the postoperative care. Many low resource countries have yet to establish a PACU in their hospitals, but should do so because more than half of perioperative cardiac arrests occur in the few hours after anesthesia and surgery end.2 If this occurs on the ward, resuscitation will be less effective.
The goal of this chapter is to provide information on the PACU care of infants and children and to provide information for people who wish to develop a PACU.
Organization of the PACU
The purpose of a PACU is to provide a safe environment where potential or real complications of anesthesia and surgery can be detected immediately and treated. This requires a room dedicated to the early postoperative care of patients. This room should be located near the operating rooms. Most importantly, the room must be continuously staffed with enough well trained nurses who are expert in interpreting and responding to the events that occur during recovery from anesthesia. PACU nurses should be trained in airway management, basic life support, and training specific to caring for the special needs of postoperative patients emerging from anesthesia. Each PACU requires a readily available source of oxygen and a means of delivering that oxygen to multiple patients at the same time when necessary. A bag valve mask must be readily available for airway management, along with masks of different sizes. Drugs (including those needed for resuscitation from cardiac arrest) must also be readily available to everyone providing care in the
Chapter 22: THE POST ANESTHESIA CARE UNIT (PACU)
612
PACU. Nurses should be trained to start IVs because children sometimes dislodge their I.V.s. Maintenance of body temperature is also important, which means a means of warming and cooling a patient is required. Since vomiting is a common occurrence after anesthesia and surgery, a suction device and a supply of suction catheters are needed to remove vomited material from the mouth and upper airway. Electronic monitors are important as they help nurses detect and treat problems before they become serious.
PACUs require a nursing and medical director (usually an anesthetist) to assure efficient and effective functioning of the unit. The two directors are not only responsible for the day-to-day running of the unit; they are also responsible for the education of the staff. They also must interact with the hospital administration to obtain needed personnel, medications, and equipment.
Equipment
The most important monitor in the PACU is the nurse who looks at the patient and interprets what he/she sees. Other monitors provide information that aids nurses in assessing the patient’s condition, but they certainly do not replace the nurse. Important considerations when purchasing any monitor includes whether the monitor can be repaired immediately if it breaks, who will repair it, and how long will it take to do the repairs? Can the repairs be done in the city/town/hospital where the monitor is used? Monitors should not be purchased unless the answers to these questions are clearly known. Otherwise, when the monitor breaks it will sit in a closet and never be used again. The following is a discussion of monitors commonly used during the PACU care of patients.
Pulse Oximeters
Trying to determine the level of oxygenation by looking at the patient’s skin color is not very effective. Physicians and nurses are no better at this than untrained family members. The oxygen saturation (SpO2) must be 80%-85% before everyone will agree that the patient is hypoxemic. If looking at skin color is the only method available for assessing oxygenation, the accuracy of the method can be improved by assessing the color of the mucus membranes of the lower eyelid, not the skin. The mucus membranes of the eyelids are less pigmented and have a larger number of capillaries, therefore, there are fewer effects on tissue color.
The presence of hypoxemia is best determined by measuring SpO2 with a pulse oximeter. These are small, lightweight, sturdy, and noninvasive devices that provide immediate information about oxygenation. They allow nurses and others to quickly respond to decreased levels of oxygen, correct its cause, and prevent serious injury to the patient. For these reasons, they are widely used in operating rooms, PACUs, ICUs, and patient wards to assess oxygenation. They seldom break down but must have their batteries replaced occasionally. Most oximeters are inexpensive
Anesthesia Care of Pediatric Patients (George A. Gregory & Dean B. Andropoulos)
613
and, depending on the manufacturer, work on both batteries and electricity from the wall. While SpO2 monitors are not affected by skin color or jaundice, they are severely affected by low cardiac output and hypothermia. Both low output and hypothermia reduce blood flow under the probe, and this reduces accuracy of the SpO2 measurement. To measure SpO2, these monitors are usually placed on a finger, ear, or, in the case of infants, a hand or foot.
How Pulse Oximeters Work
Pulse oximeters consist of a computer processor, two diodes (LEDs) that emit light at different wavelengths, and a photodiode that collects light that passes through the finger, ear, hand or foot (Figure 22-1). One wavelength is 660nm (red) and the other is 940nm (ultra violate). Oxygenated (arterial) and unoxygenated (venous) blood absorbs light at different wavelengths. The photodiode opposite the LEDs measures the amount of light that passes through and is not absorbed by the tissues between the LEDs and the photodiode. This measurement fluctuates over time because the amount of arterial blood present between the two sensors increases slightly with each heartbeat. By subtracting the minimum amount of light transmitted from the maximum amount of light transmitted, the processor can correct for the effects of tissues other than blood vessels that are between the LEDs and photodiode. The ratio of red light to infrared light (which represents the ratio of oxygenated hemoglobin to deoxygenated hemoglobin) is calculated by the processor and converted to SpO2.
Chapter 22: THE POST ANESTHESIA CARE UNIT (PACU)
614
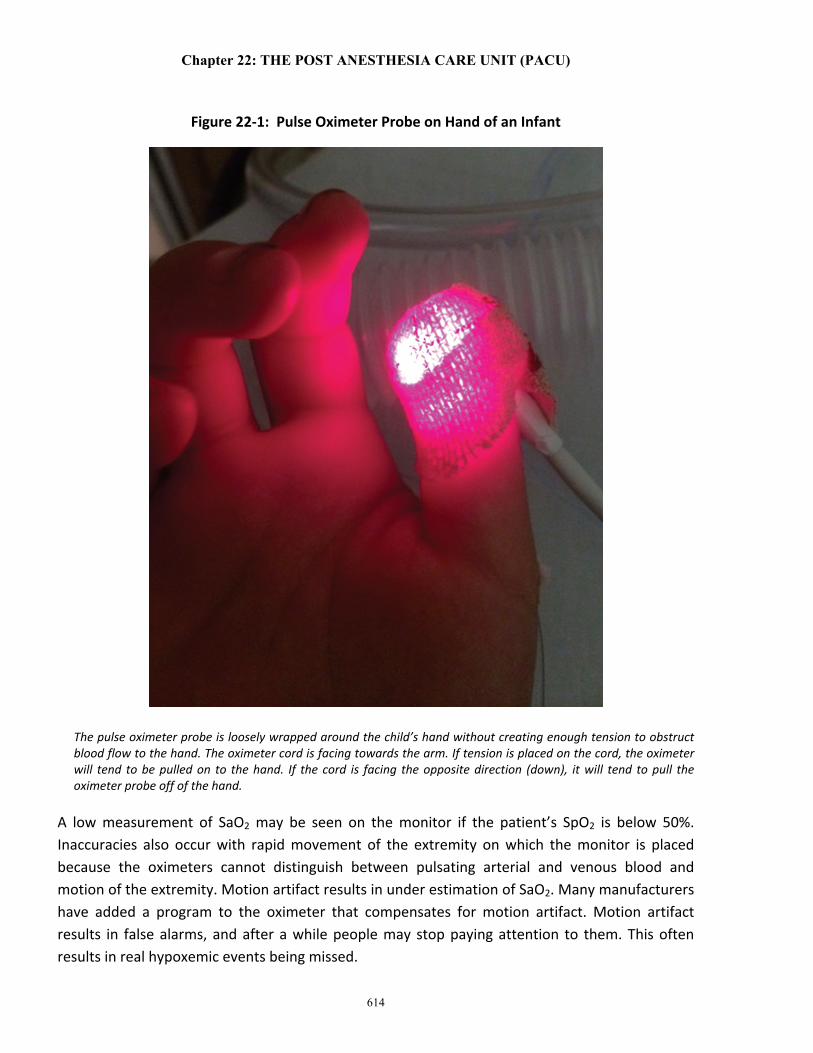
Figure 22-1: Pulse Oximeter Probe on Hand of an Infant
The pulse oximeter probe is loosely wrapped around the child’s hand without creating enough tension to obstruct blood flow to the hand. The oximeter cord is facing towards the arm. If tension is placed on the cord, the oximeter will tend to be pulled on to the hand. If the cord is facing the opposite direction (down), it will tend to pull the oximeter probe off of the hand.
A low measurement of SaO2 may be seen on the monitor if the patient’s SpO2 is below 50%. Inaccuracies also occur with rapid movement of the extremity on which the monitor is placed because the oximeters cannot distinguish between pulsating arterial and venous blood and motion of the extremity. Motion artifact results in under estimation of SaO2. Many manufacturers have added a program to the oximeter that compensates for motion artifact. Motion artifact results in false alarms, and after a while people may stop paying attention to them. This often results in real hypoxemic events being missed.
Anesthesia Care of Pediatric Patients (George A. Gregory & Dean B. Andropoulos)
615
Pulse oximeters only measure hemoglobin oxygen saturation. They provide no measure of ventilation, work of breathing, or acidosis [carbon dioxide, pH, base deficit, or serum bicarbonate (HCO3
-)] concentrations. SpO2 only tells us the amount of oxygen in hemoglobin, which, however, is about 99% of all of the oxygen in the blood. During severe anemia, the amount of oxygen in blood (oxygen content) will be reduced, but the SpO2 will be normal because the amount of hemoglobin the patient has is fully saturated with oxygen. See Chapters 1 and 2 for further discussions of oxygen content and SaO2s determinations.
Most normal children have a SpO2 of 95%-to-100%. The SpO2 of preterm infants is usually maintained between 90%-to-95% because high levels of oxygen in their blood can cause blindness (retinopathy of prematurity).
Vital Signs Monitoring
Measuring heart rate (HR), arterial blood pressure (BP), and evaluating capillary refill time, arterial pulses, and skin temperature are a vital part of PACU assessment and help to determine the appropriate care needed. Electronic vital sign monitors are commonly used because they provide continuous heart rate and electrocardiogram (ECG) data and intermittent arterial blood pressures. Many of these monitors provide continuous SpO2 and end-tidal carbon dioxide monitoring also. These monitors are expensive and at times need repair.
If electronic monitors are not available, heart rate is measured by the time-honored method of counting the patient’s pulse for 60 seconds. It is common for the HR of normal patients to vary with pain, movement, and fear, all of which can occur in the PACU and must be frequently evaluated and treated. If an electronic monitor is not available, blood pressure should be measured with a cuff and sphygmomanometer. Normal values for HR and BP are shown in Appendix 1. When the skin of a finger or toe is compressed, the skin blanches. When the pressure is released, it takes less than two seconds for the capillaries to refill with blood in adults and less than three seconds for this to happen in babies and infants. This is called capillary refill and is a valuable method of determining vascular stability of a patient. Normal patients of all ages have pulses in all of their extremities. Absent or markedly reduced pulses often indicate poor tissue perfusion, as does cool skin temperature (See Chapter 1). The heart tones should be easily heard and crisp. Distant or weak heart sounds, suggest reduced myocardial contractility. Lung assessment is done by listening to the breath sounds. Lung sounds are either normal or abnormal (wheezing, crackles and rhonchi).
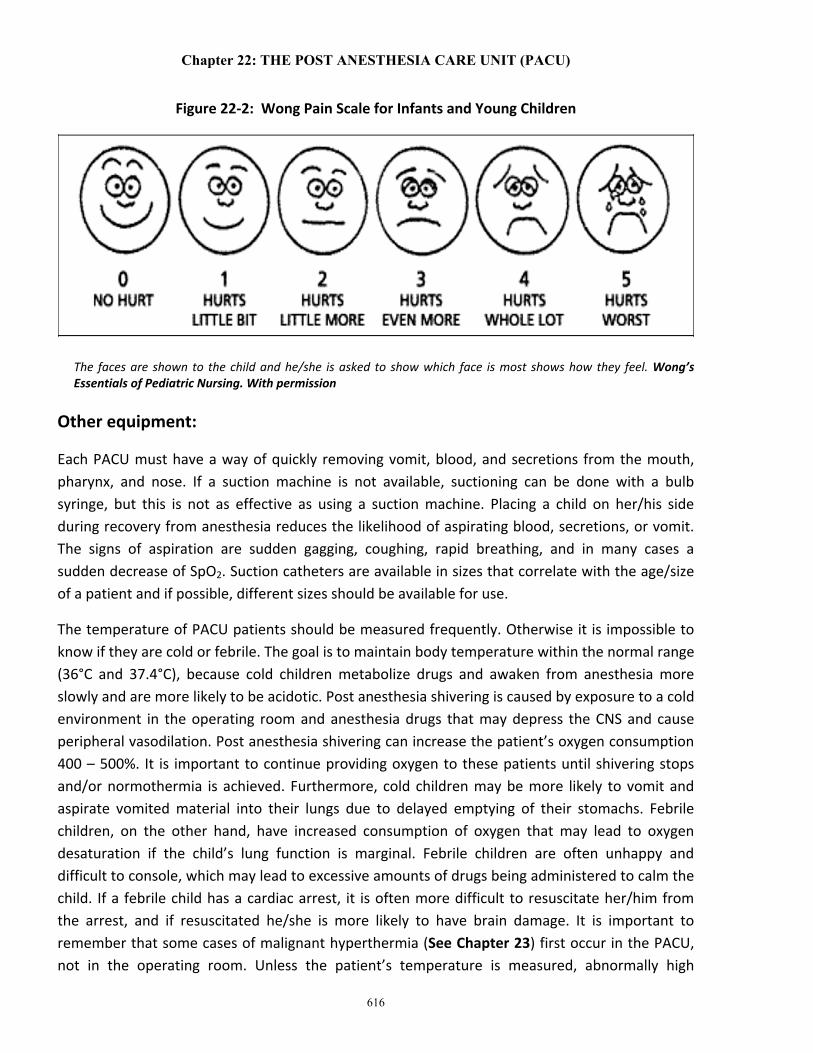
Pain assessment is often regarded as the fifth vital sign. It is an objective measurement rather than subjective. It is important for PACU nurses to assess pain frequently using age appropriate scales. These pain scales may include: simple descriptive, the numeric scale, the faces scale, or the FLACC for infants. (Figure 22-2)
Chapter 22: THE POST ANESTHESIA CARE UNIT (PACU)
616
Figure 22-2: Wong Pain Scale for Infants and Young Children
The faces are shown to the child and he/she is asked to show which face is most shows how they feel. Wong’s Essentials of Pediatric Nursing. With permission
Other equipment:
Each PACU must have a way of quickly removing vomit, blood, and secretions from the mouth, pharynx, and nose. If a suction machine is not available, suctioning can be done with a bulb syringe, but this is not as effective as using a suction machine. Placing a child on her/his side during recovery from anesthesia reduces the likelihood of aspirating blood, secretions, or vomit. The signs of aspiration are sudden gagging, coughing, rapid breathing, and in many cases a sudden decrease of SpO2. Suction catheters are available in sizes that correlate with the age/size of a patient and if possible, different sizes should be available for use.
The temperature of PACU patients should be measured frequently. Otherwise it is impossible to know if they are cold or febrile. The goal is to maintain body temperature within the normal range (36°C and 37.4°C), because cold children metabolize drugs and awaken from anesthesia more slowly and are more likely to be acidotic. Post anesthesia shivering is caused by exposure to a cold environment in the operating room and anesthesia drugs that may depress the CNS and cause peripheral vasodilation. Post anesthesia shivering can increase the patient’s oxygen consumption 400 – 500%. It is important to continue providing oxygen to these patients until shivering stops and/or normothermia is achieved. Furthermore, cold children may be more likely to vomit and aspirate vomited material into their lungs due to delayed emptying of their stomachs. Febrile children, on the other hand, have increased consumption of oxygen that may lead to oxygen desaturation if the child’s lung function is marginal. Febrile children are often unhappy and difficult to console, which may lead to excessive amounts of drugs being administered to calm the child. If a febrile child has a cardiac arrest, it is often more difficult to resuscitate her/him from the arrest, and if resuscitated he/she is more likely to have brain damage. It is important to remember that some cases of malignant hyperthermia (See Chapter 23) first occur in the PACU, not in the operating room. Unless the patient’s temperature is measured, abnormally high

Anesthesia Care of Pediatric Patients (George A. Gregory & Dean B. Andropoulos)
617
temperatures may be missed until it is too late, and the patient will either die or suffer severe brain injury.
Assessment on Admission to the PACU
When a patient arrives from the operating room, the anesthetist should provide the nurse with a description of what occurred during surgery. This report should include: the surgery performed and any surgical complications that occurred, the form of anesthesia used (sedation, general, block, spinal, epidural) and any complications that occurred, the drugs administered (including anesthesia drugs, antibiotics, muscle relaxants, narcotics or other drugs for pain relief) and their route of administration. Many drugs given during anesthesia last into the postoperative period and can affect the patient’s recovery from anesthesia. All surgeon-specific needs, including limitations or restrictions on patient positioning after surgery, dressings and their care (if any), the care of drains (if present), whether there is concern about circulation of blood to the surgical area (e.g., blood flow to a limb) should be reported to the patient’s nurse. It should be clear if arm restraints are necessary or can be used if required. The anesthetist should inform the PACU nurse of the type and volume of fluid administered during surgery (glucose or no glucose, normal saline, Ringer’s Lactate, or other balanced salt solution). The anesthetist should also report how much blood loss occurred, and if known, the patient’s hemoglobin concentration and the urine output. Before the anesthetist leaves the PACU, the child’s nurse should be completely satisfied that he/she understands what occurred in the operating room and that he/she has a way to immediately communicate with the anesthetist and get help when needed. The anesthetist is responsible for writing orders for the postoperative care of the patient in the PACU so there will be no confusion as to what the orders are. These orders should include the need for oxygen and for how long, the type of medication and drug dose for pain relief, the amount and type of intravenous fluids (ml/kg) per hour, and the time to re-administer antibiotics if necessary. Any other patient or surgery specific orders should be written at this time, including NPO status.
Initial Assessment
Initial evaluation of patients in the PACU starts when they arrive. Assessment includes an over all visual inspection of the patient including evaluation of the airway, breathing, cardiac function, surgical site, and skin color. This is done while monitors are being applied to the patient and oxygen is being administered. Oxygen can be provided using a simple facemask or by blowing oxygen by the patient’s face (‘blow by’) if the mask is not tolerated. The concentration of oxygen delivered as well as the length of time needed should be patient specific. Signs of difficult breathing are evaluated. The ribs, sternum, or the supra or infra sternal notches should show no evidence of in drawing (retraction) during inspiration, nor should one hear breathing noise during inspiration or expiration. These are signs of airway obstruction and/or increased work of breathing and should lead to immediate correction of whatever is causing the obstruction. Upper

Chapter 22: THE POST ANESTHESIA CARE UNIT (PACU)
618
airway obstruction is the most common reason for hearing noise during inspiration, and is frequently due to the tongue falling back into the throat. This often occurs because anesthesia blocks or reduces activity of the muscles that hold the tongue away from the pharyngeal wall (genioglossus and hyoglossus). Tone in these muscles returns as the patient awakens from anesthesia. When this happens, the obstruction disappears and the patient can breathe without obstruction. Snoring is a common sign of obstruction. Treatment of this type of upper airway obstruction requires moving the tongue away from the pharyngeal wall. To do this, a rolled towel is placed under the patient’s shoulders and the head is extended. If this fails to relieve the obstruction, the little fingers of ones hands are place in the angle of the jaw and the jaw is pulled forward (Figure 22-3). Since the tongue is attached to the posterior mandible, pulling the mandible forward pulls the patient’s tongue out of the pharynx. Inserting an oral or nasal airway also helps. However, oral airways occasionally cause vomiting or injure the teeth. Airways inserted through the nose can cause bleeding if they tear infected, friable adenoids tissues of young children; nasal airways are frequently avoided for this reason in young children. Oxygen should be administered by facemask when attempting to relieve the airway obstruction and should be continued until the patient can maintain a normal airway without signs of obstruction or oxygen desaturation. Retractions of the chest wall and sternum will stop and airflow within the chest will be free when the obstruction has been relieved. A noise that occurs during expiration (wheezing) is usually caused by airway obstruction within the chest (e.g., asthma). This obstruction may need to be treated with drugs (Albuterol) given by a nebulizer. Stridor is a high-pitched sound caused by a narrowed or obstructed airway. This may occur in children with croup, laryngeal edema (from a tracheal tube), or with the presence of a foreign body. Stridor is treated by providing positive pressure ventilation by mask with 100% O2. The O2 flow rate should be 10-15 liters/ min. Treatment for a partial occlusion of the airway that is caused by edema may include the use of racemic epinephrine. Any airway issue is a true emergency, and an anesthetist must be notified

Anesthesia Care of Pediatric Patients (George A. Gregory & Dean B. Andropoulos)
619
Figure 22-3: Jaw Thrust in a Child
The anesthetist is performing jaw thrust by placing one of her hands on each side of the child’s head. She has placed the tips of her little fingers in the angles of the patient’s jaw behind the mandible and is lifting the jaw forward (upward) while slightly extending the patient’s head. The facemask is being held on the patients face with the thumb and index finger of the anesthetist’s left hand. Oxygen is being delivered through the facemask. I necessary she can ventilate the patient’s lungs.
Grunting during exhalation is evidence of reduced functional residual capacity (FRC), which is the volume of gas within the chest at the end of expiration. The FRC’s function is to reduce the work required to inspire gas and to allow oxygen and carbon dioxide to be exchanged during both inspiration and expiration. When the FRC is low, the concentration of oxygen varies between inspiration and expiration. When the FRC is normal oxygenation remains relatively constant during both inspiration and expiration. The patient’s respiratory rate should be determined and should be normal for the patient’s age. (See Appendix 1) If it is not, the reason for this abnormality (pain, fever, acidosis, sepsis, hypoxemia, low FRC) should be sought and corrected when possible.
The pattern of respiration is important. Normally, the abdomen and chest move in the same direction during breathing, in with inspiration and out with expiration. During airway obstruction, the chest moves inward and the abdomen outward with inspiration. Patients who contract their chest and abdominal muscles during expiration usually have airway obstruction (asthma, tumor, mucus, blood). Movement of the head (head bobbing during breathing) and nasal flaring (widening of the nostrils during inspiration) also indicate airway obstruction during inspiration.
Chapter 22: THE POST ANESTHESIA CARE UNIT (PACU)
620
Upon arrival in the PACU, the patient’s level of consciousness is evaluated. Several questions should be answered. Does the patient respond to voice or stimulation? Those who fail to respond are more likely to have airway obstruction and to vomit and aspirate than patients who are awake when they arrive. Awake patients, on the other hand, while less likely to have airway obstruction and aspiration, need to be watched closely to prevent self-harm. IV’s, tubing and dressings need to be watched so the patient does not remove them. The goal is to have a calm, responsive patient, which requires her/him to be free or nearly free of pain. Children who have pain and are partially anesthetized often are “wild” and hard to control. One-to-one patient care may be needed until the child is calmer. It is important that gurneys have working brakes and side rails for patient safety. Treating a child’s pain allows them to rest and recover more easily and slowly. How much pain relief is required depends on the amount of pain the child has and on the amount of analgesic given during surgery. Close observation is needed to evaluate if pain is being experienced. It is more effective to begin providing pain medication before pain is experienced. Once they have significant pain, much higher amounts of drug are required to control the pain. Many times having a parent or family member at the bedside during wake up and recovery allows familiar comfort measures (holding, familiar voice, rocking, etc.) to be used, which may decrease the need for pain medication.
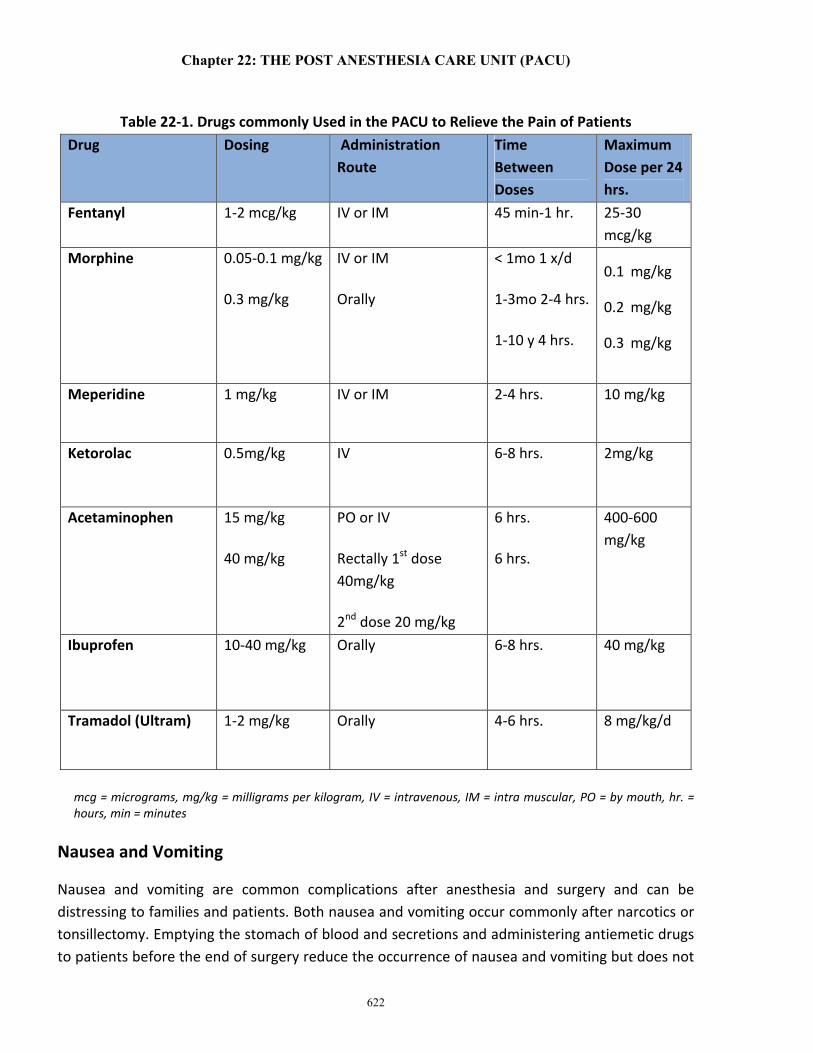
Table 22-1 gives the doses of commonly available analgesic drugs. Fentanyl 1-2 micrograms/kg (mcg/kg) effectively relieves pain for 30-60 minutes and then requires additional doses of ⅓-½ of the original dose of drug. Morphine provides 1-2 hours of pain relief. It is best to titrate the dose of analgesic drugs to achieve the effect desired (pain relief without depression of respiration). Doing so usually avoids giving too much drug. Other drugs, such as acetaminophen 15 mg/kg I.V. or orally or 40 mg/kg by rectum (as a one-time dose), often provides good pain relief for hernia repair and similar surgeries. The combination of oral acetaminophen and codeine was commonly used in the past but is seldom used at present because 15%-to-20% of patients do not get pain relief beyond that due to the acetaminophen. Codeine works because the liver converts it to morphine. Some patients, especially those in Africa and Japan, can metabolize more codeine to morphine than others, and this has caused both respiratory and cardiac arrests.3 Some of these children have died.
All drugs, including those used to relieve pain, cause unwanted side effects in some patients. Narcotics (fentanyl, morphine) cause nausea, vomiting, itching, and constipation in some patients. These drugs can also depress respiration that leads to hypoxemia. Furthermore, narcotics can reduce the tidal volumes and the respiratory rates of some patients, which may cause them to retain carbon dioxide and develop respiratory acidosis. If the respiratory depression (hypoventilation) is severe enough, apnea and cardiac arrest may occur. Naloxone (0.01 mg/kg for hypoventilation, 0.1mg/kg for respiratory and/or cardiac arrest due to narcotic overdose) - up to a total of 1 mg) is given and may be repeated every 2-3 minutes as needed to restore breathing in a patient who has significant hypoventilation and/or apnea from narcotics. It must be remembered

Anesthesia Care of Pediatric Patients (George A. Gregory & Dean B. Andropoulos)
621
that the effect of naloxone only lasts 30-45 minutes. Therefore, those patients given naloxone must be observed closely for signs that naloxone’s effects are wearing off and hypoventilation is recurring. Very large doses of acetaminophen injure the liver and may cause the patient to die. Intravenous ibuprofen relieves pain, but some surgeons do not want to use it because it has been said that it causes bleeding at surgical sites; however, this is unproven. Tramadol, another frequently available and effective analgesic, is also metabolized to morphine by the liver and has been reported to cause apnea in patients, especially those who have previous sleep apnea and when the drug is give intravenously. Respiratory depression is uncommon when the drug is given orally. The most common side effects of tramadol are nausea, vomiting, dizziness, dry mouth, and sedation. These side effects also occur less frequently when the drug is given orally. Allergic reactions have been reported but are rare. Cardiac and central nervous system effects are rare after giving normal doses of the drug.
Nerve blocks or spinal or epidural analgesia provide excellent postoperative pain relief (See Chapters 20 and 21). However, due to their effects, the stay in PACU may be prolonged. The anesthetist should evaluate the patient for stability of her/his condition before discharging the patient to the ward or the ICU.
Chapter 22: THE POST ANESTHESIA CARE UNIT (PACU)
622
Table 22-1. Drugs commonly Used in the PACU to Relieve the Pain of Patients Drug Dosing Administration
Route
Time Between Doses
Maximum Dose per 24 hrs.
Fentanyl 1-2 mcg/kg IV or IM 45 min-1 hr. 25-30 mcg/kg
Morphine 0.05-0.1 mg/kg
0.3 mg/kg
IV or IM
Orally
< 1mo 1 x/d
1-3mo 2-4 hrs.
1-10 y 4 hrs.
0.1 mg/kg
0.2 mg/kg
0.3 mg/kg
Meperidine 1 mg/kg IV or IM 2-4 hrs. 10 mg/kg
Ketorolac 0.5mg/kg IV 6-8 hrs. 2mg/kg
Acetaminophen
15 mg/kg
40 mg/kg
PO or IV
Rectally 1st dose 40mg/kg
2nd dose 20 mg/kg
6 hrs.
6 hrs.
400-600 mg/kg
Ibuprofen 10-40 mg/kg Orally 6-8 hrs. 40 mg/kg
Tramadol (Ultram) 1-2 mg/kg Orally 4-6 hrs. 8 mg/kg/d
mcg = micrograms, mg/kg = milligrams per kilogram, IV = intravenous, IM = intra muscular, PO = by mouth, hr. = hours, min = minutes
Nausea and Vomiting
Nausea and vomiting are common complications after anesthesia and surgery and can be distressing to families and patients. Both nausea and vomiting occur commonly after narcotics or tonsillectomy. Emptying the stomach of blood and secretions and administering antiemetic drugs to patients before the end of surgery reduce the occurrence of nausea and vomiting but does not
Anesthesia Care of Pediatric Patients (George A. Gregory & Dean B. Andropoulos)
623
eliminate them. Zofran (ondansetron) 0.45mg/kg – maximum dose 4 mg/dose - is an effective antiemetic. If needed, the dose of ondansetron 0.15mg/kg can be repeated every 4 hours. Reglan (Metacolpromide) 1-2mg/kg every 2-6 hours and Compazine (procloparazine) can also be used to treat nausea, but their side effects may limit their usefulness. Decadron (dexamethasone) 0.25-0.5mg/kg, (4-8mg total) when given during surgery, significantly reduces the incidence of postoperative nausea and vomiting and reduces airway swelling that may add to postoperative pain. There is little evidence that this one-time dose of Decadron increases postoperative bleeding or other complications. Specific surgeries (e.g., tonsillectomies, cleft palate repair) may bleed after surgery and cause blood to be swallowed, which may increase the incidence of postoperative nausea and vomiting. Patients who drink liquids before going home often vomit on the way home due to movement of the vehicle, especially if the drive home involves curvy roads. However, it is important to be sure the patient can drink without vomiting before a patient is discharged home from the PACU. It is best to start with water or juice and see how the patient does. If there is no nausea or vomiting, they can be discharged after warning the parents that the patient may vomit with excessive movement.
On Going Assessment
The patient’s condition must be reevaluated throughout her/his PACU stay. This includes adequacy of the airway/respiration, blood pressure, heart rate, peripheral perfusion (capillary filling, skin temperature), and pulses. It is recommended that vital signs be recorded in the patient’s chart on a nursing form every five minutes for 15 minutes, then every 15 minutes for one hour; every 30 minutes for two hours, then every hour or until the patient is discharged from the PACU. Patients who are unstable require more frequent vital signs/observation. Vital signs are recorded so that if problems occur, those caring for the patient can hopefully determine what caused the problem. The purpose of recording data in a patient chart is to evaluate the patient’s condition over time and whether treatment is improving the patient’s outcome.
Intravenous Fluid Management
Management of intravenous fluids during recovery from anesthesia is an important part of PACU care, since surgery often causes fluids to shift from one body compartment to another. This can cause the patient’s intravascular volume to become inadequate. Thus it is important for nurses to obtain as much information as possible about the surgery performed, the amount of blood lost during surgery, and the amount and type of fluid given to replace losses. Part of the assessment should include examining the patient to determine if the intravascular volume is adequate or not. (See Chapter 1) The fontanel of babies younger than three months of age is usually open and is a useful guide to the evaluation of the patient’s state of hydration. Skin over the fontanel should be even with the outer bone of the skull. If the skin is at the level of the inner bone of the skull, the patient is 5% dehydrated; if it is below the inner bone of the skull, hydration is reduced 10% or
Chapter 22: THE POST ANESTHESIA CARE UNIT (PACU)
624
more. The mucus membranes of the mouth should be wet when felt. If they are not, this is a sign on of dehydration. Babies who are less than three months of age do not make tears when they cry. Older patients do. Thus, when an older patient cries without making tears, this is a sign of dehydration. When the skin is picked up (tented) it should immediately return to its normal position if hydration is normal. If the hydration is not normal, the skin will remain tented for a few seconds and slowly return to its normal position. Pulses should be present and normal in all limbs. If the pulses are reduced or absent in the wrists and feet, the patient is about 5% dehydrated; if the popliteal or brachial pulses are absent or decreased, volume is reduced by 10%; if the femoral and axillary pulses are reduced or absent, the child’s intravascular volume is reduced by 15% or more. The arterial blood pressure should be within normal limits for the patient’s age. If it is more than 20% lower than normal for age, the child is probably hypotensive. Most children produce 1 ml/kg/hr. of urine or more. If their urine production is less than this, hypovolemia is often the cause. Finally, the examiner should place a warm hand on the child’s chest and move her/his hand out along the shoulders and arms to the patient’s fingers. The patient’s skin should be warm all the way out to the fingertips. If the skin of the forearm suddenly becomes cold, the volume is reduced by 5%; if the skin of the upper arm gets cold as the hand moves over it, the patient’s volume is depleted by 10%; if the entire arm is cold, the patient’s volume is reduced by 15% or more. When all of these factors are taken together, it is easy to estimate the patient’s intravascular volume. The information gained from this examination can be used to guide the amount of fluid needed to correct hypovolemia. Following fluid administration, the patient’s volume status must be reevaluated to determine if sufficient fluid has been administered or if more is needed. Before discharge from the PACU, the patient’s intravascular volume and perfusion should be normal.
Discharge From the PACU
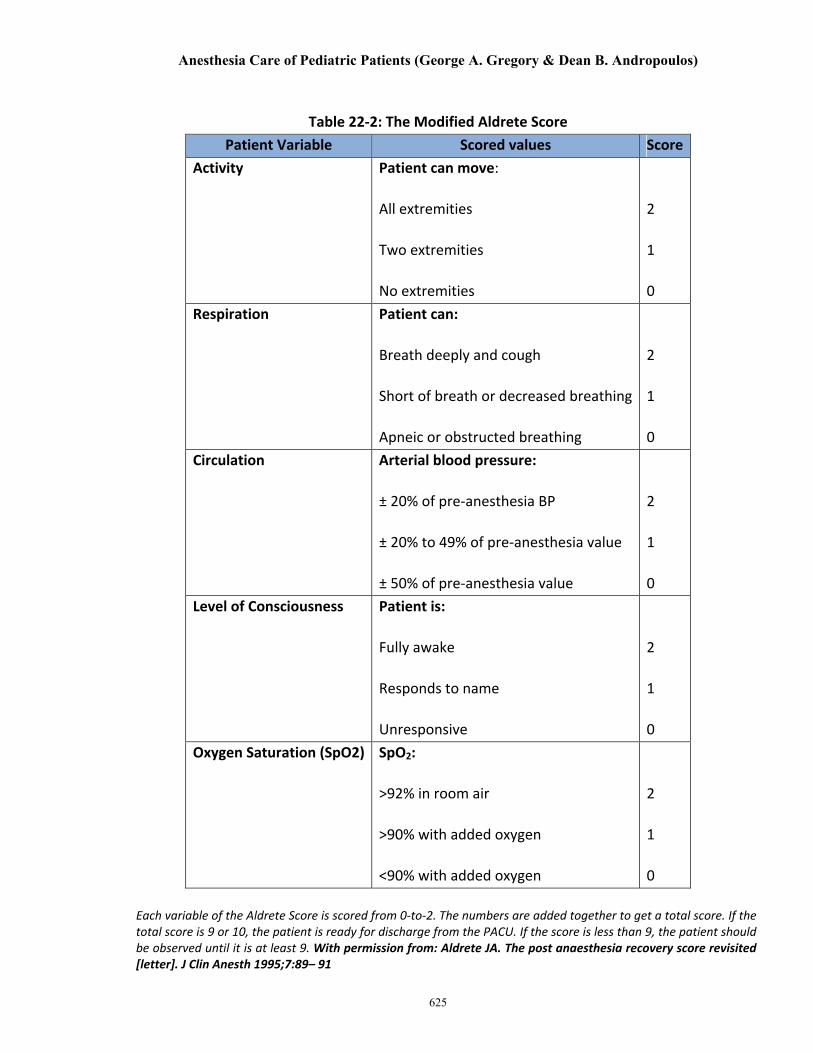
Part of on going patient assessment is to determine when the patient is ready for discharge from the PACU. In general, patients are ready to leave when they are awake, responding to voice and commands, able to maintain a normal SpO2 in room air, and have little pain. Table 22-2 is the modified Aldrete Score, which is widely used to determine if patients can be discharged from the PACU to their hospital room or to home.
Postoperative instructions are given prior to discharge from the PACU to family members and/or nursing staff. These instructions should include information on diet, pain control and surgery specific instructions (dressings, when to shower/bathe, daily activities). Follow up appointments should be provided.
Anesthesia Care of Pediatric Patients (George A. Gregory & Dean B. Andropoulos)
625
Table 22-2: The Modified Aldrete Score Patient Variable Scored values Score
Activity Patient can move:
All extremities
Two extremities
No extremities
2
1
0 Respiration Patient can:
Breath deeply and cough
Short of breath or decreased breathing
Apneic or obstructed breathing
2
1
0 Circulation Arterial blood pressure:
± 20% of pre-anesthesia BP
± 20% to 49% of pre-anesthesia value
± 50% of pre-anesthesia value
2
1
0 Level of Consciousness Patient is:
Fully awake
Responds to name
Unresponsive
2
1
0 Oxygen Saturation (SpO2) SpO2:
>92% in room air
>90% with added oxygen
<90% with added oxygen
2
1
0
Each variable of the Aldrete Score is scored from 0-to-2. The numbers are added together to get a total score. If the total score is 9 or 10, the patient is ready for discharge from the PACU. If the score is less than 9, the patient should be observed until it is at least 9. With permission from: Aldrete JA. The post anaesthesia recovery score revisited [letter]. J Clin Anesth 1995;7:89– 91
Chapter 22: THE POST ANESTHESIA CARE UNIT (PACU)
626
REFERENCES
1. Beecher HK, Todd DP. A study of deaths associated with anesthesia and surgery, Ann Surg 1954; 40:1402-34
2. Braz LG, Modolo NSP, do Nascimento P, Bruschi BAM, Castiglia YMM, Ganem EM, de Carvalho LR, Braz JRC. Perioperative cardiac arrest: a study of 53,718 anaesthethics over 9 yr. from a Brazilian teaching hospital. Brit J Anaesth 2006; 96:569-575
3. Ciszkowski C, Madadi P, Phillips MS, Lauwers, AE, Koren G. Codeine, Ultrarapid-Metabolism Genotype, and Postoperative Death. N Engl J Med 2009; 361:827-82