Embed Size (px)
Citation preview

Graefe's Arch Clin Exp Ophthalmol (1988)226:137-140 Graefe's Archive [or Clinical a~ l Experimenllal
Ophthalmology © Springer-Verlag 1988
Anomalous retinal correspondence update* J. Lang Universit/its-Augenklinik, Freiestrasse 47, CH-8032 Zfirich, Switzerland
Abstract. For orthoptists and ophthalmologists, anomalous retinal correspondence (ARC) is a reality and an important finding. But since it has not been found in animals, ARC seems to be unknown to neurophysiologists. Comparing results of different stereotests, e.g., random-dot stereograms and the two-pencil test, provides some insight into different levels of cortical binocular interaction. Patients with ortho- tropia and normal retinal correspondence (NRC) and even those with anisometropic amblyopia usually pass random- dot stereograms, whereas strabismic patients with ARC, even with microtropia, usually fail. Microtropic patients, however, may pass contour stereograms, and, in large eso- tropic angles, useful, daily-life binocular stereopsis can be found with the two-pencil test. Random-dot stereopsis sug- gests that normal binocular interaction must take place in or near area 17, where data processing for small dots occurs before form recognition. Anomalous correspondence most probably has its seat where the retinal topology is not exact, i.e., where the binocular receptive fields are very large and encompass the corpus callosum, such as in area 20 or 21. This new hypothesis may explain the different forms of ARC according to the clinical entities.
Introduction
Since Johannes Mfiller's description of strabismus incon- gruus in 1826 [14] and since that by Albrecht von Graefe of postoperative paradoxical diplopia in 1858 [3], anoma- lous retinal correspondence (ARC) has become a well- known and important clinical phenomenon. We know that about 85% of all patients with convergent strabismus show ARC.
Until about 20 years ago, ARC was thought to be cur- able, and many treatment methods have been proposed. The idea of curability has now been abandoned, since it turned out that although one can reduce the angle of anom- aly, one cannot really eliminate it. In addition, experimental animal neurophysiology, although providing insight into deprivation amblyopia, has failed to provide information and new ideas regarding ARC. These two factors may be the reason for the lack of interest seen in ARC in the past few years.
* Dedicated to Dr. G.K. yon Noorden on the occasion of his 60th birthday
At present, for the study of ARC we can rely only on clinical entities and on results of clinical examination meth- ods. All the same, it would be interesting to have a neu- rophysiological concept for ARC.
Material and methods
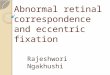
In my experience, the most important method for exact assessment of ARC has proven to be the ophthalmoscopical examination described by Cfippers [2]. This method can easily be demonstrated by simple means, even on oneself. All one must do is fixate with one eye the small light of a Maddox scale and project into the other eye the fixation star of an appropriate ophthalmoscope, then judge where the star is projected in relation to the light. When the star coincides with the light, with NRC, both the star and the light are in the foveolae of the respective eyes. To perform this examination clinically I use a viewing periscope before the fixating eye of the patient [9]. The advantage of the periscope is that the examiner does not interfere with the line of fixation of the patient and the Maddox scale does not appear to be reversed from right to left (Fig. 1). In this way, the directional value of different retinal areas in the strabismic eye can be plotted. This method requires some practice and cannot be used with young children. I have also described a method for photographic demon- stration of ARC on this same basis [12]. Other methods, such as afterimages, the synoptophore, and striated glasses are helpful. One should, however, never rely exclusively on the 4-prism base-out test to make the diagnosis of micro- tropia, since this method does not provide differentiation between microtropia with ARC and anisometropic amblyo- pia with NRC.
Until some years ago, it was believed that ARC could not permit useful stereopsis in manifest deviations. Here, one must clearly separate random-dot stereopsis from non- random-dot or contour stereopsis. Examinations in micro- tropia showed fairly good contour stereopsis on the basis of ARC but no random-dot stereopsis. Let us, therefore, take three different clinical entities, namely, amblyopia ex anisometropia, microtropia, and large angles, and consider the results gained by means of three different methods, namely, stereopsis determination with random dots (such as the Lang or the TNO stereotests), stereopsis determina- tion with a contour test (such as the Titmus test), and esti- mation of gross stereopsis with the two-pencil test [10].

138
Fig. 1. Ophthalmoscopical examination of correspondence with a periscope
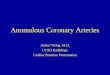
The two-pencil test most probably is the quickest and oldest test for examining stereopsis. It is also the most beau- tifully illustrated of all orthoptic tests; in 1613, Peter Paul Rubens drew a wonderful illustration of it for Franciscus Aguilonius' book, Opticorum Libri. The cherub holds a rod in front of the scholar, who tries to touch it from the side with his index finger (Fig. 2a), closing his left eye.
If Aguilonius and Rubens were still living, I would sug- gest to them that the scholar hold another rod vertically above the first in order to involve horizontal disparity in the attempt to touch the other rod (Fig. 2b). I would also suggest that the test first be carried out binocularly and then monocularly, i.e., with the nondominant eye covered (Fig. 2c) in order to compare binocular with monocular performance.
In the plast two decades the two-pencil test has been conducted in my office on almost all patients with motility disorders. Comparison was made between results with the Lang stereotest on 135 patients with microtropia and those on 40 patients with anisometropic amblyopla.
Comparison of random-dot (Lang and TNO) and non- random-dot stereopsis (Titmus) was carried out in 26 pri- mary and 19 "consecutive" or residual microtropias.
In 20 normal subjects, artificial anisometropia was pro- duced on the Phoropter in order to assess which amounts of anisometropia still permit stereopsis on the Lang stereo- test.
Results
Of 135 patients with microtropia, 118 (87%) were stereo- negative, four (3%) had partial stereopsis, and 13 (9.6%) were stereopositive on the Lang Stereotest. Partial stereop- sis means that the patient had a stereoscopic effect, mostly delayed, at the correct location but could not recognize the objects.
Of 40 patients with anisometropic amblyopia, 25 (62%) were stereopositive, four (10%) were partially positive, and 11 (27.5%) were negative. The stereonegative group had a greater degree of anisometropia.
In 20 normal subjects it could be shown that, with artifi- cial aniosmetropia, random-dot stereopsis was possible within a range of + / - 2 . 3 diopters of anisometropia [11].
Fig. 2a-e. Illustration by Rubens of the two-pencil test. a Origi- nal; b modification by Lang, showing use of a vertical rod; e modification by Lang, showing administration of test with one eye covered
Of 26 patients with primary microesotropia, all were negative on the Lang test as well as on the TNO. On the Titmus test, only one (4%) was negative; in 11 patients (42%) stereopsis was between 100" and 250"; and 14 pa- tients (54%) had stereopsis of 400" or less.
Of 19patients with consecutive microesotropia, 16 (84%) were negative on the Lang test, two (11%) were partially positive, and one patient was stereopositive. On the TNO, 17 (89%) were stereonegative and two 0 1 % )

Discussion
were positive. On the Titmus test, 17 (89%) were stereo- positive, but only two (11%) were stereonegative [15].
The patient with stereopositivity on the Lang test was reexamined. He had been operated on with a bimedial reces- sion for esotropia. Postoperatively, he sometimes showed a microestropia on the unilateral cover test and sometimes an orthotropia. The ophthalmoscopical examination re- vealed a normal correspondence. He therefore must be clas- sified as having an intermittent microesotropia with normal correspondence. This NRC was used intermittently in situa- tions of stereoscopic examination.
Our experience with the two-pencil test showed that with harmonious ARC, even in larger angles and with deep amblyopia, the binocular performance was much better than monocular performance.
7
Our findings showing a difference between random-dot and nonrandom-dot stereopsis in microtropia and anisometro- pia correspond to those of Lin and Jeng [13] and Crone [11.
Haase and Wermann [5] have largely confirmed our findings with the two-pencil test.
There seems to be an almost hierarchical order: In or- thotropic amblyopia ex anisometropia, stereopsis can be demonstrated with all three methods; in microtropia there exists no random-dot stereopsis but, instead, positive stereopsis with contour tests and with the two-pencil test, whereas in large angles with harmonious ARC, only the two-pencil test shows stereopsis (Table 1).
Let us now see if these clinical findings can give some neurophysiological clues. The work of Hubel and Wiesel [6] has shown that binocular interaction does not yet take place in layer IV of area 17 in the cortex [5] but instead immediately outside this layer.
Investigations on random-dot stereopsis by Julesz [8] yielded new knowledge on the site of stereopsis mechanisms in the cortex. Formerly, one thought that stereopsis could function only after the form, or Gestalt, of an object had been recognized. With random dots it became clear that this is not so. The stereopsis mechanism for random dots must therefore be situated at the beginning of cortical data processing, in or near area 17. In addition, NRC must have its seat where the most exact representation and topography of the retina exist.
We know that the representation of the fovea in the cortex is enlarged. According to some authors, such en- largement is 20 times, according to others even 100 times. A microtropic anomaly angle of 2 ° in the cortex would mean a distance of 12 or 60 mm, depending on which en- largement factor one uses. This distance is much larger than that of an ocular dominance column, which measures 0.5 mm. This may explain why no random-dot stereopsis is possible in microtropia.
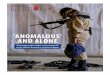
By means of degeneration experiments [7] it has been shown that from area 17 to areas 18 and 19, and further to the inferotemporal cortex (areas 20 and 21), there are many stages of visual data processing (Fig. 3). It is known that retinal topography becomes less and less exact along these projections. Additionally, in the inferotemporal cortex there exist neurons with large receptive fields encompassing the midline and the corpus callosum. It has also been shown
Table 1. Stereopsis in anisometropia, microtropia, and large angles
Random dots, Contours, Two-pencil Lang, TNO, etc Titmus, etc test
Amblyopia ex Positive Positive Positive anisometropia
Microtropia Negative Positive Positive
Large angles, Negative Negative Positive amblyopia
139
Fig. 3. Visual data processing and retinal topography form areas 17-21 (after Jones [7], modified by Lang)
that complicated visual structures can be recognized only in areas 20 and 21 [4].
Normal retinal correspondence of a high degree takes place at the beginning of cortical data processing, where disparity of small dots can be calculated. In microtropia, data processing most probably occurs where not small dots, but lines are processed binocularly and where the topo- graphical representation is still fairly good. From our pa- tients with ARC and stereopsis on the two-pencil test, we know that two widely separated retinal areas in the two eyes have the same visual direction. Interaction and process- ing of these largely separated areas most probably take place in the inferotemporal cortex where the neurons have large receptive fields and where the retinal topography is inexact.
With this in mind, we may also understand that large anomaly angles are an adaptation to the motor angle, whereas stable, small-angle ARC, as in microtropia, may be determined by a genetic factor preventing the most exact data processing. We may also understand that by reducing the motor angle we may attain a microtropia but will never

140
be able to climb to the top of the mounta in of binocular vision.
Be that as it may, this hypothesis, which is based mainly on clinical tests and entities, may bridge a gap in our neu- rophysiological knowledge. A R C seems to be a condit ion found exclusively in human beings and, with appropr ia te methods, may even be able to provide neurophysiological informat ion about the function of the human cortex.
References
1. Crone RA (1982) Discussion, strabismus II, Reinecke, ISA. Grune and Stratton, New York, p 547
2. Clippers C (1961) Grenzen und M6glichkeiten der pleoptischen Therapie. Klin Monatsbl Augenheilkd 38:33
3. Graefe A yon (1855) Uber das Doppeltsehen nach Schielopera- tionen und Incongruenz der Netzh/iute. Albrecht von Graefes Arch Ophthalmol 2 : 322-329
4. Gross CG, Rocha-Miranda CE, Bender DB (1972) Visual prop- erties of neurons in inferotemporal cortex of the macaque. J Neurophysiol 35:96--101
5. Haase W, Wermann O (1985) Postoperativer Mikrostrabismus,
Handlungssicherheit in r/iumlicher Tiefe. Klin Monatsbl Au- genheilkd 186: 337-342
6. Hubel DH, Wiesel TN (1962) Receptive field binocular interac- tion and functional architecture in the cat's visual cortex. J Physiol 160:106
7. Jones EG (1974) The anatomy of extrageniculostriate visual mechanisms. In: Schmidt FO, Worden FG (eds) The neuro- sciences, 3rd study program. MIT Press, Cambridge, Mass, pp 215-227
8. Julesz B (1971) Foundations of cyclopean perception. Universi- ty of Chicago Press, Chicago
9. Lang J (1984) Strabismus, translated by GW Cibis. Slack, Thor- ofare, NJ, pp 58ff
10. Lang J (1984) The two-pencil test and the new Lang stereotest. Br Orthopt J 41 : 51 21
11. Lang T (1985) Der Lang-Stereotest. Dissertation, Zfirich 12. Lang J, Wfirth A (1970) Photographic representation of anom-
alous retinal correspondence Ophthalmic Res 1 : 88-93 13. Lin LL-K, Jeng S (1982) Disparity in stereotests, strabismus
II, Reinecke, ISA. Grune and Stratton, New York, pp 541-547 14. Miiller J (1826) Zur vergleichenden Physiologie des Gesichts-
sinnes. Leipzig 15. Rechichi C (1986) Studio della stereopsi in varie forme di stra-
bismo. Thesis, Universit/t di Messina