Embed Size (px)
Citation preview

T
A
J
F
u
atrmpcoiPn
p
●
●
●
m
al
●
●
●
amSl
●
●
●
●
●
CW
1
EN QUESTIONS/ALLIED PROFESSIONALS
nticoagulation practice in cardiac electrophysiology
ulie B. Shea, MS, RNCS
rom Cardiac Arrhythmia Service, Cardiovascular Division, Brigham and Women’s Hospital, Boston, Massachusetts.
●
mcwwcm
c
edspIswihticpc
●●●●●●
●●
1. What is the most common indication for anticoag-lation in electrophysiology?
Answer: Atrial fibrillation (AF) is the most commonrrhythmia affecting more than two million individuals inhe United States annually. It is an important independentisk factor for stroke. Anticoagulation with warfarin is com-on practice in patients with paroxysmal, persistent, and
ermanent AF to help minimize stroke risk. Numerouslinical trials have consistently demonstrated the superiorityf adjusted-dose warfarin compared with aspirin or placebon reducing stroke risk in the AF patient population.1–8
atients with lone AF (without structural heart disease) doot necessarily require anticoagulation.
Additional indications for anticoagulation in the electro-hysiology (EP) patient population include the following:
Atrial flutter (same risk factors as for AF)After extensive ablation in the left atrium or ventricleUpper-extremity deep vein thrombosis (DVT) followingdevice implantation
2. What are the different types of anticoagulationethods used?Answer: The most common form of anticoagulation is
djusted-dose warfarin. However, the following anticoagu-ants also can be used:
Antiplatelet agents: aspirin (acetylsalicylic acid [ASA]),clopidogrelLow-molecular-weight heparin (LMWH)Unfractionated heparin (UFH)
3. What are the key patient education issues?Answer: Patient education is an integral component of
nticoagulation management, which is necessary to maxi-ize compliance and minimize potential complications.pecific topic areas to be covered should include the fol-
owing:
Purpose of the medicationDosing guidelinesInternational normalized ratio (INR) monitoringFood and medication interactionsReportable signs and symptoms
Address reprint requests and correspondence: Ms. Julie B. Shea,ardiac Arrhythmia Service, Cardiovascular Division, Brigham andomen’s Hospital, 75 Francis Street, Boston, Massachusetts 02115.
aE-mail address: [email protected].
547-5271/$ -see front matter © 2006 Heart Rhythm Society. All rights reserved
Medical alert bracelet
4. What are the follow-up considerations?Answer: Careful monitoring of the INR is essential to
aintain a therapeutic blood level and prevent potentiallyatastrophic bleeding or clotting complications. For patientsith AF, the typical target INR is 2–3 to prevent thrombushile minimizing the risk of hemorrhage. Dedicated anti-
oagulation clinics should be used routinely in the manage-ent of patients undergoing chronic warfarin therapy.5. How should anticoagulation be managed prepro-
edurally?Answer: The half-life of warfarin typically is 7 days. The
ffective half-life ranges between 20 and 60 hours, with auration of action between 2 and 5 days; therefore, warfarinhould be discontinued at least 3 to 4 days prior to thelanned procedure to allow time for normalization of theNR. For patients requiring continuous anticoagulation,uch as those with a prior history of stroke and/or patientsith artificial heart valves, bridging with LMWH typically
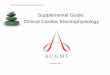
s used (Figure 1). Administration of subcutaneous LMWHas been established as a feasible method of bridging pa-ients who require uninterrupted anticoagulant therapy, butt has not been systematically evaluated by randomizedlinical trials.9 When considering a patient for thrombopro-hylaxis with LMWH, several factors should be taken intoonsideration10:
Type of procedureTimeline for the procedureThromboembolic riskHemorrhagic riskWeight (obesity)Renal function and baseline platelet count (dosage ad-justment needed for elevated creatinine)Instruction on performing self injectionsDetailed and patient-specific bridging schedule that out-linesA. When to stop oral anticoagulationB. When to start and stop LMWH
1. 12 hours prior to percutaneous procedures2. 24 hours prior to device implantation
C. Timing of postprocedure INRsD. Contact phone numbers for follow-up care
Low-risk patients with AF who do not require bridging
re individuals with lone AF, age less than 65 years, and no. doi:10.1016/j.hrthm.2005.11.015

rrotaplies5dhi
tghsp
a
sr
csprte(nwdb(immahghi
Mf
Ucvbswvbsta
atfcibspps
c
Aa
●
●
FvP
373Shea 10 Questions
isk factors for stroke, such as a history of hypertension,educed left ventricular systolic function, diabetes mellitus,r history of thromboembolism or stroke.10 In these situa-ions, the incidence of embolic stroke in the absence ofnticoagulation is less than �5% per year. In addition,atients with bioprosthetic valves who are not anticoagu-ated do not require bridging.10 High-risk patients with anydentifiable risk factor for stroke should be bridged withither LMWH or UFH, depending on the patient’s clinicalituation. Intravenous UFH should be discontinued at leasthours prior to the scheduled procedure, whereas the last
ose of subcutaneous LMWH should be given 12 to 24ours prior to the procedure, particularly in patients withmpaired renal function.
Recommendations for discontinuation of antiplateletherapy are similar to those for cardiac surgery. Aspirin canenerally be continued safely, but platelet aggregation in-ibitors (clopidogrel) should be discontinued, when permis-ible, for at least 5 days and preferably 7 days prior to therocedure.
6. How should anticoagulation be used postprocedur-lly?
Answer: In most instances, anticoagulation can be re-umed the evening of the procedure. For patients who have
igure 1 Brigham and Women’s Hospital Anticoagulation Ser-ice Critical Pathway for Bridging with LMWH. Piazza et al, Critathways in Cardiolog 2003;2:96-103.
eceived an implantable device, delaying initiation of anti-
oagulation with warfarin for 2 to 3 days, when permissible,hould be considered to allow for stabilization of the deviceocket. Special attention should be paid to those patientsequiring UFH, such as those with a mechanical heart valve,o prevent hematoma formation at the site. The measuredffect of UFH on the activated partial thromboplastin timeaPTT) is important to patient outcome, and the predomi-ant variable mediating the effect of a given dose of UFH iseight; therefore, it is important to administer the initialosage of UFH as a weight-adjusted bolus. A 60 to 70 U/kgolus followed by a maintenance infusion of 12 U/kg/hrwith a maximum 4,000-U bolus and 1,000 U/hr initialnfusion for patients weighing more than 70 kg) is recom-ended. The partial thromboplastin time (PTT) should beonitored closely, targeting a value of 60 to 80 seconds. In
ddition, a pressure dressing can be applied to the site for 24ours to reduce the incidence of hematoma. LMWH isenerally avoided after device implantation. Either form ofeparin is administered along with warfarin until the INR isn the appropriate target range.
anagement of upper-extremity DVTollowing device implantation
pper-extremity DVT after device implantation occurs as aonsequence of the presence of device hardware within theenous system that results in a reduction or cessation oflood flow. This condition typically manifests clinically aswelling in the upper or entire arm on the side ipsilateralith the device, pain/discomfort, and, later, a superficialenous pattern on the chest. The diagnosis is generally madey patient symptomatology, upper-extremity venous ultra-ound, or upper-extremity venogram (typically this diagnos-ic method is performed during concomitant thrombolysisnd/or suction thrombectomy).
Management of upper-extremity DVT involves antico-gulation with warfarin and LMWH (dosed until INR isherapeutic). Patients should be instructed to keep the af-ected limb elevated as much as possible. A graduatedompressed sleeve can be prescribed to reduce limb swell-ng and discomfort. Pain management should be consideredased on the patient’s level of discomfort. In some in-tances, depending on the severity of DVT and the patient’serceived level of discomfort related to arm swelling, aercutaneous interventional procedure (local thrombolysis,uction thrombectomy, venoplasty) can be performed.
7. What is the common anticoagulation practice afteratheter ablation?
Answer: This depends on the type of ablation procedure.t this time, no clinical data on anticoagulation practices
fter VT ablation are available.
AV nodal ablation: Lifelong anticoagulation with warfa-rin because the atria remain in fibrillationAF ablation: Pulmonary vein isolation*A. Aspirin 325 mg the morning of the procedure, then 81
mg/day

G
S
A
*†
r
twhwTs
a
d(mzbs[ceptgm
w
ti
●
Tsd
R
1
11
1
T
M
ASDPPDVMA
tdd
374 Heart Rhythm, Vol 3, No 3, March 2006
B. LMWH 1/mg/kg 6 hours after sheath removal, then0.5 mg/kg bid until INR is therapeutic
C. Resume warfarin the evening of the procedure andmaintain for a minimum of 3 months (unless AFrecurs, then anticoagulation should be continued in-definitely)
● Ventricular tachycardia ablation*
ood left ventricularfunction
Poor left ventricularfunction
mall area of ablation(ablation limited to theright ventricle)†
Extensive left ventricularablation(radiofrequency lines�3 cm)
SA 325 mg/day for 6weeks†
UFH started 6 hours postprocedure
Resume warfarinLMWH 0.5 mg/kg bid
until INR is therapeuticASA 81 mg/day
Brigham and Women’s Hospital protocol (unpublished data)Use of ASA is common practice in most centers, but dataegarding efficacy are limited
8. When are there exceptions to anticoagulation?Answer: Thromboprophylaxis should be avoided in pa-
ients who have experienced a prior untoward effect fromarfarin use, such as those with gastrointestinal bleeding oremorrhagic stroke. Heparin is contraindicated in patientsith a history of heparin-induced thrombocytopenia (HIT).he risks and benefits of anticoagulation use must be con-idered for each patient.
9. How does warfarin interact with commonly usedntiarrhythmic medications?
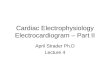
Answer: Warfarin interacts with numerous medicationsue to both pharmacodynamic and pharmacokinetic effectsTable 1). Warfarin is completely absorbed after oral ad-inistration and is metabolized by hepatic microsomal en-
ymes (cytochrome P450). Drugs can interact with warfariny means of pharmacodynamic effects (impaired hemosta-is, reduced clotting factor synthesis, antagonistic effectsvitamin K]) and/or by heredity resistance.11 The pharma-okinetic mechanisms for drug interactions are related tonzyme induction, enzyme inhibition, and/or reducedlasma protein binding. Some drugs may interact by morehan one mechanism.11 Elderly patients may exhibit areater than expected response; therefore, dosage adjust-ents should be considered in this age group.11,12
10. Are there alternatives to anticoagulation witharfarin?Answer: Alternative methods of anticoagulation for
hromboprophylaxis in patients with AF are under clinicalnvestigation.
Direct thrombin inhibitors
o date, no superior method of thromboprophylaxis fortroke reduction, compared with warfarin therapy, has been
emonstrated.eferences
1. Petersen P, Boysen G. Godtfredsen J, Anderson ED, Anderson B.Placebo-controlled, randomized trial of warfarin and aspirin for pre-vention of thromboembolic complications in chronic atrial fibrillation.The Copenhagen AFASAK study. Lancet 1989;1:175–179.
2. Gullov AL, Koefoed BG, Petersen P, Pedersen TS, Anderson ED,Godtfredsen J, et al. Fixed mini-dose warfarin and aspirin alone and incombination vs. adjusted dose warfarin for stroke prevention in atrialfibrillation: Second Copenhagen Atrial Fibrillation, Aspirin and Anti-coagulation Study. Arch Intern Med 1998;158:1513–1521.
3. Stroke Prevention in Atrial Fibrillation Study. Final results. Circula-tion 1991;84:527–539.
4. Warfarin versus aspirin for prevention of thromboembolism in atrialfibrillation: Stroke Prevention in Atrial Fibrillation II Study. Lancet1994;343:687–691.
5. Adjusted-dose warfarin versus low intensity, fixed-dose warfarin plusaspirin for high-risk patients with atrial fibrillation: Stroke Preventionin Atrial Fibrillation III randomised clinical trial. Lancet 1996;348:633–638.
6. The effect of low-dose warfarin on the risk for stroke in patients withnon-rheumatic atrial fibrillation. The Boston Area AnticoagulationTrial for Atrial Fibrillation Investigators. N Engl J Med 1990;323:1505–1511.
7. Connolly SJ, Laupacis A, Gent M, Roberts RS, Cairns JA, Joyner C.Canadian Atrial Fibrillation Anticoagulation (CAFA) Study. J AmColl Cardiol 1991;18:349–355.
8. Secondary prevention in non-rheumatic atrial fibrillation after transientischemic attack or minor stroke. EAFT (European Atrial FibrillationTrial) Study Group. Lancet 1993;342:1255–1262.
9. Kovacs MJ, Kearon C, Rodger M, Anderson DR, Turpie AG, BatesSM, Desjardins L, Douketis J, Kahn SR, Solymoss S, Wells PS.Single-arm study of bridging therapy with low-molecular-weight hep-arin for patients at risk of arterial embolism who require temporaryinterruption of warfarin. Circulation 2004;110:1658–1663.
0. Piazza G, Goldhaber SZ. Periprocedural management of the anticoag-ulated patient: critical pathways for bridging therapy. Crit PathwaysCardiol 2003;2:96–103.
1. http://coumadin.com. Last accessed October 19, 2005.2. Marine JE, Goldhaber SZ. Controversies surrounding long-term anti-
coagulation of very elderly patients in atrial fibrillation. Chest 1998;113:1115–1118.
3. Micromedix. http://www.thomsonhc.com/hcs/librarian. Last accessed
able I Drug interactions with warfarin
edication Increased INR Decreased INRNo Listed
Interaction
miodarone ��otalol �ofetillide �rocainamide �ropafenone �igoxin �erapamil �etoprolol �tenolol �
Amiodarone significantly reduces warfarin metabolism and thereforehe dosage of warfarin should be adjusted accordingly (reduce initiationose by 25%). Patients who develop hyperthyroidism secondary to amio-arone may have an additional increased anticoagulant effect.13
October 19, 2005.