Embed Size (px)
Citation preview

ooO5-7967/110/05OI-01X1102.0010
ANXIETY MANAGEMENT AND APPLIED RELAXATION IN REDUCING GENERAL ANXIETY
DONALD F. HUTCHINGS, DOUGLAS R. DENNEY,*~ JOANN BASGALL and B. KENT HOUSTON*
University of Kansas
(Rrccived I I Su/)rumhrr 1979)
Summary-Sixty-three generally anxious subjects were assigned to anxiety management training, applied relaxation training. reiaxation-only. placebo and untreated control conditions. After 6 weeks of treatment. anxiety management training led to reductions on a variety of self-report measures of state and trait anxiety and decreases in maladaptive cognitions during a laboratory stress procedure. On several measures, subjects in anxiety management training differed from relaxation-only and placebo subjects as well as untreated controls. However. treatment effects did not extend to performance and physioio~cal measures of anxiety. Applied relaxation training. which in contrast to anxiety management training lacks structured rehearsal involving the recog- nition and reduction of tension cues during the treatment sessions. resulted in less consistent decreases in measures of general anxiety.
Several behavioral techniques have been developed for the treatment of specific. circum- scribed fears. Relatively little attention, however, has been paid to the clinically more commoti problem of chronic, general anxiety. Clients who suffer from this problem experience anxiety in a variety of settings, thus making it difficult to determine specific antecedents for their emotional state. This absence of situational specificity, in turn, has impeded the development of behavioral treatments for general anxiety.
Recently, behavior therapists have devoted increasing attention to cognitive variables influencing one’s emotional state. With greater consideration being paid to the role of cognitive variables, the necessity of specifying external antecedents for anxiety may have declined. The adoption of a cognitive-mediational perspective in behavior therapy has been accompanied by an emphasis upon training in self-control (Thoresen and Mahoney, 1974). Two self-control procedures- applied relaxation training and anxiety management training-warrant consideration as treatments of chronic anxiety. Both procedures attempt to provide clients with coping skills to deal with the affective, physical and cognitive manifestations of anxiety irrespective of the external antecedent conditions in which they occur. Because these techniques do not depend upon the formulation of specific fear hierarchies, they appear to be especially appropriate for the treatment of general anxiety.
Appiied relaxation training (Denney, 1980; Goldfried, f971) is introduced with a self- control ratiohale emphasizing the attainment of voluntary control over anxiety and the application of this coping skill in anxiety-provoking situations. Clients first receive exten- sive training in the induction of relaxation. Additional instructions and discussions are then devoted to the application of relaxation in real life settings. Although several investi- gators have shown applied relaxation training to be effective in reducing test anxiety (Chang-Liang and Denney, 1976; Russell r~ al., 1976) and speech anxiety (Goldfried and Trier, 1974; Russell and Wise, 1976). no controlled outcome studies have evaluated the effectiveness of this technique in the treatment of general anxiety.
Anxiety management training (Suinn, 1976) bears many similarities to applied relaxa- tion training. Clients receive basically the same type of self-control rationale, relaxation training and application instructions used in applied relaxation training. However, an
* This study was supported by Kansas University General Research Fund award No.‘3129-x308 to D. R. Denney and No. 3293-x038 to B. K. Houston.
t Requests for reprints should be addressed to Douglas R. Denney. Department of Psychology. Fraser Hall 426, University of Kansas. Lawrence KS 66045. U.S.A.
182 DONALD F. HUTCHINGS. DOUGLAS R. DEWEY. JOANN BASGALL and B. KEUT HOUSTON
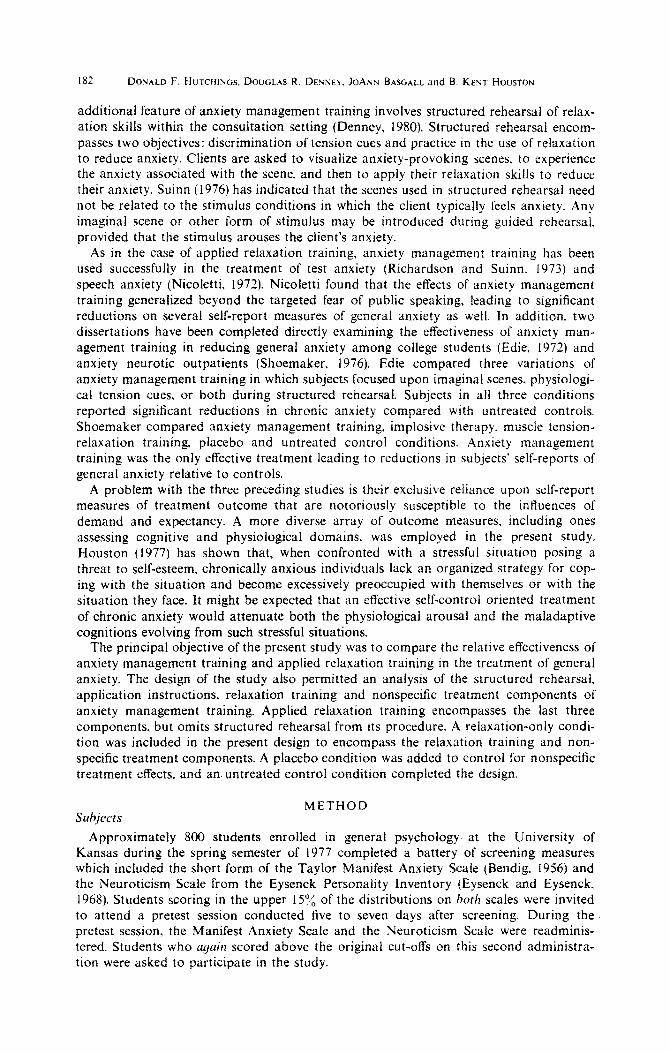
additional feature of anxiety management training involves structured rehearsal of relax- ation skills within the consultation setting (Denney, 1980). Structured rehearsal encom- passes two objectives: discrimination of tension cues and practice in the use of relaxation to reduce anxiety. Clients are asked to visualize anxiety-provoking scenes. to experience the anxiety associated with the scene, and then to apply their relaxation skills to reduce their anxiety. Suinn (1976) has indicated that the scenes used in structured rehearsal need not be related to the stimulus conditions in which the client typically feels anxiety. Any imaginai scene or other form of stimulus may be introduced during guided rehearsal, provided that the stimulus arouses the client’s anxiety.
As in the case of applied relaxation training, anxiety management training has been used successfully in the treatment of test anxiety (Richardson and Suinn. 1973) and speech anxiety (Nicoletti, 1972). Nicoletti found that the effects of anxiety management training generalized beyond the targeted fear of public speaking, leading to significant reductions on several self-report measures of general anxiety as well. In addition. two dissertations have been completed directly examining the effectiveness of anxiety man- agement training in reducing general anxiety among college students (Edie, 1972) and anxiety neurotic outpatients (Shoemaker, 1976). Edie compared three variations of anxiety management training in which subjects focused upon imaginal scenes. physiologi- cal tension cues, or both during structured rehearsal. Subjects in ail three conditions reported significant reductions in chronic anxiety compared with untreated controls. Shoemaker compared anxiety management training, implosive therapy. muscle tension- relaxation training, placebo and untreated control conditions. Anxiety management training was the only effective treatment leading to reductions in subjects’ self-reports of general anxiety relative to controIs.
A problem with the three preceding studies is their exclusive reliance upon self-report measures of treatment outcome that are notoriously susceptible to the influences of demand and expectancy. A more diverse array of outcome measures, including ones assessing cognitive and physiological domains, was employed in the present study. Houston (1977) has shown that, when confronted with a stressful situation posing a threat to self-esteem. chronically anxious individuals lack an organized strategy for cop- ing with the situation and become excessively preoccupied with themselves or with the situation they face. It might be expected that an effective seif-control oriented treatment of chronic anxiety would attenuate both the physiological arousal and the maladaptive cognitions evolving from such stressful situations.
The principal objective of the present study was to compare the relative effectiveness of anxiety management training and applied relaxation training in the treatment of general anxiety. The design of the study also permitted an analysis of the structured rehearsal. application instructions, relaxation training and nonspecific treatment components of anxiety management training. Applied relaxation training encompasses the last three components, but omits structured rehearsal from its procedure. A relaxation-only condi- tion was included in the present design to encompass the relaxation training and non- specific treatment components. A placebo condition was added to control for nonspecific treatment effects. and an. untreated control condition completed the design.
METHOD Subjects
Approximately 800 students enrolled in general psychology at the University of Kansas during the spring semester of 1977 completed a battery of screening measures which included the short form of the Taylor Manifest Anxiety Scale (Bendig. 1956) and the Neuroticism Scale from the Eysenck Personality Inventory (Eysenck and Eysenck, 1968). Students scoring in the upper 15’/, of the distributions on both scales were invited to attend a pretest session conducted five to seven days after screening. During the pretest session, the Manifest Anxiety Scale and the Neuroticism Scale were readminis- tered. Students who ugain scored above the original cut-offs on this second administra- tion were asked to participate in the study.
Anxiety management and applied relaxation 183
A total of 70 students (48 females. 22 males) who met the above criteria and could schedule the treatment sessions were randomly assigned in equal numbers to five experi- mental conditions (anxiety management training. applied relaxation training, relaxation- only, placebo and untreated control). Subjects in the four treatment conditions were further assigned to one of two treatment groups (described below). Subjects fulfilled a course-related research requirement through their participation in the study. Seven sub- jects failed to complete the study, primarily due to scheduling conflicts or disenrollment from general psychology.
Treatments
The treatment groups consisted of 5-7 subjects and.met once a week for a period of 6 weeks. Each group was led by one of two therapists, a male or a female graduate student in clinical psychology. Each therapist conducted one group in each of the four treatment conditions. A 50-page therapy manual was prepared to train the therapists in a standard- ized administration of each treatment condition. It should be noted that neither the therapist nor the investigators in this study held any preconceptions as to the relative effectiveness of anxiety management or applied relaxation training; to date, these pro- cedures had never been compared.
Treatment sessions lasted 75 min and were conducted in a group therapy room in the department’s Psychological Clinic. Subjects in the anxiety management training, applied relaxation training. and relaxation-only groups reclined on lounge chairs during each session. Those in the placebo groups sat in regular armchairs facing a 23-in. television monitor.
Expectancy measures were administered at the end of the first and second treatment session. To minimize the effects of demand upon subjects’ reports of the gains they expected to make through treatment, the second expectancy measure consisted of a single scale embedded in an anonymous questionnaire from a fictitious, university committee concerned with treatment outcome research. Basically, both expectancy measures required subjects to rate on a IO-point scale the degree of progress they expected to make in terms of overcoming their problems with anxiety.
Anxiety management training was introduced with a self-control rationale followed by a 40-min audiotaped presentation of progressive relaxation. Subjects were instructed to practice relaxation at home twice daily and were provided with ‘forms for recording their progress during homework. Subsequent treatment sessions began with a discussion of the effectiveness of the homework, followed by a brief IO-min practice in relaxation, and then three repetitions of structured rehearsal. Structured rehearsal involved having subjects visualize a scene from their past that was associated with a high level of anxiety. Further instructions to focus upon the physical and psychological aspects of anxiety were given in order to facilitate the arousal of anxiety. When all subjects had signaled that they were experiencing anxiety, they were asked to note the location and stimulus properties of this experience and then to switch off the anxiety scene and practice relaxing away the anxiety. Initially, subjects’ return to relaxation was guided by the therapist; however, during the last three sessions, subjects. relaxed on their own, without the aid of the therapist. Subjects were instructed to signal once again when they had returned to a deeply relaxed state. At the end of the third session, subjects were instructed in the application of relaxation-based coping skills in real life settings using tension as a signal to apply these skills. During subsequent sessions, time was allotted for discussion and further coaching in these in uivo applications. The anxiety management training pro- cedure used in this study was patterned after the description by Suinn (1977).
Applied relarariorl rraining utilized the same self-control rationale, homework assign- ments, and application instructions as anxiety management training. The applied relaxa-. tion procedure omitted structured rehearsal, substituting more elaborate and varied relaxation instructions in its place. Six different audiotaped relaxation mstructions were prepared for this purpose, each tape introducing a new variation (e.g. autogenic exercises, guided imagery) upon the basic progressive relaxation procedure. While applied relaxa-
184 DONALD F. HVTCHINGS. DOUGLAS R. DENNEY. JOANN BASGALL and B. KENT HOUSTON
tion training and anxiety management training both included extensive training in relax- ation, the former involved more elaborate and formal audiotaped presentations concern- ing a variety of relaxation techniques whereas the latter employed briefer. ‘live’ presen- tations largely within the context of structured rehearsal. The applied relaxation training procedure incorporated the suggestions and guidelines presented by Denney (1980).
Relaxation-only employed the same six audiotaped relaxation instructions and the same homework assignments used in applied relaxation training. Unlike anxiety manage- ment training and applied relaxation training, however, subjects in the relaxation-only groups received a passive rationale suggesting that relaxation would automatically come to supplant anxiety as they continued their relaxation training. There was no mention of voluntarily self-controlling anxiety and no instructions concerning the application of relaxation in anxiety-provoking settings.
Placebo groups received a passive rationale similar to that used in the relaxation-only condition suggesting that anxiety would dissipate automatically as the subjects continued in treatment. The placebo procedure was fashioned after T-scope therapy (Marcia et al.,
1969). Subjects were shown six I-hr videotaped programs dealing with topics relating to psychology (e.g. depression. sex roles, aggression). Vaguely distinguishable images of people’s faces, blurred movement, fire, etc.. were superimposed on the tapes for random intervals of l-l.5 set using a Sony Special Effects Generator. Subjects were told that subliminal frames containing a variety of anxiety-provoking stimuli had been implanted in the tapes. Although not consciously perceptible, these frames would purportedly serve to ‘unconsciously extinguish’ the subjects’ anxiety.
No treatment control subjects completed the pre-test and post-test battery and partici- pated in a laboratory stress procedure but received no intervening treatment.
Mrusurrs
Pretest and post-test battery. A pre-test session was conducted 1 week before the beginning of treatment, and a post-test session 1 week after the completion of treatment. The same sequence of tests was administered on both occasions and included the Mani- fest Anxiety Scale and Neuroticism Scale, described previously. the trait form of the
State-Trait Anxiety Inventory (Spielberger et al., 1970), the Anxiety Symptom Checklist and Anxiety Performance Test (both described below), and the state form of the State- Trait Anxiety Inventory.
The Anxiety Symptom Checklist was adapted from Nicoletti (1972) and consisted of a list of 40 physical and psychological symptoms of anxiety. Subjects used separate j-point scales to rate each symptom according to its frequency, intensity, and interference. The Anxiety Performance Test consisted of 24 anagram. analogy, and multiple-choice items, administered under a strict IO-min time limit. The test was introduced with anxiety- elevating instructions describing the measure as an intelligence test widely used to predict
academic and occupational success. The test was thought to constitute a potential threat to subjects’ self-esteem, and the extent to which generally anxious subjects had achieved control over anxiety might be reflected in their performance on this test. Alternate forms of the Anxiety Performance Test were used in the pre-test and post-test sessions. After finishing the test each time, subjects completed the state form of the State-Trait Anxiety Inventory indicating how anxious they felt while taking the test.
Laboratory stwss procedure. Four weeks after completing treatment, subjects indivi- dually participated in a laboratory stress procedure to determine the effectiveness of the treatment conditions in reducing physiological as well as self-report measures of anxiety and in modifying maladaptive cognitions during a stressful situation. The stress pro- cedure was similar to one employed by Houston (I 977) and consisted of four periods: baseline, limits, first performance, and second performance. During the limits period, subjects were given the Digits Backward subtest of the Wechsler Adult Intelligence Scale with standard instructions (Wechsler, 1955, p. 41). Subjects’ limits for digits backward was determined as one digit less than the level at which they failed the sub-test. Subjects were then given six more sets of digits at their limit during the first performance period.
Anxiety management and applied relaxation 185
Following this, stress-inducing instructions indicating that other students had done better at the task were delivered to a!! subjects with the exception of seven subjects from the placebo condition and six subjects from the untreated control condition who were randomly assigned to a non-stress condition to check on the effectiveness of the stress manipulation. During the second performance period, subjects again attempted six more sets of digits at their limit.
In addition to subjects’ scores on the digits backward task during the last three periods, pulse rate, finger pulse volume, skin resistance, and blood pressure readings were collected throughout the laboratory session. For purposes of analysis, these recordings were blocked into five 30-set recording periods occurring at the end of the baseline, limits, and first performance periods, immediately after the stress-inducing instructions, and finally, at the end of the second performance period. In addition to the physiological measures, the anxiety scale of the Multiple Affect Adjective Check List (Zuckerman and Lubin. 1965) was administered four times during the stress procedure, permitting subjects to indicate their levels of anxiety during the baseline and limits periods, immediately following the stress inducing instructions. and during the second performance period.
Finally. at the conclusion of the stress procedure, subjects who had received the stress-inducing instructions were asked to complete an open-ended Cognitive Coping Questionnaire concerning their thoughts and feelings during the last performance period. Subjects’ responses to the questionnaire were later judged by two clinical psychologists with regard to which of the following two groups of cognitive coping behaviors had predominated during the second performance period: (a) preoccupation with self and/or the situation, or lack of strategy for coping with stress; or (b) use of some kind of strategy for coping with stress. The psychologists were unaware of the subjects’ treatment condi- tions. Independent agreements occurred for 70% of the subjects, indicating a significant degree of interrater reliability (p c 0.02), and disagreements were subsequently resolved by conference.
Follow-up hartrry. Twelve months after post-testing, subjects were mailed a follow-up battery of self-report measures which included the Manifest Anxiety Scale, the Neuroti- cism Scale, and the Anxiety Symptom Checklist. After repeated reminders, 38 subjects (60”,/,) returned the follow-up battery. This return rate was essentially equivalent across a!! five experimental conditions.
RESULTS AND DISCUSSION Expectancy measure’s
Separate 2 (Therapists) x 4 (Treatment Conditions) analyses of variance were per- formed on subjects’ responses to the expectancy measures administered at the end of the first and second treatment sessions. These analyses revealed no significant differences between groups in terms of their levels of expectancy regarding treatment.
Prr-test, post-rest and ,follow-up mrasurrs
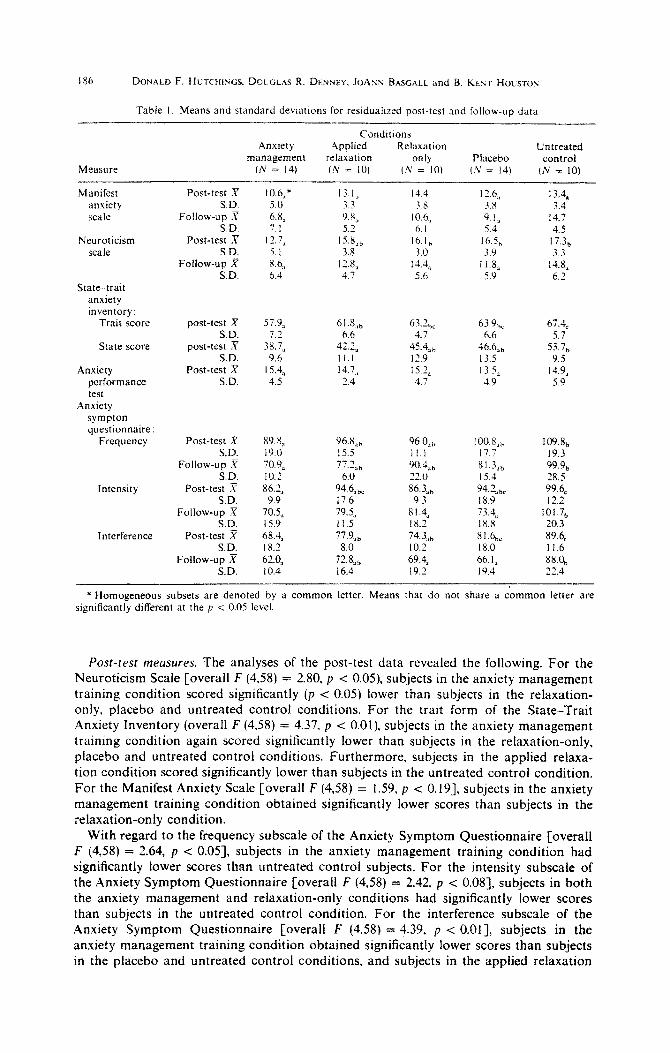
Preliminary analyses performed on the outcome measures revealed no significant ini- tial differences among the five experimental conditions and no main effects or interac- tions involving therapists. Based on the latter findings, therapist was eliminated as a factor in a!! subsequent analyses. Since base-free measures of change are desirable, resi- dualized post-test and follow-up scores (cf. Cronbach and Furby, 1970) were derived for each measure. The residualized post-test scores and the residualized follow-up scores for each outcome measure were then subjected to a one-way analysis of variance comparing all five experimental conditions. Means and standard deviations for the residualized post-test and follow-up scores for each measure are presented in Table 1. Whenever a significant overall F was obtained. paired comparisons between experimental conditions were conducted using t tests. as recommended by Carmer and Swanson (1973) and Bernhardson (1975). Whenever the overall F did not reach significance at the p < 0.05 level, paired comparisons between experimental conditions were conducted using Duncan Multiple Range Tests.
186 DONALD F. HCTCHINGS. DOUGLAS R. DENNW. JOANX BASGALL and B. KEXT HOLSTON
Table I. Means and standard deviations for residualized post-test and follow-up data
Measure
Conditions Anxiety Applied Relaxation Untreated
management relaxation Only Placebo control (Iv = 14) (N = IO) (.V = IO) (.V = 14) (N = IO)
Manifest anxiety scale
Neuroticism scale
State-trait anxiety inventory:
Trait score
State score
Anxiety performance test
Anxiety sympton questtonnaire:
Frequency
Intensity
Interference
Post-test X S.D.
Follow-up X SD.
Post-test ;Y SD.
Follow-up x SD.
10.6,’ 5.0 6.8, 7.1
17.7, 5. I 4.6, 6.4
13.1, 3.3 9.8, 5.2
15.8,, 3.8
l-1.8, 4.7
post-test X 57.9, 61.X,, S.D. 7.2 6.6
post-test X 38.7, 42.2, SD. 9.6 I I.1
Post-test X 15.4, 14.7, SD. 4.5 1.4
Post-test X 89. n,, SD. 19.0
Follow-up x’ 70.9, S.D. 10.2
Post-test X 86.2> S.D. 9.9
Follow-up x 70.5* SD. IS.9
Post-test X 68.4& SD. 18.2
Follow-up x 62.0, SD. 10.4
96.X,, 15.5 77.2,,
6.0 94.6>,, 17.6 79.5, I i.5 ??.9,,
8.0 72X,, 16.4
I-t.4 12.6, 13.4, %Y 3.8 3.4
IO.6,, 9.1, 14.7 6. I 5.4 4.5
16.1, 16.5, 17.3b 3.0 3.9 3.3
14.4, 11.8, 14.8, 5.6 5.9 6.7
63.2 hC
4.7 45.jAb 12.9 15.2, 4.1
96.0,, i I.1 90.4,, 22.0 Y6.3,,
9.3 81.4, 18.2 74.3,, 10.2 69.4, 19.2
63.9, 67.& 6.6 5.7
46.6,, 53.7, 13.5 9.5 13.5, 14.9, 4.9 5.9
lOO.X,, 109.8, 17.7 19.3 8 1 Jab 99.9, 15.4 28.5 94.2,,, 99.4 18.9 t 2.2 73.4, 101.7, L 8.8 20.3 81.& 89.6, 18.0 It.6 66.1, X8.0, 19.1 22.4
* Homogeneous subsets are denoted by a common letter. Means that do not share a common letter are significantly different at the p < 0.05 level.
Post-rest measures. The analyses of the post-test data revealed the following. For the Neuroticism Scale [overall F (4.58) = 2.80, p < 0.05), subjects in the anxiety management training condition scored significantly (p < 0.05) lower than subjects in the relaxation- only, placebo and untreated control conditions. For the trait form of the State-Trait Anxiety Inventory (overall F (4,58) = 4.37, p < 0.01). subjects in the anxiety management training condition again scored significantly lower than subjects in the relaxation-only, placebo and untreated control conditions. Furthermore, subjects in the applied relaxa- tion condition scored significantly lower than subjects in the untreated control condition. For the Manifest Anxiety Scale [overall F (4,58) = 1.59, p < 0.191, subjects in the anxiety management training condition obtained significantly lower scores than subjects in the relaxation-only condition.
With regard to the frequency subscale of the Anxiety Symptom Questionnaire [overall F (4,58) = 2.64, p < 0.051, subjects in the anxiety management training condition had significantly lower scores than untreated control subjects. For the intensity subscale of the Anxiety Symptom Questionnaire [overall F (4,58) = 2.42. p < O.OS], subjects in both the anxiety management and relaxation-only conditions had significantly lower scores than subjects in the untreated control condition. For the interference subscale of the Anxiety Symptom Questionnaire [overall F (4,58) = 4.39, p c O.Ol], subjects in the anxiety management training condition obtained significantly lower scores than subjects in the placebo and untreated control conditions, and subjects in the applied relaxation
Anxiety management and applied relaxation 187
condition obtained significantly lower scores than subjects in the untreated control condition.
Although no differences occurred in subjects’ scores on the Anxiety Performance Test (overall F < 1). scores from the state form of the State--Trait Anxiety Inventory revealed differences in the levels of anxiety that subjects experienced while working on the per- formance test [overall F (4,58) = 3.45, p < 0.01). Subjects in both anxiety management training and applied relaxation training conditions reported significantly less state anxiety than untreated control subjects.
In summary. on six of the eight measures of state or trait anxiety collected at the time of the post-test, subjects in the anxiety management training condition exhibited lower levels of anxiety than untreated controls, and on faur of these measures, subjects in the anxiety management training condition also exhibited less anxiety than relaxation-only and/or placebo subjects. Applied relaxation training, on the other hand, was consistently less effective than anxiety management training. Subjects in the applied relaxation train- ing condition differed from untreated controls on only four of the eight measures col- lected at post-test and never differed from relaxation-only or placebo subjects.
Follo~~~p nwusures. Analyses were performed comparing subjects who did and those who did not return the follow-up materials on all the pre-test and residuaiized post-test measures. No significant main effects or interactions were found involving the subject variable. thus lending support to the assumption that the subjects from whom follow-up materials were obtained were representative of all the subjects who had participated in the study.
Analyses of the 12-month follow-up data revealed the following. For the Manifest Anxiety Scale [overall F (4,32) = 2.28, p = 0.0831, subjects in the anxiety management training condition obtained significantly lower scores than subjects in the untreated control condition. With regard to the intensity subscale of the Anxiety Symptom Ques- tionnaire [overall F (4,32) = 3.61, p = 0.0151, subjects in all four treatment groups obtained significantly lower scores than untreated control subjects. For the interference subscale of the Anxiety Symptom Questionnaire [overall F (4,32) = 4.45, p < 0.0063, subjects in the anxiety management training, relaxation-only, and placebo conditions obtained significantly lower scores than untreated control subjects. For the frequency subscale of the Anxiety Symptom Questionnaire [overall F (4.32) = 2.47, p = 0.0651, subjects in the anxiety management training condition obtained significantly lower scores than subjects in the untreated control. There were no significant differences between conditions with regard to Neuroticism scores [overall F (4,32) = 1.06), however. In gen- eral. then. at the time of the 12-month follow-up, subjects who had received anxiety management training continued to exhibit lower levels of general anxiety and fewer problems with anxiety than subjects who had received no treatment. Because of the small Ns at the time of follow-up, however, the differences (a) between the anxiety management and other conditions, and (b) between other conditions and the untreated control condi- tion did not achieve statistical significance.
Lahorutor_v stress measures
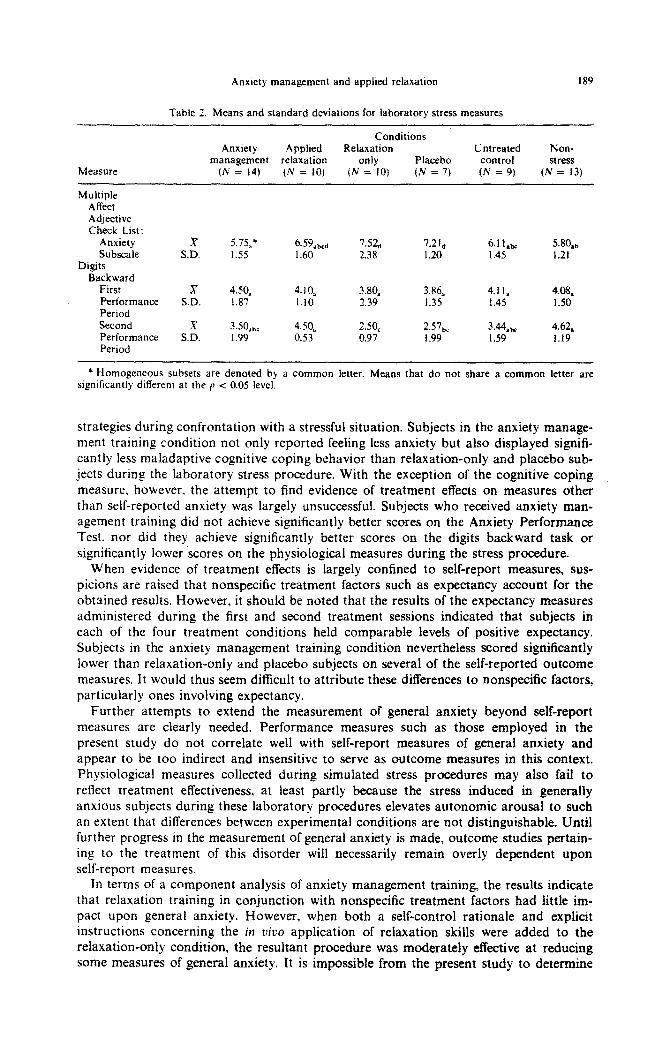
Preliminary analyses performed on' the self-reported anxiety scores and physiological scores revealed no significant baseline differences between the anxiety management train- ing. applied relaxation training, relaxation-only, placebo, untreated control, and non- stress conditions. Nevertheless, to obtain base-free measures of change, self-reported anxiety scores and physiological scores recorded during subsequent periods of the stress procedure were residualized using the respective baseline scores. A 6 (Conditions) x 3 (Periods) analysis of variance conducted on the residualized state anxiety scores from the Multiple Affect Adjective Checklist revealed a significant main effect for conditions [F (5.57) = 3.81. p -c 0.005]. The means for this main effect are reported in Table ‘2. A 6 (Conditions) x 4 (Periods) analysis of variance conducted on the residualized physiologi- cal scores revealed no significant main effects or interactions. A 6 (Conditions) x 2 (Trials) analysis of variance conducted on the digit backward scores for the first and
188 DONALD F. HUTCHINGS, DOUGLAS R. DENNEY. JOANN BASGALL and 8. KENT Hois~ow
second performance periods revealed a significant main effect for trials [F (1 S7) = 6.70. p c 0.011 which was qualified by a significant conditions by trials interaction [F (557) = 2.69, p < 0.031. The mean digit backward scores for the first and second per- formance periods are reported in Table 2. The results of subanalyses performed following the overall analyses are reported in the appropriate sections below.
Stress manipulation. Some evidence of the effectiveness of the stress manipulation is offered by the fact that subjects in the nonstress condition reported significantly less anxiety during the stress procedure than the subjects in the placebo and relaxation-only conditions. In addition, although subjects in the nonstress condition did not differ signifi- cantly from those in the other conditions in terms of their digits_ backward performance during the first ~rformance period, they did perform signi~cantly better than subjects in the placebo and relaxation-only conditions during the second performance period after these subjects had received the stress manipulation. It should be noted. however, that no significant differences were found between the nonstress condition and any of the other conditions on the physiological measures. Thus. evidence of the effectiveness of the stress manipulation is confined to the self-report and digits backward performance data.
Treatment di$ierences. Subjects in the anxiety management training and applied relaxa- tion conditions reported less anxiety throughout the stress procedure than subjects in either the placebo or relaxation-only conditions. These differences were statistically sig- nificant for the anxiety management training condition, but not for the applied relaxation training condition. Subjects in the anxiety management training and the applied relaxa- tion training conditions also performed the digits backward task better during the second performance period than subjects in either the placebo or relaxation-only conditions. These differences were statistically significant for the applied relaxation training condi- tion, but not for the anxiety management training condition. Once again. it should be noted that no significant differences between conditions occurred for the physiological measures, However, in terms of self-report and digits backward performance data, it appears that subjects in the anxiety management training and applied relaxation training conditions were less anxious in the laboratory stress procedure than subjects in the placebo and relaxation-only conditions.*
Coping behaviors. Classifications of subjects’ responses from the Cognitive Coping Questionnaires were used to determine the percentage of subjects in each condition who had evidenced either preoccupation or lack of a strategy for coping with stress engen- dered during the second performance period. Comparisons between conditions revealed that the percentage of subjects who evidenced these ineffective cognitions was lower in the anxiety management training condition (14%) than in the applied relaxation con- dition (40%, p = 0.15), the relaxation-only condition (60’4, p = 0.02), the placebo con- dition (57%, p = 0.05), and the untreated control condition (33’?& p = 0.29). None of the other comparisons between conditions was statistically significant.
CONCLUSIONS
Nicoletti (1972), Edie (19723, and Shoemaker (1976) have all reported evidence than anxiety management training is an effective treatment leading to significant decreases in subjects’ self-reports of general anxiety. The present results support this conclusion. Furthermore, this study extends the findings of previous research by demonstrating the impact of anxiety management training upon generally anxious subjects’ cognitive coping
* The untreated control condition did not differ significantly from the anxiety management training. applied relaxation training. or nonstress conditions in any of the above comparisons. In other words. untreated control subjects in the laboratory stress procedure were not very distressed. These results are incongruent with the other results of the study (e.g. Table I) showing that the post-test and follow-up anxiety scores for untreated control subjects were consistently higher than those of treated subjects. It may be that when six subjects were randomly removed from the untreated control conditton to form the nonstress condition within the laboratory stress procedure, the subjects remaining in the untreated control condition were substantially lower in anxiety and hence less prone to become upset during the stress procedure. Thus. when considering data from the stress procedure. comparisons with relaxation-only and placebo conditions rather than the untreated control condi- tion seem more appropriate.
Anxiety management and applied relaxation 189
%bie 2. Means and standard deviations for laboratory stress measures
Measure
Conditions Anxiety Applied Relaxation Untreated Non-
management relaxation only Placebo control stress (N = 14) (iV = IO) (N = IO) (N = 7) (N = 9) (N = 13)
Multiple Affect Adjective Check List:
Anxiety Subscale
Digits Backward
First Perlormance Period Second Performance Period
x .5.75,+ 6.59&G, 7.52, 7.21, 6.11,, 5.80,, SD. 1.55 1.60 2.38 1.20 I .45 1.21
x 4.50, 4.10, 3.84 3.86, 4.11, 4.08, SD. 1.87 1.10 2.39 I.35 1.45 1.50
.y 3.50,,, 4.50, 2.50, 2.57,, 344&z 4.62, S.D. 1.99 0.53 0.97 1.99 I .59 1.19
* Homogeneous subsets are denoted by a common letter. Means that do not share a common letter are significantly different at the p < 0.05 level.
strategies during confrontation with a stressful situation. Subjects in the anxiety manage- ment training condition not only reported feeling less anxiety but also displayed signifi- cantly less maladaptive cognitive coping behavior than relaxation-only and placebo sub- jects during the laboratory stress procedure. With the exception of the cognitive coping measure, however, the attempt to find evidence of treatment effects on measures other than self-reported anxiety was largely unsuccessful. Subjects who received anxiety man- agement training did not achieve significantly better scores on ,the Anxiety Performance Test. nor did they achieve significantly better scores on the digits backward task or significantly lower scores on the physiological measures during the stress procedure.
When evidence of treatment effects is largely confined to self-report measures, sus- picions are raised that nonspecific treatment factors such as expectancy account for the obtained results. However, it should be noted that the results of the expectancy measures administered during the first and second treatment sessions indicated that subjects in each of the four treatment conditions held comparable levels of positive expectancy. Subjects in the anxiety management training condition nevertheless scored significantly lower than relaxation-only and placebo subjects on several of the self-reported outcome measures. It would thus seem difficult to attribute these differences to nonspecific factors, particularly ones involving expectancy.
Further attempts to extend the measurement of general anxiety beyond self-report measures are clearly needed. Performance measures such as those employed in the present study do not correlate well with self-report measures of general anxiety and appear to be too indirect and insensitive to serve as outcome measures in this context. Physiologica measures collected during simulated stress procedures may also fail to reflect treatment effectiveness, at least partly because the stress induced in generally anxious subjects during these laboratory procedures elevates autonomic arousal to such an extent that differences between experimental conditions are not distinguishable. Until further progress in the measurement of general anxiety is made, outcome studies pertain- ing to the treatment of this disorder will necessarily remain overly dependent upon self-report measures.
In terms of a component analysis of anxiety management training, the results indicate that relaxation training in conjunction with nonspecific treatment factors had little im- pact upon general anxiety. However, when both a self-control rationale and explicit instructions concerning the in uiuo application of relaxation skills were added to the relaxation-only condition, the resultant procedure was moderately effective at reducing some measures of general anxiety. It is impossible from the present study to determine
190 DONALD F. HUTCHINGS. DOUGLAS R. DENNEY, JOANN BASGALL and B. KLST HOCSTO\
the separate contributions of the self-control rationale and the application instructions to the added effectiveness of applied relaxation training. However. a study by Denney and Rupert (1977) indicated that both rationale and procedural components may be necess- ary in fashioning effective self-control treatments for test anxiety.
The addition of a structured rehearsal component to applied relaxation training led to the most effective procedure for treating general anxiety examined in the present study. This rehearsal may assist individuals to become aware of physical signs of anxiety and tension more quickly. By practising their coping skills in the relatively safe confines of the consultation setting, subjects are also better prepared to use these skills in real life situations engendering anxiety and more confident of the ability to self-manage their anxiety in such settings.
REFERENCES
ALPI:RT R. and HARER R. N. (1960) Anxiety m academic achievement situations. J. uhr~or!!~. \oc. P.sychol. 61. 207-215.
BI:NDIG A. W. (1956) The development of a short form of the manifest anxiety scale. J. cortsulr. Pv~~chol. 20. 384. BI:RNHARDSON C. S. (1975) Type I error rates when multiple comparison procedures follow a significant f test
of ANOVA. Bio,ncrrics 31. 229-232. CARMI~R 3. G. and SWANSON M. R. (1973) An evaluation of ten pairwise multiple comparison procedures by
Monte Carlo methods. J. Ant. Sturisr. Ass. 63. 66-74. CKONRACH L. J. and F~REY L. (1970) How we should measure change-or should we’? P.syc~ho/. Bull. 74. 68-80. CHANG-LIANG R. and D~NNEY D. R. (1976) Applied relaxation as training in self-control. J. Co~!tl.sc/. Psychoi.
23. I83- 189. DENNCY D. R. and RUPFRT P. A. (1977) Desensitization and self-control in the treatment of test anxiety. J.
Cou,tsc4. Psycho/. 24, 272-280. DENNEY D. R. (1980) Self-control approaches to the treatment of text anxiety. In Tesr .Amier~ Throrv.
Rrsrarch. and Appkotions (Edited by 1. G. Sarason). Lawrence Erlbaum Associates. Hillsdale. New Jersey. EDIE C. (1972) Uses of anxiety management training in treating trait anxiety. Unpublished doctoral dissertation.
Colorado State University. Fort Collins. Colorado. EYSI:NCE; H. J. and EYSENCK S. B. G. (1968) Man& /or rho E.rse,rck Prrsomlif~~ Iwwror!~. EducatIonal and
Industrial Testing Service. San Diego. California. GOLDFRIED M. R. (1971) Systematic desensitization as training in self-control. J. comulr. cliu. Ps~~cltol. 37.
228-234. GOLDFRIED M. R. and TRIER C. S. (1974) Effectiveness of relaxation as an active coping skill. J. &rlo~t?l. Psycho/.
83. 348-355. HOUSTON B. K. (1977) Dispositional anxiety and the effectiveness of cognitive coping strategies m stressful
laboratory and classroom situations. In S:rcss and Anriery (Edited by C. D. Spielberger and 1. G Sarason). Hemisphere. Washington.
MARCIA J. E.. RUBIN B. M. and EfRAN J. S. (1969) Systematic desensitization: Expectancy change or counter- conditioning. J. ohuorrn. Ps~chol. 74. 382-387.
NI~OLE~~J J. (1972) Anxiety management training. Unpublished doctoral dissertation. Colorado State Univer- sity. Fort Collins. Colorado.
RICHARDSON F. and SUINN R. (1973) A comparison of traditional systematic desensitization. accelerated desensitization. and anxiety management training in the treatment of mathematics anxiety. Brllac. Thu. 4. 212-218.
RU~.SELL R. K. and WISE F. (1976) Treatment of speech anxiety by cue-controlled relaxation and desensttlzation with professional and paraprofessional counselors. J. Counsel. Psycho/. 23. 583-586.
RUSSELL R. K.. WISE F. and STRATOUDAKIS J. P. (1976) Treatment of test anxiety bj cue-controlled relaxation and systematic desensitization. J. Co~msrl. Psychol. 23. 563-566.
SHOEMAKER J. E. (1976) Treatments for anxiety neurosis. Unpublished doctoral dissertation. Colorado State University. Fort Collins. Colorado.
SPIELRERGER C. D.. GORSUCH R. L. and LUSHENE R. E. (1970) Marruul for rlrr Star+Twit .Amwty Imwror~.
Consulting Psychologists Press. Palo Alto. California. SL.INN R. M. (1976) Anxiety management training to control general anxietv. In Cotrrwliml Mrrhods (Edited by
J. Krumboltz and C. ?horese\). Holt. Rinehart & WinsTon. New York. S&INN R. M. (1977) Mmual-Amxirry Manayrrw~t Traiuirg. R. M. Suinn. Ft. Collins. Colorado. THORESEN C. E. and MAHONEY M. J. (1974) Behuoioral Self-Control. Holt. Rinehart & Winston. New York. WECHSLER D. (1955) Mu,ura/ /or the Wvchslrr Adult Iutrlligrrm SC&. Psychological Corporation. New York. ZUCKERMAN M. and LUBIN B. (1965) Mu/rip/v Af&cr Adjecriw Chrck List. Educational and Industrial Testing
Service. San Diego. California.