Embed Size (px)
DESCRIPTION
Aortic Emergencies. David Peterson February 3, 2005. Objectives. Define aortic dissection + AAA and demonstrate their clinical relevance Review pathophysiology and classification Discuss diagnostic modalities Discuss management options Series of questions and cases. PERSPECTIVE. - PowerPoint PPT Presentation
Citation preview

Aortic EmergenciesAortic Emergencies
David PetersonDavid PetersonFebruary 3, 2005February 3, 2005

ObjectivesObjectives
• Define aortic dissection + AAA and Define aortic dissection + AAA and demonstrate their clinical relevancedemonstrate their clinical relevance
• Review pathophysiology and Review pathophysiology and classificationclassification
• Discuss diagnostic modalitiesDiscuss diagnostic modalities• Discuss management optionsDiscuss management options• Series of questions and casesSeries of questions and cases

PERSPECTIVEPERSPECTIVE
• 1955 DeBakey outlined principles 1955 DeBakey outlined principles that remain basis for surgical that remain basis for surgical treatment of aortic dissectiontreatment of aortic dissection
• Medical treatment of aortic Medical treatment of aortic dissection was first advocated in the dissection was first advocated in the 1960s and is indicated for certain 1960s and is indicated for certain types of dissectionstypes of dissections

Aortic DissectionAortic Dissection
• ““longitudinal longitudinal cleavage of the cleavage of the aortic media aortic media created by a created by a dissecting dissecting column of column of blood” blood”
Rosen’s Emergency Rosen’s Emergency MedicineMedicine

(A) Normal blood flow in the aorta. (B) Dissection (A) Normal blood flow in the aorta. (B) Dissection occurs when the inner lining of the aorta tears and the occurs when the inner lining of the aorta tears and the blood flow ‘dissects’ between the layers of the aortic blood flow ‘dissects’ between the layers of the aortic
wall wall

Aortic DissectionAortic Dissection
John John RitterRitterAge 54Age 54DEADDEAD

EpidemiologyEpidemiology• UnderreportedUnderreported• Hypertension is the most common risk factor Hypertension is the most common risk factor
associated with aortic dissection and is seen in associated with aortic dissection and is seen in most patientsmost patients
• Incidence 5-10/ 1,000,000 and risingIncidence 5-10/ 1,000,000 and rising• Mortality 1-2%/hour (33% in 1Mortality 1-2%/hour (33% in 1stst 24 hrs) 24 hrs)• High rate of misdiagnosis ~28%High rate of misdiagnosis ~28%• One study suggests EP’s suspect AD in <50% of One study suggests EP’s suspect AD in <50% of
cases cases Sullivan et al. Am J Emerg Med 18: 46-50. Sullivan et al. Am J Emerg Med 18: 46-50.
20002000• Variable presentation including MIVariable presentation including MI• Lack of suspicion for AD is #1 cause of misdiagnosisLack of suspicion for AD is #1 cause of misdiagnosis

EpidemiologyEpidemiology• History of cardiac surgery present 18% and History of cardiac surgery present 18% and
bicuspid aortic valve in 14% of all patients with bicuspid aortic valve in 14% of all patients with aortic dissectionaortic dissection– more often in proximal dissections more often in proximal dissections
• Atherosclerosis rarely involved at site of dissectionAtherosclerosis rarely involved at site of dissection• Aortic dissection uncommon before age 40 except:Aortic dissection uncommon before age 40 except:
– Congenital heart disease, Ehlers-Danlos or Congenital heart disease, Ehlers-Danlos or Marfan syndrome, giant cell arteritis and Marfan syndrome, giant cell arteritis and possibly pregnancypossibly pregnancy
• ~ 44% of patients with Marfan syndrome develop ~ 44% of patients with Marfan syndrome develop aortic dissection and account for 6% of such cases aortic dissection and account for 6% of such cases

Ehlers-DanlosEhlers-Danlos

Marfan Marfan SyndromeSyndrome

Anatomy and PhysiologyAnatomy and Physiology• Each contraction the Each contraction the
heart swings side to side heart swings side to side resulting in flexion of resulting in flexion of both ascending aorta both ascending aorta and descending aortaand descending aorta
• Descending aorta flexes Descending aorta flexes just distal to left just distal to left subclavian artery where subclavian artery where mobile aorta is tetheredmobile aorta is tethered
• At 70 heartbeats per At 70 heartbeats per minute sequence occurs minute sequence occurs 37 million times a year 37 million times a year causing repetitive stress causing repetitive stress on the aorta on the aorta

Anatomy and PhysiologyAnatomy and Physiology• The aortic wall has The aortic wall has three distinct layers: the three distinct layers: the intima, the media, and intima, the media, and the adventitiathe adventitia• The The mediamedia is comprised is comprised of elastic tissue and of elastic tissue and smooth muscle smooth muscle
MEDIA = MiddleMEDIA = Middle INTIMA = InsideINTIMA = Inside

PathophysiologyPathophysiology• Requires 3 Requires 3
basic featuresbasic features::1.1. Abnormal Abnormal
mediamedia2.2. Blood entry Blood entry
into media by into media by intimal tearintimal tear
3.3. Pressure Pressure forces forces favoring favoring propagationpropagation

PathophysiologyPathophysiology

PathophysiologyPathophysiology• Arterial Obstruction is caused by 2 mechanismsArterial Obstruction is caused by 2 mechanisms
– By compressing from the expanding hematomaBy compressing from the expanding hematoma– From occlusion of lumen by intimal flapFrom occlusion of lumen by intimal flap– This results in peripheral complications:This results in peripheral complications:
– CerebralCerebral CVACVA,, syncope syncope – Spinal Spinal Neuro deficitsNeuro deficits– CardiacCardiac MIMI,, tamponade tamponade,, AR AR– RespiratoryRespiratory HemoptysisHemoptysis,, pleural effusion pleural effusion– GIGI HematemesisHematemesis,, dysphagia dysphagia,, mesenteric ischemia mesenteric ischemia– RenalRenal ARFARF,, HTN HTN– LimbsLimbs Extremity ischemiaExtremity ischemia

CT AD : Intimal FlapCT AD : Intimal Flap

• Intimal tears occur in Intimal tears occur in 96% of all AD cases96% of all AD cases
• Felt to occur 2Felt to occur 2oo to to shearing forces and shearing forces and hemodynamic hemodynamic stressesstresses
• Propagation factors:Propagation factors:– Degree of HTNDegree of HTN– Slope of pulse wave Slope of pulse wave
(dP/dT)(dP/dT)• Spontaneous cure = Spontaneous cure =
rupture back into rupture back into true lumen (rare)true lumen (rare)
PathophysiologyPathophysiology

Aortic dissection bursts Aortic dissection bursts into the pericardium into the pericardium
•Pericardial Pericardial TamponadeTamponade

• Hemopericardium Hemopericardium and tamponade and tamponade can occur with can occur with dissection into dissection into pericardial sacpericardial sac

The tear progresses down The tear progresses down to and occludes the to and occludes the
coronary artery coronary artery precipitating an MI precipitating an MI
•Almost always an Almost always an inferoposterior MI : RCAinferoposterior MI : RCA

•Coronary artery involvement in ~1% Coronary artery involvement in ~1% presents as MI presents as MI• 0.1-0.2%0.1-0.2% of of MI’sMI’s are complicated by incorrect are complicated by incorrect admin of lyticsadmin of lytics in in setting of setting of ADAD

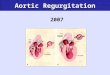
The tear can disrupt the aortic The tear can disrupt the aortic valve, producing acute valvular valve, producing acute valvular
insufficiency, a common cause of insufficiency, a common cause of acute CHF and increased risk of acute CHF and increased risk of
death death
ARAR

Clinical PresentationClinical Presentation• Sudden, severe chest pain (~76-90%)Sudden, severe chest pain (~76-90%)• Migratory CP is highly specific (~71%)Migratory CP is highly specific (~71%)• Back pain (~53%), abd painBack pain (~53%), abd pain• Other Sx depending on site of Other Sx depending on site of
involvementinvolvement– Syncope (~9%)Syncope (~9%)– Neuro Sx (~6-13%)Neuro Sx (~6-13%)– Mesenteric ischemiaMesenteric ischemia– Renal failureRenal failure
• Can be painless in up to 15% (chronic)Can be painless in up to 15% (chronic)Moore et al. Am J Card. 89:1235-1238 2002Moore et al. Am J Card. 89:1235-1238 2002Hals. Emerg Med Reports 2000Hals. Emerg Med Reports 2000

Risk Factors for ADRisk Factors for AD• Hypertension (60-90%)Hypertension (60-90%)• Age 50-70 yoAge 50-70 yo• Male (3:1)Male (3:1)• CTD’s (Marfans ~5%, Ehlers-Danlos)CTD’s (Marfans ~5%, Ehlers-Danlos)• Turners, Coarctation, Ebstein’s AnomalyTurners, Coarctation, Ebstein’s Anomaly• Congenital bi-/tricuspid AVCongenital bi-/tricuspid AV• Family Hx or previous dissectionFamily Hx or previous dissection• Cocaine, metamphetamineCocaine, metamphetamine• IatrogenicIatrogenic• TraumaTrauma
Hals. Emerg Med Reports 2000

ClassificationClassification• DeBakeyDeBakey::
– Type IType I: involve ascending aorta, arch, : involve ascending aorta, arch, and descending aortaand descending aorta
– Type IIType II: ascending aorta proximal to L : ascending aorta proximal to L subclavian arterysubclavian artery
– Type IIIType IIIaa: descending aorta only; above : descending aorta only; above diaphragm onlydiaphragm only
– Type IIIType IIIbb: descending aorta only; : descending aorta only; extension below diaphragmextension below diaphragm

DeBakeyDeBakey

StanfordStanford
• Type AType A: : involvement of ascending aortainvolvement of ascending aorta• Type BType B: : no involvement of ascending no involvement of ascending
aortaaorta• ~~62.5%62.5% of pts w/ AD have aof pts w/ AD have a Type AType A• Involvement of ascending aorta is of Involvement of ascending aorta is of
prognostic and therapeutic importanceprognostic and therapeutic importance

Diagnosing ADDiagnosing AD• Clinical suspicion above allClinical suspicion above all• 3 clinical variables shown to be useful:3 clinical variables shown to be useful:
• Aortic pain (immediate onset, tearing, ripping)Aortic pain (immediate onset, tearing, ripping)• Mediastinal widening / aortic widening on CXRMediastinal widening / aortic widening on CXR• Pulse or BP differentialsPulse or BP differentials
– Likelihood of AD:Likelihood of AD:• Ø of above variables Ø of above variables 7% risk of AD 7% risk of AD• Pain or widening alone Pain or widening alone 31 + 39% risk of AD 31 + 39% risk of AD
respectivelyrespectively• >> 2 variables or isolated BP / pulse diff 2 variables or isolated BP / pulse diff >> 83% risk of 83% risk of
ADAD Von Kodolitsch et al. Arch Intern Med. 160: 2977-82. 2000Von Kodolitsch et al. Arch Intern Med. 160: 2977-82. 2000
• Diagnostic modalitiesDiagnostic modalities• ECG, CXR, CT, TEE, Angiogram, MRIECG, CXR, CT, TEE, Angiogram, MRI

ECG findings in ADECG findings in AD
• ~85% will be abnormal~85% will be abnormal• LVH LVH • Non-specific ST-T wave changesNon-specific ST-T wave changes• MI (RCA most common)MI (RCA most common)• Bottom line: Bottom line:
– not sensitive or specificnot sensitive or specific– beware thrombolysis until AD excludedbeware thrombolysis until AD excluded

CXR findings in ADCXR findings in AD• 80-90% will be abnormal80-90% will be abnormal• Most findings non-specific:Most findings non-specific:
– Mediastinal widening (~59-75%)Mediastinal widening (~59-75%)– Calcium sign (pathognomonic)Calcium sign (pathognomonic)– Double density aortaDouble density aorta– Obliteration of aortic knuckleObliteration of aortic knuckle– Loss of PA windowLoss of PA window– Tracheal deviation to rightTracheal deviation to right– Depressed left main stem bronchusDepressed left main stem bronchus– New left pleural effusionNew left pleural effusion– Apical capApical cap– Size disparity of ascending + descending aortaSize disparity of ascending + descending aorta

CXRCXR

TEETEE• Rosen: 98% sensitive, 77% specificRosen: 98% sensitive, 77% specific• Moore et al: 88% sensitiveMoore et al: 88% sensitive• 11stst test in Europe and Japan test in Europe and Japan• Advantages:Advantages:
– Can differentiate Type A + B dissectionsCan differentiate Type A + B dissections– Rapid, can be done at bedsideRapid, can be done at bedside– No contrast or radiationNo contrast or radiation– Can detect AR and pericardial effusionCan detect AR and pericardial effusion
• DisadvantagesDisadvantages– Availability, operator dependenceAvailability, operator dependence– Limited info on distal aortaLimited info on distal aorta
Moore et al. Am J Card. 89:1235-1238. 2002Moore et al. Am J Card. 89:1235-1238. 2002

TEE : Aortic DissectionTEE : Aortic Dissection
Intra-operative Intra-operative TEE echo TEE echo demonstrating demonstrating high velocity jet high velocity jet striking aortic striking aortic wall at point of wall at point of intimal injury intimal injury

CT scanningCT scanning• Dynamic helical CT nearly 100% sensitive Dynamic helical CT nearly 100% sensitive
and specific (dye) (Moore et al: 93% sens)and specific (dye) (Moore et al: 93% sens)• Advantages:Advantages:
– Availability, can differentiate Type A + B Availability, can differentiate Type A + B – Able to identify sealed-off false lumensAble to identify sealed-off false lumens– Able to identify other pathology (eg PE)Able to identify other pathology (eg PE)
• Disadvantages:Disadvantages:– Dye reactions (1/10,000 fatal)Dye reactions (1/10,000 fatal)– No info on AV function or intimal tear locationNo info on AV function or intimal tear location– No info about extension into other arteriesNo info about extension into other arteries

CT : Aortic DissectionCT : Aortic DissectionCT of CT of abdominal abdominal aorta show aorta show intimal flap intimal flap ((dark linedark line))with true with true lumen lumen anteriorly and anteriorly and false lumen false lumen posteriorlyposteriorly

CT : Aortic DissectionCT : Aortic Dissection
Stanford Type A Aortic Stanford Type A Aortic DissectionDissection

CT : Aortic DissectionCT : Aortic Dissection
Stanford Type A Aortic DissectionStanford Type A Aortic Dissection

AngiographyAngiography• 81-87% sensitive, 96% specific81-87% sensitive, 96% specific• Previous gold standardPrevious gold standard• Advantages:Advantages:
– Anatomical delineation of aortic treeAnatomical delineation of aortic tree– Ability to demonstrate ARAbility to demonstrate AR– Can differentiate Type A + B dissectionsCan differentiate Type A + B dissections
• Disadvantages:Disadvantages:– False –ves due to false lumen thrombosisFalse –ves due to false lumen thrombosis– Invasive, time consuming, expensiveInvasive, time consuming, expensive

AngiographyAngiography

MRIMRI• Near 100% sensitivity and specificityNear 100% sensitivity and specificity• No role in critical pts but good for serial No role in critical pts but good for serial
follow-upfollow-up• Advantages:Advantages:
– Excellent anatomical delineation, info on AR, Excellent anatomical delineation, info on AR, intimal tear location, type and extent of ADintimal tear location, type and extent of AD
• Disadvantages:Disadvantages:– Time-consumingTime-consuming– Unable to monitor ptUnable to monitor pt

MRIMRI

Intravascular U/SIntravascular U/S• New technique – intravascular U/S probeNew technique – intravascular U/S probe• Currently evolving uses includeCurrently evolving uses include
– Identification of unstable plaques in CADIdentification of unstable plaques in CAD– Diagnostic and therapeutic use in ADDiagnostic and therapeutic use in AD
•3-D imaging of aorta + surrounding structures3-D imaging of aorta + surrounding structures•Guidance of intra-vascular stent placement – Guidance of intra-vascular stent placement –
less invasive procedure than classic surgeryless invasive procedure than classic surgery•Fenestration of intimal flapFenestration of intimal flap
– Not available at most centers at this timeNot available at most centers at this time
Chavan et al. Circulation 96: 2124-2127. 1997Chavan et al. Circulation 96: 2124-2127. 1997


IVUS : Aortic IVUS : Aortic DissectionDissection

So what test do I order So what test do I order 11stst??
• Moore et al: CT is initial test of Moore et al: CT is initial test of choice followed by TEE to clarify Dx choice followed by TEE to clarify Dx or better delineate surrounding or better delineate surrounding anatomy + ARanatomy + AR
Moore et al. Am J Card. 89:1235-1238. 2002Moore et al. Am J Card. 89:1235-1238. 2002
• In Calgary, TEE is considered highly In Calgary, TEE is considered highly accurate and available, and should accurate and available, and should be considered a 1be considered a 1stst line test line test
Peter Giannacarro Peter Giannacarro

Can we predict Can we predict outcomes?outcomes?
• Pulse deficit is independent predictor of 5-day Pulse deficit is independent predictor of 5-day mortality RR 2.73, 95% CI 1.7-4.4mortality RR 2.73, 95% CI 1.7-4.4
• Stat sig trend of increasing mortality with increasing Stat sig trend of increasing mortality with increasing number of pulse deficitsnumber of pulse deficits
– Bosssone et al. Am J Card 89: 851-855. 2002Bosssone et al. Am J Card 89: 851-855. 2002• Mortality predictors:Mortality predictors:
– Age Age > > 70 (OR 1.7, 95% CI 1.05-2.77)70 (OR 1.7, 95% CI 1.05-2.77)– Abrupt onset CP (OR 2.6, 95% CI 1.22-5.54)Abrupt onset CP (OR 2.6, 95% CI 1.22-5.54)– Hypotension/shock/tamponade (OR 2.97, 95% CI Hypotension/shock/tamponade (OR 2.97, 95% CI
1.25-3.29)1.25-3.29)– ARF (OR 1.77; 95% CI 1.80-12.6)ARF (OR 1.77; 95% CI 1.80-12.6)– Pulse deficit (OR 2.03; 95% CI 1.25-3.29)Pulse deficit (OR 2.03; 95% CI 1.25-3.29)– Abnormal ECG (OR 1.77; 95% CI 1.06-2.95)Abnormal ECG (OR 1.77; 95% CI 1.06-2.95)
– Rajendra et al. Circulation. 105: 200-206. 2002Rajendra et al. Circulation. 105: 200-206. 2002

ManagementManagement
• ABC’s and then 2 basic principles:ABC’s and then 2 basic principles:– Control the slope of pulse wave (dP/dT) Control the slope of pulse wave (dP/dT)
•11stst control your HR, then lower the pressure control your HR, then lower the pressure– Surgery if indicatedSurgery if indicated
•All Type A dissections need urgent ORAll Type A dissections need urgent OR• Controversies + New IdeasControversies + New Ideas
– Surgery for Type B dissectionsSurgery for Type B dissections– Intravascular repairIntravascular repair

Medical TxMedical Tx• Control HRControl HR
– IV BB’s – aim for HR 60-80 bpmIV BB’s – aim for HR 60-80 bpm•Esmolol 500 mcg/kg bolus, then titrate Esmolol 500 mcg/kg bolus, then titrate
infusion 50-200 mcg/kg/mininfusion 50-200 mcg/kg/min•Metoprolol 5 mg IVP q5minMetoprolol 5 mg IVP q5min•Propranolol 1mg IVP q5minPropranolol 1mg IVP q5min

Medical TxMedical Tx
• Control BP Control BP •aim for BP 100-120 mmHg sys or min BP aim for BP 100-120 mmHg sys or min BP
req’d to maintain end-organ perfusionreq’d to maintain end-organ perfusion•Nitroprusside 0.5 mcg/kg/min – titrate up Nitroprusside 0.5 mcg/kg/min – titrate up
prnprn
• MonotherapyMonotherapy•Labetalol 20 mg IVP, then 20-80 mg q5-Labetalol 20 mg IVP, then 20-80 mg q5-
10 min until in target HR, then 1-2 mg/hr10 min until in target HR, then 1-2 mg/hr

Surgical TxSurgical Tx• Indicated for:Indicated for:
– All Type A dissectionsAll Type A dissections– Type B w/ complications:Type B w/ complications:
• Aortic ruptureAortic rupture• Severe distal ischemiaSevere distal ischemia• Refractory HTNRefractory HTN• Progressive dissection despite TxProgressive dissection despite Tx• Intractable painIntractable pain
• Mortality for Type A repair is ~7-12%Mortality for Type A repair is ~7-12%• Co-morbidities increase mortalityCo-morbidities increase mortality• 5 yr survival is 77% Type A + 88% Type B5 yr survival is 77% Type A + 88% Type B

Why not operate on all?Why not operate on all?
• Medical Tx of Type B has ~20% Medical Tx of Type B has ~20% mortalitymortality
• Surgical Tx of Type B has 10-15% Surgical Tx of Type B has 10-15% mortality, and 3.5-36% risk of mortality, and 3.5-36% risk of paraplegiaparaplegia
• This may be changing with advent of This may be changing with advent of endovascular repair, fenestration endovascular repair, fenestration procedures, and IVUSprocedures, and IVUS

AAAAAA

AAA: some factsAAA: some facts
• Incidence rising: 2% >65 yoIncidence rising: 2% >65 yo• 9 men for every 1 female9 men for every 1 female• Most have no antecedent Sx Most have no antecedent Sx • 50-80% mortality rate50-80% mortality rate• Misdiagnosed in 30-60% of casesMisdiagnosed in 30-60% of cases

DefinitionsDefinitions
• Aneurysm = irreversible localized Aneurysm = irreversible localized dilatation of an artery to dilatation of an artery to >> 1.5 original 1.5 original diameter (~3cm in abd aorta)diameter (~3cm in abd aorta)
• Types of aneurysms:Types of aneurysms:– True = involves intima, media, and True = involves intima, media, and
adventitiaadventitia– Pseudoaneurysm = only intact + bulging Pseudoaneurysm = only intact + bulging
layer is adventitalayer is adventita– Inflammatory aneurysm = surrounding Inflammatory aneurysm = surrounding
fibrosis and adhesionsfibrosis and adhesions


PseudoaneurysmPseudoaneurysm• Damged Damged
intima + intima + mediamedia
• Adventitia Adventitia prevents prevents rupturerupture

AnatomyAnatomy1.1. AortaAorta2.2. Inf phrenicInf phrenic3.3. R hepaticR hepatic4.4. Common Common
hepatichepatic5.5. GastroduodenalGastroduodenal6.6. Inf pancreatico-Inf pancreatico-
duodenalduodenal7.7. L common iliacL common iliac8.8. L renalL renal9.9. SplenicSplenic10.10.L gastric L gastric

Risk Factors for AAARisk Factors for AAA
• Age 50-70Age 50-70• Male (9:1)Male (9:1)• WhiteWhite• AtherosclerosisAtherosclerosis• HTNHTN• SmokingSmoking• Family HxFamily Hx• Loss of elastin / CTD’s (Marfans)Loss of elastin / CTD’s (Marfans)

Clinical presentationClinical presentation• Unruptured vs. RupturedUnruptured vs. Ruptured
– Unruptured:Unruptured:•Vague abd pain / back pain / pulsations / fullnessVague abd pain / back pain / pulsations / fullness•SMA syndrome (wt loss, vomiting)SMA syndrome (wt loss, vomiting)•Renal colic, radicular Sx, embolic phenomenaRenal colic, radicular Sx, embolic phenomena
– Ruptured:Ruptured:•Classic: abd pain, pulsatile mass, hypotensionClassic: abd pain, pulsatile mass, hypotension•Atypical: Atypical:
– Back or flank pain + hematuriaBack or flank pain + hematuria– LLQ pain + GI bleedingLLQ pain + GI bleeding– Sx of high-output failureSx of high-output failure

Physical FindingsPhysical Findings
• Pulsatile abd massPulsatile abd mass– Palpate each sid of aorta; if >2.5 cm w/uPalpate each sid of aorta; if >2.5 cm w/u– PPV ~43%PPV ~43%
• Other findings neither sensitive or Other findings neither sensitive or specificspecific

How do to Diagnose AAAHow do to Diagnose AAA
• Clinical suspicionClinical suspicion• Diagnostic imagingDiagnostic imaging
– Abd U/SAbd U/S– CT abdCT abd– AngiographyAngiography– MRIMRI
• What test, when, and for whom?What test, when, and for whom?

Plain FilmsPlain Films• Initial screeningInitial screening• Findings in 60-75%Findings in 60-75%
– Calcified wallCalcified wall– Paravertebral soft Paravertebral soft
tissue masstissue mass– Loss of psoas Loss of psoas
shadowshadow– Loss of renal Loss of renal
silhouettesilhouette– Erosion of vertebral Erosion of vertebral
bodiesbodies• Negative study Negative study
does NOT exclude does NOT exclude DxDx

UltrasoundUltrasound• Test of choice, esp in unstable ptsTest of choice, esp in unstable pts• Advantages:Advantages:
– 100% sensitive + specific for AAA100% sensitive + specific for AAA– Rapid (~5 min vs. ~80 min for CT) Rapid (~5 min vs. ~80 min for CT) – can be done at bedsidecan be done at bedside– non-invasivenon-invasive
• DisadvantagesDisadvantages– Poor at identifying rupture Poor at identifying rupture – Technically difficult in obesity / bowel gasTechnically difficult in obesity / bowel gas

AAA : UltrasoundAAA : Ultrasound

Computed TomographyComputed Tomography• 100% sensitive + specific for AAA100% sensitive + specific for AAA• AdvantagesAdvantages
– Able to detect rupturesAble to detect ruptures– Obesity + bowel gas don’t limit studyObesity + bowel gas don’t limit study– Surrounding anatomySurrounding anatomy
• DisadvantagesDisadvantages– Unstable ptsUnstable pts– TimeTime– IV contrast (can do without)IV contrast (can do without)– Not 100% sensitive for ruptureNot 100% sensitive for rupture

•The CT scan done with of oral and intravenously contrast demonstrates opacification of the aorta as well as inferior vena cava•The arrow head points to the presence of the retroperitoneal hematoma, extending into the adjacent paraspinal retroperitoneal tissues
CT : Ruptured AAACT : Ruptured AAA

CT : Ruptured AAACT : Ruptured AAA

AngiographyAngiography
• NOT a ED screening toolNOT a ED screening tool• Tends to underestimate AAA sizeTends to underestimate AAA size• May aid in planning of surgery (e.g. May aid in planning of surgery (e.g.
renal a. stenosis)renal a. stenosis)• Helical CT can produce 3-D images + Helical CT can produce 3-D images +
may replace angiographymay replace angiography

AngiographyAngiography

MRIMRI
• Not useful in acute settingNot useful in acute setting• Excellent anatomical delineationExcellent anatomical delineation• Used primarily prior to elective repairUsed primarily prior to elective repair

MRIMRI

ED ManagementED Management• Depends on contextDepends on context::
– Incidental Dx of AAAIncidental Dx of AAA– Ruptured AAA in “stable” ptRuptured AAA in “stable” pt– Unstable pt with ruptured AAAUnstable pt with ruptured AAA
• Basic principles:Basic principles:– ABC’sABC’s– Surgical referral for allSurgical referral for all
• Elective surgery has ~5% mortalityElective surgery has ~5% mortality• Emergent surgery in non-ruptured AAA ~25% mortalityEmergent surgery in non-ruptured AAA ~25% mortality• Emergent surgery for RAAA ~50% mortalityEmergent surgery for RAAA ~50% mortality
• Controversies:Controversies:– Role of volume resuscitationRole of volume resuscitation

Fluid ResuscitationFluid Resuscitation• Evidence in penetrating trauma for forgoing Evidence in penetrating trauma for forgoing
aggressive volume resusitationaggressive volume resusitation– Bickell et al. N Eng J Med 1994 (331): 1105-1109Bickell et al. N Eng J Med 1994 (331): 1105-1109
• Fluids can cause dilutional coagulopathyFluids can cause dilutional coagulopathy• Ø studies compare ED resus strategies in AAAØ studies compare ED resus strategies in AAA• Recent Cochrane Review: no evidence to Recent Cochrane Review: no evidence to
support any specific fluid resus strategy in support any specific fluid resus strategy in setting of traumatic hypovolemic shocksetting of traumatic hypovolemic shock
Kwan et al. Coch Data Sys Rev. 2002Kwan et al. Coch Data Sys Rev. 2002• Recommendations are to aim for min BP Recommendations are to aim for min BP
necessary to maintain end-organ perfusion + necessary to maintain end-organ perfusion + use blood products earlyuse blood products early

Natural HxNatural Hx
• Formation Formation enlargement enlargement rupture rupture DEATH DEATH
• How can we intervene?How can we intervene?– Primary preventionPrimary prevention– Early management + observationEarly management + observation– Elective surgeryElective surgery– Emergency surgeryEmergency surgery

Risk of RuptureRisk of Rupture• Risk factorsRisk factors
– Size of AAASize of AAA– COPDCOPD– HTNHTN– smokingsmoking
• What is the risk of rupture?What is the risk of rupture?– <4 cm: ~1-1.2%<4 cm: ~1-1.2%– 4-5 cm: 1-3%4-5 cm: 1-3%
• One study suggests surgeons estimate risk of One study suggests surgeons estimate risk of rupture >2x published riskrupture >2x published risk
Lederle. Arch Intern Med 156: 1007-009. 1996Lederle. Arch Intern Med 156: 1007-009. 1996

Current Surgical Current Surgical IndicationsIndications
• All symptomatic aneurysmsAll symptomatic aneurysms• All saccular aneurysmsAll saccular aneurysms• Poor risk pt w/ AAA >6 cmPoor risk pt w/ AAA >6 cm• Good risk pt w/ AAA >5 cmGood risk pt w/ AAA >5 cm• Young, good risk pt w/ AAA 4-5 cmYoung, good risk pt w/ AAA 4-5 cm
Sternbergh et al. Surg Clin NA 78: 827-834. Sternbergh et al. Surg Clin NA 78: 827-834. 19981998

Elective repair of small Elective repair of small AAA’sAAA’s
• 5 yr survival ~76% vs ~30% for 5 yr survival ~76% vs ~30% for emergentemergent
• 2 recent RCT’s suggest no survival 2 recent RCT’s suggest no survival benefit from immediate surgery for benefit from immediate surgery for AAA’s 4-5.4 cmAAA’s 4-5.4 cm– RR 1.21; 95% CI 0.95-1.54RR 1.21; 95% CI 0.95-1.54
Lederle et al. N Eng J Med 346: 1437-44. 2002Lederle et al. N Eng J Med 346: 1437-44. 2002– RR 0.94; 95% CI 0.75-1.17RR 0.94; 95% CI 0.75-1.17
UK Small Aneurysm Trial Participants. Lancet UK Small Aneurysm Trial Participants. Lancet 352: 1649-55. 1998352: 1649-55. 1998

AAA RepairAAA Repair

AAA RepairAAA Repair

AAA RepairAAA Repair

AAA RepairAAA Repair

Traditional vs Traditional vs EndovascularEndovascular• Endovascular repair advantages:Endovascular repair advantages:
– Less invasiveLess invasive– Dec’d blood loss, procedure times, ICU stays, Dec’d blood loss, procedure times, ICU stays,
hospitalization time, and recovery timehospitalization time, and recovery time– Dec’d morbidity but not mortalityDec’d morbidity but not mortality
• DisadvantagesDisadvantages– Expense, limited long-term experience but may be Expense, limited long-term experience but may be
less durable than conventional repairless durable than conventional repair• UtilityUtility
– Clear morbidity advantage in elderly, high risk pts Clear morbidity advantage in elderly, high risk pts demonstrated in recent observational studydemonstrated in recent observational study
Sicard et al. Ann Surg 234: 427-37. 2001Sicard et al. Ann Surg 234: 427-37. 2001– No good evidence to support use in small AAA’s or No good evidence to support use in small AAA’s or
younger ptsyounger pts Brewster. Surgery 131: 363-7. 2002Brewster. Surgery 131: 363-7. 2002

Late complicationsLate complications• Graft infectionGraft infection
– Early or late (up to years after)Early or late (up to years after)– ~30-50% mortality~30-50% mortality– Staphylococcus epidermidisStaphylococcus epidermidis– Present w/ sepsis +/- AEFPresent w/ sepsis +/- AEF– Tx is abx, graft excision, + bypassTx is abx, graft excision, + bypass
• Aorto-enteric fistula (AEF)Aorto-enteric fistula (AEF)– Can form anywhere (usually duodenum)Can form anywhere (usually duodenum)– Acute or chronic GIBAcute or chronic GIB– Tx is graft replacementTx is graft replacement

The EndThe End
QuestionsQuestions??

Question 1Question 11.1. Preexisting conditions associated with an increased risk of Preexisting conditions associated with an increased risk of
aortic dissection include which of the followingaortic dissection include which of the following??
• A.A. Coarctation of the aorta Coarctation of the aorta
• B.B. Congenital heart disease Congenital heart disease
• C.C. Marfan syndrome Marfan syndrome
• D.D. Pregnancy Pregnancy
• E.E. All of the above All of the above
EE

Question 1 Short AnswerQuestion 1 Short Answer• Dissection is the most common and the most lethal Dissection is the most common and the most lethal
catastrophe involving the aorta. Aortic dissection occurs catastrophe involving the aorta. Aortic dissection occurs two to three times more frequently in males than in two to three times more frequently in males than in females, and there may be a higher incidence in blacks. females, and there may be a higher incidence in blacks. Although aortic dissection has been reported in patients as Although aortic dissection has been reported in patients as young as 14 months and as old as 100 years, the majority young as 14 months and as old as 100 years, the majority of cases occur in patients between 50 and 70 years of age. of cases occur in patients between 50 and 70 years of age. Aortic dissection is relatively rare before age 40, except in Aortic dissection is relatively rare before age 40, except in association with specific predisposing syndromes, such as association with specific predisposing syndromes, such as Marfan syndrome, Ehlers-Danlos syndrome, congenital Marfan syndrome, Ehlers-Danlos syndrome, congenital heart disease, familial incidence, pregnancy, coarctation of heart disease, familial incidence, pregnancy, coarctation of the aorta, Turner's syndrome, and trauma. The type of the aorta, Turner's syndrome, and trauma. The type of trauma that is usually associated with aortic dissection is trauma that is usually associated with aortic dissection is iatrogenic, such as cardiac surgery and cardiac iatrogenic, such as cardiac surgery and cardiac catheterization. The incidence of aortic dissection is nine catheterization. The incidence of aortic dissection is nine times higher in patients with a bicuspid valve, compared times higher in patients with a bicuspid valve, compared with a tricuspid aortic valve. Aortic dissection occurs more with a tricuspid aortic valve. Aortic dissection occurs more often in patients with a history of coarctation.often in patients with a history of coarctation.

Question 2Question 22.2. Aortic dissection occurs in which layer of the aortic wallAortic dissection occurs in which layer of the aortic wall??
• A. Adventitia A. Adventitia
• B. External elastic lamina B. External elastic lamina
• C. Intima C. Intima
• D. Media D. Media
• E. Any layer E. Any layer
DD

3.3. Regarding the Stanford classification of aortic dissections, which Regarding the Stanford classification of aortic dissections, which of the following statements is trueof the following statements is true??
• A. The majority of patients have Type B dissections. A. The majority of patients have Type B dissections.
• B. Patients with Type B dissections tend to be older, heavy B. Patients with Type B dissections tend to be older, heavy smokers with chronic lung disease, generalized atherosclerosis, smokers with chronic lung disease, generalized atherosclerosis, and/or hypertension. and/or hypertension.
• C. Type A dissections are less common and are not associated C. Type A dissections are less common and are not associated with high levels of mortality. with high levels of mortality.
• D. Type A dissections involve the distal aorta. D. Type A dissections involve the distal aorta.
• E. The Stanford classification is based on the involvement of the E. The Stanford classification is based on the involvement of the descending aorta. descending aorta.
DD
Question 3Question 3

4.4. Regarding clinical features of aortic dissections, which of the Regarding clinical features of aortic dissections, which of the following statements is not truefollowing statements is not true??
• A. Aortic regurgitation occurs in about 50% of patients with Type A A. Aortic regurgitation occurs in about 50% of patients with Type A dissectiondissection
• B. In about 20% of patients, neurologic deficit is the presenting B. In about 20% of patients, neurologic deficit is the presenting manifestation. manifestation.
• C. Pain is the most common presenting complaint. C. Pain is the most common presenting complaint.
• D. Pulse deficit, a unilaterally weakened or absent pulse, occurs in D. Pulse deficit, a unilaterally weakened or absent pulse, occurs in almost 50% of patients with proximal dissections. almost 50% of patients with proximal dissections.
• E. The most common neurologic abnormality is ischemic E. The most common neurologic abnormality is ischemic paraparesis. paraparesis.
• F. Syncope, while rare, can be the sole presenting symptom.F. Syncope, while rare, can be the sole presenting symptom.
EE
Question 4Question 4

5.5. A 66-year-old white male with a history of hypertension and A 66-year-old white male with a history of hypertension and a known patent foramen ovale has a sudden onset of ripping a known patent foramen ovale has a sudden onset of ripping chest pain that radiates to his back, a blood pressure of chest pain that radiates to his back, a blood pressure of 210/120, and a heart rate of 110. Regarding his initial 210/120, and a heart rate of 110. Regarding his initial treatment, which of the following would not be a wise treatment, which of the following would not be a wise choicechoice??
• A. Labetalol A. Labetalol
• B. Nitroprusside alone B. Nitroprusside alone
• C. Esmolol drip followed by nitroprusside C. Esmolol drip followed by nitroprusside
• D. Intravenous normal saline D. Intravenous normal saline BB
Question 5Question 5

6.6. Which of the following patients with an acute dissection Which of the following patients with an acute dissection requires immediate surgeryrequires immediate surgery??
• A. A 40-year-old pregnant female with a Type A dissection A. A 40-year-old pregnant female with a Type A dissection
• B. A 68-year-old black male with a progressive stroke B. A 68-year-old black male with a progressive stroke
• C. A 77-year-old hypertensive white male with a Type B C. A 77-year-old hypertensive white male with a Type B dissection dissection
• D. A 56-year-old Hispanic male with elevated cardiac D. A 56-year-old Hispanic male with elevated cardiac enzymes and a Type IIIA dissection enzymes and a Type IIIA dissection
• E. None of the above E. None of the above
AA
Question 6Question 6

7.7. Which of the following statements regarding laboratory Which of the following statements regarding laboratory and radiographic evaluation in the work-up of aortic and radiographic evaluation in the work-up of aortic dissection is truedissection is true??
• A. Cardiac enzymes are usually elevated. A. Cardiac enzymes are usually elevated.
• B. Chest x-rays will be abnormal in 80% to 90% of cases. B. Chest x-rays will be abnormal in 80% to 90% of cases.
• C. CT scanning requires arterial catheterization for C. CT scanning requires arterial catheterization for delivery of contrast dye. delivery of contrast dye.
• D. Aortography is no longer the gold standard. D. Aortography is no longer the gold standard.
• E. Transthoracic echocardiography has a sensitivity E. Transthoracic echocardiography has a sensitivity approaching 96%approaching 96% BB
Question 7Question 7