Embed Size (px)
Citation preview

Sodium-Glucose Sodium-Glucose Cotransporters (SGLT) Type 2 Cotransporters (SGLT) Type 2 Inhibitors: New Tools in the Inhibitors: New Tools in the
Fight Against Diabetes?Fight Against Diabetes?
Edward Chao, DOEdward Chao, DO
Endocrine Grand RoundsEndocrine Grand Rounds
April 8, 2009April 8, 2009


Outline
Challenges and a potential solution Renal glucose handling SGLT2 inhibitors: Some history and the latest Safety Potential clinical utility Unresolved questions

Normal Glucose Normal Glucose HomeostasisHomeostasis
Normal fasting glucose homeostasis involves the hormonal regulation of glucose utilization and production and the filtration and reabsorption of glucose by the kidney.
DeFronzo RA. Ann Intern Med. 1999;131:281-303. Wright EM. Am J Physiol Renal Physiol. 2001;280:F10-F18.
Skeletal muscle
LiverFat
Pancreas
Fastingplasmaglucose
90 mg/dL90 mg/dL
Kidney
InsulinInsulin InsulinInsulin Glucagon

Pathophysiology of T2DMPathophysiology of T2DM
DeFronzo RA. Ann Intern Med. 1999;131:281-303. Wright EM. Am J Physiol Renal Physiol. 2001;280:F10-F18.
Gluconeogenesis
Insulin resistance
Impaired Insulin Secretion
Skeletal muscle
+
LiverFat
Pancreas
Fastingplasmaglucose
180 mg/dL180 mg/dL
Kidney
+ - +
Insulin
GlucagonInsulin

Challenges with Current TreatmentChallenges with Current Treatment
Hyperglycemia: Hyperglycemia:
– Leads to microvascular complications Leads to microvascular complications
– Can facilitate beta-cell failure Can facilitate beta-cell failure in the pancreas and in the pancreas and worsen insulin resistance, thus triggering a cycle worsen insulin resistance, thus triggering a cycle of impaired metabolism (glucotoxicity)of impaired metabolism (glucotoxicity)
Traditional focus: developing agents that improve Traditional focus: developing agents that improve insulin sensitivity and/or enhance endogenous insulin sensitivity and/or enhance endogenous insulin secretioninsulin secretion
But hypoglycemia and weight gain are major But hypoglycemia and weight gain are major obstacles to optimizing glycemic controlobstacles to optimizing glycemic control

SGLT2 Inhibitors: A Potential SGLT2 Inhibitors: A Potential Solution?Solution?
Paradoxically, there can be an increased glucose Paradoxically, there can be an increased glucose reabsorptive capacity by the kidney in diabetesreabsorptive capacity by the kidney in diabetes
Inhibition of SGLT2-mediated glucose reabsorption Inhibition of SGLT2-mediated glucose reabsorption in the renal proximal tubule leads to increased in the renal proximal tubule leads to increased glycosuriaglycosuria
Results in: reduced plasma glucose levels, Results in: reduced plasma glucose levels, enhanced insulin sensitivity, suppressed hepatic enhanced insulin sensitivity, suppressed hepatic glucose production, and improved insulin secretionglucose production, and improved insulin secretionMechanism of action is independent of insulin Mechanism of action is independent of insulin resistance or the severity of beta-cell dysfunctionresistance or the severity of beta-cell dysfunction

The Renal Corpuscle and Glomerular The Renal Corpuscle and Glomerular FiltrationFiltration
• Glucose, water, salts, small metabolites, and other small molecules are filtered and collect in Bowman’s space
• Filtration is a process of passive diffusion
• The total amount of a substance (glucose) filtered is proportional to its plasma concentration
Afferent arteriole Efferent arteriole
Bowman’s space Proximal tubule
Fawcett.DW. A Textbook of Histology. 11th ed. WB Saunders Co.; 1986:757-759.

Renal Handling of Glucose in a Non-Renal Handling of Glucose in a Non-Diabetic IndividualDiabetic Individual
Glucose
NO GLUCOSE
S1 segment of proximal tubule
Distal S2 / S3 segment of proximal tubule
ReabsorptionCollecting
duct
Volume of plasma kidneys filter/day = 180 LNormal glucose concentration = 1000 mg/L (100 mg/dl)Glucose filtered/day = (180 L/day) (1000 mg/L) = 180 g
Wright EM. Am J Physiol Renal Physiol. 2001;280:F10-F18. Thorens B. Am J Physiol. 1996;270:G541-G553.
Under normal circumstances, virtually all the glucose filtered is reabsorbed and glucose does not appear in the
urine.
SGLT2
~90%
S
GLT
1~10%

Cellular Glucose TransportCellular Glucose TransportGlucose is a polar compound to which cell Glucose is a polar compound to which cell membranes are impermeablemembranes are impermeable
Movement across lipid-rich cell membranes thus Movement across lipid-rich cell membranes thus requires membrane-associated carrier protein requires membrane-associated carrier protein transporttransport
2 classes of glucose transporters:2 classes of glucose transporters:
- Sodium-linked active glucose transporters:- Sodium-linked active glucose transporters:
6 isoforms (SGLT1-6)6 isoforms (SGLT1-6)
- Facilitative passive glucose transporters:- Facilitative passive glucose transporters:
12 isoforms (GLUT1-12)12 isoforms (GLUT1-12)

Comparison of Sodium-Glucose Comparison of Sodium-Glucose CotransportersCotransporters
SGLT1SGLT1 SGLT2SGLT2
SiteSite Mostly small intestine,Mostly small intestine,some in kidney, heartsome in kidney, heart
Almost exclusively Almost exclusively kidneykidney
Renal LocationRenal Location Late proximal straight Late proximal straight tubule (S3 segment)tubule (S3 segment)
Early proximal Early proximal convoluted tubule convoluted tubule
(S1 segment)(S1 segment)
Affinity for Affinity for GlucoseGlucose
HighHigh Km = 0.4 mMKm = 0.4 mM
LowLowKm = 2 mMKm = 2 mM
Capacity for Capacity for Glucose Glucose
TransportTransportLowLow HighHigh
% of Renal % of Renal Glucose Glucose
ReabsorptionReabsorption10%10% 90%90%
Lee YJ. et al. Kidney Int Suppl. 2007;72:S27-S35.

SGLT2 Mediates GlucoseSGLT2 Mediates GlucoseReabsorption in the KidneyReabsorption in the Kidney
BloodLumen
S1 Proximal Tubule
Na+
Glucose
Glucose
Na+Glucose
Na+ K+
SGLT2
ATPase
GLUT2Na+ and Glucose
at 1:1 stoichiometry
Adapted from Dr. Robert Henry, New Classes of Pharmacologic Agents for the Treatment of Hyperglycemia
on the Horizon: Sodium Glucose Cotransporter (SGLT) - Type 2 Inhibitors, June 2008.

Renal Glucose HandlingRenal Glucose Handling
Schematic representation of the typical titration curve for renal glucose reabsorption in man.Adapted and modified from Silverman M, Turner RJ. Handbook of Physiology. In: Windhager EE, ed. Oxford University Press; 1992:2017-2038.
200
Reabs
orpt
i
on
Tm
300
100
300
Rate
of
Glu
cose
Filtr
ati
on
/Reab
sorp
tion
/Excre
tion
(m
g/m
in)
Plasma Glucose (mg/dL)
Actual Threshold
Tmax
180 200
Theoretical threshold

Renal Glucose Handling After Renal Glucose Handling After SGLT2 InhibitionSGLT2 Inhibition
Schematic representation of the typical titration curve for renal glucose reabsorption in man.Adapted and modified from Silverman M, Turner RJ. Handbook of Physiology. In: Windhager EE, ed. Oxford University Press; 1992:2017-2038.
200
Reabs
orpt
i
on
Tm
300
100
300
Rate
of
Glu
cose
Filtr
ati
on
/Reab
sorp
tion
/Excre
tion
(m
g/m
in)
Plasma Glucose (mg/dL)
Actual Threshold
Tmax
180 200
Theoretical threshold

A Model of SGLT2 Inhibition A Model of SGLT2 Inhibition from Naturefrom Nature
Concern due to increasing excretion of urinary Concern due to increasing excretion of urinary glucose – paradigm shiftglucose – paradigm shift
Could renal glycosuria exacerbate diabetic Could renal glycosuria exacerbate diabetic nephropathy?nephropathy?
Familial renal glycosuriaFamilial renal glycosuria: rare autosomal recessive : rare autosomal recessive d/o; mutations in the SGLT2 gene: persistent d/o; mutations in the SGLT2 gene: persistent isolated glycosuria 10-120 g/day in the face of isolated glycosuria 10-120 g/day in the face of normal fasting serum glucosenormal fasting serum glucose
Calado, et al. Nephrol Dial Transplant. 2008;23:3874-3879.

Familial Renal Glycosuria Pts Familial Renal Glycosuria Pts Typically:Typically:
Have no evidence of renal tubular dysfunctionHave no evidence of renal tubular dysfunction
Are asymptomaticAre asymptomatic
Hypoglycemia and hypovolemia rarely, if ever, Hypoglycemia and hypovolemia rarely, if ever, observedobserved– Some with mutational variations with renal Na wasting Some with mutational variations with renal Na wasting
and/or mild volume depletionand/or mild volume depletion
Renal biopsies: normal histologyRenal biopsies: normal histology
No increased incidence of UTINo increased incidence of UTI
No increased incidence of chronic renal No increased incidence of chronic renal insufficiencyinsufficiency
No increased incidence of diabetesNo increased incidence of diabetes
No obesity observedNo obesity observed

PhlorizinPhlorizin
First SGLT inhibitorFirst SGLT inhibitor
First isolated in 1835 from the root bark of the apple First isolated in 1835 from the root bark of the apple tree by French chemiststree by French chemists
Non-selective Non-selective
Used in research to establish that hyperglycemia Used in research to establish that hyperglycemia contributes to the insulin resistance that contributes to the insulin resistance that
characterizes T2DMcharacterizes T2DM Insulinopenic model of T2DM: diabetic rats with 90% Insulinopenic model of T2DM: diabetic rats with 90% of their pancreases resectedof their pancreases resected

Effect of Phlorizin on insulin Effect of Phlorizin on insulin sensitivitysensitivity
Glu
cose
upta
ke
(mg/k
g m
in)

Phlorizin was never developedPhlorizin was never developedDue to poor intestinal absorption and resultant low Due to poor intestinal absorption and resultant low bioavailabilitybioavailability
Non-selectiveNon-selective
Easily degraded Easily degraded in vivoin vivo to phloretin, which inhibits to phloretin, which inhibits
facilitative glucose transporters, such as GLUT1facilitative glucose transporters, such as GLUT1
An analogue, T-1095, is rapidly converted in the liver An analogue, T-1095, is rapidly converted in the liver to an active metabolite, T-1095A – has a high affinity to an active metabolite, T-1095A – has a high affinity and selectivity for human kidney SGLT2and selectivity for human kidney SGLT2

After PhlorizinAfter Phlorizin
By the early 1950s, phlorizin was demonstrated to block By the early 1950s, phlorizin was demonstrated to block facilitated glucose transport into erythrocytes and inhibit facilitated glucose transport into erythrocytes and inhibit transport of glucose in both the kidney and small transport of glucose in both the kidney and small intestineintestine
Interest in the mechanisms and potential significance of Interest in the mechanisms and potential significance of phlorizin-induced renal glycosuria did not develop until phlorizin-induced renal glycosuria did not develop until the early 1990s, when SGLT2 was fully characterizedthe early 1990s, when SGLT2 was fully characterized

Clinical Development of SGLT2 InhibitorsClinical Development of SGLT2 InhibitorsKipnes, M. Expert Opin Investig. Drugs. 2009 ;18(3) 335-348.Kipnes, M. Expert Opin Investig. Drugs. 2009 ;18(3) 335-348.
DrugDrug Development CompanyDevelopment Company Phase of DevelopmentPhase of Development
DapagliflozinDapagliflozin BMS / AstraZenecaBMS / AstraZeneca IIIIII
RemogliflozinRemogliflozin GSK / KisseiGSK / Kissei IIII
AVE-2268AVE-2268Sanofi-AventisSanofi-Aventis II (discontinued)II (discontinued)
TA-7284TA-7284 JNJ/Mitsubishi TanabeJNJ/Mitsubishi Tanabe IIII
TS-033TS-033 TaishoTaisho II (discontinued)II (discontinued)
YM-543, ASP-1941YM-543, ASP-1941 AstellasAstellas IIaIIa
T-1095T-1095 J & J / Tanabe SeiyakuJ & J / Tanabe Seiyaku II (discontinued)II (discontinued)
SergliflozinSergliflozin GSK / KisseiGSK / Kissei II (discontinued)II (discontinued)
R-7201R-7201 Roche/ChugaiRoche/Chugai IIII
BI 10773, BI 44847BI 10773, BI 44847 Boehringer IngelheimBoehringer Ingelheim II, III, I
DSP-3235DSP-3235 Dainippon Dainippon Sumitomo/KisseiSumitomo/Kissei II
SAR7226SAR7226 Sanofi-AventisSanofi-Aventis II

Dapagliflozin: the structureDapagliflozin: the structureContains a C-glucoside for increased in-vivostability, thus longer t1/2 (~17 hr)Can be administered PO QD in an unmodified form
A selective inhibitor of SGLT2 (~1200-fold more than SGLT1)

Dapagliflozin in Type 2 Dapagliflozin in Type 2 Diabetes: Phase II StudyDiabetes: Phase II Study
47 subjects, 55-60 years of age with T2DM and 47 subjects, 55-60 years of age with T2DM and unimpaired renal function (eGFR 60-136 unimpaired renal function (eGFR 60-136 ml/min/1.73m m2) , drug naïve or on a stable dose ml/min/1.73m m2) , drug naïve or on a stable dose metforminmetformin
Baseline characteristics were similarBaseline characteristics were similar
Randomized to: QD for 14 daysRandomized to: QD for 14 days– placebo (n = 8) placebo (n = 8) – 5 mg (n = 11) 5 mg (n = 11) – 25 mg (n = 12) 25 mg (n = 12)
- 100 mg (n = 16)- 100 mg (n = 16)
Komoroski et al. Clinical Pharm and Therap 2009 Epub Jan 7, 2009; 1-7.

Dapagliflozin Increases Urinary Dapagliflozin Increases Urinary Glucose ExcretionGlucose Excretion
Constant rate of glucosuria over 24 hrs– ~2 g/h (5 mg) ~3 g/h (25 and 100 mg)
Mean
(S
D)
Cu
mu
lati
ve
uri
nary
glu
cose (
g/d
ay)
Dapagliflozin dose (mg)
Komoroski et al. Clinical Pharm and Therap 2009 Epub Jan 7, 2009; 1-7.
2 2 4
1
2
75.3
81.3
45.2
2
70.1 69.9
36.6
0
20
40
60
80
100
120
Placebo 5 25 100
Day -1Day 1
Day 14

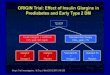
Dapagliflozin decreases mean fasting Dapagliflozin decreases mean fasting serum glucoseserum glucose

Dapagliflozin Improves Postprandial Dapagliflozin Improves Postprandial GlucoseGlucose
Komoroski et al. Clinical Pharm and Therap 2009 Epub Jan 7, 2009; 1-7.Komoroski et al. Clinical Pharm and Therap 2009 Epub Jan 7, 2009; 1-7.
-2.5
-5.2
-9.6
-17.6
-13.7
-22.6
-11.7
-18.8
*
*
*
*
*
*
* P< 0.001
Dapagliflozin dose
Day 2
Day 13

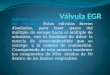
Dapagliflozin: Effect on Renal Glucose Dapagliflozin: Effect on Renal Glucose ReabsorptionReabsorption
Mean
(S
D)
% I
nh
ibit
ion
of
glu
cose r
eab
sorp
tion
Excreted
Filtered% Inhibition of
Glucose reabsorption*= × 100
0.1% 0.9%
20%20%
41%34%36%
44%
0
25
50
75
100
Day 1 Day 14
Placebo (n=8)5 mg (n=11)25 mg (n=12)100 mg (n=16)
Komoroski et al. Clinical Pharm and Therap 2009 Epub Jan 7, 2009; 1-7.
* Measured over 0-4h post-dose interval

Adverse EventsAdverse Events
No deaths or discontinuations due to serious No deaths or discontinuations due to serious adverse eventsadverse events
Adverse events did not appear to be dose-related Adverse events did not appear to be dose-related with either dapagliflozin or metforminwith either dapagliflozin or metformin
Most frequent adverse events were GIMost frequent adverse events were GI
Komoroski et al. Clinical Pharm and Therap 2009 Epub Jan 7, 2009; 1-7.

Komoroski B et al 2009 Clin Pharm Ther 2009 Jan 7 epub

Another Dapagliflozin Trial: Phase IIb
389 drug-naïve T2DM pts (348 completed) in a 389 drug-naïve T2DM pts (348 completed) in a randomized, prospective, double-blind, placebo-randomized, prospective, double-blind, placebo-controlled studycontrolled study18-79 years, A1c 18-79 years, A1c >>7 and 7 and <<10%, BMI 10%, BMI <<40 kg/m2, GFR 40 kg/m2, GFR >60 ml/min/1.73m2, SCr <1.5 mg/dL in men and <1.4 >60 ml/min/1.73m2, SCr <1.5 mg/dL in men and <1.4 mg/dL in women; urine MAU/Cr mg/dL in women; urine MAU/Cr <<300 mg/g300 mg/gAssigned to: Assigned to: DapagliflozinDapagliflozin
2.5 mg QD2.5 mg QD5 mg QD5 mg QD10 mg QD10 mg QD20 mg QD20 mg QD50 mg QD50 mg QD
List, J.F. et al Diabetes Care 2009;32:4:650-657
Metformin XR 750 mg QD titrated at week 2 to 1500 mg QDPlacebo

Outcome MeasuresOutcome Measures
Primary outcome measure: compare mean A1c Primary outcome measure: compare mean A1c change from baseline for each dapagliflozin group change from baseline for each dapagliflozin group vs placebo after 12 weeksvs placebo after 12 weeks
Secondary outcome measures – comparisons of Secondary outcome measures – comparisons of dapagliflozin vs placebo for:dapagliflozin vs placebo for:– FSG change from baselineFSG change from baseline– Dose-dependent trends in glycemic efficacyDose-dependent trends in glycemic efficacy– Proportion of pts achieving A1c < 7%Proportion of pts achieving A1c < 7%– Change in 24-hr urinary glucose to creatinine ratioChange in 24-hr urinary glucose to creatinine ratio
List, J.F. et al Diabetes Care 2009;32:4:650-657

Dapagliflozin dose Placebo Met
2.5 mg 5 mg 10 mg 20 mg 50 mg
Age (years) 55 ± 11 55 ± 12 54 ± 9 55 ± 10 53 ± 10 53 ± 11 54 ± 9
A1C (%) 7.6 ± 0.7 8.0 ± 0.9 8.0 ± 0.8 7.7 ± 0.9 7.8 ± 1.0 7.9 ± 0.9 7.6 ± 0.8
FPG (mg/dl) 145 ± 34 153 ± 48 148 ± 38 149 ± 41 153 ± 42 150 ± 46 143 ± 33
Weight (kg) 90 ± 20 89 ± 17 86 ± 17 88 ± 18 92 ± 19 89 ± 18 88 ± 20
BMI (kg/m2) 32 ± 5 32 ± 5 31 ± 5 31 ± 5 32 ± 4 32 ± 5 32 ± 5
sBP (mmHg) 127 ± 14 126 ± 13 127 ± 16 127 ± 15 126 ± 16 126 ± 16 126 ± 13
dBP (mmHg) 78 ± 8 76 ± 8 77 ± 8 77 ± 8 77 ± 9 77 ± 8 78 ± 8
Creatinine (mg/dl) 0.85 ± 0.15
0.83 ± 0.19
0.85 ± 0.17
0.88 ± 0.19
0.84 ± 0.2 0.85 ± 0.19
0.82 ± 0.17
Table 1— Baseline patient characteristics Data are means ± SD.
List, J.F. et al Diabetes Care 2009;32:4:650-657

List, J.F. et al Diabetes Care 2009;32:4:650-657
2.5 mg 5 mg
10 mg
20 mg
Mean change in A1c at Week 12Mean change in A1c at Week 12
* *
*
^
*
* P <0.001^ P =0.007

% Mean Change from Baseline in % Mean Change from Baseline in Weight after 12 wks of DapagliflozinWeight after 12 wks of Dapagliflozin
List, J.F. et al Diabetes Care 2009;32:4:650-657

Dapagliflozin Dose-Ranging 12 WeekDapagliflozin Dose-Ranging 12 WeekMonotherapy Study of Treatment-Naïve T2DMonotherapy Study of Treatment-Naïve T2D
Dapagliflozin dose (mg)Dapagliflozin dose (mg)
2.52.5
n=59n=59
55
n=58n=58
1010
n=47n=47
2020
n=59n=59
5050
n=56n=56
PBOPBO
n=54n=54
MetMet
n=56n=56
Baseline Baseline FPG FPG 145 145 153153 148 148 149149 153 153 150150 143143
Change Change
FPGFPG (mg/dL)(mg/dL)
-16.2-16.2** -19.3-19.3** -21.1-21.1** -24.4-24.4** -30.5-30.5** -5.8-5.8 -18.0-18.0
Change Change PPG PPG (mg•min/dL) (mg•min/dL)
-9382-9382[-11420, -7344][-11420, -7344]
-8478-8478[-10200, -6756][-10200, -6756]
-10,149-10,149[-12215, -8082][-12215, -8082]
-7053-7053[-8913, -5194][-8913, -5194]
-10,093-10,093[-12024, -8162][-12024, -8162]
-3182-3182[-5086, -1277][-5086, -1277]
-5891-5891[-7775, -4008][-7775, -4008]
* p<0.01 Baseline to Week 12; [95% CIs]List JF et al. Diabetes (Suppl 1), A94, 2008

Summary of List et al ResultsSummary of List et al Results
Decreases in A1c, FPG, and PPG after 12 weeks, with Decreases in A1c, FPG, and PPG after 12 weeks, with reduced FPG apparent by week 1reduced FPG apparent by week 1
Changes in FPG were dose-relatedChanges in FPG were dose-related
There was little evidence of a dose response for either There was little evidence of a dose response for either A1c or PPGA1c or PPG
Greater impact on PPG than FPGGreater impact on PPG than FPG
List, J.F. et al Diabetes Care 2009;32:4:650-657.

List et al List et al
Likely reflects an intrinsic property of dapagliflozin: Likely reflects an intrinsic property of dapagliflozin: greater impact on PPG – a “relief valve” to blunt greater impact on PPG – a “relief valve” to blunt postprandial hyperglycemiapostprandial hyperglycemia
Diuretic effect: Diuretic effect: – small dose-dependent increases in urine volume, small dose-dependent increases in urine volume, – small increases in BUN small increases in BUN – small dose-dependent increase in Hctsmall dose-dependent increase in Hct– No evidence of dehydrationNo evidence of dehydration
Polyuria in 1.4% of pts, and no nocturia was notedPolyuria in 1.4% of pts, and no nocturia was noted
List, J.F. et al Diabetes Care 2009;32:4:650-657.

Weight LossWeight Loss
All doses induced progressive weight reductions All doses induced progressive weight reductions consistent with steady caloric loss via glycosuriaconsistent with steady caloric loss via glycosuria
– Weight loss was more pronounced in week 1, Weight loss was more pronounced in week 1, especially at higher dosesespecially at higher doses
– Acute weight loss during week 1 ? due to fluid loss, Acute weight loss during week 1 ? due to fluid loss, then ?decreased adiposity represented by continued then ?decreased adiposity represented by continued gradual weight lossgradual weight loss
List, J.F. et al Diabetes Care 2009;32:4:650-657.

Adverse EventsAdverse Events2.5 mg
5 mg 10 mg 20 mg 50 mg Placebo Metformin
UTI 3 (5%)
5 (9%)
5 (11%)
4 (7%)
4 (7%)
3 (6%)
4 (7%)
Hypoglycemia 4 (7%)
6 (10%)
3 (6%)
4 (7%)
4 (7%)
2 (4%)
5(9%)
Genital infection
2 (3%)
1 (2%)
1 (2%)
4 (7%)
4 (7%)
0 (0%)
1 (2%)
Nausea 3 (5%)
4 (7%)
3 (6%)
2 (3%)
3 (5%)
3 (6%)
6 (11%)
Diarrhea 1 (2%)
1(2%)
1(2%)
4(7%)
1(2%)
1(2%)
4(7%)
Hypotension 0 0 0 0 1 (2%)
1 (2%)
2 (4%)
List, J.F. et al Diabetes Care 2009;32:4:650-657

Phase III Study of Dapagliflozin as Phase III Study of Dapagliflozin as MonotherapyMonotherapy
Multicenter, randomized, double-blind, placebo-Multicenter, randomized, double-blind, placebo-controlled trialcontrolled trialT2DM subjects ages 18-77 with inadequate glycemic T2DM subjects ages 18-77 with inadequate glycemic control; drug-naïve or treated with medication for < 24 control; drug-naïve or treated with medication for < 24 weeksweeksRandomized to dapagliflozin 2.5, 5,10 mg, or placeboRandomized to dapagliflozin 2.5, 5,10 mg, or placeboPrimary outcome measurePrimary outcome measure: change in A1c at week 24 : change in A1c at week 24 vs baselinevs baselineSecondary outcome measuresSecondary outcome measures include: changes at include: changes at week 24 vs. baseline in:week 24 vs. baseline in:– FPGFPG– total body weighttotal body weight– proportion of pts at A1c < 7.0%proportion of pts at A1c < 7.0%
US National Institutes of Health, http://www.clinicaltrials.gov/ct2/show/NCT00528372?term=dapagliflozin&rank=3. Accessed March 30, 2009.

Phase III Study of Dapagliflozin: Pts with Phase III Study of Dapagliflozin: Pts with T2DM Inadquately Controlled on Metformin T2DM Inadquately Controlled on Metformin
AloneAlone
Multicenter, randomized, double-blind, placebo-Multicenter, randomized, double-blind, placebo-controlled trialcontrolled trial
T2DM subjects on Metformin total daily dose T2DM subjects on Metformin total daily dose >> 1500 mg 1500 mg for at least 8 weeksfor at least 8 weeks
Same primary and secondary outcome measuresSame primary and secondary outcome measures
US National Institutes of Health, http://www.clinicaltrials.gov/ct2/show/NCT00528879?term=dapagliflozin&rank=4. Accessed March 30, 2009.

A Novel Approach
Antisense oligonucleotides can selectively target the kidney epithelial cells in the proximal tubuleReduces SGLT2 expression – transcription, and ultimately, translation – by up to 80% with once-weekly administrationThere were increases in glucosuria, improvements in blood glucose control, and lowering of A1C in rodent models, such as the Zucker Diabetic Fatty ratHighly selective, with no cross-reactivity with SGLT1 or GLUT 2 gene expression – in mouse, dog, monkey, ratNo compensatory increase in gene expression has been seen, even after 6 months of administration

How might SGLT2 inhibitors How might SGLT2 inhibitors potentially be used?potentially be used?
T1DM: added on to insulin T1DM: added on to insulin
T2DM : add-on to other oral agentsT2DM : add-on to other oral agents
add-on to injectablesadd-on to injectables
As an obesity treatmentAs an obesity treatment
In individuals with pre-diabetes for prevention In individuals with pre-diabetes for prevention

Unresolved QuestionsUnresolved Questions
Would urinary excretion of calories as glucose lead to a Would urinary excretion of calories as glucose lead to a compensatory increase in eating?compensatory increase in eating?
Will adverse effects such as UTI and genitourinary Will adverse effects such as UTI and genitourinary infections be found with significantly increased frequency infections be found with significantly increased frequency in long-term trials with large numbers of subjects? If so, in long-term trials with large numbers of subjects? If so, would increased surveillance be needed? would increased surveillance be needed?
What are the long-term effects on renal function?What are the long-term effects on renal function?
Are the weight loss effects sustained?Are the weight loss effects sustained?

Unresolved QuestionsUnresolved Questions
Are there any effects on bone metabolism? On Are there any effects on bone metabolism? On lipids?lipids?
To what extent do the diuretic effect and reduced To what extent do the diuretic effect and reduced adiposity contribute to weight loss?adiposity contribute to weight loss?
How will glycemic control/weight loss be affected How will glycemic control/weight loss be affected when SGLT2 inhibitors are combined with other when SGLT2 inhibitors are combined with other currently used diabetes agents?currently used diabetes agents?

Potential Advantages of SGLT2 Potential Advantages of SGLT2 InhibitorsInhibitors
Novel mechanism of action: no effect on insulin Novel mechanism of action: no effect on insulin secretion or gluconeogenesis – should not cause secretion or gluconeogenesis – should not cause hypoglycemiahypoglycemia– Could continue to be effective as diabetes progressesCould continue to be effective as diabetes progresses
Potential for negative energy balance and thus Potential for negative energy balance and thus weight lossweight loss
Minimizing GI side effects by not inhibiting SGLT1Minimizing GI side effects by not inhibiting SGLT1
Osmotic diuretic effect - ?use with TZDs, ?useful Osmotic diuretic effect - ?use with TZDs, ?useful for pts with htnfor pts with htn

SummarySummarySGLT2 inhibitors reduces both preprandial and SGLT2 inhibitors reduces both preprandial and postprandial blood glucosepostprandial blood glucose
May decrease glucotoxicity and can consequently lead May decrease glucotoxicity and can consequently lead to sustained, long-term glycemic controlto sustained, long-term glycemic control
May have broad indications, including potentially May have broad indications, including potentially prevention of diabetes, obesity, and both T1DM and prevention of diabetes, obesity, and both T1DM and T2DMT2DM
Further studies in large numbers of human subjects will Further studies in large numbers of human subjects will be needed to determine how best to utilize these agents be needed to determine how best to utilize these agents in the treatment of diabetes in the treatment of diabetes


Acknowledgments:Acknowledgments:
Dr. Daniel PorteDr. Daniel Porte
Dr. Robert HenryDr. Robert Henry
Dr. Steve EdelmanDr. Steve Edelman
Dr. Richard DalyDr. Richard Daly