Embed Size (px)
Citation preview
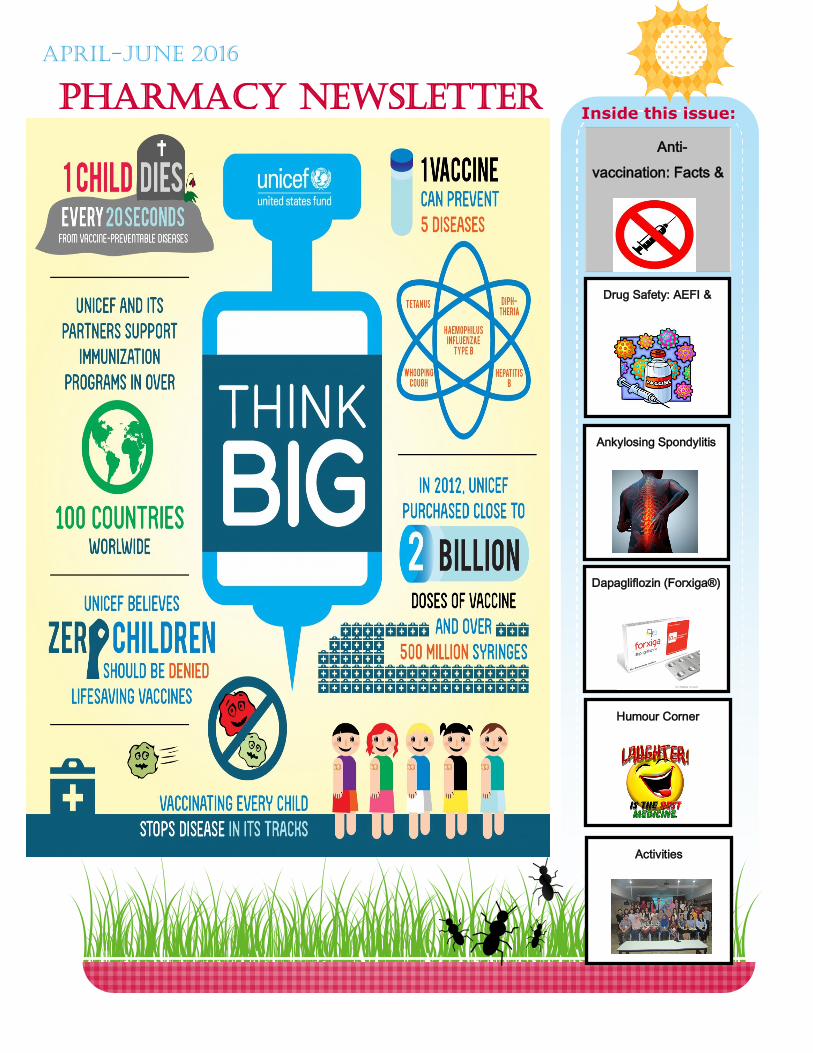
PHARMACY NEWSLETTER
April-June 2016
Anti-
vaccination: Facts &
Drug Safety: AEFI &
Inside this issue:
Ankylosing Spondylitis
Dapagliflozin (Forxiga®)
Humour Corner
Activities
2
Anti-
vaccine
groups :
Facts
and
Myths
Anti-vaccine is a
person who is op-
posed to vaccina-
tion, typically a par-
ent who does not
wish to vaccinate
their child.
The anti vaccine
has existed as long
as vaccination it-
Anti Vaccine : Facts
Critics of vaccination have taken a variety of positions, including op-
position to the smallpox vaccine in England and the United States in
the mid to late 1800s, and the
resulting is an anti-vaccination
leagues. However, the modern
anti-vaccination movement has
its origins in a study published in
The Lancet, a highly influential peer-
reviewed medical journal, in 1998.
The study was widely
criticized as being “filled with
false and fraudulent data,” and was fully redacted in 2010. But once
the study was published in the first place, the damage was already
done. Vaccination rates plummeted, and have stayed lower ever
since, as anti-vaccination activists continue to cite the infamous
study. Decades of progress in vaccine research has been nullified by
anti-vaccination advocacy based largely on a redacted scientific
study.
So if the anti-vaccination movement does not have science behind it,
how exactly does it spread? One factor behind the spread of the
movement is that several celebrities in the west have participated in
anti-vaccine activism. These celebrities include a number of actors,
including Rob Schneider, who campaigned against a bill in California
that would have made it harder to get personal exemptions from vac-
cine requirements. Another infamous anti-vaccine activist is Jenny
McCarthy, who co-hosted the view for one season and spread her anti
-vaccine views through the show.
Another reason that the movement is able to persuade par-
ents is because it uses a lot of fear-mongering and scare tactics to
frighten parents into not vaccinating their children. These tactics
range from blatant fact denial and bad science to naming ingredients
in vaccines that seem harmful to those without a scientific back-
CURRENT ISSUES
3
Understandably, vaccine safety gets more public attention than vaccination effectiveness, but inde-
pendent experts and WHO have shown that vaccines are far safer than therapeutic medicines. Vaccines
have an excellent safety record and most “vaccine scares” have been shown to be false alarms. Mis-
guided safety concerns in some countries have led to a fall in vaccination coverage, causing the re-
emergence of diseases.
Conclusion
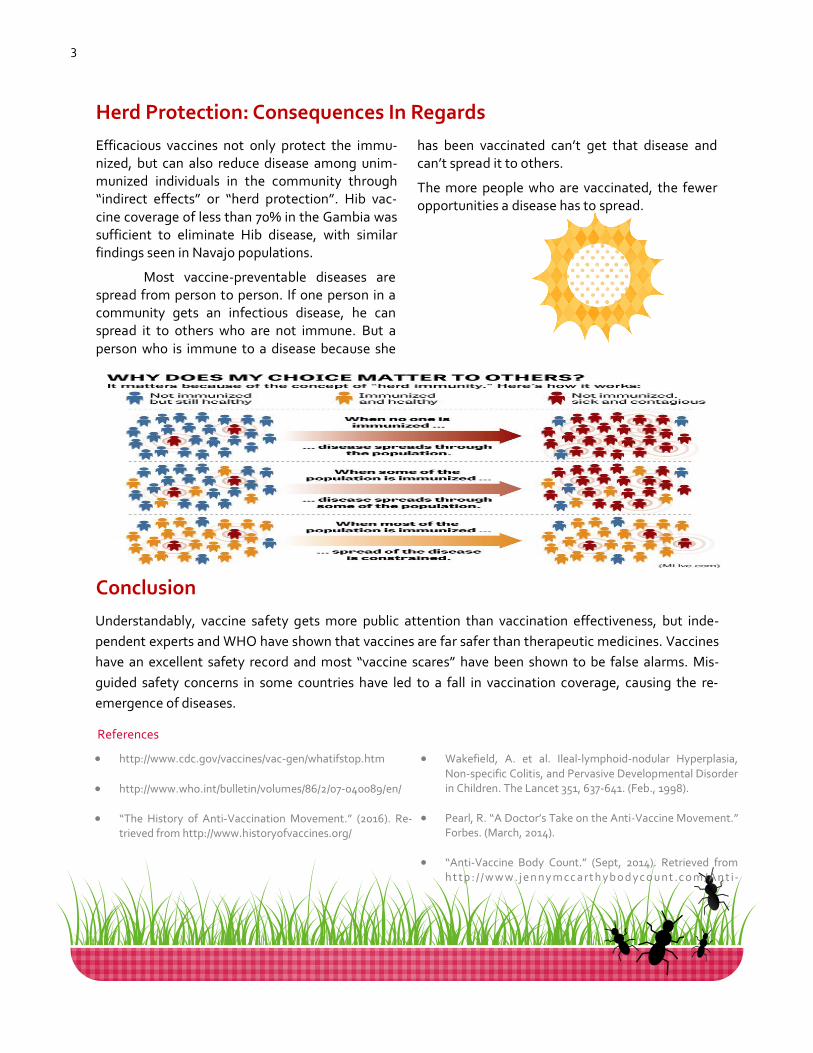
Efficacious vaccines not only protect the immu-nized, but can also reduce disease among unim-munized individuals in the community through “indirect effects” or “herd protection”. Hib vac-cine coverage of less than 70% in the Gambia was sufficient to eliminate Hib disease, with similar findings seen in Navajo populations.
Most vaccine-preventable diseases are spread from person to person. If one person in a community gets an infectious disease, he can spread it to others who are not immune. But a person who is immune to a disease because she
has been vaccinated can’t get that disease and can’t spread it to others.
The more people who are vaccinated, the fewer opportunities a disease has to spread.
Herd Protection: Consequences In Regards
http://www.cdc.gov/vaccines/vac-gen/whatifstop.htm
http://www.who.int/bulletin/volumes/86/2/07-040089/en/
“The History of Anti-Vaccination Movement.” (2016). Re-trieved from http://www.historyofvaccines.org/
Wakefield, A. et al. Ileal-lymphoid-nodular Hyperplasia, Non-specific Colitis, and Pervasive Developmental Disorder in Children. The Lancet 351, 637-641. (Feb., 1998).
Pearl, R. “A Doctor’s Take on the Anti-Vaccine Movement.” Forbes. (March, 2014).
“Anti-Vaccine Body Count.” (Sept, 2014). Retrieved from h t tp : / / w w w .j e n ny m cc a rt h yb o d yc o u nt .c o m / An t i-
References
4
“To catch the reader's attention, place an interesting sentence or quote from the story here.”
Play a part in reporting AEFI MADRAC via the National Pharmaceutical Control Bureau website (http://www.npra.gov.my)
1. Vaccine reactions
Individual’s response to inherent
properties of the vaccine.
Minor reactions includes local
pain, swelling or redness, fever,
malaise, headache which usually
occurs within a few hours of in-
fection and resolves spontane-
ously.
Severe reactions includes sei-
zures and allergic reactions
which can be life-threatening,
although, rare.
2. Immunization error-related reac-
tion
Preventable
Non-sterile injection: the reuse
of disposable syringe or needle,
or improperly sterilized syringe
Reconstitution error: inadequate
shaking of vaccine.
Injection at incorrect site: BCG
given subcutaneously, DTP/DT/
TT too superficial, injection into
buttocks.
Vaccine transported/stored in-
correctly: freezing vaccine dur-
ing transport, failure to keep
vaccine in cold chain.
Contraindication to vaccines
ignored due to unfamiliarity
3. Immunization anxiety-related
reactions
Patients react in anticipation to
and as a result of an injection.
Not related to the vaccine but to
fear of the injection.
Examples are fainting, hyperven-
tilation, vomiting or convulsions.
4. Coincidental events
Occurs after a vaccination has
been given but are not caused by
the vaccine or administration
errors.
Could be due to illness, congeni-
tal or early neurological condi-
tions.
Classifications of AEFI
How safe are vaccines?
Vaccines are the best defense we
have against serious, preventable
and sometimes, deadly contagious
diseases. However, like any other
medical products, there may be
risks.
The World Health Organization (WHO)
defines an AEFI as “a medical incident
that takes place after an immunization,
causes concern and believed to be
caused by immunization..”
Adverse events of vaccinations is not a
new news. It has been increasingly
popular in inciting anxiety and negativity
towards vaccination despite its crucial
benefits to the general population in
fighting certain infectious diseases.
Adverse events does not necessarily
have a causal relationship with the usage
of vaccine and can be temporarily asso-
ciated with immunization. As with other
medications, side effects are inevitable
but most of them such as fever and
injection site reactions are mild and clear
up quickly. More serious reactions like
anaphylaxis are rare and generally does
not result in long-term problems.
Play a part in reporting AEFI
MADRAC via the National Phar-
maceutical Control Bureau website
(http://www.npra.gov.my)
Adverse Events following Immunization (AEFI)
DRUG SAFETY/MADRAC NEWS
5
Stevens-Johnson
Syndrome ???
However there were 7 reports (12%) of Pal-
mar-plantar erythro-
dysaesthesia (PPE) or m o r e c o m m o n l y
known as hand-foot
syndrome, which is a
condition known and
documented in the
current approved pre-
scribing information of
Capecitabine (Xeloda®) is
a chemotherapy drug which
has been registered and
used in Malaysia since 2000.
Indication: Advanced or
metastatic breast cancer,
stage III colon cancer,
metastatic colorectal
c a r c i n o m a a n d
oesophagogastric cancer.
Capecitabine (Xeloda®) DRUG REVIEW
According to the Na-
tional Pharmaceutical Control Bureau (NPCB),
severe skin reactions
such as Stevens-
Johnson Syndrome
(SJS) and Toxic Epider-
mal Necrolysis (TEN),
in which some, with fa-
tal outcome has been
reported with the use
of Xeloda®. These
cases however, have
been classified as rare.
In June 2013, the Drug Safety Monitoring Centre, NPCB
has received 26 adverse drug reactions (ADR) reports
from the use of Xeloda® with 56 adverse events:
Fortunately, none of the reports in Malaysia involves
SJS nor TEN or with a fatal outcome.
16 events
of:
Nausea
Vomiting
Diarrhea
13 events
of:
Itching
Erythema
Maculo-
papular rash
12 events
of:
Back pain
Fever
Fatigue
PPE
Globally, WHO database contained 16 reports for SJS
and 13 reports of epidermal necrolysis associated
with Xeloda® from countries such as America , Africa and
Europe.
6
PATHOPHYSIOLOGY:
Primary pathology of the spondyl oarthropathies is
enthesitis with chronic inflammation, including
CD4+ and CD8+ T lymphocytes and macrophages.
Cytokines, particularly tumor necrosis factor-α
(TNF-α) and transforming growth factor-β (TGF-β),
are also important in the inflammatory process by
leading to fibrosis and ossification at sites of en-
thesitis -common genetic factors including the hu-
man leukocyte antigen (HLA) B27 gene.
ANKYLOSING SPONDYLITIS
DISEASES AND TREATMENT
DIAGNOSIS:
-Physical examination—eg: back pain and stiffness made
worse with immobility, pain for more than 3 months,
-Blood test to test for:
C-reactive protein (CRP), erythrocyte sedimentation
rate (ESR), plasma viscosity (PV). And/or HLA-B27 gene
-X-rays—for later stages .
-MRI) scans—for earlier stage of AS
-History of GI infection, uveitis, and family history of AS
TREATMENT: for active AS
A)NSAIDS (first line):
Naproxen— ORALLY; 250mg or 500mg BD. Max 1500mg/
day for 6 months .
Diclofenac—ORALLY; 150mg daily. Mild or long term: 75-
150mg daily in 2-3 divided doses.
Celecoxib—ORALLY; 200mg OD or 400mg OD max in di-
vided doses. If no improvement after 6 weeks, then 400mg/
day. Is a COX-2 inhibitor, given if patient has G1 distur-
bances when taking NSAIDs.
B) TNF-i Drugs (second line):
Golimumab— 50mg S/Q once a month
Infliximab— 5mg/kg IV over at least 2 hours given at week 0,
2 and 6, followed by maintenance therapy which 5mg/kg IV
over at least 2 hours every 6 weeks.
Etarnecept—50mg S/Q once a week .(not recommended in
pt with AS and inflammatory bowel disease)
C) Disease-modifying anti-rheumatic drugs (DMARDs)
(Conditionally recommended if TNF-s is contraindicated)
Sulfasalazine- ORALLY; initially 0.5 to 1g per day or in di-
vided doses not >8H. Maintenance, 2g/ day in divided dose
not >8H intervals.
Methotrexate– initially 7.5mg S/Q once weekly. Dose can
exceed 20mg/wk but with increase risk of toxicity. When
switching from oral to S/Q
must consider bioavailability
difference.
D) Physiotherapy and exercise.
PARAMETERS MONITORING:
Baseline serum levels of the following biomarkers were
examined: C-reactive protein (CRP), matrix metallopro-
teinase 3 (MMP3), sclerostin, Dickkopf 1 (DKK1), perio-
stin, bone morphogenetic protein (BMP) 2 and 7, osteo-
protegerin, vascular endothelial growth factor (VEGF),
procollagen type I and II N-propeptide (PINP and PIINP),
CTX-II, BALP, sRANKL, COPM, and bone sialoprotein.
7
Pharmacokinetic
Absorption
Cmax: within 2 hours
Bioavailability, oral: 78 %
Peak plasma time: 2 hrs (fasting), ~3 hrs (with high fat meal)
High fat meal decreases peak plasma concentration by up to 50 %
Distribution
Protein binding: 91 %
Metabolism
Extensive via UGT1A9 (an enzyme present in the liver and kidney)
3-O-glucuronide; to form an inactive metabolite
Excretion
Renal: 75 % (less than 2 % unchanged)
Fecal: 21%( 15 % unchanged)
Pharmacodynamic
Dapagliflozin is a highly potent, se-lective and reversible inhibitor of sodium-glucose co-transporter 2 (SGLT2).
The SGLT2 is selectively expressed in the kidney with no expression detected in > 70 other tissues in-cluding liver, skeletal muscle, adi-pose tissue, breast, bladder and brain.
SGLT2 is the predominant trans-porter responsible for reabsorption of glucose from the glomerulare filtrate back into the circulation.
Indication
Adjunct to diet and exercise to
improve glycaemic control in
adults ≥ 18 years old with type 2
DM as monotherapy, add-on
combination with metformin,
sulfonylurea, insulin, DPP4 in-
hibitor, in combination with
metformin and a sulfonylurea
and as initial combination ther-
apy with metformin (includes
poor respects for response to
metformin therapy)
Dose
Monotherapy and add-on com-bination therapy: 10 mg once daily
Initial combination therapy: 10 mg dapagliflozin + 500 mg met-formin once daily
Dosage modification
Renal impairment:
eGFR ≥60 ml/min/1.73 m2. No dosage adjustment needed
eGFR <60 ml/min/1.73 m2. Do not initiate
Not recommended with eGFR that declines persistently be-tween 30 to <60 ml/min/1.73 m2.
eGFR <30 ml/min/1.73 m2. Con-traindicated
Hepatic impairment:
Mild or moderate: No dosage adjustment needed
Severe: Not studied
Mechanism of Action
Inhibits sodium-glucose cotrans-
porter 2 (SGLT2), thereby reduc-
ing reabsorption of filtered glu-
cose, lowering the renal thresh-
old for glucose, and increasing
Dapagliflozin NEW DRUG PROFILE

8 HUMOUR CORNER
Two chemists go
into a restaurant.
The first one says "I
think I'll have an
H2O."
The second one
says "I think I'll have
an H2O too" -- and
he died.

9
BASIC STATISTICS COURSE
FOR MEDICAL
RESEARCH 2016
4TH JUNE 2016
PHARMILY TRIP TO
KUCHING, SARAWAK ON
15-17TH APRIL 2016
ACTIVITIES
Participants having hands-on experience
with SPSS Program
Group snap before dispersing.
Visiting the beautiful Fairy Cave as part
of the activities planned
Group photo when visiting the “Kampung
Kebudayaan Sarawak”

10
“To catch the reader's attention, place an interesting sentence or quote from the story here.”
If passion drives you, let reason hold the reins.”– Benjamin Franklin
KURSUS MOTIVASI ANJURAN JABATAN FARMASI HOSPITAL MELAKA
Participants enjoying the activity
Speaker sharing his experience and motivating the participants.
11
Jabatan Farmasi & Bekalan, Hospital Melaka, Jalan Mufti Hj Khalil, 57400 Melaka Phone: 06-2892583 Fax: 06-2837500 E-mail: [email protected]
Pharmacy Resources & Information Centre
ADVISOR:
Pn Saidatul Raihan Ibrahim
EDITORIAL BOARD:
Pn Syamsiah Hj Shariff
Cik Tay Eek Poei
Cik Umi Solehah binti Sa’ad
EDITOR:
Roshwini Muthiah
CONTRIBUTORS
Tan Jhii Lien
Nor Sa’adah binti Harun
References:
1.Malaysian clinical pharmacists knowledge regarding Adverse Events Following Immunization (AEFI). International Summit on Clinical Pharmacy & Dispensing. USA; Nov 2013.
2.Adverse events following immunization. World Health Organization; 2016.
3.Bulletin-MADRAC-December 2013. Xeloda® (Capecitabine): Association with Severe Skin Reac-tions such as Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN).
4.Drug Safety Update. Medicines and Healthcare products Regulatory Agency, UK. Volume 7 Issue 6, January 2014.
5.Michael M. Ward, Atul Deodhar, Elie A. Akl, et al. American College of Rheumatology/Spondylitis
Association of America/Spondyloarthritis Research and Treatment Network 2015 Recommenda-
tions for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthri-
tis. AMERICAN COLLEGE OF RHEUMATOLOGY 2015; DOI 10.1002/ART.39298(): . http://
www.rheumatology.org/Portals/0/Files/Recommendations%20for%20the%20Treatment%20of%
20Ankylosing%20Spondylitis.pdf (accessed 7th Octorber 2016).
6.Serum Biomarkers Predict Ankylosing Spondylitis Progression [Internet]. Medscape. 2016 [cited
13 June 2016]. Available from: http://www.medscape.com/viewarticle/765228
7.. Ankylosing spondylitis - Treatment - NHS Choices [Internet]. Nhs.uk. 2016 [cited 14 June 2016]. Available from: http://
8.MIMS Malaysia. 2016. [Internet] Available from : http://www.mims.com/malaysia/drug/info/forxiga
9.Medscape. 2016. [Internet] Available from : http://reference.medscape.com/drug/farxiga-dapagliflozin-999899
10.)Pharmacists Jokes at WorkJoke.com - Profession Jokes [Internet]. Workjoke.com. 2016 [cited 20 June 2016]. from: http://www.workjoke.com/pharmacists-jokes.html
12





























