Embed Size (px)
Citation preview
1
39th National Conference on Pediatric Health Care
©2018
March 19-22, 2018 CHICAGO
APRN Preceptor Workshop
APRN Precepting:Providing the Tools for Successful
Clinical Education Experiences
A joint presentation of the NAPNAP Professional Issues Committee and the Association of Faculties of Pediatric
Nurse Practitioners (AFPNP)
©2018
Disclosures
• No general disclosures• No financial disclosures• No discussion of off-label and/or investigational uses of
drugs and/or devices
2
©2018
Acknowledgements
Thanks to AFPNP for supporting this session
Thanks to presenters for sharing family picturesAll clip art courtesy of Google Images
3
©2018
Presenters• Beth Heuer, DNP, CRNP, CPNP-PC, PMHS
– Children’s Hospital of Pittsburgh of UPMC; Robert Morris University• Cynthia Danford, PhD, CRNP, PPCNP-BC, CPNP-PC
– University of Pittsburgh• Jay M. Hunter, DNP, RN, CPNP-AC, CCRN, CPEN, CPN
– Cook Children’s Health Care System, University of South Alabama• Daniel Crawford, DNP, RN, CPNP-PC
– Arizona State University• Jessica Diver-Spruit, DNP, RN, CPNP-AC
– Wayne State University• Maria Lofgren, DNP, ARNP, NNP-BC, CPNP, FAANP
– University of Iowa• Audra Rankin, DNP, APRN, CPNP
– Johns Hopkins University• Imelda Reyes, DNP, MPH, CPNP, FNP-BC
– Emory University
4
©2018
With Special Thanks to our Additional Toolkit Collaborators
• Jodi Bloxham, MSN, APRN, AC-PNP, PC-PNP– University of Iowa
• Shayna Dahan, MSN, CPNP, PMHS– NYU Rory Meyers College of Nursing
• Amanda Lee, MSN, PPCNP-BC– Access Community Health Network
5
©2018
Objectives
• Identify coaching skills necessary for effective precepting of nurse practitioner (NP) students in pediatrics
• Develop communication and educational skills to facilitate education of NP students in the pediatric clinical setting
• Utilize a preceptor toolkit to enhance preceptor satisfaction as well as NP student clinical experiences in pediatrics
6
2
©2018
Definitions
NP student = the individual who is receiving direction and guidance from the preceptor (aka the APRN)
Advanced Practice Registered Nurse (APRN) = the experienced clinician (aka the preceptor) who is providinginstruction to the NP student
7
©2018
Take 5 Ground Rules
• Turn to your neighbor (or small group of 2-3 people)
• Take 2 minutes to respond to the question(s) on the slide
• Write your response on the 3x5 card and turn in– To be collated and distributed later, as part of an updated toolkit,
for your future clinical precepting use
• The next 2-3 minutes will be discussion r/t the Take 5 content
8
©2018
Foundational Outcomes
Intellectual CuriosityMental FlexibilityClinical Expertise
Evidence-Based UnderpinningsUnparalleled Professionalism
9
©2018
Background• NPs by the numbers (AANP, 2017)
– There are more than 234,000 nurse practitioners in the United States – By 2024, the Bureau of Labor Statistics projects that the NP profession
will have grown by 35%
• NP education (AANP, 2017)
– Approx. 20,000 students graduated from NP programs from 2014-15 – There are NP programs at approximately 350 universities and colleges in
the U.S. • Many programs offer distance learning, requiring the students to find
their own preceptors and clinical sites
10
©2018
The Growing Demand for Preceptors
• High demand to meet the need for high quality NP student educational experiences
• What does this mean? What skills are needed?– Excellent clinical skills– Effective communication– Flexibility– Provision of feedback and support– Ability to meet the different learning styles of adult students– Ability to evaluate student knowledge & competencies
(Burns, Beauchesne, Ryan-Krause & Sawin, 2006)
11
©2018
Logistics
• Where do students come from?• What are clinical hour requirements?• Why are faculty so desperate?• What is my role?
12
3
©2018
Where do these students come from?
• Student preceptor assignments are established in a variety of ways
– Faculty contacts preceptor directly– Designated administrator/course coordinator contacts preceptor on
behalf of faculty and course– Student contacts preceptor directly– Preceptor’s health system may be the gatekeeper– Paid agencies may contact preceptor on behalf of student– Online applications for distance learning students
13
©2018
Student Online Application for Clinical SiteUniversity of Iowa Example
14
©2018
Student Online Application for Clinical SiteCook Children’s Medical Center Institutional Example
15
©2018
What are the clinical hour requirements?
• The typical requirement for certifying bodies is a minimum of 500 hours of supervised clinical practice in the pediatrics specialty with an experienced APRN or physician in the same specialty
• Individual APRN program requirements vary– Dependent on program and student level (BSN-DNP vs.
MSN-DNP)
16
©2018
Faculty Challenge:“Changing Climate”
• Competition for clinical experiences in various teaching arenas needs to be recognized and addressed to meet all healthcare student demands for future healthcare provider workforce– NP students– Medical students– Residents– Physician Assistants
• Need sustainable processes to recruit, retain and recognize preceptors for NP students
• Overall goal: Partnerships between APRNs and faculty to achieve mutually beneficial outcomes in healthcare 17
©2018
Affiliation Agreements
• Between educational institution and the clinical site– Number of hours needed by student– Days available– Liability coverage– Basic information about where the student is within the program
• Affiliation agreements or contractual agreements undergo university legal review before being sent to clinical sites for signatures
18
4
©2018
Defining the Preceptor• Preceptors are experienced clinical practitioners who
teach and role-model clinical and leadership skills to novice practitioners (students, new graduates, practitioners new to their setting, or new employees)
• We need you!!! We value you!!!– Preceptors are critical to the successful development
of the APRN– Important role in guiding clinical practice education– Shared role with university faculty
19
©2018
What are the qualities of good preceptors?
• Clinical competency in pediatrics• Serves as a role model• Provides constructive feedback• Interprofessional collaboration
mindset• Warmth • Respectful
• Enthusiasm • Empathy • Nonjudgmental• Fairness• Dependability• Consistency• Humor • Flexibility
20
©2018
Roles of the Preceptor
• Teacher• Coach• Leader• Influencer• Mentor
21
• Facilitator• Socializing agent• Protector• Role model
(Ulrich, 2011)
©2018
• High-quality APRN preceptors with expertise in pediatrics– Help students acquire real-time clinical skills – Help validate their competency in these skills– Help students to make the transition from being a “generalist
registered nurse” to pediatric advanced practice nursing specialist
• However…– APRNs are not taught how to be preceptors– Precepting is a new skill set that is learned and developed over time
(Horton, DePaoli, Hertach, Bowe, 2012; Link, 2009)
The Preceptor Learning Curve
22
©2018
Why Precept???
• Professional benefits• Personal benefits
23
©2018
Professional Benefits
• Sharing and demonstrating clinical knowledge and expertise
• Maintaining updated knowledge of evidence-based care– More motivation to explore the literature– Learning the ‘latest and greatest’ from students
• Narrowing the theory-practice gap• Ongoing maintenance of expert clinical skills through
teaching students24
5
©2018
Professional Benefits
• Obtaining precepting hours for pediatric recertification credit (through PNCB and ANCC)
• Building a curriculum vitae (CV)
• Completing institutional requirements for career ladder advancement
• Meeting criteria for tax incentives for preceptors (in some states)
25
©2018
Professional Benefits
26
• Networking opportunities with peds-focused colleagues• Adjunct pediatric faculty appointments• Access to university resources (such as library, pediatric
drug guide, pediatric journal access)• Opportunities to guest lecture on pediatric topics• Peer support through dialogue with faculty• Contributions toward ongoing pediatric program
development
©2018
What About Paid Preceptor Opportunities?
Several companies are open and “ready for student business”
• www.preceptorlink.com• www.nursepractitionerclinicalrotations.com• www.npclinicalmatch.com• www.clinicaltrainingnetwork.com
27
©2018
Take 5Paid Preceptorships
• What are your thoughts regarding paid preceptorships?
• Any ethical considerations?– Would you do it?
• Would some kind of payment be your only justification for precepting?
28
©2018
Personal Benefits
• Fulfillment of one’s “social contract”/giving back to the profession– Perceptive that we ‘owe it’ to the profession, to the student, to our
patients, and to ourselves
• Personal satisfaction– Despite challenges, precepting is inherently satisfying (Latessa et al., 2013)
• Solidifying one’s identity as a pediatric-focused APRN• Reflecting on one’s own practice through the eyes of the student• Adding interest, challenge, renewal, and enrichment to one’s daily
work29
©2018
Wow! Those benefits look AMAZING! Sign me up!!!
30
6
©2018
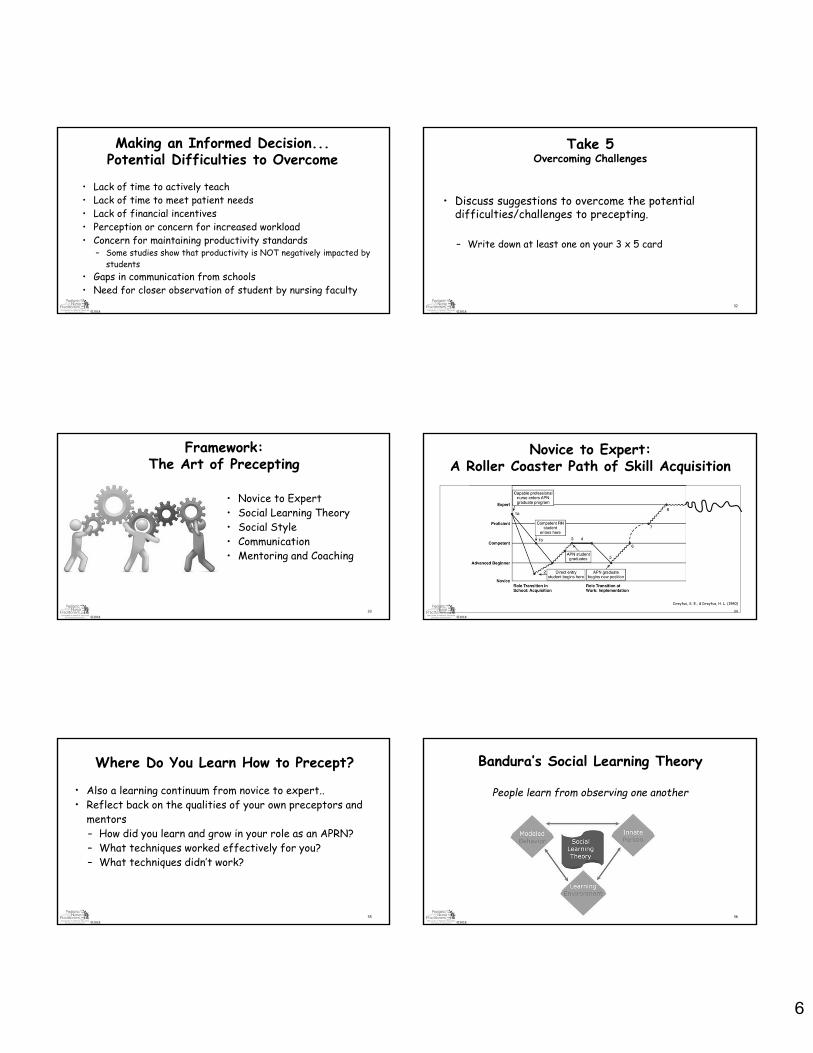
Making an Informed Decision... Potential Difficulties to Overcome
• Lack of time to actively teach• Lack of time to meet patient needs• Lack of financial incentives• Perception or concern for increased workload• Concern for maintaining productivity standards
– Some studies show that productivity is NOT negatively impacted by students
• Gaps in communication from schools• Need for closer observation of student by nursing faculty
©2018
Take 5Overcoming Challenges
• Discuss suggestions to overcome the potential difficulties/challenges to precepting.
– Write down at least one on your 3 x 5 card
32
©2018
Framework:The Art of Precepting
• Novice to Expert• Social Learning Theory• Social Style• Communication• Mentoring and Coaching
33
©2018
Novice to Expert:A Roller Coaster Path of Skill Acquisition
Dreyfus, S. E., & Dreyfus, H. L. (1980)
34
©2018
Where Do You Learn How to Precept?
• Also a learning continuum from novice to expert.. • Reflect back on the qualities of your own preceptors and
mentors – How did you learn and grow in your role as an APRN?– What techniques worked effectively for you?– What techniques didn’t work?
35
©2018
Bandura’s Social Learning Theory
People learn from observing one another
36
7
©2018
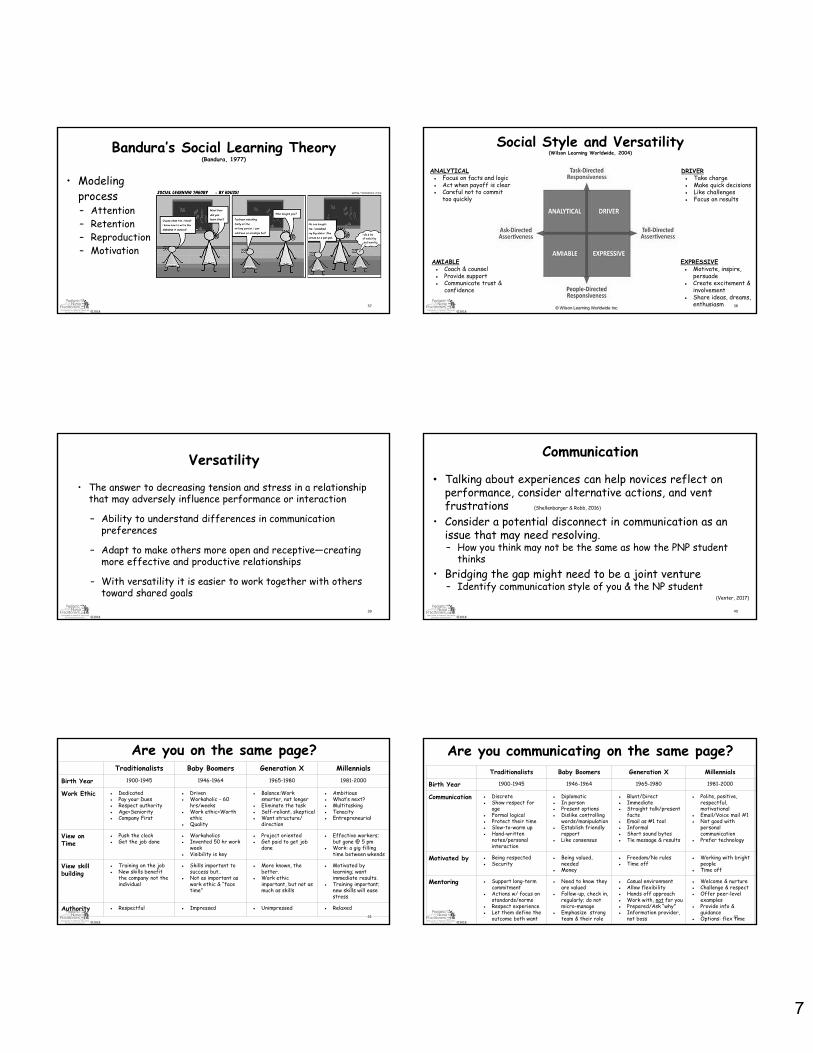
Bandura’s Social Learning Theory(Bandura, 1977)
• Modeling process– Attention– Retention– Reproduction– Motivation
37
©2018
Social Style and Versatility(Wilson Learning Worldwide, 2004)
38
ANALYTICAL● Focus on facts and logic● Act when payoff is clear● Careful not to commit
too quickly
DRIVER● Take charge● Make quick decisions● Like challenges● Focus on results
AMIABLE● Coach & counsel● Provide support● Communicate trust &
confidence
EXPRESSIVE● Motivate, inspire,
persuade● Create excitement &
involvement● Share ideas, dreams,
enthusiasm
©2018
Versatility
• The answer to decreasing tension and stress in a relationship that may adversely influence performance or interaction
– Ability to understand differences in communication preferences
– Adapt to make others more open and receptive—creating more effective and productive relationships
– With versatility it is easier to work together with others toward shared goals
39
©2018
Communication
• Talking about experiences can help novices reflect on performance, consider alternative actions, and vent frustrations (Shellenbarger & Robb, 2016)
• Consider a potential disconnect in communication as an issue that may need resolving.– How you think may not be the same as how the PNP student
thinks• Bridging the gap might need to be a joint venture
– Identify communication style of you & the NP student(Venter, 2017)
40
©2018
Are you on the same page?
41
Traditionalists Baby Boomers Generation X Millennials
Birth Year 1900-1945 1946-1964 1965-1980 1981-2000
Work Ethic ● Dedicated ● Pay your Dues● Respect authority● Age=Seniority● Company First
● Driven● Workaholic - 60
hrs/weeks● Work ethic=Worth
ethic● Quality
● Balance:Work smarter, not longer
● Eliminate the task● Self-reliant, skeptical● Want structure/
direction
● Ambitious● What’s next?● Multitasking● Tenacity● Entrepreneurial
View on Time
● Push the clock● Get the job done
● Workaholics● Invented 50 hr work
week● Visibility is key
● Project oriented● Get paid to get job
done
● Effective workers; but gone @ 5 pm
● Work: a gig filling time between wkends
View skill building
● Training on the job● New skills benefit
the company not the individual
● Skills important to success but..
● Not as important as work ethic & “face time”
● More known, the better.
● Work ethic important, but not as much as skills
● Motivated by learning; want immediate results.
● Training important; new skills will ease stress
Authority ● Respectful ● Impressed ● Unimpressed ● Relaxed
©2018
Are you communicating on the same page?
42
Traditionalists Baby Boomers Generation X Millennials
Birth Year 1900-1945 1946-1964 1965-1980 1981-2000
Communication ● Discrete● Show respect for
age● Formal logical ● Protect their time● Slow-to-warm up● Hand-written
notes/personal interaction
● Diplomatic● In person● Present options● Dislike controlling
words/manipulation● Establish friendly
rapport● Like consensus
● Blunt/Direct● Immediate● Straight talk/present
facts● Email as #1 tool● Informal ● Short sound bytes● Tie message & results
● Polite, positive, respectful, motivational
● Email/Voice mail #1 ● Not good with
personal communication
● Prefer technology
Motivated by ● Being respected● Security
● Being valued, needed
● Money
● Freedom/No rules● Time off
● Working with bright people
● Time off
Mentoring ● Support long-term commitment
● Actions w/ focus on standards/norms
● Respect experience● Let them define the
outcome both want
● Need to know they are valued
● Follow-up, check in, regularly; do not micro-manage
● Emphasize strong team & their role
● Casual environment ● Allow flexibility● Hands off approach● Work with, not for you● Prepared/Ask “why”● Information provider,
not boss
● Welcome & nurture ● Challenge & respect ● Offer peer-level
examples● Provide info &
guidance● Options: flex time
8
©2018
Take 5Communication Type
• What type of communicator are you?
• What do you expect from the NP students you precept? Is this realistic?
43
©2018
Precepting versus Mentoring (Lazarus, 2016)
• Preceptor relationship is defined by time periods and delineated objectives for clinical learning
• Mentoring relationship is long-term, voluntary, and typically does not have an established end time
• Both share some common qualities
44
©2018
Mentoring
• Common attributes of successful mentors include:– Admirable characteristics such as selflessness and
kindness– Provider of support for NP student’s career– Strong time commitment– Supporter of personal and professional life balance– Encourages NP student to carry on a legacy and become a
mentor when the time is right(Cho et al., 2011; MacLeod, 2007)
45
©2018
Qualities of a Good Mentoring Relationship
•Motivate•Empower and Encourage•Nurture self-confidence•Teach by example•Offer wise counsel•Raise the performance bar
(Souba, 1999)
46
©2018
Benefits of Being Mentored
• Increased self-confidence• Enhanced judgment• Improved leadership ability• Personal and professional
growth• Career commitment
47
©2018
What about coaching?
• The coaching role takes teaching further– “It’s not just about learning the skill; it’s about how and when to use
the skill and how to use it most effectively…” (Ulrich, 2011)
• Facilitates “safe passage” for NP students as they transition from one role to another
• Develops the NP student’s knowledge and skill in an area within the preceptor’s expertise– Leads NP students to believe in themselves
48
9
©2018
Professional Development: Building the Culture
• Student/ NP Socialization– Networking– Organizational Involvement– Continuing Education– Advocacy for APRNs– Contributions to the Profession
©2018
Benefits of Networking
• Build relationships with APRN colleagues and faculty– Develop supports within
pediatric peer group or place of employment
– Utilize social media to maintain network
50
• Enhance knowledge sharing– Seek clinical experiences in
desired specialty
• Identify professional development and collaborative activities within pediatric specialty– Co-authoring, presenting,
research opportunities
©2018
Professional Organizational Involvement
• Access to practice resources, career center, continuing education opportunities, policy and position statements
• Special interest groups (i.e. NAPNAP SIGs), committee membership (i.e. NAPNAP Professional Issues Committee) and advocacy opportunities (NAPNAP Capitol Hill Day)
• Preceptor involvement in the AFPNP• Statewide and National Professional Groups
51
©2018
Continuing Education (CE)
• Discuss what CE means to you as a practicing APRN
• Discuss ways that to obtain CEUs and share your resources– Grand Rounds -Journals providing CE
articles– Journal Clubs -Local/national
conferences and symposia– NAPNAP pedsCE -Local APRN CE events
• Invite students to attend events 52
©2018
Encouraging Advocacy• Why?
– “The essence of professionalism” (Ryan & Rosenberg, 2015)
– Involvement is essential for patient advocacy– Effective way to create change
• How?– NAPNAP advocacy and calls-to-action
• Child Health Policy Learning Collaborative– Discuss scope-of-practice regulations and how they affect
daily practice
53
©2018
Encouraging Professional Contribution• Discuss your experiences and involvement
– Volunteerism • TeamPeds• Community Engagement (Free clinics, shelters, etc.)
– Nurses on Boards Coalition– Writing for publication (peer-reviewed and consumer)
• Consumer publications – ‘Ready, Set, Grow’ – Local parenting magazines (e.g. Pittsburgh Parents)
54
10
©2018
Preparing for the Preceptor/NP Student Pediatric Experience
● Expectations from Academic Institutions● Preceptor Roadmap● Individual Student and Course Objectives● Orientation to the Site● Before Clinical Begins
55
©2018
The Nurse Practitioner Preceptor Triad: University of Iowa Exemplar
56https://www.cap2.net/
©2018
What Should Preceptors Expect From Academic Programs?
• Curriculum and access to the syllabi and course content• Individual student and course objectives
• Determine the types of learning opportunities that will best suit the student’s needs
• Evaluation tool for review– Paper or online, process for evaluating student
• Student and faculty name, contact information– Information on when to contact faculty
57
©2018
Clinical Faculty and You
• Faculty must support the student/preceptor relationship• Match student’s learning style with preceptor’s teaching style• Provide a preceptor orientation• Agree on how to assess student competency• Open communication on student progress
– Determine best method of communication (telephone, email, etc)• Provide periodic assessment of progress in the student-preceptor
relationship– Site visits
58
©2018
Roadmap for the Rotation (Expectations)
• Long term questions– What do I want the student to learn during their rotation with me?– What does the student want and need to learn during the rotation?
• Daily questions– What patients will be seen today?– What does the student want to learn from the experience today?– What objectives have not yet been met?
59
©2018
Individual Student Objectives
• Review student’s individual objectives and help monitor the student’s progress towards those objectives– Review objectives to ensure they are appropriate to the site,
realistic, and measurable– E.g. Integrate subjective and objective data in order to identify
pertinent differential diagnoses for children with respiratory concerns by mid semester
• Preceptors should share their own objectives for the student– E.g. Perform a thorough physical exam on an infant within two weeks
60
11
©2018
Take 5Objectives r/t Your Practice
• Identify pertinent objectives for your practice area. Be specific to the pediatric population and your clinical site.
• Are these realistic to present to the NP student, especially the unprepared student?
61
©2018
What to Discuss BEFORE Clinical Starts
• Contact information, what to do if late, etc.– Urgent contact information if someone cannot be reached
• Dress code • Scheduling and time management• Rundown of patient encounters
– Clinic setting (well vs sick visits)– In-patient setting (e.g. rounds, procedures)
• Documentation expectations: how, what, and where to document
62
©2018
Preceptor Suggestions for Student Preparation
• Direct the student to resources and evidence-based assigned readings– Specialty-specific readings – Review of pertinent assessment skills and developmental
expectations– Expectation that student will explore and
share new evidence
• Develop a small toolkit of essential resources for your practice
63
©2018
Orienting the Student
• Introduce student to staff and colleagues– Education program, length of rotation, their extent of involvement in
patient care
• Help student understand the patient population and services– What types of children are served? Who does what?
• Discussion of organizational policies/protocols
• Post a photo/short bio about the student in staff lounge, waiting room, exam rooms
(Lazarus, 2016)
64
©2018
Orienting the Student• Review organizational structure of
your hospital, clinic, unit, and/or team as is pertinent to NP student learning
• Review where pertinent forms, supplies, procedural areas, and other equipment are located
• EMR training as appropriate65
©2018
Expectations for Student and Preceptor
• Clear communication about what skills the studentpossesses and what skills they hope to develop in that setting
• Ask questions and seek further clarification• Ongoing feedback
– Positive experiences – Opportunities for further growth
• Integration of evidence-based practice and treatment decisions
66
12
©2018
Student Skills: Ongoing Development
• History taking and patient/family interview skills• Physical examination skills• Differential diagnosis identification• Treatment, management, developing plans of care• Reporting and presentation skills• Additional skills based on the clinical setting
– Procedures– Specialty diagnostic modalities
67
©2018
Guiding the NP Student Experience
• Introducing the NP student
• Approaches to Precepting
• Critical Thinking and Engagement Strategies
• When is the Student Ready for Independence?
68
©2018
Introducing the APRN Student
• Take a positive approach– Introduce as “NP student” NOT a “student NP”– Capitalize on the benefit of the Preceptor-NP student team …
• “This student will be speaking with and examining you/your child prior to our visit. S/he is highly skilled and we will be working together to give you the best treatment possible.”
69
©2018
Introducing the NP Student
• Reassure the child/family that they are getting the care they would normally receive PLUS the addition of an intelligent, detail-oriented, and motivated NP student
– “I have an NP student working with me. I am going to have her/him begin asking questions and complete the physical exam, then I will be back in…”
– “An NP student is working with me today. Together, we are going to begin the history, but I am going to have her/him take the lead. I am available to her/him and to you at all times.”
70
©2018
What if my patients refuse to see students?
• Tell child/family they were chosen specifically to give the NP student an opportunity to learn and you will be there every step of the way
• NP student is providing a “fresh set of eyes” • NP students are excellent source of the
“latest and greatest” information• Remind child/family the NP student is an
experienced RN who has worked with children extensively• If still refuse, reassure the NP student that it is not personal
71
©2018
Take 5Introducing the NP Student
• How do you introduce the NP student to pediatric patients and families?
• Is it effective?
• Discuss a change in your approach to be more effective & decrease the chance of the parent/child saying “no.”
72
13
©2018
Approaches to Precepting
• More than one approach can work• May depend on:
– Student’s clinical capabilities and readiness• Nudge them out of their comfort zone when safe
– Amount of time spent with current preceptor– The amount of patients and their ongoing needs through
the shift– Barriers within your clinical setting
73
©2018
Appointment Modification:Making Time to Teach
• Remove 1 appointment in the morning and 1-2 appointments in the afternoon
• This may reduce productivity so consult with your office in advance
- Ideally, managers will adjust productivity equation for preceptors
74
©2018
Observation:Beginning the Experience
• Initial strategy to see how much supervision the student needs
• NOT appropriate for more than the first few days
75
©2018
Structured Approach
• Patients carefully selected based on student skills – Start with uncomplicated routine well visits – Uncomplicated illness visit – Prior to visit student should:
• Do a complete chart review • Prepares components of anticipatory guidance and health
promotion• Formal pre-visit and post visit counseling with preceptor• Cases increase in number and complexity as student develops• Best suited for a NEW student
76
©2018
“Typical” Clinical DayThe Beginning-to-Advanced NP Student
• NP student assesses the child while preceptor is with another child/family
• Preceptor finishes – Returns and NP student presents the case to preceptor
with diagnosis and plan outlined – Validates or modifies diagnosis and plan with student in the
room• Student implements plan with assistance as needed
77
©2018
Focused Half Day • Choose 1-2 patients for the student to concentrate on
while preceptor sees other patients – Focus the visits to develop experience with various child
ages, conditions, and assessment skills aligned with course objectives
• Students use additional time to do chart review and research guidelines and develop plans
• Allows students to have an in depth experience as opposed to just observation
• Great if you have a “crazy, busy” day 78
14
©2018
Wave Scheduling
• Two or three patients are scheduled in one time block
• Student sees one patient while preceptor completes one or two patients– Remaining time at the end of the block is used for
feedback/consultation and completion of visit with NP student child/family
79
©2018
Wave Scheduling Examples
– 1:00 pm: 2 patients scheduled in 30 minute block (student sees one; preceptor completes one)
– 1:20 pm: Consultation/feedback with NP student; Wrap up with child – 1:30 pm: 2 patients scheduled in next 30 minute block (each see one)
OR
– 1:00 pm: 3 patients scheduled in 30 minute block (student sees one, preceptor completes 2)
– 1:30 pm: Consultation/feedback with NP student; Wrap up with child – 1:30 pm: 2 or 3 patients scheduled in next 30 minute block
80
©2018
“Sink or Swim”Moving towards Independence
• Student is given a variety of patients and sees them independently 1. No visible support 2. Minimal pre-visit teaching 3. Preceptor is ultimately responsible for
decisions4. Preceptor is available for backup 5. Best suited for a FINAL semester student
• Closely monitor until preceptor is comfortable
81
©2018
Clinical Days with the Acute Care Student
• Be present and participate during rounds– Students should pre-round and present patients if care
model and patient flow allows• If not, develop plans for students to learn these skills
• Procedures– See one, do one, teach one– Ensure that student knows the basics
• Indications and contraindications for procedure, safety measures, equipment needed, pain control, age-based considerations, etc.
82
©2018
Clinical Days with the Acute Care Student
• Preceptor to work closely with student performing H&P, PE, orders, and plan of care development for new patients
• Increased/progressing autonomy as rotation progresses• Patient status can affect this process
83
©2018
Clinical Days with the Acute Care Student
• Practice ongoing follow up, evaluation, and modification of the treatment plan– Prompt the student
• What are the results?• What do they mean?• How do the results change the plan of care?
• E.g.: Echocardiogram ordered during rounds. Did the student follow up? The results show poor function. How should the treatment plan be modified?
84
15
©2018
Critical Thinking and Engagement Strategies
• Using a formative evaluation process allows for a manageable way of teaching/evaluating NP student progress – Allows for discrimination of rationale behind a student’s thought
process– Asking deliberate questions also helps to distinguish rote memorization
from applied evidence based practice• Examples:
– One Minute Preceptor (OMP)– SNAPPS
85
©2018
The One-Minute Preceptor (OMP)Evidence-based, Time-efficient, Learner-centered approach
5 ‘Microskills’1. Commitment from NP student regarding differentials for child/adolescent1. Probe for underlying reasoning/supporting evidence for their assessment1. Teach the student “general rules” associated with the patient’s issue1. Provide positive feedback1. Correct errors
86
©2018
OMP in a nutshell
• “What do you think is going on?” (gain commitment)• “What led you to that conclusion?” (supporting evidence)• “Many times when ___” (teach general rules)• “You did an excellent job of ___” (positive feedback)• “Next time this happens try ___” (correct mistakes)
87
©2018
SNAPPS ModelMnemonic describes an efficient way for the student to present
patient cases and discuss clinical reasoning
• Step 1: Summarize the history and physical exam findings briefly• Step 2: Narrow the differential diagnoses• Step 3: Analyze the differential diagnoses
• Step 4: Probe the clinical instructor with questions and express caseuncertainties
• Step 5: Plan management for patient case• Step 6: Select a case-related issue for self-directed learning
88
©2018
General expectations for pediatrics
• Developmental variations• Anticipatory guidance• Individualizing advanced assessment skills• Immunization awareness• Health promotion• Basic principles of pharmacology• Basic pathophysiology
89
©2018
Promoting Safe NP Student Practice
• Follow standards as outlined in the facility or organization’s policy and procedures manual
• Be aware of one’s limitations and seeking assistance• Utilize strategies that prevent harm or injury to
pediatric patients and families • Be aware of principles behind nursing actions• Communicate honestly with NP student
(Wolff , Regan, Pesut, & Black, 2010)
16
©2018
Tips to Engage the NP Student in Pediatric Patient Encounters
• Remind the NP student to WATCH you• Role model how you approach the child or adolescent
– Sitting on ‘even ground’– Conversation style– Asking questions– Tailoring the physical exam to the child’s age– Making the exam fun
91
©2018
Questions/Statements to Facilitate Learning
• 1. What do you think?
• 2. Why do you think that?
• 3. What led you to consider that conclusion?
• 4. What else did you consider and rule out?
• 5. Specifically, you did a good job of _____ and this is why it is important…
• 6. You did well based on your knowledge of older children but how can you factor in the infant’s development?
• 7. I disagree with…. A more efficient way is……
• 8. The key point I want you to remember is….
• 9. What did we learn from this?
92
©2018
Reflective Journaling
• Student writes a one-page journal entry about a specific clinical experience – Review how they applied critical thinking skill or habit to
the situation• Student reflects on their initial actions and thoughts• Focuses on enhancing their critical thinking skills to improve
clinical decision making
• Examples and rubric for reviewing journal entries in Toolkit appendices
(Raterink, 2016)93
©2018
When is the student ready to be independent?????
94
©2018
Competent Proficient Learner
• Solid skills in HPI, physical assessment, evaluation and management
• Can relate past experiences to current situations • Preceptor steps out • NP student should know their limitations and when to
seek assistance • NP student follows expected time frames for H & Ps,
visits, follow-up, plan of care reevaluation, etc. • Exhibits strong presentation/reporting skills
95
©2018
Transitional Learner
• Preceptor steps back • Shorten pre- and post-encounter consults • NP student establishes basic priorities for each
encounter independently • NP student gathers essential relevant data and conducts
visits with efficiency and effectiveness
96
17
©2018
When Do I Call Faculty?
1. Any concerns about student performance- Identification of red flags- Safety issues- The difficult student
2. Mismatch with student- Personality (attempts to resolve unsuccessful)
3. Mismatch of clinical site4. Receiving insufficient feedback and guidance
97
©2018
Site Visits• Schedule the site visits early and at a convenient time
for the preceptor– Extra site visits may be scheduled for:
• new preceptors• students experiencing difficulty
• Site visit focus:– Student
• Verifying competency • Verifying types of patients seen are suitable • Verifying course/student objectives
– Student/preceptor interactions98
©2018
The Difficult Student
• What to Do?• Concerns
– Amount of Direction Provided– Mismatch
• Difficult Types– The Shy Student– The Unmotivated Student; Lacking Commitment– The Inflexible Student– The “Know-it-all”– The Unprepared Student
99
©2018
What To Do With The Difficult NP Student?
• Identify where the area of concern is:– Lack of focus– Relating with patient– Communication with patients, preceptor or staff– Decision making, using evidence based practice– Knowing boundaries
• Contact school early on for intervention– Remediation is best handled by faculty; Not the
responsibility of the preceptor to “fix” the problem100
©2018
Concern:
Amount of Direction Provided
Problem● Providing too much help
– Stalls movement towards independence
– Fosters dependence
● Providing too little help– Leaves NP student
floundering– Inhibits progress toward
independence
101
Strategy● Engage the NP student &
review their objectives● Have the NP student talk
with peers regarding the direction they are receiving
● Bring info back to the preceptor & strategize a realistic plan
©2018
Concern:
Mismatch
Problem● Mismatch can result due to:
○ Conflicting personalities○ Differing career goals○ Incongruence in understanding
clinical objectives○ Differences in work ethic
● Preceptor finds that valuable time is being wasted
Strategy● Identify and address a
potential mismatch early● Seek faculty support● Redefine goals and objectives
& approach for a successful pediatric experience
● Early site visit by faculty to mediate and help strategize
102
18
©2018
The Shy or Dependent NP Student
Problem• Hesitant to approach
child/family• Little initiative to seek new
experiences• Lack confidence• Prefers to shadow preceptor
and/or other HCPs
Strategy• Capitalize on strengths
– Direct NP Student to child/family of comfort
– Gradually introduce to other ages
• Positive reinforcement
• Graduated approach to history, physical exam, and reporting
103
©2018
The Graduated Approach• Revisit the objectives at the beginning of each experience
– Set specific parameters to move the student away from sole dependence
• Wean from shadowing preceptor– Joint history & PE x 3 visits; – NP student history alone w/joint PE– Gradually increasing responsibility– Designate time to complete tasks
• The detailed report– Allow detail initially to ensure the student has identified all relevant
information within a given timeframe– Over a designated time guide NP student to focus on pertinent
positives and negatives104
©2018
NP Student Lacking Commitment
Problem● Perceived lack of motivation &
commitment of NP student for successful career development
● NP student is at risk for failing
● Preceptor finds that valuable time is being wasted
● Overall frustration
Strategy● Discuss concern with NP
student to determine the cause
● Often there is another issue underlying the problem
● Question a possible lack of appeal for the NP students career focus
105
©2018
The Inflexible NP Student
Problem• Missed learning
opportunities• Potential for unsafe
practice• Compromised interaction
with child/family leading to decreased trust
• Rigid in approach to History, PE
Strategy• Point out examples of
inflexibility• Discuss specific examples &
resulting repercussions• Discuss effect on child &
parents• Identify examples of NP
student showing flexibility & discuss benefits
106
©2018
The “Know-It-All”
Problem• Proceeds too quickly
– Fast PE & history• At-risk for unsafe practice
– Not staying up-to-date on the evidence
– Misses pertinent Hx/PE data• Questionable safe
management of child• Potential for mistakes• At risk for alienating team
Strategy• Remind NP student to
provide rationale for differentials, management, treatment plan
• Point out omissions/errors• Discuss how to maintain
best practice• Revisit objectives to
identify how NP student can improve
107
©2018
The Unprepared NP Student
Problem• Safety of child• General time management
– Wasting preceptor’s time– Inefficient interaction with
child/family• Decreased progress toward
professionalism
Strategy• Review NP student
objectives & preceptor expectations
• Set measurable parameters– Identify critical points of
preparation– Pertinent evidence to review
• Specify a realistic time for expected behavior change
• Provide ongoing feedback108
19
©2018
The Bottom Line
• Never, ever hesitate to contact the NP student’s faculty by phone or email at any time
• Be prepared to discuss the NP student concern– Summarize the concern(s)– Provide examples– Include any steps toward resolution
• Determine new strategies with faculty• Identify need for an early site visit by faculty
109
©2018
Can you “Fire” an NP Student?• Yes, … but ...• Be able to justify your decision with evidence
– Lack of ability to followed the specified guidelines presented at the beginning of the experience
– Inability to follow through or improve following constructive feedback
– Unsafe practice– Compromising the care of the child/family– Lack of respect for the setting and Health Care providers
• Late arrival; early departure• Inaccurate, deceptive reporting
110
©2018
Take 5Difficult Student Experience
• Briefly describe an experience with a “difficult student.”
• What strategy did you use to resolve the problem?
111
©2018
Balancing Work, Teaching, and Life
• The Preceptor Balancing Act• Self Care For the Busy
Preceptor• Managing Burnout• Using the Engaged Feedback
Reflective Inventory
112
©2018
The Preceptor Balancing Act
• Balance productivity with teaching
• Seeking student contributions to enhance the day, not hinder work
• Modifying approach to precepting may enhance the balance
• Work smarter, not harder113
©2018
Self Care for the Busy Preceptor• Enhance your well-being!• Model what we tell our patients:
– Promote positive self care strategies• Healthy diet• Regular exercise
– Use of stress management techniques• Explore coping patterns• Practice relaxation techniques• Promote positive self-care strategies
– Maintain healthy interpersonal relationships– Engage in spiritual growth practices
114
20
©2018
Preceptor Burnout
Three Dimensions• Emotional exhaustion• Depersonalization• Reduced personal
accomplishment
115
©2018
Minimizing Preceptor Burnout
• Explore sharing the preceptor role with a colleague• Consider a half-semester OR one-day specialty
experience• Avoid scheduling students every day• Take a semester off• Learn to say ‘no’- it’s OK to say ‘no’
116
©2018
Clinical Pearls for Maintaining Sanity
• Every case can be a teachable moment, but not every case has to be…
• Focus on what can be learned from new and challenging cases each week
• One or two “focused moments” spent pointing out key principles can produce a lot of learning in a short time
(Weber, 2015) 117
©2018
Engaged Feedback Reflective Inventory:Reflecting on your precepting experience
(Rosa & Santos, 2016)
• Method of effective communication that can aid in self care of the preceptor– Rooted in concepts of shared accountability, respect, and
partnership
• The preceptor engages vulnerability, acts as an authentic presence, manages uncertainty, and finds compassion for the student’s experience– Enhances the preceptor’s ability to listen more effectively– Promotes healthy professional relationship between preceptor and
NP student118
©2018
Engaged Feedback Reflective Inventory (Santos & Rosa, 2016)
I’m ready to sit next to you rather than across from you What does my body language reflect as we communicate?
I’m ready to put the problem in front of us Can I look at the challenges objectively?
I’m ready to listen, ask questions, and accept that I may not fully understand the issue
Can I ask for clarification, let go of assumptions, and address concerns ‘in the moment’?
I want to acknowledge what you do well rather than picking apart your mistakes
Can I identify, acknowledge, and celebrate my student’s accomplishments?
I recognize your strengths and how you can use them to address your challenges
Can I help build on the NP student’s strengths? Can I help them use those strengths in facing challenges/obstacles?
I can hold you accountable without shaming/blaming you Can I accept that mistakes are a normal part of the process? Do I provide constructive feedback?
I’m willing to do my part Do I own and express responsibility for my part in the process?
I can genuinely thank you for your efforts rather than criticizing you for your shortcomings
Am I thanking the student for their efforts? Do I thank myself for being available to the NP student?
I can talk about how resolving these challenges will lead to your growth and opportunity
Am I focusing on the student’s growth or failure? Do I resolve challenges quickly or prolong them unnecessarily?
I can model the vulnerability and openness that I expect to see from you
Do I value vulnerability and honesty in professional relationships, or does the concept make me uncomfortable?
119
©2018
Managing Barriers in the Clinical Site
120
• Electronic Medical Record– Lack of student access or
restricted access• Too Much to Do• Not Enough to Do• If the Patient/Parent
Refuses to See Child• CMS/Medicaid Regulations• Managing Prescriptions
21
©2018
Lack of Access to the EMR
• Students with limited or restricted EMR access can document on a form that can help the preceptor complete his/her electronic charting
• SOAP notes on all patient encounters: handwritten or a Word doc– Facilitates acquisition of time management skills– Eases later transition from NP student to APRN
121
©2018
Managing Prescriptions
• Student should be planning treatment with preceptor input, choosing medications using best evidence, and calculating dosages/timing/mL equivalents and quantity needed
• APRN typically writes/electronically enters/sign prescriptions
• Discuss impact of prescriptive authority on your practice– DEA registration, drug schedules and limitations– Obtaining pharmacology CE per state/certification requirements
122
©2018
NP Student and ‘Perceived Downtime’ • Assign directed reading on specific clinical topics
that arise• Discussion of new pediatric evidence• Reflective journaling• Additional materials can be developed by the
NP student, such as patient education• Students may enter their clinical cases into
electronic tracking systems • Additional projects (QI, etc)• Case discussions (see ‘Difficult Student’ slides..)• Update medication knowledge 123
©2018
Take 5Perceived Downtime
• In your practice setting, identify 1-2 solutions to direct the student during perceived downtime.
124
©2018
“What do I do with my student if I am too busy?”
• 1. Everyday is a busy day
• 2. Send student to patient care focused rounds, conferences, or meetings
• 3. Establish a buddy system where another NP can help the student
• 4. If another NP/HCP has an interesting case ask them to pull out the student
• 5. Spend time with child life worker, social services, therapist, dental technician, or other discipline within the practice
• 6. Patient follow up calls
• 7. OR bring them along for the ride
(Burns et al, 2006)
125
©2018
CMS Documentation Guidelines
• Medicare payments only cover services provided by physicians and other licensed practitioners – In general, to bill for a service rendered, you must be considered an
eligible provider of care (enrolled in Medicare as a provider or credentialed by the insurance carrier)
• Student can contribute to billable service but it must be done in the physical presence of the billing provider
126
22
©2018
CMS Documentation Guidelines
• Students can document only – Past Medical Hx – Social Hx– Family Hx– ROS
• Preceptor must repeat and document HPI, relevant PE and medical decision making
127
©2018
Evaluating the NP Student
• Evaluation Criteria• Types of Evaluation• Red Flags• Competencies• Unique Challenges
128
©2018
Evaluating the NP Student• Evaluation criteria should be based on:
– Skills required for the role– Curriculum content/expectations– Objectives & Goals
• Program• Student• Preceptor
• Communication throughout the experience is essential to feedback and evaluation– Engagement by preceptor, student, & faculty
129
©2018
Evaluating the NP Student
• Types of evaluation– Formative
• Progress towards objectives and goals• Ongoing throughout the experience
– Summative• Achievement of objectives and goals• End of clinical rotation/semester
130
©2018
Evaluating the NP Student
• Examples of formative evaluation in the clinical setting– Case presentations/discussion– Informal discussion– Informal feedback– Questioning exercises– Mid-term evaluations
131
©2018
Evaluating the NP Student
• Examples of summative evaluation in the clinical setting– Formal evaluation tool (most common)
• Based on NONPF competencies– Student self-evaluation– Preceptor evaluation of site-specific goals– Student evaluation of site and preceptor
132

23
©2018
Evaluating the NP StudentCompetencies required for all NP students, regardless of setting and specialty
• Professionalism• Respect for individuals• Effective communication• Adherence to confidentiality• Ability to work within a team
Failure to demonstrate these should be communicated to faculty promptly
133
©2018
Evaluating the NP Student: Red Flags
Primary Care• Developmentally appropriate• Anticipatory guidance• Attention to immunizations• Advanced assessment skills• Basic knowledge & questions• Family-centered care• Scope of Practice
Acute and Specialty Care• Developmentally appropriate• Advanced assessment skills• Basic knowledge & questions• Consideration of
differential diagnoses• Family-centered care• Scope of Practice
134
©2018
Evaluating the NP Student
• NONPF Competency Domains– Scientific Foundation Competencies– Leadership Competencies– Quality Competencies– Practice Inquiry Competencies– Technology and Information Literacy Competencies– Policy Competencies– Health Delivery System Competencies– Ethics Competencies– Independent Practice Competencies
135
©2018
Evaluating the NP Student
Unique challenges in the acute care setting:
• Evaluation tools may evaluate students based on “independence” or ability to perform skills “with minimal supervision”
• This is challenging, as many AC PNPs work within interprofessional teams and even the most experienced still are not completely “independent” or “with minimal supervision”
136
©2018
Evaluating the NP Student
Unique challenges in the pediatric specialty care setting
• Depending on the setting, many specialty care PNPs may not be able to let the student work independently– Procedures may have to be performed by the preceptor with student
observing– Interprofessional teams
137
©2018
Take 5Mistakes and What We Have Learned
• Have you had a less-than-positive experience as a preceptor?
• How was this a “teaching moment” for you?
• What could you do differently?
138
24
©2018
Hallmarks of Professional Growth
Intellectual CuriosityMental FlexibilityClinical Expertise
Evidence-Based UnderpinningsUnparalleled Professionalism
139
©2018
Take 5 HomeworkPhilosophy of Clinical Education
Based on what you have learned today, including your past experience, state your philosophy of clinical education in 1-2 sentences.
E.g.: As an APRN in pediatrics, I am committed to providing a supportive learning environment that will foster independence and help the NP student provide individualized, developmentally appropriate care to the children and families they encounter.
140
©2018
We can only build the future of pediatric health care by working together
(What the Dalai Lama would have said if he was a pediatric-focused NP)
141
©2018
Resources
• Websites– National Organization of Nurse Practitioner Faculties
• http://www.nonpf.org/?page=PreceptorPortal_Main– Association of Faculties of Pediatric Nurse Practitioners
• http://www.afpnp.org/afpnp/resources.html
142
©2018
ReferencesAagaard, E., Teherani, A., & Irby, D. (2004). Effectiveness of the one-minute preceptor model for diagnosing the patient and the learner: Proof of
concept. Academic Medicine, 79(1), 42-49.
American Association of Nurse Practitioners (2017). NP Fact Sheet. Retrieved from: https://www.aanp.org/all-about-nps/np-fact-sheet.
Barker, E. & Pittman, O. (2010). Becoming a super preceptor: A practical guide to preceptorship in today’s clinical climate. Journal of the American Academy of Nurse Practitioners, 22, 144-149. doi: 10.1111.j.1745-7599.2009.00487.x
Bandura, A., (1977). Social learning theory. New York: General Learning Press.
Bengtsson, M. & Carlson, E. (2015). Knowledge and skills needed to improve as preceptor: Development of a continuous professional development course- a qualitative study part I. BMC Nursing, 14(51). doi: 10.1186/s12912-015-0103-9
Brooks, M. & Niederhauser, V. (2010). Preceptor expectations and issues with nurse practitioner clinical rotations. Journal of the American Academy of Nurse Practitioners, 22, 573-579. doi: 10.1111/j.1745-7599.2010.00560.x
Brykczynski, K.A. (2009). Role development of the advanced practice nurse. In A. Hamric, J. Spross, & C. Hanson, Advanced practice nursing: An integrative approach (4th ed.), (pp. 95-120). Philadelphia: Saunders.
Buchel, T. & Edwards, F. (2005). Characteristics of effective clinical teachers. Family Medicine, 37(1), 30-35.
Burns, C., Beauchesne, M., Ryan-Krause, P., & Sawin, K. (2006). Mastering the preceptor role: Challenges of clinical teaching. Journal of Pediatric Health Care, 20(3), 172-183. doi: 10/1016.j.pedhc.2006.10.012.
143
©2018
ReferencesCho, C., Ramanan, R., & Feldman, M. (2011). Defining the ideal qualities of mentorship: A qualitative analysis of the characteristics of outstanding
mentors. The American Journal of Medicine, 124, 453-458. doi: 10.1016/j.amjmed.2010.12.007
Donley, R., Flaherty, MJ., Sarsfield, E., Burkhard, A., O’Brien, S., & Anderson, K.(2014). Graduate clinical nurse preceptors: Implications for improved intraprofessional collaboration. OJIN: The Online Journal of Issues in Nursing, 19(3). doi: 10.3912/OJIN.Vol19No03PPT01
Dreyfus, S. E., & Dreyfus, H. L. (1980, February). A five stage model of the mental activities involved in direct skills acquisition. United States Air Force Operations Research Center Report 80-2.
Facione, P. (1990). Critical thinking: A statement of expert consensus for purposes of educational assessment and instruction. Millbrae, CA: The California Academic Press.
Farrell, K., Payne, C., & Heye, M. (2015). Integrating interprofessional collaboration skills in o the advanced practice registered nurse socialization process. Journal of Professional Nursing, 31(1), 5-10. doi: http://dx.doi.10.1016/j.profnurs.2014.05.006
Farwell, A. L. (2009). Practitioner preceptors: A shortage of willing mentors. Journal of Pediatric Health Care, 23(3), 198-200. doi:10.1016/j.pedhc.2009.02.009
Forsberg, I., Swartwout, K., Murphy, M., Danko, K., & Delaney, K. R. (2014). Nurse practitioner education: Greater demand, reduced training opportunities. Journal of the American Association of Nurse Practitioners, 27(2), 66-71. doi:10.1002/2327-6924.12175
Furney, S., Orsini, A., Orsetti, K., Stern, D., Gruppen, L., & Irby, D. (2001). Teaching the one-minute preceptor: A randomized controlled trial. Journal of General Internal Medicine, 16, 620-624.
Gorton, K., & Hayes, J. (2014). Challenges of assessing critical thinking and clinical judgment in nurse practitioner students. Journal of Nursing Education, 53(3), suppl., S26-S29. doi: 10.3928/0144834-20140217-02
144
25
©2018
ReferencesGoss, C. (2015). Systematic review building a preceptor support system. Journal for Nurses in Professional Development, 31(1), E7-E14. doi:
10.1097/NND.0000000000000117
Green, J., & Jackson, D. (2014). Mentoring: Some cautionary notes for the nursing profession. Contemporary Nurse: A Journal For The Australian Nursing Profession, 47(1-2), 79. doi:10.5172/conu.2014.47.1-2.79
Heinrichs, S., Vela, L., & Drouin, J. (2013). A learner-centered technique and clinical reasoning, reflection and case presentation attributes in athletic training students. Journal of Athletic Training, 48(3), 362-371. doi: 10.4085/1062-6050-48.2.17
Horton, C., DePaoli, S., Hertach, M., & Bower, M. (2012). Enhancing the effective of nurse preceptors. Journal for Nurses in Staff Development 28(4), E1-E7. doi: 10.1097/NDD.0b013e31825dfb90
Latessa, R., Colvin, G., Beaty, N., Steiner, B., & Pathman, D. (2013). Satisfaction, motivation and future of community preceptors: What are the current trends? Academic Medicine, 88(8) 1164-1170.
Lazarus, J. (2016). Precepting 101: Teaching strategies and tips for success for preceptors. Journal of Midwifery & Women’s Health, 61(supp 1), S11-S21. doi: 10.1111/jmwh.12520.
Leimbach, M. & Wilson Learning Worldwide (2018). Social styles versatile communication avoiding the hidden costs of communication misalignment.Retrieved from: http://www.wilsonlearning.com/wlw/articles/w/hidden-cost-com
Link, D. (2009). The teaching-coaching role of the APN. Journal of Perinatal and Neonatal Nursing, 23(3), 279-283.
Logan, B., Kovacs, K., & Barry, T. (2015). Precepting nurse practitioner students: One medical center’s efforts to improve the precepting process. Journal of the American Association of Nurse Practitioners, 27, 676-682. doi: 10.1002/2327-6924.12265
Macleod, S. (2007). The challenge of providing mentorship in primary care. Postgraduate Medical Journal, 83, 317-319.
145
©2018
ReferencesNational Task Force on Quality Nurse Practitioner Education (2016). Criteria for evaluation of nurse practitioner programs (5th ed.). Washington, DC:
American Association of Colleges of Nursing & National Organization of Nurse Practitioner Faculties.
Neher J., Gordon K., & Meyer B. (1992). A five-step "microskills" model of clinical teaching. Journal of American Board of Family Practice, 5(4), 419-424.
Nilson, L. (2010). Teaching at its best (3rd Ed.). San Francisco, CA: John Wiley & Sons.
Nowell, L., Norris, J., Mrklas, K., & White, D. (2017). A literature review of mentorship programs in academic nursing. Journal of Professional Nursing, 33(5), 334-344. https.//doi.org/10.1016/j.profnurs.2017.02.007
O’Connor, B. (2012). New American Association of Colleges of Nursing data show enrollment surge in baccalaureate and graduate programs amid calls for more highly educated nurses. Journal of Professional Nursing, 28, 137-138.
Onieal, M.-E. (2016). Precepting: Holding students and programs accountable. Clinician Reviews, 11-17.
Pearson, T., Garrett, L., Hossler, S., McConnell, P., & Walls, J. (2012). A progressive nurse practitioner student evaluation tool. Journal of the American Association of Nurse Practitioners, 24(6), 352-357. doi: 10.1111/j.1745-7599.2012.00713.x
Raterink, G. (2016). Reflective journaling for critical thinking development in advanced practice registered nurse students. Journal of Nursing Education, 55(2), 11-104. https://doi.org/10.3928/01484834-20160114-08
Rosa, W., & Santos, S. (2016). Introduction of the engaged feedback reflective inventory during a preceptor training program. Journal for Nurses in Professional Development, 32(4), E1-E7. doi: 10.1097/NND.0000000000000280
Ryan, S., & Rosenberg, S. (2015). Nurse practitioners and political engagement: Findings from a nurse practitioner advanced practice focus group & national online survey. Overland Park, KS: American Nurse Practitioners Foundation.
146
©2018
ReferencesScheffer, B., & Rubenfeld, G. (2000). A consensus statement on critical thinking in nursing. Journal of Nursing Education, 39(8), 352-359.
https://doi.org/10.3928/0148-4834-20001101-06
Shellenbarger, T., & Robb, M. (2016). Effective mentoring in the clinical setting. American Journal of Nursing, 116(4), 64-68.
Shinners, J., & Franqueiro, T. (2017). The nursing professional development practitioner and preceptor role development. Journal for Nurses in Professional Development. Retrieved from: www.jnpdonline.com
Sims, S., & Swenson, M. (2015). Module III: Preceptor guidelines. In: Dumas, J. (ed.) Partners in NP education: A preceptor manual for NP programs, faculty, preceptors & students (2nd Ed). Washington, DC: The National Organization of Nurse Practitioner Faculties.
Souba, W.W. (1999). Mentoring young academic surgeons, our most precious asset. Journal of Surgical Residency, 82, 113-120.
Swihart, D., & Figueroa, S. (2014). The preceptor program builder: Tools for a successful preceptor program. Danvers, MA: HCPro.
The National Organization of Nurse Practitioner Faculties (NONPF) NP Core Competencies Content Work Group (2017). Nurse practitioner core competencies content. Retrieved from: http://www.nonpf.org/?page=14
Ulrich, B. (2011). Mastering precepting: A nurse’s handbook for success. Indianapolis, IN: Sigma Theta Tau International Honor Society of Nursing.
Venter, E. (2017). Bridging the communication gap between generation Y and the baby boomer generation. International Journal of Adolescence and Youth, 22(4), 497-507. doi: 10.1080/02673843.2016.1267022
Ventola, C. L. (2014). Social media and health care professionals: Benefits, risks, and best practices. Pharmacy and Therapeutics, 39(7), 491–520.
Vrabie, A. (2014). Improve team communication with the social style model. Retrieved from:http://blog.sandglaz.com/improve-team-communication-by-understanding-the-social-style-model/
147
©2018
ReferencesWebb, J., Lopez R., P., & Guarino, A.J. (2015). Incentives and barriers to precepting nurse practitioner students. Journal for Nurse Practitioners,
11(8), 782-789. doi: 10.1016/j.nurpra.2015.06.003.
Weber, R. (2015). The perfect preceptor. The Journal of Craniofacial Surgery, 25(8), 2257-2260. doi: 10.1097/SCS.0000000000002211
Wenger, E., McDermott, R. A., & Snyder, W. (2002). Cultivating communities of practice: A guide to managing knowledge. Boston, MA: Harvard Business School Press.
Wilson, L, (2004). The social styles handbook: Find your comfort zone and make people feel comfortable with you. Portland, OR: Nova Vista Publishing.
Windey, M., Lawrence, C., Guthrie, K., Weeks, D., Sullo, E., & Chapa, D. (2015). A systematic review on interventions supporting preceptor development. Journal for Nurses in Professional Development, 31(6), 312-323. doi: 10.1097/NND.0000000000000195
Wirtz Rugen, K., & Jorbridge, S. (2016). Precepting in a busy clinic. [https://vimeo.com/153056353]. Retrieved fromhttp://www.nonpf.org/?page=PreceptorPortal_Main.
Wolff, A., Regan, S., Pesut, B., & Black, J. (2010). Ready for what? An explanation of the meaning of new graduate nurses’ readiness for practice. International Journal of Nursing Education Scholarship, 7(1), ISSN (Online) 1548-923X, doi: https://doi.org/10.2202/1548-923X.1827
Wolpaw, T., Papp, K., & Bordage, G. (2009). Using SNAPPS to facilitate the expression of clinical reasoning and uncertainties: A randomized comparison group trial. Academic Medicine, 84(4), 517-524.
148





























