Embed Size (px)
Citation preview

at SciVerse ScienceDirect
Placenta 33 (2012) 227e229
Contents lists available
Placenta
journal homepage: www.elsevier .com/locate/placenta
Short communication
Arterio-arterial vascular anastomoses in monochorionic twin placentas withand without twin anemia-polycythemia sequence
S. de Villiers a, F. Slaghekke b, J.M. Middeldorp b, F.J. Klumper b, F.J. Walther a, D. Oepkes b, E. Lopriore a,*
aDivision of Neonatology, Department of Pediatrics, J6-S, Leiden University Medical Center, PO Box 9600, 2300 RC Leiden, The NetherlandsbDivision of Fetal Medicine, Department of Obstetrics, Leiden University Medical Center, Leiden, The Netherlands
a r t i c l e i n f o
Article history:Accepted 5 January 2012
Keywords:Monochorionic placentaTwin anemia-polycythemia sequenceVascular anastomosesArterio-arterial anastomosis
* Corresponding author. Tel.: þ31 0 71 5262909; faE-mail address: [email protected] (E. Lopriore).
0143-4004/$ e see front matter � 2012 Elsevier Ltd.doi:10.1016/j.placenta.2012.01.009
a b s t r a c t
We performed a matched caseecontrol study to analyze the placental angioarchitecture, in particular thediameter of arterio-arterial (AA) anastomoses in monochorionic placentas from pregnancies withspontaneous twin anemia-polycythemia sequence (TAPS) compared to a control group of uncomplicatedmonochorionic placentas. Placental angioarchitecture was analyzed using colored dye injection. AAanastomoses were detected in 20% (3/15) of spontaneous TAPS placentas. The median diameter of AAanastomoses in the group with and without TAPS was 0.4 mm and 2.2 mm, respectively (p ¼ 0.01). Inconclusion, AA anastomoses are rarely detected in TAPS placentas. When present, the AA anastomosis isvery small, preventing equilibration of hemoglobin levels between both twins.
� 2012 Elsevier Ltd. All rights reserved.
1. Introduction
Feto-fetal blood transfusion occurs in all monochorionic (MC)twins because of the invariable presence of placental vascularanastomoses and may lead to the development of twin anemia-polycythemia sequence (TAPS) [1]. TAPS is characterized by largeinter-twin hemoglobin differences in the absence of amniotic fluiddiscordances [1]. The typical angioarchitecture in TAPS placentasafter colored dye injection demonstrates only a few minusculearterio-venous (AV) anastomoses [2]. Arterio-arterial (AA) anasto-moses are reported to be rare (10%) in TAPS [1]. In contrast, AAanastomoses are almost ubiquitous in normal monochorionicplacentas [2], suggesting that AA anastomoses may play a protect-ing role against the development of TAPS [2].
We previously hypothesized that the diameter of AA anasto-moses in TAPS may be smaller, preventing adequate inter-twinblood volume equilibration [3,4]. However, evidence to supportthis hypothesis is currently lacking. The objective of this study wasto compare the diameter of AA anastomoses in MC twin placentaswith and without TAPS.
2. Methods
All consecutive TAPS placentas examined at our center between June 2002 andNovember 2011 were included in this study. For the purpose of this study we
x: þ31 0 71 5248198.
All rights reserved.
excluded TAPS placentas without AA anastomoses.We also excluded TAPS cases thatoccurred after laser treatment -for twinetwin transfusion syndrome (TTTS). Eachspontaneous TAPS placenta was compared with 3 control placentas from uncom-plicated MC twin pregnancies and matched for gestational age at birth (�1 weekgestation). TAPS was diagnosed using standard antenatal ultrasound criteria and/orpostnatal criteria [1].
Each MC placenta examined at our center is routinely injected with colored dyeaccording to a previously described protocol [5]. After colored dye injection,placentas are photographed in a plain view, and digital pictures are saved forcomputer analysis. Data on placenta angioarchitecture, including the number andtype of anastomoses, the percentage of placental territory and the type of umbilicalcord insertion are prospectively entered in a dedicated database.
The primary outcomewas the diameter of the AA anastomoses. Diameters of theAA anastomoses and individual placental territories were measured using ImageTool for Windows version 3.0 (Image Tool, San Antonio, Texas, USA, http://ddsdx.uthscsa.edu/dig/itdesc.html). Part of the placental data reported in this study wasincluded previously in a case report on AA anastomoses in TAPS [1,4].
Results of continuous and categorical variables were analyzed using the MannWhitney U test and Fisher exact test. A p-value <0.05 was considered to indicatestatistical significance. All statistical datawere analyzed using SPSS statistics version17.0 (SPSS Inc., Chicago, IL, USA).
3. Results
A total of 491 MC placentas were injected during the studyperiod, of which 44 (9%) fulfilled the diagnostic criteria for ante-natal or postnatal TAPS. TAPS cases occurred after incomplete lasertreatment for TTTS in 66% (29/44) of cases and occurred sponta-neously in 34% (15/44) of cases. In this subgroup of 15 cases withspontaneous TAPS, an AA anastomosis was identified in 3 placentas(20%, 3/15). None of these TAPS cases were treated antenatally withfetoscopic laser coagulation. Each TAPS placenta (n ¼ 3) was

Table 1Placental characteristics in the study group (TAPS placentas with an AA anasto-mosis) and control group (uncomplicated MC placentas with an AA anastomosis).
Study group(n ¼ 3)
Control group(n ¼ 9)
p-value
Number of anastomosesper placentaa
5 (3e6) 10 (3e16) 0.32
VV anastomoses present e (%) 0 (0) 2 (22) 0.55AV anastomoses present e (%) 3 (100) 9 (100) 1.0Diameter of AA
anastomosis (mm)a0.4 (0.3e0.6) 2.2 (0.7e3.5) 0.01
Placental share discordance - %a 42 (24e64) 26 (11e43) 0.08Unequal placental
sharing > 20% e n (%)3 (100) 2 (22) 0.11
Velamentous cordinsertion e n (%)b
2/6 (33) 6/18 (33) 0.70
Marginal cord insertion e n (%)b 2/6 (33) 2/18 (11) 0.25Velamentous or marginal
cord insertion e n (%)b4/6 (66) 8/18 (44) 0.32
AA: arterio-arterial; VV: veno-venous; AV: arterio-venous.a Value given as median (range).b Refers to the type of cord insertion per fetus.
S. de Villiers et al. / Placenta 33 (2012) 227e229228
matched with 3 control MC placentas (n ¼ 9). Mean gestational ageat delivery was 32.3 weeks in both groups (range 29e36 weeks).
The median diameter of AA anastomoses in the group with andwithout TAPS was 0.4 mm (range: 0.3e0.6) and 2.2 mm (range:0.7e3.5), respectively (p ¼ 0.01). The diameter of the AA anasto-mosis was � 1 mm in each TAPS placenta whereas only 2 AAanastomoses in the control group had a diameter� 1mm (22.2%, 2/9), leading to a sensitivity of 100% (3/3) and a specificity of 77.8% (7/9). A total of 11 AV anastomoses were detected in the 3 TAPS cases.
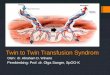
Fig. 1. TAPS placenta after colored dye injection (blue and green for arteries, pink and orangeDetail of the AA anastomosis is shown in the bottom-right corner. The two green stars ind
The direction of the AVs in the TAPS cases was mostly (64%, 7/11)from the anemic fetus to the polycythemic one. Further details onplacental characteristics in both groups are shown in Table 1. Anexample of a TAPS placenta with a small AA anastomosis is shownin Fig. 1.
4. Discussion
This study shows that in the rare TAPS cases with an AA anas-tomosis, the diameter of the AA anastomosis is extremely small(�1 mm), in accordance with our hypothesis [4]. In addition, thisstudy confirms that only aminority of TAPS placentas (20%) containsan AA anastomosis [1], a significantly lower incidence compared touncomplicated MC pregnancies (89%) [2]. Although the presence ofan AA anastomosis may have an important protective effect, it doesnot preclude the development of TAPS [3,4,6].
The exact pathophysiologic role of the small AA anastomosis inthe development of TAPS is not entirely clear. As previously shown,the pathogenesis of TAPS seems to be based on a uniqueangioarchitecture characterized by the presence of a paucity ofminuscule vascular anastomoses [2]. The few small anastomosesallow a slow transfusion of blood (as low as 5e15 ml/24h) from thedonor to the recipient, leading gradually to highly discordanthemoglobin levels [6,7].
AA anastomoses are bidirectional anastomoses and are thoughtto have protective properties against hemodynamic imbalancecaused by AV anastomoses [8e10], as confirmed by a mathematicalcomputer model [11]. However, the blood flow through aminusculeAA anastomosis is probably extremely low and insufficient to allowfor adequate equilibration of the blood volumes between both
for veins) with a small AA anastomosis (white star)(diameter of anastomosis: 0.3 mm).icate two small AV anastomoses.

S. de Villiers et al. / Placenta 33 (2012) 227e229 229
twins. Inter-twin blood flow volume and velocity is known to bestrongly correlated to the diameter of an anastomosis, according toPouiseuille’s equation. Flow resistance depends linearly upon theviscosity and the length of a vessel, but depends to the fourth powerupon the radius. Minuscule AA anastomoses may thus have a highflow resistance and thus fail to prevent the development of TAPS.
In conclusion, AA anastomoses in placentas with TAPS are rare.When present, the diameter of the AA anastomosis is small(�1 mm), subsequently inhibiting adequate compensatory mech-anisms and allowing development of TAPS.
Disclosure
All authors report no conflict of interest.
References
[1] Slaghekke F, Kist WJ, Oepkes D, Pasman SA, Middeldorp JM, Klumper FJ, et al.Twin anemia-polycythemia sequence: diagnostic criteria, classification, peri-natal management and outcome. Fetal Diagn Ther 2010;27:181e90.
[2] Lopriore E, Deprest J, Slaghekke F, Oepkes D, Middeldorp JM,Vandenbussche FP, et al. Placental characteristics in monochorionic twinswith and without twin anemia-polycythemia sequence. Obstet Gynecol 2008;112:753e8.
[3] Weingertner AS, Kohler A, Kohler M, Bouffet N, Hunsinger MC, Mager C, et al.Clinical and placental characteristics in four new cases of twin anemia-polycythemia sequence. Ultrasound Obstet Gynecol 2010;35:490e4.
[4] van Meir H, Slaghekke F, Lopriore E, van Wijngaarden WJ. Arterio-arterialanastomoses do not prevent the development of twin anemia-polycythemiasequence. Placenta 2010;31:163e5.
[5] Lopriore E, Slaghekke F, Middeldorp JM, Klumper FJ, van Lith JM, Walther FJ,et al. Of vascular anastomoses in monochorionic placenta using colored dye.J Vis Exp 2011;5:e3208.
[6] Lopriore E, van den Wijngaard JP, Middeldorp JM, Oepkes D, Walther FJ, vanGemert MJ, et al. Assessment of feto-fetal transfusion flow through placentalarterio-venous anastomoses in a unique case of twin-to-twin transfusionsyndrome. Placenta 2007;28:209e11.
[7] Lopriore E, Middeldorp JM, Oepkes D, Kanhai HH, Walther FJ,Vandenbussche FP. Twin anemia-polycythemia sequence in two mono-chorionic twin pairs without oligo-polyhydramnios sequence. Placenta 2007;28:47e51.
[8] Denbow ML, Cox P, Taylor M, Hammal DM, Fisk NM. Placental angioarchi-tecture in monochorionic twin pregnancies: relationship to fetal growth,fetofetal transfusion syndrome, and pregnancy outcome. Am J Obstet Gynecol2000;182:417e26.
[9] Umur A, van Gemert MJ, Nikkels PG. Monoamniotic-versus diamniotic-monochorionic twin placentas: anastomoses and twin-twin transfusionsyndrome. Am J Obstet Gynecol 2003;189:1325e9.
[10] Bajoria R, Wigglesworth J, Fisk NM. Angioarchitecture of monochorionicplacentas in relation to the twin-twin transfusion syndrome. Am J ObstetGynecol 1995;172:856e63.
[11] Umur A, van Gemert MJ, Nikkels PG, Ross MG. Monochorionic twins and twin-twin transfusion syndrome: the protective role of arterio-arterial anasto-moses. Placenta 2002;23:201e9.