Embed Size (px)
Citation preview

Arthrogryposis Multiplex Congenita
Harold Chen
ContentsSynonyms and Related Disorders . . . . . . . . . . . . . . . . . . 1
Genetics/Basic Defects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Clinical Features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Diagnostic Investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Genetic Counseling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Arthrogryposis multiplex congenita comprisesnonprogressive conditions characterized by mul-tiple joint contractures throughout the body atbirth. The term encompasses a very heteroge-neous group of disorders having the commonfeature of multiple congenital joint contractures.The overall prevalence of arthrogryposis isapproximately 1 in 3,000 live births (Hall 1985a,b; Fahy and Hall 1990).
Synonyms and Related Disorders
Amyoplasia; Distal arthrogryposis (distotarlardysmorphism, Freeman-Sheldon syndrome,Sheldon-Hall syndrome, Gordon syndrome,Hecht syndrome, Beals syndrome)
Genetics/Basic Defects
1. Major causes1. Arthrogryposis as a physical sign observed
in many specific clinical conditions:1. Single-gene defects2. Chromosomal abnormalities3. Known or unknown syndromes or
conditions4. Environmental effects: mutagenic
agents, mitotic abnormalities, toxicchemicals or drugs, hyperthermia, neu-romuscular blocking agents, and
H. Chen (*)Shriners Hospitals for Children, Shreveport, LA, USA
Perinatal and Clinical Genetics, Department of Pediatrics,LSU Health Sciences Center, Shreveport, LA, USAe-mail: [email protected]
# Springer Science+Business Media New York 2015H. Chen (ed.), Atlas of Genetic Diagnosis and Counseling,DOI 10.1007/978-1-4614-6430-3_16-2
1

mechanical immobilization (Swinyardand Bleck 1985)
2. Fetal akinesia due to fetal abnormalities:1. Neurogenic abnormalities: the most
common cause of arthrogryposis1. Meningomyelocele2. Anencephaly3. Hydranencephaly4. Holoprosencephaly5. Spinal muscular atrophy6. Cerebro-oculo-facio-skeletal
syndrome7. Marden-Walker syndrome
2. Muscular abnormalities: relatively rarecauses of arthrogryposis1. Congenital muscular dystrophies2. Congenital myopathies3. Intrauterine myositis4. Mitochondrial disorders
3. Connective tissue abnormalities in ten-don, bone, joint, or joint liningrestricting fetal movements, resulting incongenital contractures. Examplesinclude:1. Synostosis2. Lack of joint development3. Aberrant fixation of joints (as in dia-
strophic dysplasia and metatropicdwarfism)
4. Aberrant laxity of joints with disloca-tions (as in Larsen syndrome)
5. Aberrant soft tissue fixations (as inpopliteal pterygium syndrome)
6. Failure of normally developed tendonto attach to the appropriate placearound the joint or bone in someforms of distal arthrogryposis,resulting in abnormal lack of move-ment of the joints with secondarycontractures at birth
4. Mechanical limitations to movement.Limited space for fetal movement insidethe uterus may contribute to develop-ment of contractures. Examples include:1. Multiple births
2. Uterine structural abnormalities suchas bicornuate uterus
3. Umbilical cord wrapping4. Oligohydramnios in renal agenesis5. Early persistent leakage of amniotic
fluid5. Intrauterine vascular compromise
resulting in loss of nerve and musclefunction with development of fetalakinesia and secondary joint contrac-tures. Examples include:1. Severe maternal bleeding during
pregnancy2. Failed attempts at termination of
pregnancy (Hall 1996)3. Fetal akinesia due to maternal disorders,
examples include:1. Infections
1. Rubella2. Poliomyelitis
2. Drugs/chemicals1. Methocarbamol2. Alcohol3. Carbon monoxide poisoning
3. Trauma4. Vitamin deficiency5. Hyperthermia (e.g., prolonged sauna)6. Radiation7. Other maternal illnesses
1. Maternal autoantibodies2. Diabetes mellitus3. Myotonic dystrophy4. Maternal multiple sclerosis
2. Pathophysiology1. Joint development
1. Almost always normal during earlyembryogenesis
2. Fetal motion essential for normal devel-opment of joints and their contiguousstructures
2. Lack of fetal movement (Hall 1989)1. Causing extra connective tissue to
develop around the joint2. Resulting in fixation of the joint
2 H. Chen

3. Limiting movement that further aggra-vates the joint contracture
4. Contractures secondary to fetal akinesia:more severe in patients who are diag-nosed early in pregnancy and who expe-rience akinesia for longer periods of timeduring gestation
Clinical Features
1. Family history (Hall 1997, 2014):1. Presence of congenital contractures in the
family1. Affected siblings2. Other affected family members
2. Marked intrafamilial variability1. Mildly affected parent2. A parent with contractures early in
infancy3. Consanguinity
1. Increasing the chance that the parentswill both carry the same disease gene
2. Observed more frequently in familieswith rare recessive diseases than inthose with common recessive diseases
4. Increased parental age1. Some chromosomal abnormalities:
increasing dramatically with advancedmaternal age
2. Single-gene dominant mutations:increasing with advanced paternal age
5. History of previous miscarriages orstillbirths
6. Multiple consecutively affected child:consider maternal antibodies to fetalneurotransmitter
2. Pregnancy history (Hall 2014):1. Diminished fetal movement2. Infants born to mothers affected with the
following disorders:1. Myotonic dystrophy: A child who
inherits the gene and is severelyaffected with resistant contractures.
2. Myasthenia gravis and multiple sclero-sis: Children may be born with congen-ital contractures.
3. Diabetes.3. Maternal infections leading to CNS or
peripheral nerve destruction with second-ary congenital contractures:1. Rubella2. Rubeola3. Coxsackievirus4. Enterovirus5. Akabane
4. Maternal fever or hyperthermia causingcontractures due to abnormal nerve growthor migration
5. Exposure to teratogens leading todecreased fetal movement1. Additive drugs2. Alcohol3. Curare4. Methocarbamol5. Misoprostol6. Phenytoin7. Radiation8. Robaxin
6. Amniotic fluid volume1. Oligohydramnios, chronic leakage of
amniotic fluid: causes fetal constraintand secondary deformationalcontractures
2. Polyhydramnios, hydrops: indicatingfetal compromise
7. Uterine abnormalities1. Bicornuate uterus with a septum2. Uterine fibroid
8. Other maternal complications1. Toxemia2. Severe hypotension at critical time3. Severe hypoxia (e.g., carbon monoxide
poisoning) during pregnancy4. Abnormal fetal lies5. Threatened abortion6. Attempted termination7. Trauma such as trauma to the abdomen8. Early amniocentesis
3. Delivery history (Hall 2014)1. Breech or transverse fetal position.
1. Relatively common2. Usually normal length of gestation3. Induction of labor often prolonged
Arthrogryposis Multiplex Congenita 3

4. Fracture of a limb during traumaticdelivery in 5–10 % of cases
2. Abnormal placenta, membranes, or cordinsertion in case of amniotic bands or vas-cular compromise. The umbilical cordmay be shortened or wrapped around alimb, leading to compression.
3. Prematurity.4. Multiple births or twins.
1. Lack of movement due to uterinecrowding.
2. The death of one twin may lead to vas-cular compromise in theremaining twin.
4. Common physical characteristics1. Involved extremities
1. Fusiform or cylindrical in shape2. Thin subcutaneous tissue3. Absence of skin creases
2. Deformities1. Usually symmetric2. Severity increasing distally3. Hands and feet typically being the most
deformed3. Joint rigidity4. Associated joint dislocations, especially
the hips and, occasionally, the knees5. Muscles
1. Atrophy2. Absence
6. Sensation1. Usually intact2. Diminished or absent deep tendon
reflexes5. Contractures
1. Distal joints affected more frequently thanproximal joints
2. Types of contractures1. Flexion versus extension2. Limitation of movement (fixed
vs. passive vs. active)3. Complete fusion vs. ankylosis and soft
tissue contracture3. Intrinsically derived contractures
1. Frequently associated withpolyhydramnios
2. Symmetric contractures3. Accompanied by taut skin
4. Pterygia across joints5. Lack of flexion creases6. Recurrence risk and prognosis depen-
dent on etiology4. Extrinsically derived contractures
1. Associated with positional limb anom-alies, large ears, loose skin, and normalor exaggerated flexion creases
2. Excellent prognosis3. A low recurrence risk
6. Deformities (Hall 2014)1. Limb deformities
1. Pterygium (webbing)2. Shortening3. Cord wrapping4. Amniotic bands5. Compression (e.g., due to cord
wrapping)6. Absent patella7. Dislocated radial heads8. Dimples
2. Face deformities1. Asymmetry2. Flat nasal bridge3. Hemangioma4. Jaw deformities including
micrognathia and trismus3. Other deformities
1. Scoliosis/kyphosis (fixed or flexible)2. Genital deformities
1. Cryptorchidism2. Microphallus3. Lack of labia
3. Hernias1. Inguinal2. Umbilical
4. Other features of the fetal akinesiasequence1. Intrauterine growth retardation2. Pulmonary hypoplasia3. Craniofacial anomalies
1. Hypertelorism2. Cleft palate3. Depressed nasal tip4. High nasal bridge
4. Functional short gut with feedingproblems
5. Short umbilical cord
4 H. Chen

5. Absent or distorted crease abnormalitiesresulting from aberrant form or functionin early hand or foot development
7. Malformations (Hall 2014)1. Craniofacial malformations
1. CNS1. Structural malformations2. Seizures3. Mental retardation/intellectual
disability2. Skull
1. Craniosynostosis2. Asymmetry3. Microencephaly
3. Eyes1. Small and malformed eyes2. Corneal opacities3. Ptosis4. Strabismus
4. Palate1. High-arched2. Cleft3. Submucous cleft
2. Respiratory problems affecting lungfunction1. Tracheal and laryngeal clefts and
stenosis2. Hypoplasia or weak muscles of
diaphragm3. Limb malformations
1. Reduction anomalies2. Radioulnar synostosis3. Syndactyly4. Shortened digits
4. Skin/vasculature abnormalities1. Hemangiomas and cutis marmorata2. Cold and blue distal limbs
5. Cardiac problems1. Congenital heart defects2. Cardiomyopathy
6. Urogenital structural anomalies1. Kidneys2. Ureters3. Bladder
7. Nervous system problems1. Loss of vigor2. Lethargy
3. Slow, fast, or absent deep tendonreflexes
4. Sensory deficits8. Muscle malformations
1. Decreased muscle mass2. Soft muscle texture3. Fibrous bands4. Abnormal tendon attachments5. Muscle changing with time
8. Connective tissue abnormalities (Hall 2014)1. Skin webs (pterygia) across joints with
limitation of movement2. Skin dimples observed frequently over
joints where movement is limited3. Soft, doughy, thick, or extensible skin4. Decreased or increased subcutaneous fat5. Inguinal, umbilical, or diaphragmatic
hernias6. Thickness in joints7. Symphalangism8. Abnormalities in tendon attachment and
length9. Associated skin defects including scalp
defects, amniotic bands on limbs, andnail defects
9. Disorders with mainly limb involvement(Hall 1997; Bamshad et al. 2009)1. Amyoplasia (Hall et al. 1983a, b, 2014;
Sarwark et al. 1990; Sells et al. 1996;Bevan et al. 2007)1. The most common type of
arthrogryposis seen in clinical practiceand constitutes about one third of cases
2. Incidence: about 1 in 10,000 live births3. A sporadic condition, not observed in
siblings or offspring (recurrence risknot increased)
4. Characterized by typical and symmetriccongenital, rigid contractures of thelimbs
5. Internally rotated and adductedshoulders
6. Fixed extended elbows7. Pronated forearms8. Flexed wrists and fingers9. A severe talipes equinovarus deformity10. Gracile, osteoporotic long bones
Arthrogryposis Multiplex Congenita 5

11. Muscles: hypoplastic (markeddecrease in limb muscle mass) andusually replaced by fibrous and fattytissue
12. Normal intelligence2. Distal arthrogryposes: Bamshad classifica-
tion (Hall et al. 1982a; Bamshedet al. 1996; Hall 2014)1. Type 1A (distotarlar dysmorphism)
1. An autosomal dominant disorder2. Medially overlapping fingers3. Tightly clenched fists at birth4. Ulnar deviation of fingers and
camptodactyly in adults5. Positional foot contractures6. Usually normal intelligence7. Caused by mutations in TPM2,
MYBPC1, TNN12, and MYH32. Type 2A (Freeman-Sheldon syndrome,
also known as whistling facesyndrome)1. An autosomal dominant disorder2. A mask-like face with a small
mouth, giving a whistling faceappearance
3. Deep-set eyes4. Small nose with a broad nasal bridge5. Epicanthal folds6. Strabismus7. High-arched palate8. Small tongue9. AnH-shaped cutaneous dimpling on
the chin10. Flexion of fingers11. Equinovarus feet with contracted
toes12. Kyphoscoliosis13. Caused by MYH3 mutation
3. Type 2B (Sheldon-Hall syndrome)(Toydemir et al. 2006; Toydemir andBamshad 2009)1. An autosomal dominant disorder2. Contractures of the distal joints of
the limbs3. Triangular face4. Down-slanting palpebral fissures5. Small mouth6. High-arched palate
7. Caused by mutations in eitherMYH3, TNNI2, or TNNT3 (�50 %of cases)
4. Type 3 (Gordon syndrome)1. Short stature (90 %)2. Cleft palate3. Bifid uvula4. Epicanthal folds5. Congenital ptosis6. Short neck7. Camptodactyly8. Caused by PIEZO2 mutation
5. Type 4 (may include Goodmansyndrome)1. Scoliosis2. Finger contractures
6. Type 51. Ophthalmoplegia (limited ocular
motility)2. Ptosis3. Finger contractures4. Caused by PIEZO2 (AD) or ECEL1
(AR) mutations7. Type 6
1. Sensorineural hearing loss2. Finger contractures3. Caused by FGFR3 mutation
8. Type 7 (Hecht syndrome, KentuckyDutch syndrome)1. Trismus pseudocamptodactyly2. Inability to fully open mouth3. Facultative camptodactyly4. Caused by MYH8 mutation
9. Type 8 (autosomal dominant multiplepterygium syndrome)1. Multiple pterygium2. Finger contractures
10. Type 9 (Beals syndrome, congenitalcontractural arachnodactyly)1. An autosomal dominant disorder2. Joint contractures3. A long, thin body builds4. Crumpling ears5. Lacking cardiovascular and ocular
abnormalities of Marfan syndrome6. Caused by fibrillin 2 mutation
11. Type 10 (congenital plantarcontractures)
6 H. Chen

3. Bony fusion likely to be confused witharthrogryposis1. Symphalangism (e.g., fusion of
phalanges)2. Coalition (e.g., fusion of the carpals
and tarsal bones)3. Synostosis (e.g., fusion of long bones)
4. Other associated syndromes andconditions1. Absence of dermal ridges2. Absence of distal interphalangeal (DIP)
joint creases3. Amniotic bands4. Antecubital webbing5. Camptodactyly6. Congenital clasped thumbs7. Familial impaired pronation and supi-
nation of forearm8. Humeroradial synostosis9. Liebenberg syndrome10. Nail-patella syndrome11. Nievergelt-Pearlman syndrome12. Poland anomaly13. Radioulnar synostosis14. Tel-Hashomer camptodactyly
10. Disorders with involvement of limbs andother body parts (Hall 1997)1. Multiple pterygium syndrome (Chen
et al. 1980)1. Autosomal recessive type: character-
ized by multiple joint contractureswith marked pterygia, dysmorphicfacies (flat, sad, motionless facialappearance), and cervical vertebralanomalies
2. Autosomal dominant type: character-ized by multiple pterygia with or with-out mental retardation
2. Multiple pterygium syndrome (pterygiawith flexion contractures) associated withscoliosis, cleft palate, and malignanthyperthermia
3. Multiple pterygium syndrome, Escobartype (Escobar et al. 1978)1. Webbing of the neck that increases with
age2. Webbing of the knees and elbows that
develops before adolescence
3. Multiple joint contractures4. Lumbar lordosis
4. Lethal multiple pterygium syndrome(Chen et al. 1983, 1984; Hall 1984c; Porter1995; Chen 2015)1. An autosomal recessive disorder2. Characteristic features
1. Early lethality2. Hydrops fetalis3. Cystic hygroma4. Dysmorphic facies (hypertelorism,
markedly flattened nasal bridgewith hypoplastic nasal alae, cleftpalate, micrognathia, and low-setears)
5. Marked webbing and flexion con-tractures of multiple joints
6. Short neck7. Small chest8. Hypoplastic lungs
3. Classification by Hall (1984a, b, c) andEntezami et al. (1998)1. Type I (Gillin-Pryse-Davis syn-
drome): multiple pterygia, pulmo-nary hypoplasia, genital anomalies,and marked flexed extremities witha reduced muscle mass
2. Type II (Chen syndrome) (Chenet al. 1984): multiple pterygia,hygroma colli, facial anomalies,undermodeled long bones, cartilagi-nous fusion of joints and bonyfusion of the spinous processes ofthe vertebrae, polyhydramnios,hypoplastic lungs and heart, and dia-phragmatic hernia
3. Type III (van Regemorter syn-drome): multiple pterygia, pulmo-nary hypoplasia, facial anomalies,thin extremities with reduced mus-cle mass, and fusions of the longtubular bones
4. Type IV (Herva syndrome): multiplepterygia, degeneration of the ante-rior horn cells of the spinal cord,and observed particularly in Finland
5. Popliteal pterygium syndrome1. An autosomal dominant disorder
Arthrogryposis Multiplex Congenita 7

2. Popliteal webs3. Cleft lip or palate4. Webs in the mouth5. Unusual nails
6. Lethal popliteal pterygium syndrome(Bartsocas-Papas syndrome)1. An autosomal recessive disorder2. Severe webs across the knee3. Associated with facial clefting and
fused digits (synostosis of the handand foot bones) in the newborn period
4. Usually lethal7. Osteochondrodysplasias known to be
associated congenital contractures1. Camptomelic dysplasia2. Conradi-H€unermann
(chondrodysplasia punctata)3. Diastrophic dysplasia4. Focal femoral dysplasia5. Geleophysic syndrome6. Kniest dysplasia7. Metaphyseal dysplasia, Jansen type8. Metatropic dysplasia9. Larsen dysplasia10. Nail-patella syndrome11. Oculodentodigital syndrome12. Orocraniodigital syndrome13. Osteogenesis imperfecta type II14. Otopalatodigital syndrome15. Parastremmatic dysplasia16. Perinatal lethal osteogenesis
imperfecta17. Pfeiffer syndrome18. Saul-Wilson syndrome19. Synspondylism20. Spondyloepiphyseal dysplasia
congenita21. Otospondylomegaepiphyseal
dysplasia8. Other associated syndromes and
conditions1. Hand muscle wasting and sensorineural
deafness2. Holt-Oram syndrome3. Kuskokwim syndrome4. Leprechaunism5. Megalocornea with multiple skeletal
anomalies
6. Möbius syndrome7. Nemaline myopathy8. Ophthalmomandibulomelic dysplasia9. Prader-Willi habitus/osteoporosis/hand
contractures10. Pseudothalidomide syndrome11. Puretic-Murray syndrome12. Sacral agenesis13. Schwartz-Jampel syndrome14. Sturge-Weber syndrome15. Tuberous sclerosis16. VATER (vertebral defects, imperfo-
rate anus, tracheoesophageal fistula,radial and renal dysplasia) complex
17. Weaver syndrome18. Winchester syndrome19. X-trapezoidocephaly with midfacial
hypoplasia and cartilageabnormalities
11. Disorders with limb involvement and CNSdysfunction (Hall 1997)1. Associated chromosome abnormalities.
1. Sex chromosome anomalies (45,X, 47,XXY/48,XXXY, 49,XXXXX, 49,XXXXY)
2. Autosomal trisomies (4p, 8, 8 mosai-cism, 9, 9q, 10p, 10q, 11q, 13, 14,15, 18, 21)
3. Other chromosome anomalies2. Cerebro-oculo-facio-skeletal syndrome.
1. A common lethal condition2. Contractures3. Brain anomalies4. Dysmyelination5. Microphthalmia6. Cataracts7. Renal anomalies8. Other visceral anomalies
3. Neu-Laxova syndrome.1. A lethal autosomal recessive disorder2. Dramatic contractures3. Intrauterine growth retardation4. Microcephaly5. Open eyes6. Tight ichthyotic skin7. Severe CNS anomalies
4. Restrictive dermopathy (Verloeset al. 1992).
8 H. Chen

1. A lethal autosomal recessive disorder2. Contractures and failure of fetal skin to
grow normally restricting fetal move-ment and leading to secondarycontractures
5. Pena-Shokeir phenotype (Chenet al. 1980; Moerman and Fryns 1990):Phenotype is caused by fetal akinesiarather than a specific syndrome.1. Short, fixed limbs2. Pulmonary hypoplasia3. Intrauterine growth retardation4. Polyhydramnios5. Short umbilical cord6. Unusual craniofacies
12. Other associated syndromes and conditions1. Adducted thumbs2. Bowen-Conradi syndrome3. C syndrome4. Congenital myotonic dystrophy5. Congenital myasthenia gravis6. Faciocardiomelic syndrome7. Fetal alcohol syndrome8. FG syndrome9. Marden-Walker syndrome10. Meckel syndrome11. Meningomyelocele12. Mietens-Weber syndrome13. Miller-Dieker syndrome14. Neu-Laxova syndrome15. Neurofibromatosis16. Popliteal pterygium with facial clefts17. Potter syndrome18. Pseudotrisomy 1819. Spinal muscular atrophy20. Syndrome of cloudy cornea, diaphrag-
matic defects, and distal limb deformities21. Syndrome of craniofacial and brain
anomalies and intrauterine growthretardation
22. Syndrome of cryptorchidism, chestdeformity, and contractures
23. Toriello-Bauserman syndrome24. Walker-Warburg syndrome
25. X-linked lethal arthrogryposis (Hallet al. 1982b)
26. Zellweger syndrome13. Prognosis (Hall 1986)
1. Poor prognosis for ventilator-dependentneonates (Bianchi and Van Marter 1994)
2. Prenatal factors that potentially predictrespiratory insufficiency1. Decreased fetal movements2. Polyhydramnios3. Micrognathia4. Thin ribs5. Decreased fetal movement often
resulting in delayed developmentalmilestones
3. Skeletal changes secondary to the originaldeformities1. Scoliosis2. Deformed carpal and tarsal bones3. Under growing of limbs after
longstanding contractures4. External genitalia often abnormal (e.g.,
cryptorchidism, absent labia majora)because of abnormal hip position
4. Intrinsically or extrinsically deriveddefects1. Extrinsically derived contractures: an
excellent prognosis2. Intrinsically derived contractures: a
prognosis dependent on etiology5. Prognosis depending on the condition’s
natural history1. Developmental landmarks (attainment
of motor, social, and languagemilestones)
2. Growth of affected limbs3. Progression of contractures4. CNS damage (lethal, stable,
improving)5. Asymmetry of contractures (improv-
ing, worsening)6. Changes in trunk or limbs7. Intellectual ability8. Socialization
Arthrogryposis Multiplex Congenita 9

6. Prognosis depending on the patient’sresponse to therapy1. Spontaneous improvement2. Response to physical therapy3. Response to casting4. Types of surgery at appropriate time5. Development of motor strength propor-
tionate to limb size
Diagnostic Investigations
1. Laboratory evaluation (Hall 1981, 2014)1. Laboratory tests, in general, are not useful.2. Creatine phosphokinase (CPK) levels when
the following conditions are present:1. Generalized weakness2. Doughy or decreased muscle mass3. Progressive worsening
3. Viral cultures for an infectious process(intrauterine growth retardation, eyeinvolvement, and hepatosplenomegaly)
4. Immunoglobulin M levels and specific viraltiters (e.g., coxsackievirus, enterovirus,Akabane virus) in the newborn for intrauter-ine infection
5. Maternal antibodies to neurotransmitters inthe infant indicating myasthenia gravis orrecurrent affected pregnancies withoutdiagnosis
6. Video of movement including facial, rangeof movement, and strength repeat at regularintervals
7. Cytogenetic study/comparative genomichybridization (CGH) array indicated in thefollowing situations:1. Multiple organ or system involvement2. Presence of CNS abnormalities, such as
microcephaly, mental retardation, leth-argy, degenerative changes, or eyeanomalies
3. Streaky or segmental involvement4. Fibroblast chromosome study if lympho-
cyte chromosomes are normal and thepatient has mental retardation/intellec-tual disability without diagnosis
5. Consider exome studies if familyavailable
8. Nuclear DNA mutation analysis to identifycertain disorders1. Exome sequencing identifies aa domi-
nant TNNT3 mutations in a large familywith distal arthrogryposis (Dalyet al. 2014)
2. Spinal muscular dystrophy9. Mitochondrial mutation analysis to identify
certain disorders, such as mitochondrialmyopathy
10. Spinal muscular atrophy (SMN) DNAtesting if accompanying hypotonia andintellectual disability
11. Metabolic screening if presence oforganomegaly
2. Imaging studies1. Patient’s photographs
1. To document the extent of deformities(range of motion and position ofarthrogryposis)
2. To assess progress during treatment2. Radiographs to evaluate the following skel-
etal and joint abnormalities:1. Bony abnormalities (e.g., gracile bones,
fusions, extra or missing carpals, andtarsals)
2. Disproportionately short stature (i.e.,skeletal dysplasias)
3. Scoliosis4. Ankylosis5. Absence of patella6. Humeroradial synostosis7. Dislocations (hips, radial head, patella)
3. Ultrasonography1. To evaluate the CNS and other viscera
for anomalies2. To establish potential muscle tissue
4. CTscan to evaluate the CNS and the musclemass
5. MRI to evaluate CNS (brain and spinalcord) and muscle mass obscured bycontractures
6. Ophthalmological evaluation for opacityand retinal degeneration
3. Histologic studies (Banker 1985, 1986)1. Neurogenic types
10 H. Chen

1. Muscle fiber type predominance or dis-proportion is the most common neuro-genic abnormality in arthrogryposis(26 %). These are nonspecificalterations.
2. Dysgenesis of the motor nuclei of thespinal cord and brainstem causes thereplacement of fasciculi of muscle fibersby small muscle fibers and adipose tis-sue. Examples include Pierre Robin syn-drome and Möbius syndrome.
3. Dysgenesis of the CNS: the second mostcommon neurogenic abnormality inarthrogryposis (23 %), with disorganiza-tion and decrease in neurons of the cor-tex and motor nuclei of the brainstemand spinal cord. Clinical syndromeswith this abnormality include trisomy18, partial deletion of the long arm ofchromosome 18 syndrome, andZellweger syndrome.
4. Dysgenesis of the anterior horn, anothercommon neurogenic abnormality inarthrogryposis.
5. Spinal muscular atrophy (e.g., Werdnig-Hoffmann disease): another neurogenicabnormality in arthrogryposis.
2. Myopathic types1. Central core disease: a form of
arthrogryposis in which the central por-tion of each muscle fiber contains a zonein which oxidative enzyme activity isabsent.
2. Nemaline myopathy indicated by abnor-mal thread-like structures in musclecells. In type I nemaline myopathy,nemaline rods are present. In type II,the number of fibers with central nucleiis increased.
3. Congenital muscular dystrophy indi-cated by muscle fibers that demonstratea rounded configuration and conspicu-ous variation in diameter. Perimysialand endomysial connective tissues areincreased markedly.
4. Mitochondrial cytopathy indicated bynumerous ragged red fibers on musclebiopsy. It is associated with CNS
abnormalities consistent with mitochon-drial disease (Gordon 1998).
5. Myoneural junction abnormality (e.g.,congenital myasthenia gravis): anothermyopathic type of arthrogryposis.
4. Procedures1. Eye examination for opacities and retinal
degeneration.2. Skin biopsy for culture of fibroblasts to be
used for chromosome analysis and meta-bolic studies.
3. Muscle biopsy:1. Probably the most important diagnostic
procedure (Thompson and Bilenker1985). It should be included in all autop-sies and at time of surgery.
2. Do biopsy earlier and examine mito-chondria, if elevated CPK or unusualmuscle response present.
3. Distinguish myopathic from neuropathicconditions by obtaining muscle speci-mens from normal and affected areas.
4. Special histopathologic and electronmicrographic studies to evaluate fattyand connective tissue replacement ofmuscle fibers and variations in fibersize, such as decreased fiber diameter.All are nonspecific signs of muscleatrophy.
4. Electromyography (EMG) (Södergårdet al. 1997) in normal and affected areasuseful in differentiating neurogenic andmyopathic causes (Gordon 1998).
5. Nerve conduction tests to measure conduc-tion velocities in motor and sensory nerves.These should be performed when a periph-eral neuropathy is suspected.
6. An autopsy to investigate the following:1. CNS (i.e., brain neuropathology)2. Spinal cord (number and size of anterior
horn cells, presence or absence of tractsat various levels)
3. Ganglia and peripheral nerves4. Eye (i.e., neuropathology)5. Muscle tissue from different muscle
groups (i.e., electron microscopy andspecial stains)
6. Fibrous bands replacing muscle
Arthrogryposis Multiplex Congenita 11

7. Tendon attachments8. Other visceral anomalies,
malformations, deformations, anddisruptions
Genetic Counseling
1. Recurrence risk: Recurrence risk depends onwhether the contractures are extrinsically orintrinsically derived. Extrinsically derivedcontractures have a low recurrence risk, whilethe recurrence risk for intrinsically derivedcontractures depends on etiology.Arthrogryposis may be inherited in the follow-ing ways with different recurrence risks:1. Patient’s sib
1. Autosomal recessive: 25 %2. Autosomal dominant: not increased
unless a parent is affected or havinggonadal mosaicism
3. X-linked recessive: 50 % of male sibsaffected if the mother is a carrier
2. Patient’s offspring1. Autosomal recessive: not increased
unless the spouse is also a carrier.2. Autosomal dominant: 50 %.3. X-linked recessive: All daughters of
affected males will be carriers. All sonsof an affected male will be normal.
3. Multifactorial: Combined effects of multi-ple genes and environmental factors causemultifactorial traits. For most multifactorialdiseases, empirical risks (risks based ondirect observation of data) have beenderived. For example, empirical recurrencerisks of neural tube defects for siblings of anaffected individual range from 2% to 5% inmost populations.
4. Mitochondrial: A small but significant num-ber of diseases are caused by mitochondrialmutations. Because of the unique propertiesof mitochondria, these diseases displaycharacteristic modes of inheritance (i.e.,inherited exclusively through the maternalline) with wide phenotypic variability. Onlyfemales can transmit the disease mutation to
their offspring (e.g., distal type IIBarthrogryposis).
5. Sporadic: For those families in which aspecific diagnosis cannot be made, theempiric recurrence risk to unaffected par-ents of an affected child, or to the affectedindividual with arthrogryposis, is about3–5 %.
2. Prenatal diagnosis (Bendon et al. 1987; Batyet al. 1988; Hageman et al. 1988; Dimitrakiet al. 2011):1. Prenatal ultrasonography to detect the
following:1. Diminished fetal movement (main man-
ifestation shared by various conditionswith congenital contractures)
2. Joint contractures (bilateral fixed flexiondeformities of the hands, elbows, shoul-ders, hips and knees, or talipes)
3. Detection of subcutaneous edema (fetalhydrops)
4. Cystic hygroma5. Increased nuchal translucency (Madazli
et al. 2002)6. Abnormal fetal lie7. Polyhydramnios or oligohydramnios8. Other associated anomalies (e.g.,
distended bladder in early urethralobstruction sequence; microcephaly,hydrocephaly, or hydranencephaly in“cerebral dysgenesis”-induced congeni-tal contractures)
2. Chromosome analysis by amniocentesis orCVS for chromosome disorders
3. Molecular genetic analysis for certaingenetic disorders with demonstrablemutations
3. Management (Shriner’s Manual) (McCall andGates, 1999, Personal communication):1. No completely successful approach to
treatment2. Overall goals
1. Proper alignment of the lower limbs2. Upper limb function for self-care
3. Early vigorous physical therapy to stretchcontractures1. To improve joint motion2. To avoid muscle atrophy
12 H. Chen

3. Excellent functional outcome in patientswith amyoplasia or distal arthrogryposis
4. May be harmful in diastrophic dysplasiabecause it may lead to joint ankylosis
5. Frequent recurrence of deformities fol-lowing stretching, often requires surgery
4. Splinting combined with physical therapy1. Preferable to continuous casting2. Night splinting after surgical procedures
indicated to maintain increased range ofmotion
5. Feeding assistance and intubation needed inpatients with severe trismus
6. Specific joint problems1. Should be addressed with regard to treat-
ment of other joints and the goals for thepatient
2. Early soft tissue surgery withosteotomies when the growth iscompleted
3. Tenotomies accompanied bycapsulotomies in soft tissue releaseprocedures
4. Long-term bracing and assistive devicesusually needed
7. Feet1. A rigid talipes equinovarus deformity:
the most common deformity (Guideraand Drennan 1985)
2. Bilateral talectomy in the managementof bilateral rigid clubfeet (Letts 1999)
3. Goal of treatment: a plantigrade,braceable foot
8. Knees (Thomas et al. 1985; Murray andFixsen 1997)1. Goal of treatment: an extended knee for
ambulation2. Fixed flexion knee deformities more
common than fixed extension kneedeformities and more resistant totreatment
9. Hips (Huurman and Jacobsen 1985; Staheliet al. 1987)1. Hip surgery follows foot and knee sur-
gery, especially in the presence of kneeextension deformities.
2. Hip surgery in patients younger than1 year to facilitate ambulation. In some
patients with bilateral hip dislocationsand extremely mobile hips, open reduc-tion may be attempted.
3. A one-stage open reduction and varusshortening femoral derotationalosteotomy for all unilateral hip disloca-tions and those bilateral hip dislocationsthat have a less severe generalizedinvolvement and an aggressive tractionprogram with appropriate soft tissuereleases during the neonatal period forpatients with subluxation and/or markedlimitation of motion of the hip (St. Clairand Zimbler 1985)
10. Upper extremities (Bennett et al. 1985;Williams 1985)1. Treatment involves development of
self-help skills (e.g., feeding andtoileting) (Bayne 1985) and mobilityskills (e.g., pushing out of chair andusing crutches).
2. Consider overall function of the entireextremity rather than function of theindividual joints in evaluating theupper extremities.
3. Consider upper extremity surgery untilthe patient is older than 5–6 years.
4. Emphasis is placed on evaluation of thedisability by repeated testing and obser-vation. In many cases, the deformitieswill be accepted and improvements infunction will be gained by orthoses orattention to details of seating, dressing,and toileting.
5. Surgery is indicated in some cases,especially at the elbow, to obtain mobil-ity, flexor power, or both. Arthrodesingthe wrist is also useful in some cases.
6. When surgery is indicated, it is oftendesirable to rearrange all three levels –shoulder, elbow, and wrist.
11. Elbows1. Goals: passive or active flexion capa-
bility (feeding arm) and extension capa-bility (toilet arm) (Axt et al. 1997).
2. Achieve elbow mobility beforecorrecting a wrist deformity becausethe elbow is crucial to hand function.
Arthrogryposis Multiplex Congenita 13

12. Wrists1. Stretching and splinting for the major
wrist deformity (flexion with ulnardeviation)
2. Proximal row carpectomy with or with-out fusion for a severe deformity
13. Fingers1. Passive stretching and splinting for
minimal to moderate flexiondeformities
2. Soft tissue releases with proximalinterphalangeal joint fusions for moresevere deformities
3. Thumb-in-palm deformity to becorrected to provide opposition-improved grasp
14. Spine1. The spine affected in about one third of
patients.2. Scoliosis beginning early and
progressing to become a long, severe,rigid, C-shaped curve. This curveresponds poorly to orthoses, as it isprogressive.
3. Curves greater than 35�: treated withspinal fusion and instrumentation.
15. Complications1. Anesthesia: difficult to administer
because vascular access often isrestricted.
2. Intubation: posing problems forpatients with a small underdevelopedjaw, limited movement of the temporo-mandibular joint, or a narrow airway.
3. Osseous hypoplasia associated withdecreased mechanical use in develop-ing bone: prone to fracture at multiplesites. Multiple perinatal fractures havebeen observed in osteopenic bones.
16. Feeding and toileting devices for a childwith arthrogryposis (Hall and Hammock1979)
17. Summary of the 2nd International Sympo-sium on Arthrogryposis, St. Petersburg,Russia, September 17–19, 2014 (Hallet al. 2015)
1. Ponseti type casting should begin by1–2 months of age for clubfeet, andknee dislocations should be casted.
2. Early imaging of muscle by ultrasoundor MRI: important as a baseline fordetermination of best therapy andlong-term outcomes, for instance, as towhether or not walking can beanticipated.
3. Reports of dramatic improvement inthe upper limbs of individuals withamyoplasia, utilizing vigorous physicaltherapy and muscle transfers.
4. Orthotics for adults with arthrogryposisfor stabilization during walk and a car-bon spring built into an ankle-footorthosis may function as muscle whenmuscles are absent or very weak.
5. Use of the “8-plate”: provides tempo-rary hemiepiphysiodesis with a smallplate and screws. It has revolutionizedthe treatment of malaligned knees in theolder child, since it is less traumaticthan osteotomies and spares muscletissue.
6. Growing rods: very useful in individ-uals with arthrogryposis and scoliosis.
7. Adults with arthrogryposis should keepas active as possible, since immobiliza-tion in adults with arthrogryposis leadsto disproportionate weakness and mus-cle atrophy.
18. Physical activity1. Limited because of existing orthopedic
problems2. Passive motion therapy for infants with
arthrogryposis (Palmer et al. 1985).3. As a group, patients cope well socially
and participate in social activitiescorresponding to their needs.
4. More restricted walking in patientswith flexion contractures of the lowerextremities than in those with extensioncontractures. Flexion contractures ofthe hips severely impair walkingability.
14 H. Chen

5. Contracture of the elbow causing a sig-nificant degree of disability in handfunction.
6. Impossible to use crutches in patientswith upper extremity involvementassociated with severe spinaldeformity.
7. Dependent on help from other people toa higher degree in patients with moresevere joint involvement than thosewith less severe joint involvement.
8. Independent living with productivelives for most children with normalintelligence despite severe handicaps.However, many remain partiallydependent on others, such as parents,relatives, and government subsidy.Dependency is related more closely topersonality, education, and overall cop-ing skills than to the degree of physicaldeformity.
9. Good family support, a proper educa-tional environment, and promotion ofindependence at an early age: requiredto achieve maximal function in additionto appropriate surgical correction(Carlson et al. 1985; Hahn 1985).
References
Axt, M. W., Niethard, F. U., Doderlein, L., et al. (1997).Principles of treatment of the upper extremity inarthrogryposis multiplex congenita type I. Journal ofPediatric Orthopedics, 6, 179–185.
Bamshad, M., van Heest, A. E., & Pleasure, D. (2009).Arthrogryposis: A review and update. The Journal ofBone Joint Surgery American, 91, 40–46.
Bamshed,M., Jorde, L. B., & Carey, J. C. (1996). A revisedand extended classification of the distal arthrogryposes.American Journal of Medical Genetics, 65, 277–281.
Banker, B. Q. (1985). Neuropathologic aspects ofarthrogryposis multiplex congenita.Clinical Orthopae-dics, 194, 30–43.
Banker, B. Q. (1986). Arthrogryposis multiplex congenita:Spectrum of pathologic changes. Human Pathology,17, 656–672.
Baty, B. J., Cubberley, D., Morris, C., et al. (1988). Prena-tal diagnosis of distal arthrogryposis. American Jour-nal of Medical Genetics, 29, 501–510.
Bayne, L. G. (1985). Hand assessment and management ofarthrogryposis multiplex congenita.Clinical Orthopae-dics, 194, 68–73.
Bendon, R., Dignan, P., & Siddiqi, T. (1987). Prenataldiagnosis of arthrogryposis multiplex congenita. Jour-nal of Pediatrics, 111, 942–947.
Bennett, J. B., Hansen, P. E., Granberry, W. M.,et al. (1985). Surgical management of arthrogryposisin the upper extremity. Journal of Pediatric Orthope-dics, 5, 281–286.
Bevan, W. P., Hall, J. G., Bamshad, M., et al. (2007).Arthrogryposis multiplex congenita (amyoplasia): Anorthopaedic perspective. Journal of Pediatric Orthope-dics, 27, 594–600.
Bianchi, D. W., & VanMarter, L. J. (1994). An approach toventilator-dependent neonates with arthrogryposis.Pediatrics, 94, 682–686.
Carlson, W. O., Speck, G. J., Vicari, V., et al. (1985).Arthrogryposis multiplex congenita. A long-term fol-low-up study. Clinical Orthopaedics, 194, 115–123.
Chen, H. (2015). Arthrogryposis. Medscape reference.Updated 2 Mar 2015. Available at: http://emedicine.medscape.com/article/941917-overview
Chen, H., Chang, C. H., Misra, R. P., et al. (1980). Multiplepterygium syndrome. American Journal of MedicalGenetics, 7, 91–102.
Chen, H., Blumberg, B., & Immken, L. (1983). The Pena-Shokeir syndrome: Report of five cases and furtherdelineation of the syndrome. American Journal of Med-ical Genetics, 16, 213–224.
Chen, H., Immken, L., Lachman, R., et al. (1984). Syn-drome of multiple pterygia, camptodactyly, facialanomalies, hypoplastic lungs and heart, cystichygroma, and skeletal anomalies: Delineation of anew entity and review of lethal forms of multiple pte-rygium syndrome. American Journal of MedicalGenetics, 17, 809–826.
Daly, S. B., Shah, H., O’Sullivan, J., et al. (2014). Exomesequencing identifies a dominant TNNT3 mutation in alarge family with distal arthrogryposis. MolecularSyndromology, 5, 218–228.
Dimitraki, M., Tsikouras, P., Bouchlariotou, S.,et al. (2011). Prenatal assessment of arthrogryposis. Areview of the literature. The Journal of Maternal-Fetaland Neonatal Medicine, 24, 32–36.
Entezami, M., Runkel, S., Kunze, J., et al. (1998). Prenataldiagnosis of a lethal multiple pterygium syndrome typeII. Case report. Fetal Diagnosis and Therapy, 13,35–38.
Escobar, V., Bixler, D., Gleiser, S., et al. (1978). Multiplepterygium syndrome. American Journal of Diseases ofChildren, 132, 609–611.
Fahy, M. J., & Hall, J. G. (1990). A retrospective study ofpregnancy complications among 828 cases ofarthrogryposis. Genetic Counseling, 1, 3–11.
Gordon, N. (1998). Arthrogryposis multiplex congenita.Brain & Development, 20, 507–511.
Arthrogryposis Multiplex Congenita 15

Guidera, K. J., & Drennan, J. C. (1985). Foot and ankledeformities in arthrogryposis multiplex congenita.Clinical Orthopaedics, 194, 93–98.
Hageman, G., Ippel, E. P. F., Beemer, F. A., et al. (1988).The diagnostic management of newborns with congen-ital contractures: A nosologic study of 75 cases. Amer-ican Journal of Medical Genetics, 30, 883–904.
Hahn, G. (1985). Arthrogryposis. Pediatric review andhabilitative aspects. Clinical Orthopaedics, 194,104–114.
Hall, J. G. (1981). An approach to congenital contractures(arthrogryposis). Pediatric Annals, 10, 15–26.
Hall, J. C. (1984a). An approach to research on congenitalcontractures. Birth Defects Original Article Series, 20(6), 8–30.
Hall, J. G. (1984b). Craniofacial development inarthrogryposis (congenital contractures). Birth DefectsOriginal Article Series, 20, 99–111.
Hall, J. G. (1984c). The lethal multiple pterygium syn-dromes. American Journal of Medical Genetics, 17,803–807.
Hall, J. G. (1985a). Genetic aspects of arthrogryposis.Clinical Orthopaedics, 194, 44–53.
Hall, J. G. (1985b). In utero movement and use of limbs arenecessary for normal growth: A study of individualswith arthrogryposis. Progress in Clinical and Biologi-cal Research, 200, 155–162.
Hall, J. G. (1986). Diagnostic approaches and prognosis inarthrogryposis (congenital contractures). Pathologica,78, 701–708.
Hall, J. G. (1989). Arthrogryposis. American Family Phy-sician, 39, 113–119.
Hall, J. G. (1996). Arthrogryposis associated with unsuc-cessful attempts at termination of pregnancy. AmericanJournal of Medical Genetics, 63, 293–300.
Hall, J. G. (1997). Arthrogryposis multiplex congenita:Etiology, genetics, classification, diagnostic approach,and general aspects. Journal of Pediatric Orthopedics.Part B, 6, 159–166.
Hall, J. G. (2014). Arthrogryposis (multiple congenitalcontractures): Diagnostic approach to etiology, classi-fication, genetics, and general principles. AmericanJournal of Medical Genetics, 57, 464–472.
Hall, K.W., & Hammock, M. (1979). Feeding and toiletingdevices for a child with arthrogryposis. American Jour-nal of Occupational Therapy, 33, 644–647.
Hall, J. G., Reed, S. D., & Greene, G. (1982a). The distalarthrogryposes: Delineation of new entities-review andnosologic discussion. American Journal of MedicalGenetics, 11, 185–239.
Hall, J. G., Reed, S. D., Scott, C. I., et al. (1982b). Threedistinct types of X-linked arthrogryposis seen in 6 fam-ilies. Clinical Genetics, 21, 81–97.
Hall, J. G., Reed, S. D., & Driscoll, E. P. (1983a). PartI. Amyoplasia: A common, sporadic condition withcongenital contractures. American Journal of MedicalGenetics, 15, 571–590.
Hall, J. G., Reed, S. D., McGillivray, B. C., et al. (1983b).Part II. Amyoplasia: Twinning in amyoplasia-a specific
type of arthrogryposis with an apparent excess of dis-cordantly affected identical twins. American Journal ofMedical Genetics, 15, 591–599.
Hall, J. G., Aldinger, K. A., & Tanaka, K. I. (2014).Amyoplasia revisited. American Journal of MedicalGenetics. Part A, 164A, 700–730.
Hall, J. G., Ogranovich, A., Ponten, A., et al. (2015). Sum-mary of the 2nd international symposium onarthrogryposis, St. Petersburg, Russia, September17–19, 2014. American Journal of Medical Genetics.Part A, 167A, 1193–1195.
Huurman, W. W., & Jacobsen, S. T. (1985). The hip inarthrogryposis multiplex congenita.Clinical Orthopae-dics, 194, 81–86.
Letts, M. (1999). The role of bilateral talectomy in themanagement of bilateral rigid clubfeet. The AmericanJournal of Orthopedics, 28, 106–110.
Madazli, R., T€uys€uz, B., Aksoy, F., et al. (2002). Prenataldiagnosis of arthrogryposis multiplex congenita withincreased nuchal translucency but without any under-lying fetal neurogenic or myogenic pathology. FetalDiagnosis and Therapy, 17, 29–33.
Moerman, P., & Fryns, J. P. (1990). The fetal akinesiadeformation sequence. A fetopathological approach.Genetic Counseling, 1, 25–33.
Murray, C., & Fixsen, J. A. (1997). Management of kneedeformity in classical arthrogryposis multiplexcongenita (amyoplasia congenita). Journal of PediatricOrthopedics, B-6, 186–191.
Palmer, P. M., MacEwen, G. D., Bowen, J. R., et al. (1985).Passive motion therapy for infants with arthrogryposis.Clinical Orthopaedics, 194, 54–59.
Porter, H. J. (1995). Lethal arthrogryposis multiplex con-genital (fetal akinesia deformation sequence, FADS).Pediatric Pathology & Laboratory Medicine, 15,617–637.
Sarwark, J. F., MacEwen, G. D., & Scott, C. I. (1990).Amyoplasia (a common form of arthrogryposis). TheJournal of Bone Joint Surgery, 72-A, 465–469.
Sells, J. M., Jaffe, K. M., & Hall, J. G. (1996). Amyoplasia,the most common type of arthrogryposis: The potentialfor good outcome. Pediatrics, 97, 225–231.
Södergård, J., Hakamies-Blomqvist, L., Sainio, K.,et al. (1997). Arthrogryposis multiplex congenita: Peri-natal and electromyographic findings, disability, andpsychosocial outcome. Journal of Pediatric Orthope-dics, B-6, 167–171.
St. Clair, H. S., & Zimbler, S. (1985). A plan of manage-ment and treatment results in the arthrogrypotic hip.Clinical Orthopaedics, 194, 74–80.
Staheli, L. T., Chew, D. E., & Elliott, J. S. (1987). Man-agement of hip dislocations in children witharthrogryposis. Journal of Pediatric Orthopedics, 7,681–685.
Swinyard, C. A., & Bleck, E. E. (1985). The etiology ofarthrogryposis (multiple congenital contracture). Clin-ical Orthopaedics and Related Research, 194, 15–29.
Thomas, B., Schopler, S., &Wood, W. (1985). The knee inarthrogryposis. Clinical Orthopaedics, 194, 87–92.
16 H. Chen

Thompson, G. H., & Bilenker, R. M. (1985). Comprehen-sive management of arthrogryposis multiplexcongenita. Clinical Orthopaedics, 194, 6–14.
Toydemir, R. M., & Bamshad, M. J. (2009). Sheldon-Hallsyndrome. Orphanet Journal of Rare Diseases, 4,115–119.
Toydemir, R.M., Rutherford, A.,Whitby, F. G., et al. (2006).Mutations in embryonic myosin heavy chain (MYH3)cause Freeman-Sheldon syndrome and Sheldon-Hallsyndrome. Nature Genetics, 38, 561–565.
Verloes, A., Mulliez, N., Gonzales, M., et al. (1992).Restrictive dermopathy, a lethal form of arthrogryposismultiplex with skin and bone dysplasia: Three newcases and review of the literature. American Journalof Medical Genetics, 43, 539–547.
Williams, P. F. (1985). Management of upper limb prob-lems in arthrogryposis. Clinical Orthopaedics, 194,60–67.
Arthrogryposis Multiplex Congenita 17

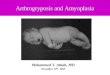
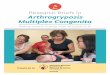
Fig. 1 (a–c) Three infants with amyoplasia congenitashowing typical, symmetrical positioning of the limbs,internally rotated and adducted shoulders, fixed extended
elbows, pronated forearms, flexed wrists and fingers, andsevere talipes equinovarus deformity
Fig. 2 (a–b) Two infantswith arthrogryposismultiplex congenitacharacterized by flexioncontractures of the kneesand fingers and equinovarusdeformities of the feet
18 H. Chen

Fig. 3 (a–b) An infantwith distal arthrogryposisshowing predominantlydistal contractures withoverlapping fingercontractures, ulnardeviation of fingers, andclubfeet
Arthrogryposis Multiplex Congenita 19

Fig. 4 (a–c) A 33-year-old female was followed forarthrogryposis multiplex congenita. At birth, flexion con-tractures of the fingers and hands, dysplastic hips, bilateralrocker bottom feet, and “generalized stiffness”were noted.At recent visit, flexion contractures of the elbows,
limitation of supination of the wrists, contractures of thethumbs and PIP joints, and operation scars of webbingrelease between 1st and 2nd fingers and Achilles tendonrelease were noted
20 H. Chen

Fig. 5 (a–d) A 4-year-oldgirl was seen forarthrogryposis multiplexcongenita. MRI image ofthe brain (a) demonstrateshypoplastic cerebellum,particularly the vermis(black arrow). This findingcan be seen in theneurogenic arthrogryposismultiplex. Pelvicradiography (b)demonstrates generalizeosteopenia, bilateral coxavalga, and mild lateraluncovering of the femoralheads. Radiographs of theleft foot demonstrateosteopenia, exaggeratedplanovalgus deformity (c),and a rocker-bottomconfiguration (d). The rightfoot has similar deformities(not shown). The family andbirth histories were notavailable since the patientwas adopted. High-resolution chromosomestudy was normal.Molecular studies,including TPM2, MYH3,and SMN1 (homozygousdeletion of SMN1) genes,were negative (Courtesy ofDr. Grace Guo)
Arthrogryposis Multiplex Congenita 21