Embed Size (px)
Citation preview
Journal of Neurology, Neurosurgery, anid Psychiatry, 1972, 35, 425-434
Arthrogryposis multiplex congenitaPart 1: Clinical and electromyographic aspects
E. P. BHARUCHA, S. S. PANDYA, AND DARAB K. DASTUR
From the Children's Orthopaedic Hospital, and the Neuropathology Unit,J.J. Group of Hospitals, Bombay-8, India
SUMMARY Sixteen cases with arthrogryposis multiplex congenita were examined clinically andelectromyographically; three of them were re-examined later. Joint deformities were present in allextremities in 13 of the cases; in eight there was some degree of mental retardation. In two cases,there was clinical and electromyographic evidence of a myopathic disorder. In the majority, theappearances of the shoulder-neck region suggested a developmental defect. At the same time,selective weakness of muscles innervated by C5-C6 segments suggested a neuropathic disturbance.EMG revealed, in eight of 13 cases, clear evidence of denervation of muscles, but without anyregenerative activity. The non-progressive nature of this disorder and capacity for improvement inmuscle bulk and power suggest that denervation alone cannot explain the process. Re-examinationof three patients after two to three years revealed persistence of the major deformities and muscleweakness noted earlier, with no appreciable deterioration.
Otto (1841) appears to have been the first torecognize this condition. Decades later, Magnus(1903) described it as multiple congenital con-tractures with muscle defects. In 1913, Rochergave the designation 'multiple congenital articu-lar rigidity' and suggested that intrauterinepressure, such as that due to hydramnios, mightrestrict foetal movement and produce jointchanges secondarily. In 1923, Stern proposedthe term 'arthrogryposis multiplex congenita'(AMC), from two Greek words, meaning a'crooking' of joints. Up to this time, jointdeformities were generally considered the pri-mary defect. There are also some reports in theliterature suggesting a primary muscle disorder.These are reviewed by Dastur, Razzak, andBharucha (1972).
It was not till 1933 that attention shifted tothe central nervous system as the primary site ofpathology in AMC. In this year, Price (1933)and Scarzella (1933) independently describeddiminution in size, degeneration, and a falloutof anterior horn cells in the spinal cord in casesof this disorder that went to necropsy. Sincethen, many papers have stressed the spinal cordchanges in AMC (Gilmour, 1946; Brandt, 1947;Kanof, Aronson, and Volk, 1956; Fowler, 1959;and Swinyard, 1960). Anomalies of the cerebralcortex, such as abnormal gyri and dilated
425
ventricles, have been described (Adams, Denny-Brown, and Pearson, 1953; Fowler, 1959), inaddition to the spinal cord changes.
In the past decade, with the use of electro-myography, the nervous system and especiallythe spinal cord remained the focus of attention,as a large proportion of cases revealed denerva-tion potentials (Lefebvre and Chaumont, 1957;Swinyard, 1960; Smith, Bender, and Stover,1963; Amick, Johnson, and Smith, 1967).Thus, by the mid-1960s, two major types of
AMC were being recognized-the neurogenicand the myopathic. At times a primary processof maldevelopment of neuromuscular elementswas also envisaged.The study reported here was undertaken in an
attempt to resolve some of these differences ofopinion regarding the pathogenesis of this con-dition, through a combined clinical, electro-myographic, and histopathological evaluation.The presence of limiting deformities at two ormore joints (excepting talipes) from birthonwards, was considered essential for thediagnosis.
METHODS
During the three years 1966 to 1968, we examinedand studied 15 cases (and added one of the oldercases) of AMC, as observed at the Children's
Protected by copyright.
on March 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.35.4.425 on 1 August 1972. D
ownloaded from
E. P. Bhlarucha, S. S. Pandya, and Darab K. Dastur
Orthopaedic Hospital in Bombay. A detailed ante-natal, natal, and postnatal history, with a familyhistory and a careful evaluation of the develop-mental milestones, was obtained from the parents ofeach child. This was followed by a detailed neuro-logical examination and, generally, a psychologicalevaluation. Radiographs of the bones and joints oflimb and trunk were available in 13 cases.
Electromyography was carried out on 13 of thecases, using either a RAF type IlIc single channel ora Disa two-channel electromyograph coupled with aTektronix type 564 storage oscilloscope, and con-centric needle electrodes. A general sampling of oneor two muscles each of the upper and the lower limb,usually including the deltoid and the quadriceps, wascarried out in all cases. Nerve conduction velocitycould be measured in only one case. In each muscleas many sites were needled as were necessary to study10 motor units. With the RAF type IlIc singlechannel instrument only rough visual measurementswere possible, but use of the coupled DISA andTektronix instrument enabled accurate determina-tion of amplitude and duration.
Three of these children could be recalled two tothree years later and were examined carefully andrepeat biopsy specimens obtained (Dastur et al.,1972).
OBSERVATIONSINITIAL EXAMINATION
HISTORY: POSSIBLE PREDISPOSING FACTORS Genetic(Cases 1, 8, 9, 15.) The parents of case 1 were relatedto each other; there was a sib with arthrogryposismultiplex in the family of case 8. The father andsister of case 15 had a congenital heart lesion, whilean uncle of the same patient had bilateral talipesequinovarus (TEV). On the other hand, case 9 hadan unaffected twin sister.
Pregnancy (Cases 1, 14.) In the majority of cases,this was quite normal. However, a rash all over thebody in case l's mother at the seventh month ofpregnancy may have been due to measles. Anothermother (case 14) had vaginal bleeding from thethird to the seventh months of pregnancy. Two
mothers complained of abdominal pain 15 days andtwo months before delivery respectively.
Delivery (Cases 2, 8, 12, 13, 14.) It was surprisingto note how frequently these children with fixed limbdeformities were born at home without obstetricalassistance. Two were vertex presentations, with legsflexed at the hips and extended at the knees. Onebreech presenting baby also had legs extended at theknees. However, case 13 required a caesarean sectionafter prolonged labour. During delivery of case 12the head came out 20 minutes before the rest of thebody, with the legs entwined around the neck andthe arms tethered to the side by loops of umbilicalcord.There was no clear history of hydramnios or
oligohydramnios in any of these cases. Somemothers however did complain of feebleness offoetal movements during this pregnancy comparedwith their other pregnancies. Cases 6 and 16 had adelay in crying after birth, while case 1 suckedpoorly and had a feeble cry for the first month.
Developmental milestones A delay in motor de-velopment was present in 15 of 16 cases. The soleexception was case 7, who was seen only once at theage of 5 months, when it was difficult to establishmotor retardation. In eight cases, there was alsomental retardation, suggesting an associated cerebraldefect. Isolated motor delay with normal mentalstatus was present in the remainder, and here thegross mechanical handicap resulting from arm andleg deformities was probably the major contributoryfactor. This is particularly true of cases 4 and 14,where normal mental development accompaniednormal early motor milestones with delay in standingand walking.
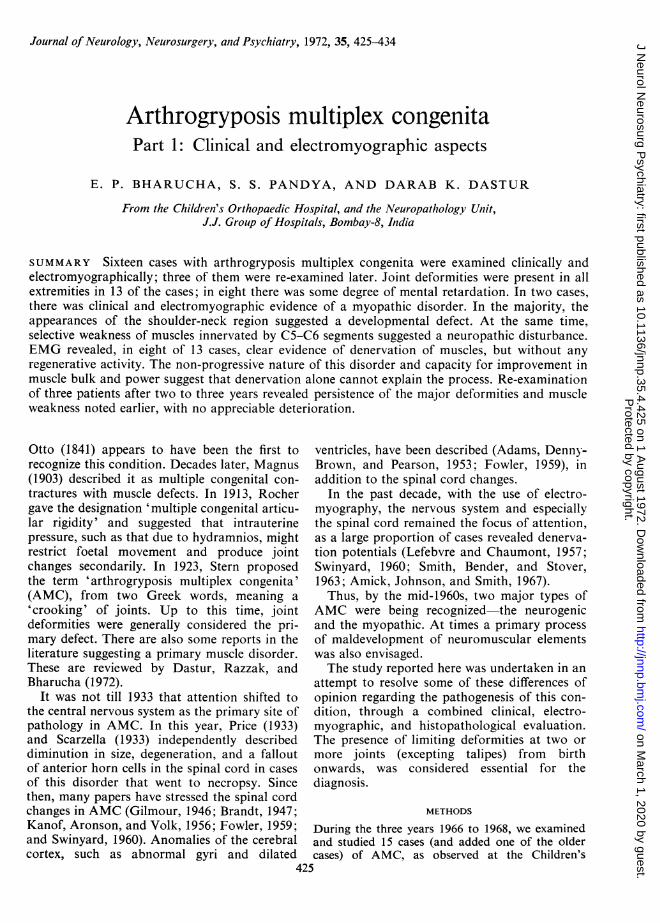
CLINICAL FEATURES All 16 cases of arthrogryposismultiplex congenita in the present series showeddeformities of two or more joints from birth. Theirages at the first examination varied from 2 days to15 years and there were nine males and sevenfemales. The salient clinical findings are summarizedin Table 1.
BLE 1SUMMARY OF MAIN CLINICAL AND ELECTROMYOGRAPHIC FINDINGS IN 16 CASES
Case Sex Age Main deformities Other clinical Electromyography FMG Otherno. (yr) and/or contractures features diagnosis informaticn
Fibrilla- Motor unit potential Inter-tions ference
Doira- Ampli- Poly- patterntion tude phasics
(msec) (,u V) (%)
1 F 2 2/12 Arms: 'policeman-tip' Mild myopathic No 1-2 300 50 Full Myo-A.L. Legs: mild flexion facies; proximal
weakness
2 F 8/12 Arms: normal Weak arms, proximal NoA.K.C. Legs: marked extension distal. Hip-movements
with TE fair despite dislocations
pathic
6 1000 None Full Normal
426P
rotected by copyright. on M
arch 1, 2020 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.35.4.425 on 1 A
ugust 1972. Dow
nloaded from
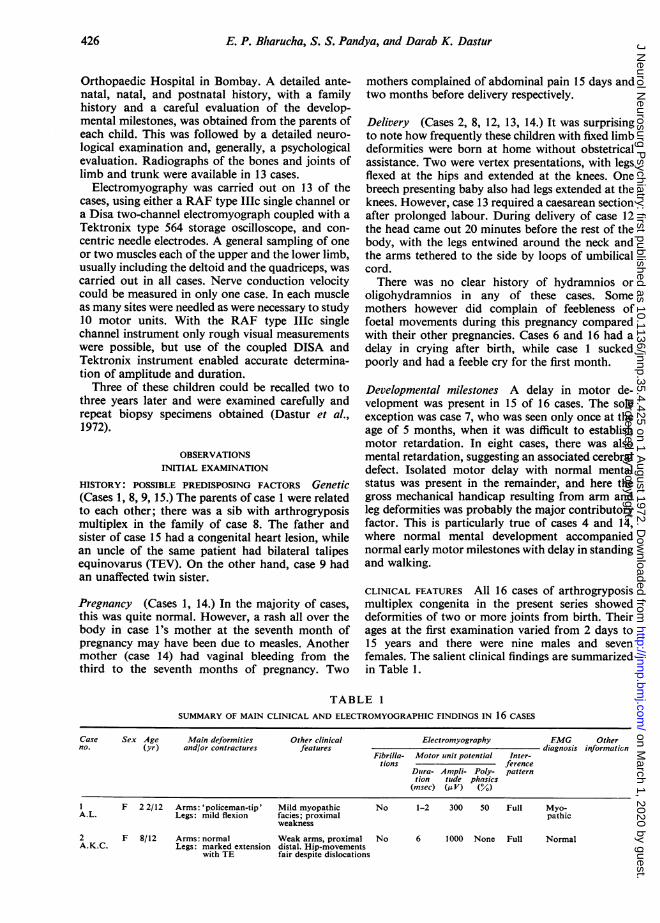
Arthrogryposis multiplex congeniita 427
TABLE 1 -(continued)
Case Sex Age Main deformities Other clinical Electromyography EMG Otherno. (Iyr) and/or contractures features diagnosis information
Fibrilla- Motor unit potential Inter-tions ference
Dura- Ampli- Poly- patterntion tude phasics
(msec) (MV) (%)
M 3 6/12 Arms: minimal flexiondeformity atelbows
Legs: in flexion
M 2 Arms: 'policeman-tip'Legs: almost normal
M 11 Arms: 'policeman-tip'Legs: some flexion at
hips, knees;ankles fixed inmid-position
F 1 3/12 Arms: 'policeman-tip'Legs: kept in 'diamond
shaped position
M 5/12 Legs: in flexion, with'hockey-stick'feet
F 3 Arms: only slight elbowflexion
Legs: knees-posteriordislocation withhyperextension
F 5 9/12 Arms: normal (mildspasticity of leftarm)
Legs: marked lordosiswith hips flexed,knees extended
M 1 2/12 Arms:'policeman-tip'Legs: in extension
M 3 Arms: mild, modified' policeman-tip'
Legs: generalizedflexion
'Bird-like facies',first 3 fingers almostequalMR+
Right foot prehensileTakes a few stepswhen led. MR+
Spina bifida occultaseveral operationsdone on all these 3joints; walking withcrutches
Stands with support
Bilateral hip disloca-tion and spina bifida
Drooping eyelidsBilateral hip disloca-tion with lateral rota-tion of leg. MR+
MR-mildVSD-heart
No power, exceptsome at hips
'Bird-like' facies,kyphoscoliosisWalks a little bentforward. MR+
No 5 800 None Full Normal Prominentsoft tissueshadows inx-rays
High 6fre-quencydis-charges
1000 100 Single Neuro-oscilla- pathictions
No 6 1000 10 Singleoscilla-tions
No
Neuro-pathic
1-3 800 25 Full Myo- One olderpathic sib similarly
affected
Yes 14 400 100 Single Neuro- One twinoscilla- pathic sister nor-tions mal
No 6 600 10 Singleoscilla-tions
No 5 200 None Full
Neuro-pathic
Normal
M 3 10/12 Arms: 'policeman-tip' Odd facies withLegs: hips extended, hypognathism.
knees flexed, TEV MR-mild
F 11 Arms: 'policeman-tip' Marked wasting ofat birth; surgical C5-C6 muscles. Atcorrections later regular school in VI
Legs: only ankle plantar standard.flexed Walks with support
F 2 Arms: 'policeman-tip' Arms and calvesLegs: generalized extremely thin.
flexion. Bilateral Shuffles on bottom.TEV MR+
M 16 Shoulders: elevated and Arms very muscularforwards, merg- but poor abductioning with neck Legs: several opera-
Legs: fixed in extension tions; walks withcrutches
No 6 800 10 Single Neuro-oscilla- pathictions (upper
andlowerlimbs)
No 10 600 50 Single Neuro-oscilla- pathictions
Yes 10 1500 50 Singleoscilla-tions
Neuro- Good im-pathic provement
with re-
habilitativeand surgicalprocedures.Studyingwell
M 1 6/12 Arms: 'policeman-tip' Most joints fixed; allLegs: mild generalized movements very poor.
flexion; bilateral MR +TEV
MR = Mental retardation. VSD = Ventricular septal defect.
3M.N.
4M.R.G.
5H.B.
6L.P.S.
7J.R.A.
8A.K.
9M.G.
10D.G.M.
I IT.M.
12S.D.
13K.P.
14S.M.S.
15C.K.
16R.V.D.
TEV = talipes equinovarus.
Protected by copyright.
on March 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.35.4.425 on 1 August 1972. D
ownloaded from
E. P. Bharucha, S. S. Panidya, and Darab K. Dastur
.-...
.......
,A",' t ....
.. <~~~~~~~~~~~~~~~~~~~~~~~~~~~~............
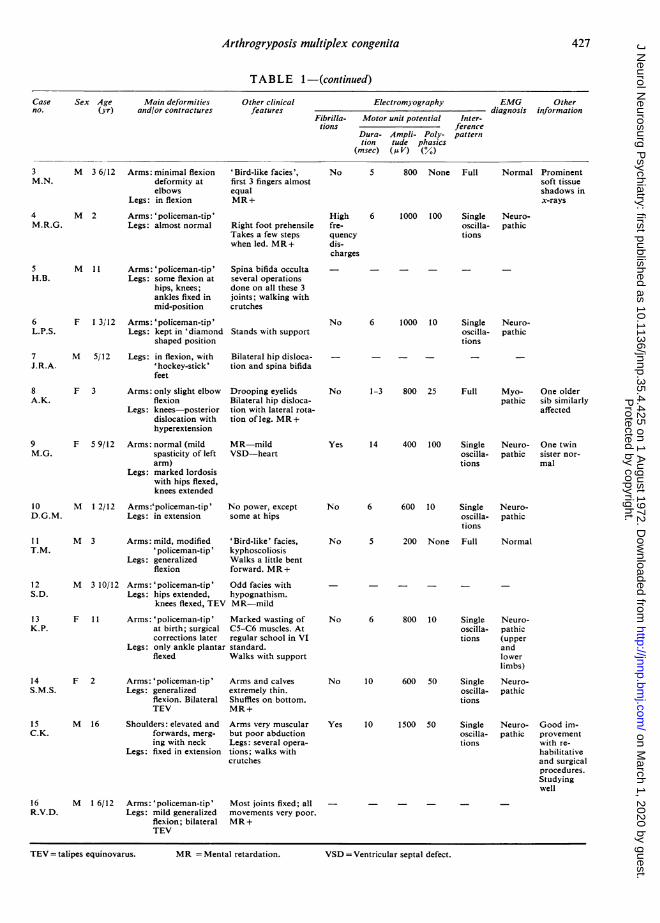
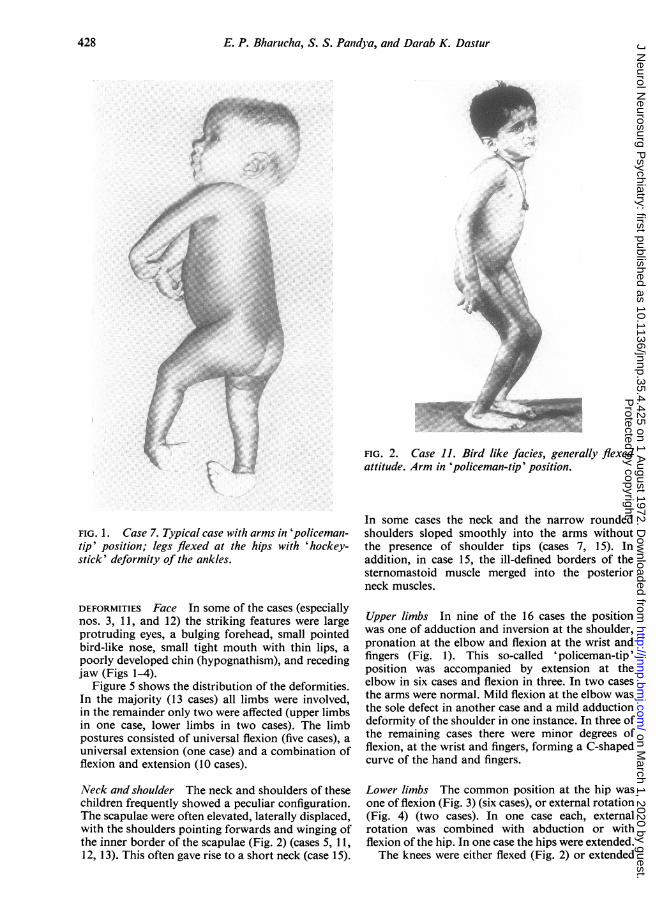
FIG. 1. Case 7. Typical case with arms in 'policeman-tip' position; legs flexed at the hips with 'hockey-stick' deformity of the ankles.
DEFORMITIES Face In some of the cases (especiallynos. 3, 11, and 12) the striking features were largeprotruding eyes, a bulging forehead, small pointedbird-like nose, small tight mouth with thin lips, apoorly developed chin (hypognathism), and recedingjaw (Figs 1-4).
Figure 5 shows the distribution of the deformities.In the majority (13 cases) all limbs were involved,in the remainder only two were affected (upper limbsin one case, lower limbs in two cases). The limbpostures consisted of universal flexion (five cases), a
universal extension (one case) and a combination offlexion and extension (10 cases).
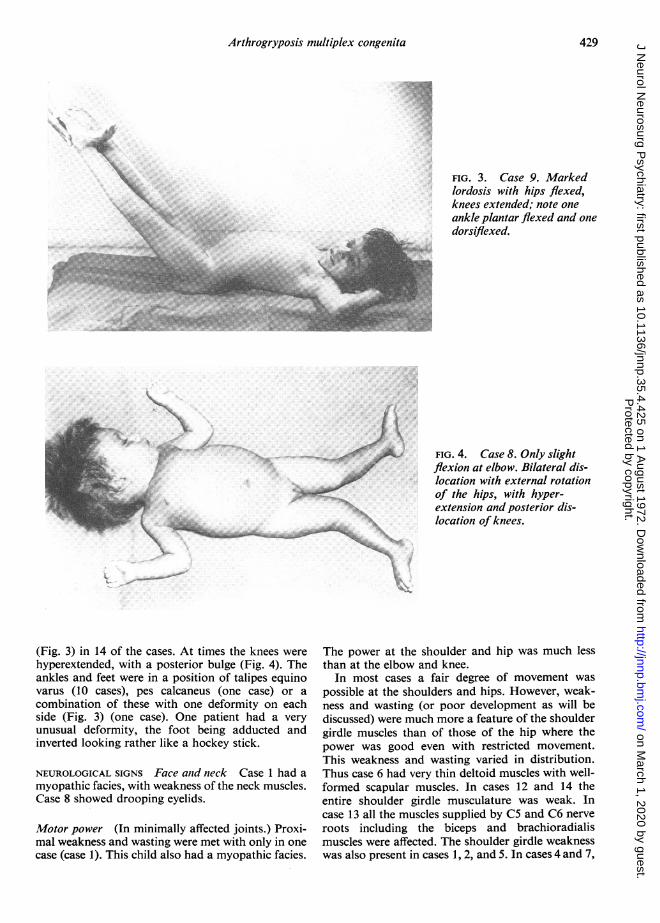
Neck and shoulder The neck and shoulders of thesechildren frequently showed a peculiar configuration.The scapulae were often elevated, laterally displaced,with the shoulders pointing forwards and winging ofthe inner border of the scapulae (Fig. 2) (cases 5, 11,12, 13). This often gave rise to a short neck (case 15).
FIG. 2. Case 11. Bird like facies, generally flexedattitude. Arm in 'policeman-tip' position.
In some cases the neck and the narrow roundedshoulders sloped smoothly into the arms withoutthe presence of shoulder tips (cases 7, 15). Inaddition, in case 15, the ill-defined borders of thesternomastoid muscle merged into the posteriorneck muscles.
Upper limbs In nine of the 16 cases the positionwas one of adduction and inversion at the shoulder,pronation at the elbow and flexion at the wrist andfingers (Fig. 1). This so-called 'policeman-tip'position was accompanied by extension at theelbow in six cases and flexion in three. In two casesthe arms were normal. Mild flexion at the elbow wasthe sole defect in another case and a mild adductiondeformity of the shoulder in one instance. In three ofthe remaining cases there were minor degrees offlexion, at the wrist and fingers, forming a C-shapedcurve of the hand and fingers.
Lower limbs The common position at the hip wasone of flexion (Fig. 3) (six cases), or external rotation(Fig. 4) (two cases). In one case each, externalrotation was combined with abduction or withflexion of the hip. In one case the hips were extended.The knees were either flexed (Fig. 2) or extended
428P
rotected by copyright. on M
arch 1, 2020 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.35.4.425 on 1 A
ugust 1972. Dow
nloaded from
Arthrogryposis multiplex congenita
(Fig. 3) in 14 of the cases. At times the knees were
hyperextended, with a posterior bulge (Fig. 4). Theankles and feet were in a position of talipes equinovarus (10 cases), pes calcaneus (one case) or a
combination of these with one deformity on eachside (Fig. 3) (one case). One patient had a very
unusual deformity, the foot being adducted andinverted looking rather like a hockey stick.
NEUROLOGICAL SIGNS Face anid neck Case 1 had a
myopathic facies, with weakness of the neck muscles.Case 8 showed drooping eyelids.
Motor power (In minimally affected joints.) Proxi-mal weakness and wasting were met with only in onecase (case 1). This child also had a myopathic facies.
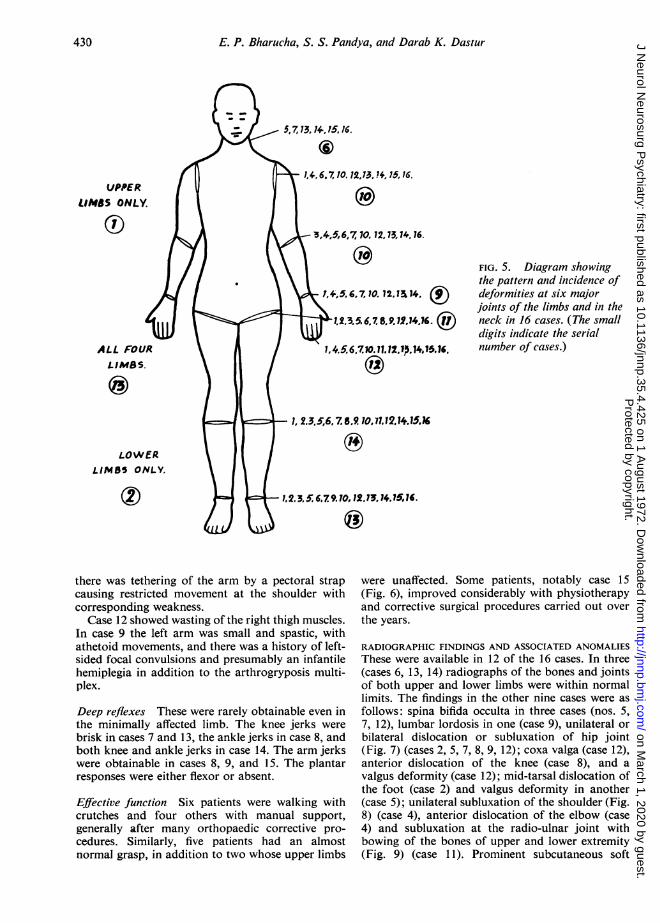
FIG. 3. Case 9. Markedlordosis with hips flexed,knees extended; note oneankle plantar flexed and onedorsiflexed.
FIG. 4. Case 8. Only slightflexion at elbow. Bilateral dis-location with external rotationof the hips, with hyper-extension and posterior dis-location of knees.
The power at the shoulder and hip was much lessthan at the elbow and knee.
In most cases a fair degree of movement was
possible at the shoulders and hips. However, weak-ness and wasting (or poor development as will bediscussed) were much more a feature of the shouldergirdle muscles than of those of the hip where thepower was good even with restricted movement.This weakness and wasting varied in distribution.Thus case 6 had very thin deltoid muscles with well-formed scapular muscles. In cases 12 and 14 theentire shoulder girdle musculature was weak. Incase 13 all the muscles supplied by C5 and C6 nerve
roots including the biceps and brachioradialismuscles were affected. The shoulder girdle weaknesswas also present in cases 1, 2, and 5. In cases 4 and 7,
- "l
/
- V.
4'-
429
.4
'.. ri
,wh,I
-I..v..
.. Pi.
4I.
I...4
Protected by copyright.
on March 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.35.4.425 on 1 August 1972. D
ownloaded from
E. P. Bharucha, S. S. Pandya, and Darab K. Dastur
UPPERLIMBS ONLY.
ALL FOURLIMBS.
LOWERLIMBS ONLY.
5,7,13,14 75,16.
6.J 6710, 12,73,7+, 75,16.1 6)
3,4,5,6, 170, 12,73,14, 76.
'(:oIj+1,5.6,7. 10. 12,1 t14. t1.2.3,5. 6,7. 8.9.12.14,16.
(ii)620.11,p1,1.C
FIG. 5. Diagram showingthe pattern and incidence ofdeformities at six majorjoints of the limbs and in theneck in 16 cases. (The smalldigits indicate the serialnumber of cases.)
1, 2.3,5,6,7 .610,(1.12)14.15.6
there was tethering of the arm by a pectoral strapcausing restricted movement at the shoulder withcorresponding weakness.
Case 12 showed wasting of the right thigh muscles.In case 9 the left arm was small and spastic, withathetoid movements, and there was a history of left-sided focal convulsions and presumably an infantilehemiplegia in addition to the arthrogryposis multi-plex.
Deep reflexes These were rarely obtainable even inthe minimally affected limb. The knee jerks werebrisk in cases 7 and 13, the ankle jerks in case 8, andboth knee and ankle jerks in case 14. The arm jerkswere obtainable in cases 8, 9, and 15. The plantarresponses were either flexor or absent.
Effective function Six patients were walking withcrutches and four others with manual support,generally after many orthopaedic corrective pro-cedures. Similarly, five patients had an almostnormal grasp, in addition to two whose upper limbs
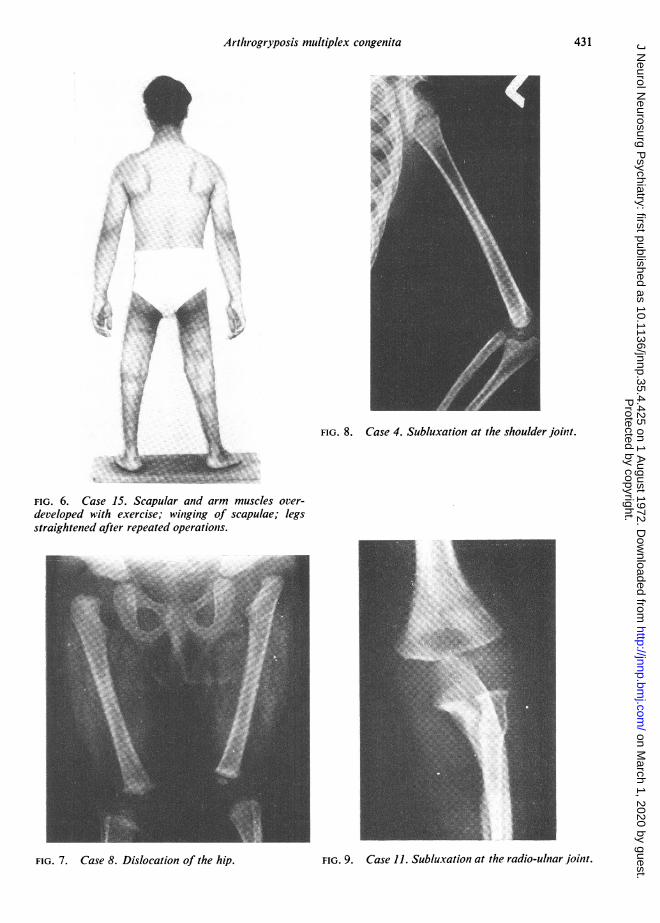
were unaffected. Some patients, notably case 15(Fig. 6), improved considerably with physiotherapyand corrective surgical procedures carried out overthe years.
RADIOGRAPHIC FINDINGS AND ASSOCIATED ANOMALIESThese were available in 12 of the 16 cases. In three(cases 6, 13, 14) radiographs of the bones and jointsof both upper and lower limbs were within normallimits. The findings in the other nine cases were asfollows: spina bifida occulta in three cases (nos. 5,7, 12), lumbar lordosis in one (case 9), unilateral orbilateral dislocation or subluxation of hip joint(Fig. 7) (cases 2, 5, 7, 8, 9, 12); coxa valga (case 12),anterior dislocation of the knee (case 8), and avalgus deformity (case 12); mid-tarsal dislocation ofthe foot (case 2) and valgus deformity in another(case 5); unilateral subluxation of the shoulder (Fig.8) (case 4), anterior dislocation of the elbow (case4) and subluxation at the radio-ulnar joint withbowing of the bones of upper and lower extremity(Fig. 9) (case 1 1). Prominent subcutaneous soft
430
1, 2.3.5'.
Protected by copyright.
on March 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.35.4.425 on 1 August 1972. D
ownloaded from
Arthrogryposis multiplex congenita
4.~~~~~~
FIG. 8. Case 4. Subluxation at the shoulder joint.
FIG. 6. Case 15. Scapular and arm muscles over-developed with exercise; winging of scapulae; legsstraightened after repeated operations.
FIG. 9. Case 11. Subluxation at the radio-ulnar joint.
431
FIG. 7. Case 8. Dislocation of the hip.
Protected by copyright.
on March 1, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.35.4.425 on 1 August 1972. D
ownloaded from
E. P. Bharucha, S. S. Pandya, and Darab K. Dastur
tissue shadows were observed in two cases (nos. 3 and4). Thus thejoint affected most often was the hip andthe changes observed there were due both to anill-formed head of the femur and to a shallowacetabulum.
In addition, clinical examination revealed pigeonchest in one (case 1), kyphoscoliosis in two (cases 5and 11). There was a ventricular septal defect in case9 and a congenital inguinal hernia in case 16.
ELECTROMYOGRAPHIC FINDINGS Electromyography(EMG) performed in 13 of the 16 cases, showed aclear neuropathic pattern in eight cases, a myopathicpicture in two (cases 1 and 8). It was normal in three(cases 2, 3, 11). The main findings are summarizedin Table 1.
It will be seen that the essential neuropathic
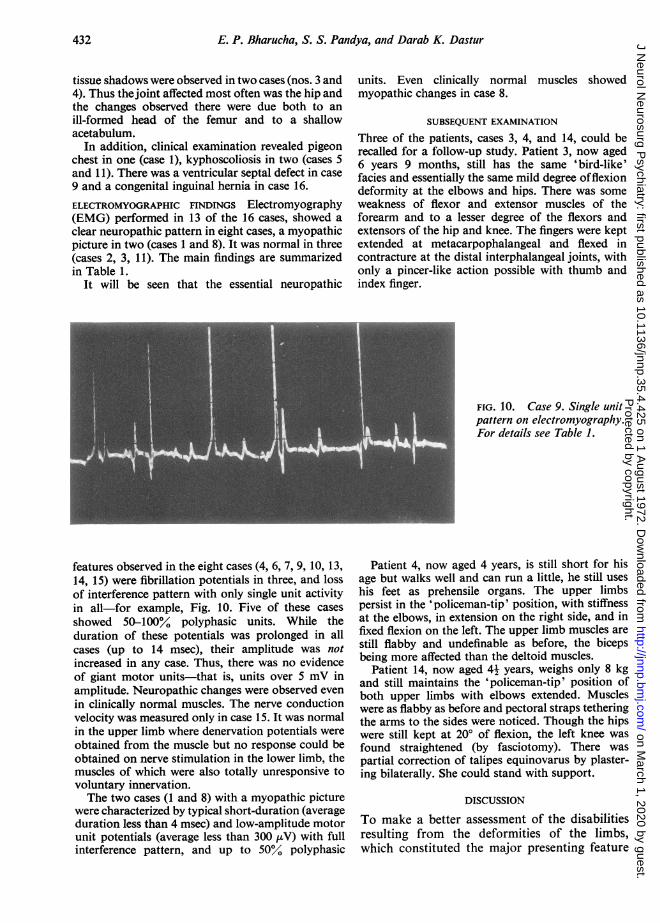
features observed in the eight cases (4, 6, 7, 9, 10, 13,14, 15) were fibrillation potentials in three, and lossof interference pattern with only single unit activityin all-for example, Fig. 10. Five of these cases
showed 50-100% polyphasic units. While theduration of these potentials was prolonged in allcases (up to 14 msec), their amplitude was notincreased in any case. Thus, there was no evidenceof giant motor units-that is, units over 5 mV inamplitude. Neuropathic changes were observed even
in clinically normal muscles. The nerve conductionvelocity was measured only in case 15. It was normalin the upper limb where denervation potentials were
obtained from the muscle but no response could beobtained on nerve stimulation in the lower limb, themuscles of which were also totally unresponsive tovoluntary innervation.The two cases (1 and 8) with a myopathic picture
were characterized by typical short-duration (averageduration less than 4 msec) and low-amplitude motorunit potentials (average less than 300 ,uV) with fullinterference pattern, and up to 5000 polyphasic
units. Even clinically normal muscles showedmyopathic changes in case 8.
SUBSEQUENT EXAMINATION
Three of the patients, cases 3, 4, and 14, could berecalled for a follow-up study. Patient 3, now aged6 years 9 months, still has the same 'bird-like'facies and essentially the same mild degree offlexiondeformity at the elbows and hips. There was someweakness of flexor and extensor muscles of theforearm and to a lesser degree of the flexors andextensors of the hip and knee. The fingers were keptextended at metacarpophalangeal and flexed incontracture at the distal interphalangeal joints, withonly a pincer-like action possible with thumb andindex finger.
FIG. 10. Case 9. Single unitpattern on electromyography.For details see Table 1.
Patient 4, now aged 4 years, is still short for hisage but walks well and can run a little, he still useshis feet as prehensile organs. The upper limbspersist in the 'policeman-tip' position, with stiffnessat the elbows, in extension on the right side, and infixed flexion on the left. The upper limb muscles arestill flabby and undefinable as before, the bicepsbeing more affected than the deltoid muscles.
Patient 14, now aged 41 years, weighs only 8 kgand still maintains the 'policeman-tip' position ofboth upper limbs with elbows extended. Muscleswere as flabby as before and pectoral straps tetheringthe arms to the sides were noticed. Though the hipswere still kept at 200 of flexion, the left knee wasfound straightened (by fasciotomy). There waspartial correction of talipes equinovarus by plaster-ing bilaterally. She could stand with support.
DISCUSSION
To make a better assessment of the disabilitiesresulting from the deformities of the limbs,which constituted the major presenting feature
432P
rotected by copyright. on M
arch 1, 2020 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.35.4.425 on 1 A
ugust 1972. Dow
nloaded from
Arthrogryposis multiplex congenita
of our cases of AMC, an attempt was made tocorrelate them with the functional status of thelimbs. Deformities were graded in the arms andlegs as I, II, and III, according to the number ofjoints affected. The functional loss in the upperlimbs was graded as A, B, or C, according to theability to grip with the hands. Thus with theseverest degree of loss (grade C), no prehensionwas possible with the hands. With grade B, afeeble grasp was possible, while with grade A, afairly good grasp was present. In the legs, if thechild was over I12 years and could not walk, thefunctional loss was considered to be grade C.With grade B loss, walking was possible withappliances, and with grade A, only a stick orslight support was required. In children underII years who had not yet started to walk, thepower was graded according to the ability tokick freely while lying in bed. Table 2 showsthese relationships for the arms and legs.
TABLE 2RELATION OF DEFORMITY TO FUNCTION
Deformlity Case no. Functional No. ofloss cases
A: in arms (16 cases)Normal 2, 3 Nil 2Grade 1 5, 8, 9, 15, Normal 1
Grade A 2Grade C 1
Grade II 7, 11, 13 Grade A 2Grade C I
Grade III 1, 4, 6, 10, 12, 14, 16 Grade C 7
B: in legs (16 cases)Normal 4 Nil 1Grade I 11, 13 Grade A 1
Grade B IGrade II 3, 6, 7, 8, 10, 14 Grade A 2
Grade B 2Grade C 2
Grade IIl 1, 2, 5, 9, 12, 15, 16 Grade B 3Grade C 4
The important joints in the upper limbsappear to be those of the wrist and fingers. Asthe Table shows, with only one pair of jointsinvolved (grade I deformity), if the wrist andfingers were affected there could be a grade Cfunctional loss. Contrariwise, a grade II deform-ity involving the elbow and shoulder only mightbe compatible with grade A function. In the legsthere was greater correlation between thenumber of joints involved and functional in-capacity. However, a person with all three joints
involved may walk with support, provided thatthe feet sit well on the ground, the knees arefixed in extension, and some movements areavailable at the hip. Hence, occasionally it isfound (cases 6, 8) that the functional incapacityis less than the degree of deformity would havewarranted.
There were two features of note in the follow-up study of three of the children, carried out twoto three years after the initial examination. Themajor deformities associated with actual fibroticcontractures-for example, the 'policeman-tip'position, had remained in status quo. The overallgrowth of the children was also poor. However,there was no deterioration in any specific move-ment, deformity, or function of a muscle group.Our ideas on the pathogenesis of arthrogry-
posis multiplex congenita will be elaborated inPart 2 but it appears necessary to draw someinferences from the clinical and electrical data.It is noteworthy that even clinically, most of our16 cases did not reveal any features suggestive ofa myopathic disorder. While nine of the casesevidenced weakness of the shoulder girdle, onlytwo of these presented bilateral facial weaknessand proximal muscle weakness of the limbsconsistent with a myopathy. Only these twopatients showed EMG evidence of myopathy(Table 1). The fact that the proximal weaknessof the upper limbs did not equally involve all theabductor muscles of the shoulder spoke againsta typical muscular dystrophy. Thus, for instance,either the deltoid alone was weak, or the deltoidand spinati muscles were affected. Furthermore,the weakness also tended to involve the bicepsand brachialis muscles, creating the impression ofa C5-C6 segmental lesion of the spinal cord. Themost frequently observed picture of the upperlimbs in these cases namely, the 'policeman-tip' position, seemed to have been brought aboutby this selective muscular involvement, and wasreminiscent of upper brachial plexus birth injuryas in Erb's palsy.The majority of cases also did not manifest
any clear signs of a neurogenic disorder. How-ever, it is realized that against a background ofmultiple joint deformities and contractures whichare most pronounced distally, the demonstrationof distal weakness and the elicitation of deep andsuperficial reflexes are bound to be difficult orimpossible. Fasciculations were not clinicallydemonstrable. Nevertheless, as revealed byelectromyography, eight of the 13 patients hadevidence of a denervation process. While single
433P
rotected by copyright. on M
arch 1, 2020 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.35.4.425 on 1 A
ugust 1972. Dow
nloaded from

E. P. Bharucha, S. S. Pandya, and Darab K. Dastur
motor unit potentials were constantly present andfibrillations were frequent, giant polyphasicmotor unit potentials (indicating regeneration inthe motor units) were never detected. Consider-ing the fact that a number of sites in severalmuscles were examined, the absence of such re-innervation seemed significant, being unusualfor most motor neurone diseases of long dura-tion.
There are some clinical and surgical featuresalso pointing in the direction of a primary defectin muscle formation. The characteristic positionof the shoulder region-namely, high placedlaterally rotated scapulae with a short neckmerging with the arms without clear shouldertips-points to an incomplete embryonic descentof the scapulae and lack of differentiation of theshoulder girdle muscles. Obvious congenitalmalformation of the hip joint may occasionallybe accompanied by retention of a fair amount ofpower in the muscles of the hip. This suggests aprimary developmental defect or a dysplasticprocess. Clinical improvement is noticed overthe years with gain in muscle bulk and power, asthe infant with AMC grows up, especially withthe help of physiotherapy, as for instance in ourcase 15.
REFERENCES
Adams, R. D., Denny-Brown, D. E., and Pearson, C. M.(1953). Diseases of Muscle: A Study in Pathology. Hoeber:New York.
Amick, L. D., Johnson, W. W., and Smith, H. L. (1967).
Electromyographic and histopathologic correlations inarthrogryposis. Archives of Neurology, 16, 512-523.
Brandt, S. (1947). A case of arthrogryposis multiplex con-genita anatomically appearing as foetal spinal muscularatrophy. Acta Paediatrica, 34, 365-381.
Dastur, D. K., Razzak, Z. A., and Bharucha, E. P., Arthro-gryposis multiplex congenita; Part 2: Muscle pathologyand pathogenesis. Journal of Neurology, Neurosurgery,and Psychiatry, 35, 435-450.
Fowler, M. (1959). A case of arthrogryposis multiplexcongenita with lesions in the nervous system. Archives ofDisease in Childhood, 34, 505-510.
Gilmour, J. R. (1946). Amyoplasia congenita. Journal ofPathology and Bacteriology, 58, 675-685.
Kanof, A., Aronson, S. M., and Volk, B. W. (1956). Arthro-gryposis: a clinical and pathological study of three cases.Paediatrics, 17, 532-540.
Lefebvre, J., and Chaumont, P. (1957). Examen electrolo-gique dans l'arthrogrypose. Revue Neurologique, 96, 439-440.
Magnus, F. (1903). Ein Fall von multiplen congenitalenContracturen mit Muskeldefecten. Zeitschrift fuir ortho-padische Chirurgie, 11, 424-432.
Otto, A. G. (1841). Monstrorum sexcentorum descriptioanatomica. No. 572. Monstrum humanum trunco nimisbrevi et extremitatibus incuratis. In Museum Anatomico-Pathologicum Vratislaviense, p. 323. Hirt: Vratislaviae.
Price, D. S. (1933). A case of amyoplasia congenita, withpathological report. Archives of Disease in Childhood, 8,343-354.
Rocher, H.-L. (1913). Les raideurs articulaires congenitalesmultiples. Journal de Medicine de Bordeaux, 84, 772-780,798-801, 815-818, 828-831.
Scarzella, M. (1933). Su di un caso di distrofia muscolarefetale. Archivio Italiano di Pediatrica e Puencoltura, 1,447-474.
Smith, E. M., Bender, L. F., and Stover, C. N. (1963).Lower motor neuron deficit in arthrogryposis. An EMGstudy. Archives of Neurology, 8, 97-100.
Stern, W. G. (1923). Arthrogryposis multiplex congenita.Journal of the American Medical Association, 81, 1507-1510.
Swinyard, C. A. (1960). Progressive muscular dystrophy andatrophy and related conditions: diagnosis and manage-ment. Pediatric Clinics of North America, 7, 703-732.
434P
rotected by copyright. on M
arch 1, 2020 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.35.4.425 on 1 A
ugust 1972. Dow
nloaded from