Embed Size (px)
Citation preview

MAY 2014 | Volume 37 • Number 5
n Review Article
educational objectives
Instructions1. Review the stated learning objectives at the beginning of the CME article and determine if these objectives match your individual learning needs.
2. Read the article carefully. Do not neglect the tables and other illustrative materials, as they have been selected to enhance your knowledge and understanding.
3. The following quiz questions have been designed to provide a useful link between the CME article in the issue and your everyday practice. Read each question, choose the correct answer, and record your answer on the CME Registration Form at the end of the quiz.
4. Type or print your full name and address and your date of birth in the space provided on the CME Registration Form.
5. Indicate the total time spent on the activity (reading article and completing quiz). Forms and quizzes cannot be processed if this section is incomplete. All participants are required by the accreditation agency to attest to the time spent completing the activity.
6. Complete the Evaluation portion of the CME Regi stration Form. Forms and quizzes cannot be processed if the Evaluation portion is incomplete. The Evaluation portion of the CME Registration Form will be separated from the quiz upon receipt at OrthOpedics. Your evaluation of this activity will in no way affect the scoring of your quiz.
7. Send the completed form, with your $15 payment (check or money order in US dollars drawn on a US bank, or credit card information) to: OrthOpedics CME Quiz, PO Box 36, Thorofare, NJ 08086, OR take the quiz online. Visit www.Healio.com/EducationLab/Orthopedics for details.
8. Your answers will be graded, and you will be advised whether you have passed or failed. Unanswered questions will be considered incorrect. A score of at least 80% is required to pass. If a passing score is achieved, Keck School of Medicine of USC will issue an AMA PRA Category 1™ certificate within 4-6 weeks.
9. Be sure to mail the CME Registration Form on or before the deadline listed. After that date, the quiz will close. CME Registration Forms received after the date listed will not be processed.
CME ACCREDITATIONThis activity has been planned and implemented
in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Keck School of Medicine of USC and OrthOpedics. Keck School of Medicine of USC is accredited by the ACCME to provide continuing medical education for physicians.
Keck School of Medicine of USC designates this Journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
This CME activity is primarily targeted to orthopedic surgeons, hand surgeons, head and neck surgeons, trauma surgeons, physical medicine specialists, and rheumatologists. There is no specific background requirement for participants taking this activity.
FULL DISCLOSURE POLICYIn accordance with the Accreditation Council for Continuing
Medical Education’s Standards for Commercial Support, all CME providers are required to disclose to the activity audience the relevant financial relationships of the planners, teachers, and authors involved in the development of CME content. An individual has a relevant financial relationship if he or she has a financial relationship in any amount occurring in the last 12 months with a commercial interest whose products or services are discussed in the CME activity content over which the individual has control.
The authors have no relevant financial relationships to disclose. Dr Aboulafia, CME Editor, has no relevant financial relationships to disclose. Dr D’Ambrosia, Editor-in-Chief, has no relevant financial relationships to disclose. The staff of OrthOpedics have no relevant financial relationships to disclose.
UNLABELED AND INVESTIGATIONAL USAGEThe audience is advised that this continuing medical
education activity may contain references to unlabeled uses of FDA-approved products or to products not approved by the FDA for use in the United States. The faculty members have been made aware of their obligation to disclose such usage.
cmeARTICLE
Evaluation of the Cellular Origins of Heterotopic OssificationLixin Kan, MD, PhD; John a. KessLer, MD
AbstrActHeterotopic ossification (HO), acquired or hereditary, is featured by the formation of bone outside of the normal skeleton. Typical acquired HO is a common, de-bilitating condition associated with trau-matic events. Cardiovascular calcifica-
tion, an atypical form of acquired HO, is prevalent and associated with high rates of cardiovascular mortality. Hereditary HO syndromes, such as fibrodysplasia ossificans progressiva and progressive osseous heteroplasia, are rare, progres-sive, life-threatening disorders. The cel-
As a result of reading this article, physicians should be able to:
1. Update the current knowledge about candidate cell populations as het-erotopic ossification (HO) contributors.
2. Understand the potential limitations of the experimental designs and tech-niques underlying the identification of putative HO contributors.
3. Clarify the confusion about the phenotypes of candidate populations in the literature.
4. Contrast the fundamental cellular differences between HO and normal skeletogenesis to identify potential disease-specific targets.
The authors are from the Department of Neurology (LK, JAK), Northwestern University’s Feinberg Medical School, Chicago, Illinois; and the Department of Pathophysiology (LK), School of Basic Medi-cine, Anhui Medical University, Anhui, China.
The material presented in any Keck School of Medicine of USC continuing education activity does not necessarily reflect the views and opinions of Orthopedics or Keck School of Medicine of USC. Neither Orthopedics nor Keck School of Medicine of USC nor the authors endorse or recommend any techniques, commercial products, or manufacturers. The authors may discuss the use of materials and/or products that have not yet been approved by the US Food and Drug Administration. All readers and continuing educa-tion participants should verify all information before treating patients or using any product.
Correspondence should be addressed to: Lixin Kan, MD, PhD, Department of Neurology, North-western University’s Feinberg School of Medicine, Ward Building 10-233, 303 E Chicago Ave, Chicago, IL 60611 ([email protected]).
Received: April 19, 2013; Accepted: November 22, 2013; Posted: May 14, 2014.doi: 10.3928/01477447-20140430-07
329

ORTHOPEDICS | Healio.com/Orthopedics
n Review Article
cmeARTICLE
lular origins of HO remain elusive. Some bona fide contributing cell populations have been found through genetic lineage tracing and other experiments in vivo, and various other candidate populations have been proposed. Nevertheless, be-cause of the difficulties in establishing cellular phenotypes in vivo and other confounding factors, the true identities of these populations are still uncertain. This review critically evaluates the accumulat-ing data in the field. The major focus is on the candidate populations that may give rise to osteochondrogenic lineage cells directly, not the populations that may contribute to HO indirectly. This issue is important not solely because of the clini-cal implications, but also because it high-lights the basic biological processes that govern bone formation. [Orthopedics. 2014; 37(5):329-340.]
Heterotopic ossification (HO), which commonly refers to bone formation at an abnormal ana-
tomical site, is a serious health problem. Typical acquired HO is a common and costly complication of various types of traumatic events, including fracture, total joint replacement (TJR), traumatic brain injury (TBI), spinal cord injury (SCI), or combat-related trauma.1,2 Cardiovascular calcification, an atypical acquired HO, is commonly associated with calcific aortic stenosis and other highly prevalent car-diovascular conditions that can eventu-ally lead to early cardiovascular mortal-ity.3,4 By contrast, hereditary syndromes of HO, such as fibrodysplasia ossificans progressiva (FOP) and progressive osse-ous heteroplasia (POH), are rare but pro-gressive and potentially life-threatening disorders.5,6 Gain-of-function mutations of activin A receptor, type I (ACVRI), a type I bone morphogenetic protein (BMP) receptor, are known to cause FOP, and loss-of-function mutations of the imprint-ing guanine nucleotide binding protein, alpha stimulating (GNAS) complex locus cause POH. Nevertheless, the identity of
the precursor cells that actually differen-tiate along the osteochondrogenic lineage to form HO—the so-called bona fide in vivo HO contributors—remains unclear in these disorders as well as in acquired HO. Thus, a broad spectrum of various cell populations have been proposed as candidates to be HO contributors (Table).
The aims of the current review are to:1. Evaluate candidate cell popu-
lations as HO contributors and delineate the hierarchical relationships among these populations, based on current data;
2. Objectively weigh the experi-mental designs and techniques underlying the identification of putative HO contribu-tors and discuss potential limitations;
3. Clarify the profound confusion about the phenotypes of candidate popu-lations in the literature;
4. Critically evaluate the mecha-nisms underlying osteogenic induction of different contributing populations;
5. Contrast the fundamental cel-lular differences between HO and nor-mal skeletogenesis to identify potential disease-specific targets; and
6. Briefly discuss the practical im-plications and future directions.
cAndidAte PoPulAtionsThe numerous candidate populations
can be categorized according to their original germ layer (ectoderm, mesoderm, or endoderm), their original location (lo-cal or bone marrow/circulating), or their stemness (pluripotent and multipotential stem cells, bipotential progenitors, com-mitted progenitors, or terminally differen-tiated cells).
Candidate Populations of Ectoderm Origin
There are only limited data that suggest that ectoderm-derived cells contribute to HO.7-9 As early as the 1970s, Anderson9 reported that FL, HeLa, and other nonmu-rine epithelial cells are capable of induc-ing chondro-osseous differentiation when brought into contact or close proxim-
ity with mouse thigh mesenchymal cells. Anderson9 hypothesized that short-range diffusion of inductive substance(s) and/or direct inductive stimuli from epithelial cells might be responsible for the osteo-genic activities. Boyan et al7 later reported that intramuscularly implanted epithelial cell lines (FL and WISH cells) produced tumors and induced large islands of bone with focal areas of cartilage immediately adjacent to the tumors. Although the con-sistent finding was interesting, these stud-ies did not address the key question of which cells—donor, host, or both—gave rise to osteogenic lineage cells and turned into bone.
Rutherford et al8 further reported that BMP-7–transduced human oral keratino-cyte cells (HOKC) induced ectopic bone. To further clarify whether these cells give rise to osteogenic lineage cells them-selves, they implanted BMP-7–transduced HOKC into a diffusion chamber that ex-cluded the host cells from infiltrating into and donor epithelial cells out of the cham-ber. They found that no bone-like tissue formed within diffusion chambers, al-though ectopic bones still formed close to the implanted diffusion chamber.8 These observations suggested that the host cells, not donor epithelial cells, turned into bone in response to osteogenic factors.
Theoretically, cells of ectoderm ori-gin could give rise to osteogenic lin-eage cells and directly contribute to HO through the process of epithelial-to-mes-enchymal transition (EMT). Epithelial-to- mesenchymal transition was a paradigm that evolved first from observations of early embryonic development, and EMT is a necessary first step for normal em-bryonic skeletogenesis. In adults, EMT also plays a key role in various conditions such as fibrosis, wound repair, inflam-mation, and malignancy.10 Epithelial-to-mesenchymal transition can generate cells with stem cell properties in vitro,11 and theoretically such epithelium-derived mesenchymal cells could then give rise to osteogenic lineage cells and contribute to
330

MAY 2014 | Volume 37 • Number 5
n Review Article
cmeARTICLE
HO. However, there are currently no data to substantiate this hypothesis. Moreover, studies of POH, which is characterized by HO formation in skin (an ectoderm derivative), find no evidence of ectoder-mal cell contribution to HO.12 To summa-rize, currently available data suggest that epithelial cells may secrete BMP or other osteogenic factors and thereby contribute
to HO indirectly, but they do not directly give rise to osteolineage cells.
Candidate Populations of Endoderm Origin
Although some observations suggest that cells of endoderm origin can con-tribute directly to HO, the overwhelming body of evidence indicates that endoder-
mal cells contribute to HO only indirectly, similar to cells of ectodermal origin. The available data supporting a possible role for endodermal lineage cells come from 3 lines of evidence.
Data From In Vitro Experiments. Aguilar-Vázquez et al13 reported that hu-man umbilical vein endothelial cells (ECs) can differentiate along an osteogenic lin-
Table
Summary of Potential Candidate Heterotopic Ossification–Contributing Populations
Germ Layer and Population
In Vitro Osteogenic Potential?
Indirect Contribution to
HO?In Vivo HO
Contributor? Reference
Cells of ectoderm origin
Epithelial cell lines (FL, HeLa, WISH) No Yes No 7, 9
BMP-7–transduced HOKCs No Yes No 8
Cells of endoderm origin
Human umbilical vein ECs Yes - No 13
Mitral valve leaflets ECs Yes - No 14
CEPCs No - No 14
CEPCs Yes - - 15, 16
ECs (Tie2-labeled cells) Yes? - Yes? 19
ECs No Yes No
Cells of mesoderm origin
MSCs Yes - Yes? 45
PCMOs Yes - - 70
Tie2-labeled cells Yes - No 21
GLAST-CreERT - - Yes 2
Mesenchymal progenitor cells Yes - Yes 55, 74, 75, 76
Muscle satellite cells Yes - No 1, 79, 80
MOPCs - - Yes 83, 84
COPs Yes - Yes 85
CD34-mesenchymal precursor cells Yes - - 86
Circulating fibrocytes Yes - - 87
Marrow-derived myeloid precursors Yes - - 88, 90
Cells of hematopoietic origin Yes - No 1, 93
SMCs Yes - Yes? 4, 20, 94, 95
Fibroblasts/fibrocytes Yes - - 101, 102
Myofibroblasts Yes - - 110
Pericytes Yes - No? 115
Abbreviations: BMP-7, bone morphogenetic protein 7; CEPCs, circular endothelial progenitor cells; COPs, circulating osteogenic precursor cells; ECs, endothelial cells; GLAST, glutamate aspartate transporter; HOKCs, human oral keratinocyte cells; MOPCs, circulating bone marrow–derived osteoblast progenitor cells; MSCs, mesenchymal stem cells; PCMOs, programmable cells of monocytic origin; SMCs, smooth muscle cells.
331

ORTHOPEDICS | Healio.com/Orthopedics
n Review Article
cmeARTICLE
eage in culture, but this result has not been repeated. Wylie-Sears et al14 reported that mitral valve leaflets contain ECs with multilineage mesenchymal differentiation potential, including osteogenic differentia-tion, but they nevertheless agree that this is not a universal property of ECs.
Data From Circulating Endothelial Progenitor Cells. Gössl et al15 reported that circulating endothelial progenitor cells (CEPCs) in patients with coronary athero-sclerosis express osteocalcin (OCN), an os-teoblastic marker. Peris et al16 reported that bisphosphonate treatment downregulates expression of osteogenic genes in CEPCs, suggesting a possible mechanism by which bisphosphonates may inhibit vascular cal-cification. However, Wylie-Sears et all4 reported that CEPCs have no osteogenic potential. Three major issues complicate drawing meaningful conclusions about CEPCs: (1) Because there is no consensus on CEPC-defining markers,17 identification of such cells is problematical; (2) the num-ber of putative CEPCs in peripheral blood is exceedingly low, which makes it implau-sible that they have a significant effect on pathophysiological processes, such as HO; and (3) there is no evidence that CEPCs ac-tually contribute to HO in vivo.
Data In Vivo. Similar to cells of ecto-dermal origin, ECs can undergo a process termed endothelial-mesenchymal transi-tion (EndMT), which is of importance in mediating many physiological and patho-logical processes. The observation that prostate tumor ECs can undergo EndMT and generate ectopic calcification is con-sistent with the idea that cells of endoderm origin could be contributors to HO.18 Fur-thermore, constitutively activated ACVRI (found in FOP) caused morphological changes of ECs to mesenchymal-like cells and induced coexpression of the mesen-chymal markers in vitro, a process similar to EndMT.19 Importantly, these cells could differentiate into the osteogenic lineage.19
Cells in FOP chondrogenic lesions coexpress Tie2 and vWF, putative endo-thelial markers, with the chondrogenic
gene SOX9, whereas osteogenic lesions coexpress Tie2 and vWF with the osteo-genic marker OCN.19 These observations were interpreted as evidence that EC can be contributors to HO. Furthermore, Cre-lox–based genetic lineage tracing in vivo with Tie2-cre also found that Tie2-labeled cells contribute significantly to all stages of HO.20,21 The current authors also found that Tie2-labeled cells contrib-ute significantly to normal skeletogenesis (Figure). Unfortunately, Tie2 is not a specific marker of ECs, which limits any conclusions about lineage contributions to HO based on Tie2 expression. Tie2 is expressed by at least 3 distinct cell types: ECs, proangiogenic monocyte cells of hematopoietic origin, and pericyte precur-sors of mesenchymal origin. In addition, in the lineage-tracing studies cited previ-ously, Tie2 expression was also detected in BMP-induced lesional cells themselves, raising the possibility that Cre-dependent labeling resulted from de novo Tie2-Cre expression rather than reflecting a direct relationship with the Tie2+ lineage.21 Im-portantly, transplantation of the endothe-lial fraction of Tie2+ cells (Tie2+CD31+) does not contribute to HO, whereas the nonendothelial fraction of Tie2+ cells (Tie2+CD31-) does contribute. Moreover, lineage tracing with another Cre line, VE-Cadherin-Cre, which specifically labels endothelium/endothelial precursors, did not contribute to HO in an appreciable manner.21 Together, these data strongly suggest that Tie2+ progenitor cells that contribute to HO in vivo are not of endo-thelial origin.21
Thus, there are no convincing data that endodermal cells themselves give rise to osteogenic lineage cells in vivo. In contrast, substantial evidence suggests that ECs regulate osteogenic differen-tiation of other cells (mesenchymal cells) and contribute to HO indirectly, likely through mechanisms of paracrine or EC- mesenchymal cells crosstalk.22-44 This leaves cells of mesoderm origin as the major direct contributors to HO.
Candidate Populations of Mesoderm Origin
Because many proposed candidate populations are of mesoderm origin, the authors review these populations sequen-tially according to their stemness.
Mesenchymal Stem Cells. In 1970s, Friedenstein et al45 established an assay to examine the clonogenic potential of plastic-adherent marrow cells. Subsequent experiments revealed the remarkable plas-ticity of these marrow-derived cells and how their fate could be determined by en-vironmental cues. These observations led to the hypothesis that most cells of adult mesodermal origin are differentiated from these mesenchymal fibroblast-like stem cells (variously referred to as mesenchymal stem cells [MSCs], mesenchymal stromal cells, bone marrow stromal cells [BMSCs], or skeletal stem cells [SSCs]). Mesenchy-mal stem cells can be isolated from many tissues, including the umbilical cord,46 bone marrow,47,48 adipose tissue,49 adult and fetal muscle,50 corneal stroma,51 glom-eruli,52,53 placenta,54 aortic valve,55 human parathyroid gland,56 endometrium,57 scalp skin,58 human amniotic membrane,59 hu-man neonatal thymus,60 dental pulp of de-ciduous baby teeth,61 liver,62 synovium,63 pancreas,64 lung,65 or amniotic fluid66 by simple plastic-adherent culture. Mesen-chymal stem cell–like cells can also come from circulation or suspension culture.67-69 Pufe et al70 also reported that peripheral ve-nous blood contained programmable cells of monocytic origin (PCMOs) that have multilineage potential comparable with that of MSCs and can generate collagen type II–producing chondrocytes.
The characteristic features of MSCs are the abilities to self-renew and to dif-ferentiate into all mesoderm-type lineag-es, including osteoblasts, chondrocytes, adipocytes, smooth muscle cells, and myocytes, but not hematopoietic cells. Mesenchymal stem cells have been used to produce bony implants and in the repair of bony defects,48 and the potential of hu-man MSCs for osteogenic differentiation
332

MAY 2014 | Volume 37 • Number 5
n Review Article
cmeARTICLE
has been confirmed in immunocompro-mised mice.71 Choi et al72 also reported that undifferentiated human adipose tissue–derived MSCs can differentiate into osteocytes or osteoblasts in athymic nude rat calvaria. These observations sug-gest MSCs as a prime candidate popula-
tion for contributing to HO. Although unequivocal demonstration of MSC con-tribution to HO has not been possible because of technical limitations and the lack of unequivocal MSC-specific mark-ers, independent data from lineage tracing and other experiments provide strong evi-
dence that tissue-resident MSC/progeni-tor cell populations represent bona fide cells of origin for HO.2,21
Wosczyna et al21 reassessed Tie2+ progenitors and found that, unlike the endothelial fraction of Tie2, the non- endothelial fraction consistently incorpo-
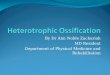
Figure: Significant numbers of FoxD1-Cre– and Tie2-Cre–labeled (but not glutamate aspartate transporter [GLAST]-Cre–labeled) cells were detected in normal bones and bone marrow. Typical fluorescence image showing no appreciable GLAST-Cre–labeled cells (green) in the bone marrow of adult GLAST-Cre;Zsgreen mice (A). Typical fluorescence image showing significant numbers of FoxD1-Cre–labeled cells (green) in the bone marrow of adult FoxD1-Cre;Zsgreen mice (B). Typical LacZ staining of the bone marrow of adult Tie2-Cre;ROSA26 mice showing significant numbers of Tie2-Cre–labeled cells (dark blue) (C). Typical fluo-rescence image showing GLAST-Cre–labeled cells (green) in the periosteum and surrounding connective tissues of long bones (femur shown here); few labeled cells were found within the osseous tissue of adult GLAST-Cre;Zsgreen mice (D). Typical fluorescence image showing significant numbers of FoxD1-Cre–labeled cells (green) in tail vertebrae of adult FoxD1-Cre;Zsgreen mice (E). Typical LacZ staining showing significant numbers of Tie2-Cre–labeled cells (dark blue) in tail vertebrae of adult Tie2-Cre;ROSA26 mice (F). Broken lines in Figures D through F outline the boundaries between the bony structures and the associated con-nective tissues. Nucleic DAPI counterstains in (A, B, D, and E) are in blue, and fast red counterstains in (C and F) are in red. Abbreviation: NP, nucleus pulposus of the intervertebral disk.
333

ORTHOPEDICS | Healio.com/Orthopedics
n Review Article
cmeARTICLE
rated into chondrogenic and osteogenic lesions. Further fractionation implicated the nonendothelial and nonhematopoi-etic fraction of Tie2+ cells (Tie2+CD31-
CD45-) cells as the major contributor to HO. More than 90% of these cells were PDGFRa+Sca1+ (both are MSC/progenitor cell markers), suggesting a mesenchymal, not endodermal, ori-gin of these cells. Clonal analysis of the Tie2+PDGFRa+Sca1+ cells demonstrated both BMP-2–dependent osteogenic dif-ferentiation and BMP-2–independent ad-ipogenic and smooth muscle/fibroblastic differentiation, suggesting that these cells are indeed multipotent.21
A recent lineage-tracing study by Kan et al2 suggested that another subpopula-tion of mesenchymal progenitor/stem cells, glutamate aspartate transporter (GLAST)-expressing cells, may also be a contributor to HO. They tested 2 Cre lines, GLAST-CreERT and FoxD1-Cre, and found that both of these Cre lines la-beled similar mesenchymal populations in subcutaneous connective tissue and in the interstitium of skeletal muscles with slightly different labeling profiles. Inter-estingly, many of the labeled cells, either GLAST-CreERT or FoxD1-Cre labeled, were closely associated with the vascula-ture but did not colocalize with EC mark-ers. Remarkably, the FoxD1-Cre–labeled cells contributed significantly to normal endogenous bone formation, but the con-tribution of the FoxD1-Cre–labeled popu-lation to HO was negligible. By contrast, GLAST-CreERT–labeled cells did not contribute significantly to normal bone formation, but they contributed signifi-cantly to HO at all stages.2
Colabeling studies indicate that the FoxD1-Cre– and GLAST-CreERT– labeled cells partially overlap with each other (both colabeled with a battery of mesenchymal progenitor/stem cell mark-ers), but both only minimally colabel with Tie2, suggesting that they are large-ly independent populations.2 Significant numbers of FoxD1+ and Tie2+, but not
GLAST-CreERT+ cells are found within bone marrow (Figure), suggesting that GLAST-CreERT–labeled cells that con-tribute to HO do not arise from bone mar-row. FoxD1+ mesenchymal cells give rise to pericytes, and FoxD1-derivative inter-stitial cells expand and differentiate into SMA+ myofibroblasts during fibrosis in the kidney,73 consistent with the possibil-ity that they are stem cells. However, the multipotentiality of GLAST-CreERT– or FoxD1–labeled cells has not been directly tested, and it is unclear whether GLAST-CreERT– and/or FoxD1–labeled cells are indeed MSC or just bipotent or even unipotent progenitors. Moreover, the pre-cise hierarchical relationship between FoxD1+, Tie2+, and GLAST-CreERT+ populations is still unclear.
Mesenchymal Progenitor Cells. Mes-enchymal progenitor cell is a general term that refers to any undifferentiated cell of mesenchymal origin, excluding progeni-tor cells of hematopoietic origin. This term is also sometimes used interchange-ably with MSC and others, such as fibro-blasts/fibrocytes, which creates confusion in the field. Another confusing fact is that mesenchymal progenitor cells can be tri-potent, bipotent, or unipotent progenitor cells. Numerous reports suggest that both local and circulating mesenchymal pro-genitor cell populations may contribute to HO. As early as 1975, Buring74 proposed that the cell populations that develop into osteoblasts and osteocytes in response to osteoinductors are the progeny of perivas-cular mesenchymal cells. Later experi-ments showed that human skeletal muscle contains osteogenic progenitor cells.75,76 These cells can be easily cultured and ex-panded based on cell adhesion character-istics, but the true identities of these high-ly proliferative cells (positive for HOP-26, a marker of pericytes), are unclear.
In a grafted periosteum model, Ueno et al75 found that grafted periosteum forms bone by endochondral ossification and that the osteogenic progenitor cells in the fibrous layer of long bone contribute to
chondrogenesis. Analyses in vitro and lin-eage-tracing experiments in vivo in a new bone formation (fracture-healing) model with a smooth muscle actin-CreERT2 (SMA-CreERT2) confirmed the osteogen-ic phenotype of smooth muscle a-actin (aSMA)-positive mesenchymal progeni-tor cells.76 Although Grcevic et al76 called these aSMA-CreERT2–labeled cells mes-enchymal progenitor cells, the cells were heterogeneous (a high proportion of these cells expressed both hematopoietic cell [CD45] as well as MSC [Sca1] mark-ers), and the true identity is still unknown. Chen et al55 claimed that valve interstitial cells (VICs) contain mesenchymal pro-genitor cells with robust osteogenic calci-fication potential55 as well as adipogenic, chondrogenic, and myofibrogenic poten-tial, similar to MSCs. However, it has been reported that although osteogenic VICs displayed an osteoblast-like pheno-type, there were stark differences between the VIC-derived cells and other true osteo-blastic cell types, implying that VICs may not have true osteogenic potential.77
In keeping with the uncertainty about the contribution of the general mesenchy-mal progenitor cell pool to HO, some sub-populations, such as muscle satellite cells, have been virtually excluded as potential contributors to HO, whereas the evidence for others, such as circulating osteogenic mesenchymal precursors, is stronger.
Muscle-specific Mesenchymal Progen-itor Cells. Mesenchymal progenitor cells located in muscle tissue are also termed muscle satellite cells. Wada et al78 report-ed that muscle satellite cells in adult mice can differentiate into osteoblasts, adipo-cytes, and myotubes. Hashimoto et al79 reported that human myogenic progenitor cells retain the capacity to act as osteopro-genitor cells that form ectopic bone spon-taneously. Similarly, rat skeletal muscle myoblasts (L6)80 and a mouse myoblast (C2C12)81 cell line expressed osteogenic phenotypes when induced with BMP. However, more vigorous in vivo lineage tracing, with myogenic lineage mark-
334

MAY 2014 | Volume 37 • Number 5
n Review Article
cmeARTICLE
ers (Myf5-Cre and MyoD-Cre) found that neither Myf5-Cre– nor MyoD-Cre– labeled myogenic progenitors contribute to HO directly, which virtually excluded local myogenic progenitors as candidate populations of HO.1,20
Circulating Osteogenic Mesenchymal Precursors. Circulating mesenchymal progenitor cells can be either hemato-poietic or nonhematopoietic, although the original, more exclusive definition of mesenchymal progenitor cells excluded hematopoietic progenitors. Recent studies suggest the existence of an array of differ-ent osteogenic mesenchymal precursors in the circulation. For example, Otsuru et al82 examined the contribution to HO of bone marrow–derived osteoblast pro-genitor cells (MOPCs) in a BMP-induced model following GFP+ bone marrow transplantation in mice and found a signif-icant number of GFP+ osteoblastic cells in the newly generated HO. This study sug-gests that bone marrow–derived MOPCs could be an important contributor to HO in vivo. In a subsequent study, Otsuru at al83 further analyzed cell surface markers of these MOPCs and found that they ex-press CD44 and CXCR4 but not hemato-poietic (eg, CD45) or endothelial lineage markers, suggesting a mesodermal origin of these cells. Notably, MOPCs are not the same as either the previously mentioned CEPC15 or the circulating osteogenic precursor cells reported by Suda et al.84 Circulating osteogenic precursor cells are bone marrow–derived collagen I+/CD45+ mononuclear adherent cells, which are present in early preosseous fibroprolifera-tive lesions in patients with FOP and HO in a murine in vivo implantation assay.84 Because these cells are CD45+, they are likely hematopoietic in origin. Zvaifler et al85 reported that in the circulation of normal individuals, there is a small popu-lation of CD34- mesenchymal precursor cells that proliferate rapidly in culture as an adherent population but with variable morphologies. These cells can differenti-ate into several lineages, including fibro-
blasts, osteoblasts, and adipocytes.85 Choi et al86 found that bone marrow–derived human circulating fibrocytes (CD34+, CD45+, Col I+, fibronectin+, and CXCR4+) behave as mesenchymal progenitor cells and have the capacity to differentiate into osteoblasts and chondrocytes. However, Kuznetsov et al87 reported that such stem cells are found reproducibly in guinea pigs, mice, and other animals but rarely in postnatal humans.
Doehring et al88 further reported that bone marrow–derived myeloid precursors (CD34+ CD13+) give rise to chondrocyte-like cells in atherosclerotic intima calcifi-cation through transdifferentiation. Shafer et al89 suggested that early chondrocyte progenitors in atherosclerotic lesions are of circulating myeloid origin. Similarly, Olmsted-Davis et al90 reported that primi-tive adult hematopoietic stem cells, a self-renewing population of bone marrow– derived cells (Lin- Sca1+ cKit+ CD45+), can generate functional osteoblasts through a mesenchymal intermediate, in-dicating an extended potential of this pop-ulation. Furthermore, in a rabbit total hip arthroplasty model, Rumi et al91 reported that osteoprogenitor cells responsible for HO originate predominantly from bone marrow but also from local (hip abduc-tors) sources. However, after bone marrow transplantation into an FOP patient, cells of hematopoietic origin contributed only to the early inflammatory and late marrow- repopulating stages of BMP-4–induced HO but were not represented in the fibro-proliferative, chondrogenic, or osteogenic stages.92 Furthermore, lineage tracing in vivo with multiple hematopoietic lineage markers, such as Lyz-Cre (which labels the hematopoietic stem cell/monocyte/macrophage lineage), CD19-Cre (B-cells lineage), and LCK-Cre (T-cells lineage), found no evidence that circulating hema-topoietic progenitors contribute directly to HO.1
Overall, although the data for the he-matopoietic precursor cells convincingly exclude these cells as direct contributors
to HO, the current data for nonhematopoi-etic circulating mesenchymal precursor cells are insufficient to draw a firm con-clusion.
Other Mesenchymal Cells. There is some provocative but incomplete evidence that suggests that even some terminally differentiated mesenchymal cells, such as smooth muscle cells (SMCs), fibroblasts/fibrocytes, and pericytes, can give rise to osteogenic lineage cells and potentially contribute to HO.
Smooth muscle cells are unstriated, spindle-shaped, terminally differentiated cells that normally form thin layers or sheets in the walls of the internal organs, such as the stomach, intestine, bladder, and blood vessels. Smooth muscle cells express high levels of smooth muscle ac-tin (SMA) and can contract without con-scious control. Liu et al93 demonstrated that hepatocyte growth factor (HGF) can induce osteogenic differentiation of vas-cular SMCs via c-Met/Akt/Notch3 sig-naling in vitro. Yan et al94 also reported that oxidative stress-mediated decorin glycosaminoglycan (GAG) chain synthe-sis triggers transforming growth factor-ß signaling and osteogenic differentiation of vascular SMCs in vitro. Shimizu et al95 further reported that azelnidipine, a dihy-dropyridine subclass of calcium channel blockers, inhibits Msx2-dependent osteo-genic differentiation and matrix mineral-ization of vascular SMCs in vitro. Using an SMC-specific SM22-Cre line, Speer et al4 found that SM22-Cre–labeled cells gave rise to osteochondrogenic precursor and chondrocyte-like cells in calcified blood vessels of matrix Gla protein defi-cient (MGP-/-) mice in vivo. Furthermore, they found that the potential fate change of SMCs occurred before calcium depo-sition. Based on these data, they hypoth-esized that adult SMCs can transdifferen-tiate and that SMC transdifferentiation is an important process that drives vascular calcification.4 Similarly, Bobryshev96 also found some SMCs with a reduced content of aSMA (an SMC marker) and increased
335

ORTHOPEDICS | Healio.com/Orthopedics
n Review Article
cmeARTICLE
Sox9 (a chondrocyte or chondroprogeni-tor marker) in atherosclerotic plaques in vivo, again suggesting that transdifferen-tiation of SMC into chondrocytes contrib-utes to atherosclerotic calcification.
The term transdifferentiation was orig-inally coined by Selman and Kafatos97 in 1974 to describe the change in cell prop-erties as cuticle-producing cells became salt-secreting cells in silk moths undergo-ing metamorphosis. Currently, transdif-ferentiation is defined as a process where one mature somatic cell type transforms into another mature somatic cell without undergoing an intermediate pluripotent state or progenitor cell type.98 Although transdifferentiation has been demonstrat-ed frequently in vitro, only rare examples of transdifferentiation have been shown in vivo. Thus, the physiological or patho-physiological significance of this process in vivo is still in question. Furthermore, transdifferentiation is not the only pos-sible interpretation of the aforementioned data. For example, based on other lineage-tracing experiments, it is reasonable to ar-gue that the SM22-Cre– or aSMA-labeled cells that contributed to HO may actually be mesenchymal progenitor cells or even myofibroblasts, not SMCs. Grcevic et al76 posited that the aSMACre-ERT2–labeled cells that contribute to ossifica-tion are mesenchymal progenitor cells, not SMCs. In addition, Lounev et al20 found that another SMC-specific Cre line, SMMHC-Cre, did not contribute cells to BMP-induced HO, which argues against a direct contribution of SMCs to HO. Fur-thermore, because myofibroblasts are also aSMA+ (and colabel with SM22), it is possible that SM22-Cre–labeled cells are actually myofibroblasts, not to mention the additional possibility of cell fusion. Thus, the issue of whether SMCs have osteogenic potential is unresolved and awaits the development of a Cre line that exclusively labels SMCs.
Fibroblasts and fibrocytes are thought to be 2 states of the same cells, and cur-rently there is a tendency to call both
forms fibroblasts. Although all fibroblasts are morphologically similar, they are likely heterogeneous. For example, clonal analysis of dermal fibroblasts showed that 6.4% of the single-cell–derived clones were tripotent, 19.1% of the clones were bipotent, and 10.6% of the clones were unipotent, suggesting that fibroblasts comprise a heterogeneous population in-cluding progenitors with various levels of differentiation potential.99 For example, it was reported that it is possible to isolate a multipotent MSC subpopulation from human gingival fibroblasts by culturing on chitosan membranes.100 Adding to the confusion, fibroblasts are sometimes re-ferred to as myofibroblasts, especially in their activated differentiated state,101 and the term fibrocytes has sometimes been used interchangeably with mesenchymal progenitor cells.102,103 Because there are apparently multipotential subpopulations in fibroblasts, it is not surprising that fi-broblasts can reportedly differentiate into both osteoblastic104 and osteoclast-like cells.105 Numerous reports have suggested the existence of circulating fibrocytes, and Choi et al86 found that human circu-lating fibrocytes have the capacity to dif-ferentiate osteoblasts and chondrocytes. However, the contribution of fibroblasts/fibrocytes to HO in vivo has not been vig-orously tested, partially due to a lack of specific markers and Cre lines.
Myofibroblasts are intriguing cells that include phenotypic traits of both fibro-blasts and SMCs. They are a-SMA+ fibro-blast-like cells that are closely associated with connective tissue matrix remodeling/repair106 and other pathological condi-tions. Myofibroblasts are found subepi-thelially in many mucosal surfaces and are involved in fibrosis, wound strengthening, and contraction. Confusingly, pericytes, another mesenchymal cell subpopulation, are sometimes called modified myofibro-blast cells.
Myofibroblasts may be derived from many different origins, including SMCs, stellate cells, mesenchymal progenitor
cells resident in a stromal tissue, circu-lating mesenchymal precursors, or even epithelial cells through EMT.107 In turn, myofibroblasts are capable of differenti-ating into various cell types both in vitro and in vivo, including calcified vascular cells and osteoblasts, and are known to be involved in the ossification of heart valves and arteries.108 Because myofibroblasts colabel with SM22, some of the previous-ly discussed findings about the putative osteogenic potential of SMCs may actu-ally reflect the lack of distinction from myofibroblasts.109
Pericytes, also known as Rouget cells or mural cells, are defined by their ana-tomic features in vivo. They are contrac-tile cells that wrap around the ECs of cap-illaries and venules, where they play key physiological roles through communica-tion with ECs. Recently, it has become appreciated that these cells have impres-sive stem/progenitor cell–like features. Pericytes reportedly have osteogenic potential in vitro110,111 and in vivo112 and are capable of giving rise to cells of mul-tiple lineages, including chondrocytes, adipocytes, and fibroblasts, as well as osteoblasts. Some investigators even be-lieve that all MSCs are pericytes,113 and it is conceivable that pericytes and MSCs are 2 states of the same cells, similar to fibroblasts and fibrocytes. Interestingly, a subpopulation of pericytes are among the cell types that express GLAST.114 More importantly, the characteristic anatomic distribution and the labeling pattern of GLAST-CreERT–labeled cells in the re-cent study by Kan et al2 are consistent with the idea that some or all of the these GLAST-CreERT–labeled cells that con-tribute to HO may be pericytes. However, a lineage-tracing study with an NG2-Cre line (intended to label pericytes) showed no significant contribution of labeled cells to HO.115 Nevertheless, the heterogene-ity of pericytes114 and the lack of valida-tion of the NG2-Cre line make it unclear whether these negative data are sufficient to exclude the candidacy of pericytes.
336

MAY 2014 | Volume 37 • Number 5
n Review Article
cmeARTICLE
contrAst between HeterotoPic ossificAtion And normAl skeletogenesis
Although there is substantial debate about the cellular origins of HO, it has generally been thought that the processes leading to HO and the formation of nor-mal bone are largely the same because HO produces bone that faithfully replicates the appearance of normal bone. However, studies of the cellular origins of HO pro-vide substantial evidence to challenge this dogma:
(1) It is known that EMT is a necessary first step for normal, embryonic skeleto-genesis. Although EMT can also generate cells with properties of stem cells in vitro,11 there is currently no evidence that epithe-lia can give rise to osteogenic lineage cells and/or contribute to HO through EMT in vivo in adults. This is indirect evidence that embryonic skeletogenesis and HO in adults may have different cellular origins.
(2) In a recent study, Kan et al2 found that FoxD1-Cre–labeled cells contribute significantly to normal skeletogenesis but not to HO at any stage, whereas GLAST-CreERT–labeled cells are just the oppo-site (ie, they do not contribute to normal skeletogenesis but are a major contributor to HO). This provides direct evidence of different cellular origins for embryonic skeletogenesis and HO in adults.
(3) Nevertheless, Tie2-labeled cells contribute to both HO and normal skeleto-genesis (Figure), suggesting that HO and normal skeletogenesis are not completely unrelated and that some populations may participate in both processes.
Understanding the differences in the cellular mechanisms underlying HO and normal skeletogenesis is not only of high scientific interest but will also be critical for identifying disease-specific molecular loci for therapeutic intervention.
conclusionThe preponderance of evidence sug-
gests that mesenchymal—not endodermal or ectodermal—populations are the major
bona fide populations of cells that contrib-ute to HO. However, more detailed stud-ies in vivo are necessary to completely exclude the candidacies of endodermal or ectodermal populations.
It is likely that more than one subpopu-lation of stem/progenitor cells contributes to HO, and further studies are necessary to identify the predominant contribut-ing subpopulations. This may eventually identify specific cellular targets for pos-sible therapeutic intervention.
Due to lack of deep understanding of different mesenchymal subpopulations, the precise identities and hierarchical re-lationships among HO contributing popu-lations are still unclear.
Recent data suggest that HO and nor-mal skeletogenesis have different cellular origins. Thus, additional studies are need-ed to explore potential disease-specific loci for future therapeutic intervention.
references 1. Kan L, Liu Y, McGuire TL, et al. Dysregula-
tion of local stem/progenitor cells as a com-mon cellular mechanism for heterotopic os-sification. Stem Cells. 2009; 27(1):150-156.
2. Kan L, Peng CY, McGuire TL, Kessler JA. Glast-expressing progenitor cells contrib-ute to heterotopic ossification. Bone. 2013; 53(1):194-203.
3. Nakagawa Y, Ikeda K, Akakabe Y, et al. Para-crine osteogenic signals via bone morphoge-netic protein-2 accelerate the atherosclerotic intimal calcification in vivo. Arterioscler Thromb Vasc Biol. 2010; 30(10):1908-1915.
4. Speer MY, Yang HY, Brabb T, et al. Smooth muscle cells give rise to osteochondrogenic precursors and chondrocytes in calcifying ar-teries. Circ Res. 2009; 104(6):733-741.
5. Pignolo RJ, Shore EM, Kaplan FS. Fibro-dysplasia ossificans progressiva: clinical and genetic aspects. Orphanet J Rare Dis. 2011; 6:80.
6. Zhang S, Kaplan FS, Shore EM. Different roles of GNAS and cAMP signaling during early and late stages of osteogenic differen-tiation. Horm Metab Res. 2012; 44(10):724-731.
7. Boyan BD, Swain LD, Schwartz Z, Ramirez V, Carnes DL Jr. Epithelial cell lines that in-duce bone formation in vivo produce alkaline phosphatase-enriched matrix vesicles in cul-ture. Clin Orthop Relat Res. 1992; (277):266-276.
8. Rutherford RB, Racenis P, Fatherazi S, Izut-
su K. Bone formation by BMP-7-transduced human gingival keratinocytes. J Dent Res. 2003; 82(4):293-297.
9. Anderson HC. Osteogenetic epithelial-mes-enchymal cell interactions. Clin Orthop Relat Res. 1976; (119):211-223.
10. Kovacic JC, Mercader N, Torres M, Boehm M, Fuster V. Epithelial-to-mesenchymal and endothelial-to-mesenchymal transition: from cardiovascular development to disease. Cir-culation. 2012; 125(14):1795-1808.
11. Mani SA, Guo W, Liao MJ, et al. The epithe-lial-mesenchymal transition generates cells with properties of stem cells. Cell. 2008; 133(4):704-715.
12. Liu JJ, Russell E, Zhang D, Kaplan FS, Pi-gnolo RJ, Shore EM. Paternally inherited gsalpha mutation impairs adipogenesis and potentiates a lean phenotype in vivo. Stem Cells. 2012; 30(7):1477-1485.
13. Aguilar-Vázquez R, Carballo-Molina OA, Collazo-Navarrete O, et al. Osteogenesis of human vascular endothelial cells in cul-ture [in Spanish]. Rev Invest Clin. 2008; 60(6):496-501.
14. Wylie-Sears J, Aikawa E, Levine RA, Yang JH, Bischoff J. Mitral valve endothelial cells with osteogenic differentiation poten-tial. Arterioscler Thromb Vasc Biol. 2011; 31(3):598-607.
15. Gössl M, Mödder UI, Atkinson EJ, Lerman A, Khosla S. Osteocalcin expression by cir-culating endothelial progenitor cells in pa-tients with coronary atherosclerosis. J Am Coll Cardiol. 2008; 52(16):1314-1325.
16. Peris P, Atkinson EJ, Gössl M, et al. Effects of bisphosphonate treatment on circulating osteogenic endothelial progenitor cells in postmenopausal women. Mayo Clin Proc. 2013; 88(1):46-55.
17. Timmermans F, Plum J, Yöder MC, Ingram DA, Vandekerckhove B, Case J. Endothelial progenitor cells: identity defined? J Cell Mol Med. 2009; 13(1):87-102.
18. Dudley AC, Khan ZA, Shih SC, et al. Calcifi-cation of multipotent prostate tumor endothe-lium. Cancer Cell. 2008; 14(3):201-211.
19. Medici D, Shore EM, Lounev VY, Kaplan FS, Kalluri R, Olsen BR. Conversion of vas-cular endothelial cells into multipotent stem-like cells. Nat Med. 2010; 16(12):1400-1406.
20. Lounev VY, Ramachandran R, Wosczyna MN, et al. Identification of progenitor cells that contribute to heterotopic skeletogenesis. J Bone Joint Surg Am. 2009; 91(3):652-663.
21. Wosczyna MN, Biswas AA, Cogswell CA, Goldhamer DJ. Multipotent progenitors resi-dent in the skeletal muscle interstitium exhib-it robust BMP-dependent osteogenic activity and mediate heterotopic ossification. J Bone Miner Res. 2012; 27(5):1004-1017.
22. Bulnheim U, Müller P, Neumann HG, et al. Endothelial cells stimulate osteogenic differ-
337

ORTHOPEDICS | Healio.com/Orthopedics
n Review Article
cmeARTICLE
entiation of mesenchymal stem cells on cal-cium phosphate scaffolds [published online ahead of print October 5, 2012]. J Tissue Eng Regen Med.
23. Steiner D, Lampert F, Stark GB, Finkenzeller G. Effects of endothelial cells on prolif-eration and survival of human mesenchymal stem cells and primary osteoblasts. J Orthop Res. 2012; 30(10):1682-1689.
24. Saleh FA, Whyte M, Genever PG. Effects of endothelial cells on human mesenchymal stem cell activity in a three-dimensional in vitro model. Eur Cell Mater. 2011; 22:242-257.
25. Bidarra SJ, Barrias CC, Barbosa MA, Soares R, Amedee J, Granja PL. Phenotypic and pro-liferative modulation of human mesenchy-mal stem cells via crosstalk with endothelial cells. Stem Cell Res. 2011; 7(3):186-197.
26. Kolbe M, Xiang Z, Dohle E, Tonak M, Kirkpatrick CJ, Fuchs S. Paracrine effects influenced by cell culture medium and con-sequences on microvessel-like structures in cocultures of mesenchymal stem cells and outgrowth endothelial cells. Tissue Eng Part A. 2011; 17(17-18):2199-2212.
27. D’Alimonte I, Nargi E, Mastrangelo F, et al. Vascular endothelial growth factor enhances in vitro proliferation and osteogenic differ-entiation of human dental pulp stem cells. J Biol Regul Homeost Agents. 2011; 25(1):57-69.
28. Saleh FA, Whyte M, Ashton P, Genever PG. Regulation of mesenchymal stem cell activi-ty by endothelial cells. Stem Cells Dev. 2011; 20(3):391-403.
29. Ern C, Krump-Konvalinkova V, Docheva D, et al. Interactions of human endothelial and multipotent mesenchymal stem cells in co-cultures. Open Biomed Eng J. 2010; 4:190-198.
30. Trkov S, Eng G, Di Liddo R, Parnigotto PP, Vunjak-Novakovic G. Micropatterned three-dimensional hydrogel system to study human endothelial-mesenchymal stem cell interactions. J Tissue Eng Regen Med. 2010; 4(3):205-215.
31. Ma J, van den Beucken JJ, Yang F, et al. Coculture of osteoblasts and endothelial cells: optimization of culture medium and cell ratio. Tissue Eng Part C Methods. 2011; 17(3):349-357.
32. Wu Y, Cao H, Yang Y, et al. Effects of vascu-lar endothelial cells on osteogenic differen-tiation of noncontact co-cultured periodontal ligament stem cells under hypoxia. J Peri-odontal Res. 2013; 48(1):52-65.
33. Kang Y, Kim S, Fahrenholtz M, Khademhos-seini A, Yang Y. Osteogenic and angiogenic potentials of monocultured and co-cultured human-bone-marrow-derived mesenchymal stem cells and human-umbilical-vein en-dothelial cells on three-dimensional porous beta-tricalcium phosphate scaffold. Acta Bio-
mater. 2013; 9(1):4906-4915.
34. Zhao X, Liu L, Wang FK, Zhao DP, Dai XM, Han XS. Coculture of vascular endothe-lial cells and adipose-derived stem cells as a source for bone engineering. Ann Plast Surg. 2012; 69(1):91-98.
35. Wang J, Ye Y, Tian H, et al. In vitro osteogen-esis of human adipose-derived stem cells by coculture with human umbilical vein endo-thelial cells. Biochem Biophys Res Commun. 2011; 412(1):143-149.
36. Zhang Y, Andrukhov O, Berner S, et al. Os-teogenic properties of hydrophilic and hy-drophobic titanium surfaces evaluated with osteoblast-like cells (MG63) in coculture with human umbilical vein endothelial cells (HUVEC). Dent Mater. 2010; 26(11):1043-1051.
37. Neeley WW, Carnes DL, Cochran DL. Os-teogenesis in an in vitro coculture of human periodontal ligament fibroblasts and human microvascular endothelial cells. J Periodon-tol. 2010; 81(1):139-149.
38. Hager S, Lampert FM, Orimo H, Stark GB, Finkenzeller G. Up-regulation of alkaline phosphatase expression in human primary osteoblasts by cocultivation with primary endothelial cells is mediated by p38 mitogen-activated protein kinase-dependent mRNA stabilization. Tissue Eng Part A. 2009; 15(11):3437-3447.
39. Usami K, Mizuno H, Okada K, et al. Com-posite implantation of mesenchymal stem cells with endothelial progenitor cells en-hances tissue-engineered bone formation. J Biomed Mater Res A. 2009; 90(3):730-741.
40. Kaigler D, Krebsbach PH, West ER, Horg-er K, Huang YC, Mooney DJ. Endothe-lial cell modulation of bone marrow stromal cell osteogenic potential. FASEB J. 2005; 19(6):665-667.
41. Meury T, Verrier S, Alini M. Human endo-thelial cells inhibit BMSC differentiation into mature osteoblasts in vitro by interfer-ing with osterix expression. J Cell Biochem. 2006; 98(4):992-1006.
42. Bryan BA, D’Amore PA. Pericyte isolation and use in endothelial/pericyte coculture models. Methods Enzymol. 2008; 443:315-331.
43. Leszczynska J, Zyzynska-Granica B, Koziak K, Ruminski S, Lewandowska-Szumiel M. Contribution of endothelial cells to human bone-derived cells expansion in coculture. Tissue Eng Part A. 2013; 19(3-4):393-402.
44. Sahar DE, Walker JA, Wang HT, et al. Effect of endothelial differentiated adipose-derived stem cells on vascularity and osteogenesis in poly(D,L-lactide) scaffolds in vivo. J Cranio-fac Surg. 2012; 23(3):913-918.
45. Friedenstein AJ, Deriglasova UF, Kulagina NN, et al. Precursors for fibroblasts in dif-ferent populations of hematopoietic cells as detected by the in vitro colony assay method.
Exp Hematol. 1974; 2(2):83-92.
46. Gang EJ, Jeong JA, Hong SH, et al. Skeletal myogenic differentiation of mesenchymal stem cells isolated from human umbilical cord blood. Stem Cells. 2004; 22(4):617-624.
47. Bochev I, Elmadjian G, Kyurkchiev D, et al. Mesenchymal stem cells from human bone marrow or adipose tissue differently modu-late mitogen-stimulated B-cell immunoglob-ulin production in vitro. Cell Biol Int. 2008; 32(4):384-393.
48. Chang SC, Tai CL, Chung HY, Lin TM, Jeng LB. Bone marrow mesenchymal stem cells form ectopic woven bone in vivo through endochondral bone formation. Artif Organs. 2009; 33(4):301-308.
49. Rangappa S, Fen C, Lee EH, Bongso A, Sim EK. Transformation of adult mesenchymal stem cells isolated from the fatty tissue into cardiomyocytes. Ann Thorac Surg. 2003; 75(3):775-779.
50. Lei H, Yu B, Huang Z, et al. Comparative analysis of mesenchymal stem cells from adult mouse adipose, muscle, and fetal mus-cle. Mol Biol Rep. 2013; 40(2):885-892.
51. Branch MJ, Hashmani K, Dhillon P, Jones DR, Dua HS, Hopkinson A. Mesenchy-mal stem cells in the human corneal limbal stroma. Invest Ophthalmol Vis Sci. 2012; 53(9):5109-5116.
52. Bruno S, Camussi G. Isolation and character-ization of resident mesenchymal stem cells in human glomeruli. Methods Mol Biol. 2012; 879:367-380.
53. Bruno S, Bussolati B, Grange C, et al. Isola-tion and characterization of resident mesen-chymal stem cells in human glomeruli. Stem Cells Dev. 2009; 18(6):867-880.
54. Jang MJ, Kim HS, Lee HG, et al. Placenta-derived mesenchymal stem cells have an im-munomodulatory effect that can control acute graft-versus-host disease in mice. Acta Hae-matol. 2012; 129(4):197-206.
55. Chen JH, Yip CY, Sone ED, Simmons CA. Identification and characterization of aortic valve mesenchymal progenitor cells with ro-bust osteogenic calcification potential. Am J Pathol. 2009; 174(3):1109-1119.
56. Shih YR, Kuo TK, Yang AH, Lee OK, Lee CH. Isolation and characterization of stem cells from the human parathyroid gland. Cell Prolif. 2009; 42(4):461-470.
57. Spitzer TL, Rojas A, Zelenko Z, et al. Peri-vascular human endometrial mesenchymal stem cells express pathways relevant to self-renewal, lineage specification, and functional phenotype. Biol Reprod. 2012; 86(2):58.
58. Yamanishi H, Fujiwara S, Soma T. Perivascu-lar localization of dermal stem cells in human scalp. Exp Dermatol. 2012; 21(1):78-80.
59. Díaz-Prado S, Muiños-López E, Hermida-Gómez T, et al. Isolation and characteriza-tion of mesenchymal stem cells from human
338

MAY 2014 | Volume 37 • Number 5
n Review Article
cmeARTICLE
amniotic membrane [published online ahead of print August 30, 2010]. Tissue Eng Part C Methods.
60. Siepe M, Thomsen AR, Duerkopp N, et al. Human neonatal thymus-derived mesenchy-mal stromal cells: characterization, differen-tiation, and immunomodulatory properties. Tissue Eng Part A. 2009; 15(7):1787-1796.
61. Kerkis I, Caplan AI. Stem cells in dental pulp of deciduous teeth. Tissue Eng Part B Rev. 2012; 18(2):129-138.
62. Campagnoli C, Roberts IA, Kumar S, Ben-nett PR, Bellantuono I, Fisk NM. Identifica-tion of mesenchymal stem/progenitor cells in human first-trimester fetal blood, liver, and bone marrow. Blood. 2001; 98(8):2396-2402.
63. De Bari C, Dell’Accio F, Tylzanowski P, Luyten FP. Multipotent mesenchymal stem cells from adult human synovial membrane. Arthritis Rheum. 2001; 44(8):1928-1942.
64. Hu Y, Liao L, Wang Q, et al. Isolation and identification of mesenchymal stem cells from human fetal pancreas. J Lab Clin Med. 2003; 141(5):342-349.
65. In’t Anker PS, Noort WA, Kruisselbrink AB, et al. Nonexpanded primary lung and bone marrow-derived mesenchymal cells promote the engraftment of umbilical cord blood-de-rived CD34(+) cells in NOD/SCID mice. Exp Hematol. 2003; 31(10):881-889.
66. In’t Anker PS, Scherjon SA, Kleijburg-van der Keur C, et al. Amniotic fluid as a nov-el source of mesenchymal stem cells for therapeutic transplantation. Blood. 2003; 102(4):1548-1549.
67. Baksh D, Davies JE, Zandstra PW. Adult human bone marrow-derived mesenchymal progenitor cells are capable of adhesion-in-dependent survival and expansion. Exp He-matol. 2003; 31(8):723-732.
68. Baksh D, Zandstra PW, Davies JE. A non-contact suspension culture approach to the culture of osteogenic cells derived from a CD49elow subpopulation of human bone marrow-derived cells. Biotechnol Bioeng. 2007; 98(6):1195-1208.
69. Wan C, He Q, McCaigue M, Marsh D, Li G. Nonadherent cell population of human mar-row culture is a complementary source of mesenchymal stem cells (MSCs). J Orthop Res. 2006; 24(1):21-28.
70. Pufe T, Petersen W, Fandrich F, et al. Pro-grammable cells of monocytic origin (PCMO): a source of peripheral blood stem cells that generate collagen type II-pro-ducing chondrocytes. J Orthop Res. 2008; 26(3):304-313.
71. Xia Z, Locklin RM, Triffitt JT. Fates and osteogenic differentiation potential of hu-man mesenchymal stem cells in immuno-compromised mice. Eur J Cell Biol. 2008; 87(6):353-364.
72. Choi JW, Park EJ, Shin HS, Shin IS, Ra JC,
Koh KS. In vivo differentiation of undif-ferentiated human adipose tissue-derived mesenchymal stem cells in critical-sized calvarial bone defects. Ann Plast Surg. 2014; 72(2):225-233.
73. Humphreys BD, Lin SL, Kobayashi A, et al. Fate tracing reveals the pericyte and not epithelial origin of myofibroblasts in kidney fibrosis. Am J Pathol. 2010; 176(1):85-97.
74. Buring K. On the origin of cells in hetero-topic bone formation. Clin Orthop Relat Res. 1975; (110):293-301.
75. Ueno T, Kagawa T, Mizukawa N, Nakamura H, Sugahara T, Yamamoto T. Cellular origin of endochondral ossification from grafted periosteum. Anat Rec. 2001; 264(4):348-357.
76. Grcevic D, Pejda S, Matthews BG, et al. In vivo fate mapping identifies mesenchymal progenitor cells. Stem Cells. 2012; 30(2):187-196.
77. Monzack EL, Masters KS. Can valvular in-terstitial cells become true osteoblasts? A side-by-side comparison. J Heart Valve Dis. 2011; 20(4):449-463.
78. Wada MR, Inagawa-Ogashiwa M, Shimizu S, Yasumoto S, Hashimoto N. Generation of different fates from multipotent muscle stem cells. Development. 2002; 129(12):2987-2995.
79. Hashimoto N, Kiyono T, Wada MR, et al. Os-teogenic properties of human myogenic pro-genitor cells. Mech Dev. 2008; 125(3-4):257-269.
80. Yamaguchi A, Katagiri T, Ikeda T, et al. Re-combinant human bone morphogenetic pro-tein-2 stimulates osteoblastic maturation and inhibits myogenic differentiation in vitro. J Cell Biol. 1991; 113(3):681-687.
81. Katagiri T, Yamaguchi A, Komaki M, et al. Bone morphogenetic protein-2 converts the differentiation pathway of C2C12 myoblasts into the osteoblast lineage. J Cell Biol. 1994; 127(6 Pt 1):1755-1766.
82. Otsuru S, Tamai K, Yamazaki T, Yoshikawa H, Kaneda Y. Bone marrow-derived osteo-blast progenitor cells in circulating blood contribute to ectopic bone formation in mice. Biochem Biophys Res Commun. 2007; 354(2):453-458.
83. Otsuru S, Tamai K, Yamazaki T, Yoshikawa H, Kaneda Y. Circulating bone marrow-de-rived osteoblast progenitor cells are recruited to the bone-forming site by the CXCR4/stromal cell-derived factor-1 pathway. Stem Cells. 2008; 26(1):223-234.
84. Suda RK, Billings PC, Egan KP, et al. Cir-culating osteogenic precursor cells in het-erotopic bone formation. Stem Cells. 2009; 27(9):2209-2219.
85. Zvaifler NJ, Marinova-Mutafchieva L, Ad-ams G, et al. Mesenchymal precursor cells in the blood of normal individuals. Arthritis Res. 2000; 2(6):477-488.
86. Choi YH, Burdick MD, Strieter RM. Human circulating fibrocytes have the capacity to differentiate osteoblasts and chondrocytes. Int J Biochem Cell Biol. 2010; 42(5):662-671.
87. Kuznetsov SA, Mankani MH, Leet AI, Ziran N, Gronthos S, Robey PG. Circulating con-nective tissue precursors: extreme rarity in humans and chondrogenic potential in guinea pigs. Stem Cells. 2007; 25(7):1830-1839.
88. Doehring LC, Heeger C, Aherrahrou Z, et al. Myeloid CD34+CD13+ precursor cells transdifferentiate into chondrocyte-like cells in atherosclerotic intimal calcification. Am J Pathol. 2010; 177(1):473-480.
89. Shafer J, Davis AR, Gannon FH, et al. Oxy-gen tension directs chondrogenic differentia-tion of myelo-monocytic progenitors during endochondral bone formation. Tissue Eng. 2007; 13(8):2011-2019.
90. Olmsted-Davis EA, Gugala Z, Camargo F, et al. Primitive adult hematopoietic stem cells can function as osteoblast precursors. Proc Natl Acad Sci U S A. 2003; 100(26):15877-15882.
91. Rumi MN, Deol GS, Singapuri KP, Pellegrini VD Jr. The origin of osteoprogenitor cells responsible for heterotopic ossification fol-lowing hip surgery: an animal model in the rabbit. J Orthop Res. 2005; 23(1):34-40.
92. Kaplan FS, Glaser DL, Shore EM, et al. He-matopoietic stem-cell contribution to ectopic skeletogenesis. J Bone Joint Surg Am. 2007; 89(2):347-357.
93. Liu Y, Wang T, Yan J, et al. HGF/c-Met sig-nalling promotes Notch3 activation and hu-man vascular smooth muscle cell osteogenic differentiation in vitro. Atherosclerosis. 2011; 219(2):440-447.
94. Yan J, Stringer SE, Hamilton A, et al. Deco-rin GAG synthesis and TGF-beta signaling mediate Ox-LDL-induced mineralization of human vascular smooth muscle cells. Arterio-scler Thromb Vasc Biol. 2011; 31(3):608-615.
95. Shimizu T, Tanaka T, Iso T, Kawai-Kowase K, Kurabayashi M. Azelnidipine inhibits Msx2-dependent osteogenic differentiation and matrix mineralization of vascular smooth muscle cells. Int Heart J. 2012; 53(5):331-335.
96. Bobryshev YV. Transdifferentiation of smooth muscle cells into chondrocytes in atherosclerotic arteries in situ: implications for diffuse intimal calcification. J Pathol. 2005; 205(5):641-650.
97. Selman K, Kafatos FC. Transdifferentiation in the labial gland of silk moths: is DNA re-quired for cellular metamorphosis? Cell Dif-fer. 1974; 3(2):81-94.
98. Graf T, Enver T. Forcing cells to change lin-eages. Nature. 2009; 462(7273):587-594.
99. Chen FG, Zhang WJ, Bi D, et al. Clonal anal-ysis of nestin(-) vimentin(+) multipotent fi-
339

ORTHOPEDICS | Healio.com/Orthopedics
n Review Article
cmeARTICLE
broblasts isolated from human dermis. J Cell Sci. 2007; 120(Pt 16):2875-2883.
100. Hsu SH, Huang GS, Feng F. Isolation of the multipotent MSC subpopulation from human gingival fibroblasts by culturing on chitosan membranes. Biomaterials. 2012; 33(9):2642-2655.
101. Kalluri R, Zeisberg M. Fibroblasts in cancer. Nat Rev Cancer. 2006; 6(5):392-401.
102. Strieter RM, Keeley EC, Hughes MA, Burdick MD, Mehrad B. The role of cir-culating mesenchymal progenitor cells (fi-brocytes) in the pathogenesis of pulmonary fibrosis. J Leukoc Biol. 2009; 86(5):1111-1118.
103. Keeley EC, Mehrad B, Strieter RM. The role of circulating mesenchymal progeni-tor cells (fibrocytes) in the pathogenesis of fibrotic disorders. Thromb Haemost. 2009; 101(4):613-618.
104. Umehara K, Iimura T, Sakamoto K, et al. Ca-nine oral mucosal fibroblasts differentiate into osteoblastic cells in response to BMP-2. Anat Rec (Hoboken). 2012; 295(8):1327-1335.
105. Yu F, Cui Y, Zhou X, Zhang X, Han J. Os-
teogenic differentiation of human ligament fibroblasts induced by conditioned medium of osteoclast-like cells. Biosci Trends. 2011; 5(2):46-51.
106. Hinz B, Phan SH, Thannickal VJ, et al. Re-cent developments in myofibroblast biology: paradigms for connective tissue remodeling. Am J Pathol. 2012; 180(4):1340-1355.
107. Hinz B, Phan SH, Thannickal VJ, Galli A, Bochaton-Piallat ML, Gabbiani G. The myo-fibroblast: one function, multiple origins. Am J Pathol. 2007; 170(6):1807-1816.
108. Lai CF, Shao JS, Behrmann A, Krchma K, Cheng SL, Towler DA. TNFR1-activated reactive oxidative species signals up-reg-ulate osteogenic Msx2 programs in aor-tic myofibroblasts. Endocrinology. 2012; 153(8):3897-3910.
109. Simionescu A, Simionescu DT, Vyavahare NR. Osteogenic responses in fibroblasts ac-tivated by elastin degradation products and transforming growth factor-beta1: role of myofibroblasts in vascular calcification. Am J Pathol. 2007; 171(1):116-123.
110. Schor AM, Allen TD, Canfield AE, Sloan P,
Schor SL. Pericytes derived from the retinal microvasculature undergo calcification in vi-tro. J Cell Sci. 1990; 97(Pt 3):449-461.
111. Canfield AE, Sutton AB, Hoyland JA, Schor AM. Association of thrombospondin-1 with osteogenic differentiation of retinal pericytes in vitro. J Cell Sci. 1996; 109(pt 2):343-353.
112. Doherty MJ, Ashton BA, Walsh S, Beres-ford JN, Grant ME, Canfield AE. Vascular pericytes express osteogenic potential in vitro and in vivo. J Bone Miner Res. 1998; 13(5):828-838.
113. Caplan AI. All MSCs are pericytes? Cell Stem Cell. 2008; 3(3):229-230.
114. Goritz C, Dias DO, Tomilin N, Barbacid M, Shupliakov O, Frisen J. A pericyte origin of spinal cord scar tissue. Science. 2011; 333(6039):238-242.
115. Lounev VY, Kaplan FS, Shore EM. Lack of pericyte contribution to BMP4-induced heterotopic ossification. Paper presented at the American Society for Bone and Mineral Research Annual Meeting; October 15-19, 2010; Toronto, Ontario, Canada.
340













![Transcriptional Network Controlling Endochondral Ossification · branous ossification and endochondral ossification.[1] During intramembranous ossification, osteoblasts produce type](https://img.pdfslide.net/doc/110x75/5e8cf0c24763783dcf0d78ef/transcriptional-network-controlling-endochondral-ossification-branous-ossification.jpg)