Embed Size (px)
Citation preview

Journal of Substance Abuse Treatment 35 (2008) 427–433
Regular article
Assessing spirituality/religiosity in the treatment environment:The Treatment Spirituality/Religiosity Scale
Jason Lillis, (Ph.D.)⁎, Elizabeth Gifford, (Ph.D.),Keith Humphreys, (Ph.D.), Rudolf Moos, (Ph.D.)
VA Palo Alto Health Care System, Stanford University Medical School, Menlo Park, CA 94025, USA
Received 18 October 2007; received in revised form 30 January 2008; accepted 18 February 2008
Abstract
There has been much interest in measuring and evaluating the role of spirituality/religiosity (S/R) in substance use disorder (SUD)treatment. This study presents the initial evaluation of a new measure of S/R in the treatment environment: the Treatment Spirituality/Religiosity Scale (TSRS). The TSRS has 10 items and can be completed by both patient and staff to measure the emphasis on S/R in a giventreatment program, which may have important implications for patient–program fit. Data on the TSRS were gathered from 3,018 patients and329 staff members from 15 residential SUD treatment programs within the Department of Veterans Affairs Health Care System. The TSRSshowed good internal consistency (α = .77), a single-factor structure, close agreement between patients and staff members (r = .93), and gooddiscriminant validity. The TSRS appears to be a brief, easily administered, and potentially useful measure of the emphasis on S/R inresidential SUD treatment programs. Published by Elsevier Inc.
Keywords: Spirituality; Religiosity; SUD; Substance use; Scale; Treatment environment
1. Introduction
Recent reviewshave called formore research to identify theactive ingredients of effective treatments for substance abusedisorders (Finney, Wilbourne, & Moos, 2007; Moos, 2007).Spirituality/Religiosity (S/R) may be one such ingredient,particularly in Twelve-Step Facilitation (TSF) treatmentprograms, which have been shown to produce positivesubstance use and functioning outcomes (Connors, Tonigan,& Miller, 2001; Humphreys, 1993; Moos, Finney, Ouimette,& Suchinsky, 1999; Ouimette, Moos, & Finney, 1998; ProjectMATCH Research Group 1998; Tonigan, Toscova, &Miller, 1996).
Treatments other than TSF, such as cognitive–behavioraltherapy (CBT) and Eclectic treatment that offers a combina-
⁎ Corresponding author. Center for Health Care Evaluation, 795 WillowRoad (152-MPD), Menlo Park, CA 94025, USA. Tel.: +1 650 4935000x27828.
E-mail address: [email protected] (J. Lillis).
0740-5472/08/$ – see front matter. Published by Elsevier Inc.doi:10.1016/j.jsat.2008.02.002
tion of elements of TSF and CBT, may also emphasizeaspects of S/R that contribute to good treatment outcomes(Moos & Moos, 1998). Because the S/R component of TSFand other evidence-based treatments may be one of their keyactive ingredients (Humphreys & Gifford, 2006), thesefindings highlight the need to assess the emphasis on S/R inthe treatment environment.
Many patients show considerable interest in S/R in thetreatment environment. Inpatients (Dermatis, Guschwan,Galanter, & Bunt, 2004) and outpatients (Arnold, Avants,Margolin, & Marcotte, 2002) with substance use disorder(SUD), particularly inner-city and ethnic minority patients(Dermatis et al., 2004), report wanting more emphasis onspirituality in treatment programs. Moreover, religiousbeliefs and practices (Tonigan, Miller, & Connors, 2000),belief in God (Tonigan, Miller, & Schermer, 2002), self-reported spirituality (Jarusiewicz, 2000), and experiencing aspiritual awakening (Kaskutas, Turk, Bond, & Weisner,2003) have all been associated with positive substance useand mental health outcomes among individuals with alcohol

428 J. Lillis et al. / Journal of Substance Abuse Treatment 35 (2008) 427–433
use disorders (Pardini, Plante, Sherman, & Stump, 2000).Recent evidence also suggests that increases in S/R arerelated to decreased heavy drinking (Robinson, Cranford,Webb, & Brower, 2007). Conversely, some patients report anegative reaction to S/R content (Klaw & Humphreys,2000). A measure designed to assess S/R could improvepatient–program fit for these patients as well.
Despite this growing literature, reviews of spirituality inaddictions research concluded that the construct was oftenpoorly defined and measured (Cook, 2004; Gorsuch, 1993;Hill et al., 2000) or difficult to examine (Miller, 1998). Veryfew studies assess aspects of patients' spirituality orreligiosity (Dominguez et al., 2005), and, to our knowledge,there have been few attempts to measure these constructswithin SUD treatment programs. One study (Montgomery,Miller, & Tonigan, 1993) developed three items to assessmembers' perceptions of S/R in Alcoholics Anonymous(AA) and found variability in this construct among threeAA groups.
A variety of self-report measures have been designed toassess different aspects of patients' S/R, including transcen-dence (Piedmont, 2004), spiritual meaning (Mascaro, Rosen,&Morey, 2004), religious background (Connors, Tonigan, &Miller, 1996), daily spiritual experiences (Underwood &Teresi, 2002), purpose in life (Tonigan, Miller, & Connors,2001), and other related constructs (Robinson et al., 2007).In fact, Morgan (2002) identified a number of reliable andvalid measures designed to address aspects of patients' S/R.In contrast, our search yielded no measures of the emphasison S/R in the treatment environment.
The treatment environment is one of a variety of factorsthat influence SUD outcomes (Moos, 1997; Moos et al.,1999). Because spiritual and religious factors can beimportant aspects of the treatment milieu, it would be usefulto systematically assess the construct of S/R and clearlyidentify its role in the recovery process. SUD treatmentprograms vary with respect to their emphasis on S/R, and theubiquity of TSF activities can blur the distinction amongtypes of programs. Indeed, a recent study showed consider-able similarity among “traditional” and “faith-based” SUDtreatment programs (Neff, Shorkey, & Windsor, 2006).However, some consistency across types of programs can beassumed. For example, a TSF program should contain moreS/R content than a program that emphasizes other evidence-based psychological approaches. In addition, if the measuretruly taps an aspect of the program context, patients andtreatment providers should agree about the program'semphasis on S/R and the extent to which this emphasis isassociated with other aspects of the treatment milieu, such assupport and spontaneity.
We address these issues by presenting a new measure ofS/R in the treatment environment: the Treatment Spirituality/Religiosity Scale (TSRS). The measure is also a newsubscale of the Community-Oriented Programs EnvironmentScale (COPES; Moos, 1996). The COPES measures theactual, preferred, and expected social climate of community
treatment programs. It has 10 subscales that assess relation-ship dimensions (Involvement, Support, and Spontaneity),personal growth dimensions (Autonomy, Practical Orienta-tion, Personal Problem Orientation, and Anger and Aggres-sion), and system maintenance dimensions (Order andOrganization, Program Clarity, and Staff Control). Wedeveloped a new subscale to assess the emphasis on S/R,which reflects a personal growth dimension.
In this article, we (a) describe the development of theTSRS to measure the emphasis on spiritual and religiousaspects of the SUD treatment environment, (b) presentpreliminary psychometric and normative information onthe TSRS as perceived by patients and by staff members,(c) examine the extent to which patients' and staff members'perceptions of S/R discriminate among SUD programswith different treatment orientations, and (d) identify theassociations between spirituality and other aspects of thetreatment environment.
2. Materials and methods
2.1. Sample
Patient and staff data were obtained from a large,naturalistic, multisite study of Department of VeteransAffairs (VA) residential SUD treatment programs (Mooset al., 1999). The purposes of the main study were tocompare treatment outcomes of patients treated in TSF,CBT, and Eclectic (a combination of TSF and CBT)treatment programs; examine interactions between patientand treatment program characteristics; and identify pre-dictors of patient outcomes (Ouimette et al., 1997; Ritsher,McKellar, Finney, Otilingam, & Moos, 2002). The data setincluded 3,018 patients and 329 staff members from15 representative treatment programs drawn from anationwide sample. Programs were classified as TSF,CBT, or Eclectic on the basis of information obtainedfrom program proposals, telephone interviews, and 1- to2-day onsite visits conducted to ensure fidelity of treatmentorientation. The 15 programs were selected because of theirorientation, allowing for appropriate geographic distribu-tion (for details on program selection procedures, seeOuimette et al., 1997). Because the programs were indifferent geographical locations, participants were not ableto choose among different programs. All participantsprovided informed consent, and study procedures were inaccord with institutional review board standards.
2.2. Item development and selection
Potential items for the TSRS were created based onobservations of different treatment programs, discussionwith staff members and program coordinators, and perusal ofthe literature on S/R in treatment programs. The initial poolincluded about 20 items. As a result of eliminating redundant
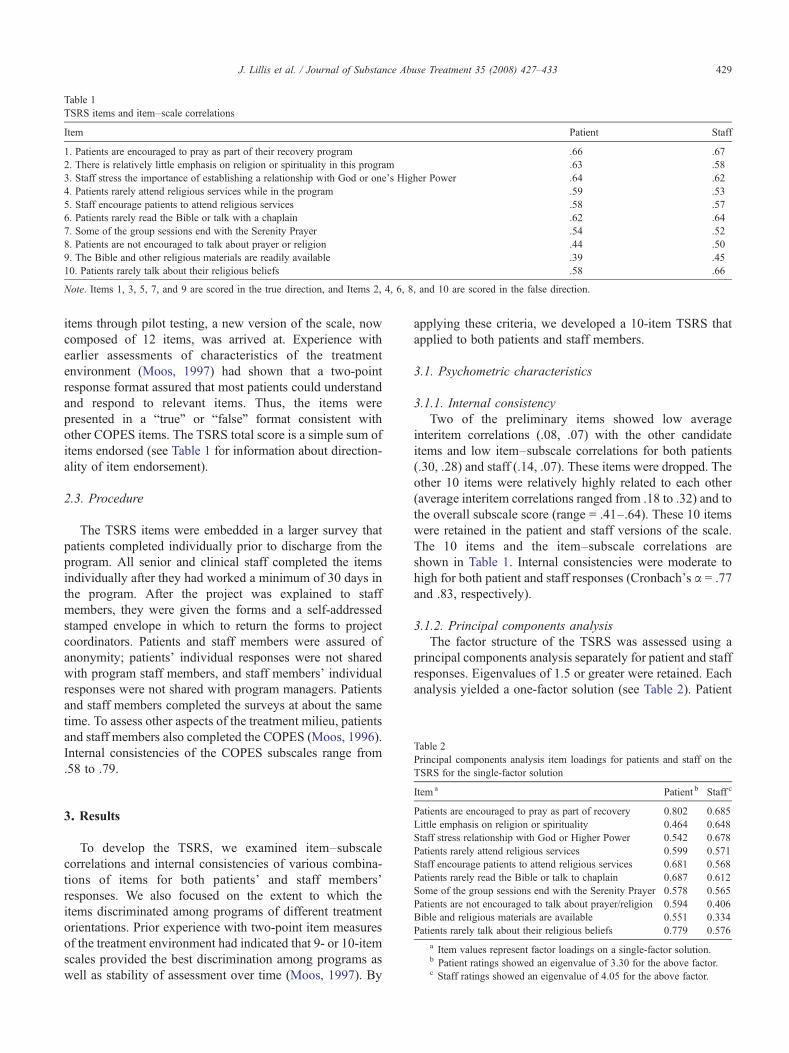
Table 1TSRS items and item–scale correlations
Item Patient Staff
1. Patients are encouraged to pray as part of their recovery program .66 .672. There is relatively little emphasis on religion or spirituality in this program .63 .583. Staff stress the importance of establishing a relationship with God or one's Higher Power .64 .624. Patients rarely attend religious services while in the program .59 .535. Staff encourage patients to attend religious services .58 .576. Patients rarely read the Bible or talk with a chaplain .62 .647. Some of the group sessions end with the Serenity Prayer .54 .528. Patients are not encouraged to talk about prayer or religion .44 .509. The Bible and other religious materials are readily available .39 .4510. Patients rarely talk about their religious beliefs .58 .66
Note. Items 1, 3, 5, 7, and 9 are scored in the true direction, and Items 2, 4, 6, 8, and 10 are scored in the false direction.
Table 2Principal components analysis item loadings for patients and staff on theTSRS for the single-factor solution
429J. Lillis et al. / Journal of Substance Abuse Treatment 35 (2008) 427–433
items through pilot testing, a new version of the scale, nowcomposed of 12 items, was arrived at. Experience withearlier assessments of characteristics of the treatmentenvironment (Moos, 1997) had shown that a two-pointresponse format assured that most patients could understandand respond to relevant items. Thus, the items werepresented in a “true” or “false” format consistent withother COPES items. The TSRS total score is a simple sum ofitems endorsed (see Table 1 for information about direction-ality of item endorsement).
2.3. Procedure
The TSRS items were embedded in a larger survey thatpatients completed individually prior to discharge from theprogram. All senior and clinical staff completed the itemsindividually after they had worked a minimum of 30 days inthe program. After the project was explained to staffmembers, they were given the forms and a self-addressedstamped envelope in which to return the forms to projectcoordinators. Patients and staff members were assured ofanonymity; patients' individual responses were not sharedwith program staff members, and staff members' individualresponses were not shared with program managers. Patientsand staff members completed the surveys at about the sametime. To assess other aspects of the treatment milieu, patientsand staff members also completed the COPES (Moos, 1996).Internal consistencies of the COPES subscales range from.58 to .79.
Item a Patient b Staff c
Patients are encouraged to pray as part of recovery 0.802 0.685Little emphasis on religion or spirituality 0.464 0.648Staff stress relationship with God or Higher Power 0.542 0.678Patients rarely attend religious services 0.599 0.571Staff encourage patients to attend religious services 0.681 0.568Patients rarely read the Bible or talk to chaplain 0.687 0.612Some of the group sessions end with the Serenity Prayer 0.578 0.565Patients are not encouraged to talk about prayer/religion 0.594 0.406Bible and religious materials are available 0.551 0.334Patients rarely talk about their religious beliefs 0.779 0.576
a Item values represent factor loadings on a single-factor solution.b Patient ratings showed an eigenvalue of 3.30 for the above factor.c Staff ratings showed an eigenvalue of 4.05 for the above factor.
3. Results
To develop the TSRS, we examined item–subscalecorrelations and internal consistencies of various combina-tions of items for both patients' and staff members'responses. We also focused on the extent to which theitems discriminated among programs of different treatmentorientations. Prior experience with two-point item measuresof the treatment environment had indicated that 9- or 10-itemscales provided the best discrimination among programs aswell as stability of assessment over time (Moos, 1997). By
applying these criteria, we developed a 10-item TSRS thatapplied to both patients and staff members.
3.1. Psychometric characteristics
3.1.1. Internal consistencyTwo of the preliminary items showed low average
interitem correlations (.08, .07) with the other candidateitems and low item–subscale correlations for both patients(.30, .28) and staff (.14, .07). These items were dropped. Theother 10 items were relatively highly related to each other(average interitem correlations ranged from .18 to .32) and tothe overall subscale score (range = .41–.64). These 10 itemswere retained in the patient and staff versions of the scale.The 10 items and the item–subscale correlations areshown in Table 1. Internal consistencies were moderate tohigh for both patient and staff responses (Cronbach's α = .77and .83, respectively).
3.1.2. Principal components analysisThe factor structure of the TSRS was assessed using a
principal components analysis separately for patient and staffresponses. Eigenvalues of 1.5 or greater were retained. Eachanalysis yielded a one-factor solution (see Table 2). Patient
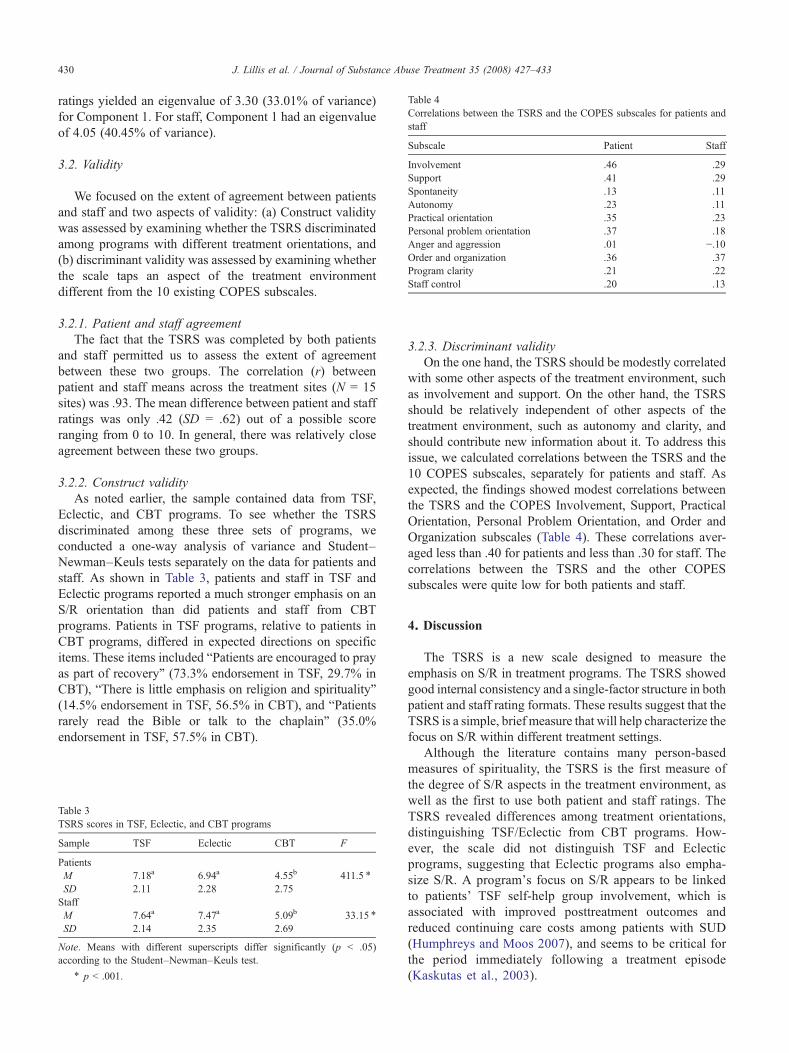
Table 4Correlations between the TSRS and the COPES subscales for patients andstaff
Subscale Patient Staff
Involvement .46 .29Support .41 .29Spontaneity .13 .11Autonomy .23 .11Practical orientation .35 .23Personal problem orientation .37 .18Anger and aggression .01 −.10Order and organization .36 .37Program clarity .21 .22Staff control .20 .13
430 J. Lillis et al. / Journal of Substance Abuse Treatment 35 (2008) 427–433
ratings yielded an eigenvalue of 3.30 (33.01% of variance)for Component 1. For staff, Component 1 had an eigenvalueof 4.05 (40.45% of variance).
3.2. Validity
We focused on the extent of agreement between patientsand staff and two aspects of validity: (a) Construct validitywas assessed by examining whether the TSRS discriminatedamong programs with different treatment orientations, and(b) discriminant validity was assessed by examining whetherthe scale taps an aspect of the treatment environmentdifferent from the 10 existing COPES subscales.
3.2.1. Patient and staff agreementThe fact that the TSRS was completed by both patients
and staff permitted us to assess the extent of agreementbetween these two groups. The correlation (r) betweenpatient and staff means across the treatment sites (N = 15sites) was .93. The mean difference between patient and staffratings was only .42 (SD = .62) out of a possible scoreranging from 0 to 10. In general, there was relatively closeagreement between these two groups.
3.2.2. Construct validityAs noted earlier, the sample contained data from TSF,
Eclectic, and CBT programs. To see whether the TSRSdiscriminated among these three sets of programs, weconducted a one-way analysis of variance and Student–Newman–Keuls tests separately on the data for patients andstaff. As shown in Table 3, patients and staff in TSF andEclectic programs reported a much stronger emphasis on anS/R orientation than did patients and staff from CBTprograms. Patients in TSF programs, relative to patients inCBT programs, differed in expected directions on specificitems. These items included “Patients are encouraged to prayas part of recovery” (73.3% endorsement in TSF, 29.7% inCBT), “There is little emphasis on religion and spirituality”(14.5% endorsement in TSF, 56.5% in CBT), and “Patientsrarely read the Bible or talk to the chaplain” (35.0%endorsement in TSF, 57.5% in CBT).
Table 3TSRS scores in TSF, Eclectic, and CBT programs
Sample TSF Eclectic CBT F
PatientsM 7.18a 6.94a 4.55b 411.5 ⁎
SD 2.11 2.28 2.75StaffM 7.64a 7.47a 5.09b 33.15 ⁎
SD 2.14 2.35 2.69
Note. Means with different superscripts differ significantly (p b .05)according to the Student–Newman–Keuls test.
⁎ p b .001.
3.2.3. Discriminant validityOn the one hand, the TSRS should be modestly correlated
with some other aspects of the treatment environment, suchas involvement and support. On the other hand, the TSRSshould be relatively independent of other aspects of thetreatment environment, such as autonomy and clarity, andshould contribute new information about it. To address thisissue, we calculated correlations between the TSRS and the10 COPES subscales, separately for patients and staff. Asexpected, the findings showed modest correlations betweenthe TSRS and the COPES Involvement, Support, PracticalOrientation, Personal Problem Orientation, and Order andOrganization subscales (Table 4). These correlations aver-aged less than .40 for patients and less than .30 for staff. Thecorrelations between the TSRS and the other COPESsubscales were quite low for both patients and staff.
4. Discussion
The TSRS is a new scale designed to measure theemphasis on S/R in treatment programs. The TSRS showedgood internal consistency and a single-factor structure in bothpatient and staff rating formats. These results suggest that theTSRS is a simple, brief measure that will help characterize thefocus on S/R within different treatment settings.
Although the literature contains many person-basedmeasures of spirituality, the TSRS is the first measure ofthe degree of S/R aspects in the treatment environment, aswell as the first to use both patient and staff ratings. TheTSRS revealed differences among treatment orientations,distinguishing TSF/Eclectic from CBT programs. How-ever, the scale did not distinguish TSF and Eclecticprograms, suggesting that Eclectic programs also empha-size S/R. A program's focus on S/R appears to be linkedto patients' TSF self-help group involvement, which isassociated with improved posttreatment outcomes andreduced continuing care costs among patients with SUD(Humphreys and Moos 2007), and seems to be critical forthe period immediately following a treatment episode(Kaskutas et al., 2003).

431J. Lillis et al. / Journal of Substance Abuse Treatment 35 (2008) 427–433
The TSRS can be used clinically to examine patient andstaff agreement within programs to clarify treatmentenvironment goals. Our findings suggest that patients andstaff often agree on the degree to which S/R is emphasized inthe treatment environment. However, in some cases, there isrelative disagreement. One outlier treatment site showed amean difference of 1.89 between patient and staff full scalescores on the TSRS, with patients reporting consistentlyhigher scores than staff members. Not surprisingly, thisprogram was characterized as Eclectic.
It would be useful for staff to know the degree to whichpatients believe S/R is addressed or supported by staff, andthe scale could provide an opportunity to open dialogue onthis issue among staff or between patients and staff. Thisdialogue could be particularly important for inner-city andethnic minority patients (Dermatis et al., 2004), who reportwanting more emphasis on spirituality in treatment pro-grams. Furthermore, research indicates that increasing S/Rwithin treatment may increase involvement in self-helpgroups after a treatment episode (Carrico, Gifford, & Moos,2007). Conversely, dialogue may also be useful for patientswho desire less S/R relative to what is currently being offeredin a given program. Length of stay is an important indicatorof posttreatment SUD outcomes. Thus, it would be useful toidentify a mismatch of patient to program in either direction.
Given the growing interest in S/R and in identifyingactive ingredients in treatment programs, the TSRS couldhelp researchers compare the degree of S/R in differenttreatment programs and examine whether it mediates ormoderates treatment outcomes. This could help addressseveral relevant issues about S/R in SUD treatmentprograms. For example, how strongly is S/R emphasized inprograms other than TSF, such as CBT and relapseprevention programs? Our study suggests that S/R may bepresent in a variety of programs within the VA system.Also, does patient and staff agreement about the level ofS/R predict more positive outcomes? Or does an emphasison S/R benefit some patients more than others, and, can itbe harmful? In relation to this, the TSRS could be usedprospectively to address relevant questions of program–patient match. For example, what preferences about theemphasis on S/R do patients desire in a program? Forthis purpose, TSRS items could be reworded to assesspreferences, consistent with other COPES subscales (Moos,1996). This would make it possible to examine whetherthe match between the program emphasis on S/R andpatients' preferences relates to patient retention, dropout,AA/Narcotics Anonymous involvement, or participationin aftercare.
Several limitations of this work should be noted. Thegeneralizability of VA patients and treatment sites isunknown. However, the large sample includes a variety oftreatment programs and activities, in addition to a full rangeof SUD problems, which strengthen the likely generality ofthe measure. Additionally, although the measure success-fully discriminated between TSF- and CBT-oriented pro-
grams, it did not discriminate between TSF and Eclecticprograms. This may be an accurate finding, but it may alsoreflect a lack of specificity of the measure. Unfortunately, wedo not have data to conduct an in-depth analysis of thespecific activities in each program that might haveinfluenced patient and staff responses to the TSRS. Also,while CBT programs scored lower on each item on averagewhen compared to TSF programs, patients and staff in CBTprograms responded “false” to the item “patients rarelyattend religious services while in the program” almost asfrequently as patients and staff in TSF programs did,indicating that further examination of construct validityissues may prove useful.
Finally, the measure is brief and meant to be practicallyuseful. As such, it does not distinguish between spiritualityand religiosity and does not capture some of the aspects ofS/R that may be important in SUD treatment. For example,program characteristics that may promote transformativespiritual experiences are not assessed. Moreover, some itemscontain references to Judeo–Christian traditions (e.g., theBible) and do not cover aspects of different spiritualapproaches, such as Native American, Hindu, or Buddhist.However, the TSRS assesses the general emphasis on S/R inthe treatment environment in a brief, effective manner.
Future studies can examine the use of broader, moreinclusive language (e.g., referring to “religious texts” asopposed to “the Bible”) or the addition of other religiousterminology (e.g., using the term “the Koran” in addition to“the Bible”) in the current items. Studies can also focus onthe relation of the TSRS to SUD outcomes. The TSRS wasused in one previous study, which found that patients in moresupportive and goal-directed treatment environments, whichhad a moderate to high emphasis on spirituality as measuredby the TSRS, participated in more treatment services, weremore involved in self-help groups and more satisfied with theprogram, improved more during treatment, and were morelikely to participate in outpatient mental health care afterdischarge (Moos & Moos, 1998).
Spiritual and religious values may help some patients intreatment develop skills that contribute to long-termrecovery. These values support the emphasis on helpingothers, which tends to increase the helper's sense of purposeand personal responsibility, rewards for remaining sober, andcommitment to recovery (Pagano, Friend, Tonigan, & Stout,2004; Zemore, Kaskutas, & Ammon, 2004). They also canenhance acceptance-based skills, which support sustainedinvolvement in self-help programs (Carrico et al., 2007).Acceptance-based skills include the awareness/acceptance ofinternal states such as temptation and the ability to makeconstructive choices during these experiences. This kind ofacceptance-based responding has also been linked to long-term reductions in SUD impairment after treatment (Gifford,Ritsher, McKellar, & Moos, 2006). In addition, treatmentssuch as motivational interviewing support patient values,which often include S/R, as a means of improvingengagement in treatment (Miller & Rollnick, 1991). Future

432 J. Lillis et al. / Journal of Substance Abuse Treatment 35 (2008) 427–433
studies could help clarify the relationships between S/R intreatment and proximal and distal outcomes and the extent towhich any such relationships are mediated by patient–program alliance, acceptance-based responding, and post-treatment TSF group involvement.
Acknowledgments
Preparation of this article was supported in part by the VAHealth Services Research and Development Service. Wethank Peg Maude Griffin for her help in the initialformulation of the TSRS items. The views expressed hereare the authors' and do not necessarily represent the viewsof the VA.
References
Arnold, R. M., Avants, S. K., Margolin, A., & Marcotte, D. (2002). Patientattitudes concerning the inclusion of spirituality into addiction treatment.Journal of Substance Abuse Treatment, 23, 319−326.
Carrico, A. W., Gifford, E. V., & Moos, E. V. (2007). Spirituality/religiositypromotes acceptance-based responding and 12-step involvement. Drugand Alcohol Dependence, 89, 66−73.
Connors, G. J., Tonigan, J. S., & Miller, W. R. (1996). Measure ofreligious background and behavior for use in behavior change research.Psychology of Addictive Behaviors, 10, 90−96.
Connors, G. J., Tonigan, J. S., & Miller, W. R. (2001). A longitudinal modelof intake symptomatology, AA participation and outcome: Retrospectivestudy of the Project MATCH outpatient and aftercare samples. Journalof Studies on Alcohol, 62, 817−825.
Cook, C. C. H. (2004). Addiction and spirituality. Addiction, 99, 539−551.Dermatis, H., Guschwan, M. T., Galanter, M., & Bunt, G. (2004).
Orientation toward spirituality and self-help approaches in thetherapeutic community. Journal of Addictive Diseases, 23, 39−54.
Dominguez, A. W., Ip, C. C., Hoover, D., Oleari, A., McMinn, M. R., Lee,T. W., et al. (2005). Faith-based substance abuse treatment programs.In M. R. McMinn, & A. W. Dominguez (Eds.), Psychology and thechurch (pp. 19−30). Nova Science Publishers.
Finney, J., Wilbourne, P., & Moos, R. (2007). Psychosocial treatments forsubstance use disorders. In P. E. Nathan, & J. M. Gorman (Eds.), Aguide to treatments that work (3rd. ed., pp.179–202). New York:Oxford.
Gifford, E. V., Ritsher, J. B., McKellar, J. D., & Moos, R. H. (2006).Acceptance and relationship context: A model of substance use disordertreatment outcome. Addiction, 101, 1167−1177.
Gorsuch. (1993). Assessing spiritual values in Alcoholics Anonymousresearch. In B. S. McCrady, & W. R. Miller (Eds.), Research onAlcoholics Anonymous: Opportunities and alternatives (pp. 301−318).New Brunswick, NJ: Rutgers University Press.
Hill, P., Pargament, K., Hood, R., McCullough, M., Swyers, J., Larson, D.,& Zimbauer, B. (2000). Conceptualizing religion and spirituality: Pointsof commonality, points of departure. Journal for the Theory of SocialBehaviour, 30, 51−77.
Humphreys, K. (1993). Psychotherapy and the twelve step approach forsubstance abusers: The limits of integration. Psychotherapy, 30,207−213.
Humphreys, K., & Gifford, E. V. (2006). Religion, spirituality, and thetroublesome use of substances. In W. R. Miller, & K. M. Carroll (Eds.),Rethinking substance abuse: What the science shows, and what weshould do about it (pp. 257−274). New York: Guilford Press.
Humphreys, K., & Moos, R. H. (2007). Encouraging posttreatment self-helpgroup involvement to reduce demand for continuing care services: Two-year clinical and utilization outcomes. Alcoholism: Clinical andExperimental Research, 31, 64−68.
Jarusiewicz, B. (2000). Spirituality and addiction: Relationship to recoveryand relapse. Alcoholism Treatment Quarterly, 18, 99−109.
Kaskutas, L. A., Turk, N., Bond, J., & Weisner, C. (2003). The role ofreligion, spirituality and Alcoholics Anonymous in sustained sobriety.Alcoholism Treatment Quarterly, 21, 1−15.
Klaw, E., & Humphreys, K. (2000). Life stories of moderation managementmutual help group members. Contemporary Drug Problems, 27,779−803.
Mascaro, N., Rosen, D. H., & Morey, L. C. (2004). The development,construct validity, and clinical utility of the Spiritual Meaning Scale.Personality and Individual Differences, 37, 845−860.
Miller, W. R. (1998). Researching the spiritual dimensions of alcohol andother drug problems. Addiction, 93, 979−990.
Miller, W. R., & Rollnick, S. (1991). Motivational interviewing: Preparingpeople to change addictive behaviors. New York: Guilford Press.
Montgomery, H., Miller, W. R., & Tonigan, J. S. (1993). Differences amongAA groups: Implications for research. Journal of Studies on Alcohol, 54,502−504.
Moos, R. H. (1996). Community oriented programs environment scalemanual: Development, applications, research (3rd ed). Palo Alto, CA:Mind Garden.
Moos, R. (1997). Evaluating treatment environments: The quality ofpsychiatric and substance abuse programs. New Brunswick, NJ:Transaction.
Moos, R. (2007). Theory-based active ingredients of effective treatmentsfor substance use disorders. Drug and Alcohol Dependence, 88,109−121.
Moos, R. H., Finney, J. F., Ouimette, P. C., & Suchinsky, R. T. (1999). Acomparative evaluation of substance abuse treatment: I. Treatmentorientation, amount of care, and 1-year outcomes. Alcoholism: Clinicaland Experimental Research, 23, 529−536.
Moos, R., & Moos, B. (1998). The staff workplace and the quality andoutcome of substance abuse treatment. Journal of Studies on Alcohol,59, 43−51.
Morgan, J. M. (2002). Alcohol problems, alcoholism and spirituality: Anoverview of measurement and scales. Alcholism Treatment Quarterly,20, 1−18.
Neff, J., Shorkey, C., & Windsor, L. (2006). Contrasting faith-based andtraditional substance abuse treatment programs. Journal of SubstanceAbuse Treatment, 30, 49−61.
Ouimette, P. C., Finney, J. W., & Moos, R. (1997). Twelve step andcognitive behavioral treatment for substance abuse: A comparison oftreatment effectiveness. Journal of Consulting and Clinical Psychology,65, 220−234.
Ouimette, P. C., Moos, R. H., & Finney, J. F. (1998). Influence ofoutpatient treatment and 12-step group involvement on one-yearsubstance abuse treatment outcomes. Journal of Studies on Alcohol,59, 513−522.
Pagano, M. E., Friend, K. B., Tonigan, J. S., & Stout, R. L. (2004). Helpingother alcoholics in Alcoholics Anonymous and drinking outcomes:Findings from Project MATCH. Journal of Studies on Alcohol, 65,766−773.
Pardini, D. A., Plante, T. G., Sherman, A., & Stump, J. E. (2000). Religiousfaith and spirituality in substance abuse recovery: Determining themental health benefits. Journal of Substance Abuse Treatment, 19,347−354.
Piedmont, R. L. (2004). Spiritual transcendence as a predictor ofpsychosocial outcome from an outpatient substance abuse program.Psychology of Addictive Behaviors, 18, 213−222.
Project MATCH Research Group. (1998). Matching alcoholismtreatments to client heterogeneity: Project MATCH three-year drinkingoutcomes. Alcoholism: Clinical and Experimental Research, 22,1300−1311.
Ritsher, J. B., McKellar, J. D., Finney, J. W., Otilingam, P. G., & Moos, R.H. (2002). Psychiatric comorbidity, continuing care, and mutual help aspredictors of five-year remission from substance use disorders. Journalof Studies on Alcohol, 63, 709−715.

433J. Lillis et al. / Journal of Substance Abuse Treatment 35 (2008) 427–433
Robinson, E. A., Cranford, J. A., Webb, J. R., & Brower, K. J. (2007). Six-month changes in spirituality, religiousness, and heavy drinking in atreatment-seeking sample. Journal of Studies on Alcohol, 68, 282−290.
Tonigan, J. S., Miller, W. R., & Connors, G. J. (2000). Project MATCH clientimpressions about Alcoholics Anonymous: Measurement issues andrelationship to treatment outcome. Alcoholism Treatment Quarterly, 18,25−41.
Tonigan, J. S., Miller, W. R., & Connors, G. J. (2001). The search formeaning in life as a predictor of alcoholism treatment outcome. ProjectMATCH: Hypotheses, results and causal chain analyses (pp. 154−165).NIH Publication 01-4238.
Tonigan, J. S., Miller, W. R., & Schermer, C. (2002). Atheists, agonists, andAlcoholics Anonymous. Journal of Studies on Alcohol, 63, 534−541.
Tonigan, J. S., Toscova, R., & Miller, W. R. (1996). Meta-analysis of theliterature on Alcoholics Anonymous: Sample and study characteristicsmoderate findings. Journal of Studies on Alcohol, 57, 65−72.
Underwood, L. G., & Teresi, J. A. (2002). The Daily Spiritual ExperiencesScale: Development, theoretical description, reliability, exploratoryfactor analysis, and preliminary construct validity using health-relateddata. Annals of Behavior Medicine, 24, 22−33.
Zemore, S. E., Kaskutas, L. A., & Ammon, L. N. (2004). In 12-step groups,helping helps the helper. Addiction, 99, 1015−1023.





























