Embed Size (px)
Citation preview
Assessing students’ ability to detect melanomas usingstandardized patients and moulage
Claudia Hernandez, MD,a Robin Mermelstein, PhD,b June K. Robinson, MD,c andRachel Yudkowsky, MD, MHPEd
Chicago, Illinois
From
Re
D
C
ve
Dr H
W
su
Conf
This
D
4-
Background: Detection of melanoma by physicians via opportunistic surveillance during focused physicalexaminations may reduce mortality. Medical students may not encounter a clinical case of melanomaduring a dermatology clerkship.
Objective: This study examined the proficiency of fourth-year University of Illinois at Chicago medicalstudents at detecting melanomas.
Methods: Melanoma moulages were applied to the second digit of the left hand of standardized patients(SPs) participating in a wrist pain scenario during a required clinical skills examination. An observerreviewed videotapes of the examination, written SP checklists, and student notes for evidence that thestudent noticed the moulage, obtained a history, or provided counseling.
Results: Among the 190 fourth-year medical students, 56 students were observed noticing the lesion;however, 13 failed to write it in their notes or advise the patient. The detection rate was 22.6% (43 of 190students). Students who detected the probable melanoma consistently inquired about changes in the lesionand symptoms, but did not examine the rest of the skin or regularly palpate for adenopathy.
Limitations: Testing one class of students from a single medical school with a time-restricted SP encounterwhile focusing the students’ attention toward a different presenting symptom may hinder exploration ofmedical issues.
Conclusion: The low detection rate and failure of students who noticed the moulage to identify the lesionas atypical represents a lost opportunity to provide a patient intervention. Use of SP examinations may helpphysicians in training build confidence and competence in cutaneous malignancy screening. ( J Am AcadDermatol 2013;68:e83-8.)
Key words: assessment; detection rate; medical students; melanoma; skin surveillance; standardizedpatients.
ecause melanoma is detected by visual identifying its classic findings.1,2 However, access
B inspection of the skin, opportunistic screen-ing can be provided by physicians during
usual care and all physicians should have sufficientexperience during their training to be comfortable
the Department of Dermatology,a Institute for Health
search and Policy and Department of Psychology,b and
epartment of Medical Education,d University of Illinois at
hicago; and Department of Dermatology, Northwestern Uni-
rsity Feinberg School of Medicine.c
ernandez is the recipient of the Dermatology Foundation
omen’s Health Career Development Award, which partially
pported this research.
licts of interest: None declared.
article was a poster presented at the American Academy of
ermatology 2011 Annual Meeting, New Orleans, LA, February
8, 2011.
to patients willing and able to model skin diseaseduring teaching experiences is a challenge indermatology medical education. Physicians intraining may not encounter a melanoma during
Accepted for publication October 22, 2011.
Reprints not available from the authors.
Correspondence to: Claudia Hernandez, MD, Department of
Dermatology (MC 624), University of Illinois at Chicago, 808 S
Wood St, Room 376 CME, Chicago, IL 60612. E-mail: claudiah@
uic.edu.
Published online December 26, 2011.
0190-9622/$36.00
� 2011 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2011.10.032
e83

J AM ACAD DERMATOL
MARCH 2013e84 Hernandez et al
the clinical experience of a brief dermatologyclerkship. Perhaps for this reason, Moore et al3
found that only 28.2% of medical students ratedthemselves as somewhat or very skilled in theperformance of skin examinations. Others havealso found low rates of physician training, physi-cian confidence, and performance of skin cancer
CAPSULE SUMMARY
d Nondermatologists have been previouslyreported to have low confidenceregarding their skin examination skills.
d Despite performing well on a multiplechoice examination, fourth-year medicalstudents at one US medical college had alow melanoma detection rate (22.6%)during a standardized patient clinicalexamination.
d Standardized patient assessments mayassist in identifying physicians both intraining and in practice who requirefurther training in melanoma detection.
screening examinations bynondermatologists.4-6
The medical students’second-year curriculum inclinical pathophysiology atthe University of Illinois atChicago (UIC) includes arequired 1-hour dermatologylecture reviewing the presen-tation of cutaneous malig-nancies including melanomaand performance of skin ex-aminations. Students may at-tend lectures and listen to arecording, and presentationslides are uploaded to themedical student World WideWeb site allowing them toreview the materials at their
convenience. To explore gaps in the melanomascreening skills of medical students, a study atUIC examined the proficiency of medical studentsearly in their fourth year at (1) detecting, (2)inquiring about, (3) conducting a screening phys-ical examination for, and (4) advising patientsabout melanomas during a nondermatologic simu-lated encounter with an incidental finding of asuspicious lesion.METHODSThis study was approved by the UIC Institutional
Review Board. All fourth-year UIC medical studentsundergo a comprehensive assessment of their clin-ical skills through a series of simulated clinicalencounters using standardized patients (SPs), pro-fessional actors trained to accurately portray ascripted clinical patient presentation consistentlyand accurately during multiple encounters.7 Achecklist of items that students must perform cor-rectly to successfully complete the examination isprepared for each case by medical center facultywho have expertise in the particular disease beingsimulated and is reviewed with the actors. Thescenarios are practiced until they are reliably repro-duced. Four female actors were trained to portraythis simulated case and each underwent approxi-mately 6 hours of training according to standardclinical performance center protocols. Students have
12 Objective Structured Clinical Examination stationsto complete as part of their examinations.
The SP case involved a 40- to 45-year-old womanpresenting with occasional numbness, weakness,and tingling of the first, second, third, and fourthdigits. A melanoma moulage (Medart-FX, New York,NY) was applied to the SP’s second digit of the left
hand in an area where itwould be easily visible dur-ing the physical examinationof the hands (Fig 1). Themoulage measured approxi-mately 3 to 4 mm in diameterand was applied using amedical-grade adhesiveblending into the skin sothat it appeared quite natural.A board-certified dermatolo-gist approved the realistic ap-pearance of the moulageprosthetic for each SP.
A dermatologist (C. H.)coached the SPs how to an-swer questions about the his-tory and symptoms of thesimulated melanoma. The
SP was instructed not to mention the nevus in herhistory or review of systems unless the moulage wasnoticed by the student. Only then would the SPanswer specific questions by the student. The historyprepared for this case included reporting heavy sunexposure while growing up in Florida and multiple(4-5) blistering sunburns. She had no skin cancerhistory, did not perform regular skin self-examinations, and had noted no other changes inany other moles. The lesion was to be reported asnewwith no pre-existing nevus at the site. Symptomssuch as rapid growth of the lesion over a period ofless than 6 months, color change, occasional sun-screen use, and no family history of skin cancer wereto be reported if asked.
During the standard orientation, students are toldto obtain an appropriate history and perform apertinent physical examination. Everything they ob-served should be considered part of the patient’spresenting findings. Scenarios with multiple medicalproblems beyond the stated chief symptom are notrare in simulated encounters. Each student had 15minutes to conduct their history and physical exam-ination with the SP. Their documentation shouldinclude pertinent history, physical examination find-ings, differential diagnosis (up to 5 items ranked),and plans for further workup (up to 5 items).Students were given 10 minutes to enter a chartnote into an electronic medical record system made

Fig 1. Melanoma moulage applied to second digit ofstandardized patient.
J AM ACAD DERMATOL
VOLUME 68, NUMBER 3Hernandez et al e85
specifically for simulation centerebased assessmentsand the encounters were also video recorded.
Immediately after the encounter, the SPs com-pleted a checklist regarding the history, physicalexamination, and follow-up recommendations, anda patient satisfaction survey. Student notes, SPchecklists, and video recordings were all reviewedby one of the authors (C. H.) to determine whetherthe student noticed the melanoma prosthetic, ob-tained a history relevant to the melanoma, per-formed the indicated screening physicalexamination, and counseled the patient regardingcare of the pigmented lesion (Table I).
RESULTSA total of 190 students were tested during July
through December 2009. Of the 190 SP examinationscompleted, 189 students (99.5%) correctly docu-mented carpal tunnel syndrome in their differentialdiagnosis for the patient’s wrist pain. In contrast, only56 students (29%) noticed the melanoma moulageaccording to the SP, who recorded students whoverbally mentioned the nevus and/or asked ques-tions regarding it. A review of the medical notes, SPchecklist, and video recordings revealed that somestudents incorrectly concluded the melanoma pros-thesis was benign. Of the 56 students who noticedthe lesion, 13 students told the SP ‘‘not to worryabout it’’ or failed to comment on it any further, eitherverbally to the patient or in their written notes. Thenumber of students who recommended follow-up/biopsy was used to determine the detection rate. Theoverall detection rate for the entire class was 43 of190 students (22.6%).
Students who detected the probable melanomaconsistently asked the two most important questionsto predict the risk of malignancy: a history of changein the lesion (size, color) or symptoms from thelesion (itching, tingling, bleeding) (Table II). Only 5students obtained a family history of skin cancer, and
two asked about a prior diagnosis of skin cancer.One student palpated for lymphadenopathy afterdetection of the lesion and another examined othercutaneous sites for atypical pigmented lesions. Nopatient was offered a full-body skin examination.
DISCUSSIONThis study found that 56 students (29%) noticed
the moulage; however, only 43 of 190 students(22.6%) correctly concluded the lesion was atypicaland warranted further investigation. The failure ofstudents who noticed the moulage but concluded itwas benign is disappointing as it represented a lostopportunity to intervene. In addition to document-ing a low detection rate, our study adds to thesimulation literature that those who detected thelesion obtained the two salient aspects of the historyto assist with diagnosis: symptoms and change in thelesion. We also determined that even if a studentdetected the atypical lesion, examining other cuta-neous sites was not performed. We acknowledgethat time limitations during the clinical testing sce-narios may reduce the number of students perform-ing a skin examinations (please see study limitationdiscussion below).
UIC medical students learn about melanoma indidactic sessions during their second year in theclinical pathophysiology course. Multiple-choiceformats are widely used to assess dermatologicknowledge at the end of a rotation focusing onlyon the base of the Miller pyramid of clinical com-petence, ‘‘knows’’ or factual recall.8 However, theability to recall information does not translate intothe ability to use the information, physician’s actualperformance in real life, the tip of the Miller pyra-mid ‘‘does’’ (Fig 2). The multiple choice examina-tion that students take at the completion of theirclinical pathophysiology course consists of 98 ques-tions, with two examination questions dealing spe-cifically with melanoma. One question dealt withcommon melanoma locations and the other withrisk factors for its development. Of the students,91% correctly answered the question regardingcommon melanoma anatomic locations, whereas61% of the class correctly answered the risk factorquestion. This same medical school class had a22.6% detection rate using SPs, which focuses onthe third step of the pyramid ‘‘show how.’’ Althoughour students could recapitulate knowledge, theyhad not successfully integrated it into a clinical skillindicating the need for further refinement of ourcurriculum.
Our results support the findings of previousstudies reporting a low rate of melanoma detectionby medical students.9,10 Robinson and McGaghie9
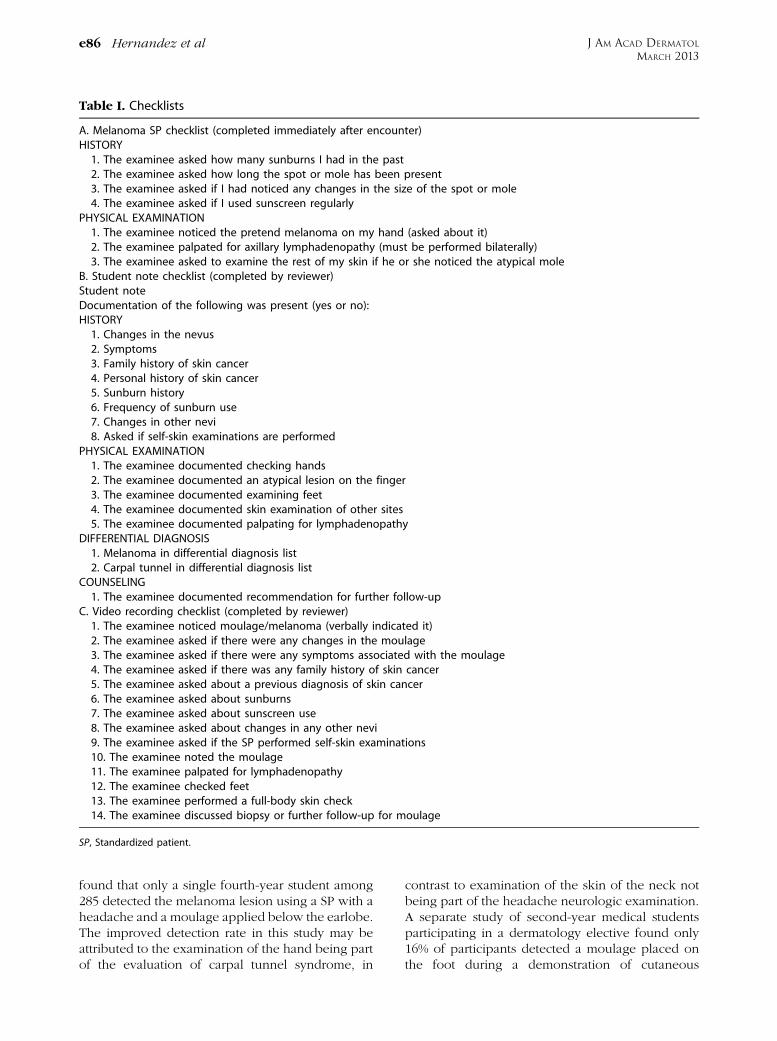
Table I. Checklists
A. Melanoma SP checklist (completed immediately after encounter)HISTORY1. The examinee asked how many sunburns I had in the past2. The examinee asked how long the spot or mole has been present3. The examinee asked if I had noticed any changes in the size of the spot or mole4. The examinee asked if I used sunscreen regularly
PHYSICAL EXAMINATION1. The examinee noticed the pretend melanoma on my hand (asked about it)2. The examinee palpated for axillary lymphadenopathy (must be performed bilaterally)3. The examinee asked to examine the rest of my skin if he or she noticed the atypical mole
B. Student note checklist (completed by reviewer)Student noteDocumentation of the following was present (yes or no):HISTORY1. Changes in the nevus2. Symptoms3. Family history of skin cancer4. Personal history of skin cancer5. Sunburn history6. Frequency of sunburn use7. Changes in other nevi8. Asked if self-skin examinations are performed
PHYSICAL EXAMINATION1. The examinee documented checking hands2. The examinee documented an atypical lesion on the finger3. The examinee documented examining feet4. The examinee documented skin examination of other sites5. The examinee documented palpating for lymphadenopathy
DIFFERENTIAL DIAGNOSIS1. Melanoma in differential diagnosis list2. Carpal tunnel in differential diagnosis list
COUNSELING1. The examinee documented recommendation for further follow-up
C. Video recording checklist (completed by reviewer)1. The examinee noticed moulage/melanoma (verbally indicated it)2. The examinee asked if there were any changes in the moulage3. The examinee asked if there were any symptoms associated with the moulage4. The examinee asked if there was any family history of skin cancer5. The examinee asked about a previous diagnosis of skin cancer6. The examinee asked about sunburns7. The examinee asked about sunscreen use8. The examinee asked about changes in any other nevi9. The examinee asked if the SP performed self-skin examinations10. The examinee noted the moulage11. The examinee palpated for lymphadenopathy12. The examinee checked feet13. The examinee performed a full-body skin check14. The examinee discussed biopsy or further follow-up for moulage
SP, Standardized patient.
J AM ACAD DERMATOL
MARCH 2013e86 Hernandez et al
found that only a single fourth-year student among285 detected the melanoma lesion using a SP with aheadache and a moulage applied below the earlobe.The improved detection rate in this study may beattributed to the examination of the hand being partof the evaluation of carpal tunnel syndrome, in
contrast to examination of the skin of the neck notbeing part of the headache neurologic examination.A separate study of second-year medical studentsparticipating in a dermatology elective found only16% of participants detected a moulage placed onthe foot during a demonstration of cutaneous
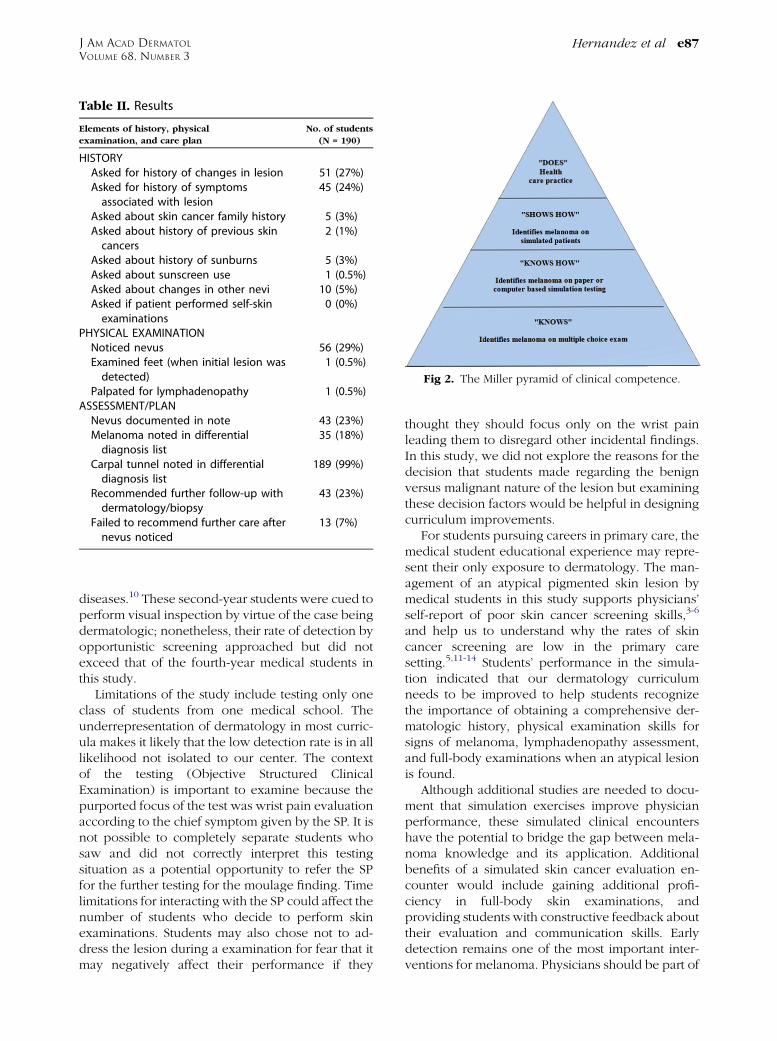
Table II. Results
Elements of history, physical
examination, and care plan
No. of students
(N = 190)
HISTORYAsked for history of changes in lesion 51 (27%)Asked for history of symptomsassociated with lesion
45 (24%)
Asked about skin cancer family history 5 (3%)Asked about history of previous skincancers
2 (1%)
Asked about history of sunburns 5 (3%)Asked about sunscreen use 1 (0.5%)Asked about changes in other nevi 10 (5%)Asked if patient performed self-skinexaminations
0 (0%)
PHYSICAL EXAMINATIONNoticed nevus 56 (29%)Examined feet (when initial lesion wasdetected)
1 (0.5%)
Palpated for lymphadenopathy 1 (0.5%)ASSESSMENT/PLANNevus documented in note 43 (23%)Melanoma noted in differentialdiagnosis list
35 (18%)
Carpal tunnel noted in differentialdiagnosis list
189 (99%)
Recommended further follow-up withdermatology/biopsy
43 (23%)
Failed to recommend further care afternevus noticed
13 (7%)
Fig 2. The Miller pyramid of clinical competence.
J AM ACAD DERMATOL
VOLUME 68, NUMBER 3Hernandez et al e87
diseases.10 These second-year students were cued toperform visual inspection by virtue of the case beingdermatologic; nonetheless, their rate of detection byopportunistic screening approached but did notexceed that of the fourth-year medical students inthis study.
Limitations of the study include testing only oneclass of students from one medical school. Theunderrepresentation of dermatology in most curric-ula makes it likely that the low detection rate is in alllikelihood not isolated to our center. The contextof the testing (Objective Structured ClinicalExamination) is important to examine because thepurported focus of the test was wrist pain evaluationaccording to the chief symptom given by the SP. It isnot possible to completely separate students whosaw and did not correctly interpret this testingsituation as a potential opportunity to refer the SPfor the further testing for the moulage finding. Timelimitations for interacting with the SP could affect thenumber of students who decide to perform skinexaminations. Students may also chose not to ad-dress the lesion during a examination for fear that itmay negatively affect their performance if they
thought they should focus only on the wrist painleading them to disregard other incidental findings.In this study, we did not explore the reasons for thedecision that students made regarding the benignversus malignant nature of the lesion but examiningthese decision factors would be helpful in designingcurriculum improvements.
For students pursuing careers in primary care, themedical student educational experience may repre-sent their only exposure to dermatology. The man-agement of an atypical pigmented skin lesion bymedical students in this study supports physicians’self-report of poor skin cancer screening skills,3-6
and help us to understand why the rates of skincancer screening are low in the primary caresetting.5,11-14 Students’ performance in the simula-tion indicated that our dermatology curriculumneeds to be improved to help students recognizethe importance of obtaining a comprehensive der-matologic history, physical examination skills forsigns of melanoma, lymphadenopathy assessment,and full-body examinations when an atypical lesionis found.
Although additional studies are needed to docu-ment that simulation exercises improve physicianperformance, these simulated clinical encountershave the potential to bridge the gap between mela-noma knowledge and its application. Additionalbenefits of a simulated skin cancer evaluation en-counter would include gaining additional profi-ciency in full-body skin examinations, andproviding students with constructive feedback abouttheir evaluation and communication skills. Earlydetection remains one of the most important inter-ventions for melanoma. Physicians should be part of

J AM ACAD DERMATOL
MARCH 2013e88 Hernandez et al
the solution for early melanoma detection and not afactor in the delay of care.
REFERENCES
1. Mark R. Prevention and control of melanoma: the public
health approach. CA Cancer J Clin 1996;46:199-216.
2. Richard MA, Grob JJ, Avril MF, Delaunay M, Gouvernet J,
Wolkenstein P, et al. Delays in diagnosis and melanoma
prognosis (II): the role of doctors. Int J Cancer 2000;89:280-5.
3. Moore M, Geller A, Zhang Z, Hayes B, Bergstrom K, Graves J,
et al. Skin cancer examination teaching in US medical educa-
tion. Arch Dermatol 2006;142:439-44.
4. American Cancer Society. 1989 Survey of physicians’ attitudes
and practice in early cancer detection. CA Cancer J Clin 1990;
40:77-101.
5. Federman DG, Concato J, Caralis PV, Hunkele GE, Kirsner RS.
Screening for skin cancer in primary care settings. Arch
Dermatol 1997;133:1423-5.
6. Cassileth BR, Clark W Jr, Lusk EJ, Fredrick BE, Thompson CJ,
Walsh WP. How well do physicians recognize melanoma
and other problem lesions? J Am Acad Dermatol 1986;14:
555-60.
7. Barrows HS. An overview of the uses of standardized patients
for teaching and evaluating clinical skills; AAMC. Acad Med
1993;68:443-51.
8. Miller G. The assessment of clinical skills/competence/per-
formance. Acad Med 1990;65:S63-7.
9. Robinson JK, McGaghie WC. Skin cancer detection in a clinical
practice examination with standardized patients. J Am Acad
Dermatol 1996;34:709-11.
10. Robinson JK, Lio P, Hernandez C, Kim N, Lee K, Wickless H,
et al. Medical student detection of melanoma: clinical skills.
Arch Dermatol 2010;146:1175-7.
11. Kirsner RS, Muhkerjee S, Federman DG. Skin cancer screening
in primary care: prevalence and barriers. J Am Acad Dermatol
1999;41:564-6.
12. Oliveria SA, Christos PJ, Marghoob AA, Halpern AC. Skin cancer
screening and prevention in the primary care setting: national
ambulatory medical care survey 1997. J Gen Intern Med 2001;
16:297-301.
13. Wender RC. Barriers to effective skin cancer detection. Cancer
1995;75(Suppl):691-8.
14. Dolan NC, Martin GJ, Robinson JK, Rademaker AW. Skin cancer
control practices among physicians in a university general
medicine practice. J Gen Intern Med 1995;10:515-9.