Embed Size (px)
Citation preview

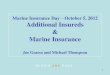
Assessment Module Layout
Questions
Correct Answers
Incorrect Answers
Link to Additional Study Materials
Link to Didactic Content for
Additional Study
Revisit Initial Questions &
Answer Correctly
Critique/Rationale
Link to Additional Study Materials
Other Enduring Materials (CME)
Digitally Captured Live Presentations
Post to a Discussion Forum
Materials Outside of AGA Including TheGut.org
Other
Application to Practice
Critique/Rationale
Evaluation

Question answered correctly
A 52 year old Caucasian male is referred to you for heartburn. He has a 20 yr history of heartburn with
intermittent symptoms while on once a day PPI therapy. He denies dysphagia, nausea or vomiting. His physical examination is notable for a BMI of 40, but his physical examination and laboratory studies
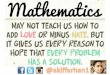
are otherwise unremarkable. EGD shows the following in the distal esophagus:
Endoscopic biopsies are likely to show:
A: Normal gastric epithelium.B: Intestinal metaplasia.C: Erosive esophagitis.
D: Squamous cell carcinoma.E: Adenocarcinoma.

Critique/Rationale:
Barrett’s esophagus is found in approximately 6 to 12% of patients undergoing endoscopy for symptoms
of GERD and in 1% or less of unselected patient populations undergoing endoscopy. The prevalence
of long-segment Barrett’s esophagus (3 cm or more of interstitial metaplasia) is approximately 5%, whereas that of short-segment Barrett’s esophagus (less than 3 cm of interstitial metaplasia) is approximately 6 to
12% in patients undergoing endoscopy in a variety of settings. Autopsy data suggest that the majority of cases of Barrett’s esophagus go undetected in the
general population. This may be due to the observation that esophageal sensitivity to acid
perfusion is impaired in these patients. Furthermore, only approximately 5% of patients with esophageal adenocarcinoma have an antecedent diagnosis of
Barrett’s esophagus.

Correct Answerswill Link to Additional Study
Materials
AGA Institute Cases Online A Woman with Worsening GERD and Barrett’s
Esophagus
TheGut.org
High Stakes and High Risk: Improving the Odds in Barrett's Esophagus, Colorectal Cancer and NSAID-
Induced Complications
PubMedThe development and validation of an endoscopic
grading system for Barrett's esophagus:
the Prague C & M criteria
Practice guidelines
ASGE: Role of Endoscopy in The Management of Barrett's Esophagus
SSAT: Patient Care Guidelines
Management of Barrett's Esophagus

Additional Links for Reference and Study
AGA InstitutePosition Statement and Technical
Review Role of the Gastroenterologist in the
Management of Esophageal Carcinoma
GI Core Curriculum Training in Acid-Peptic Disease
(chapter 1, third edition, May 2007)
Future Trends CommitteeEndoscopic advances (October 2006)

Question answered incorrectly
A 52 year old Caucasian male is referred to you for heartburn. He has a 20 yr history of heartburn with
intermittent symptoms while on once a day PPI therapy. He denies dysphagia, nausea or vomiting. His physical examination is notable for a BMI of 40, but his physical examination and laboratory studies are otherwise remarkable. EGD shows the following
in the distal esophagus:
Endoscopic biopsies are likely to show:
A: Normal gastric epithelium.B: Intestinal metaplasia.C: Erosive esophagitis.
D: Squamous cell carcinoma.E: Adenocarcinoma.

Incorrect Answers will Link to Didactic Content for
Additional Study
Barrett’s esophagus is a complication of gastroesophageal reflux disease. Endoscopically, this
lesion is recognized by displacement of the squamocolumnar junction proximal to the
gastroesophageal junction. Histologically, it is characterized by metaplastic transformation of the esophageal squamous epithelium to a specialized
columnar intestinal metaplastic epithelium with acid mucin-containing goblet cells
Return to question for retest:

Revisit Initial Question & Answer Correctly
Question
A 52 year old Caucasian male is referred to you for heartburn. He has a 20 yr history of heartburn with
intermittent symptoms while on once a day PPI therapy. He denies dysphagia, nausea or vomiting. His physical examination is notable for a BMI of 40, but his physical examination and laboratory studies
are otherwise unremarkable. EGD shows the following in the distal esophagus:
Endoscopic biopsies are likely to show:
A: Normal gastric epithelium.B: Intestinal metaplasia.C: Erosive esophagitis.
D: Squamous cell carcinoma.E: Adenocarcinoma.

Critique/Rationale:
Barrett’s esophagus is found in approximately 6 to 12% of patients undergoing endoscopy for symptoms
of GERD and in 1% or less of unselected patient populations undergoing endoscopy. The prevalence
of long-segment Barrett’s esophagus (3 cm or more of interstitial metaplasia) is approximately 5%, whereas that of short-segment Barrett’s esophagus (less than 3 cm of interstitial metaplasia) is approximately 6 to
12% in patients undergoing endoscopy in a variety of settings. Autopsy data suggest that the majority of cases of Barrett’s esophagus go undetected in the
general population. This may be due to the observation that esophageal sensitivity to acid
perfusion is impaired in these patients. Furthermore, only approximately 5% of patients with esophageal adenocarcinoma have an antecedent diagnosis of
Barrett’s esophagus.

Correct Answerswill Link to Additional Study
Materials
AGA Institute Cases Online A Woman with Worsening GERD and Barrett’s
Esophagus
TheGut.org
High Stakes and High Risk: Improving the Odds in Barrett's Esophagus, Colorectal Cancer and NSAID-
Induced Complications
PubMedThe development and validation of an endoscopic
grading system for Barrett's esophagus:
the Prague C & M criteria
Practice guidelines
ASGE: Role of Endoscopy in The Management of Barrett's Esophagus
SSAT: Patient Care Guidelines
Management of Barrett's Esophagus

Additional Links for Reference and Study
AGA InstitutePosition Statement and Technical
Review Role of the Gastroenterologist in the
Management of Esophageal Carcinoma
GI Core Curriculum Training in Acid-Peptic Disease
(chapter 1, third edition, May 2007)
Future Trends CommitteeEndoscopic advances (October 2006)

Application to Practice(didactic)
The epidemiology of Barrett's esophagus is incompletely described. Published studies indicate it is
more prevalent in older, white males, a pattern that mirrors that of esophageal adenocarcinoma (EAC). Emerging data suggests that Barrett's may be as
prevalent in Hispanics as whites, and that rates among women and other minority groups are increasing.
In patients with esophageal reflux disease, those with Barrett's are more likely to report the onset of GERD at
an early age, have increased duration of symptoms, increased severity of nocturnal symptoms and more
GERD-related complications such as esophagitis, ulceration, stricture and bleeding. The increased risk of Barrett's in this type of patient may be great, with some
studies citing a 6.4 fold increase in those with symptoms greater than 10 years. Thus, symptoms of
Barrett's are indistinguishable from symptoms of GERD without Barrett's complications. Further, many with
Barrett's have no symptoms at all.
Other factors have also emerged as potentially related to the development of EAC, including tobacco use, diet low in fruits and vegetables, and increased body mass index (BMI). Interestingly, evidence suggests that use of aspirin/NSAIDs may be associated with decreased
risks of EAC.

AGA CME Café (2005):Barrett's Esophagus and
Adenocarcinoma

AGA InstituteDiscussion Forum

AGA InstituteDiscussion Forum
“How frequently do you screen your at risk patients?
Every two or three years?”

Practice Improvement Modules (PIMs)
Option for members to build their own PIMs around Barrett’s Esophagus:
• How does your practice track patients with interstitial metaplasia, interstitial metaplasia with low-grade and high-grade metaplasia?
• What performance measures will you use to prospectively track how you manage
these patients? Etc.
[PIMs satisfy specific point requirements for MOC and are eligible for CME credit]

Assess learner’s experience
• Helpful, not helpful in making clinical decisions with your patients?
• How would you rank the utility of these educational materials on this topic?
• Are there any revisions you would you make to this educational material?
[Offer the member an opportunity to post their thoughts to an AGA Institute
discussion forum]

Back office functions:Log responses & route them
• To the member’s personal learning portfolio (populates CME credit and points toward MOC)
• To an activity database that aggregates member feedback
– Continuous needs assessment data
– Continuous member assessment of activity effectiveness (dynamic ranking
of materials when members search)
– Determine when educational activities need revision, content accuracy or
teaching effectiveness may have eroded

Benefits
• Real time assessment and modification of the questions and critiques
• Updates quicker based on learner responses and changes in the science
• Granular: substantive learning can be done in 10-15 minute increments
• Ubiquitously available from a desktop PC or PDA
• Paperless production will control costs

The Next Question
Four modules, thematically related, in sequence, and by design.
The plan:
“Think big, start small, scale fast.”
The concept:
“Aesthetic rigor: elegance, economy and formal coherence.”

Information Disseminated
Encourage Curiosity
Build a Professional Community
Support Research Enterprise
(Basic Science & Clinical)
Patient Care is
Delivered
Mission of a National Medical Society
Member Personal Learning Portfolio

Thanks to:
JB McGee, MD
Geoff Braden, MD
Jay Kuemmerle, MD
Ashley Lombard
Carrie Smith
Kwesi Agyeman