Embed Size (px)
Citation preview
Asthma Control: Setting Asthma Control: Setting GoalsGoals
Session: SY 1Session: SY 1
WAO – WISC2010Dubai December 2010
Eric D. BatemanEric D. BatemanProfessor of Respiratory Medicine, University of Cape TownProfessor of Respiratory Medicine, University of Cape TownDirector of University of Cape Town Lung InstituteDirector of University of Cape Town Lung Institute
Presenter DisclosuresPresenter DisclosuresEric D Bateman
Lecture Fees: AstraZeneca, Alk Abello, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Nycomed, Pfizer, TEVA
Consultancy or Advisory Boards: Almirall, AlkAbello, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Forest, Hoffmann la Roche, GlaxoSmithKline, Merck, Morria Biopharmaceuticals, Novartis, Nycomed, Pfizer, ScheringPlough
Industry-sponsored grants (Institution): Aeras, Almirall, Altana, AstraZeneca, Boehringer Ingelheim, Chiesi, Hoffmann la Roche, GlaxoSmithKline, Merck, Morria Biopharmaceuticals, Novartis, Nycomed, Pfizer.
Learning objectivesLearning objectives
Asthma Control: Setting GoalsAsthma Control: Setting Goals
� To review current thinking on what defines acceptable asthma control
� To review tools that are available to evaluate control
� To review how to set goals to achieve asthma control
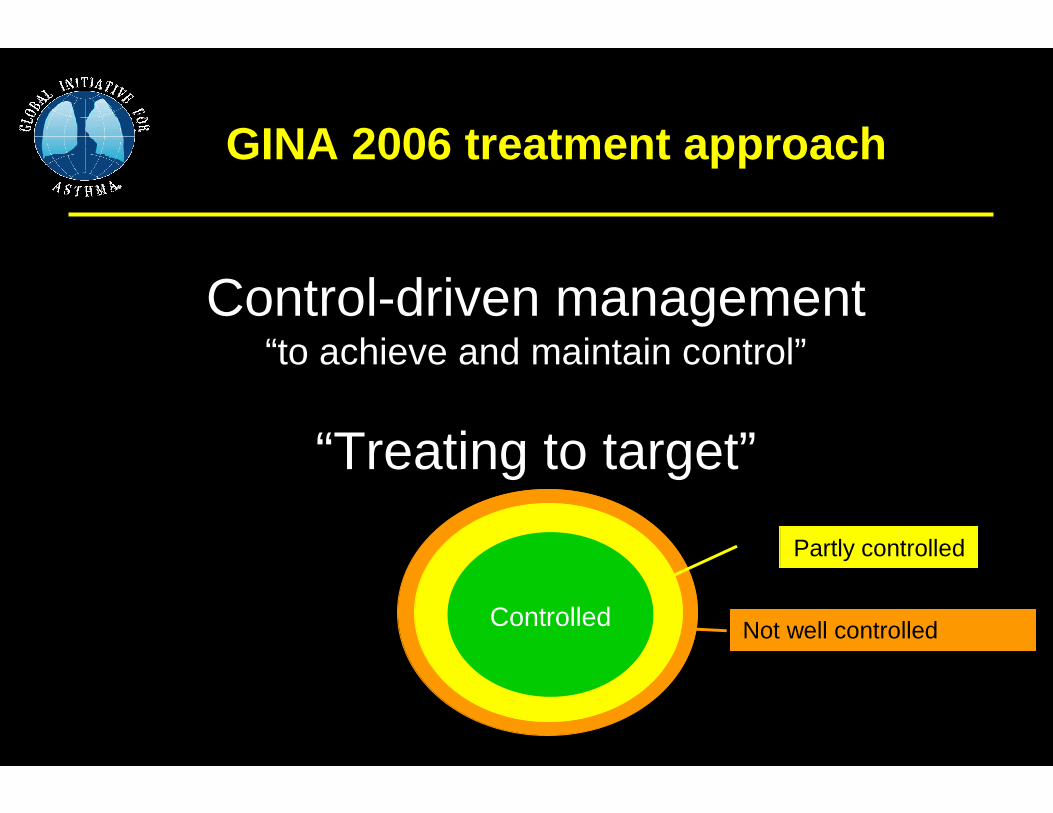
Not well controlled
GINA 2006 treatment approach
Control-driven management“to achieve and maintain control”
“Treating to target”
Partly controlled
Controlled
What do you view as What do you view as
Asthma Control: Setting GoalsAsthma Control: Setting Goals
� Acceptable control of asthma?
� Optimal control?
� Ideal control?
� Are they different?
Why ?
Why ?
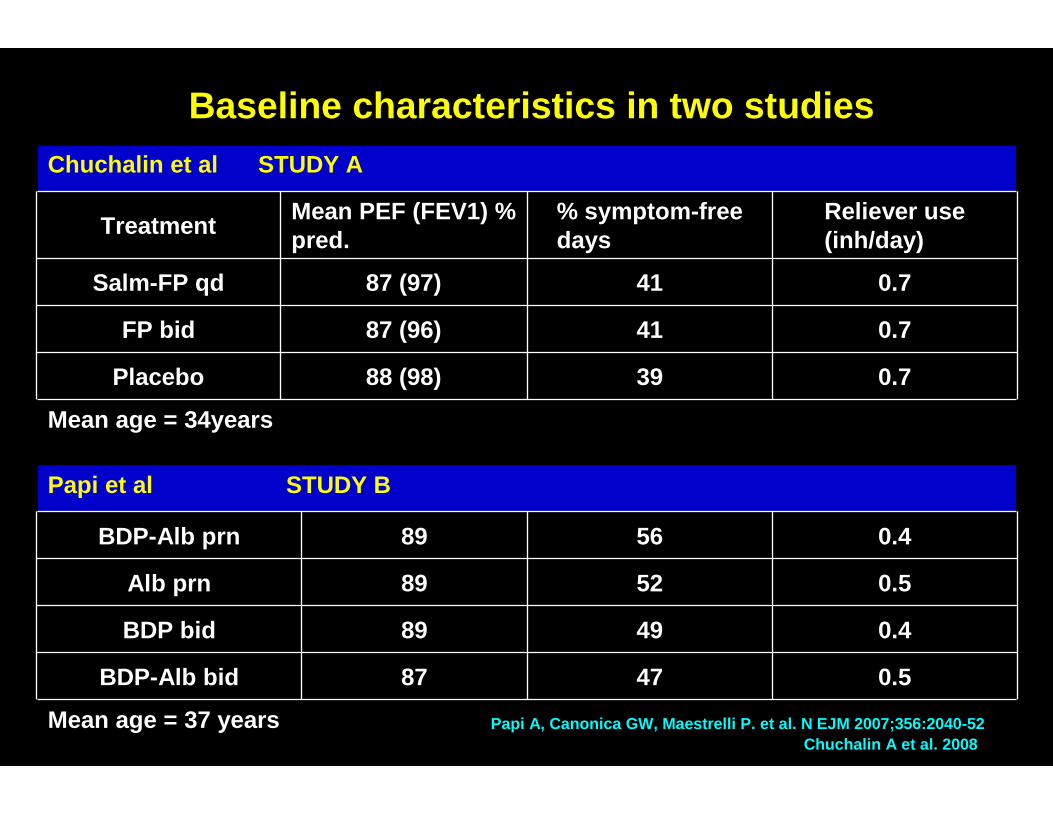
Baseline characteristics in two studiesChuchalin et al STUDY A
TreatmentMean PEF (FEV1) % pred.
% symptom-free days
Reliever use (inh/day)
Salm-FP qd 87 (97) 41 0.7
FP bid 87 (96) 41 0.7
Placebo 88 (98) 39 0.7
Mean age = 34years
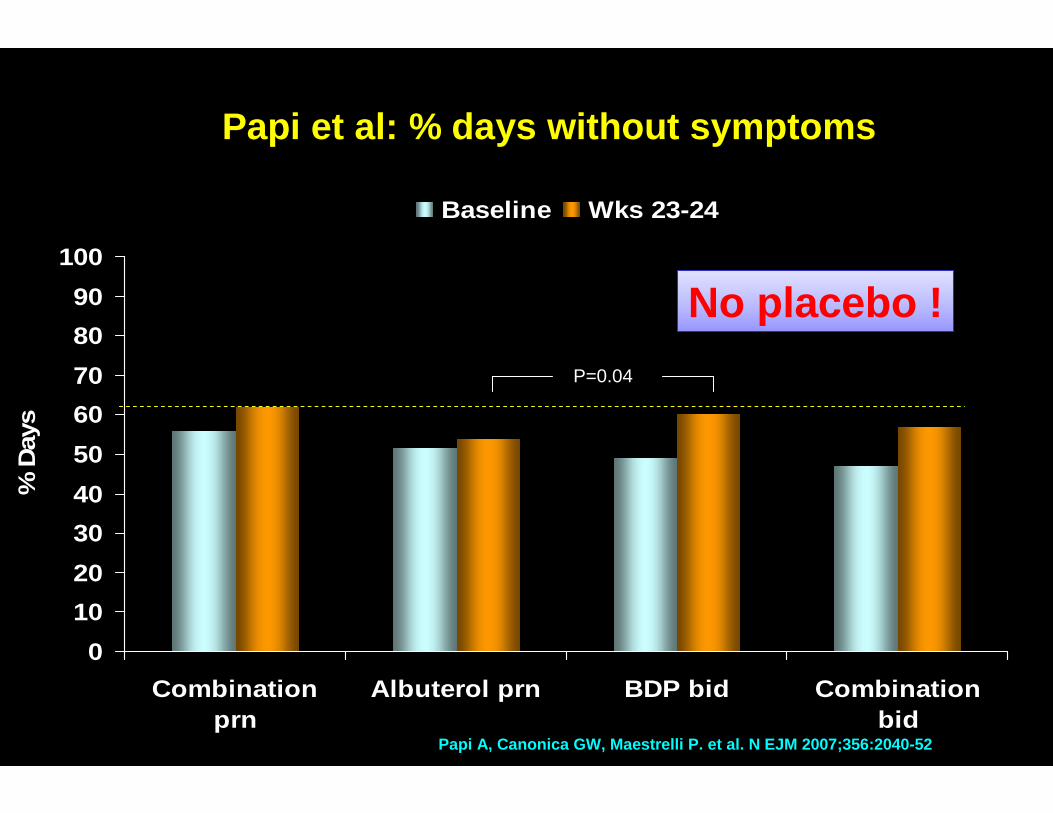
Papi et al STUDY B
BDP-Alb prn 89 56 0.4
Alb prn 89 52 0.5
BDP bid 89 49 0.4
BDP-Alb bid 87 47 0.5
Mean age = 37 yearsChuchalin A et al. 2008
Papi A, Canonica GW, Maestrelli P. et al. N EJM 2007 ;356:2040-52
0
10
20
30
40
50
60
70
80
90
100
Combinationprn
Albuterol prn BDP bid Combinationbid
% D
ays
Baseline Wks 23-24
P=0.04
Papi A, Canonica GW, Maestrelli P. et al. N EJM 2007;356:2040-52
Papi et al: % days without symptoms
No placebo !No placebo !
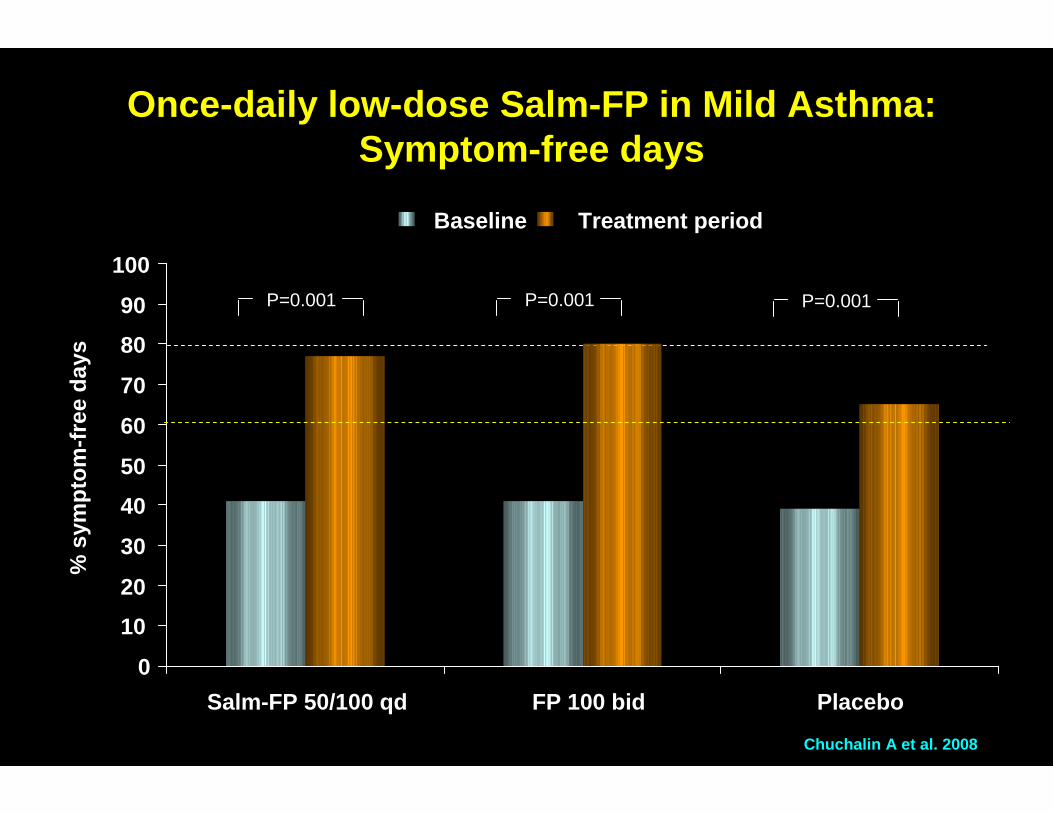
Once-daily low-dose Salm-FP in Mild Asthma:Symptom-free days
P=0.001
Chuchalin A et al. 2008
0
10
20
30
40
50
60
70
80
90
100
Salm-FP 50/100 qd
P=0.001 P=0.001
FP 100 bid Placebo
% s
ympt
om-f
ree
days
Baseline Treatment period
ATS/ERS Task Force Report, ATS/ERS Task Force Report, ATS/ERS Task Force Report, ATS/ERS Task Force Report, AJRCCM, AJRCCM, AJRCCM, AJRCCM, 2009; 180:592009; 180:592009; 180:592009; 180:59----99999999....
ATS/ERS Statement: Asthma Control and Exacerbations
Asthma goals are based on:Asthma goals are based on:
� What is possible to achieve with treatment
� Benefit – the immediate and long-term benefits of treatment
� Cost – financial / short and long-term side-effects of treatment
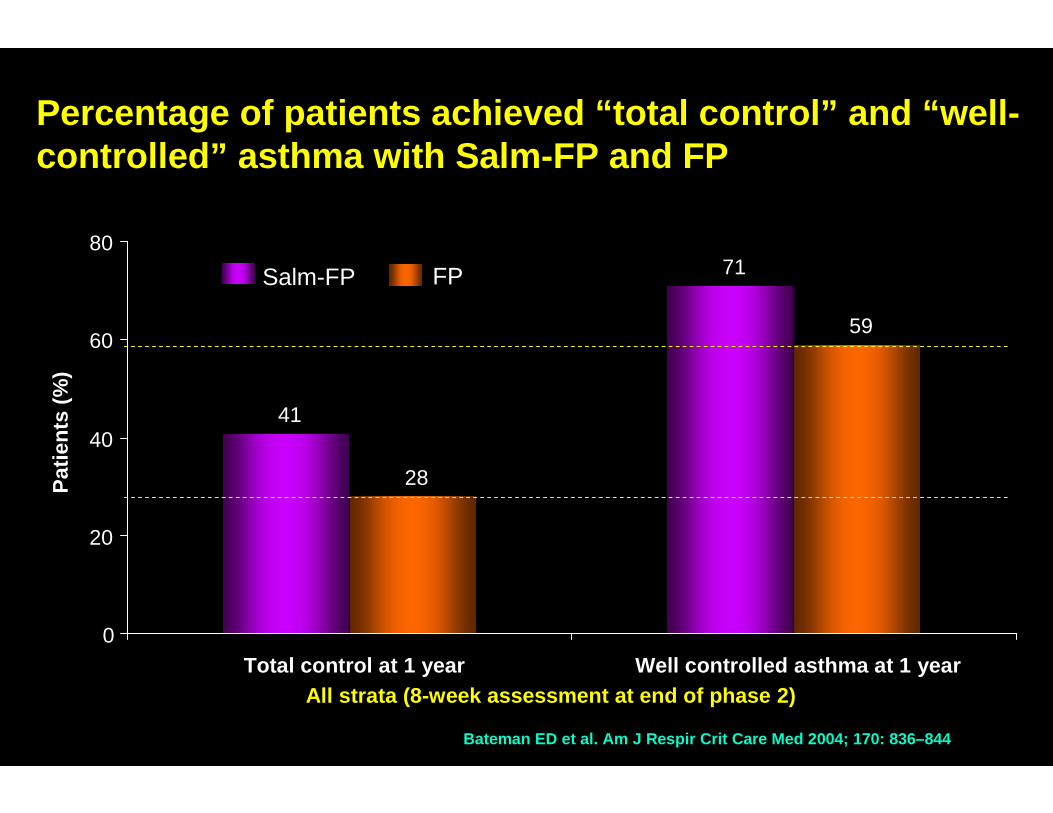
Percentage of patients achieved “total control” and “well-controlled” asthma with Salm-FP and FP
Bateman ED et al. Am J Respir Crit Care Med 2004; 170: 836–844
Salm-FP FP
41
71
28
59
0
20
40
60
80
Total control at 1 year Well controlled asthma at 1 year
Pat
ient
s (%
)
All strata (8-week assessment at end of phase 2)
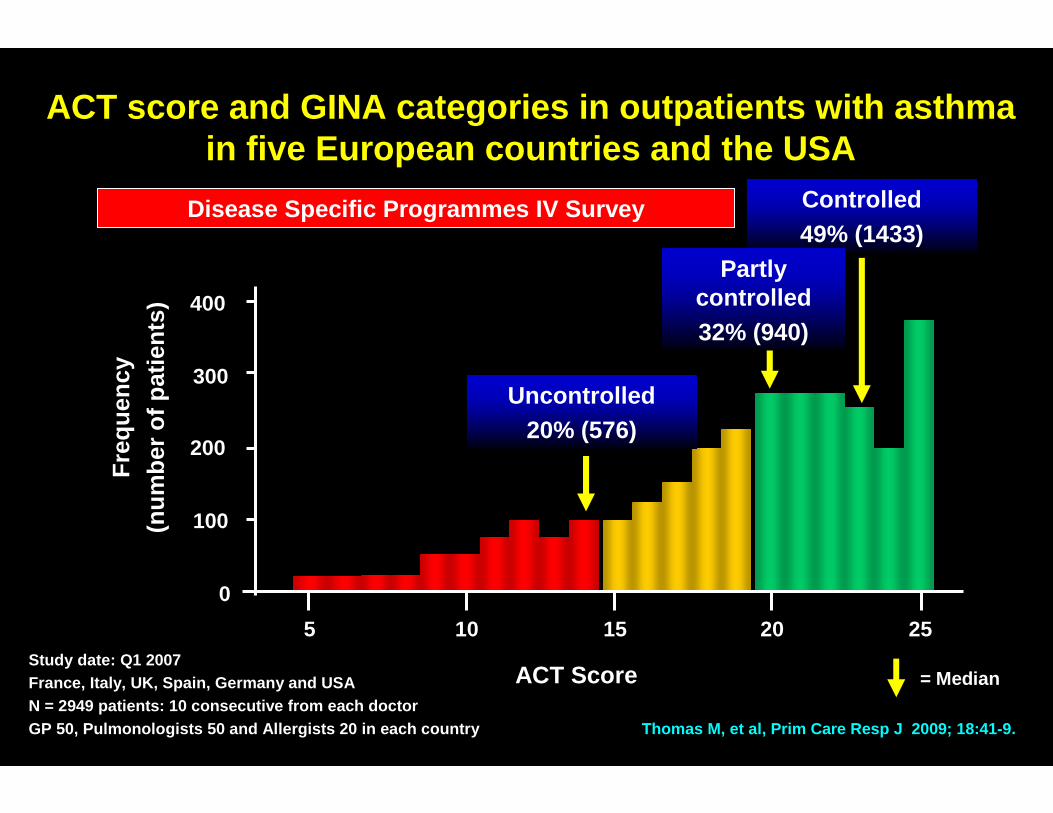
ACT score and GINA categories in outpatients with a sthma in five European countries and the USA
Thomas M, et al, Prim Care Resp J 2009; 18:41-9.
Study date: Q1 2007France, Italy, UK, Spain, Germany and USAN = 2949 patients: 10 consecutive from each doctorGP 50, Pulmonologists 50 and Allergists 20 in each country
Fre
quen
cy
(num
ber
of p
atie
nts)
ACT Score
400
300
200
100
0
5 10 15 20 25
Uncontrolled20% (576)
Controlled49% (1433)
= Median
Partly controlled32% (940)
Disease Specific Programmes IV Survey
GOAL: Who is less likely to achieve Well-Controlled asthma?
� Smokers < ex-smokers
� Men
� Longer duration of asthma
� Lower lung function
� Lack of control on ICS
Pedersen SE et al, JACI 2007
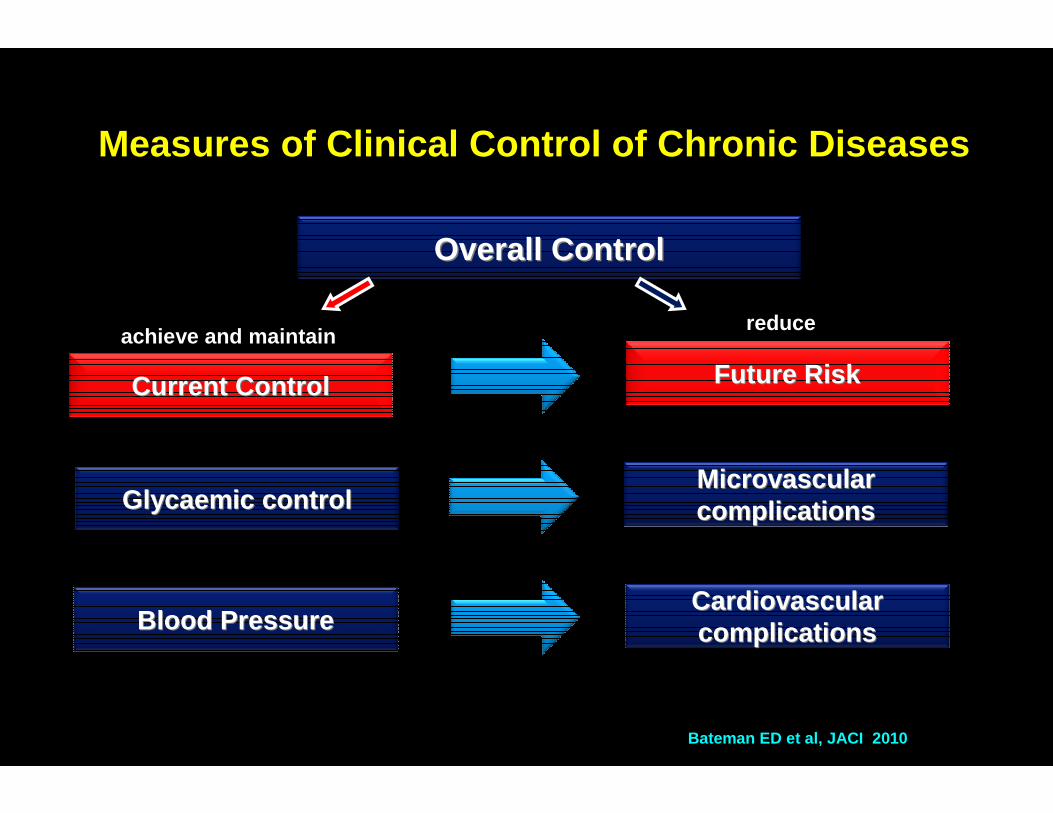
Measures of Clinical Control of Chronic Diseases
Overall ControlOverall Control
Current ControlCurrent Control
achieve and maintain
Future RiskFuture Risk
reduce
Bateman ED et al, JACI 2010
Glycaemic controlGlycaemic controlMicrovascularMicrovascularcomplicationscomplications
Blood PressureBlood PressureCardiovascularCardiovascularcomplicationscomplications
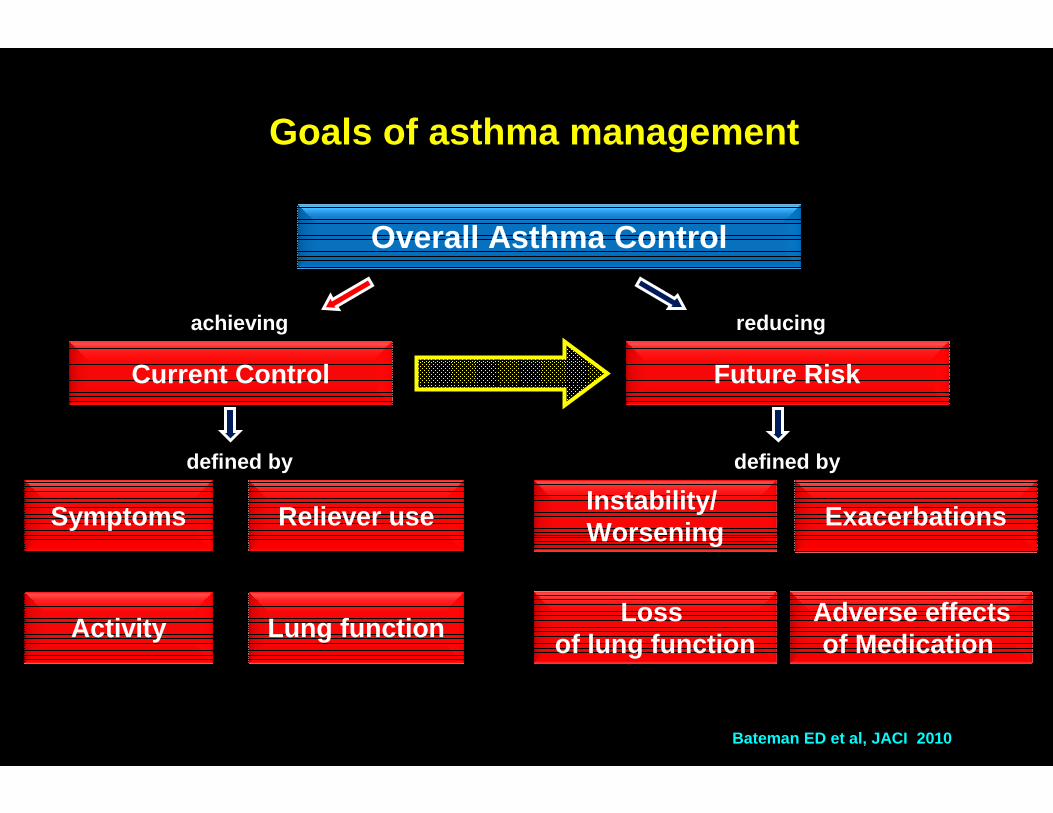
Goals of asthma management
Overall Asthma Control
Current Control
achieving
Symptoms
Activity
Reliever use
Lung function
defined by
Future Risk
Instability/ Worsening
Loss of lung function
Exacerbations
Adverse effectsof Medication
reducing
defined by
Bateman ED et al, JACI 2010
Measures of Asthma Control: categorical versus continuous measures?
“Control should preferably be described using continuous variables”Examples –ACQ, ACT, ACSS, ATAQ
“… if categorical descriptors are used, they should be based on clinically meaningful cut points”Examples –controlled, partly controlled, uncontrolled (GINA 2006)
Taylor DR Taylor DR Taylor DR Taylor DR et al, ERJ et al, ERJ et al, ERJ et al, ERJ 2008; 32:5452008; 32:5452008; 32:5452008; 32:545----554554554554
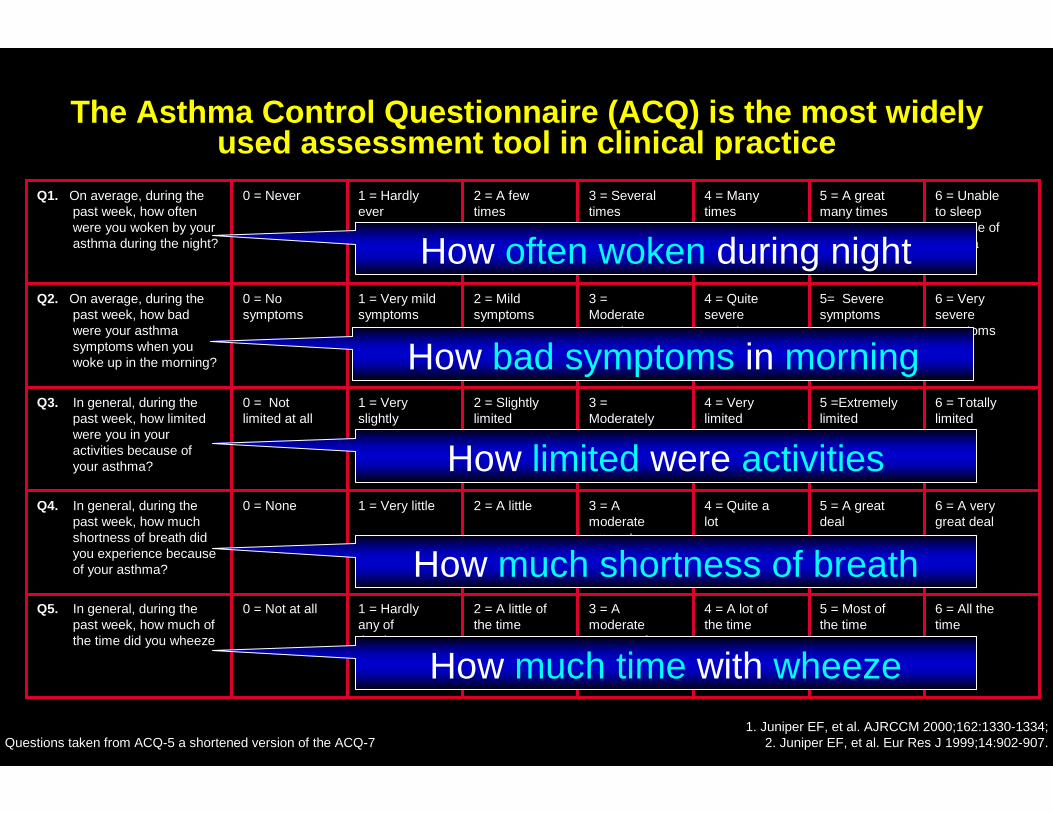
The Asthma Control Questionnaire (ACQ) is the most widely used assessment tool in clinical practice
6 = All thetime
5 = Most ofthe time
4 = A lot of the time
3 = A moderateamount ofthe time
2 = A little of the time
1 = Hardly any ofthe time
0 = Not at allQ5. In general, during the past week, how much of the time did you wheeze
6 = A verygreat deal
5 = A greatdeal
4 = Quite alot
3 = Amoderateamount
2 = A little1 = Very little0 = NoneQ4. In general, during the past week, how much shortness of breath did you experience because of your asthma?
6 = Totallylimited
5 =Extremelylimited
4 = Verylimited
3 = Moderatelylimited
2 = Slightly limited
1 = Very slightlylimited
0 = Not limited at all
Q3. In general, during the past week, how limited were you in your activities because of your asthma?
6 = Veryseveresymptoms
5= Severesymptoms
4 = Quite severesymptoms
3 =Moderatesymptoms
2 = Mild symptoms
1 = Very mild symptoms
0 = No symptoms
Q2. On average, during the past week, how bad were your asthma symptoms when you woke up in the morning?
6 = Unableto sleepbecause ofasthma
5 = A greatmany times
4 = Manytimes
3 = Several times
2 = A few times
1 = Hardly ever
0 = NeverQ1. On average, during the past week, how often were you woken by your asthma during the night?
1. Juniper EF, et al. AJRCCM 2000;162:1330-1334;2. Juniper EF, et al. Eur Res J 1999;14:902-907.Questions taken from ACQ-5 a shortened version of the ACQ-7
How often woken during night
How bad symptoms in morning
How limited were activities
How much shortness of breath
How much time with wheeze
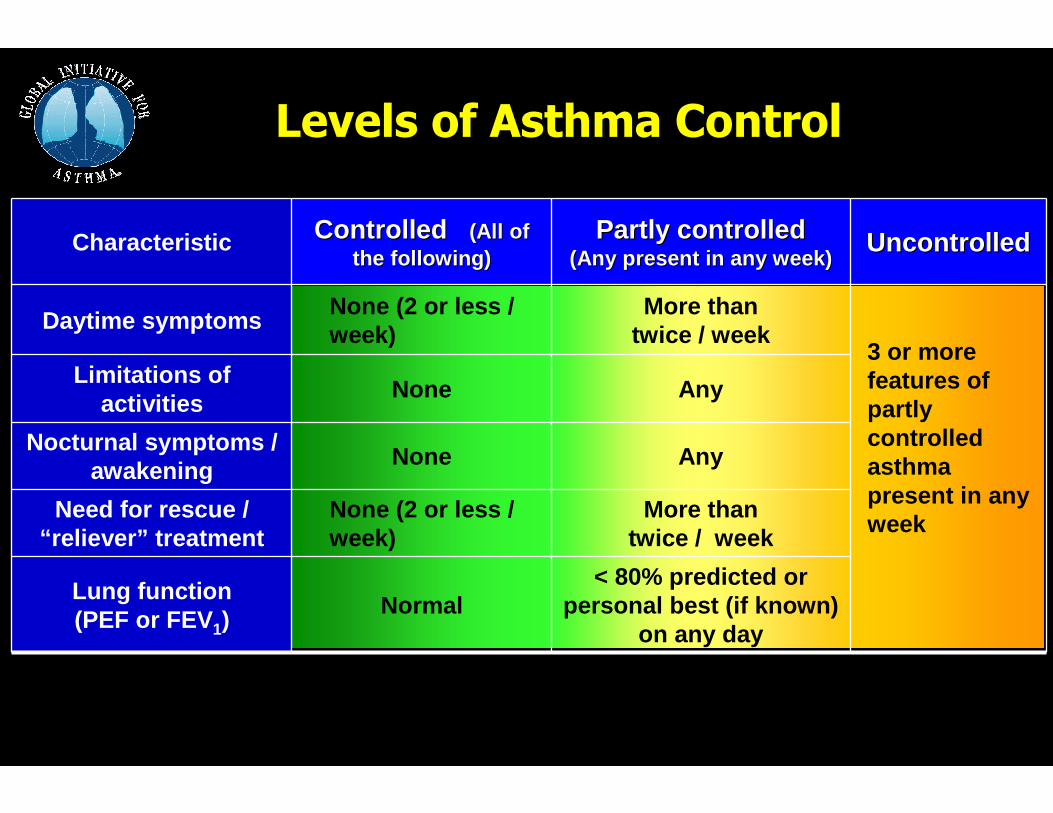
Levels of Asthma Control
Characteristic Controlled Controlled (All of (All of the following)the following)
Partly controlledPartly controlled(Any present in any week)(Any present in any week)
Uncontrolled Uncontrolled
Daytime symptomsNone (2 or less / week)
More than twice / week
3 or more features of partly controlled asthma present in any week
Limitations of activities
None Any
Nocturnal symptoms / awakening
None Any
Need for rescue / “reliever” treatment
None (2 or less / week)
More than twice / week
Lung function (PEF or FEV1)
Normal< 80% predicted or
personal best (if known) on any day
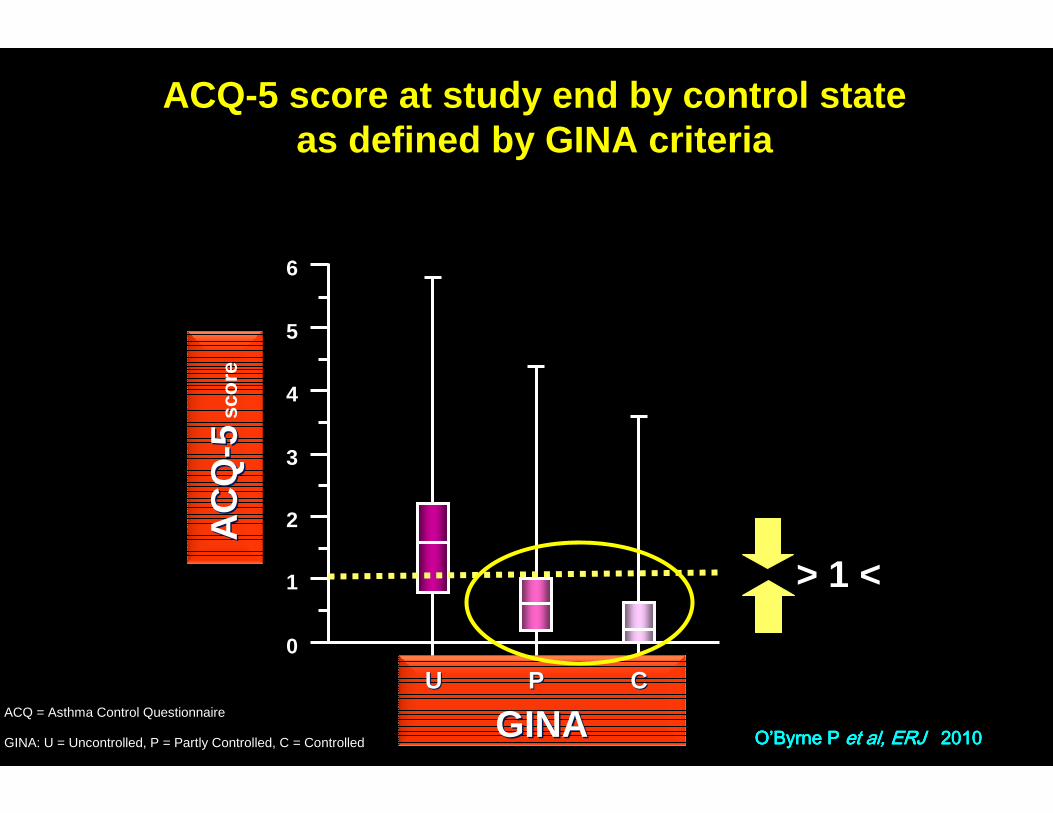
GINA GINA UU
0
6
2
1
3
4
5
PP CC
GINA: U = Uncontrolled, P = Partly Controlled, C = Controlled
ACQ = Asthma Control Questionnaire
OOOO’’’’Byrne P Byrne P Byrne P Byrne P et al, ERJ et al, ERJ et al, ERJ et al, ERJ 2010201020102010
ACQ-5 score at study end by control stateas defined by GINA criteria
> 1 <
AC
QA
CQ
-- 55sc
ore
What do ourWhat do ourpatients want?patients want?
No fear ofNo fear ofExacerbationsExacerbations
(attacks)(attacks)
More stability/More stability/predictabilitypredictability
No symptomsNo symptoms(Normal life)(Normal life)
Less medicinesLess medicinesLess costLess cost
Less side effectsLess side effects
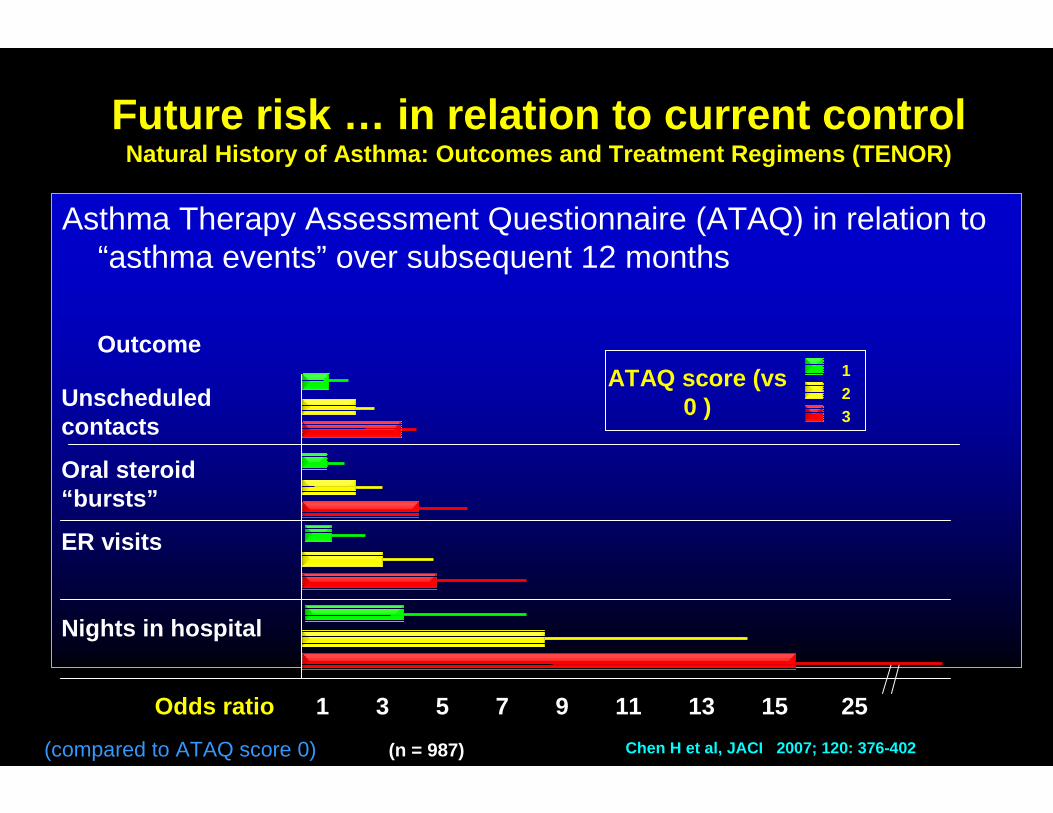
Asthma Therapy Assessment Questionnaire (ATAQ) in relation to “asthma events” over subsequent 12 months
Future risk … in relation to current controlNatural History of Asthma: Outcomes and Treatment R egimens (TENOR)
Unscheduled contacts
Oral steroid “bursts”
ER visits
Nights in hospital
1 3 5 7 9 11 13 15 25Odds ratio
ATAQ score (vs 0 )
123
(compared to ATAQ score 0)
Outcome
Chen H et al, JACI 2007; 120: 376-402(n = 987)
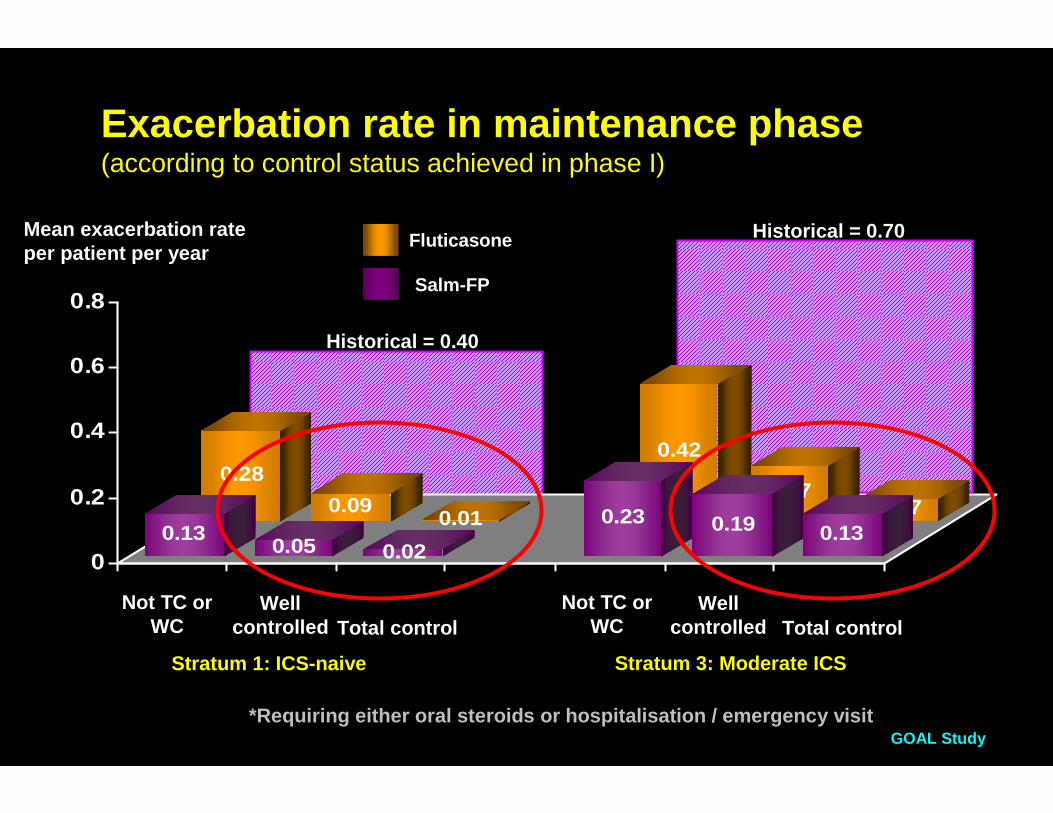
Historical = 0.40
Historical = 0.70
0.28
0.090.01
0.42
0.170.07
0.130.05 0.02
0.23 0.19 0.130
0.2
0.4
0.6
0.8
Stratum 1: ICS-naive Stratum 3: Moderate ICS
*Requiring either oral steroids or hospitalisation / emergency visitGOAL Study
Exacerbation rate in maintenance phase(according to control status achieved in phase I)
Not TC or WC
Well controlled Total control
Not TC or WC
Well controlled Total control
Mean exacerbation rate per patient per year
Fluticasone
Salm-FP
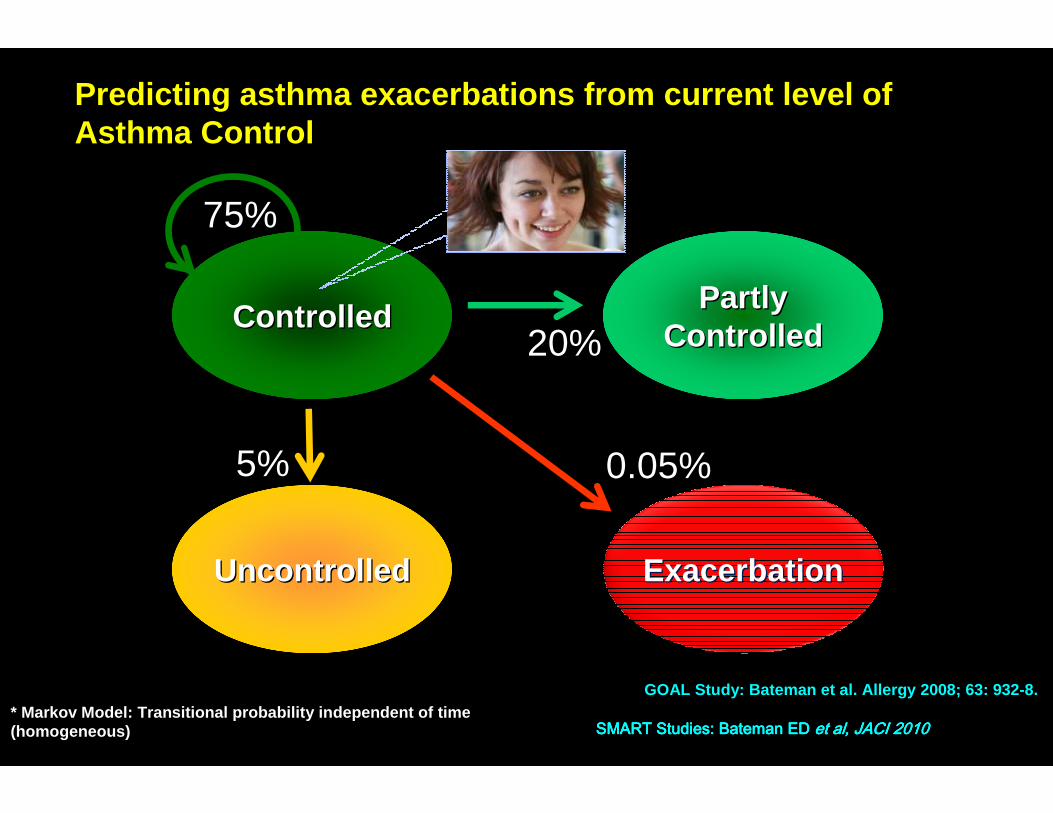
Predicting asthma exacerbations from current level of Asthma Control
PartlyPartlyControlledControlled
UncontrolledUncontrolled ExacerbationExacerbation
ControlledControlled
* Markov Model: Transitional probability independen t of time (homogeneous) SMART Studies: Bateman ED SMART Studies: Bateman ED SMART Studies: Bateman ED SMART Studies: Bateman ED et al, JACI 2010et al, JACI 2010et al, JACI 2010et al, JACI 2010
GOAL Study: Bateman et al. Allergy 2008; 63: 932-8.
75%
20%
5% 0.05%
PartlyPartlyControlledControlled
UncontrolledUncontrolled
ControlledControlled
* Markov Model: Transitional probability independen t of time (homogeneous) SMART Studies: Bateman ED SMART Studies: Bateman ED SMART Studies: Bateman ED SMART Studies: Bateman ED et al, JACI 2010et al, JACI 2010et al, JACI 2010et al, JACI 2010
GOAL Study: Bateman et al. Allergy 2008; 63: 932-8.
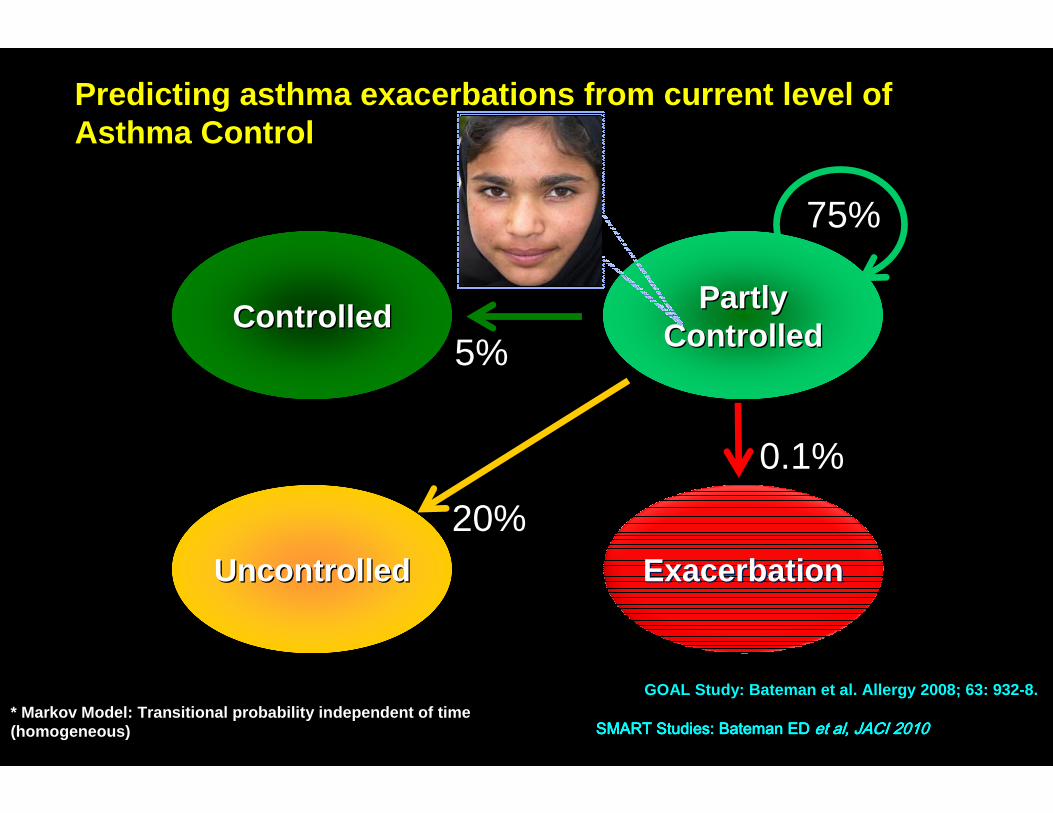
Predicting asthma exacerbations from current level of Asthma Control
ExacerbationExacerbation
75%
5%
20%
0.1%
PartlyPartlyControlledControlled
UncontrolledUncontrolled
ControlledControlled
* Markov Model: Transitional probability independen t of time (homogeneous) SMART Studies: Bateman ED SMART Studies: Bateman ED SMART Studies: Bateman ED SMART Studies: Bateman ED et al, JACI 2010et al, JACI 2010et al, JACI 2010et al, JACI 2010
GOAL Study: Bateman et al. Allergy 2008; 63: 932-8.
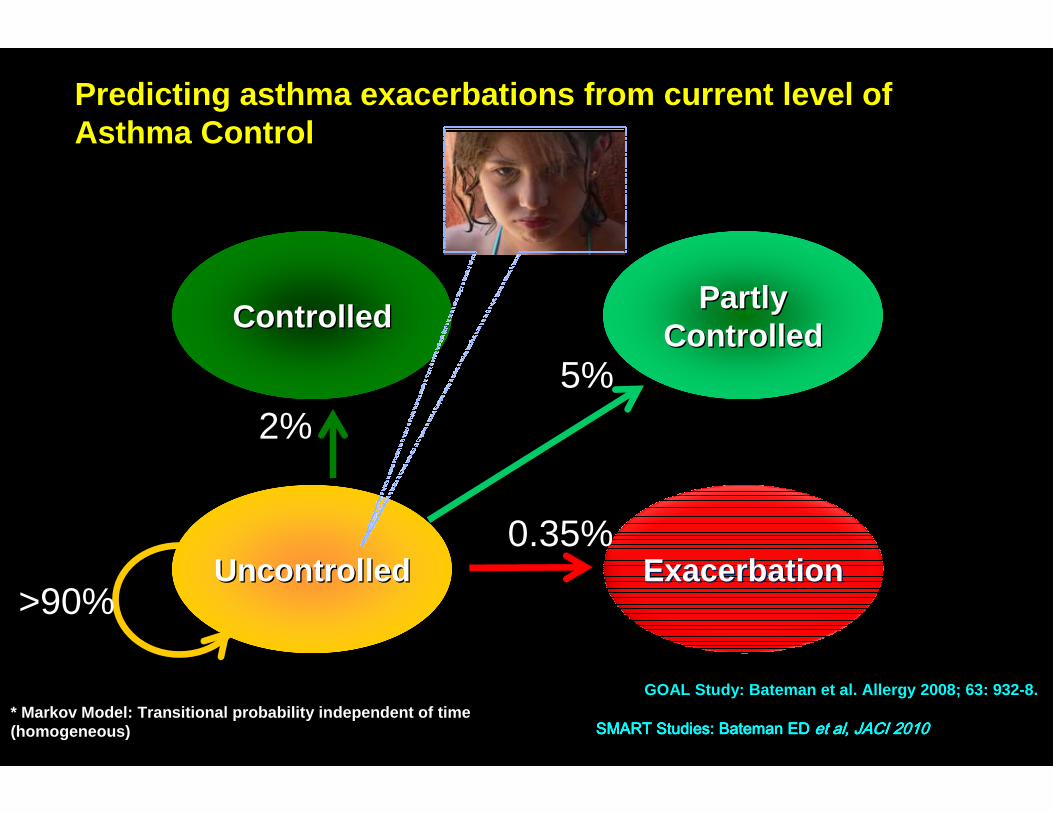
Predicting asthma exacerbations from current level of Asthma Control
ExacerbationExacerbation
2%5%
>90%
0.35%
SummarySummaryAsthma Control: Setting GoalsAsthma Control: Setting Goals
� What is acceptable asthma control? - Partly controlled or better
� How to measure control? – Composite measure (e.g. ACT) or categorical method (e.g. GINA)
� How to set goals? Individualize but understand risks and benefits, and differential effects of drugs