Embed Size (px)
Citation preview
Atelectasis, Pulmonary Edema, Acute Lung Injury and Acute
Respiratory Distress Syndrome
By: Shefaa’ Qa’qa’
Atelectasis (Collapse)
• Atelectasis refers either to incomplete expansion of the lungs (neonatal atelectasis) or to the collapse of previously inflated lung, producing areas of relatively airless pulmonary parenchyma.
• The main types of acquired atelectasis, which is encountered principally in adults, are the following:
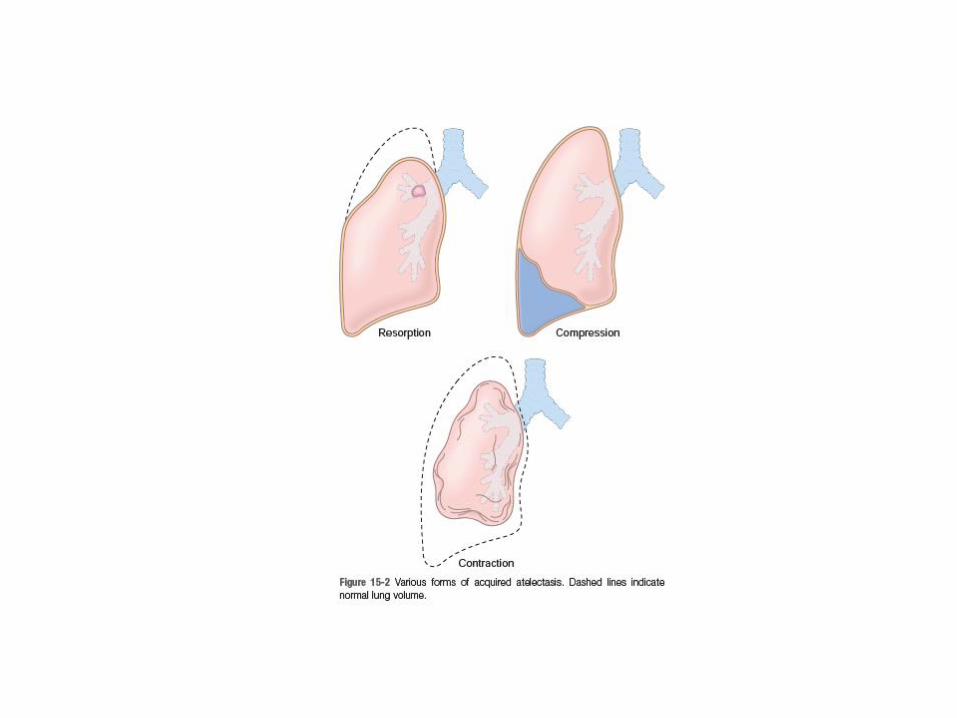
1. Resorption atelectasis: - stems from complete obstruction of an airway. Over time, air is resorbed from the dependent alveoli, which collapse. - Since lung volume is diminished, the mediastinum shifts toward the atelectatic lung. - Airway obstruction is most often caused by excessive secretions (e.g., mucus plugs) or exudates within smaller bronchi, as may occur in bronchial asthma, chronic bronchitis, bronchiectasis, and postoperative states. Aspiration of foreign bodies and, rarely, fragments of bronchial tumors may also lead to airway obstruction and atelectasis.
2. Compression atelectasis: - Results whenever significant volumes of fluid (transudate, exudate or blood), tumor, or air (pneumothorax) accumulate within the pleural cavity. - The mediastinum shifts away from the affected
lung. 3. Contraction atelectasis: occurs when focal or generalized pulmonary or pleural fibrosis prevents full lung expansion.
• Significant atelectasis reduces oxygenation and predisposes to infection.
• Except in cases caused by contraction, atelectasis is a reversible disorder.
Pulmonary Edema
• Pulmonary edema: leakage of excessive interstitial fluid which accumulates in alveolar spaces.
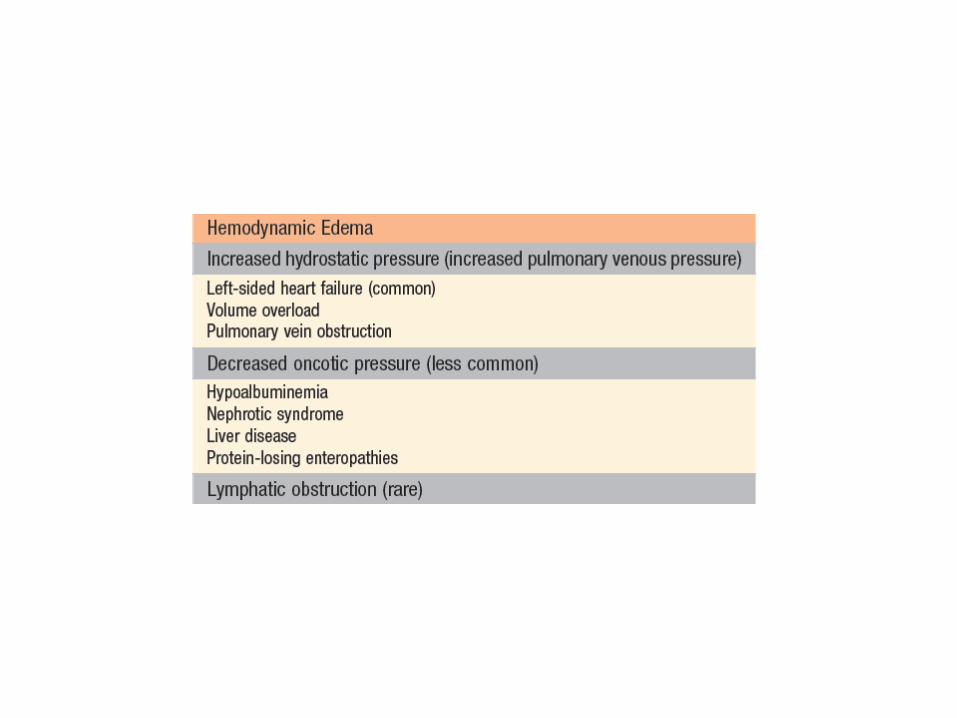
Hemodynamic Pulmonary Edema
• due to increased hydrostatic pressure, as occurs most commonly in left sided congestive heart failure.
• Fluid accumulates initially in the basal regions of the lower lobes because hydrostatic pressure is greatest in these sites (dependent edema).
• Histologically, the alveolar capillaries are engorged, and an intra-alveolar transudate appears as finely granular pale pink material.
• Alveolar microhemorrhages and hemosiderin laden macrophages (“heart failure” cells) may be present.
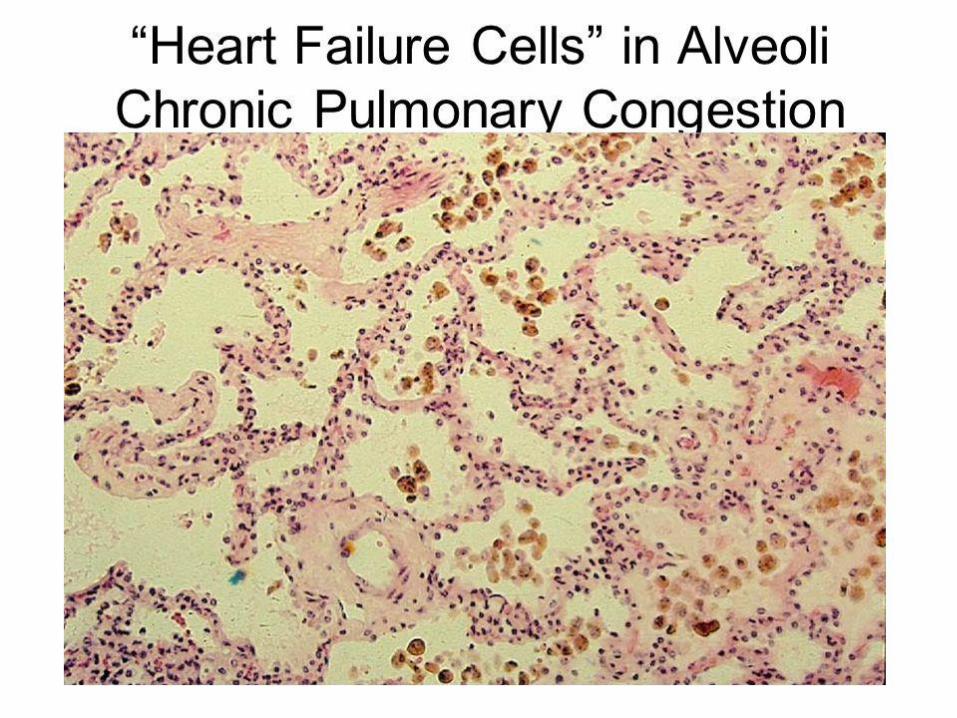
• In long-standing pulmonary congestion (e.g., as seen in mitral stenosis), hemosiderin-laden macrophages are abundant, and fibrosis and thickening of the alveolar walls cause the soggy lungs to become firm and brown (brown induration).
• These changes not only impair normal respiratory function but also predispose to infection.
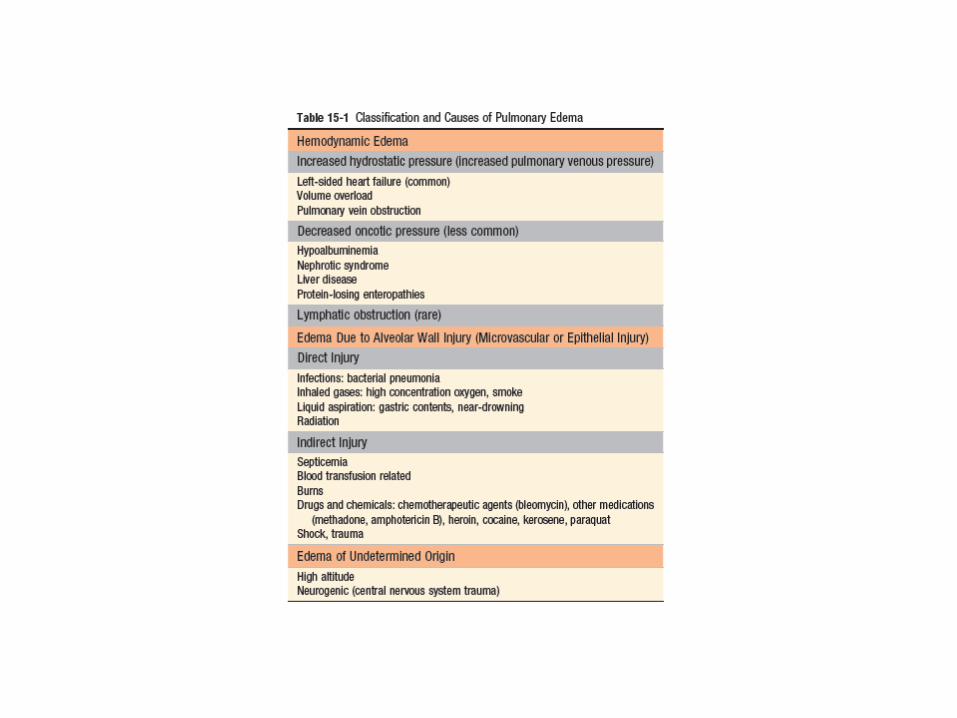
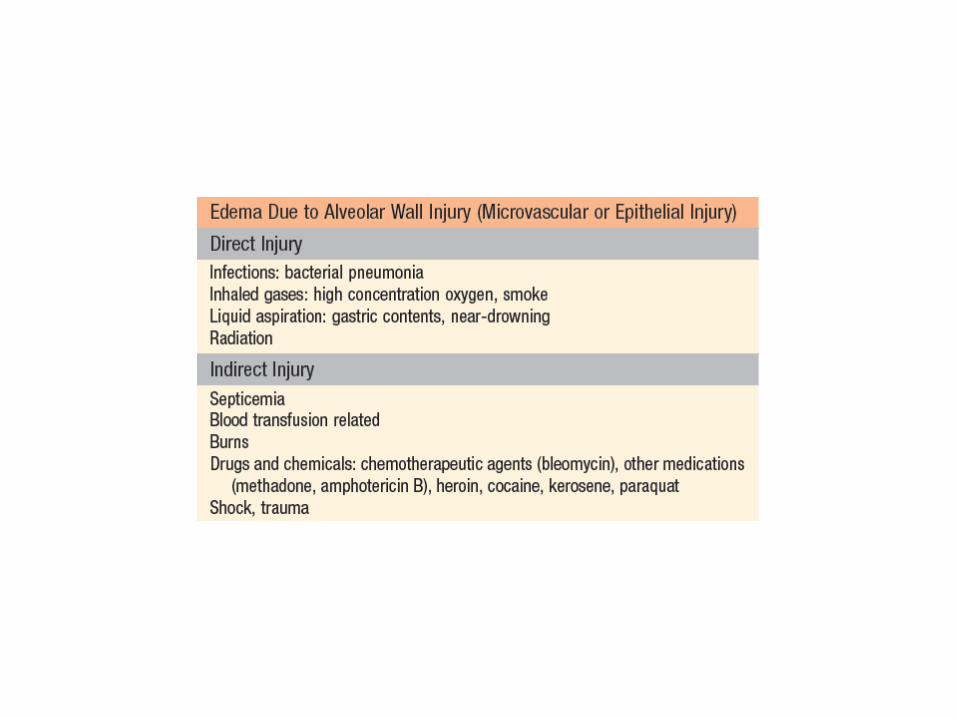
Edema Caused by Microvascular (Alveolar) Injury
• Non-cardiogenic pulmonary edema.
• Primary injury to the vascular endothelium or damage to alveolar epithelial cells (with secondary microvascular injury) produces an inflammatory exudate that leaks into the interstitial space and, in more severe cases, into the alveoli.
• Localized
• Diffuse ------- acute respiratory distress syndrome
Acute Lung Injury and Acute Respiratory Distress Syndrome
(Diffuse Alveolar Damage)
• Acute lung injury (ALI) also called noncardiogenic pulmonary edema.
• characterized by the abrupt onset of significant hypoxemia and bilateral pulmonary infiltrates in the absence of cardiac failure.
• Acute respiratory distress syndrome (ARDS) is a manifestation of severe ALI.
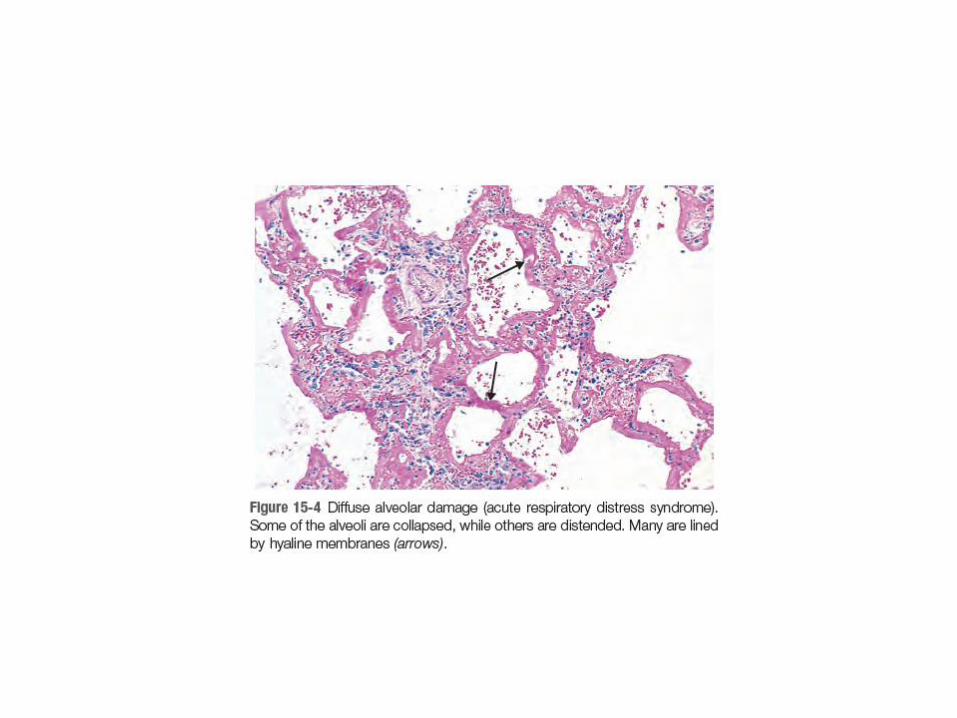
• The histologic manifestation of these diseases is diffuse alveolar damage (DAD).
• ALI is a well-recognized complication of diverse conditions, including both direct injuries to the lungs and systemic disorders.
• In many cases, a combination of predisposing conditions is responsible (e.g., shock, oxygen therapy, and sepsis).
• Nonpulmonary organ dysfunction may also be present in severe cases.

• Pathogenesis:
ALI/ARDS is initiated by injury of pneumocytes and pulmonary endothelium, setting in motion a viscous cycle of increasing inflammation and pulmonary damage.
• Endothelial activation is an important early event:
- Directly---- circulating inflammatory mediators (e.g, sepsis)
- Secondary to pneumocyte injury----inflammatory mediators from resident inflammatory cells (alveolar macrophages--- TNF)
• Adhesion and extravasation of neutrophils. they degranulate and release inflammatory mediators, including proteases, reactive oxygen species, and cytokines. causing more endothelial injury, and local thrombosis.
• Accumulation of intraalveolar fluid and formation of hyaline membranes.
Endothelial activation and injury make pulmonary capillaries leaky, allowing interstitial and Intra-alveolar edema fluid to form.
Damage and necrosis of type II alveolar pneumocytes leads to surfactant abnormalities, further compromising alveolar gas exchange.
Ultimately, the inspissated protein-rich edema fluid and debris from dead alveolar epithelial cells organize into hyaline membranes, a characteristic feature of ALI/ARDS.
• Resolution of injury is impeded in ALI/ARDS due to epithelial necrosis and inflammatory damage that impairs the ability of remaining cells to assist with edema resorption.
• Eventually, however, if the inflammatory stimulus lessens, macrophages remove intraalveolar debris and release fibrogenic cytokines such as (TGF-β) and (PDGF) leading to fibrosis of alveolar walls .
• Bronchiolar stem cells proliferate to replace pneumocytes.
• Endothelial restoration occurs through proliferation of uninjured capillary endothelium.
• Clinical Course:
Individuals who develop ALI are usually hospitalized for one of the predisposing conditions listed earlier. Profound dyspnea and tachypnea herald ALI, followed by increasing cyanosis and hypoxemia, respiratory failure, and the appearance of diffuse bilateral infiltrates on radiographic examination.
• Hypoxemia may be refractory to oxygen therapy due to ventilation perfusion mismatching.
• The functional abnormalities in ALI are not evenly distributed throughout the lungs. The lungs have areas that are infiltrated, consolidated, or collapsed (and thus poorly aerated and poorly compliant) and regions that have nearly normal levels of compliance and ventilation. Poorly aerated regions continue to be perfused, producing ventilation perfusion mismatch and hypoxemia.
• There are no proven specific treatments; however, due to improvements in therapy for sepsis, mechanical ventilation, and supportive care, the mortality rate among the 200,000 ALI/ARDS cases seen yearly in the United States has decreased from 60% to about 40%,
• with the majority of deaths attributable to sepsis or multiorgan failure and, in some cases, direct lung injury.
• Most survivors recover pulmonary function but many have persistent impairment in physical and cognitive functions.
• In a minority of patients, the exudate and diffuse tissue destruction result in scarring, interstitial fibrosis, and chronic pulmonary disease.