Embed Size (px)
Citation preview

Huntington Disease
Huntington disease (HD) is an autosomal dominant,
progressive neurodegenerative disorder, typically
characterized by a movement disorder, affecting
middle-aged adults. It is the most frequent cause of
genetic chorea with reported prevalence rates in North
America and Europe ranging from 3 to 7 per 100,000
(Cardoso et al. 2006).
Synonyms and Related Disorders
Huntington chorea
Genetics/Basic Defects
1. Caused by a mutation in the IT15 gene, which
is a 210-kb gene located near the tip of the short
arm of chromosome 4 (4p16.3), resulting in the
N-terminal region of huntingtin protein (Htt) (The
Huntington’s Disease Collaborative Research
Group 1993; Cardoso 2009; Harris et al. 2009)
2. Patients with Huntington disease have an expanded
and unstable trinucleotide CAG (cytosine-adenine-
guanine) repeat in the IT15 gene within exon 1
(Rubinsztein et al. 1996). Huntington disease is,
therefore, considered one of the trinucleotide repeat
disorders.
a. Normal CAG repeat length in theHD gene: 35 or
lower
b. Expansions of 40 or more cause HD with com-
plete penetrance.
c. Individuals with 36–39 repeats may also
develop HD but penetrance is incomplete
(Rubinsztein et al. 1996).
d. A CAG repeat range between 27 and 35:
considered normal allele with particular risk for
expansion into the HD range in the paternal
germline (Ranen et al. 1995; Laccone et al. 1999)
e. The number of CAG repeats
i. Has significant implications for age at onset,
disease severity, and stability of the gene
between generations
ii. Presence of a robust inverse correlation
between the number of polyglutamine
repeats and the age at disease onset so that
longer repeat lengths are associated with
earlier onset of Huntington disease
(Shelbourne et al. 2007)
iii. The number of CAG repeats, however, is not
an absolute prediction of disease onset.
3. The nature of the genetic defect in the HD gene
(Myers et al. 1998) explains many of the genetic
features of the disorder, including:
a. The variability in age at onset
b. The tendency for juvenile disease to be inherited
from fathers
i. Merritt et al. (1969) first observed that
a disproportionate number of cases with
onset before the age of 21 had inherited the
HD gene from affected fathers.
ii. The observation of earlier ages at onset in
successive generations, termed “anticipa-
tion,” is seen in several of the trinucleotide
repeat disorders including HD.
iii. Meiotic instability of the HD repeat in pater-
nal transmission explains the observation of
anticipation in HD.
c. The sporadic appearance of new mutations
to HD
H. Chen, Atlas of Genetic Diagnosis and Counseling, DOI 10.1007/978-1-4614-1037-9_121,# Springer Science+Business Media, LLC 2012
1073

4. Pathophysiology (Roze et al. 2008)
a. The expanded polyglutamine repeat alters the
normal functions of Htt.
b. The mutated protein, Exp-Htt, is itself toxic.
c. Htt interacts with an array of proteins in neuronal
cells
d. One important characteristic of Huntington
disease is the particular vulnerability of
a particular brain region, the caudate–putamen,
despite similar expression of the mutated protein
in other brain areas.
Clinical Features
1. A triad of HD (Cardoso 2009; Harris et al. 2009)
a. Movement disorder (Leigh et al. 1983; Carella
et al. 1993; Jankovic and Ashizawa 1995; Reuter
et al. 2000; Tan et al. 2000)
i. Full spectrum of motor impairment
a) Eye movement abnormalities
b) Parkinsonian features
c) Dystonia (particularly in juvenile HD)
d) Myoclonus
e) Tics
f) Ataxia
g) Dysarthria
h) Dysphagia
i) Spasticity with hyperreflexia and
extensor plantar responses
ii. Chorea: often superseded by dystonia or
akineto-rigid parkinsonian features with
progressing illness
iii. Dystonia: found in more than 90% of
patients with HD in one study (Louis et al.
1999) although rarely it becomes as promi-
nent as in idiopathic dystonias
b. Cognitive decline
i. Universally go through cognitive decline,
mental slowing, impaired problem-solving
abilities, and other signs of a frontal
dysexecutive syndrome, and they eventually
become demented. These patients present
with the prototype of so-called subcortical
dementia (Lawrence et al. 1996; Kirkwood
et al. 2001; Ho et al. 2003).
ii. Cognitive decline also heralds the juvenile
onset of HD (Ribai et al. 2007).
iii. Asymptomatic carriers of the HD gene have
decreased phonemic fluency (Larsson et al.
2008).
c. Behavioral changes
i. Universal and may occasionally antedate
motor manifestations
ii. Major depression is common, diagnosed
in more than 40% of subjects, and res-
ponsible for increased suicide rates
in HD
iii. Broad spectrum of behavioral abnormalities
(Caine and Shoulson 1983; Mendez 1994;
Schoenfeld et al. 1984; Shiwach 1994;
Rosenblatt and Leroi 2000; Rosenblatt
et al. 2003; Guttman et al. 2003)
a) Anxiety or panic attacks
b) Obsessive compulsive symptoms
c) Manic features
d) Psychosis
e) Irritability and aggressive behavior
f) Sexual disinhibition
g) Apathy
h) In presymptomatic HD, significantly
more psychiatric symptoms (specially
depression, anxiety, and obsessive-com-
pulsiveness) were reported than for the
controls (Duffin et al. 2007)
i) Similarly, psychiatric difficulties are
indicators of juvenile HD onset (Ribai
et al. 2007).
2. End-stage HD
a. Relentlessly progressive course with death
occurring 15–20 years after symptom onset
with particularly rapid progression in the juve-
nile Westphal variant
b. Typically rigid and akinetic, demented, and
mute
c. Immobility and dysphagia often lead to aspira-
tion pneumonia, the most common cause of
death in these patients (Marshall 2004; Sorensen
and Fenger 1992; Lanska et al. 1988).
3. Differential diagnosis
a. Choreoacanthocytosis: the most likely disorder
to be confused
i. Dementia
ii. Involuntary movements
iii. Caudate atrophy
iv. Abnormal red blood cell morphology
1074 Huntington Disease

v. Neuropathy
vi. Seizures
vii. Myopathy
viii. Elevated creatine phosphokinase
ix. Self-mutilation
x. An unusual eating dystonia
b. Different causes of chorea
i. Genetic causes
a) Huntington disease
b) Huntington disease–like illnesses
c) Neuroacanthocytosis
d) McLeod syndrome
e) Wilson disease
f) Benign hereditary chorea
g) Spinocerebellar atrophy types 2, 3, 17
h) Dentatorubropallidoluysian
degeneration
i) Ataxia-telangiectasia
j) Ataxia associated with oculomotor
apraxia
k) Neuroferritinopathy
l) Pantothenate kinase associated
degeneration
m) Leigh disease and other mitochondrio-
pathies
n) Lesch–Nyhan disease
o) Creutzfeldt–Jakob disease
p) Neuronal ceroid lipofuscinosis
q) Glutaric aciduria
r) Polycythemia vera
s) Celiac disease
t) Benign familial chorea
ii. Immunologic causes
a) Sydenham chorea
b) Systemic lupus erythematosus
c) Antiphospholipid antibody syndrome
iii. Drug-induced chorea
a) Amantadine
b) CNS stimulants (amphetamines, methyl-
phenidate, cyproheptadine)
c) Anticholinergics
d) Anticonvulsants (carbamazepine,
phenytoin)
e) Carbon monoxide
f) Cocaine
g) Dopamine agonists
h) Dopamine-receptor blockers
i) Estrogens
j) Ethanol
k) Levodopa
l) Levofloxacin
m) Lithium
n) Sympathomimetics
o) Theophylline
p) Tricyclic antidepressants
q) Carbamazepine
r) Drugs that cause tardive dyskinesia
s) Withdrawal emergent syndrome
iv. Infections
a) AIDS-related (toxoplasmosis, progres-
sive multifocal leukoencephalopathy,
HIV encephalitis)
b) Bacteria (diphtheria, scarlet fever,
whooping cough)
c) Encephalities (B19 parvovirus, Japanese
encephalitis, measles, mumps, West
Nile river encephalitis, others)
d) Parasites (neurocysticercosis)
e) Protozoan (malaria, syphilis)
v. Endocrine-metabolic dysfunction
a) Adrenal insufficiency
b) Hyper/hypocalcemia
c) Hyper/hypoglycemia
d) Hypomagnesemia
e) Hypernatremia
f) Liver failure
vi. Vascular
a) Postpump chorea (cardiac surgery)
b) Stroke
c) Subdural hematoma
vii. Miscellaneous
a) Anoxic encephalopathy
b) Cerebral palsy
c) Kernicterus
d) Multiple sclerosis
e) Normal maturation (less than 12months
old)
f) Nutritional (e.g., B12 deficiency)
g) Posttraumatic (brain injury)
h) Chorea gravidarum hyperthyroidism
i) External pallidal atrophy
j) Pick disease
k) Paraneoplastic syndromes
l) Acute disseminated encephalo
myelopathy
m) Multiple system atrophy
Huntington Disease 1075

Diagnostic Investigations
1. A confirmed family history of Huntington disease
combined with clinical manifestations: sufficient
for diagnosis (Harris et al. 2009)
2. Neuroimaging (MRI and CT)
a. Severe atrophy of the caudate nucleus in moder-
ately disabled patients
b. May be relatively normal in patients in the early
stages
3. Pet scan: Atrophy of the caudate nucleus can be
detected in a presymptomatic state by the finding
of head of caudate hypometabolism
4. Neuropathological features
a. Neuronal loss and gliosis in the cortex and stria-
tum, particularly the caudate nucleus: the most
prominent neuropathologic features (Roth et al.
2005)
b. Neuronal injury occurs initially in the caudate
tail, in the medial paraventricular caudate, and in
the dorsal part of the putamen.
c. Further neuronal loss and an increase in astro-
cytes can be observed in widespread cortical and
subcortical regions as the neurodegenerative
process progresses.
d. Pathologic observation of affected striatum
shows loss of GABAergic spiny projection neu-
rons with preservation of the aspiny interneurons
and large aspiny acetylcholinesterase-positive
neurons.
e. A decrease of important neurotransmitters and
neuropeptides, such as g-aminobutyric acid
(GABA), calbindin, enkephalin, and substance
P, as a result of selective loss of the medium
spiny neurons
5. Three main types of genetic testing of HD
a. To confirm or rule out disease
b. Presymptomatic testing to determine the carrier
status of an individual at genetic risk for
inheriting the disease
i. To assist in making decisions about mar-
riage, procreation, or career
ii. The emotional impact of the result can be
difficult to anticipate and can evoke substan-
tial adverse emotional reactions (Taylor and
Myers 1997; Almqvist et al. 1999).
iii. Appropriate pretest counseling is important
to assist the at-risk individual in considering
the risks and benefits of genetic testing for
diseases such as HD for which available
treatment does not justify testing
c. Prenatal testing to determine the carrier status of
a fetus
Genetic Counseling
1. Recurrence risk (Warby et al. 2010)
a. Patient’s sib
i. A 50% risk if a parent is affected or has
a CAG size of 40 or greater.
ii. An estimated risk as high as 5% (50% �10%) of inheriting a mutant allele (�36
CAG repeats) if the father has an
intermediated allele (Chong et al. 1997)
iii. A sib who inherits anHD allele with reduced
penetrance may or may not develop symp-
toms of HD.
b. Patient’s offspring
i. A 50% risk of inheriting the disease-causing
mutation from a parent with heterozygosity
for the HD allele
ii. A 100% risk of inheriting the disease-causing
allele from a parent with homozygosity for
CAG repeat expansion in the HD gene
2. Prenatal diagnosis (Warby et al. 2010)
a. Prenatal diagnosis is possible for pregnancies at
50% risk by analyzing DNA extracted from fetal
cells obtained by amniocentesis or CVS, pro-
vided the disease-causing allele in the affected
parent or in an affected relative has been
confirmed.
b. Preimplantation genetic diagnosis may be avail-
able for families in which the disease-causing
mutations have been identified in an affected
family member.
3. Management (Harris et al. 2009)
a. No definitive cure
b. Limited therapeutic options currently
c. Multidisciplinary team approach
i. Medical
ii. Social work
iii. Physical therapy
d. Selective serotonin reuptake inhibitors: effective
in treating depression symptoms:
i. Depression
ii. Mania
1076 Huntington Disease

iii. Delusions
iv. Paranoia
v. Chorea
vi. Other symptoms related to depression
a) Rumination
b) Perseveration
c) Obsessive-compulsive disorder
d) Suicide
vii. Mood stabilizers (valproate, carbamaze-
pine, lamotrigine, or lithium) for bipolar
disorders
e. Neuroleptic for delusions and paranoia symp-
toms as well as chorea
f. Atypical antipsychotics (risperidone, clozapine,
olanzapine, and quetiapine): provide sufficient
control of psychotic symptoms with a lower risk
for extrapyramidal adverse effects and tardive
dyskinesia.
g. Nutritional management
h. Palliative care in managing the latter stage of the
disease
i. Bedridden
ii. Mute
iii. Rigid
iv. Dysphagia
v. Aspiration
References
Almqvist, E. W., Bloch, M., Brinkman, R., et al. (1999).
A worldwide assessment of the frequency of suicide, suicide
attempts, or psychiatric hospitalization after predictive test-
ing for Huntington disease. American Journal of HumanGenetics, 64, 1293–1304.
Caine, E. D., & Shoulson, I. (1983). Psychiatric syndromes in
Huntington’s disease. The American Journal of Psychiatry,140, 728–733.
Cardoso, F. (2009). Huntington disease and other choreas.
Neurologic Clinics, 27, 719–736.Cardoso, F., Seppi, K., Mair, K. J., et al. (2006). Seminar on
choreas. Lancet Neurology, 5, 589–602.Carella, F., Scaioli, V., Ciano, C., et al. (1993). Adult onset myo-
clonic Huntington’s disease.Movement Disorders, 8, 201–205.Chong, S. S., Almqvist, E., Telenius, H., et al. (1997). Contribu-
tion of DNA sequence and CAG size to mutation frequencies
of intermediate alleles for Huntington disease: Evidence
from single sperm analyses. Human Molecular Genetics, 6,301–309.
Duffin, K., Paulsen, J. S., Beglinger, L. J., et al. (2007). Psychi-
atric symptoms in Huntington’s disease before diagnosis:
The predict-HD study. Biological Psychiatry, 62,1341–1346.
Greenamyre, J. (2007). Timothy: Huntington’s disease – making
connections. The New England Journal of Medicine, 356,518–520.
Guttman, M., Alpay, M., Chouinard, S., et al. (2003). Clinical
management of psychosis and mood disorders in
Huntington’s disease. In M. A. Bedard, Y. Agid, S.
Chouinard, S. Fahn, A. D. Korczyn, & P. Lesperance
(Eds.), Mental and behavioral dysfunction in movementdisorders (pp. 409–426). Totowa, NJ: Humana Press.
Harris, M. K., Shneyder, N., Horazanci, A., et al. (2009). Move-
ment disorders. Medical Clinics of North America, 93,371–388.
Ho, A. K., Sahakian, B. J., Brown, R. G., et al. (2003). Profile of
cognitive progression in early Huntington’s disease. Neurol-ogy, 61, 1702–1706.
Jankovic, J., & Ashizawa, T. (1995). Tourettism associated
withHuntington’s disease.MovementDisorders, 10, 103–105.Kim, M., Lee, S.-T., Chu, K., et al. (2008). Stem cell-based cell
therapy for Huntington disease: A review. Neuropathology,28, 1–9.
Kirkwood, S. C., Su, J. L., Conneally, P., et al. (2001). Progres-
sion of symptoms in the early and middle stages of Hunting-
ton disease. Archives of Neurology, 58, 273–278.Laccone, F., Engel, U., Holinski-Feder, E., et al. (1999). DNA
analysis of Huntington’s disease: Five years of experience in
Germany, Austria, and Switzerland. Neurology, 53, 801–806.Lanska, D. J., Lanska, M. J., Lavine, L., et al. (1988). Conditions
associated with Huntington’s disease at death. A case-control
study. Archives of Neurology, 45, 878–880.Larsson, M. U., Almkvist, O., Luszcz, M. A., et al. (2008).
Phonemic fluency deficits in asymptomatic gene carriers for
Huntington’s disease. Neuropsychology, 22, 596–605.Lawrence, A. D., Sahakian, B. J., Hodges, J. R., et al. (1996).
Executive and mnemonic functions in early Huntington’s
disease. Brain, 119(Pt 5), 1633–1645.Leigh, R. J., Newman, S. A., Folstein, S. E., et al. (1983).
Abnormal ocular motor control in Huntington’s disease.
Neurology, 33, 1268–1275.Louis, E. D., Lee, P., Quinn, L., et al. (1999). Dystonia in
Huntington’s disease: Prevalence and clinical characteristics.
Movement Disorders, 14, 95–101.Marshall, F. (2004). Clinical features and treatment of
Huntington’s disease. In R. L. Watts & W. C. Koller (Eds.),
Movement disorders: Neurological principles and practice(pp. 589–601). New York: McGraw-Hill.
Mendez, M. F. (1994). Huntington’s disease: Update and review
of neuropsychiatric aspects. International Journal of Psychi-atry in Medicine, 24, 189–208.
Merritt, A. D., Conneally, P. M., Rahman, N. F., et al. (1969).
Juvenile Huntington’s chorea. In A. Barbeau & T. R.
Brunette (Eds.), Progress in neurogenetics (pp. 645–650).
Amsterdam: Excerpta Medica Foundation.
Mestre, T., Ferreira, J., Coelho, M. M., et al. (2009). Therapeutic
interventions for disease progression in Huntington’s disease
(Review). Cochrane Database of Systematic Reviews, (3),CD006455. The Cochrane Collaboration, Published by John
Wiley & Sons.
Myers, R. H. (2004). Huntington’s disease genetics. NeuroRx, 1,255–262.
Myers, R. H., Marans, K., & MacDonald, M. E. (1998).
Huntington’s disease. In S. T. Warren & R. T. Wells (Eds.),
Huntington Disease 1077

Genetic instabilities and hereditary neurological diseases(pp. 301–323). New York: Academic.
Ranen, N. G., Stine, O. C., Abbott, M. H., et al. (1995). Antic-
ipation and instability of IT-15 (CAG)n repeats in parent-
offspring pairs with Huntington disease. American Journal ofHuman Genetics, 57, 593–602.
Reuter, I., Hu, M. T., Andrews, T. C., et al. (2000). Late onset
levodopa responsive Huntington’s disease with minimal cho-
rea masquerading as Parkinson plus syndrome. Journal ofNeurology, Neurosurgery, and Psychiatry, 68, 238–241.
Ribai, P., Nguyen, K., Hahn-Barma, V., et al. (2007). Psychiatric
and cognitive difficulties as indicators of juvenile Huntington
disease onset in 29 patients. Archives of Neurology, 64,813–819.
Rosenblatt, A., Anderson, K., Goumeniouk, A. D., et al. (2003).
Clinical management of aggression and frontal syndromes in
Huntington’s disease. In M. A. Bedard, Y. Agid, S.
Chouinard, S. Fahn, A. D. Korczyn, & P. Lesperance
(Eds.), Mental and behavioral dysfunction in movement dis-orders (pp. 427–441). Totowa, NJ: Humana Press.
Rosenblatt, A., & Leroi, I. (2000). Neuropsychiatry of
Huntington’s disease and other basal ganglia disorders. Psy-chosomatics, 41, 24–30.
Ross, P. A. (2010). Huntington’s disease: A clinical review.
Orphanet Journal of Rare Diseases, 5, 40.Roth, J., Klempis, J., Jech,R., et al. (2005). Caudate nucleus atrophy
in Huntington’s disease and its relationship with clinical and
genetic parameters. Functional Neurology, 20, 127–130.Roze, E., Saudou, F., & Caboche, J. (2008). Pathophysiology of
Huntington’s disease: From huntingtin functions to potential
treatments. Current Opinion in Neurology, 21, 497–503.
Rubinsztein, D. C., Leggo, J., Coles, R., et al. (1996). Phenotypic
characterization of individuals with 30–40 CAG repeats
in the Huntington disease (HD) gene reveals HD cases with
36 repeats and apparently normal elderly individuals with
36–39 repeats. American Journal of Human Genetics, 59,16–22.
Schoenfeld, M., Myers, R. H., Cupples, L. A., et al. (1984).
Increased rate of suicide among patients with Huntington’s
disease. Journal of Neurology, Neurosurgery, and Psychia-try, 47, 1283–1287.
Shelbourne, P. F., Keller-McGandy, C., Bi, L. W., et al. (2007).
Triplet repeat mutation length gains correlate with cell-type
specific vulnerability in Huntington disease brain. HumanMolecular Genetics, 16, 1133–1142.
Shiwach, R. (1994). Psychopathology in Huntington’s disease
patients. Acta Psychiatrica Scandinavica, 90, 241–246.Sorensen, S. A., & Fenger, K. (1992). Causes of death in patients
with Huntington’s disease and in unaffected first degree
relatives. Journal of Medical Genetics, 29, 911–914.Tan, E. K., Jankovic, J., & Ondo, W. (2000). Bruxism in
Huntington’s disease. Movement Disorders, 15, 171–173.Taylor, C. A., & Myers, R. H. (1997). Long-term psychological
impact of Huntington’s disease linkage testing. AmericanJournal of Medical Genetics, 70, 365–370.
The Huntington’s Disease Collaborative Research Group.
(1993). A novel gene containing a trinucleotide repeat that
is expanded and unstable on Huntington’s disease chromo-
somes. Cell, 72, 971–983.Warby, S. C., Graham, R. K., & Hayden, M. R. (2007). Hunting-
ton disease. GeneReviews. Retrieved April 22, 2010.
Available at: http://www.ncbi.nlm.nih.gov/books/NBK1305/
1078 Huntington Disease

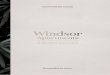
Fig. 1 The patient, a 42-year-
old lady, was evaluated for
increasing weakness of her
legs over the past 1 year,
dropping things out of her
hands and increased balance
difficulties. She was
ambulatory but had difficulty
going upstairs and on uneven
surfaces. She later developed
typical movement disorders,
chorea, dystonia, cognitive
decline, and behavioral
changes. The family history
was significant for affected
family members (mother and
two brothers). The diagnosis
of Huntington disease was
confirmed by the presence of
over 40 CAG repeats
Huntington Disease 1079