Embed Size (px)
Citation preview

Mowat–Wilson Syndrome
In 1998, Mowat et al. described a new syndrome, now
known as Mowat–Wilson syndrome (MWS),
consisting of Hirschsprung disease or severe constipa-
tion, microcephaly, mental retardation, and character-
istic facial features, including hypertelorism, medially
flared and broad eyebrows, prominent columella,
pointed chin, and uplifted earlobes.
The prevalence of MWS is currently unknown.
However, it seems probable that the syndrome is
underdiagnosed, particularly in patients without
Hirschsprung disease. Approximately 171 patients
with ZEB2 mutations, deletions or cytogenetic abnor-
malities have been reported and over 100 mutations
have been described.
Synonyms and Related Disorders
Hirschsprung disease-mental retardation syndrome;
Microcephaly, mental retardation, and distinct facial
features with or without Hirschsprung disease
Genetics/Basic Defects
1. Caused by heterozygous mutations and deletions
in the gene ZEB2 on chromosome 2 (also known
as ZFHX1B or SIP-1) in approximately 81% of
cases
2. Typically resulting from a de novo dominant
mutation
3. Cytogenetic deletions or translocations of the chro-
mosome 2q21-q23 region were found in several
patients
Clinical Features
1. Typical facial features
a. Seen in all individuals with this combination of
characteristics were found to have mutations or
deletions in the ZEB2 gene (Zweier et al. 2005)
i. Ocular hypertelorism
ii. Medially flared and broad eyebrows
iii. Prominent columella
iv. Prominent or pointed chin
v. Open-mouthed expression
vi. Uplifted earlobes with a central depression
a) Earlobes described as resembling
“orechietta pasta” or “red blood
corpuscles.”
b) Ear configuration not changing signifi-
cantly with age with the exception of
the central depression, which is less
obvious in adults.
b. Additional suggestive facial features (Mowat
et al. 2003; Adam et al. 2006)
i. Telecanthus
ii. Deep-set eyes
iii. Broad nasal bridge with prominent and
rounded nasal tip
iv. Full or everted lower lip
v. Posteriorly rotated ears
c. Natural history of facial phenotype (Wilson et al.
2003; Horn et al. 2004)
i. More pronounced facial phenotype with
age, making diagnosis easier in older
individuals
ii. Lengthening of the nasal tip and becoming
more depressed
H. Chen, Atlas of Genetic Diagnosis and Counseling, DOI 10.1007/978-1-4614-1037-9_160,# Springer Science+Business Media, LLC 2012
1391

iii. More pronounced columella, leading to
appearance of a short philtrum
iv. Elongation of the face
v. More prominent jaw
vi. Eyebrows becoming heavier with an
increased medial flare
2. Spectrum of structural anomalies
a. Gastrointestinal anomalies
i. Hirschsprung disease
a) A strong cross-reference marker when
present
b) Not a constant finding
c) Present in approximately 57–63% of
cases
ii. Pyloric stenosis
b. Genitourinary anomalies, particularly hypospa-
dias in males
c. Congenital heart defects, including abnormali-
ties of the pulmonary arteries and/or valves
d. Agenesis or hypogenesis of the corpus callosum
e. Ophthalmologic anomalies, including
microphthalmia and Axenfeld anomaly
f. Teeth anomalies
i. Widely spaced teeth
ii. Dental crowding
iii. “Malpositioned” teeth
iv. Delayed tooth eruption
3. Other features
a. Mental retardation, typically in the moderate
to severe range, with severe speech impairment
but relative preservation of receptive language
b. Seizures
c. Growth retardation (short stature) with
microcephaly
d. Chronic constipation in those without
Hirschsprung disease
Diagnostic Investigations
1. Cytogenetic testing
a. Chromosomal rearrangements that disrupt the
ZEB2 gene cause MWS in approximately 2% of
cases
b. FISH analysis. Large deletions encompassing all
or part of the ZEB2 gene detectable by FISH in
approximately 15% of cases
2. Molecular genetic testing
a. ZEB2 mutation detection rate by sequencing/
FISH/QPCR for individuals with the “typical
MWS” facial phenotype approaches 100%
b. No evidence of locus heterogeneity for MWS
3. Hirschsprung disease evaluation
4. MRI imaging of the brain for CNS anomalies
5. Echocardiograph for congenital heart disease
6. Ophthalmologic evaluation for eye anomalies
7. Renal ultrasound for renal anomalies
8. EEG for seizures
Genetic Counseling
1. Recurrence risk
a. Patient’s sib
i. De novo mutation: low recurrence risk
ii. Possibility of constitutional and/or germline
mosaicism: low recurrence risk but greater
than that of the general population (1–2%)
a) Possibility of germline mosaicism
suggested in two families with two and
three affected sibs, respectively
b) Low-level paternal mosaicism observed
in a family with two affected sibs has
been reported
b. Patient’s offspring: individuals with MWS and
an unbalanced chromosome rearrangement
unlikely to reproduce
2. Prenatal diagnosis
a. Prenatal diagnosis of a pregnancy at theoretically
increased risk because of constitutional and/or
germline mosaicism in a clinically unaffected
parent.
i. Disease-causing allele of an affected family
member being identified prior to prenatal
diagnosis
ii. Molecular genetic analysis on DNA extracted
from fetal cells obtained by amniocentesis or
chorionic villus sampling
b. Prenatal diagnosis of a pregnancy at increased
risk because of parental balanced structural
rearrangement: possible by chromosome analy-
sis of fetal cells obtained by amniocentesis or
chorionic villus sampling.
c. Preimplantation genetic diagnosis: available for
families at increased risk because of parental
1392 Mowat–Wilson Syndrome

mosaicism in which the disease-causing muta-
tions have been identified.
3. Management
a. Mostly supportive including seizure control and
developmental intervention
b. Specific management for structural anomalies,
including Hirschsprung disease
References
Adam, M. P., Bean, L. J. H., & Miller, V. R. (2008).
Mowat–Wilson syndrome. GeneReviews. Updated February
11, 2008. Available at: http://www.ncbi.nlm.nih.gov/books/
NBK1412/.
Adam, M. P., Schelley, S., Gallagher, R., et al. (2006). Clinical
features and management issues in Mowat-Wilson syn-
drome. American Journal of Medical Genetics. Part A, 140,2730–2741.
Amiel, J., Espinosa-Parrilla, Y., Steffann, J., et al. (2001). Large-
scale deletions and SMADIP1 truncating mutations in
syndromic Hirschsprung disease with involvement of mid-
line structures. American Journal of Human Genetics, 69,1370–1377.
Cacheux, V., Dastot-Le Moal, F., K€a€ari€ainen, H., et al. (2001).Loss-of-function mutations in SIP1 Smad interacting protein
1 result in a syndromic Hirschsprung disease. Human Molec-ular Genetics, 10, 1503–1510.
Cerruti Mainardi, P., Pastore, G., Zweier, C., et al. (2004).
Mowat-Wilson syndrome and mutation in the zinc finger
homeo box 1B gene: A well-defined clinical entity. Journalof Medical Genetics, 41, e16.
Dastot-Le Moal, F., Wilson, M., Mowat, D., et al. (2007).
ZFHX1B mutations in patients with Mowat-Wilson syn-
drome. Human Mutation, 28, 313–321.Garavelli, L. (2007). Cerruti Mainardi PC: Mowat-Wilson syn-
drome. Orphanet Journal of Rare Diseases, 2, 42.Garavelli, L., Donadio, A., Zanacca, C., et al. (2003).
Hirschsprung disease, mental retardation, characteristic
facial features, and mutation in the gene ZFHX1B (SIP1):
Confirmation of the Mowat-Wilson syndrome. AmericanJournal of Medical Genetics. Part A, 116, 385–388.
Horn, D., Weschke, B., Zweier, C., & Rauch, A. (2004). Facial
phenotype allows diagnosis of Mowat-Wilson syndrome in
the absence of Hirschsprung disease. American Journal ofMedical Genetics. Part A, 124, 102–104.
Ishihara, N., Yamada, K., Yamada, Y., et al. (2004). Clinical and
molecular analysis of Mowat-Wilson syndrome associated
with ZFHX1B mutations and deletions at 2q22-q24.1.
Journal of Medical Genetics, 41, 387–393.Kaariainen, H., Wallgren-Pettersson, C., Clarke, A., et al.
(2001). Hirschsprung disease, mental retardation and
dysmorphic facial features in five unrelated children. Clini-cal Dysmorphology, 10, 157–163.
Lurie, I. W., Supovitz, K. R., Rosenblum-Vos, L. S., et al.
(1994). Phenotypic variability of del(2) (q22-q23): Report
of a case with a review of the literature. Genetic Counseling,5, 11–14.
McGaughran, J., Sinnott, S., Dastot-Le Moal, F., et al. (2005).
Recurrence of Mowat-Wilson syndrome in siblings with the
same proven mutation. American Journal of MedicalGenetics. Part A, 137, 302–304.
Mowat, D. R., Croaker, G. D., Cass, D. T., et al. (1998).
Hirschsprung disease, microcephaly, mental retardation,
and characteristic facial features: Delineation of a new syn-
drome and identification of a locus at chromosome 2q22-q23.
Journal of Medical Genetics, 35, 617–623.Mowat, D. R., Wilson, M. J., & Goossens, M. (2003). Mowat-
Wilson syndrome. Journal of Medical Genetics, 40,305–310.
Nagaya, M., Kato, J., Niimi, N., et al. (2002). Clinical features
of a form of Hirschsprung’s disease caused by a novel
genetic abnormality. Journal of Pediatric Surgery, 37,1117–1122.
Wakamatsu, N., Yamada, Y., Yamada, K., et al. (2001). Muta-
tions in SIP1, encoding Smad interacting protein-1, cause
a form of Hirschsprung disease. Nature Genetics, 27,369–370.
Wilson, M., Mowat, D., Dastot-Le Moal, F., et al. (2003). Fur-
ther delineation of the phenotype associated with heterozy-
gous mutations in ZFHX1B. American Journal of MedicalGenetics. Part A, 119, 257–265.
Yamada, K., Yamada, Y., Nomura, N., et al. (2001). Nonsense
and frameshift mutations in ZFHX1B, encoding Smad-
interacting protein 1, cause a complex developmental disor-
der with a great variety of clinical features. American Journalof Human Genetics, 69, 1178–1185.
Yoneda, M., Fujita, T., Yamada, Y., et al. (2002). Late infantile
Hirschsprung disease-mental retardation syndrome with
a 3-bp deletion in ZFHX1B. Neurology, 59, 1637–1640.Zweier, C., Albrecht, B., Mitulla, B., et al. (2002). “Mowat-
Wilson” syndrome with and without Hirschsprung disease
is a distinct, recognizable multiple congenital anomalies-
mental retardation syndrome caused by mutations in the
zinc finger homeo box 1B gene. American Journal of Med-ical Genetics, 108, 177–181.
Zweier, C., Horn, D., Kraus, C., et al. (2006). Atypical ZFHX1B
mutation associated with a mild Mowat-Wilson syndrome
phenotype. American Journal of Medical Genetics. Part A,140, 869–872.
Zweier, C., Temple, I. K., Beemer, F., et al. (2003). Character-
isation of deletions of the ZFHX1B region and genotype-
phenotype analysis in Mowat-Wilson syndrome. Journal ofMedical Genetics, 40, 601–605.
Zweier, C., Thiel, C. T., Dufke, A., et al. (2005). Clinical and
mutational spectrum of Mowat-Wilson syndrome. EuropeanJournal of Medical Genetics, 48, 97–111.
Mowat–Wilson Syndrome 1393

a b
cd
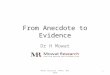
Fig. 1 (a–d) A three-and-a-half-year-old boy was noted to have
Mowat–Wilson syndrome. Note the unusual facies
(hypertelorism, telecanthus, strabismus, wide prominent nasal
bridge, an unusual nose with a rounded tip and prominent colu-
mella, a prominent chin, and unusual ears with fleshy uplifted ear
lobes), long tapering fingers, and an unusual stereotypic use of
his hands in which he moves his fingers in front of his face and
regards them. He is severely developmentally delayed and has
hypotonia. Chromosome microarray analysis revealed a loss in
copy number in the long arm of chromosome 2, detected with
two clones, spanning at least 100 kb (including the ZFHX1B
gene), and confirmed by FISH analysis. Deletions in this region
have been associated with Mowat–Wilson syndrome
1394 Mowat–Wilson Syndrome