Embed Size (px)
Citation preview
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2017
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1353
Attention Deficit/HyperactivityDisorder in Adults
Prevalence, Psychiatric Comorbidities and Long-termOutcome
DAN EDVINSSON
ISSN 1651-6206ISBN 978-91-513-0029-0urn:nbn:se:uu:diva-327892

Dissertation presented at Uppsala University to be publicly examined in Gunnesalen, Ing10, Akademiska sjukhuset, Uppsala, Saturday, 30 September 2017 at 09:15 for the degree ofDoctor of Philosophy (Faculty of Medicine). The examination will be conducted in Swedish.Faculty examiner: Professor Bo Söderpalm (Sahlgrenska Akademin, Sektionen för psykiatrioch neurokemi vid Institutionen för neurovetenskap och fysiologi).
AbstractEdvinsson, D. 2017. Attention Deficit/Hyperactivity Disorder in Adults. Prevalence,Psychiatric Comorbidities and Long-term Outcome. Digital Comprehensive Summaries ofUppsala Dissertations from the Faculty of Medicine 1353. 67 pp. Uppsala: Acta UniversitatisUpsaliensis. ISBN 978-91-513-0029-0.
Attention Deficit/Hyperactivity Disorder (ADHD) was originally thought to occur only inchildren, but is increasingly recognised as causing functional impairment also in adulthood. Theoverall aim of this thesis was to achieve a comprehensive understanding of ADHD in adulthood.
A questionnaire based on the DSM-IV criteria of ADHD, reported childhood symptoms,reading and spelling problems, difficulties and suffering and general assessment of functioning(GAF) was distributed to three samples: the general population (GP), outpatient psychiatry(OPP) and female prison inmates. Symptoms consistent with ADHD were more than three timeshigher in the OPP sample than in the GP sample (6.6 versus 2.1%). ADHD symptoms and relatedproblems occurred in 50% of the prison inmates.
A cohort of 168 patients diagnosed with ADHD in adulthood was interviewed about currentADHD symptoms and psychiatric comorbidity on axis I and II. The lifetime prevalence ofpsychiatric comorbidity on axis I was 92% and current comorbidity, including autism spectrumdisorders and Tourette’s syndrome, was 47%. The sex-specific pattern of the comorbid disor-ders was similar to that in the general population. Forty-six per cent of the patients endorsed thespecific criteria for at least one personality disorder.
After a mean follow-up of six years, there was remission of adult ADHD in about 30% of thepatients, regardless of whether there was ongoing medication or not. There were no differencesin function and quality of life, except for global general improvement, which was better inpatients currently on medication.
The most prevalent long-term side effects of pharmacological treatment with mainlystimulants were decreased appetite, dry mouth, anxiousness/restlessness and an increase in pulsefrequency. The discontinuation rate was about 50%: 29% discontinued because of a perceivedlack of effect, followed by elevated mood or hypomania (11%). No detectable evidence oftolerance and increased need for dosage over time was observed.
To conclude, Symptoms of ADHD is highly overrepresented in OPP and in female inmatescompared with the GP. Furthermore, adults diagnosed with ADHD have a high lifetimeprevalence of psychiatric comorbidity. Long-term pharmacological treatment with stimulants issafe with relatively mild and tolerable adverse effects. Continued medication, however, is notrelated to remission.
Keywords: ADHD, adults, prevalence, inmates, psychiatric comorbidity, long-term outcome,side effects, adverse events, stimulants, atomoxetine.
Dan Edvinsson, Department of Neuroscience, Psychiatry, University Hospital, Akademiskasjukhuset, Uppsala University, SE-751 85 Uppsala, Sweden.
© Dan Edvinsson 2017
ISSN 1651-6206ISBN 978-91-513-0029-0urn:nbn:se:uu:diva-327892 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-327892)

With gratefulness and admiration, I dedicate this thesis to the persons who generously shared their life ex-periences and participated in these studies.

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Edvinsson D, Bingefors K, Lindström E, Lewander T. (2010)
ADHD-related symptoms among adults in out-patient psychia-try and female prison inmates as compared with the general population. Ups J Med Sci, 115(1):30-40
II Edvinsson D, Lindström E, Lewander T, Bingefors K, Ekselius L. (2013) Gender differences of axis I and II comorbidity in subjects diagnosed with ADHD as adults. Acta Neuropsychiatr, 25(3):165-174.
III Edvinsson D, Ekselius L. (2017) Six-Year Outcome in Subjects Diagnosed with Attention-Deficit/Hyperactivity Disorder as Adults. Submitted for publication.
IV Edvinsson D, Ekselius L. (2017) Long-Term Tolerability and Safety of Pharmacological Treatment of Adult Attention-Deficit/Hyperactivity Disorder. Submitted for publication.
Reprints were made with permission from the respective publishers.
Papers I and II in this thesis, and a discussion on them, were the basis for a licentiate degree in medicine at Uppsala University, defended on October 11, 2012.

Abbreviations
AD/HD Attention Deficit/Hyperactivity Disorder ADD Attention Deficit Disorder ASD Autism Spectrum Disorder ASPD Antisocial Personality Disorder ASRS Adult ADHD Self-Report Scale AUDIT Alcohol Use Disorders Identification Test BPD Borderline Personality Disorder CAADID Conners’ Adult ADHD Diagnostic Interview for DSM-IV CBT Cognitive Behavioural Therapy CD Conduct Disorder CGI-I Clinical Global Impression - Improvement DAMP Deficits in Attention, Motor Control and Perception DIP-I ICD-10 Personality Interview DIVA Diagnostisk Intervju för ADHD hos vuxna DSM Diagnostic Statistical Manual of Mental Disorders DUDIT Drug Use Disorders Identification Test ED Emotional Dysregulation ESSENCE Early Symptomatic Syndromes Eliciting Neurodevelop-
mental Clinical Examination EQ-VAS EuroQol-Visual Analogue Scales EQ-5D EuroQol-5 Dimension Questionnaire GAF Global Assessment of Functioning HKD Hyperkinetic Disorder HRQoL Health-related quality of life ICD International Statistical Classification of Diseases and Re-
lated Health Problems LD Learning disability MTA-study The multimodal treatment study of children with ADHD ODD Oppositional defiant disorder PTSD Posttraumatic stress disorder RCT Randomized controlled trial SCID-I The Structured Clinical Interview for DSM-IV axis I SCID-II The Structured Clinical Interview for DSM-IV axis II SDS Sheehan Disability Scale SUD Substance use disorder

Contents
Introduction ................................................................................................... 11
Background ................................................................................................... 12Historical perspectives on ADHD ............................................................ 12Current diagnostic criteria of ADHD ....................................................... 14Prevalence and impairment of ADHD ..................................................... 14Aetiology .................................................................................................. 15Coexisting disorders and ADHD .............................................................. 16ADHD in prison inmates .......................................................................... 17Diagnostic assessment of ADHD in adulthood ........................................ 18Multimodal treatment of ADHD .............................................................. 19Pharmacological treatment of ADHD ...................................................... 20Outcome predictors .................................................................................. 21
Aims and scope ............................................................................................. 22
Method .......................................................................................................... 23Study design and participants ................................................................... 23Procedures and measurements ................................................................. 25Statistics ................................................................................................... 28Ethics ........................................................................................................ 28
Results ........................................................................................................... 29ADHD-related symptoms (Paper I) .......................................................... 29Sex differences (Paper II) ......................................................................... 31Six-Year Outcome (Paper III) .................................................................. 33Long-Term Tolerability and Safety (Paper IV) ........................................ 37
Discussion ..................................................................................................... 41Methodological considerations ................................................................ 41General discussion and clinical implications ........................................... 45Future aspects ........................................................................................... 51
Conclusions ................................................................................................... 52
Acknowledgements ....................................................................................... 53
References ..................................................................................................... 55


11
Introduction
At the turn of the century, the knowledge of adult ADHD within psychiatry was almost non-existent, and sometimes even the existence of ADHD in adulthood was outright put in question. To optimize resources to obtain, assess and optimally use the new knowledge on ADHD in adulthood, and to develop and implement procedures for accurate evaluation and treatment, a specialized neuropsychiatric team was established within the Department of Psychiatry at Uppsala University Hospital. The first part of this thesis is the result of attempts to obtain relevant knowledge in order to ensure optimal clinical practice. Therefore, the two first papers in this thesis investigate the prevalence of adult ADHD in various settings and psychiatric comorbidity in adults previously not diagnosed with ADHD.
Effectiveness and safety of pharmacological treatment as well as predic-tors of favourable outcome are important issues to consider when planning for scientifically based treatment programs. In an increasing number of sci-entific publications, pharmacological treatment has been demonstrated to be effective and safe in the short term. The long term outcome and safety of pharmacological treatment is, however, still less well investigated. The se-cond part of this thesis demonstrates the long-term outcome and safety of pharmacological treatment of a clinical sample of subjects diagnosed and treated for ADHD as adults.

12
Background
Historical perspectives on ADHD The earliest description of attention difficulties in the medical literature, with reference to the present concept of ADHD, is the publication by the German physician Melkior Adam Weikard. In 1775, possibly even a few years earli-er, he anonymously published the textbook Der Philosophische Artzt (Eng-lish: The Philosophical Physician) [15]. In this textbook Weikard describes the symptoms of inattention and distractibility – Attentio Volubilis, which overlap part of the current inattentive ADHD diagnostic criteria. Interesting-ly, his clinical examples included adults. Environmental factors such as up-bringing were identified as the cause of inattention but Weikard also dis-cussed the possibility of a neurological impact of these external causes. Fur-thermore, he considered inattention to be more common in childhood than in old people and that the symptoms described should be treated with a distrac-tion-free environment and physical exercise, among other measures [15].
In 1798, the Scottish physician Alexander Crichton published a chapter on inattention in his textbook An Inquiry into the Nature and Origin of Men-tal Derangement [41]. Crichton states that a patient suffering from “disease of inattention” is agitated by impressions and easily distracted, which causes mental restlessness and “fidgets”. He concludes that a person with the disor-der “may be either born with it or it may be the effect of accidental diseas-es”. He further recommended special educational interventions in that physi-cal punishment (“terrors of the rod”) seemed ineffective in these children.
Several descriptions of children with ADHD appeared later like the char-acter Struwwelpeter (English: Shockheaded Peter) in the illustrated book Lustige Geschichten und drollige Bilder (English: Funny stories and droll pictures) by the German physician Heinrich Hoffman [72]. Since its appear-ance in 1845, the character has constituted a prominent part of the literature for children in German-speaking countries. Both the inattentive and the hy-peractive/impulsive subtypes of ADHD can be clearly recalled from Hoff-man’s poetic examples.
Until recently, the British physician Sir George Frederick Still was con-sidered the first to present scientific descriptions of childhood ADHD. In a series of lectures delivered in 1902 and later published in the Lancet, Still describes a clinical panorama of children with a “defect of moral control” [135]. Many of these children were described as hyperactive and today
13
would probably be considered to suffer from comorbid oppositional defiant disorder (ODD). Of interest are Still’s observations of comorbid psychiatric disorders and criminality among adult relatives of these children [14; 135; 136].
In 1947, the book Psychopathology and Education of the Brain Injured Child was published by Alfred Strauss and Laura Lehtinen in which the con-cept “minimal brain damage” was introduced [137]. The concept was based on institutionalised children with distractibility, perseveration, hyperactivity and motor and learning problems for whom specific educational plans were later developed.
The concept of “minimal brain dysfunction” (MBD) appeared in an article by Clements and Peters in 1962 describing school-age children with specific learning, motor and coordination deficits together with “hyperkinesis”, im-pulsivity, emotional lability, distractibility, “equivocal” neurological signs and an EEG with a “6- and 14-per-second positive spiking pattern” [38]. DSM-II, published in 1968, included the entity “The hyperkinetic reaction of childhood”, mainly implying that symptoms were a reaction to the environ-ment and usually outgrown later in life with increased developmental ma-turity [5].
In 1980, this concept was succeeded by the diagnostic entity “attention deficit disorder” (ADD), which was introduced in DSM-III: diagnostics were clarified by dividing the diagnosis into inattentional problems with and without hyperactivity [6].
DSM-III-R, published in 1987, introduced the diagnosis “attention deficit hyperactivity disorder (ADHD)”, with a unidimensional approach listing a total of 14 symptoms with a diagnostic cut-off of ≥8 diagnostic criteria [7].
In 1982, Gillberg and Rasmussen separately introduced the concept “per-ceptual, motor and attentional deficits” (PMAD) based on a survey of Swe-dish seven-year-old children [60]. This concept was changed to “deficit in attention, motor control and perception” (DAMP) in 1987 [58]. The DAMP concept is used mostly in Scandinavia. In DSM-IV and DSM-5 it approxi-mately corresponds to ADHD in combination with “developmental coordi-nation disorder” (DCD) [58].
DSM-IV, published in 1994 [8], with a text revision, DSM-IV-TR in 2000 [9], lists nine symptomatic criteria of inattention and hyperactivi-ty/impulsivity The cut-off for a diagnosis is set at ≥6 items in each domain, resulting in the possibility of three subtypes: ADHD with predominantly inattention, ADHD with predominantly hyperactivity/impulsivity and the combined subtype (criterion A). The onset of symptoms causing impairment should be present before the age of seven years (criterion B). Impairment should be present in more than two settings (criterion C). There should be clear evidence of clinically significant impairment in social, academic or occupational functioning (criterion D). Symptoms that occur should not be accounted for solely by another mental disorder (criterion E). Because the
14
DSM-IV diagnostic criteria were originally adopted for children, questions were raised as to whether they are optimal for use in an adult population. This issue will be further addressed regarding the DSM-5 criteria (i.e. the current diagnostic criteria of ADHD).
Current diagnostic criteria of ADHD DSM-5, published in 2013, presented some minor but important changes in the diagnostic criteria of ADHD. The childhood symptom items of criterion A are now supplemented by examples of how childhood symptoms can be presented in adults. Furthermore, only ≥5 current items in each domain are required for older adolescents and adults aged ≥17. Criterion B was changed to childhood symptom presentation to before 12 years of age. Criteria C and D were left unchanged. For criterion E, pervasive developmental disorders (PDDs), such as previous autism spectrum disorder (ASD), were removed as exclusion criteria [10].
The 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) was published by The World Health Organisation (WHO) in 1992 and has been in clinical use in Sweden since 1997 [161]. The ICD-10 uses a narrower definition of ADHD, namely hy-perkinetic disorder (HKD). A diagnosis of HKD requires symptoms of hy-peractivity/impulsivity, and accordingly, ICD-10 does not recognise the pre-dominantly inattentive subtype of ADHD. Thus, in comparison with DSM-IV (and partly DSM-5), HKD roughly corresponds to the combined and pre-dominantly hyperactive/impulsive subtypes. The 11th Revision of the Inter-national Classification of Diseases (ICD-11) has been announced to be due out in 2018.
In addition, emotional dysregulation (ED) has been demonstrated to be linked to ADHD, although not formally included in the diagnostic criteria of DSM-5 and ICD-10. The "Wender Utah criteria" include ED as an important part of ADHD. ED has been demonstrated to respond to treatment with stimulants [118].
Prevalence and impairment of ADHD ADHD is widely recognised as one of the most common psychiatric disor-ders of school-age children, with a prevalence rate of 3-7%. Data indicate that boys tend to be diagnosed [88] and treated more often than girls [11]. In adulthood, research presents a much more differentiated picture, which has been suggested to be explained by referral bias in combination with differ-ences in assessment and methodology [154]. Although prospective studies indicate a frequent decline of ADHD symptoms with increasing age, signifi-

15
cant loss of functioning may remain despite sub-threshold diagnostic status [21; 50; 84]. Adult functioning after childhood ADHD varies but is generally worse with persistence of ADHD symptoms [70]. Thus, the functional im-pairment caused by ADHD in adulthood is increasingly acknowledged in a broad variety of domains. For example, motor vehicle accidents among adults with ADHD have been demonstrated to be substantially lower during periods of medication [34]. In summary, the prevalence of adult ADHD in the general population (GP) is estimated to be at least 2-4% [51; 83].
Aetiology The aetiology of ADHD is still largely unknown, but it is widely recognized that there is a substantial genetic component. Follow-up studies of monozy-gotic and dizygotic twins report that persistent genetic influences explain between 45 and 90% of the total genetic variance in hyperactivity-impulsivity and inattention from childhood to adolescence [90]. The genetic structure of ADHD has proven to be complex, although gene studies of ADHD have produced evidence of the involvement of several genes in the aetiology of the disorder. Meta-analyses are supportive of the involvement of genes coding for serotonergic and dopaminergic receptors, together with various proteins involved in dopamine transportation and membrane fusion [104].
Environmental factors have also been reported to be important in ADHD. An increased risk of ADHD has been demonstrated in children with prenatal exposure to smoking [43], low birthweight [75], preterm birth [37], and low Apgar scores [65]. Furthermore, nutritional factors [123], TV and computer games have been discussed regarding ADHD [52; 140]. Severe institutional deprivation has also been reported to be related to persistent symptomatolo-gy of ADHD [80].
On a group level, ADHD children, regardless of sex, have been shown to have smaller brain volume compared with controls [31]. The most frequently replicated neuroanatomic deviations have been identified in brain areas in-volved in executive functioning (e.g., the dorsolateral prefrontal cortex, cau-date nucleus, globus pallidus, corpus callosum and cerebellum) [126]. Neu-robiological deviations have been identified with functional magnetic reso-nance imaging in boys with ADHD compared with age-matched non-ADHD controls while performing visual go-stop tests. Relative underfunctioning of the dorsomedial and left inferior frontal cortex, posterior cingulate and parie-tal brain regions has been demonstrated in persons with ADHD, and has been shown to be normalised with the use of methylphenidate, a central stimulant used for ADHD treatment [122]. Finally, positron emission tomog-raphy has demonstrated a decreased function in the dopamine reward path-
16
way in the brain in never previously medicated adults with ADHD [158], and has been associated with motivation deficits in adult ADHD.
Coexisting disorders and ADHD Coexisting disorders in childhood ADHD To clarify the broad spectrum of disorders coexisting with ADHD in child-hood and symptom sharing across disorders, the concept and acronym ES-SENCE (early symptomatic syndromes eliciting neurodevelopmental clinical examination) has been devised to cover children with impairing symptoms in defined areas/domains before age 3 to 5 years [59]. Major problems in at least one ESSENCE domain before age 5 years often signals major problems in the same or overlapping domains years later. The ESSENCE perspective is that one should not view neuropsychiatric symptoms in early childhood as discrete disorders or syndromes, but from a perspective of early brain dys-functions that goes beyond syndromes. ESSENCE refers to deviance in syn-dromes included cover a wide spectrum comprising ASD and PPD, ADHD, ODD, specific language impairment, learning disability (LD), non-verbal LD, tic disorders, bipolar disorder, behavioural phenotype syndromes, epi-lepsy syndromes and reactive attachment disorders. This broad ESSENCE perspective is consistent with a report from the US on over 60 000 children aged 6 to 17 years, which concluded that 46% of children with ADHD had a LD, 27% a conduct disorder (CD), 18% an anxiety disorder, 14% depression and 12% speech problems. Thirty-three per cent of the ADHD children had at least one comorbid disorder, 16% two comorbid disorders and 18% three or more comorbid disorders. Comorbidity widely exceeded that of persons without ADHD [89].
Sex differences have been investigated in a study of 140 boys and 140 girls aged 6-17 years who were referred for and diagnosed with ADHD. Compared with boys, girls were more likely to have the predominantly inat-tentive subtype and less at risk for major depression, CD or ODD, whereas the risk of substance use disorder (SUD) was higher in girls with ADHD than in boys [22].
Coexisting disorders in adults with ADHD Several studies have investigated psychiatric comorbidity in adult ADHD. In a German study clinically referred adults with ADHD were reported to have a lifetime comorbidity on axis I of 77% compared with 46% in age- and sex-matched controls [130]. Affective and eating disorders, together with SUD, were more frequently associated with adult ADHD, with a sex bias for SUD, which was more prevalent in men. Slightly lower figures were reported in a
17
Canadian study with a current and lifetime axis I comorbidity of 47% in adults with ADHD versus 27% in age- and sex-matched controls. Coexist-ence of axis II comorbidity was reported to affect half of the individuals [42]. Studies of subtype differences in comorbidity patterns have found ex-ternalising disorders (e.g., ODD, CD, SUD) and antisocial personality disor-der (ASPD) to be more frequently associated with the combined subtype. In general, ADHD was more frequently associated with clusters B and C per-sonality disorders, regardless of subtype, when compared with a non-ADHD comparison group [101]. Another study reported the combined subtype to be associated with significantly higher rates of lifetime CD, bipolar disorders and psychosis compared with the inattentive and hyperactive/impulsive sub-types [153]. Reversely, previously unidentified ADHD has been found to be prevalent in samples of persons diagnosed with various psychiatric disorders such as SUD [146], bipolar disorder [125], posttraumatic stress disorder (PTSD) [93] and borderline personality disorder (BPD) [111]. Another im-portant clinical issue is the frequency of sleeping disorders in adult ADHD, which has been reported to be widely increased, especially in the combined and hyperactive/impulsive subtypes [27]. The aetiology is poorly understood but circadian rhythm disruption and an increased prevalence of restless legs syndrome have been proposed as possible explanations [40; 128; 129]. In accordance with the ESSENCE acronym, a high prevalence of learning disa-bilities [28; 99] and reading difficulties has been reported in children, ado-lescents, and adults with ADHD [45]. Studies have also indicated difficulties in written language expression in persons with ADHD [134].
ADHD in prison inmates Several studies have reported an increased prevalence of ADHD in incarcer-ated men, affecting about 4 of 10 inmates [62; 120]. Female inmates have been studied less frequently but a German study of 110 incarcerated females found a lifetime prevalence of ADHD of 24.5% with 10% for persisting diagnostic criteria according to DSM-IV. The subjects reported a decline in the prevalence of persisting ADHD with age, from 17.9% (age ≤25 years) to 10% (age 26–45 years), and with none persisting above the age of 45 [121]. The coexistence of reading difficulties in male prison inmates has been re-ported [116]. In a meta-analysis, the estimated general prevalence in incar-cerated patients was 25.5%, with no significant differences for sex and age, although with significant country differences [163]. Finally, pharmacological treatment of inmates with ADHD has been linked to positive long-term func-tional outcome [63].
18
Diagnostic assessment of ADHD in adulthood Several screening instruments and diagnostic interviews are available for adult ADHD. The World Health Organisation Adult ADHD Self-Report Scale (ASRS) contains 18 items, one for each of the DSM-IV criteria, which can be used for interviews, treatment evaluation, or both [82; 84; 145]. There is also an abbreviated 6-item short screening version of current symptoms based on selected DSM-IV criteria (50). This has been reported to have a total classification accuracy of 97.9 % when applied to population survey data (50) but is less specific when used in subsamples of diagnostic entities such as subjects with SUD (51). The Brown ADD Scale concentrates on the inattentive aspects of ADHD [124]. Conners’ Adult ADHD Rating Scale is based on the 18 DSM-IV criteria with symptomatic descriptions adapted for an adult population [2]. The Wender Utah Rating Scale [100]. is available for a retrospective screening of childhood ADHD, including additional symptoms often associated with ADHD (e.g., temper, affective lability and emotional overreactivity). Finally, the parent questionnaire "Five to Fifteen" is available for screening of symptoms and problems typical of ADHD and its comorbidities [77].
To secure diagnostic accuracy after positive screening, semi-structured in-terviews are available including the Conners’ Adult ADHD Diagnostic In-terview for DSM-IV (CAADID) [47] and the Diagnostic Interview for ADHD in adults (DIVA). CAADID is not available in an authorized Swe-dish version and the original version in English is subject to copyright issues. DIVA has been translated into several languages, including Swedish, and is available free of charge on the Internet. The Spanish version of DIVA has recently been validated against CAADID [48; 115].
Apart from past and present symptoms of ADHD, the influence of psy-chiatric comorbidity, somatic disease, ongoing substance use and signs of behavioural phenotype syndromes must be considered before a clinical diag-nosis of adult ADHD is established. Neuropsychological testing with evalua-tion of the cognitive level and profile often provides valuable information to facilitate the diagnostic procedure. Sometimes computerized continuous performance tests, e.g. QBtest [74], can be of value as part of the evaluation process.
The European Network Adult ADHD was founded in 2002 to advance the recognition and treatment of adult ADHD in Europe. An extensive review article and consensus statement on the diagnostics and treatment of adult ADHD was published by members of the network in 2010 and an updated version is expected to be presented shortly [87].
19
Multimodal treatment of ADHD A combination of pharmacological and non-pharmacological treatment, as well as psychosocial and pedagogic interventions are often considered the gold standard when treating subjects with ADHD. The multimodal treatment study of children with ADHD (MTA study) constitutes a cornerstone in the subsequent view on ADHD treatment [143]. The MTA group followed 597 children with the combined subtype over a period of 14 months. The chil-dren were randomised to one of four treatment strategies: 1) carefully titrated and monitored medication with stimulants, 2) intensive behavioural treat-ment, 3) a combination of strategies 1 and 2, and finally 4) standard commu-nity care (control group). The outcome demonstrated significantly greater ADHD symptom reduction in groups 1 and 3 compared with groups 2 and 4. There was no difference in symptom reduction when comparing groups 1 and 3, but combining carefully monitored treatment with stimulants with behavioural treatment reduced parallel symptoms (e.g., aggressive/-oppositional and internalising symptoms) known to be frequently associated with ADHD in childhood.
Treatment of adults with ADHD has been the subject of several guide-lines. The previously mentioned European Network has presented a treat-ment algorithm of psychoeducation, pharmacotherapy, coaching, cognitive behavioural therapy and family therapy. In this approach, the importance of considering treatment of coexisting psychiatric comorbidity is underlined [87]. The National Institute for Health and Care Excellence guidelines, pub-lished in 2008 and updated in 2016, advocate pharmacotherapy to be the first-line of treatment as a part of a comprehensive treatment programme addressing interventions and treatment of psychological, behavioural and educational or occupational needs [141]. Treatment recommendations of ADHD by the Swedish Medical Products Agency (Swedish: Läke-medelsverket) [98] underline pharmacological treatment as a component of a multimodal approach including psycho-social and pedagogic interventions.
The effect of non-pharmacological treatment has been investigated in pa-tients receiving treatment with stimulants or placebo undergoing either be-havioural group psychotherapy or individual clinical management. After three months of treatment, there was no difference in symptom reduction in those treated with group psychotherapy or individual clinical management. However, significantly decreased symptoms were found in patients treated with stimulants compared with those treated with placebo. These results were stable at a one-year follow-up [110].
20
Pharmacological treatment of ADHD Mechanisms of action of stimulants and atomoxetine Stimulants are thought to work primarily in dopamine and norepinephrine pathways, especially in striatal areas of the brain by blocking the reuptake of these neurotransmitters [155; 156; 157; 159].
The exact functional mechanism of atomoxetine remains unresolved but is thought to be a selective inhibitor of the norepinephrine transporter in-creasing norepinephrine causing α2-adrenergic receptor activation [56; 138]. In addition, atomoxetine appears to increase dopamine in the prefrontal cor-tex through nonspecific action of the norepinephrine transporter [12].
Effectiveness and safety of pharmacological treatment of ADHD in adulthood Only a handful of randomised controlled trials (RCTs) of stimulants and atomoxetine have been conducted for ≥24 weeks in adults with ADHD [76; 61; 1; 23; 121; 162]. Moreover, some short-term trials of stimulants have been supplemented with open-label extensions confirming a similar pattern of relatively mild side effects [3; 29; 64; 149; 150]. The most frequent side effects reported for methylphenidate were headache, decreased appetite, dry mouth/mucosal dryness, nasopharyngitis and difficulty falling asleep; atomoxetine was linked to nausea, dry mouth, decreased appetite, headache and fatigue.
Despite evidence of beneficial effect and treatment safety, the clinical rel-evance of these short-term RCTs and/or open-label studies could be ques-tioned since psychiatric comorbidity often excludes RCT participation. A few prospective and/or naturalistic studies have been published up to date. In a one-year study 30 % of participants experienced any side effect on methylphenidate and 12 % terminated treatment on any ADHD drug due to side effects [55]. Another study that included patients with a high degree of psychiatric comorbidity found that half of the patients remained on treatment with stimulants after two years. Only 15% discontinued treatment because of lack of effect and 17% did so because of anxiety or depression. The most frequently reported side effects during treatment were decreased appetite, dry mouth and initial insomnia [17]. Finally, a four-year outcome question-naire study of pharmacologically treated adults with ADHD reported a 37% discontinuation rate at follow-up. Side effects were the most frequent reason for cessation of medication, followed by lack of efficacy and misuse [95].
Because ADHD medication has been associated with a moderate mean increase in blood pressure and pulse, questions on the long-term risks of cardiovascular adverse events have been rightfully raised [68].

21
Outcome predictors Outcome predictors in childhood A six-year follow-up study of a European cohort of children diagnosed with ADHD at a mean age of 11 years reported a correlation between younger baseline age, higher ADHD symptom severity and higher impairment at baseline and poorer overall functioning. Interestingly, pharmacological treatment demonstrated no impact on either ADHD symptom severity or overall functioning at follow-up [148]. Furthermore, a meta-analysis of stud-ies on children identified ADHD severity, treatment for ADHD, comorbid CD and comorbid major depressive disorder to be predictors in childhood for ADHD persistence in adulthood [32]. In a longitudinal study of twins, adult persistence was associated with more symptoms and lower IQ [4].
Outcome predictors in adulthood
With an increasing number of adults seeking evaluation and treatment of ADHD, predictors at baseline for future outcome are clinically important to identify and consider in clinical practice.
Patients diagnosed with ADHD in adulthood reported better outcome on all measures when pharmacologically treated for two years or more com-pared with those with a shorter treatment time after a mean observation peri-od of 4.5 years and at a mean age of 36.5 years at follow-up. In this study, comorbidity at baseline predicted poorer outcome [95]. A seven-year clinical study of patients diagnosed with ADHD at a mean age of 34 years reported that approximately 30% did not maintain ADHD criteria and 12% presented full remission (defined as <4 symptoms at follow-up). Predictors of diagnos-tic persistence were higher number of inattention and hyperactivi-ty/impulsivity symptoms, previous ODD and social phobia at baseline [78].�
22
Aims and scope
The overall aim of this thesis is to broaden the understanding of ADHD in adulthood by screening for prevalence and investigating psychiatric comor-bidity in adults with ADHD, as well as to demonstrate long-term outcome and treatment safety in those diagnosed with ADHD as adults. The specific aims of this thesis follow a stepwise pattern closely coupled to experienced practical patient issues in everyday clinical practice.
The specific aims of this thesis are: • To survey the frequency and severity of self-reported ADHD-related
symptoms, difficulties and suffering, functional impairment and reading and spelling difficulties in patients seeking outpatient psychiatric care and in female prison inmates in comparison with a sample of the GP.
• To examine prevalence and sex differences of axis I and II comorbidity in a clinical sample of patients diagnosed with ADHD as adults. Specific interest was focused on analysing the prevalence and gender differences of personality disorders with and without fulfilment of the general diag-nostic criteria.
• To assess long-term outcome with respect to symptom reduction and function in a well-defined sample of patients first diagnosed with ADHD as adults, to compare outcome in the patients who were still on medica-tion versus those who discontinued medication, and also to identify po-tential baseline predictors of favourable outcome.
• To evaluate tolerability and safety of long-term treatment in adults with ADHD by assessing reasons for discontinuation as well as self-reported side effects in patients under current long-term treatment. To assess baseline predictors for adherence to treatment and to determine partici-pants own perceived outcome since diagnosed with ADHD and subse-quent treatment with stimulants and atomoxetine.

23
Method
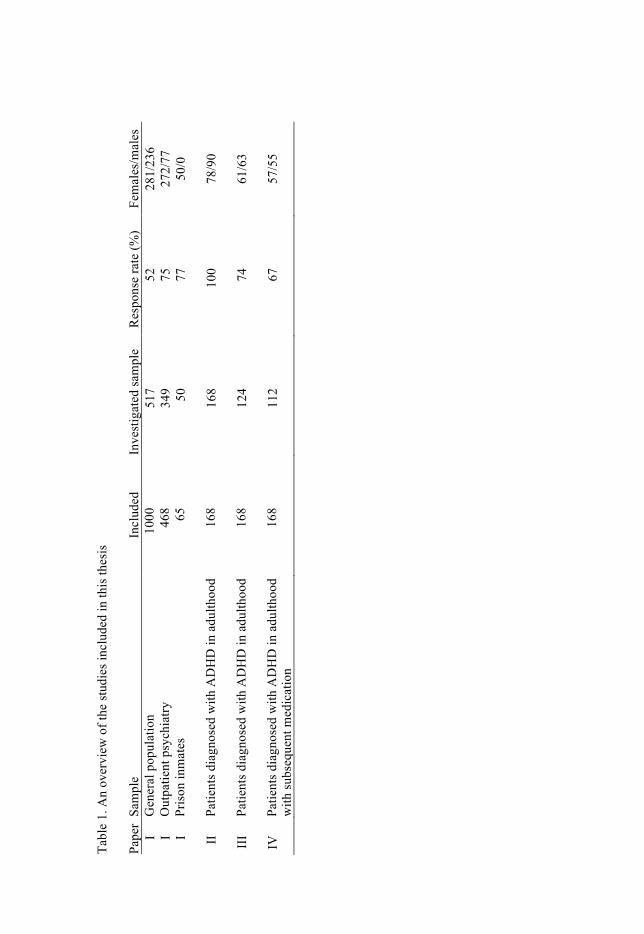
Study design and participants This thesis is based on cohort-studies performed in a piecemeal manner be-cause of different and subsequent aims. An overview of the studies is given in Table 1.
Paper I contains three studies investigating the prevalence of ADHD symptomatology in three cohorts: the GP, adult psychiatric outpatients and female prison inmates. The GP sample included of 1000 patients between 18 and 55 years of age who were randomly selected from the population regis-try in Uppsala County by an independent company. The patients were re-minded twice by mail after the initial request to participate. In all, 236 men and 281 women were included, representing a participation rate of 52%. The recruitment took place in autumn 2003. The psychiatric outpatient sample was made up of adult psychiatric outpatients in Uppsala County seeking care mainly for affective, anxiety, sleep and personality disorders, i.e. common comorbid disorders in adult ADHD. The reception personnel were instructed to inform every Swedish-speaking patient between 18 and 55 years of age about the study, both orally and in writing, and to invite them to participate. Four hundred and sixty-eight (n=468) patients were invited to participate in the study and 400 (85%) volunteered to take part. Of the 400 patients, 369 (92%) completed the study. However, 20 patients were excluded because of incomplete answers, leaving 77 men and 272 women for analysis, represent-ing a participation rate of 75% (349/468). The recruitment took place in De-cember 2003. The female prison sample comprised inmates from the Hinse-berg Prison, which is the largest prison for women in Sweden with the high-est security level. The prison is intended for female convicts from the entire country who are sentenced to long-term (six years on average) imprison-ment. The two most common crimes for which inmates were convicted were severe drug-related crimes (44%) and murder/manslaughter (21%). At the time of the study, there were 104 inmates; however, 17 had been transferred to a special unit for treatment of alcohol and drug addiction, 18 had been moved to an open-wing section because they had been convicted of minor crimes and 4 had been admitted to hospital. Accordingly, 65 high-security prisoners were available for the study and were invited to participate. Fifty women gave informed consent and the overall participation rate was 77 % (50/65). The recruitment took place in March-May 2004.
Tabl
e 1.
An
over
view
of t
he st
udie
s inc
lude
d in
this
thes
is
Pape
r Sa
mpl
e In
clud
ed
Inve
stig
ated
sam
ple
Res
pons
e ra
te (%
) Fe
mal
es/m
ales
I
Gen
eral
pop
ulat
ion
1000
51
7 52
28
1/23
6 I
Out
patie
nt p
sych
iatry
46
8 34
9 75
27
2/77
I
Pris
on in
mat
es
65
50
77
50/0
II
Patie
nts d
iagn
osed
with
AD
HD
in a
dulth
ood
168
168
100
78/9
0
III
Patie
nts d
iagn
osed
with
AD
HD
in a
dulth
ood
168
124
74
61/6
3
IV
Patie
nts d
iagn
osed
with
AD
HD
in a
dulth
ood
with
subs
eque
nt m
edic
atio
n 16
8 11
2 67
57
/55

25
Paper II included adults diagnosed with ADHD in adulthood. In 2002, a special outpatient clinic for referral of adult patients with suspected diagno-ses of ADHD, ASD and Tourette’s syndrome was established at Uppsala University Hospital. Of 233 consecutively referred patients, 168 (78 women and 90 men) were diagnosed with adult ADHD and subsequently included in this study. The recruitment took place in April 2002-October 2010.
Paper III is a follow-up study of participants included in paper II. Of the 168 eligible patients, 124 (74%) participated in the follow-up. The recruit-ment took place in March-October 2013.
Paper IV included the same participants who took part in study II and III who had been put on medication after being diagnosed with ADHD in adult-hood. Of the 168 patients diagnosed with ADHD in adulthood, 112 (67%) took part in the follow-up. The recruitment period was identical to paper III.
Procedures and measurements In paper I, the first part of the study questionnaire covered the 18 symptoms of ADHD according to DSM-IV. Each question was supplemented with a short description of possible adult expressions of the symptoms. The re-sponse format was four-fold, depending on current presence and burden of symptoms of ADHD: “never/seldom”, “sometimes”, “often” and “very of-ten”. Each answer corresponded to a score from 0 to 3. Thus, the scoring system is based on a minimum total score of 0 points and a maximum total score of 54 points (maximum score for hyperactivity-impulsivity=27 and inattention=27). A score of ≥2 for at least six of nine symptoms of inatten-tion or six of nine symptoms of hyperactivity-impulsivity was required to be categorised as an inattentive or hyperactive type of adult ADHD. Questions about ADHD symptoms during childhood, as reported to the participant by parents or other informants, were asked separately. The GP sample and psy-chiatric outpatient sample were asked about childhood hyperactivi-ty/impulsivity only, whereas the female inmates were also asked about childhood inattention. The first two samples were categorised as “hyperac-tive” if they endorsed hyperactivity in childhood or adulthood. The inmate sample was categorised as ADHD if they endorsed childhood hyperactivity or inattention or six of nine DSM-IV criteria as adults. The second part of the questionnaire contained questions on age and sex, as well as reading and spelling difficulties (dichotomised answers: yes/no). Functional impairment was assessed by asking the participants to rate difficulties and suffering caused by the current ADHD-related symptoms, using two 100-mm visual analogue scales (VASs) (end points: no difficulties/no suffering to totally handicapped), as well as to self-rate their social, occupation and psychologi-cal functioning using the Global Assessment of Functioning (GAF) scale during the past year and the past two weeks [25; 114]. The psychiatric pa-
26
tients were also asked about reasons for seeking care and about ongoing medication. The female prison inmates were screened for CD and ASPD by using relevant subscales of the self-report version of the DSM-IV and the ICD-10 personality questionnaire (DIP-Q) [8; 25].
In paper II, a multidisciplinary team made up of senior psychiatrists, clin-ical psychologists, social workers and occupational therapists performed all evaluations. The diagnostic procedure aimed at establishing best estimate diagnoses was confirmed by all participating professionals reaching consen-sus on the diagnostic outcome as well as on attributed impairment or suffer-ing [92]. All patients underwent a physical examination that included basic neurologic status, as well as routine laboratory testing, including urine screening for drugs. All patients were interviewed about current symptoms and behaviours associated with ADHD using a semi-structured interview based on the 18 DSM-IV criteria [8]. The interview included realistic exam-ples from everyday life that were obtained in clinical practice from adult patients. The patients were encouraged to give their own examples of adult ADHD with subsequent impairment in accordance with each diagnostic item. The answers were evaluated and rated according to four categories, depending on symptom frequency and impairment: “never”, “sometimes”, “often”, and “very often”. An answer of “often” or “very often” was catego-rised as a fulfilled criterion. Six or more of the maximum nine subtype crite-ria were required to fulfil a diagnosis of adult ADHD. A social worker or clinical psychologist collected and documented a developmental and social history from childhood to the present. The clinical version of the Structured Clinical Interview for DSM-IV axis I (SCID-I) [54], was administered by a senior psychiatrist (author, DE) with training in the use of this instrument to assess coexisting Axis I disorders. Evaluations of suspected ASD included semi-structured developmental interviews, i.e. the Diagnostic Interview for Social and Communication Disorders [94], and the Autism Diagnostic Inter-view-Revised [91], which were performed by senior clinical psychologists [91; 94]. Criteria for DSM-IV Axis II disorders were initially assessed by means of the DSM-IV and ICD-10 Personality Interview (DIP-I) [108]. It was later replaced by the Structured Clinical Interview for DSM-IV axis II (SCID II) [53], which is very similar to the DIP-I and was used for half (n=84) of the participating patients. ASPD was only considered if a previous history of CD had been confirmed. All interviews relative to personality disorders were performed by a senior psychiatrist (DE) with training in the use of the respective instruments.
In paper III, questionnaires were sent to the participants with questions about current symptoms of ADHD using a self-report version of the semi-structured interview used at baseline. Current functioning was assessed by a self-report version of the Global Assessment of Functioning Scale (GAF) [25; 114]. Potential improvement since baseline was measured by the Clini-cal Global Impressions Improvement scale (CGI-I). The CGI-I is a seven-

27
point scale from “very much improved” to “very much worse” [66]. Disabil-ity and impairment were investigated by the Sheehan Disability Scale (SDS) [96] a scale that covers three domains: work/school, social life and family life/home responsibilities. The SDS has recently been psychometrically evaluated in adult ADHD [39]. Health-related quality of life (HRQoL) was measured by EQ-5D and EQ-VAS [44; 142]. Alcohol consumption was as-sessed by the Alcohol Use Disorders Identification Test (AUDIT) [13] and drug consumption by the Drug Use Disorders Identification Test (DUDIT) [19]. When the questionnaires had been returned, a telephone interview was conducted covering demographics as well as details of the participants’ past and current medical condition. Participants’ information on previous medica-tion periods was validated against data in their patient files if available. In case of contradictory data, we choose to rely on patient file data.
In paper IV, data from paper III were supplemented with information about each treatment period, defined as being of at least one month’s length and with an intervening one-month period of non-medication or more before another attempt of pharmacological treatment was considered. Patients’ in-formation about previous medication periods and reasons for discontinuation were validated against data in their patient records. In case of contradictory data, we again choose to rely on patient record data. If there were several treatment periods, the final reason for discontinuation was registered for each pharmacological substance. In patients with ongoing medication, cur-rent adverse effects were assessed by a form covering 31 adverse effects which was used as part of the clinical routine in patients treated at the clinic for neuropsychiatry at Uppsala University Hospital. The frequency of ad-verse symptoms was categorised as “Never”, “Sometimes” (corresponding to 1-2 times/week), “Often” (corresponding to 3-6 times/week) and “Very of-ten” (corresponding to daily/always). There were also questions on the pa-tients’ experience of the effect of current medication, adherence and dosage pattern. Finally, participants were asked to respond to five statements about how their status had changed since baseline: “My quality of life has im-proved”, “My level of functioning has improved”, “My understanding of my way of functioning has increased”, “I have encountered greater understand-ing from the environment of my way of functioning” and “I find it worthwhile having been evaluated for ADHD”. Answers to the first four statements were categorised in a four-step scale from “Not at all” to “Exactly correct”; the last statement (...worthwhile having been evaluated...) was categorised in the opposite order from “Yes, indeed” to “Not at all”. Data on deceased par-ticipants’ cause of death among dropouts in paper III and their ongoing pharmacological treatment at the time of death were supplied by The Swe-dish National Board of Health and Welfare.

28
Statistics All statistical analyses were performed using PASW Statistics, version 12.0.1 (paper I), version 18.0 (paper II) and version 23 (paper III and IV). P-values ˂0.05 were considered statistically significant.
Dichotomous data were analysed using chi-square test statistics or Fisher’s exact test when applicable with a cell count number of ˂5.
A Kolmogorov-Smirnov test was used to test for normality. When appro-priate, the non-parametric Mann-Whitney U test was employed to determine group differences; otherwise, the t-test was performed for continuous data.
Inter-rater reliability of continuous scale data was tested by single-measure intraclass correlation and diagnostic agreement was tested using Cohen’s kappa.
Because symptom and GAF scores in paper I were not normally distribut-ed, differences in mean scores were analysed using the Mann-Whitney U test for independent samples. Confounding by skewed sex proportions and a higher prevalence of hyperactivity in the outpatient sample was corrected using Mantel-Haenszel statistics. Because age was unevenly distributed among men and in the number of diagnoses on axis I in both sexes, the Mann-Whitney U test was used for analysis of sex differences in paper II. All baseline variables (e.g., age, sex, ADHD subtype and score, psychiatric comorbidity, sociodemographic data and treatment-related variables) were tested for possible inclusion in univariate logistic regression models with remission as the dependent variable in paper III and ongoing pharmacologi-cal treatment in paper IV. None of these variables were significantly related to either of the dependent variables, however.
Ethics All studies included in this thesis were approved by the Regional Ethics Re-view Board at Uppsala University: 02-452 (paper I), 2006/241 (paper II), 2012/544 (paper III and IV).
29
Results
ADHD-related symptoms among adults in outpatient psychiatry and female prison inmates as compared with the general population (Paper I) This study aimed to compare the prevalence of symptoms consistent with ADHD and related problems in adults in the GP, in outpatient psychiatry (where females are in the majority) and in female convicts. Detailed infor-mation concerning participating subject characteristics is given in paper I.
Prevalence of ADHD-symptomatology One third (32.4%) of the participants in the outpatient psychiatry sample reported hyperactivity versus about one sixth (15.1%) in the GP sample. All three subgroups (childhood only, both childhood and adult and adult only) were more prevalent in the outpatient sample than in the GP sample. The prevalence of both adult and childhood hyperactivity/impulsivity was ap-proximately three times higher among participants in the outpatient sample compared with the GP sample (6.6 versus 2.1%).
Fifty per cent of the female inmates reported symptoms of ADHD in childhood or as adults; 6 of the 50 participants (12%) reported inattention only in childhood. Fifteen participants (30%) had both childhood inattention and adult symptoms of ADHD. The frequencies of inmates endorsing the criteria for CD and ASPD, self-rated GAF values and reading and spelling difficulties in inmates, with and without symptoms of ADHD, are summa-rised in Table 2.
Difficulties and suffering attributed to ADHD-related symptoms The levels of difficulties and suffering due to ADHD-related symptoms in the outpatient sample were significantly higher in those classified as hyper-active and in those not classified as hyperactive as compared with the GP sample. Within the GP sample, only the subgroup that reported both child-hood and adult hyperactivity had significantly higher levels of difficulties and suffering as compared with the non-hyperactive group. In the outpatient sample, all subgroups had significantly higher levels of difficulties and suf-fering as compared with the non-hyperactive group. There were no major differences between men and women within the two samples. In the inmate
30
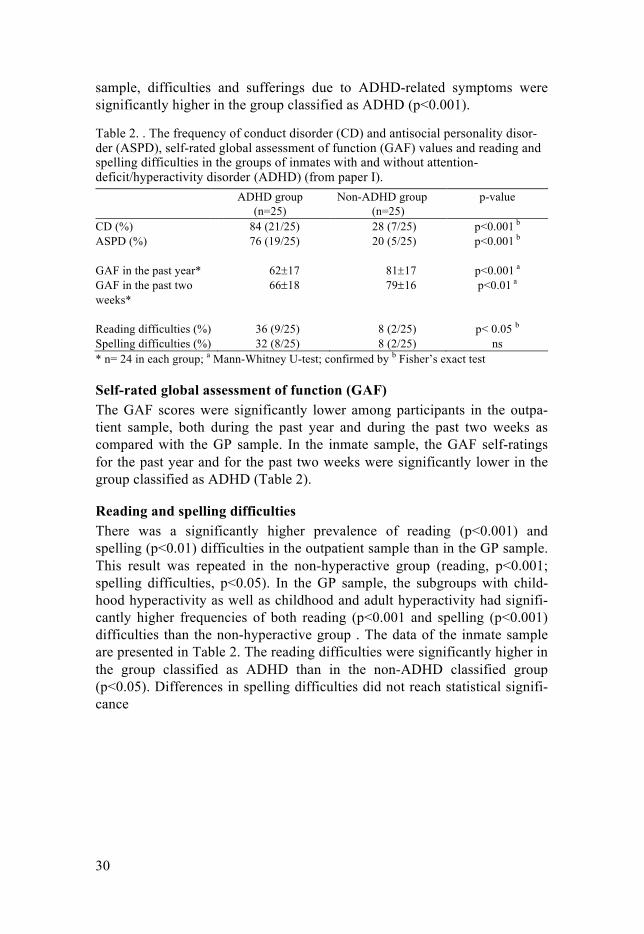
sample, difficulties and sufferings due to ADHD-related symptoms were significantly higher in the group classified as ADHD (p<0.001).
Table 2. . The frequency of conduct disorder (CD) and antisocial personality disor-der (ASPD), self-rated global assessment of function (GAF) values and reading and spelling difficulties in the groups of inmates with and without attention-deficit/hyperactivity disorder (ADHD) (from paper I). ADHD group
(n=25) Non-ADHD group
(n=25) p-value
CD (%) 84 (21/25) 28 (7/25) p<0.001 b ASPD (%) 76 (19/25) 20 (5/25) p<0.001 b GAF in the past year* 62±17 81±17 p<0.001 a GAF in the past two weeks*
66±18 79±16 p<0.01 a
Reading difficulties (%) 36 (9/25) 8 (2/25) p< 0.05 b Spelling difficulties (%) 32 (8/25) 8 (2/25) ns * n= 24 in each group; a Mann-Whitney U-test; confirmed by b Fisher’s exact test
Self-rated global assessment of function (GAF) The GAF scores were significantly lower among participants in the outpa-tient sample, both during the past year and during the past two weeks as compared with the GP sample. In the inmate sample, the GAF self-ratings for the past year and for the past two weeks were significantly lower in the group classified as ADHD (Table 2).
Reading and spelling difficulties There was a significantly higher prevalence of reading (p<0.001) and spelling (p˂0.01) difficulties in the outpatient sample than in the GP sample. This result was repeated in the non-hyperactive group (reading, p<0.001; spelling difficulties, p˂0.05). In the GP sample, the subgroups with child-hood hyperactivity as well as childhood and adult hyperactivity had signifi-cantly higher frequencies of both reading (p<0.001 and spelling (p˂0.001) difficulties than the non-hyperactive group . The data of the inmate sample are presented in Table 2. The reading difficulties were significantly higher in the group classified as ADHD than in the non-ADHD classified group (p<0.05). Differences in spelling difficulties did not reach statistical signifi-cance
31
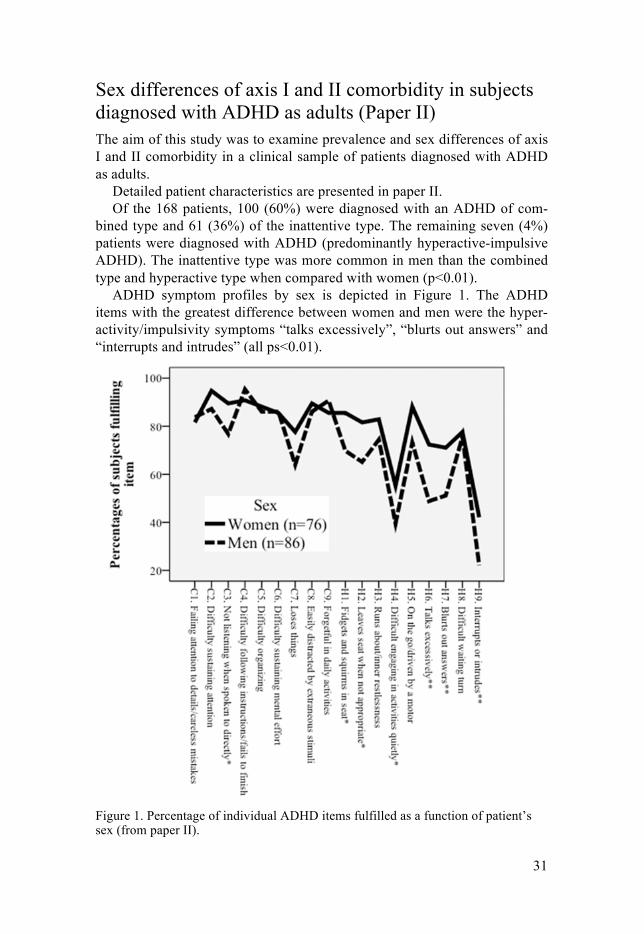
Sex differences of axis I and II comorbidity in subjects diagnosed with ADHD as adults (Paper II) The aim of this study was to examine prevalence and sex differences of axis I and II comorbidity in a clinical sample of patients diagnosed with ADHD as adults.
Detailed patient characteristics are presented in paper II. Of the 168 patients, 100 (60%) were diagnosed with an ADHD of com-
bined type and 61 (36%) of the inattentive type. The remaining seven (4%) patients were diagnosed with ADHD (predominantly hyperactive-impulsive ADHD). The inattentive type was more common in men than the combined type and hyperactive type when compared with women (p<0.01).
ADHD symptom profiles by sex is depicted in Figure 1. The ADHD items with the greatest difference between women and men were the hyper-activity/impulsivity symptoms “talks excessively”, “blurts out answers” and “interrupts and intrudes” (all ps<0.01).
Figure 1. Percentage of individual ADHD items fulfilled as a function of patient’s sex (from paper II).
32
The lifetime prevalence of any comorbid axis I disorder was 95% in women and 90% in men (Table 3). The mean number of lifetime diagnoses, includ-ing ASD and Tourette’s syndrome, was 2.7±1.5 (range 1-7) in women and 2.7±1.8 (range 1-11) in men. Women were significantly more often diag-nosed with mood and eating disorders, whereas men significantly more often fulfilled criteria for SUD (Table 3).
The presence of at least one current Axis I disorder, including ASD and Tourette’s syndrome was diagnosed in 47 % (45 % in the women and 49 % in the men).
Table 3. Prevalence of psychiatric comorbidity on axis I in the clinical cohort of patients investigated from paper II. Prevalence Disorder Women; n (%) Men; n (%) χ2 p-value1
Axis I disorders
Lifetime
Any mood disorder 71 (91.0) 60 (66.7) 14.44 <0.001 Any anxiety disorder 33 (42.3) 37 (41.1) 0.25 ns Any somatoform disorder 2 (2.6) 1 (1.1) 0.50 ns Any eating disorder 17 (21.8) 0 (0) 21.82 <0.001 Adjustment disorder 1 (1.3) 1 (1.1) 0.10 ns Any psychotic disorder 1 (1.3) 2 (2.2) 0.21 ns Any substance use disorder 26 (33.0) 45 (50.0) 4.76 <0.05
Comorbid neuropsychiatric disorders Any autism spectrum disorder 6 (7.7) 11 (12.2) 0.94 ns Tourette’s syndrome 2 (2.6) 6 (6.7) 1.55 ns
Any Axis I disorder, including comorbid neuropsychiatric disorder
74 (94.9) 81 (90.0) 1.39 ns
Current Any Axis I disorder, including comorbid neuropsychiatric disorder
35 (44.9) 44 (48.9) 0,27 ns
1 women vs. men
When the general diagnostic criteria for a personality disorder were consid-ered, only six women (8%) and 10 men (11%) were diagnosed with an Axis II disorder. However, when only considering the specific criteria for at least one personality disorder, 36 women (46%) and 41 men (46%) fulfilled spe-cific criteria (Table 4). The only observable sex differences concerned ful-filment of the specific criteria for histrionic personality disorder and for CD, with the former more common in women (p<0.05) and the latter more com-mon in men (p<0.01). In addition, men more often fulfilled specific criteria for ASPD compared with women, but the difference was not statistically significant (p=0.06).
33
Table 4. Comorbidity of personality disorders without considering the general diag-nostic criteria in the investigated group of patients (from paper II). Fulfilment of specific criteria
Women; n (%) Men; n (%) χ2 p-value a
Cluster A 5 (6.4) 4 (4.4) 0.32 ns Cluster B 20 (25.6) 26 (28.9) 0.22 ns
Antisocial 8 (10.3) 19 (21.1) 3.65 0.056 Conduct disorder 26 (33.3) 54 (60.0) 11.91 <0.01
Borderline 11 (14.1) 13 (14.4) 0.04 ns Histrionic 4 (5.1) 0 (0) 4.23 <0.05 Narcissistic 0 (0) 3 (11.1) 2.64 ns
Cluster C 23 (29.5) 17 (18.9) 0.11 ns Any cluster 36 (46.2) 41 (45.6) 0.01 ns a women vs. men.
Twenty-nine (17%) of the 168 patients were directly referred for evaluation of ADHD. The remaining 139 patients had a previous history in adult psy-chiatry (with a mean duration of 7.3±6.2 years, range 0-28) before being identified as potential ADHD patients and subsequently referred for evalua-tion by either adult psychiatry or primary health care. Twenty-seven women (35%) and 35 men (39%) reported previous contact with child and adoles-cent outpatient psychiatric clinics (one man had ongoing contact).
At the time of the evaluation, 110 (65%) of the patients were on medica-tion. The five most common prescribed pharmaceuticals were medication for somatic disorders: for example, hypertensives and antibiotics, analgesics excluded, 25%), followed by antidepressants other than serotonin reuptake inhibitors (SSRIs, 21%), SSRIs (18%), benzodiazepines (14%) and hypnot-ics other than benzodiazepines (11%). Women were prescribed SSRIs more frequently than men (p<0.01); no other sex differences were identifiable.
Six-Year Outcome in Subjects Diagnosed with Attention-Deficit/Hyperactivity Disorder as Adults (Paper III) The study aimed to assess long-term outcome for symptom reduction and function in a cohort of patients first diagnosed with ADHD as adults in rela-tion to current medication (or not) and to identify potential baseline predic-tors of favourable outcome. The primary outcome measure was remission, which was defined as not fulfilling any ADHD subtype and a GAF score of ≥70 during the past year.
34
Participants constitute a subgroup of patients presented in paper II and de-tailed information of patient characteristics is presented in paper III.
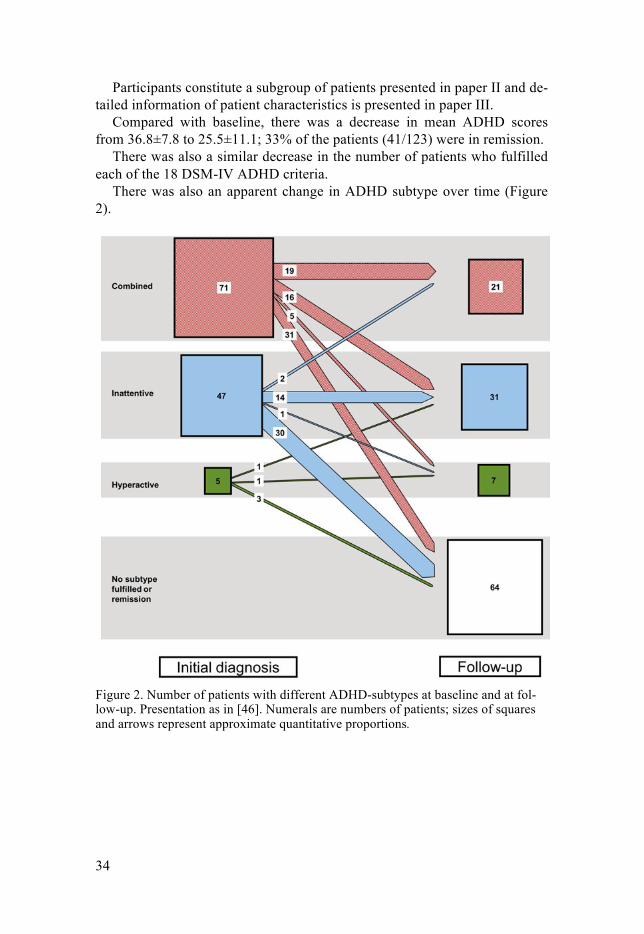
Compared with baseline, there was a decrease in mean ADHD scores from 36.8±7.8 to 25.5±11.1; 33% of the patients (41/123) were in remission.
There was also a similar decrease in the number of patients who fulfilled each of the 18 DSM-IV ADHD criteria.
There was also an apparent change in ADHD subtype over time (Figure 2).
Figure 2. Number of patients with different ADHD-subtypes at baseline and at fol-low-up. Presentation as in [46]. Numerals are numbers of patients; sizes of squares and arrows represent approximate quantitative proportions.

35
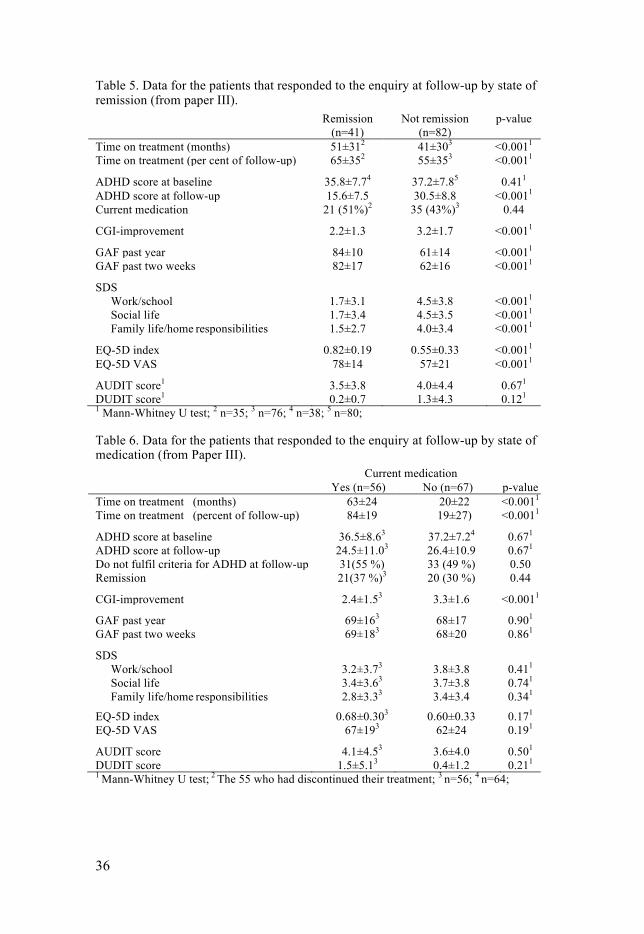
In general, patients with a combined ADHD subtype at baseline remained as a combined subtype, changed into an inattentive subtype, or did not fulfil the criteria for a diagnosis of ADHD at follow-up Patients with an inattentive ADHD subtype either maintained the diagnosis or did not fulfil criteria for a diagnosis of ADHD. There was no decline in the number of patients with the hyperactive type, whereas the number of patients with a combined ADHD subtype decreased from 71 to 21 (i.e. with 70%) and the number of patients with an inattentive ADHD subtype decreased from 47 to 31 (i.e. with 34%). Patients in remission reported similar ADHD scores at baseline as those who were not in remission (Table 5). Furthermore, there was no difference in current medication between the groups (51 versus 43%). Patients in remis-sion reported significantly better global functioning, less disability, better quality of life (QoL) and better clinical improvement than those who were not in remission. There was no difference in mean alcohol consumption, as measured by AUDIT scores, and drug use, as assessed by DUDIT scores. Scores above limits for harmful drinking [13] however, were observed in 7% of those in remission versus 24% of those who were not (p=0.03), and risk scores for potential drug-related problems [19] in 2% of those in remission versus 11% of those who were not (p=0.16).
Reciprocally, there was no difference in remission rate between patients in the current medication group, (37%) and in those not currently medicated (30%). Medicated patients reported similar ADHD scores as those without ongoing medication, both at baseline and at follow-up. They also reported similar global functioning, disability and QoL than those not medicated, although medicated patients showed better clinical improvement (Table 6).
All baseline variables and treatment-related variables were tested for pos-sible inclusion in a regression model with remission as the dependent varia-ble. None of these variables were significantly related to remission.
36
Table 5. Data for the patients that responded to the enquiry at follow-up by state of remission (from paper III).
Remission (n=41)
Not remission (n=82)
p-value
Time on treatment (months) 51±312 41±303 <0.0011 Time on treatment (per cent of follow-up) 65±352 55±353 <0.0011
ADHD score at baseline 35.8±7.74 37.2±7.85 0.411 ADHD score at follow-up 15.6±7.5 30.5±8.8 <0.0011 Current medication 21 (51%)2 35 (43%)3 0.44
CGI-improvement 2.2±1.3 3.2±1.7 <0.0011
GAF past year 84±10 61±14 <0.0011 GAF past two weeks 82±17 62±16 <0.0011
SDS Work/school 1.7±3.1 4.5±3.8 <0.0011 Social life 1.7±3.4 4.5±3.5 <0.0011 Family life/home responsibilities 1.5±2.7 4.0±3.4 <0.0011
EQ-5D index 0.82±0.19 0.55±0.33 <0.0011 EQ-5D VAS 78±14 57±21 <0.0011
AUDIT score1 3.5±3.8 4.0±4.4 0.671 DUDIT score1 0.2±0.7 1.3±4.3 0.121 1 Mann-Whitney U test; 2 n=35; 3 n=76; 4 n=38; 5 n=80;
Table 6. Data for the patients that responded to the enquiry at follow-up by state of medication (from Paper III). Current medication Yes (n=56) No (n=67) p-value Time on treatment (months) 63±24 20±22 <0.0011 Time on treatment (percent of follow-up) 84±19 19±27) <0.0011 ADHD score at baseline 36.5±8.63 37.2±7.24 0.671 ADHD score at follow-up 24.5±11.03 26.4±10.9 0.671 Do not fulfil criteria for ADHD at follow-up 31(55 %) 33 (49 %) 0.50 Remission 21(37 %)3 20 (30 %) 0.44 CGI-improvement 2.4±1.53 3.3±1.6 <0.0011 GAF past year 69±163 68±17 0.901 GAF past two weeks 69±183 68±20 0.861 SDS
Work/school 3.2±3.73 3.8±3.8 0.411 Social life 3.4±3.63 3.7±3.8 0.741 Family life/home responsibilities 2.8±3.33 3.4±3.4 0.341
EQ-5D index 0.68±0.303 0.60±0.33 0.171 EQ-5D VAS 67±193 62±24 0.191 AUDIT score 4.1±4.53 3.6±4.0 0.501 DUDIT score 1.5±5.13 0.4±1.2 0.211 1 Mann-Whitney U test; 2 The 55 who had discontinued their treatment; 3 n=56; 4 n=64;
37
Long-Term Tolerability and Safety of Pharmacological Treatment of Adult Attention-Deficit/Hyperactivity Disorder (Paper IV) The aim of this study was to evaluate tolerability and safety of long-term treatment in adults with ADHD by examining patient reasons for discontinu-ation as well as self-reported side effects in patients currently on long-term treatment. The study also assessed baseline predictors for adherence to treatment and attempted to determine participants’ perceived outcome since being diagnosed with ADHD.
Participants constitute a subgroup of patients presented in paper II and III. Detailed information on patient characteristics is presented in paper IV. Data on dropouts in paper III revealed that five persons had died since their ADHD diagnosis and only one by way of natural causes.
Fifty-seven patients were currently on treatment and 55 had discontinued treatment. There were no significant differences in baseline data between current treatment and the off-treatment patients. Time on medication was longer in patients on treatment compared with those who had discontinued (63±24 versus 24±22 months).
Of the currently medicated patients, 46 were on treatment with methylphenidate, 8 with amphetamine and 3 on a combination of methylphenidate and atomoxetine. Of the eight patients currently treated with amphetamine, seven had previously been on methylphenidate. Five patients had previously been treated with atomoxetine but discontinued. Of the currently medicated patients, 56 had a lifetime history of treatment with methylphenidate, 13 with amphetamine and 8 with atomoxetine.
The maximum dosage during treatment was 84±37 mg for methylpheni-date, 43±10 mg for amphetamine and 68±23 for atomoxetine. The current dose was 60±32 mg for methylphenidate, 42±9 mg for amphetamine and 38±13 mg for atomoxetine.
Most patients on treatment with methylphenidate were treated with medi-um- or long-acting agents All patients treated with amphetamine were on short-acting tablets.
Seventy-eight per cent of the patients took their medication once or twice daily. Eighty-four per cent of the patients stated that they took their medica-tion in the exact dosage as prescribed, whereas 16% reported that they used a lower dosage. Eighty-eight per cent reported daily adherence to treatment.
The total time on treatment was 61±24 months for stimulants, i.e. time of treatment with methylphenidate and amphetamine added together; for atomoxetine, the time was 9±17 months for the first treatment period. The number of stimulant treatment periods was 2±1). When corrected for over-lapping time of treatment with stimulants and atomoxetine, the total treat-ment time increased to 63±24 months.
38
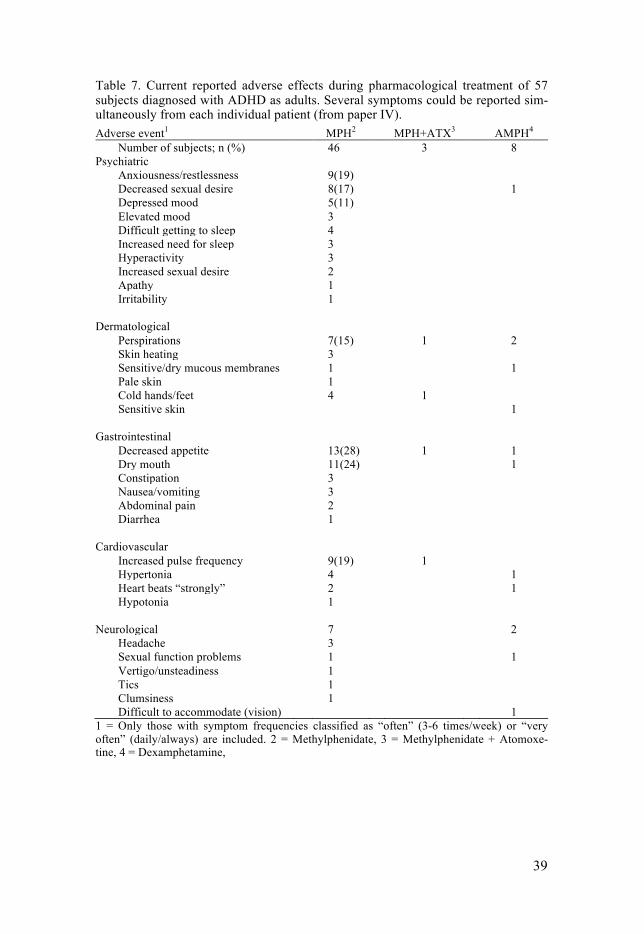
Current adverse effects during pharmacological treatment of patients di-agnosed with ADHD as adults are presented in Table 7. The most common adverse effects related to methylphenidate were decreased appetite (28%), dry mouth (24%) and anxiousness/restlessness, increased pulse frequency (19%).
Finally, 81% of the patients reported a pronounced beneficial effect of their ongoing medication and an additional 16% reported a moderate benefi-cial effect.
The dosage at the time of discontinuation for those patients without cur-rent medication was 68±42 mg for methylphenidate, 47±18 mg for amphet-amine and 57±28 mg for atomoxetine. The total time on treatment with stimulants was 22±21 months; the total time on treatment with atomoxetine was 6±12 months. The number of treatment periods was 2±1 for stimulants (no patients had been treated with atomoxetine more than once). When cor-rected for overlapping time of treatment with stimulants and atomoxetine, the total treatment time increased to 24±22 months.
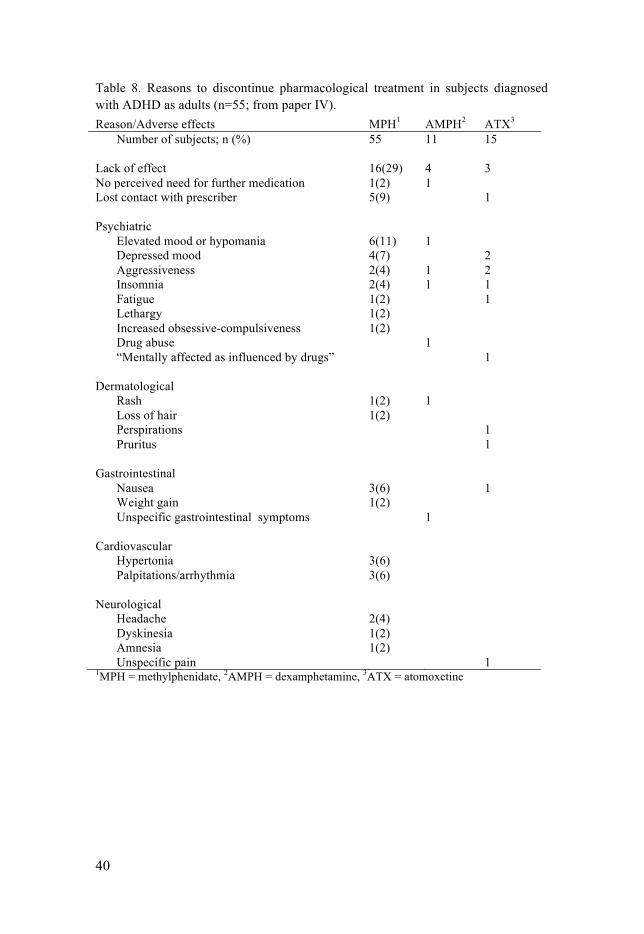
The reasons for discontinuation of treatment are given in Table 8. The top three reasons for discontinuation of treatment with methylphenidate were lack of effect (29%), elevated mood or hypomania (11%) and not being able to maintain contact with the prescriber (9%). None of the patients who dis-continued methylphenidate or amphetamine because of elevated mood or hypomania had been diagnosed with a bipolar disorder before medication. One patient had been diagnosed with bipolar type II and one with bipolar NOS at baseline; these two patients were treated with methylphenidate only. In both these cases, depressive symptoms were the reason for discontinua-tion. Fifteen patients had been treated with atomoxetine and the most com-mon reason for discontinuation was, as with stimulants, lack of effect. Fur-ther reasons for discontinuation were widespread, but in almost half of the patients discontinuation was related to psychiatric side effects.
The statements, "My quality of life has improved", "My level of function-ing has improved" and "Encountered increased understanding" were en-dorsed to a higher degree among those patients still on medication.
39
Table 7. Current reported adverse effects during pharmacological treatment of 57 subjects diagnosed with ADHD as adults. Several symptoms could be reported sim-ultaneously from each individual patient (from paper IV). Adverse event1 MPH2 MPH+ATX3 AMPH4
Number of subjects; n (%) 46 3 8 Psychiatric
Anxiousness/restlessness 9(19) Decreased sexual desire 8(17) 1 Depressed mood 5(11) Elevated mood 3 Difficult getting to sleep 4 Increased need for sleep 3 Hyperactivity 3 Increased sexual desire 2 Apathy 1 Irritability 1
Dermatological
Perspirations 7(15) 1 2 Skin heating 3 Sensitive/dry mucous membranes 1 1 Pale skin 1 Cold hands/feet 4 1 Sensitive skin 1
Gastrointestinal
Decreased appetite 13(28) 1 1 Dry mouth 11(24) 1 Constipation 3 Nausea/vomiting 3 Abdominal pain 2 Diarrhea 1
Cardiovascular
Increased pulse frequency 9(19) 1 Hypertonia 4 1 Heart beats “strongly” 2 1 Hypotonia 1
Neurological 7 2
Headache 3 Sexual function problems 1 1 Vertigo/unsteadiness 1 Tics 1 Clumsiness 1 Difficult to accommodate (vision) 1
1 = Only those with symptom frequencies classified as “often” (3-6 times/week) or “very often” (daily/always) are included. 2 = Methylphenidate, 3 = Methylphenidate + Atomoxe-tine, 4 = Dexamphetamine,
40
Table 8. Reasons to discontinue pharmacological treatment in subjects diagnosed with ADHD as adults (n=55; from paper IV). Reason/Adverse effects MPH1 AMPH2 ATX3
Number of subjects; n (%) 55 11 15 Lack of effect 16(29) 4 3 No perceived need for further medication 1(2) 1 Lost contact with prescriber 5(9) 1 Psychiatric
Elevated mood or hypomania 6(11) 1 Depressed mood 4(7) 2 Aggressiveness 2(4) 1 2 Insomnia 2(4) 1 1 Fatigue 1(2) 1 Lethargy 1(2) Increased obsessive-compulsiveness 1(2) Drug abuse 1 “Mentally affected as influenced by drugs” 1
Dermatological
Rash 1(2) 1 Loss of hair 1(2) Perspirations 1 Pruritus 1
Gastrointestinal
Nausea 3(6) 1 Weight gain 1(2) Unspecific gastrointestinal symptoms 1
Cardiovascular
Hypertonia 3(6) Palpitations/arrhythmia 3(6)
Neurological
Headache 2(4) Dyskinesia 1(2) Amnesia 1(2) Unspecific pain 1
1MPH = methylphenidate, 2AMPH = dexamphetamine, 3ATX = atomoxetine

41
Discussion
The principal aim of this thesis was to aid in the understanding of ADHD in adulthood by screening for prevalence and investigating psychiatric comor-bidity in adults with ADHD, as well as demonstrating long-term outcome and treatment safety in persons diagnosed with ADHD as adults.
Methodological considerations Design, samples and methods For practical reasons, we decided in paper I to restrict participants in the GP and outpatient sample to persons residing in Uppsala County and belonging to a certain age group, which per se entails a selection bias. The age span of 18-55 years was arbitrarily chosen to diminish the risk for confounding dis-orders occurring in older age groups. Uppsala County spans a widely diverse geographic area that includes an expanding university city as well as less populated areas with traditional industry, much like the rest of the country of Sweden. This diversity would, to some extent, contribute to ensuring that both the GP sample and the outpatient sample are representative of the Swe-dish population.
Anonymous participation was chosen in all three samples to extract truth-ful and honest answers as well as a high participation rate. This approach unfortunately prevented attrition analyses. Concerning dropouts, ADHD-related symptoms in combination with reading difficulties might be more frequent in non-participants. Previous studies on attrition that examined oth-er psychiatric disorders have reported a number practical issues [160], where low income, low education level and a previous psychiatric diagnosis were associated with lower participation rates [18]. From our own experiences in the follow-up study, it cannot be ruled out that non-participants in paper I may have had an even higher prevalence of ADHD symptomatology than the patients included in the study.
Furthermore, it is important to stress that symptom reporting in paper I did not include clinical evaluations, but describes patient self-reports of symptomatology in accordance with ADHD. Self-report questionnaires, in general, are easily administered and time-saving, but they have some inher-ent issues that must be considered. Apart from various degrees of validity

42
and reliability of each instrument, systematic biases can be pronounced [36]. Another point to consider concerns issues such as who; the patient of next of kin, in reality answered the questionnaires, how the questionnaires were administered, and the fact that respondents used the questionnaires to freely comment and communicate on symptom patterns and experiences. At the time of Study I there were no validated screening instruments for current symptoms of adult ADHD available for a Swedish population. The ADHD questionnaire used by us in this study was constructed and based solely on the DSM-IV diagnostic criteria but shared the disadvantage of not being validated. The scale questions were, however, similar or almost identical to the official WHO rating scale to evaluate adult ADHD, ASRS, that was pub-lished later [82].
To optimise the length of the questionnaire, it only focused on present symptoms of ADHD. Regarding childhood history, we chose to use a di-chotomous Yes/No approach because we feared that an almost duplicated questionnaire which also included questions on lifetime problems would markedly increase attrition. The mixed sex samples of the GP and outpa-tients were only asked about childhood hyperactivity as there was an initial focus on the combined and hyperactive/impulsive subtypes according to DSM-IV, which are equivalent to the HKD of ICD-10. In the all-female prison inmate sample, a question on childhood inattention was supplement-ed. It is regrettable that this was not done in the first two samples. To distin-guish between shortcomings attributable to symptoms of ADHD and other reasons for reduced functioning, the participants were asked to report about difficulties and suffering exclusively caused by current ADHD symptoms. For this purpose, we decided on a scale with a construction similar to the GAF. Self-rated GAF scores have been shown to constitute a valid and relia-ble instrument [114]. Outpatients and prison inmates with known ongoing substance abuse, a feature which is recognised as being associated with high prevalence rates of ADHD and related problems, were not included in the present surveys and may have biased the observed prevalence rates. The advantage of that decision was, however, that we could demonstrate that ADHD and related problems among non-addicts and patients in abstinence of drugs are common and need to be recognised. On the other hand, there were no questions on SUD in any of the questionnaires, why it is possible anyway that a number of unidentified patients with SUD were included.
Paper II is a descriptive study of a prospective sample of patients evaluat-ed and diagnosed with ADHD as adults. The study design was based on in-formation that could be extracted from the patient files. Selection bias may have been introduced into the sample because the majority of the patients were referred and had a previous history of psychiatric treatment, although not diagnosed with ADHD. Still, by using consecutive inclusion, we hoped to reduce the risk of further selection bias. All evaluations were performed in the same outpatient clinic with a multi-professional neuropsychiatric team. A

43
reliable process to diagnose ADHD in adulthood in a scientific way was complicated as there was no validated semi-structured interview available for adults in Swedish in 2002 when the evaluations started. CAADID was published in English in 2001 but was, and is, restricted to copyright law and not available in Swedish. We chose to do the evaluation of adult ADHD symptoms using a self-constructed and semi-structured interview according to DSM-IV, which was similar to the questionnaire distributed in the previ-ous studies. Because this interview had not previously been validated, diag-nostic validity was ensured through interviews being videotaped and inde-pendently and blindly rated by a second senior psychiatrist with long experi-ence in clinical encounters with patients suffering from neuropsychiatric disorders. Inter-rater reliability was excellent for individual ADHD items, as well as the final diagnostic outcome (paper II).
Another potential problem concerns the possibility for patient recall bias, particularly regarding retrospective assessment of lifetime axis I disorders. This problem has been noticed in a previous study where a birth cohort was followed from age 18 to 32 years, and where the prevalence of lifetime psy-chiatric disorders almost doubled when assessed prospectively as compared to when assessed retrospectively [102].
Another limitation was the lack of a specific assessment of overall func-tioning (e.g. GAF) in the patient records. However, complete and extensive demographic data were collected and analysed, indicating, at least indirectly, some measure of overall social functioning. Only 34% of the participants were working full or part time, which is lower than figures reported from previous comorbidity studies [83; 132], where 61% and 72% respectively were working.
Best estimate diagnoses were established by members of the professional team who independently participated in the evaluation process. In general, we consider the best estimate diagnostic process for all the participating patients to provide reasonable evidence of functional impairment in accord-ance with ADHD. Psychiatric comorbidity was investigated by SCID-I and SCID-II interviews to secure validity of axis I and axis II disorders.
Paper III and IV included a follow-up of the sample described in paper II. The follow-up was based across a broad spectrum of instruments. Being a long-term follow-up study with a mean time of six years (range up to 11 years), the study design was subject to several practical and important issues. Previously documented everyday difficulties which were presented by pa-tients with ADHD were challenges to be considered in order to maximise participation rate. The protocol was therefore designed to optimise data col-lection. In addition, we assumed that a potential part of the participants would have moved far away from the original catchment area and maybe even abroad. We therefore decided on a two-step study design with initial self-questionnaires to be followed by an interview and validation of the an-swers given to the items in the questionnaires. In this way, missing infor-
44
mation, obvious misunderstandings and other potential problems in the first step of the protocol could be resolved in the protocol’s second step. This approach proved to be successful as it became clear that a number of partici-pants needed assistance (e.g., telephone, a personal visit at the clinic or a home visit) to complete the questionnaires. Another issue is that baseline ADHD symptoms had been obtained using a semi-structured interview; while the symptoms at follow up were obtained using a self-report question-naire, although with the same questions. Here it must be considered that adults with ADHD have been found to be their best informants regarding their symptoms but tend to underreport the severity of their symptoms [86]. Adding informant reports from partners and significant others, as in the di-agnostic process, would probably had accessed additional information.
To assess function apart from GAF, we choose to use the SDS because it had recently been psychometrically evaluated in adult ADHD. This scale is a comprehensive but short instrument measuring everyday functioning do-mains applicable to any psychiatric as well as somatic disorder. The Weiss Functional Impairment Rating Scale (WFIRS) [144] would probably have yielded more detailed and specific information on impairment related to ADHD but was omitted because our protocol already contained a large num-ber of questionnaires.
We choose the ERQ-5D to assess HRQoL. EQ-5D is short and easy to administer. We also choose AUDIT and DUDIT instruments for screening of alcohol and substance abuse, respectively. These are regarded as the gold standard for screening, and have been used for this purpose in numerous studies.
The fact that there was no information on overall or cognitive functioning at baseline might have influenced and biased the comparison in the different groups at follow-up. Information from a parallel non-pharmacological treat-ment and support arm, as well as an evaluation of psychiatric comorbidity at follow-up would have contributed to more precise analyses. Obviously, an RCT with a placebo treated control group would have been the most optimal design to collect comparison data on long-term outcome. However, such a design would be both practically impossible over a period of up to 11 years and ethically extremely questionable. Another option, such as that used in follow-up studies of the original MTA study, would be to attach a normal matched control group to compare outcome [139]. This would have been a more elaborate and extensive study design to demonstrate long-term out-come of adult ADHD and would have facilitated interpretation of the data obtained and demonstrated in papers III and IV.
Finally, no formal calculation of statistical power was performed before designing any of the studies. In paper I, we assumed that a sample of 1000 patients in the GP would be sufficient based on a previously reported preva-lence rate of ADHD in children of 3-7%. In the outpatient sample, we hy-pothesised a potentially higher prevalence rate and thus restricted the num-

45
ber of distributed questionnaires to 400. The female inmates constituted all high-security internees at the only prison available for investigation at the time. Patients in paper II, III and IV were those that were consecutively evaluated and diagnosed over a specific period. Nevertheless, it is highly probable that a higher number of participants would have facilitated detailed sub-analyses and identification of potential outcome predictors in the regres-sion analyses in paper III and IV.
Ethical considerations Because anonymous screening of psychiatric disorders can evoke the neces-sity for psychiatric evaluation, all participants in paper I in the GP sample and within outpatient psychiatry were invited to contact a specialised unit for questions and assistance. The female inmates had access to health care facili-ties within the prison for the same purpose. In preparation for paper II, it was clearly stated in the application to the Ethics Committee that research on data from patient files is an ethically delicate matter and must be carefully considered based on the potential scientific outcome. To secure anonymity, all study data were decoded from individual patient information before anal-ysis. In paper III and IV, the principal ethical issue concerns evoking poten-tial memories and emotional reactions when addressing and contacting pa-tients who have undergone diagnostic procedures and long periods of treat-ment. Generally, most participants expressed gratitude for being contacted. Some participants conveyed a need for renewed medical contact and treat-ment, and accordingly, were assisted with referrals to psychiatric outpatient clinics in their residential area. Some of the participants had a need to ex-press opinions and share their experiences with the interviewer since being diagnosed with ADHD in adulthood. As many participants saw themselves as being among the first individuals in the country to be diagnosed with ADHD as adults, it was felt that many of the participants perceived them-selves as "pioneers", a fact that probably contributed to the high participation rate.
General discussion and clinical implications The principal aim of this thesis was to expand our understanding of ADHD by investigating prevalence, psychiatric comorbidity and long-term outcome and safety of pharmacological intervention in persons diagnosed with ADHD as adults.
46
Prevalence Our data confirm the high prevalence of ADHD-related symptoms associat-ed with increased difficulties and suffering, lower general functioning and increased frequencies of reading and spelling difficulties in outpatient psy-chiatry, regardless of sex. These findings were also observed in female pris-on inmates. No major sex differences were identified in outpatient psychiatry versus the GP. The high prevalence of reading difficulties in those with ADHD symptoms was not unexpected and concurs with the ESSENCE con-cept. Half of the female prison inmates reported symptoms of ADHD in childhood or as adults, and approximately 30 % reported inattention in childhood and symptoms of ADHD as adults. This is similar to the previous-ly mentioned meta-analysis with an average ADHD prevalence rate of 25.5 % in prison inmates [163]. High prevalence rates of ADHD in both patients and inmates prompt awareness of potential ADHD-related problems. Such awareness should be beneficial in attaining optimal treatment, care and reha-bilitation in patients who are in contact with outpatient psychiatry as well as prison establishments [62; 106]. Currently, the awareness of ADHD as an important factor for outcome in correctional treatment has increased substan-tially. In addition, treating inmates diagnosed with ADHD has demonstrated successful long-term outcome [63]. Finally, pharmacological treatment of patients with ADHD has been linked to lower criminality rates in both men and women compared with periods when patients are off medication [97].
Comorbidity In our clinical sample of patients diagnosed with ADHD in adulthood, 9 out of 10 patients had experienced at least one lifetime axis I disorder, and usu-ally in the form of a mood disorder. This supports a published observation of a genetic correlation of ADHD and bipolar disorder [147]. Thus, identifying and treating potential coexisting mood disorders is an important part of adult ADHD, especially as register data suggest that stimulant medication is relat-ed to a decreased risk of suicide [35]. Our data reveal few sex differences for an axis I disorder but confirm the results of previous studies in which mood and eating disorders were more frequent in females [117; 119] and SUD more common in males [20; 67; 117]. Accordingly, a recent study related to the ESSENCE concept performed on adults with ADHD, ASD, or both con-firmed that almost one fifth of the participants reported severely or moder-ately disturbed eating behaviour [79].
The relatively low prevalence of ongoing substance use in our material might be explained by compulsory drug screening and the request for drug abstinence during the evaluation period. Although ADHD has been demon-strated to be overrepresented in patients with SUD, a prospective study of twins has linked the risk of alcohol problems during adolescence to external-
47
ising behaviour rather than to core ADHD symptoms [113]. Moreover, pro-posed concerns of evoking SUD or provoking relapse of previous SUD by treating ADHD with classified drugs has not been confirmed [33; 112].
In our sample, ASD and Tourette’s syndrome greatly exceeded the preva-lence rates in the GP [16; 85]. Conversely, there is an increased risk for ADHD in patients with ASD and their relatives [57] suggesting a genetic overlap of the two disorders. This finding underscores the need to consider coexisting symptoms of ASD and tics when treating patients diagnosed with ADHD as adults.
Nearly half of the patients confirmed the specific criteria for one or more personality disorders but only one tenth was considered to fulfil a best esti-mate diagnosis. The low prevalence of personality disorders in the present study is probably explained by the restrictive methodology applied, separat-ing specific personality criteria from a best estimate diagnosis on axis II. The diagnostic overlap between personality disorder criteria and ADHD has not been sufficiently examined, especially in relation to cluster B disorders such as ASPD and BPD. Borderline development in ADHD has been reported to be related to certain environmental factors such as emotional abuse in child-hood [111]. To elucidate and explain the variable extent of emotional lability in ADHD, a gradient model of "cool" and "hot" executive functions with different neuroanatomical correlations has been proposed [109]. The former would be correlated to classical ADHD while the latter would be tied to anti-social and borderline functioning. In parallel, non-emotional and emotional processing would involve the basal ganglia with modulatory effects of the dopamine system. In all, this dual concept would be a model to stepwise integrate ADHD with emotional lability, ASPD and BPD.
The adult ADHD concept Recently, data from a small number of studies have raised the question of whether onset of ADHD could occur first in adulthood, an issue which would further complicate the diagnostic procedure insofar as symptom re-quirement before the age of 12 is still requested according to DSM-5 [4; 32; 49; 103]. Further studies are required to elucidate factors that influence age of symptom onset and phenotypic expression of ADHD. Genetic research is intense and several candidate genes have been proposed but still with limited success in detecting common genetic variants for the diagnostic phenotype of ADHD [26]. Accordingly, viewing ADHD as a dimensional rather than as a categorical construct, together with increases in study sample sizes, have been proposed for future genetic research [69]. In addition, to identify spe-cific genetic correlations and biological markers predicting pharmacological treatment response would be important to clinical practise. Polymorphism of catechol-O-methyltransferase (COMT) has been linked to treatment response to methylphenidate in children [81]. In adults, polymorphism in the gene

48
SLC6A3 has been reported to be associated to methylphenidate response [86].
Long-term outcome The principal outcome of the long-term follow-up is that one third of the patients first diagnosed with ADHD as adults went into remission during a mean observation period of six years. This result is consistent with findings of a recently published seven-year longitudinal study of adults with ADHD [78]. After being taken off medication and re-evaluated, one third of the latter patients did not maintain ADHD criteria and 12% were in full remis-sion. Another important finding in this thesis is that, despite a high percent-age of psychiatric comorbidity at baseline, adult ADHD in general seems to have a favourable long-term functional outcome as judged from the GAF scores at follow-up, which were similar to scores reported from the GP in paper I. Furthermore, the domain means on the SDS were below the cut-off for significant functional impairment when assessed at follow-up, and inde-pendent of ADHD remission. The EQ-5D index, a health status index related to HRQoL, was similar to population sample scores [30] in patients in remis-sion, but lower in those not. This finding must be given an interpretation with caution, however, because substantial variability was noted between individuals for these measures, indicating that some of the patients still per-ceived substantial impairment in disability and HRQoL. Altogether, the re-sults reflect the complexity of adult ADHD with all its nuances beyond core symptomatology when evaluating aspects of treatment and treatment out-come. A somewhat unexpected finding was that alcohol consumption (as measured by AUDIT) in patients with ADHD was similar to that in the GP. On the other hand, a DUDIT score which reflected any use of drugs was reported in 14% overall, and in 17% of non-remitters, which is higher than the 3% in the Swedish GP [19].
A noteworthy finding was that the remission rate and the ADHD scores were similar in patients currently undergoing treatment with central stimu-lants and in those not treated. Our data add to the present literature with presently no accepted evidence based on longitudinal assessments, suggest-ing that there are long-term benefits from medication in individuals first diagnosed with ADHD as adults [71] Moreover, a six-year follow-up study of participants with ADHD combined type in late adolescence and early adulthood found no effect of pharmacological treatment on either ADHD symptom severity or overall functioning despite an increasing rate of phar-macological treatment over time [148]. In addition to that, time on medica-tion did not predict persistence of ADHD in the previously mentioned study [71]. This finding is, however, in contrast with those from another recent study in adults with ADHD [95] which reported that 56% of the patients currently on medication were below a cut-off for ADHD after a mean obser-

49
vation time of 4.5 years compared with 34% of those without ongoing medi-cation, and also a better outcome on all measures in patients treated for two years or more compared with those given shorter pharmacological treatment.
Although patients who were currently on medication did not report better ADHD or SDS scores, they did report higher improvement as measured by the CGI-I scale. This result may suggest that there are medication-related improvements beyond core symptomatology of inattention and hyperactivi-ty/impulsivity. It is also possible that the patients’ ratings contain a placebo-related mechanism in the compliant patients as suggested and discussed in reference [73]. There may also be differences in patient characteristics that are not discerned, and also a variable amount and quality of psychoeduca-tional measures and information that may have affected the tendency to dis-continue medication. Psychiatric comorbidity at follow-up and data on the participants’ cognitive level and profile, which were not assessed by us, are also factors that could have influenced coping strategies and adherence to medication.
It is particularly noteworthy that no baseline factors predicted outcome six years after the patients were first diagnosed with ADHD in adulthood. This observation is discordant with studies showing that psychiatric comor-bidity at baseline is a negative prognostic factor [95; 78]. An explanation could be that comorbidities are registered and diagnosed differently in dif-ferent studies. Another issue can be that the primary outcome measure dif-fered between studies. It has been recommended that clinical research in ADHD should use remission as the primary outcome [133], which also was used in this study. Our paper defined remission as not fulfilling any ADHD subtype and a GAF value of ≥70 during the past year. Nevertheless, we also calculated persistence of symptoms as performed and defined by Biederman et al. [24] in the form of full or subthreshold ADHD based on the DSM-IV diagnostic criteria, or failure to attain functional remission (GAF score ≤60). Irrespective of how outcome was assessed there was no significant differ-ence between patients who were on current medication and those who were not (data not shown).
Pharmacological treatment Half of the medicated patients were still on medication at follow-up, which is consistent with previous data [17]. Most of these patients perceived a pro-nounced or moderate effect on their ADHD, with a mean stimulant dosage within recommended limits. Adherence to treatment was reported excellent in this group, both with respect to dosage and to regularity of intake. Self-reported adverse effects during treatment demonstrated a broad spectrum of symptoms of the sort reported in previous studies: the five most common complaints were decreased appetite, dry mouth, anxiousness, increased pulse frequency and decreased sexual desire [76; 121]. The results indicate the

50
importance of a wide and systematic evaluation of adverse effects when treating adults with ADHD. Most importantly, our data do not indicate that there is tolerance or a need for increased dosage over time to the preserve treatment effect, but rather the contrary. The reason for this could only be speculative, but possibly long-term medication creates "a window" that ena-bles and increases the possibility to profit by other non-medical interventions and treatments. Further research will likely increase our knowledge of fac-tors influencing the dose required for clinical effect over time. Nevertheless, this thesis confirms that the long-term pharmacological treatment of patients diagnosed with ADHD in adulthood, and who present a high degree of psy-chiatric comorbidity at the time of the diagnostic evaluation, is safe and tol-erable after a mean period of six years. Being based on a clinical sample with no exclusion criteria attached, the present results seem representative of a typical patient sample from an adult outpatient psychiatric clinic.
The other half of the participating patients had discontinued treatment at follow-up. This observation is similar to observations made in other long-term studies [17; 95]. We noticed a mean treatment time of two years in this group, suggesting that there had been sufficient time to evaluate treatment and to adjust dosage of the pharmaceuticals used to be in accordance with dosage used in everyday clinical practice. It also raises the question of whether the efficacy of treatment diminishes over time, or if, once again, the non-pharmacological interventions that run parallel with medication, affects the perceived need for pharmacological support. Furthermore, lack of effect was the most common cause for discontinuation. Only one patient discontin-ued methylphenidate and one amphetamine because they saw no need for further medication.
Notably, none of the patients who had reported elevated mood or hypo-mania had been diagnosed with a bipolar disorder at baseline, whereas those two who had been diagnosed with a bipolar disorder at baseline discontinued treatment because of depressed mood. This finding agrees with results of a report suggesting that comorbidity of bipolar disorders and ADHD is more frequently linked to depressive episodes than to manic episodes [125]. The necessity of treating patients who present with comorbid bipolar disorder and ADHD with mood stabilisers before stimulants has recently been demonstrated [152]. It can also be discussed whether some patients with SUD were offered optimal treatment in that data on patients with ADHD and SUD indicate that dosage in the higher range may increase adherence to treatment with methylphenidate [127].
Another important observation is that nearly one tenth of the participants had discontinued treatment because of the perceived inability to stay in con-tact with the prescribing physician. It cannot be ruled out that a change in the panorama of comorbidity over the six-year period may have influenced ad-herence to treatment as well as the reported adverse effects. Furthermore, differences in non-pharmacological treatment or supporting interventions

51
since baseline are potential factors that could have biased the results. Con-versely, combined data on pharmacological and non-pharmacological treat-ment have demonstrated medication to be superior in outcome (at least for one year) compared with supportive interventions and psychological treat-ment [110].
Finally, patients’ own perception was that of an increased QoL, an in-creased level of functioning and better understanding from the surroundings in those with ongoing medication. This observation must not be underesti-mated as an important feature of adult ADHD is the general effect of the disorder on both the patients and their family members.
Future aspects ADHD in adulthood may be a more complex diagnostic entity to evaluate and treat than in childhood as it is associated with a wider spectrum of comorbidity and also with secondary consequences of SUD and somatic conditions.
The role of epigenetics in ADHD is still relatively unknown but has slow-ly emerged over the past years. Taking this into account, ADHD in adult-hood often displays a heterogeneous clinical presentation with aspects to consider that go beyond the present categorical diagnostic system and core symptomatology of inattention and hyperactivity/impulsivity. Reports on possible adult onset of ADHD further complicates this issue. Future clinical studies of ADHD in adulthood therefore need a wide spectrum of approaches concerning genetics, diagnostics, treatment, and psychiatric as well as so-matic comorbidity. Not to mention the link between cognitive impairment and the clinical presentation and treatment outcome.
In the present study four persons had died of unnatural causes since diag-nosed with ADHD, which is in line with the perspective that ADHD is relat-ed to suicidal behaviour or other adverse health outcomes [105]. Key issues to investigate are to further assess whether such an association is the effect of comorbid psychiatric conditions, e.g. mood disorders and SUD, and if so, to what extent a comorbid ADHD only acts as a risk amplifier.
A key issue is that the characteristics of ADHD as such contain elements that affect adherence to structured treatment protocols negatively. Any treatment protocol that only reaches half of those in need is in vain for a substantial subgroup of patients. Research on how to organize care, and how to effectively reach patients with psychoeducational interventions and coach-ing in order to improve adherence to protocols is highly desired [107] The rapid technological development allows for new approaches in such psy-choeducational interventions and coaching. To date, some success has e.g. been reported for Internet-based interventions and coaching [151; 131].
52
Conclusions
• There is a high prevalence of ADHD-related symptoms associated with increased difficulties and suffering, lower general functioning and in-creased frequencies of reading and spelling difficulties in psychiatric outpatients, regardless of sex. These findings were also observed in fe-male prison inmates.
• There was a high prevalence of psychiatric comorbidity in both women and men diagnosed with ADHD as adults, with women more vulnerable to mood disorders and men more at risk for substance-use disorders.
• Patients diagnosed with ADHD as adults report diagnostic remission in about 3 of 10 cases after a mean period of six years, irrespective of on-going pharmacological treatment at follow-up, and despite a high per-centage of psychiatric comorbidity at baseline.
• Long-term pharmacological treatment (mainly with stimulants) of adults with ADHD is safe with generally mild and tolerable adverse effects. The discontinuation rate of about 50%, with almost a third of which due to perceived lack of effect of methylphenidate, suggests that close sur-veillance and a strategy to change drugs, drug combinations and dosages should be assessed as a way to increase retention to treatment. Long-term data do not indicate tolerance or a need for increased dosage over time to preserve the treatment effect, but rather the contrary.
53
Acknowledgements
I would like to express my gratitude to all those who assisted me in the prac-tical arrangements to make the respective studies, and finally the thesis, pos-sible. I am particularly grateful to: Lisa Ekselius, professor of psychiatry and my main supervisor, who "inherit-ed" me as a PhD-student. I am most grateful to her for accepting the role as my main supervisor. Without her this thesis would not have been possible. She has always been available, encouraging, supporting and demanding in the best possible way. I have especially appreciated her ability to swiftly observe and focus on essential matters in this project which on many occa-sions prevented me from losing track. Apart from a broad experience of clin-ical psychiatry and research in general, her keen interest in and knowledge of personality disorders, have been particularly stimulating in our discussions during this project. Tommy Lewander, associate professor of psychiatry, my co-supervisor, for his accuracy in discussions, analyses and reviews of data, papers and manu-scripts. Lena Malmlöv Karlsson, RN and clinical collaborator, with admiration and gratefulness for invaluable contribution in performing clinical interviews and for impeccable logistics. Eva Lindström, associate professor of psychiatry, my initial main supervisor, for support and with admiration of her brightness in clinical psychiatric evaluations. Kerstin (Chris) Bingefors, PhD, lecturer, my co-supervisor, for her valuable support on statistics and reviews of data. Frits-Axel Wiesel, late professor of psychiatry and my previous senior su-pervisor, who was the first to “inherit me” as a PhD-student and who gave me generous support during a short period of time.
54
Ann-Mari Ahl, social worker and clinical collaborator. I am admired by ac-curate clinical work and relevant, distinct and systematic documentation in the patient files. Hans Arinell, BA, for excellent statistical support. Caisa Öster, RN, associate professor and lecturer and Josefin Bäckström, RN, PhD and lecturer, for their valuable support with various practical and theoretical issues including encouraging discussions at coffee breaks. Ann-Charlotte Åslund, secretary at Uppsala University Hospital Department of Psychiatry, together with Lottie Söder, Lena Bohlin and Ann-Charlotte Fält, secretaries at the Department of Neuroscience, for never ending will-ingness to assist with various practical issues. Ing-Marie Wieselgren, Åsa Hagberg, Björn Milesson Fors, Gunilla Svedström and Tarja-Leena Kirvesniemi, my clinical superiors over the years at Uppsala University Hospital, for encouragement of clinical reseach and priorites of time for research. Ulf Durling, legendary criminal author and senior consultant in psychiatry, for persuading me to become a psychiatrist. You are the still my role model in everyday clinical practise. And finally, to my mother Elisabeth and brother Björn. I am proud of you both. This project has been supported by grants from the Uppsala County Council, The Märta and Nicke Nasvell Foundation and The Bror Gadelius Founda-tion.
55
References
1 Adler L, Tanaka Y, Williams D, Trzepacz PT, Goto T, et al. Executive function in adults with attention-deficit/hyperactivity disorder during treatment with atomoxetine in a randomized, placebo-controlled, withdrawal study. J Clin Psychopharmacol 2014;34: 461-6.
2 Adler LA, Faraone SV, Spencer TJ, Michelson D, Reimherr FW, et al. The reliability and validity of self- and investigator ratings of ADHD in adults. J Atten Disord 2008;11: 711-9.
3 Adler LA, Spencer T, McGough JJ, Jiang H, Muniz R. Long-term effectiveness and safety of dexmethylphenidate extended-release capsules in adult ADHD. J Atten Disord 2009;12: 449-59.
4 Agnew-Blais JC, Polanczyk GV, Danese A, Wertz J, Moffitt TE, et al. Evaluation of the Persistence, Remission, and Emergence of Attention-Deficit/Hyperactivity Disorder in Young Adulthood. JAMA Psychiatry 2016;73: 713-20.
5 American Psychiatric Association. Diagnostic and statistical manual of mental disorders (2nd ed.). Washington DC. 1968;
6 American Psychiatric Association. Diagnostic and statistical manual of mental disorders (3rd ed.). Washington DC. 1980;
7 American Psychiatric Association. Diagnostic and statistical manual of mental disorders (3rd ed., rev.). Washington DC. 1987;
8 American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed.). Washington DC. 1994;
9 American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed. text revision). Washington DC. 2000;
10 American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Washington DC. 2013;
11 Angold A, Erkanli A, Egger HL, Costello EJ. Stimulant treatment for children: a community perspective. J Am Acad Child Adolesc Psychiatry 2000;39: 975-84; discussion 84-94.
12 Arnsten AF. Catecholamine influences on dorsolateral prefrontal cortical networks. Biol Psychiatry 2011;69: e89-99.
13 Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. AUDIT. The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care. . Second. ed: World Health Organization. Department of Mental Health and Substance Dependence., 2001.
56
14 Barkley RA. The relevance of the still lectures to attention-deficit/hyperactivity disorder: a commentary. J Atten Disord 2006;10: 137-40.
15 Barkley RA, Peters H. The earliest reference to ADHD in the medical literature? Melchior Adam Weikard's description in 1775 of "attention deficit" (Mangel der Aufmerksamkeit, Attentio Volubilis). J Atten Disord 2012;16: 623-30.
16 Baron-Cohen S, Scott FJ, Allison C, Williams J, Bolton P, et al. Prevalence of autism-spectrum conditions: UK school-based population study. Br J Psychiatry 2009;194: 500-9.
17 Bejerot S, Ryden EM, Arlinde CM. Two-year outcome of treatment with central stimulant medication in adult attention-deficit/hyperactivity disorder: a prospective study. J Clin Psychiatry 2010;71: 1590-7.
18 Bergman P, Ahlberg G, Forsell Y, Lundberg I. Non-participation in the second wave of the PART study on mental disorder and its effects on risk estimates. Int J Soc Psychiatry 2010;56: 119-32.
19 Berman AH, Bergman H, Palmstierna T, Schlyter F. Evaluation of the Drug Use Disorders Identification Test (DUDIT) in criminal justice and detoxification settings and in a Swedish population sample. European addiction research 2005;11: 22-31.
20 Biederman J, Faraone SV, Monuteaux MC, Bober M, Cadogen E. Gender effects on attention-deficit/hyperactivity disorder in adults, revisited. Biol Psychiatry 2004;55: 692-700.
21 Biederman J, Mick E, Faraone SV. Age-dependent decline of symptoms of attention deficit hyperactivity disorder: impact of remission definition and symptom type. Am J Psychiatry 2000;157: 816-8.
22 Biederman J, Mick E, Faraone SV, Braaten E, Doyle A, et al. Influence of gender on attention deficit hyperactivity disorder in children referred to a psychiatric clinic. Am J Psychiatry 2002;159: 36-42.
23 Biederman J, Mick E, Surman C, Doyle R, Hammerness P, et al. A randomized, 3-phase, 34-week, double-blind, long-term efficacy study of osmotic-release oral system-methylphenidate in adults with attention-deficit/hyperactivity disorder. J Clin Psychopharmacol 2010;30: 549-53.
24 Biederman J, Petty CR, Evans M, Small J, Faraone SV. How persistent is ADHD? A controlled 10-year follow-up study of boys with ADHD. Psychiatry Res 2010;177: 299-304.
25 Bodlund O, Kullgren G, Ekselius L, Lindstrom E, von Knorring L. Axis V--Global Assessment of Functioning Scale. Evaluation of a self-report version. Acta Psychiatrica Scandinavica 1994;90: 342-7.
26 Bonvicini C, Faraone SV, Scassellati C. Attention-deficit hyperactivity disorder in adults: A systematic review and meta-
57
analysis of genetic, pharmacogenetic and biochemical studies. Mol Psychiatry 2016;21: 872-84.
27 Brevik EJ, Lundervold AJ, Halmoy A, Posserud MB, Instanes JT, et al. Prevalence and clinical correlates of insomnia in adults with attention-deficit hyperactivity disorder. Acta Psychiatr Scand 2017;136: 220-27.
28 Brook U, Boaz M. Attention deficit and hyperactivity disorder (ADHD) and learning disabilities (LD): adolescents perspective. Patient Educ Couns 2005;58: 187-91.
29 Buitelaar JK, Trott GE, Hofecker M, Waechter S, Berwaerts J, et al. Long-term efficacy and safety outcomes with OROS-MPH in adults with ADHD. Int J Neuropsychopharmacol 2012;15: 1-13.
30 Burstrom K, Johannesson M, Diderichsen F. Swedish population health-related quality of life results using the EQ-5D. Quality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation 2001;10: 621-35.
31 Castellanos FX, Lee PP, Sharp W, Jeffries NO, Greenstein DK, et al. Developmental trajectories of brain volume abnormalities in children and adolescents with attention-deficit/hyperactivity disorder. JAMA 2002;288: 1740-8.
32 Caye A, Spadini AV, Karam RG, Grevet EH, Rovaris DL, et al. Predictors of persistence of ADHD into adulthood: a systematic review of the literature and meta-analysis. Eur Child Adolesc Psychiatry 2016;25: 1151-59.
33 Chang Z, Lichtenstein P, Halldner L, D'Onofrio B, Serlachius E, et al. Stimulant ADHD medication and risk for substance abuse. J Child Psychol Psychiatry 2014;55: 878-85.
34 Chang Z, Quinn PD, Hur K, Gibbons RD, Sjolander A, et al. Association Between Medication Use for Attention-Deficit/Hyperactivity Disorder and Risk of Motor Vehicle Crashes. JAMA Psychiatry 2017;74: 597-603.
35 Chen Q, Sjolander A, Runeson B, D'Onofrio BM, Lichtenstein P, et al. Drug treatment for attention-deficit/hyperactivity disorder and suicidal behaviour: register based study. BMJ 2014;348: g3769.
36 Choi BC, Pak AW. A catalog of biases in questionnaires. Prev Chronic Dis 2005;2: A13.
37 Chu SM, Tsai MH, Hwang FM, Hsu JF, Huang HR, et al. The relationship between attention deficit hyperactivity disorder and premature infants in Taiwanese: a case control study. BMC Psychiatry 2012;12: 85.
38 Clements SD, Peters JE. Minimal brain dysfunctions in the school-age child. Diagnosis and treatment. Arch Gen Psychiatry 1962;6: 185-97.
39 Coles T, Coon C, DeMuro C, McLeod L, Gnanasakthy A. Psychometric evaluation of the Sheehan Disability Scale in adult
58
patients with attention-deficit/hyperactivity disorder. Neuropsychiatric disease and treatment 2014;10: 887-95.
40 Coogan AN, McGowan NM. A systematic review of circadian function, chronotype and chronotherapy in attention deficit hyperactivity disorder. Atten Defic Hyperact Disord 2017;
41 Crichton A. An inquiry into the nature and origin of mental derangement : comprehending a concise system of the physiology and pathology of the human mind, and a history of the passions and their effects. London, UK.: T. Cadell, junior and W. Davies, 1798.
42 Cumyn L, French L, Hechtman L. Comorbidity in adults with attention-deficit hyperactivity disorder. Can J Psychiatry 2009;54: 673-83.
43 de Zeeuw P, Zwart F, Schrama R, van Engeland H, Durston S. Prenatal exposure to cigarette smoke or alcohol and cerebellum volume in attention-deficit/hyperactivity disorder and typical development. Transl Psychiatry 2012;2: e84.
44 Dolan P. Modeling valuations for EuroQol health states. Medical care 1997;35: 1095-108.
45 Dykman RA, Ackerman PT. Attention deficit disorder and specific reading disability: separate but often overlapping disorders. J Learn Disabil 1991;24: 96-103.
46 Dyster-Aas J, Willebrand M, Wikehult B, Gerdin B, Ekselius L. Major depression and posttraumatic stress disorder symptoms following severe burn injury in relation to lifetime psychiatric morbidity. J Trauma 2008;64: 1349-56.
47 Epstein JN, Johnson, D., & Conners, C. K. . Conners’ Adult ADHD Diagnostic Interview for DSM-IV North Tonawanda, NY: Multi-Health Systems, Inc., 2000.
48 Epstein JN, Kollins SH. Psychometric properties of an adult ADHD diagnostic interview. J Atten Disord 2006;9: 504-14.
49 Faraone SV, Biederman J. Can Attention-Deficit/Hyperactivity Disorder Onset Occur in Adulthood? JAMA Psychiatry 2016;73: 655-6.
50 Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med 2006;36: 159-65.
51 Fayyad J, De Graaf R, Kessler R, Alonso J, Angermeyer M, et al. Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. The British journal of psychiatry : the journal of mental science 2007;190: 402-9.
52 Ferguson CJ. The influence of television and video game use on attention and school problems: a multivariate analysis with other risk factors controlled. J Psychiatr Res 2011;45: 808-13.
53 First MB, Gibbon M, Spitzer RL, Williams JBW, Benjamin LS. Structured Clinical Interview for DSM-IV Axis II Personality
59
Disorders (SCID-II). Washington, DC.: American Psychiatric Press, Inc. 1997;
54 First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for DSM-IV axis I Disorders, Clinical Version (SCID-CV). . Washington, DC.: American Psychiatric Press, Inc. 1996;
55 Fredriksen M, Dahl AA, Martinsen EW, Klungsoyr O, Haavik J, et al. Effectiveness of one-year pharmacological treatment of adult attention-deficit/hyperactivity disorder (ADHD): an open-label prospective study of time in treatment, dose, side-effects and comorbidity. Eur Neuropsychopharmacol 2014;24: 1873-84.
56 Gamo NJ, Wang M, Arnsten AF. Methylphenidate and atomoxetine enhance prefrontal function through alpha2-adrenergic and dopamine D1 receptors. J Am Acad Child Adolesc Psychiatry 2010;49: 1011-23.
57 Ghirardi L, Brikell I, Kuja-Halkola R, Freitag CM, Franke B, et al. The familial co-aggregation of ASD and ADHD: a register-based cohort study. Mol Psychiatry 2017;
58 Gillberg C. Deficits in attention, motor control and perception: follow-up from pre-school to early teens. Thesis. Uppsala University 1987;
59 Gillberg C. The ESSENCE in child psychiatry: Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examinations. Res Dev Disabil 2010;31: 1543-51.
60 Gillberg C, Rasmussen P. Perceptual, motor and attentional deficits in seven-year-old children: background factors. Dev Med Child Neurol 1982;24: 752-70.
61 Ginsberg Y, Arngrim T, Philipsen A, Gandhi P, Chen CW, et al. Long-term (1 year) safety and efficacy of methylphenidate modified-release long-acting formulation (MPH-LA) in adults with attention-deficit hyperactivity disorder: a 26-week, flexible-dose, open-label extension to a 40-week, double-blind, randomised, placebo-controlled core study. CNS Drugs 2014;28: 951-62.
62 Ginsberg Y, Hirvikoski T, Lindefors N. Attention Deficit Hyperactivity Disorder (ADHD) among longer-term prison inmates is a prevalent, persistent and disabling disorder. BMC Psychiatry 2010;10: 112.
63 Ginsberg Y, Langstrom N, Larsson H, Lindefors N. Long-Term Treatment Outcome in Adult Male Prisoners With Attention-Deficit/Hyperactivity Disorder: Three-Year Naturalistic Follow-Up of a 52-Week Methylphenidate Trial. J Clin Psychopharmacol 2015;35: 535-43.
64 Ginsberg Y, Lindefors N. Methylphenidate treatment of adult male prison inmates with attention-deficit hyperactivity disorder: randomised double-blind placebo-controlled trial with open-label extension. Br J Psychiatry 2012;200: 68-73.
65 Grizenko N, Eberle ML, Fortier ME, Cote-Corriveau G, Jolicoeur C, et al. Apgar Scores Are Associated with Attention-
60
Deficit/Hyperactivity Disorder Symptom Severity. Can J Psychiatry 2016;61: 283-90.
66 Guy W. ECDEU assessment Manual for Psychpharmacology.: Rockville, MD, USA: US Department of Health, Education and Welfare, 1976.
67 Halmoy A, Fasmer OB, Gillberg C, Haavik J. Occupational outcome in adult ADHD: impact of symptom profile, comorbid psychiatric problems, and treatment: a cross-sectional study of 414 clinically diagnosed adult ADHD patients. J Atten Disord 2009;13: 175-87.
68 Hammerness PG, Karampahtsis C, Babalola R, Alexander ME. Attention-deficit/hyperactivity disorder treatment: what are the long-term cardiovascular risks? Expert Opin Drug Saf 2015;14: 543-51.
69 Hawi Z, Cummins TD, Tong J, Johnson B, Lau R, et al. The molecular genetic architecture of attention deficit hyperactivity disorder. Mol Psychiatry 2015;20: 289-97.
70 Hechtman L, Swanson JM, Sibley MH, Stehli A, Owens EB, et al. Functional Adult Outcomes 16 Years After Childhood Diagnosis of Attention-Deficit/Hyperactivity Disorder: MTA Results. J Am Acad Child Adolesc Psychiatry 2016;55: 945-52 e2.
71 Hinshaw SP, Arnold LE, MTA Cooperative Group. Attention-deficit hyperactivity disorder, multimodal treatment, and longitudinal outcome: evidence, paradox, and challenge. Wiley Interdiscip Rev Cogn Sci 2015;6: 39-52.
72 Hoffmann H. Lustige Geschichten und drollige Bilder (English: Funny stories and droll pictures). Frankfurt a. M, Germany: Literarische Anstalt (J. Rütten) 1845.
73 Horwitz RI, Horwitz SM. Adherence to treatment and health outcomes. Arch Intern Med 1993;153: 1863-8.
74 Hult N, Kadesjo J, Kadesjo B, Gillberg C, Billstedt E. ADHD and the QbTest: Diagnostic Validity of QbTest. J Atten Disord 2015;
75 Hultman CM, Torrang A, Tuvblad C, Cnattingius S, Larsson JO, et al. Birth weight and attention-deficit/hyperactivity symptoms in childhood and early adolescence: a prospective Swedish twin study. J Am Acad Child Adolesc Psychiatry 2007;46: 370-7.
76 Huss M, Ginsberg Y, Tvedten T, Arngrim T, Philipsen A, et al. Methylphenidate hydrochloride modified-release in adults with attention deficit hyperactivity disorder: a randomized double-blind placebo-controlled trial. Adv Ther 2014;31: 44-65.
77 Kadesjo B, Janols LO, Korkman M, Mickelsson K, Strand G, et al. The FTF (Five to Fifteen): the development of a parent questionnaire for the assessment of ADHD and comorbid conditions. Eur Child Adolesc Psychiatry 2004;13 Suppl 3: 3-13.
78 Karam RG, Breda V, Picon FA, Rovaris DL, Victor MM, et al. Persistence and remission of ADHD during adulthood: a 7-year clinical follow-up study. Psychol Med 2015;45: 2045-56.
61
79 Karjalainen L, Gillberg C, Rastam M, Wentz E. Eating disorders and eating pathology in young adult and adult patients with ESSENCE. Compr Psychiatry 2016;66: 79-86.
80 Kennedy M, Kreppner J, Knights N, Kumsta R, Maughan B, et al. Early severe institutional deprivation is associated with a persistent variant of adult attention-deficit/hyperactivity disorder: clinical presentation, developmental continuities and life circumstances in the English and Romanian Adoptees study. J Child Psychol Psychiatry 2016;57: 1113-25.
81 Kereszturi E, Tarnok Z, Bognar E, Lakatos K, Farkas L, et al. Catechol-O-methyltransferase Val158Met polymorphism is associated with methylphenidate response in ADHD children. Am J Med Genet B Neuropsychiatr Genet 2008;147B: 1431-5.
82 Kessler RC, Adler L, Ames M, Demler O, Faraone S, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med 2005;35: 245-56.
83 Kessler RC, Adler L, Barkley R, Biederman J, Conners CK, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psychiatry 2006;163: 716-23.
84 Kessler RC, Adler LA, Barkley R, Biederman J, Conners CK, et al. Patterns and predictors of attention-deficit/hyperactivity disorder persistence into adulthood: results from the national comorbidity survey replication. Biol Psychiatry 2005;57: 1442-51.
85 Khalifa N, von Knorring AL. Psychopathology in a Swedish population of school children with tic disorders. J Am Acad Child Adolesc Psychiatry 2006;45: 1346-53.
86 Kooij JS, Boonstra AM, Vermeulen SH, Heister AG, Burger H, et al. Response to methylphenidate in adults with ADHD is associated with a polymorphism in SLC6A3 (DAT1). Am J Med Genet B Neuropsychiatr Genet 2008;147B: 201-8.
87 Kooij SJ, Bejerot S, Blackwell A, Caci H, Casas-Brugue M, et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD. BMC Psychiatry 2010;10: 67.
88 Köster I SI, Döpfner M, Adam C, Ihle P, Lehmkuhl G. Children and adolescents with hyperkinetic disorder. Frequency of the claims diagnosis in primary care based on the data of a regional Statutory Health Insurance Sample--Versichertenstichprobe AOK Hessen/KV Hessen (1998-2001). Z Kinder Jugendpsychiatr Psychother 2004;32: 157-66.
89 Larson K, Russ SA, Kahn RS, Halfon N. Patterns of comorbidity, functioning, and service use for US children with ADHD, 2007. Pediatrics 2011;127: 462-70.
62
90 Larsson H, Lichtenstein P, Larsson JO. Genetic contributions to the development of ADHD subtypes from childhood to adolescence. J Am Acad Child Adolesc Psychiatry 2006;45: 973-81.
91 Le Couteur A, Rutter M, Lord C, Rios P, Robertson S, et al. Autism diagnostic interview: a standardized investigator-based instrument. J Autism Dev Disord 1989;19: 363-87.
92 Leckman JF, Sholomskas D, Thompson WD, Belanger A, Weissman MM. Best estimate of lifetime psychiatric diagnosis: a methodological study. Archives of general psychiatry 1982;39: 879-83.
93 Lee DY, Lee CS, Park CS, Kim BJ, Cha BS, et al. Effect of symptoms of adult attention deficit hyperactivity disorder on symptoms of post traumatic stress disorder in Korean conscripts. Psychiatry Investig 2012;9: 154-60.
94 Leekam SR, Libby SJ, Wing L, Gould J, Taylor C. The Diagnostic Interview for Social and Communication Disorders: algorithms for ICD-10 childhood autism and Wing and Gould autistic spectrum disorder. J Child Psychol Psychiatry 2002;43: 327-42.
95 Lensing MB, Zeiner P, Sandvik L, Opjordsmoen S. Four-year outcome in psychopharmacologically treated adults with attention-deficit/hyperactivity disorder: a questionnaire survey. J Clin Psychiatry 2013;74: e87-93.
96 Leon AC, Olfson M, Portera L, Farber L, Sheehan DV. Assessing psychiatric impairment in primary care with the Sheehan Disability Scale. International journal of psychiatry in medicine 1997;27: 93-105.
97 Lichtenstein P, Halldner L, Zetterqvist J, Sjolander A, Serlachius E, et al. Medication for attention deficit-hyperactivity disorder and criminality. N Engl J Med 2012;367: 2006-14.
98 Läkemedelsverket. Läkemedel vid ADHD - behandlingsrekommendation. Information från Läkemedelsverket 2016;27: 13-55.
99 Mayes SD, Calhoun SL, Crowell EW. Learning disabilities and ADHD: overlapping spectrumn disorders. J Learn Disabil 2000;33: 417-24.
100 McCann BS, Scheele L, Ward N, Roy-Byrne P. Discriminant validity of the Wender Utah Rating Scale for attention-deficit/hyperactivity disorder in adults. J Neuropsychiatry Clin Neurosci 2000;12: 240-5.
101 Miller TW, Nigg JT, Faraone SV. Axis I and II comorbidity in adults with ADHD. J Abnorm Psychol 2007;116: 519-28.
102 Moffitt TE, Caspi A, Taylor A, Kokaua J, Milne BJ, et al. How common are common mental disorders? Evidence that lifetime prevalence rates are doubled by prospective versus retrospective ascertainment. Psychol Med 2010;40: 899-909.
103 Moffitt TE, Houts R, Asherson P, Belsky DW, Corcoran DL, et al. Is Adult ADHD a Childhood-Onset Neurodevelopmental Disorder?
63
Evidence From a Four-Decade Longitudinal Cohort Study. Am J Psychiatry 2015;172: 967-77.
104 Nigg JT. Future directions in ADHD etiology research. J Clin Child Adolesc Psychol 2012;41: 524-33.
105 Nigg JT. Attention-deficit/hyperactivity disorder and adverse health outcomes. Clin Psychol Rev 2013;33: 215-28.
106 Nylander L, Holmqvist M, Gustafson L, Gillberg C. ADHD in adult psychiatry. Minimum rates and clinical presentation in general psychiatry outpatients. Nord J Psychiatry 2009;63: 64-71.
107 Osterberg L, Blaschke T. Adherence to medication. N Engl J Med 2005;353: 487-97.
108 Ottosson H, Bodlund O, Ekselius L, Grann M, von Knorring L, et al. DSM-IV and ICD-10 personality disorders: a comparison of a self-report questionnaire (DIP-Q) with a structured interview. Eur Psychiatry 1998;13: 246-53.
109 Petrovic P, Castellanos FX. Top-Down Dysregulation-From ADHD to Emotional Instability. Front Behav Neurosci 2016;10: 70 doi: 10.3389/fnbeh.2016.00070.
110 Philipsen A, Jans T, Graf E, Matthies S, Borel P, et al. Effects of Group Psychotherapy, Individual Counseling, Methylphenidate, and Placebo in the Treatment of Adult Attention-Deficit/Hyperactivity Disorder: A Randomized Clinical Trial. JAMA Psychiatry 2015;72: 1199-210.
111 Philipsen A, Limberger MF, Lieb K, Feige B, Kleindienst N, et al. Attention-deficit hyperactivity disorder as a potentially aggravating factor in borderline personality disorder. Br J Psychiatry 2008;192: 118-23.
112 Quinn PD, Chang Z, Hur K, Gibbons RD, Lahey BB, et al. ADHD Medication and Substance-Related Problems. Am J Psychiatry 2017;epub ahead of print appiajp201716060686: appiajp201716060686.
113 Quinn PD, Pettersson E, Lundstrom S, Anckarsater H, Langstrom N, et al. Childhood attention-deficit/hyperactivity disorder symptoms and the development of adolescent alcohol problems: A prospective, population-based study of Swedish twins. Am J Med Genet B Neuropsychiatr Genet 2016;171: 958-70.
114 Ramirez A, Ekselius L, Ramklint M. Axis V - Global Assessment of Functioning scale (GAF), further evaluation of the self-report version. European psychiatry : the journal of the Association of European Psychiatrists 2008;23: 575-9.
115 Ramos-Quiroga JA, Nasillo V, Richarte V, Corrales M, Palma F, et al. Criteria and Concurrent Validity of DIVA 2.0: A Semi-Structured Diagnostic Interview for Adult ADHD. J Atten Disord 2016;
64
116 Rasmussen K, Almvik R, Levander S. Attention deficit hyperactivity disorder, reading disability, and personality disorders in a prison population. J Am Acad Psychiatry Law 2001;29: 186-93.
117 Rasmussen K, Levander S. Untreated ADHD in adults: are there sex differences in symptoms, comorbidity, and impairment? J Atten Disord 2009;12: 353-60.
118 Reimherr FW, Marchant BK, Gift TE, Steans TA, Wender PH. Types of adult attention-deficit hyperactivity disorder (ADHD): baseline characteristics, initial response, and long-term response to treatment with methylphenidate. Atten Defic Hyperact Disord 2015;7: 115-28.
119 Robison RJ, Reimherr FW, Marchant BK, Faraone SV, Adler LA, et al. Gender differences in 2 clinical trials of adults with attention-deficit/hyperactivity disorder: a retrospective data analysis. J Clin Psychiatry 2008;69: 213-21.
120 Rosler M, Retz W, Retz-Junginger P, Hengesch G, Schneider M, et al. Prevalence of attention deficit-/hyperactivity disorder (ADHD) and comorbid disorders in young male prison inmates. Eur Arch Psychiatry Clin Neurosci 2004;254: 365-71.
121 Rosler M, Retz W, Yaqoobi K, Burg E, Retz-Junginger P. Attention deficit/hyperactivity disorder in female offenders: prevalence, psychiatric comorbidity and psychosocial implications. Eur Arch Psychiatry Clin Neurosci 2009;259: 98-105.
122 Rubia K, Halari R, Mohammad AM, Taylor E, Brammer M. Methylphenidate normalizes frontocingulate underactivation during error processing in attention-deficit/hyperactivity disorder. Biol Psychiatry 2011;70: 255-62.
123 Rucklidge JJ, Frampton CM, Gorman B, Boggis A. Vitamin-mineral treatment of attention-deficit hyperactivity disorder in adults: double-blind randomised placebo-controlled trial. Br J Psychiatry 2014;204: 306-15.
124 Rucklidge JJ, Tannock R. Validity of the Brown ADD scales: an investigation in a predominantly inattentive ADHD adolescent sample with and without reading disabilities. J Atten Disord 2002;5: 155-64.
125 Ryden E, Thase ME, Straht D, Aberg-Wistedt A, Bejerot S, et al. A history of childhood attention-deficit hyperactivity disorder (ADHD) impacts clinical outcome in adult bipolar patients regardless of current ADHD. Acta Psychiatr Scand 2009;120: 239-46.
126 Seidman LJ, Valera EM, Makris N. Structural brain imaging of attention-deficit/hyperactivity disorder. Biol Psychiatry 2005;57: 1263-72.
127 Skoglund C, Brandt L, Almqvist C, D'Onofrio BM, Konstenius M, et al. Factors Associated With Adherence to Methylphenidate Treatment in Adult Patients With Attention-Deficit/Hyperactivity Disorder and Substance Use Disorders. J Clin Psychopharmacol 2016;36: 222-8.
65
128 Snitselaar MA, Smits MG, Spijker J. Prevalence of Restless Legs Syndrome in Adult ADHD and Its Subtypes. Behav Sleep Med 2016;14: 480-8.
129 Snitselaar MA, Smits MG, van der Heijden KB, Spijker J. Sleep and Circadian Rhythmicity in Adult ADHD and the Effect of Stimulants. J Atten Disord 2017;21: 14-26.
130 Sobanski E, Bruggemann D, Alm B, Kern S, Deschner M, et al. Psychiatric comorbidity and functional impairment in a clinically referred sample of adults with attention-deficit/hyperactivity disorder (ADHD). Eur Arch Psychiatry Clin Neurosci 2007;257: 371-7.
131 Soderqvist H, Kajsa E, Ahlstrom BH, Wentz E. The caregivers' perspectives of burden before and after an internet-based intervention of young persons with ADHD or autism spectrum disorder. Scand J Occup Ther 2017;24: 383-92.
132 Sprafkin J, Gadow KD, Weiss MD, Schneider J, Nolan EE. Psychiatric comorbidity in ADHD symptom subtypes in clinic and community adults. J Atten Disord 2007;11: 114-24.
133 Steele M, Jensen PS, Quinn DM. Remission versus response as the goal of therapy in ADHD: a new standard for the field? Clin Ther 2006;28: 1892-908.
134 Stevenson J, Pennington BF, Gilger JW, DeFries JC, Gillis JJ. Hyperactivity and spelling disability: testing for shared genetic aetiology. J Child Psychol Psychiatry 1993;34: 1137-52.
135 Still GF. The Goulstonian lectures On some abnormal psychical conditions in children. Lancet 1902;159: 1008-12, 77-82, 163-68.
136 Still GF. Some abnormal psychical conditions in children: excerpts from three lectures. J Atten Disord 2006;10: 126-36.
137 Strauss AA, Lehtinen LE. Psychopathology and education of the brain-injured child. New York: Grune and Stratton, 1947.
138 Swanson CJ, Perry KW, Koch-Krueger S, Katner J, Svensson KA, et al. Effect of the attention deficit/hyperactivity disorder drug atomoxetine on extracellular concentrations of norepinephrine and dopamine in several brain regions of the rat. Neuropharmacology 2006;50: 755-60.
139 Swanson JM, Arnold LE, Molina BSG, Sibley MH, Hechtman LT, et al. Young adult outcomes in the follow-up of the multimodal treatment study of attention-deficit/hyperactivity disorder: symptom persistence, source discrepancy, and height suppression. J Child Psychol Psychiatry 2017;58: 663-78.
140 Swing EL, Gentile DA, Anderson CA, Walsh DA. Television and video game exposure and the development of attention problems. Pediatrics 2010;126: 214-21.
141 The British Psychological Society and The Royal College of Psychiatrists. NICE. Attention Deficit Hyperactivity Disorder: The
66
NICE guideline on diagnosis and managment of ADHD in children, young people and adults. 2008.
142 The EuroQol Group. EuroQol - a new facility for the measurement ofhealth-related quality of life. Health Policy 1990;16: 199-208.
143 The MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. . Arch Gen Psychiatry 1999;56: 1073-86.
144 Thompson T, Lloyd A, Joseph A, Weiss M. The Weiss Functional Impairment Rating Scale-Parent Form for assessing ADHD: evaluating diagnostic accuracy and determining optimal thresholds using ROC analysis. Qual Life Res 2017;26: 1879-85.
145 van de Glind G, van den Brink W, Koeter MW, Carpentier PJ, van Emmerik-van Oortmerssen K, et al. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend 2013;132: 587-96.
146 van Emmerik-van Oortmerssen K, van de Glind G, van den Brink W, Smit F, Crunelle CL, et al. Prevalence of attention-deficit hyperactivity disorder in substance use disorder patients: a meta-analysis and meta-regression analysis. Drug Alcohol Depend 2012;122: 11-9.
147 van Hulzen KJ, Scholz CJ, Franke B, Ripke S, Klein M, et al. Genetic Overlap Between Attention-Deficit/Hyperactivity Disorder and Bipolar Disorder: Evidence From Genome-wide Association Study Meta-analysis. Biol Psychiatry 2016;epub. http://dx.doi.org/10.1016/j.biopsych.2016.08.040
148 van Lieshout M, Luman M, Twisk JW, van Ewijk H, Groenman AP, et al. A 6-year follow-up of a large European cohort of children with attention-deficit/hyperactivity disorder-combined subtype: outcomes in late adolescence and young adulthood. Eur Child Adolesc Psychiatry 2016;25: 1007-17.
149 Weisler R, Young J, Mattingly G, Gao J, Squires L, et al. Long-term safety and effectiveness of lisdexamfetamine dimesylate in adults with attention-deficit/ hyperactivity disorder. CNS Spectr 2009;14: 573-85.
150 Wender PH, Reimherr FW, Marchant BK, Sanford ME, Czajkowski LA, et al. A one year trial of methylphenidate in the treatment of ADHD. J Atten Disord 2011;15: 36-45.
151 Wentz E, Nyden A, Krevers B. Development of an internet-based support and coaching model for adolescents and young adults with ADHD and autism spectrum disorders: a pilot study. Eur Child Adolesc Psychiatry 2012;21: 611-22.
152 Viktorin A, Ryden E, Thase ME, Chang Z, Lundholm C, et al. The Risk of Treatment-Emergent Mania With Methylphenidate in Bipolar Disorder. Am J Psychiatry 2017;174: 341-48.
67
153 Wilens TE, Biederman J, Faraone SV, Martelon M, Westerberg D, et al. Presenting ADHD symptoms, subtypes, and comorbid disorders in clinically referred adults with ADHD. J Clin Psychiatry 2009;70: 1557-62.
154 Williamson D, Johnston C. Gender differences in adults with attention-deficit/hyperactivity disorder: A narrative review. Clin Psychol Rev 2015;40: 15-27.
155 Volkow ND, Fowler JS, Wang G, Ding Y, Gatley SJ. Mechanism of action of methylphenidate: insights from PET imaging studies. J Atten Disord 2002;6 Suppl 1: S31-43.
156 Volkow ND, Wang G, Fowler JS, Logan J, Gerasimov M, et al. Therapeutic doses of oral methylphenidate significantly increase extracellular dopamine in the human brain. J Neurosci 2001;21: RC121.
157 Volkow ND, Wang GJ, Fowler JS, Gatley SJ, Logan J, et al. Dopamine transporter occupancies in the human brain induced by therapeutic doses of oral methylphenidate. Am J Psychiatry 1998;155: 1325-31.
158 Volkow ND, Wang GJ, Newcorn JH, Kollins SH, Wigal TL, et al. Motivation deficit in ADHD is associated with dysfunction of the dopamine reward pathway. Mol Psychiatry 2011;16: 1147-54.
159 Volkow ND, Wang GJ, Tomasi D, Kollins SH, Wigal TL, et al. Methylphenidate-elicited dopamine increases in ventral striatum are associated with long-term symptom improvement in adults with attention deficit hyperactivity disorder. J Neurosci 2012;32: 841-9.
160 Woodall A, Howard L, Morgan C. Barriers to participation in mental health research: findings from the Genetics and Psychosis (GAP) Study. Int Rev Psychiatry 2011;23: 31-40.
161 World Health Organization (WHO). International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10). 1992.
162 Young JL, Sarkis E, Qiao M, Wietecha L. Once-daily treatment with atomoxetine in adults with attention-deficit/hyperactivity disorder: a 24-week, randomized, double-blind, placebo-controlled trial. Clin Neuropharmacol 2011;34: 51-60.
163 Young S, Sedgwick O, Fridman M, Gudjonsson G, Hodgkins P, et al. Co-morbid psychiatric disorders among incarcerated ADHD populations: a meta-analysis. Psychol Med 2015;45: 2499-510.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1353
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-327892
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2017
























