Embed Size (px)
Citation preview
Autonomic Nervous System
Chapter 16, 17, 18, 19, 20
Clinical Drug Therapy
Nervous System
Two main divisions Central Nervous System or CNS Peripheral Nervous System or PNS
Central Nervous System or CNS Brain and spinal cord: receives and
processes incoming sensory information and responds by sending out signals that initiate or modify a process.
Peripheral Nervous System or PNS Includes all the neurons and ganglia found
outside the CNS Afferent (sensory): modify motor output Efferent:
Afferent Neurons
Afferent neurons carry sensory input from the periphery to the CNS and modify motor output through the reflex arc.
Efferent Neurons
Efferent neurons carry motor signals from the CNS to the peripheral areas of the body.
ANS / SNS
Autonomic nervous system controls involuntary activities of smooth muscle, secretory glands and the visceral organs of the body such as the heart (involuntary activities of smooth muscle)
Somatic nervous system innervates the skeletal muscles and controls voluntary movement
Autonomic Nervous System
Sympathetic Nervous System Para sympathetic System Enteric System
The Race Horse and the Cow
Sympathetic Nervous System
Sympathetic System
Fight or Flight – stimulated by physical or emotional stress (exercise or work), pain, hemorrhage, intense emotions, temperature extremes
Sympathetic Nervous System
Protective mechanisms designed to help person cope with the stress or get away from it.
Neurotransmitters
Neurotransmitters Acetylcholine: skeletal muscle Norepinepherine: stress response
Norepinephrine and epinephrine Both always present in the blood. Norepinephrine varies according to the
amount of stress present and will cause transient changes in heart rate and systemic arteries and veins.
Epinephrine is a constant in regulating heart rate, vasoconstriction in systemic arteries and veins and vasodilation of muscles and liver.
Dopamine
Adrenergic neurotransmitter – essential for normal brain function. Studies focus on connection between dopamine
malfunction in schizophrenia and Parkinson’s Disease.
Role of dopamine in drug addition to drugs: stimulants and depressants.
Protective Mechanisms
Intensity of response depends on Norepinephrine and epinephrine
Fight or flight
Body Responses
Increase in blood pressure and cardiac output.
Increase blood flow to brain, heart and skeletal muscles.
Decrease blood flow to skin and organs not needed for “flight”.
Increase in glycogen for energy, mental activity, muscle strength, blood coagulation, respiratory rate, pupil dilation to aid vision, and increase in sweating.
Fight of Flight Response
Can be a problem if the body stay in the “fight or flight” mode.
Type A personalities? High stress environment? Medications may be needed reduce the
physiologic body responses.
Parasympathetic Nervous System
Rest and Digest Save energy Decreased heart rate
Adrenergic Receptors
Norepinephrine and epinephrine interact with two adrenergic receptors Alpha and beta
Alpha 1 Alpha 2 Beta 1 Beta 2
Alpha 1
Alpha 1 receptors allows calcium ions to move into the cell and produce muscle contraction.
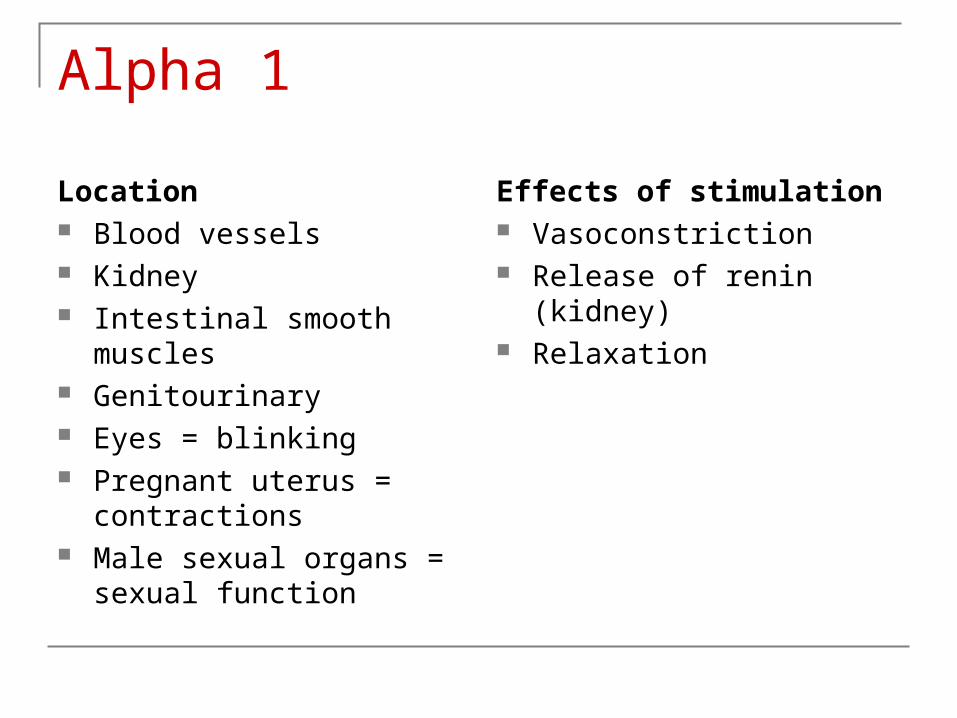
Alpha 1
Location Blood vessels Kidney Intestinal smooth muscles Genitourinary Eyes = blinking Pregnant uterus =
contractions Male sexual organs =
sexual function
Effects of stimulation Vasoconstriction Release of renin (kidney) Relaxation
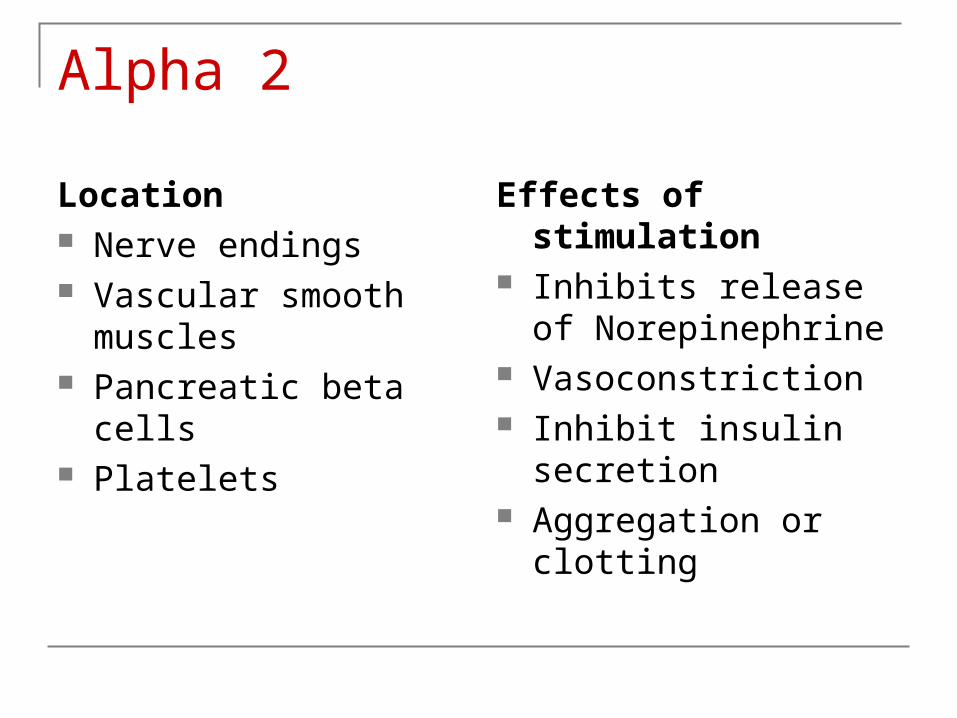
Alpha 2
Location Nerve endings Vascular smooth
muscles Pancreatic beta cells Platelets
Effects of stimulation Inhibits release of
Norepinephrine Vasoconstriction Inhibit insulin secretion Aggregation or clotting
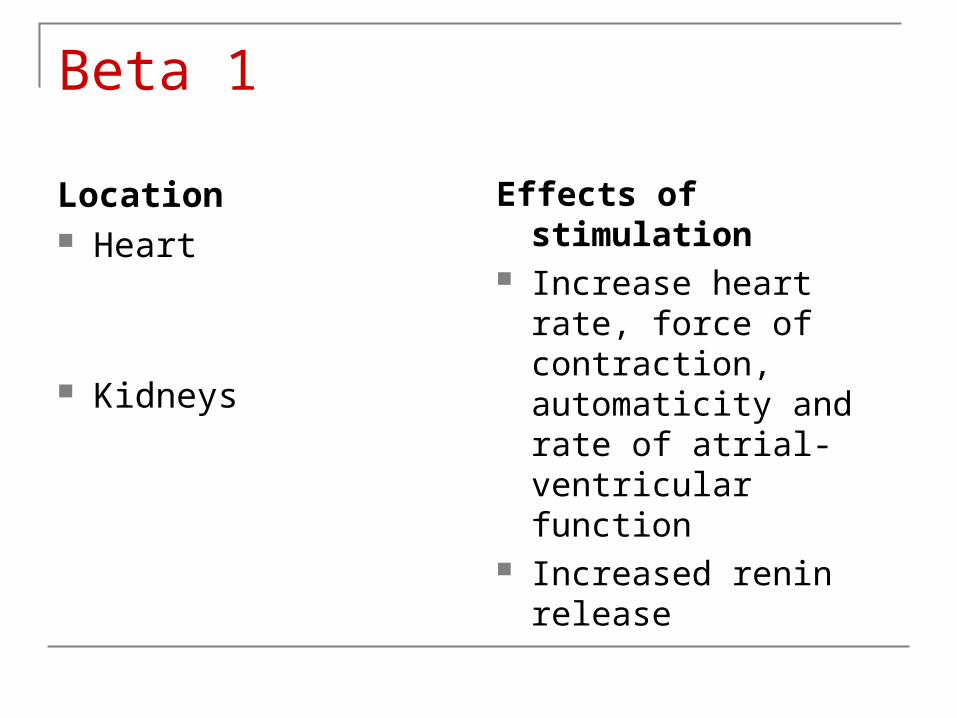
Beta 1
Location Heart
Kidneys
Effects of stimulation Increase heart rate,
force of contraction, automaticity and rate of atrial-ventricular function
Increased renin release
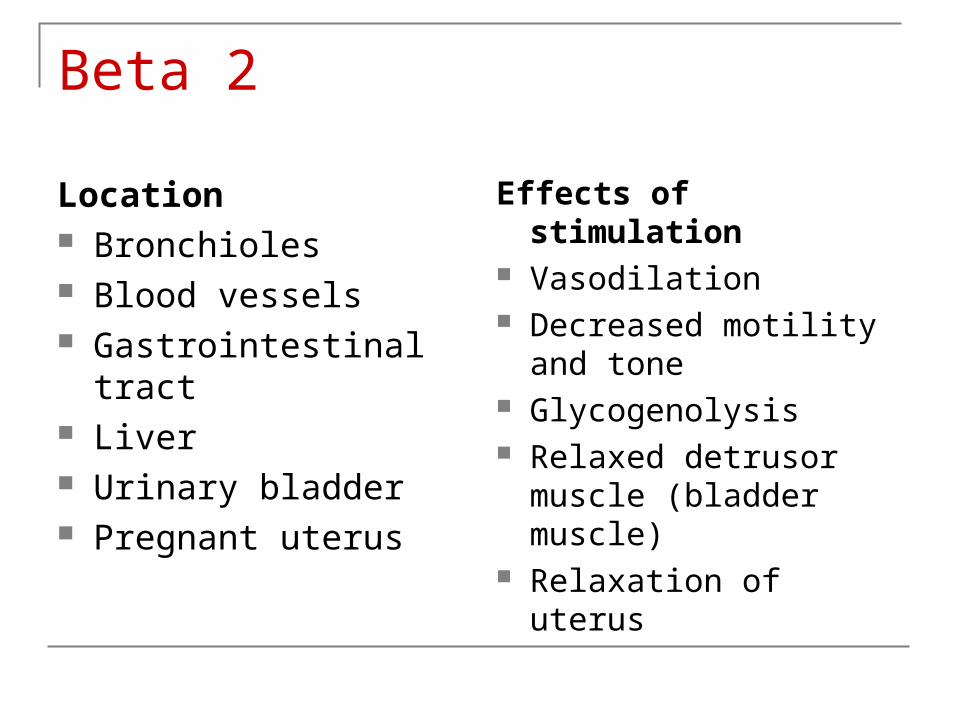
Beta 2
Location Bronchioles Blood vessels Gastrointestinal tract Liver Urinary bladder Pregnant uterus
Effects of stimulation Vasodilation Decreased motility and
tone Glycogenolysis Relaxed detrusor
muscle (bladder muscle)
Relaxation of uterus
Dopamine
Location Blood vessels of
kidney, heart, and other viscera
Effects of stimulation Vasodilation
Parasympathetic Nervous SystemFunctions stimulated by PNS: Resting,
reparative, or vegetative function
Body Responses
Dilation of blood vessels in skin Decrease heart rate (bradycardia) Increase secretion of digestive enzymes Constriction of smooth muscle of bronchi Increase in sweat glands Contraction of smooth muscles of urinary
bladder Contraction of smooth muscle of skeletal
system
Neurotransmitter
Acetylcholine Two types of cholinergic receptors
Nicotinic: located in motor nerves and skeletal muscles
Muscarinic: located in internal organs, cardiovascular, respiratory, GI and GU
Autonomic Drugs
Drugs used due to their ability to stimulate or block activity of the sympathetic or parasympathetic nervous system.
Effect of Drugs
Drugs that act of ANS usually affect the entire body.
Effects depend on whether you are trying to stimulate or inhibit function.
Receptor Activity
Drugs are developed to stimulate or inhibit particular subtypes of receptors.
More selective on particular body tissues. Decrease adverse effects on other body
tissues – side effects.
Simulation of SNS
Stimulation of sympathetic nervous system can be divided into drug classifications: Adrenergic Sympathomimetic Alpha and beta adrenergic agonists
Agonist
In pharmacology an agonist is a substance that binds to a specific receptor and triggers a response in the cell.
Blockage of SNS
Drugs that inhibit sympathetic nervous system are classified as Antiadrenergic Sympatholytic anticholinergic
Stimulation of PNS
Parasympathetic nervous system stimulation drug classifications Cholinergic Parasympathomimenic Cholinomimetic
Blocking of PNS
Drugs that inhibit parasympathetic stimulation are classified as: Anticholinergic Parasympatholytic Cholenergic blocking drugs
Classifications: SNS
Sympathetic nervous system drug classifications Adrenergic - stimulating Antiadrenergic - blocking
Classifications: PNS
Parasympathetic nervous system drugs Cholinergic Anticholinergic
Adrenergic Drugs
Chapter 17

Adrenergic Drugs
What do they do? Stimulation of the sympathetic nervous
system.
Mechanism of Action
Three mechanisms: Directly with alpha 1 or beta-adrenergic receptors
on surface membrane. Indirect effects of postsynaptic adrenergic
receptors. Mixed action – combination of action on direct and
indirect receptor.
Heart
Direct stimulation of receptors Alpha 1 - Vasoconstriction of blood vessels which
increases blood pressure – pressor or vasopressor effect.
Beta 2 - increased force of myocardial contraction - Increased speed of electrical conduction in the heart.
Lungs
Asthma and COPD (Chronic Obstructive Pulmonary Disease): Beta 2 drugs or bronchodilators are used to relieve broncho-constriction and broncho-spasm.

Pregnancy
Adrenergic drugs used to relax uterine muscles in preterm labor.
OTC Adrenergic Drugs
Common cold: anti-histamines Allergy: nasal or oral to relieve nasal
congestion
Adrenergic Drugs
Epinephrine Pseudoephedrine – Sudafed Isoproterenol (Isuprel) Phenylephrine (Neo-Synephrine) Clonidine (antihypertensive)
How does one choose a drug? How emergent is the situation PO or IM or IV
Allergic Response
Runny nose, itchy eyes, cough Asthma: Cough with bronchospasms,
difficulty breathing or SOB (shortness of breath)
Anaphylactic shock – edema of airway
Allergy Response
Nasal congestion, itchy eyes, non-productive cough
Seasonal response to environmental causes Commonly mixed with other drugs in cold
medications
Pseudoephedrine
Therapeutic classification: allergy, cold, and cough remedies, nasal drying, and decongestants.
Indications: symptomatic management of nasal congestion associated with acute viral upper respiratory tract infection. Most often used in combination with other drugs.
Action: stimulates Alpha and beta-adrenergic receptors – vasoconstriction in respiratory tract mucosa – possible bronchodilation
Therapeutic effects: reduction of nasal congestion, and swelling of nasal passages.
Forms and Dosage
How supplied: tabs, chew tabs, extended release tabs, liquid or drops
Dosing: 30 to 60 mg / dose q 6-8 hours PO Maximum dose 240 mg/24 hours Sustained release: 120 mg PO q 12 hours
Contraindications
Severe Hypertension Severe CAD / coronary artery disease Use with caution in pregnancy, breast feeding
and renal failure
Use with caution!
Mild or moderate hypertension, hyperglycemia, hyperthyroidism, and cardiac disease.
Side Effects
Dizziness, nervousness, restlessness, insomnia and arrhythmias
Seizures Cardiovascular collapse
Additional Information
OTC used in combination with anti-histamines
Primarily excreted renally – adjust in patients with renal impairment
May cause false-positive for amphetamines – athletes
Currently need to ask pharmacist for Sudafed – OTC has been limited due to abuse
Nursing Implications
Assess for congestion Monitor pulse and blood pressure before
beginning therapy Assess lung sound for signs of bronchial
secretions
Severe Anaphylactic Shock
Usually involving the airways Some thing as simple as food allergy can
trigger it Peanuts, shell fish, legumes, bee sting,
medications Symptoms usually starts with numbness and
tingling of lips and leads to swelling of the glottis or epiglottis – this can result in closure of the airway.
How Do You Treat It?
Epinephrine would be the drug of choice Classification: adrenergic Action: affects both the beta (cardiac) and
beta (pulmonary) receptors – produces bronchodilation – inhibits hypersensitivity reaction of mast cells.
Epinephrine
Therapeutic Effects: Bronchodilation Maintenance of heart rate and blood pressure
Adverse Side Effects: Nervousness, restlessness, tremors, angina,
arrhythmias, hypertension, tachycardia
How it is given?
Sub-Q or IV or inhaled The subcutaneous or intramuscular
administration will help it to get into the blood stream quicker – epi-pen is given to clients with severe allergy reactions
Not given by mouth because drug is inactivated by gastric juices
Can be inhaled in asthma attack

CAUTION!
Check dose, concentration, and route of administration – fatalities have occurred from medication errors – us TB syringe for subcutaneous administration
Inhaled provided as metered dose inhaler 160 to 250 mcg – broncho-constriction is asthma
IV would be 0.1 to 0.25 mg (cardiopulmonary resuscitation)
Precautions with Use
Tachyarrhythmia's (fast irregular heart rate), headache, nausea, and palpitations
Short acting so more definitive treatment needs to be initiated
Need cardio-respiratory monitoring Pulse oximetry Cardiac monitor
Cardiac Arrest
Epinephrine is the best studied and most
widely administered adrenergic agonist used
for the treatment of cardiac arrest.
Used to jump start the heart.
Vasopressor / Inotropic Drugs Used extensively along with Dopamine to
maintain myocardial and cerebral perfusion post cardiac arrest.
Administered in small, consistent amounts intravenous.
Antiadrenergic Drugs
Chapter 18
Clinical Drug Therapy
Antiadrenergic Drugs
Blocks the effects of the sympathetic nerve stimulation, endogenous catecholamine and adrenergic drugs.
Mechanism of Action
Act on alpha or beta receptors Receptors are blocked by adrenergic
antagonists or pre-synaptic alpha 2 receptors are stimulated.
When Used?
To manage hypertension and a number of cardiovascular disorders.
Anti – hypertensive Medication Clonidine: Catapres, Catapres TTS, Dixarit,
Duracion Pharmacologic classification: adrenergic
(centrally acting) Therapeutic classification: antihypertensive
Clonidine
Action: Stimulates the alpha-adrenergic receptors in the CNS which results in decreased sympathetic outflow inhibiting cardioacceleration and vasoconstriction centers. Prevents pain signal transmission to the CNS by stimulating alpha-adrenergic receptors in the spinal cord.
Therapeutic Effects: decreased blood pressure. Decreased pain.
Cholinergic Drugs
Chapter 19
Clinical Drug Therapy
Cholinergic Drugs
Cholinergic drugs stimulate the parasympathetic nervous system.
Mechanism of Action
Direct acting cholinergic drugs are synthetic derivative of choline.
Effects of drug Decrease heart rate, vasodilation, and changes in
BP Increase tone and contractibility of smooth muscle Increase tone and contractibility of bronchial
smooth muscles Increased respiratory secretions
Indications for Use
Urinary retention without obstruction Postoperative abdominal distention due to
paralytic ileus Myasthenia gravis – muscle weakness During surgery to reverse the effects of
muscle relaxants used during surgery
Nursing Assessment: urine retention Urinary retention
Bladder distention Fluid intake Time of last void
How do you know drug is working? Fluid intake equal to urine output Patient has voided within the last 8 hours
Nursing Assessment: paralytic ileus Paralytic ileus
Hypo-peristalsis Decreased bowel sounds No gas or bowel movement
How do you know drug is working? Bowel sounds heart in all four quadrants Client states has passes gas Client states has had a bowel movement
Nursing Assessment: Myasthenia Gravis Signs and symptoms: muscle weakness,
ptosis (droopy eye lid), diplopia (double vision), difficulty chewing and swallowing, decreased activity intolerance.
How do you know medication is working? Increased muscle tone, no droopy eye lid or double vision, increased activity tolerance.
Nursing Assessment: Alzheimer Signs and symptoms: loss of memory,
cognitive function and decreased self-care Signs medication is working: increase
memory and cognitive function and increase interest in activities of daily living
Use in Older Adults
May be used in myasthenia gravis or Alzheimer’s disease
Contraindications
Renal obstruction Liver disease
Anticholinergic Drugs
Chapter 20
Clinical Drug Therapy
Anticholinergic Drugs
Anticholinergics are a class of medications that inhibit parasympathetic nerve impulses by selectively blocking the binding of the neurotransmitter acetylcholine to its receptor in nerve cells.
Mechanism of Action
Drugs act by occupying receptor sites on target organs innervated by parasympathetic nervous system leaving fewer receptor sites free to respond to acetylcholine.
Parasympathetic response is absent or decreased depending on number of receptors blocked.
Effects of Anticholinergic Drugs CNS stimulation followed by depression Decreased cardiovascular response to
parasympathetic (vagal) stimulation that slows heart rate
Bronchodilation and decrease respiratory secretions
Antispasmodic effects in GI system Change in intra-ocular pressure in patients
with glaucoma
Uses
GI disorders – peptic ulcer disease, gastritis, increased gastric acid secretion – relax gastric smooth muscle (replaced by newer drugs)
Genitourinary – anti-spasmodic – urgency Excessive secretions Ophthalmology – relax eye for exam Respiratory disorder – asthma or bronchitis –
inhaled form only Cardiac disorders – bradycardia or heart block Parkinson’s disease
Side Effects
Hyperthermia, hot, dry flushed skin, dry mouth, tachycardia, delirium, paralytic ileus and urinary retention
Atropine
Pharmacological classification: anticholinergic
Therapeutic classification: antiarrhythmic Action: Inhibits the action of acetylcholine at
postganglionic sites located in the smooth muscle, secretory glands, CNS. Low doses decrease: sweating, salivation and respiratory secretions.
Atropine
Therapeutic effects: Increased heart rate Decreased GI and respiratory secretions Reversal of muscarinic effects May have spasmodic action on the biliary and
genitourinary tracts.
Atropine
Side effects: drowsiness, blurred vision, tachycardia, dry mouth, urinary hesitancy.
Atropine
Prototype of anticholineric drugs – atropine sulfate
Therapeutic
Previously used in preoperative patients to reduce secretions – other newer drugs have replaced