Embed Size (px)
Citation preview

Letter to the Editor
Autosomal Dominant Inheritance of ScapuloiliacDysostosis
To the Editor:
Scapuloiliac dysostosis (pelvis-shoulder dysplasia,OMIM 169550) is a rare and apparently heterogeneousfocal skeletal dysostosis. Only 6 cases have been docu-mented in the literature [Kosenow et al., 1970; Thomaset al., 1977; Walbaum et al., 1982; Blane et al., 1984;Hauser et al., 1998] (see Table I). The major featurescomprise hypoplasia of the ilia, acetabula and scapu-lae, lumbar lordosis, and congenital hip dislocation.Ophthalmological abnormalities have been describedin two cases, and include microphthalmia, coloboma ofthe iris or optic nerve, ectopic pupil and corneal cloud-ing. Other variable features include spina bifida oc-culta, abnormal external ears, rib abnormalities, digi-tal abnormalities and hypoplasia of the fibulae. Thesyndrome of pelvis-shoulder dysplasia with epiphysealchanges, facial abnormalities and rhizomelic shortstature, described in the offspring of consanguineousparents [Cousin et al., 1982], probably represents a dis-tinct autosomal recessive syndrome.
Sporadic occurrence has been a feature of all cases ofscapuloiliac dysostosis with the exception of one case[Kosenow et al., 1970]. In that case the father of the
affected female refused to be examined, but was de-scribed as having a marked lumbar lordosis, smallscapulae and abnormal gait. A single X-ray taken atage 11 years showed marked hypoplasia of the iliacbones and sacral spina bifida occulta, findings consis-tent with the diagnosis of scapuloiliac dysostosis.
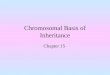
We report the first documented instance of father-son transmission of scapuloiliac dysostosis. The 29-year-old affected father has previously been reported inthe literature [Hauser et al., 1998]. His main featureswere congenitally dislocated hips, marked hypoplasiaof the ilia and acetabula (Fig. 1.) and lumbar lordosis.The scapulae and clavicles were spared. His first child,a male, was born after a normal pregnancy. The pelviswas noted to be narrow at delivery and hip dislocationwas suspected clinically.
Radiographs taken at 14 months showed global hy-poplasia of the ilia that were ovoid in shape with noevidence of formation of the of the acetabula or sacro-sciatic notches (Fig. 2A). The pubic bones and ischiawere normal in size and shape. The proximal femoraappeared normal and the capital femoral epiphyseswere ossified but hypoplastic for age. There was hypo-plasia of the body of the scapulae and mild glenoid
*Correspondence to: David Amor, Victorian Clinical GeneticsService, Flemington Rd, Parkville 3052, Australia.E-mail: [email protected]
Received 28 December 1999; Accepted 10 August 2000
TABLE I. Features of Reported Cases of Scapuloiliac Dysostosis*
Kosenowet al.,[1970]Case 1
Kosenowet al.,[1970]Case 2
Kosenowet al.,[1970]
(Father ofCase 2)
Thomaset al.,[1977]
Walbaumet al.,[1982]
Blaneet al.,[1984]
Hauseret al.,[1998]
Present report.(Son of case ofHauser et al.,
[1998])
Gender F F M F F NS M MHypoplastic scapulae + + NXR + + + − +Hypoplastic clavicles + + NXR + − + − −Hypoplastic ilia + + + + + + + +Hypoplastic acetabulae + + − − + − + +Hip dislocation/sublaxation + + − − NS − + +Lumbar lordosis + + + + − NS + −Spina bifida occulta − + + + − − − −Eye abnormality + − − − − + − −Malformed ears + − − + − + − −Clinodactyly − − − − − + + −Absent 5th finger − − − − + − − −Fibula hypoplasia − − − − + − − −Rib abnormalities + − NXR + − − − −
*NXR, not x-rayed; NS, not stated.
American Journal of Medical Genetics 95:507–509 (2000)
© 2000 Wiley-Liss, Inc.

hypoplasia (Fig. 2B). The remaining skeleton was nor-mal, including the clavicles, ribs and humeri. Thesefindings are consistent with scapuloiliac dysostosis, afinding that confirms the autosomal dominant trans-mission of this rare skeletal dysostosis.
REFERENCESBlane CE, Holt JF, Vine AK. 1984. Scapuloiliac dysostosis. Br J Radiol
57:526–528.
Cousin J, Walbaum R, Cegarra P, Huguet J, Louis J, Pauli A, Fournier A,Fontaine G. 1982. Familial pelvic-scapulary dysplasia with anomaliesof the epiphyses, dwarfism and dysmorphy: a new syndrome? Arch FrPediatr 39:173–175.
Hauser SE, Chemke JM, Bankier A. 1998. Pelvis-shoulder dysplasia. Pe-diatr Radiol 28:681–682.
Kosenow W, Niederle J, Sinios A. 1970. Pelvis-shoulder dysplasia. FortschrGeb Rontgenstr Nuklearmed 113:39–48.
Thomas PS, Reid MM, McCurdy AM. 1977. Pelvis-shoulder dysplasia. Pe-diatr Radiol 5:219–223.
Walbaum R, Titran M, Durieux Y, Crepin G. 1982. Tetradactyly of bothhands, hypoplasia of both fibulas and scapuloiliac hypoplasia: a newsyndrome? J Genet Hum 30:309–312
David J. Amor*Ravi SavarirayanAgnes BankierVictorian Clinical Genetics ServiceRoyal Children’s HospitalMelbourne, Australia
Fred JensenMonash Medical CentreMelbourne, Australia
Simon P. HauserNorthern HospitalMelbourne, Australia
Fig. 1. AP radiograph of pelvis of affected father at age 29 years showing small ilia, large iliac crest ossification centres and bilateral hip dislocation.
508 Amor et al.

Fig. 2. Radiographs of affected child at age 14 months. A: AP radiograph of the pelvis and hips, demonstrating marked hypoplasia of the ilia andabsent acetabula. B: AP radiograph of the chest demonstrating mild glenoid hypoplasia and hypoplasia of the body of the scapulae.
Letter to the Editor 509





![Autosomal recessive ichthyosis with limb reduction defect ... · including autosomal dominant, autosomal recessive and X-linked inheritance [1,2]. Associated cutaneous and extracutaneous](https://img.pdfslide.net/doc/110x75/5ec8c9b91adfdf12ab3e663c/autosomal-recessive-ichthyosis-with-limb-reduction-defect-including-autosomal.jpg)