Embed Size (px)
Citation preview

American Journal of Medical Genetics 35:516-518 (1990)
Brief Clinical Report
Autosomal Recessive Inheritance of a Syndrome of Hypertelorism, Hypospadias, and Tetralogy of Fallot?
Talaat I. Farag and Ahmad S. Teebi Kuwait Medical Genetics Centre, Maternity Hospital, Kuwait
We report on 3 brothers with hypertelorism, hypospadias, and tetralogy of Fallot. Parents are first cousins once removed; the father has apparent hypertelorism. An apparently nor- mal paternal uncle who is married to a second cousin also has a daughter with hypertelor- ism and tetralogy of Fallot. All similarly af- fected relatives have mild or borderline men- tal retardation. The combination of anomalies may represent a previously undescribed auto- soma1 recessive disorder.
KEY WORDS: midline field defect, new syn- drome, Opitz syndrome, men- tal retardation, consanguinity
INTRODUCTION The hypertelorism-hypospadias syndrome was first
described by Opitz et al. [1969al in 2 apparently distinct forms designated the BBB syndrome [Opitz et al., 1969al and the G syndrome [Opitz et al., 1969bl. Subse- quent reports on these “syndromes” [Opitz, 1987; Stevens and Wilroy, 1988; Wilson and Oliver, 19881 sug- gested considerable phenotypic overlap. However, the occurrence of both BBB and G syndrome phenotypes in different members of the same family [Frias et al., 1983; Opitz, 1987; Allanson, 19881 suggested that BBB and G syndromes represent variable expression of the same mutant gene. Cappa et al. [1987] and Neri and Cappa [1988] proposed that they both be designated by the common term “Opitz syndrome” given that both syn- dromes are most likely transmitted in an autosomal dominant manner with increased expressivity in males.
Here we describe another distinct hypertelorism-hy- pospadias syndrome with tetralogy of Fallot in several members of an Arab family.
Received for publication April 5,1989; revision received August
Address reprint requests t o Dr. Ahmad S. Teebi, PO Box 36660 24, 1989.
Raas, 24757, Kuwait.
CLINICAL REPORTS Patient 1
The propositus (V-10, Fig. 1) weighed 3,100 g a t birth and had apparent hypertelorism, glandular hypo- spadias, but no feeding problems. At 3 months he devel- oped central cyanosis and a cyanotic heart defect was suspected. ECG and echocardiogram demonstrated a ventricular septa1 defect (VSD), right ventricular hy- pertrophy, large aorta, and aortic override. Cardiac catheterization at 2 years showed valvular and infun- dibular pulmonary artery stenosis, hypoplasia of the pulmonary artery, large subaortic VSD, and overriding aorta. The findings were consistent with tetralogy of Fallot with patent foramen ovale.
At 3% years he weighed 18 kg, was 103 cm tall (90th centile), and had an OFC 50 cm (50 centile). He had apparent hypertelorism with an innercanthal distance ( E D ) of 3.2 cm and an interpupillary distance (IPD) of 5.5 cm (97th centile), bilateral epicanthic folds, narrow palpebral fissures, flat nasal bridge, long philtrum, pro- truding lower lip, posteriorly angulated and apparently low-set ears, glandular hypospadias, peripheral and central cyanosis, bulging precordinum, and clubbing of fingers and toes. His I& was 65 (Standford-Binet intel- ligence scale). Chromosomes were normal. Skeletal ra- diographs were normal except for spina bifida occulta (L5 and Sl). Hearing, vision, and smell were normal. At age 6% years he underwent corrective cardiac surgery after which he did well.
Patient 2 (V-11, Fig. 1). At birth he weighed 2,950 g and had
central cyanosis with feeding difficulties. At 7 months he weighed 6,900 g, was 66 cm long (3rd centile), and had an OFC of 45 cm (50th centile) with severe cyanosis, clubbing of fingers and toes, a bulging precordinum with asymmetry, and other manifestations similar to those of his brother (Table I). ICD was 2.8 cm (90th centile) and IPD was 5 cm (97th centilej. Diagnosis of tetralogy of Fallot was suspected on clinical, ECG, and echocardiographic data. He died a t age one year after a severe cyanotic spell.
0 1990 Wiley-Liss, Inc.

Hypertelorism, Hypospadias, Tetralogy and Fallot 517
I @-I@
I
IV
1 2-6 7-9 10 1 1 12 13 14 15 16 /”
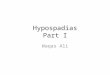
Fig. 1. Family pedigree. @ @ :Hypertelorism, tetralogy of Fallot, and hypospadias in males.
:Hypertelorism only.
Patient 3 (V-15, Fig. 1). At birth he weighed 3 kg and had mild
central cyanosis but no feeding problems. ECG and echocardiogram were suggestive of tetralogy of Fallot. Cardiac catherization at age 7 months (Great Ormond Street, London) disclosed tetralogy of Fallot with absent pulmonary valve and aneurysmal dilatation of pulmon- ary arteries. Examination at age one year showed mani- festations similar to those of his sibs (Table I) with tal- ipes equinovarus deformity of the right foot. His OFC was 45.6 cm (25th centile), ICD 3.2 cm, and IPD 5.3 cm (97th centile). He had corrective cardiac surgery done in London (UK) after which he did well.
Patient 4 (V-1, Fig. 1). Data were retrieved from hospital re-
cords. She had cyanosis and feeding problems soon after birth. ECG, echocardiogram, and cardiac catheteriza- tion at age 3 years disclosed a tetralogy of Fallot with high VSD below the pulmonary and the aortic valves “doubly committed.” In addition she had a patent ductus arteriosus together with the manifestations in Table I. She had corrective cardiac surgery done at 6 years after which she died from complications.
FAMILY HISTORY Parents of the first 3 patients are first cousins once
removed Palestinian Arabs. The father (36 years old) had hypertelorism (ICD 4 cm, IPD 7.5 cm) without hypo- spadias or congenital heart defect. The mother (26 years old) is phenotypically normal. They have 3 normal chil- dren (including a twin pair) and a history of one early spontaneous abortion. The 3 affected sibs were born normally after unremarkable pregnancies. Her father and mother are second cousins and look phenotypically normal (from a photograph). No other relative had hypo- spadias or a congenital heart defect. Unfortunately, photo permit was not possible for any of the affected members.
DISCUSSION Patients here have hypospadias and a characteristic
facial appearance with hypertelorism, flat nasal bridge, epicanthic folds, narrow palpebral fissures, and poste- riorly angulated ears resembling those seen in G syn- drome [Opitz, 1987; Wilson and Oliver, 19881. None had an esophageal abnormality, and their feeding diffi- culties were the consequence of dyspnea related to their cyanotic heart defect. Without dysphagia i t is just as reasonable to consider the BBB syndrome in our pa- tients.
Recent reviews [Opitz, 1987; Stevens and Wilroy, 1988; Wilson and Oliver, 19881 indicate that patients with the G and BBB forms of the Opitz syndrome may have a variety of cardiovascular anomalies such as VSD, ASD, vascular ring, coarctation of the aorta, drainage of left superior vena cava into the coronary sinus, patent ductus arteriosus, pulmonary valve insufficiency, etc. However, all of our patients have documented tetralogy of Fallot, which is not described in the Opitz syndrome; thus, it seems unlikely that they represent the Opitz syndrome.
Our 4 patients had an apparent hypertelorism and tetralogy of Fallot with minor variations. In addition, the males have variable degrees of hypospadias and mild or borderline mental retardation. Such a consistent constellation of these midline field defects hitherto not
TABLE I. Manifestationa in 4 Patients with Hypertelorism-Hypospadias-Tetralogy of Fallot Syndrome
Manifestations Patient 1 (sib) Patient 2 (sib) Patient 3 (sib) Patient 4 (cousin) DOB 13/5/1979 2013/82 20/10/85 8/10/80. Sex M M M F Cyanosis +(3 months) +(at birth) +(at birth) +(a t birth) Feeding problems -
Apparent hypertelorism + + + + Epicanthic folds i- + ? Narrow palpebral fissures + + + ? Flat nasal bridge + + + ? Long philtrum + Posteriorly angulated ap- + - -
Hypospadias + (glandular) + (glandular) + (penoscrotal) -
Tetralogy of Fallot + + + + Other cardiac defects Patent foramen ovale - Absent pulmonary valve Patent ductus arteriosus Mildhorderline MR +(I& 65) ? +(I& 60) Chromosomes Normal 46,XY
+ - + -
? - -
+ parently low-set ears
+ (degree not assessed) - - -

518 Faraq and Teebi
reported may represent a variant of the Opitz syndrome, or, more likely, a distinct entity.
The inheritance of the syndrome is unclear. In the case of autosomal dominant transmission, hypertelor- ism in the father of the 3 affected brothers may repre- sent mild heterozygote expression. If the hypothesis of autosomal dominant inheritance is correct, the consan- guinity in the parents of the affected patients may indi- cate presence of the Opitz syndrome with coincidental autosomal recessive tetralogy of Fallot.
The more likely possibility is autosomal recessive in- heritance supported by the presence of parental consan- guinity in 2 sibships, similarly affected male and fe- males, and absence of affected relatives in previous generations in the family except for hypertelorismin the father, which may be a heterozygote manifestation. More reports on similar cases will help to further the characterization and to determine the scope of intra- familial and interfamilial variability and mode of inher- itance.
ACKNOWLEDGMENTS
REFERENCES Allanson J E (1988): G syndrome: An unusual family. Am J Med Genet
Cappa M, Borelli P, Marini R, Neri G (1987): The Opitz syndrome: A new designation for the clinically indistinguishable BBB and G syndromes. Am J Med Genet 28:303-309.
Frias JL, Roberts SF, McReynolds JW, Condron C (1983): Occurrence of the Opitz and the Opitz-Frias syndromes in the same family. David Smith Morphogenesis Meeting (abstract).
Neri G, Cappa M (1988): The Opitz syndrome (Letter). Am J Med Genet 302351 (only).
Opitz JM (1987): G syndrome (hypertelorism with esophageal abnor- mality and hypospadias, or hypospadias-dysphagia, or “Opitz- Frias” or Opitz G syndrome”-Perspective in 1987 and bibliogra- phy. Am J Med Genet 28:275-285.
Opitz JM, Summitt RL, Smith DW (1969a): The BBB Syndrome: Fa- milial Telecanthus With Associated Congenital Anomalies. In Bergsma D (ed): “The Clinical Delineation of Birth Defects Part 11. Malformation syndromes.” New York: Alan R. Liss, Inc., for the National Foundation-March of Dimes, BD:OAS V(2):86-94.
Opitz JM, Frias JL, Gutenberger JE , Pellett JR (1969b): The G Syn- drome of Multiple Congenital Anomalies. In Bergsma D (ed): “The Clinical Delineation of Birth Defects. Part 11. Malformation Syn- dromes.” New York: Alan R Liss, Inc., The National Foundation- March of Dimes, BD:OAS V(2):95-101.
31:637-642.
Stevens CA, Wilroy RS Jr (1988): The telecanthus-hypospadias syn- drome, Med Genet 25:536-542.
Wilson GN, Oliver wJ (1988): Further delineation of the G syndrome: A manageable genetic cause of infantile dysphagia. J Med Genet 25:157-163.
we thank Mr. Hani Shuhaiber (cardiac Surgeon) and Dr. Youssef Abu-Zanona (pediatric cardiologist) for help in evaluating some of the cases. Also we thank Dr. Sylva P. Shuhaiber and Dr. Moussa Y. Hammouri for develop- mental assessment.