Embed Size (px)
Citation preview
13
13. Starr, J. I., Rubenstein, A. H. J. clin. Endocr. 1974, 38, 305.14. Hernandez, A., Zorilla, E., Gershberg, H. J. Lab. clin. Med. 1969, 73, 25.15. Record, C. O., Alberti, K. G. M. M., Williamson, D. H., Wright, R. Clin.
Sci. molec. Med. 1973, 45, 677.16. Record, C. O., Chase, R. A., Alberti, K. G. M. M., Williams, R. ibid. 1975,
49, 473.17. Collins, J. R., Lacy, W. W., Stiel, J. N., Crofford, O. B. Archs intern. Med.
1970, 126, 608. 18. Sönksen, P. H. Personal communication.19. Terns, S., Steiner, D. F. J. clin. Invest. 1975, 57, 885.20. Gragnoli, G., Genazzani, A. R., Geser, C. A., Palazzuoli, U., Tanganelli, I.,
Felber, J. P. Excerpta med. Int. Congr. Ser. 1973, 280, abstr. 251.21. Mako, M., Block, M., Starr, J., Neilson, E., Friedman, E., Rubenstein, A.
Clin. Res. 1973, 21, 631.22. Sobel, H. J., Wayne, J. D. Gastroenterology, 1963, 45, 341.23. Conn, H. O. Am. J. med. Sci. 1970, 259, 394.24. Conn, H. O. Gastroenterology, 1972, 62, 61.
AUTOSOMAL RECESSIVE INHERITANCE OFSUSCEPTIBILITY TO TINEA IMBRICATA
SUSAN SERJEANTSON* GREGOR LAWRENCE
Institute of Medical Research, Goroka, Papua New Guinea
Summary Familial distribution of chronic tineaimbricata in an untreated Melanesian
population was consistent with a genetic predispositionto this disease. The pattern suggested that susceptibilityto chronic Trichophyton concentricum infection is reces-sively inherited and controlled by genes at a single auto-somal locus. In married couples there was no concor-dance of the disease above that expected by chance andthe observed segregation of tinea imbricata accordedwell with that predicted by the genetic hypothesis.
Introduction
TINEA imbricata (T.I.), also called "tokelau" and
locally in Papua New Guinea (P.N.G.) "grille", is a
superficial skin infection with an unmistakable clinicalappearance of patches of fragile, flaky, concentric ringsof scaling skin. It is chronic, usually affects large areasof body surface, although not hair and nails, and, if un-treated, recovery is rare. Warmth, high humidity, andinfrequent bathing have all been implicated in its de-
velopment.1 T.I. is common in parts of P.N.G. andOceania’ and has been reported in Mexico and SouthAmerica. 3
The mode of transmission of T.t. is unknown althoughsome members of patients’ families may be heavilyaffected while others are free of the disease. 1 2 one of us(G.L.) noticed the familial nature of T.I. and the occur-rence of both normal and severely affected individuals inMelanesian families and proposed that susceptibilitymight be inherited.
Simple mendelian inheritance of susceptibility to in-fectious disease is not common, although the reports ofdisease associations with the HLA system suggest thatpredisposition to some infectious diseases may be gov-erned by genes segregating at one or a small number ofloci.4 Other chronic dermatophytoses are known to beassociated with atopy, the mode of inheritance of whichis not settled, and with other rarer immunologicaldefects.5 6
*Present address: Department of Human Biology, John Curtin School of Medi-cal Research, Canberra, Australia.
Patients and Methods
During a general medical survey of seven villages in theGogol Valley, 50 km inland from Madang on the north coastof the P.N.G. mainland, 550 people were examined in familygroups. i he seven villages, although no more than 10 km
apart, represented three different language groups: the Hamlanguage of Austronesian classification, the Amaimon isolateof the Adelbert Range super-stock and the Kokon languagebelonging to the Madang super-stock. 7
T.I. was recorded as absent, mild, or severe involvement ofvisible skin; the area between midthigh and waist was not seenexcept in small children. Mild cases were almost entirely con-fined to children aged less than five years, where non-confluentpatches of T.I. may have been the early stages of potentiallysevere disease. Squames were taken from 6 typical cases andTrichophyton concentricum was found in all.Family relationships were ascertained by recording fathers’
and mothers’ names on presentation and these were cross-checked against independently prepared pedigrees that notedadoptions, and with blood genetic data for ABO, MNS, Ger-bich, and oval red-cell systems. Two discrepancies were clari-fied by repeat interview and blood-grouping tests.
Inspection of the pedigrees eliminated the possibility ofdominant or sex-linked inheritance of susceptibility. Possibleautosomal recessive inheritance of predisposition to chronicT.I.was tested by the segregation analysis of Smith.8 As the ageof onset is almost always less than two years of age,3 no age-groups were excluded, from analysis. There were 66 familiesin which both parents were examined, 37 families in which oneparent was examined, and 40 sibships in which neither parentwas seen. Of these 169 parents, 8 were included twice becauseof widowhood and remarriage or polygamy. 16 (9-9%) of 161parents and 41 (10.3%) of the 399 offspring had T.I. The
hypothetical recessive-gene frequency for calculation of
expected familial distributions of T.I. was estimated from theparental incidence as 0.3153. Sibships in which one or neitherparent was examined were combined for segregation analysisbecause of the small number of sibships examined.
Results
In 54 of the 66 families in which both parents wereexamined neither spouse was affected, in 11 families onespouse was affected, and in one family both husband andwife were affected. Under conditions of random mating,the expected numbers of mating types, when the genefrequency is 0.315 3 are 5 3 5, 11-8, and 0 7 for neither,one, and both spouses affected, respectively. These
expected numbers are not different from those observed(&khgr;2=0.19). Therefore there is no evidence of increasedconcordance of T.I. in husbands and wives above thatexpected by chance and neither is there any evidence ofassortative mating for the trait.
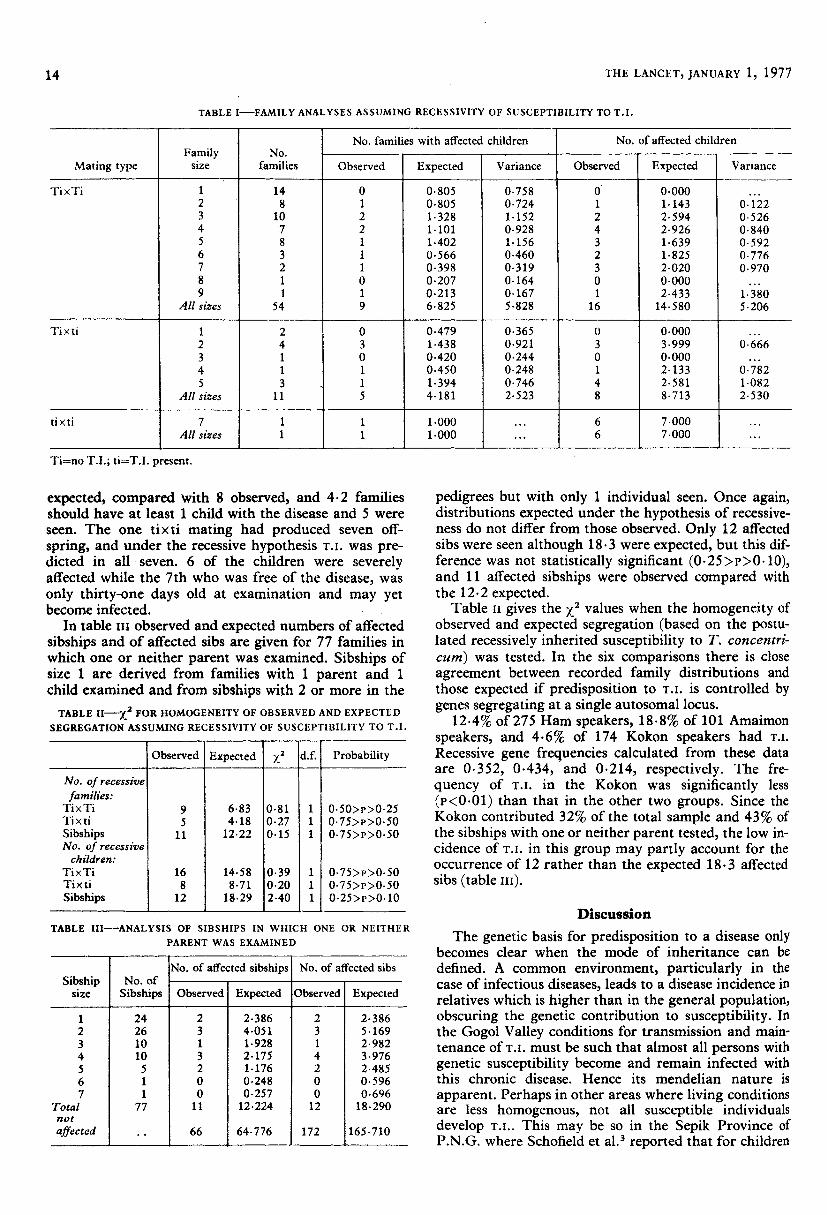
In Table I the observed and expected numbers offamilies with affected children, and observed andexpected totals of affected children are given for familiesin which both parents were examined. Individuals with1’.1. are shown as ti and those free of the disease as Ti.In 54 matings of type TixTi, 14.6 affected children areexpected if the hypothesis or recessivity is correct, and16 were seen. Of these 54 families, 6.8 are predicted tohave at least one child with the disease and 9 wereobserved. These observed and expected values are verysimilar as shown by ;:2 values, estimated according toSmith,8 in table n.The number of Ti x ti matings was small but observed
familial distribution of the disease was once again simi-lar to that expected from the genetic hypothesis. Fromthe distribution of family sizes 8.7 affected children are
14
TABLE I-FAMILY ANALYSES ASSUMING RECESSIVITY OF SUSCEPTIBILITY TO T.I.
Ti=no T.I.; ti=T,I. present.
expected, compared with 8 observed, and 4.2 familiesshould have at least 1 child with the disease and 5 wereseen. The one tixti mating had produced seven off-
spring, and under the recessive hypothesis T.I. was pre-dicted in all seven. 6 of the children were severelyaffected while the 7th who was free of the disease, wasonly thirty-one days old at examination and may yetbecome infected. ’
In table III observed and expected numbers of affectedsibships and of affected sibs are given for 77 families inwhich one or neither parent was examined. Sibships ofsize 1 are derived from families with 1 parent and 1child examined and from sibships with 2 or more in theTABLE II—&khgr;2 FOR HOMOGENEITY OF OBSERVED AND EXPECTED
SEGREGATION ASSUMING RECESSIVITY OF SUSCEPTIBILITY TO T.I.
TABLE III-ANALYSIS OF SIBSHIPS IN WHICH ONE OR NEITHER
PARENT WAS EXAMINED
pedigrees but with only 1 individual seen. Once again,distributions expected under the hypothesis of recessive-ness do not differ from those observed. Only 12 affectedsibs were seen although 18.3 were expected, but this dif-ference was not statistically significant (0.25>P>0.10),and 11 affected sibships were observed compared withthe 12.2 expected.
Table n gives the X2 values when the homogeneity ofobserved and expected segregation (based on the postu-lated recessively inherited susceptibility to T. concentri-cum) was tested. In the six comparisons there is closeagreement between recorded family distributions andthose expected if predisposition to T.I. is controlled bygenes segregating at a single autosomal locus.
12.4% of 275 Ham speakers, 18.8% of 101 Amaimonspeakers, and 4.6% of 174 Kokon speakers had T.I.
Recessive gene frequencies calculated from these dataare 0.352, 0.434, and 0.214, respectively. The fre-
quency of T.I. in the Kokon was significantly less
(P<0.01) than that in the other two groups. Since theKokon contributed 32% of the total sample and 43% ofthe sibships with one or neither parent tested, the low in-cidence of T.I. in this group may partly account for theoccurrence of 12 rather than the expected 18.3 affectedsibs (table III).
Discussion
The genetic basis for predisposition to a disease onlybecomes clear when the mode of inheritance can bedefined. A common environment, particularly in thecase of infectious diseases, leads to a disease incidence inrelatives which is higher than in the general population,obscuring the genetic contribution to susceptibility. Inthe Gogol Valley conditions for transmission and main-tenance of T.I. must be such that almost all persons withgenetic susceptibility become and remain infected withthis chronic disease. Hence its mendelian nature is
apparent. Perhaps in other areas where living conditionsare less homogenous, not all susceptible individuals
develop T.!.. This may be so in the Sepik Province ofP.N.G. where Schofield et al.3 reported that for children

15
with neither, one, or both parents with T.i. the propor-tions affected were 16%, 40%, and 63%, respectively.With a gene frequency of 0.530 calculated from theSepik data, the corresponding expected proportions are16%, 35%, and 100% if the hypothesis of recessivenessis correct. Absence of closer agreement between observedand predicted frequencies may also be due to inclusionof newborn children and to the uncertainty of parentagein this population in which as Schofield et al. noted,adultery was common.
In the Gogol Valley there was the following evidencefor autosomal recessive control of susceptibility to T.I.
(1) There is no evidence of concordance of T.I. in mar-ried couples although the condition is known to beacquired by bodily contact and close association withthose affected.2 (2) In formal segregation analysis thedata are comparable with expected family distributionsbased on a hypothesis of recessiveness. For families inwhich both parents were seen =1-67 with
0-90>p>0-73. Also, the only ti x ti mating resulted insix of seven children being affected, the seventh beingseen when only a few weeks old. (3) The frequency ofT.I. in one of the three language groups sharing anapparently common environment was significantly dif-ferent from the other two. A similar finding was
reported in P.N.G. by Schofield et al.,3 and in Fiji,Dompmartin1 found T.I. in Melanesians but rarely in In-dians. These ethnic and racial differences could be
expected if predisposition to the disease is geneticallydetermined.The conditions that permitted recognition of simple
mendelian inheritance of T.I. susceptibility, includinguniversal exposure to an unremitting disease, an earlyage of onset and absence of differential mortality, temptspeculation that if such "ideal" conditions existed forother diseases, further instances of single-locus controlof disease susceptibility might be found. The associationbetween Reiter’s syndrome and W27 HL-A antigen9may be another example of susceptibility to a disease,perhaps infectious, being determined by a small numberof loci.The mechanisms of decreased resistance to T.i. are not
known. It is known that increased susceptibility to
chronic dermatophytoses is associated with atopy, and
immunological mechanisms have been suggested to
account for it.’ The immunological status of the GogolValley patients and their non-affected sibs will be exa-mined. Although we suspect that an immunologicalmechanism is responsible for the inherited susceptibilitydemonstrated, it is possible that its basis is biochemicalin that the patients’ sweat or skin composition favoursthe growth of Trichophyton concentricum more thanthat of normal people. If this is so then the biochemicalvariation must be inherited in a mendelian recessivefashion.
REFERENCES
1. Dompmartin, D. S. P. c. q. Bull. 1976, 26, 30.2. da Fonseca, O. in Essay on Tropical Dermatology (edited by J. Marshall);
vol. 2, p. 339. Amsterdam, 1972.3. Schofield, F. D., Parkinson, A. D., Jeffrey, D. Trans. R. Soc. trop. Med.
Hyg. 1963, 57. 214.4. McDevitt, H., Bodmer, W. Lancet, 1974, i, 1269.5. Jones, H. E., Reinhardt, J. H., Rinaldi, M. G. Archs Derm. 1974, 110, 213.6. Miller, M. E., Norman, M. E., Koblenzer, P. J., Schonauer, R. A. J. Lab.
clin. Med. 1973, 82, 1.7. Z’Graggen, J. A. Pacific Linguistics, Ser. D. 1973, 25.8. Smith, C. A. B. Ann. Hum. Genet. 1956, 20, 257.9. Brewerton, D. A., Caffrey, M., Nicholls, A., Walters, D., Oates, J. K., James,
D. C. O. Lancet, 1973, ii, 996.
SUBCUTANEOUS FAT IN NEWBORN INFANTSOF DIABETIC MOTHERS: AN INDICATION OF
QUALITY OF DIABETIC CONTROL
ANDREW WHITELAW
Department of Child Health, Institute of Child Health,University of London
Summary Biceps, triceps, subscapular, and supra-iliac skinfolds were measured in 40
newborn infants of diabetic mothers. Maternal fastingblood-glucose and mean blood-glucose in the thirdtrimester correlated significantly with neonatal skinfoldthickness. Skinfold measurement, when compared witha reference range for gestational age, may be a con-venient way of assessing one effect of maternal diabeteson the fetus. Gluteal adipose-cell diameter was measuredin 31 infants of diabetic mothers. The fattest babies hadthe largest adipose cells and there was a significant posi-tive correlation between maternal fasting blood-glucoseand neonatal adipose cell diameter. These findings areconsistent with the hypothesis that in diabetic preg-nancy fetal hyperglycæmia and hyperinsulinism stimu-late increased triglyceride synthesis in adipose cells andenlargement of adipose cells and lead to an increase infetal subcutaneous fat.
Introduction
INFANTS of diabetic mothers tend to have more adi-
pose tissue than normal at birth and this is thought tobe caused by fetal hyperglycaemia and hyperinsulinism.’ 1Pedersen2 suggested that neonatal body fat should beregarded as a criterion by which to judge the treatmentof maternal diabetes mellitus. An increase in adipose tis-sue may result from enlargement of adipose cells, an in-crease in the number of adipose cells, or a combinationof both processes. Salans et a1. found that baby ratsgiven insulin developed enlarged adipose cells with noincrease in the number of cells.
,
The present study was designed to determine whetherthere is a connection between maternal blood-glucoseconcentrations and subcutaneous fat in newborn infantsas measured by skinfold and size of adipose cell.
Patients
I examined 40 infants of mothers with established diabetesmellitus or gestational diabetes (two-hour 50 g oral glucosetolerance test result above 6-7 mmoJ;14) within seventy-twohours of birth. z
,
14 mothers did not require insulin in pregnancy, and thusbelonged to class A of White’s classification.’ 16 mothers
belonged to class B (onset of diabetes after twenty years of age,and requiring insulin in pregnancy), and 7 to class C (onset ofdiabetes before twenty years of age). There was 1 mother eachin class D (diabetes for more than twenty years), class F (dia-betic nephropathy), and class R (diabetic proliferative retino-pathy). The infants were delivered at six hospitals in Lon-don-Queen Charlotte’s Maternity Hospital, St Mary’sHospitals at Praed Street and Harrow Road, Middlesex Hospi-tal, Central Middlesex Hospital, and Hammersmith Hospital.
Usually mothers on insulin therapy were admitted to hospi-tal some weeks before the expected date of delivery, for blood-glucose monitoring and adjustment of insulin dosage and diet.Venous blood-glucose samples were taken at intervals duringday and night, although the frequency of blood-sampling var-ied. Some of the mothers with gestational diabetes not treated





























