Embed Size (px)
Citation preview
Avian and Pandemic InfluenzaVaccine Development
John TreanorProfessor of Medicine
University of Rochester Medical CenterRochester, NY

Options for Pandemic Vaccines
• Inactivated vaccine resembling currently licensed inactivated vaccine
• Live vaccine resembling currently licensed live vaccine
• Inactivated vaccines with experimental adjuvants/route of administration
• Experimental approaches

Inactivated Vaccine Approach
• Proven technology
– Used successfully in 1957 and 1968
– Efficacy data exist for both pandemic and interpandemic years
– Large experience with clinical use
• Largest existing manufacturing capacity
• Licensing would be relatively straight-forward

Inactivated Vaccine Approach
• Unlikely to induce mucosal immunity
• Protection may be strain specific
• Requires multiple doses
• Manufacturing capacity limited by availability of eggs and capacity for expansion limited
Evaluation of Unadjuvanted Inactivated H5 Influenza Vaccines
• Avoid cleavage
– Duck Singapore/97 (H5N3)
– Recombinant, baculovirus-expressed HA of A/Hong Kong/156/97 (rH5)
– Subvirion rgA/Vietnam/1203/04 vaccine (H5N1)
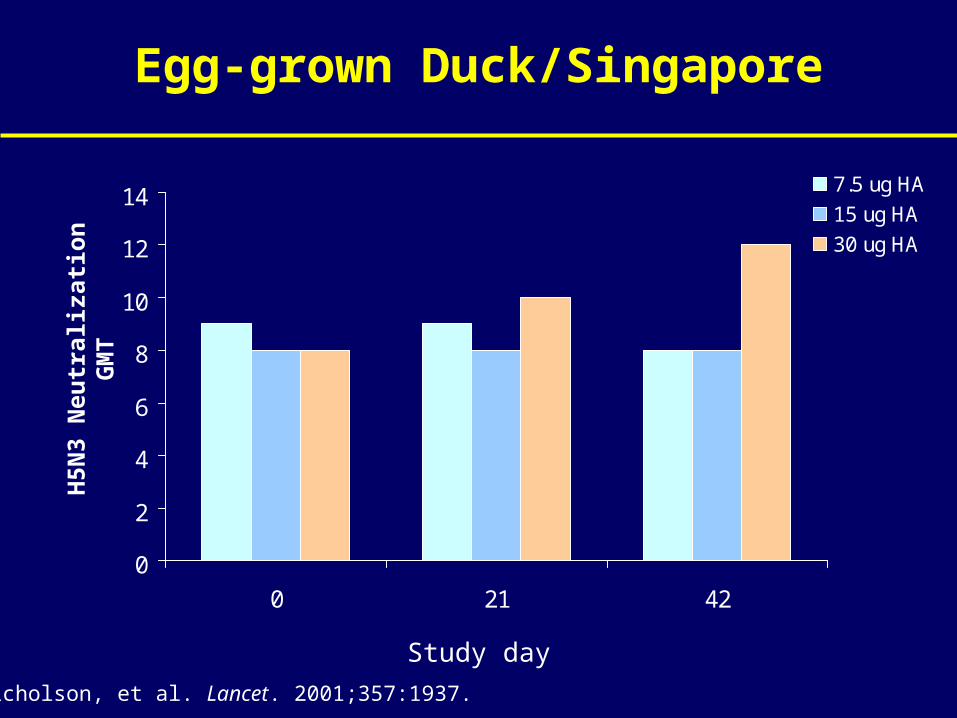
Egg-grown Duck/Singapore
0
2
4
6
8
10
12
14
0 21 42
7.5 ug HA
15 ug HA
30 ug HA
Nicholson, et al. Lancet. 2001;357:1937.
Study day
H5N
3 N
eutr
aliz
atio
n G
MT
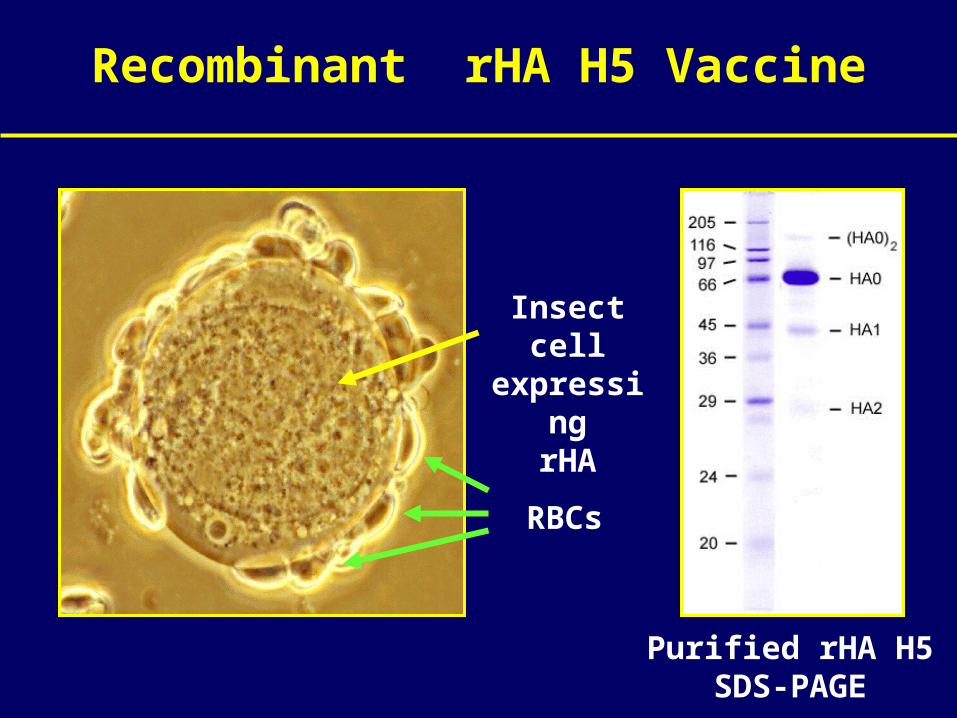
Recombinant rHA H5 Vaccine
Insect cell expressing
rHA
RBCs
Purified rHA H5SDS-PAGE
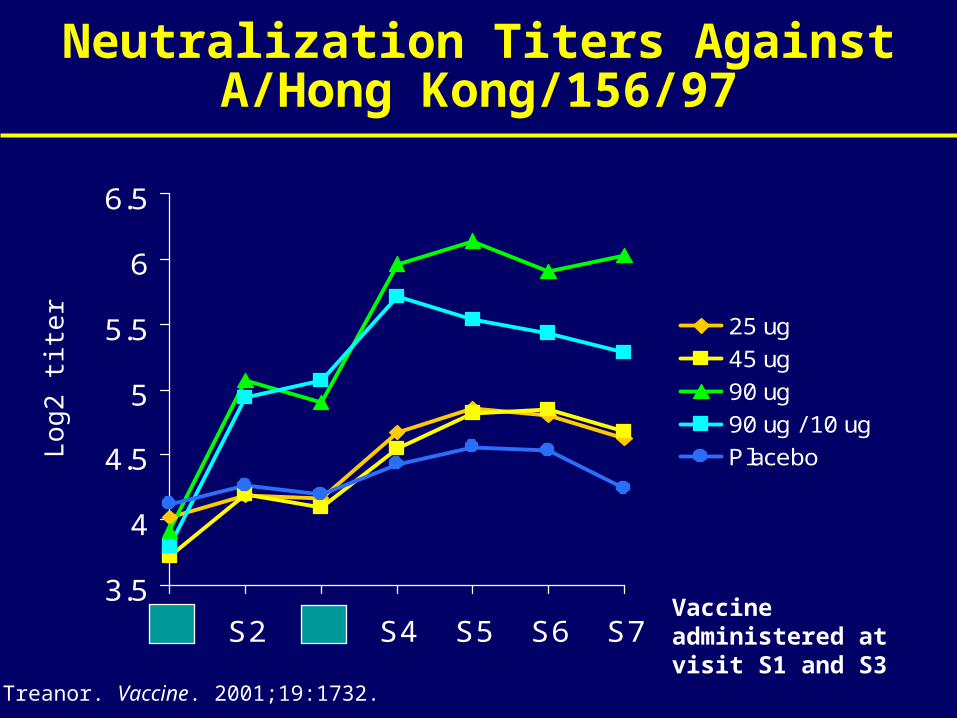
Neutralization Titers Against A/Hong Kong/156/97
3.5
4
4.5
5
5.5
6
6.5
S1 S2 S3 S4 S5 S6 S7
25 ug
45 ug
90 ug
90 ug / 10 ug
Placebo
Log
2 ti
ter
Treanor. Vaccine. 2001;19:1732.
Vaccine administered at visit S1 and S3
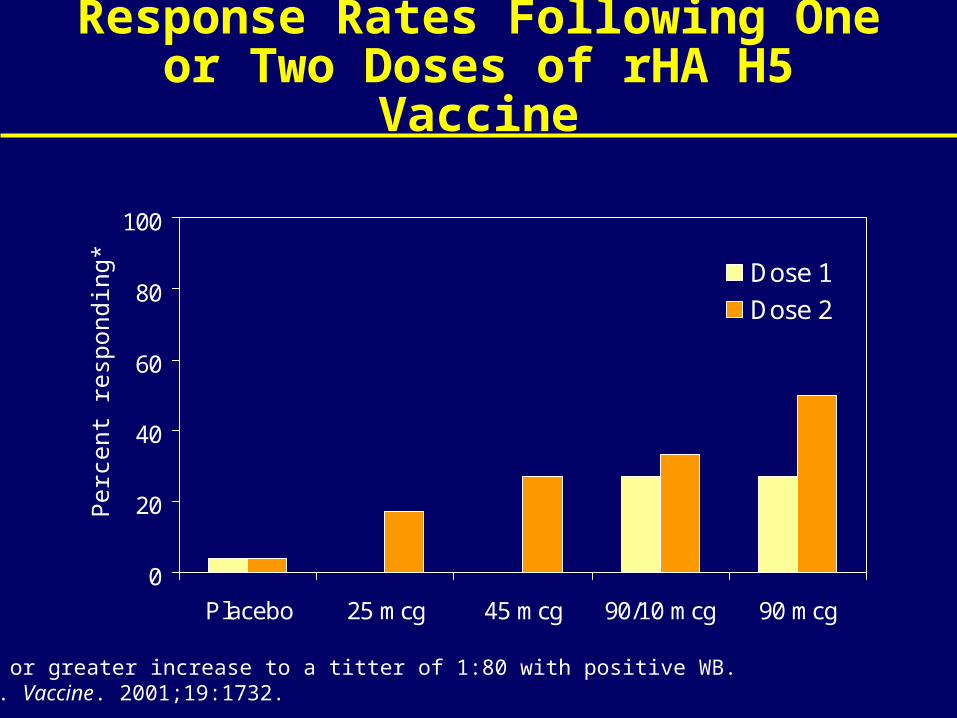
Response Rates Following One or Two Doses of rHA H5 Vaccine
0
20
40
60
80
100
Placebo 25 mcg 45 mcg 90/10 mcg 90 mcg
Dose 1
Dose 2
Per
cent
res
pond
ing*
*4-fold or greater increase to a titter of 1:80 with positive WB.Treanor. Vaccine. 2001;19:1732.
Evaluation of rgA/Vietnam/1203/04 (H5N1) Subvirion Vaccine (DMID 04-063)
• Subjects: Healthy adults ages 18 to 64
• Design: Prospective, randomized, double blind
• Interventions: Two IM doses H5 vaccine separated by 28 days
– Placebo, 7.5 mcg, 15 mcg, 45 mcg, 90 mcg
– 1:2:2:2:2 randomization
• Endpoints
– Safety: solicited and unsolicited AEs
– Immunogenicity: neutralizing titer of 1:40
DMID 04-063: Preliminary Results
• Vaccine was well tolerated at all doses
• Dose related local pain and tenderness
• Some neutralizing responses seen at all doses
• Best responses seen at highest doses – only 45 mcg and 90 mcg gave “acceptable” responses
• Results are very consistent with previous evaluation of rHA H5 vaccine
Strategies to Overcome Poor Responsiveness
• Booster strategies – include vaccine in annual vaccination, prime population
• Adjuvant strategies – add adjuvants with dose sparing potential
• Alternative routes of administration strategies
Strategies to Overcome Poor Responsiveness
• Booster strategies – include vaccine in annual vaccination, prime population
• Adjuvant strategies – add adjuvants with dose sparing potential
• Alternative routes of administration strategies
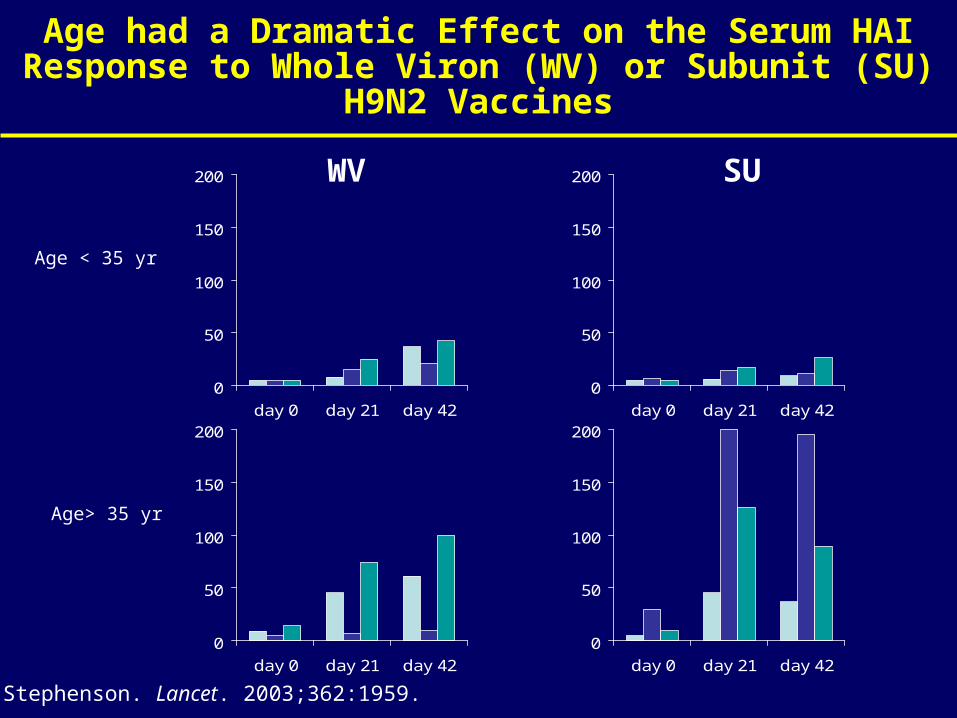
Age had a Dramatic Effect on the Serum HAI Response to Whole Viron (WV) or Subunit (SU) H9N2 Vaccines
0
50
100
150
200
day 0 day 21 day 42
0
50
100
150
200
day 0 day 21 day 42
0
50
100
150
200
day 0 day 21 day 42
0
50
100
150
200
day 0 day 21 day 42
Age < 35 yr
Age> 35 yr
WV SU
Stephenson. Lancet. 2003;362:1959.
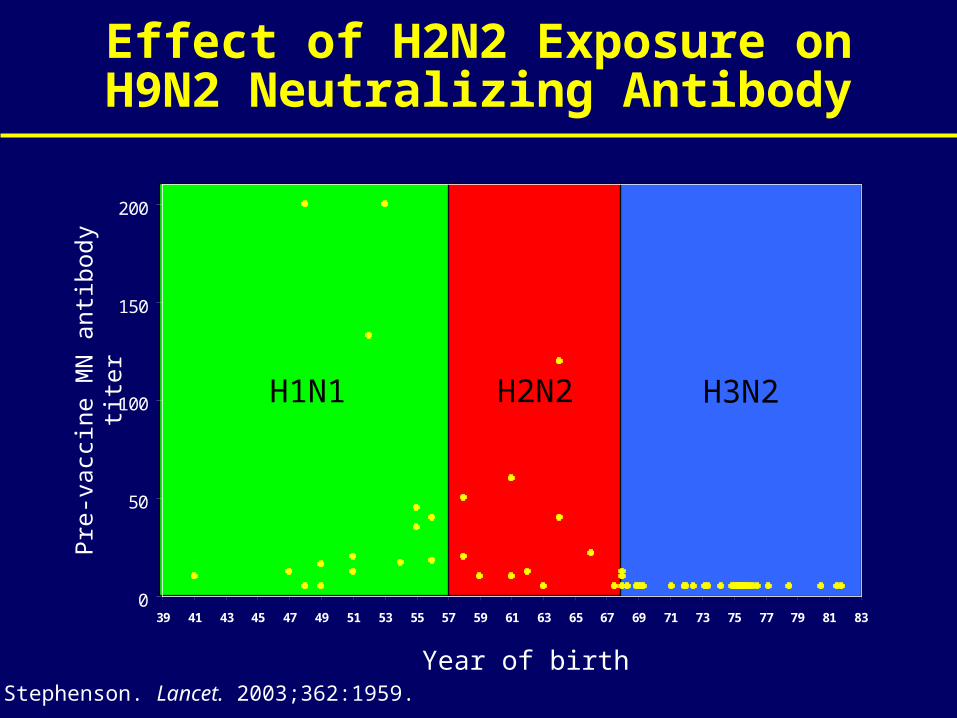
H1N1 H2N2 H3N2
0
50
100
150
200
39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 81 83
Effect of H2N2 Exposure on H9N2 Neutralizing Antibody
Year of birthStephenson. Lancet. 2003;362:1959.
Pre
-vac
cine
MN
ant
ibod
y tit
er
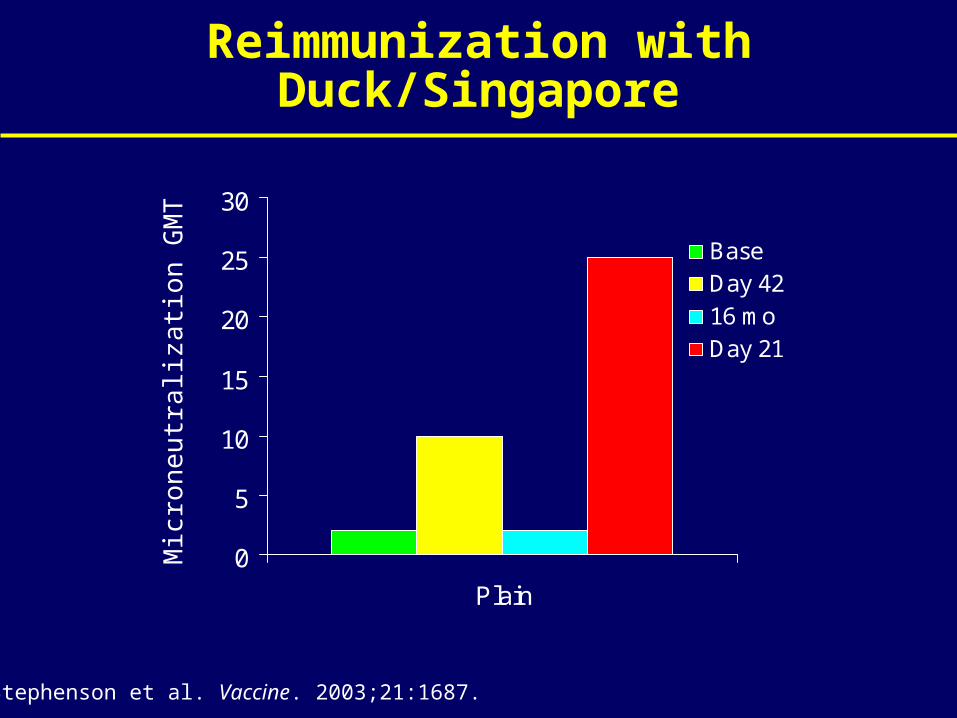
Reimmunization with Duck/Singapore
0
5
10
15
20
25
30
Plain
BaseDay 4216 moDay 21
Mic
ron
eu
tra
liza
tion
GM
T
Stephenson et al. Vaccine. 2003;21:1687.
Booster Strategies
• DMID 05-043: Boosting of subjects who have previously received rH5 with rgA/VN/1203/04
• DMID 05-090: Boosting subjects in 04-063 with a third dose at 6 months
• Proposed: interaction studies with TIV
Strategies to Overcome Poor Responsiveness
• Booster strategies – include vaccine in annual vaccination, prime population
• Adjuvant strategies – add adjuvants with dose sparing potential
• Alternative routes of administration strategies
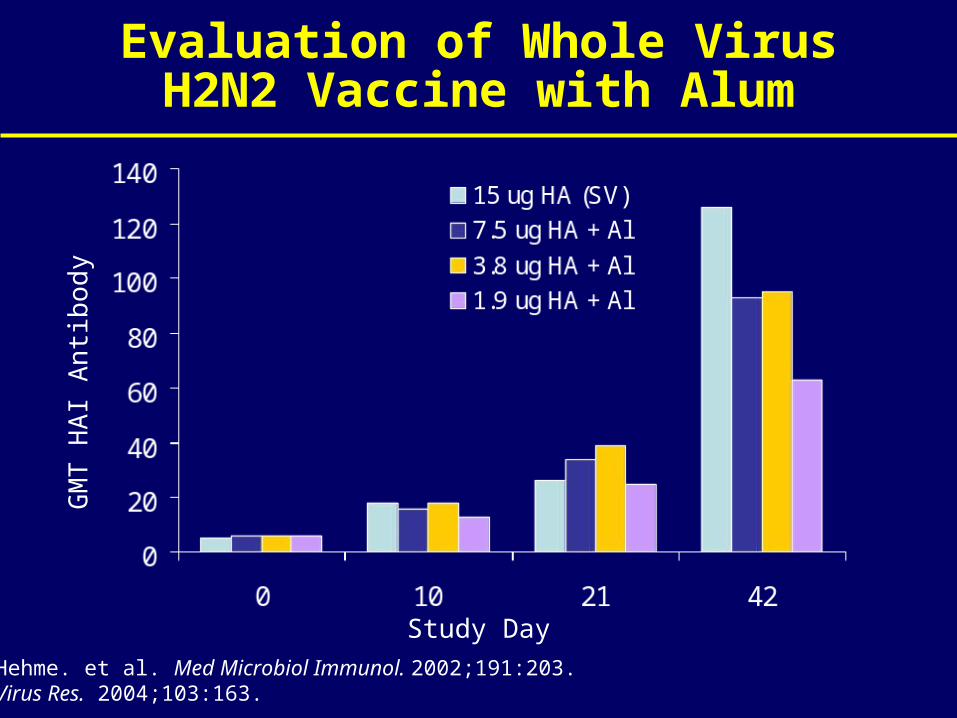
Evaluation of Whole Virus H2N2 Vaccine with Alum
Study Day
GM
T H
AI A
ntib
ody
Hehme. et al. Med Microbiol Immunol. 2002;191:203. Virus Res. 2004;103:163.
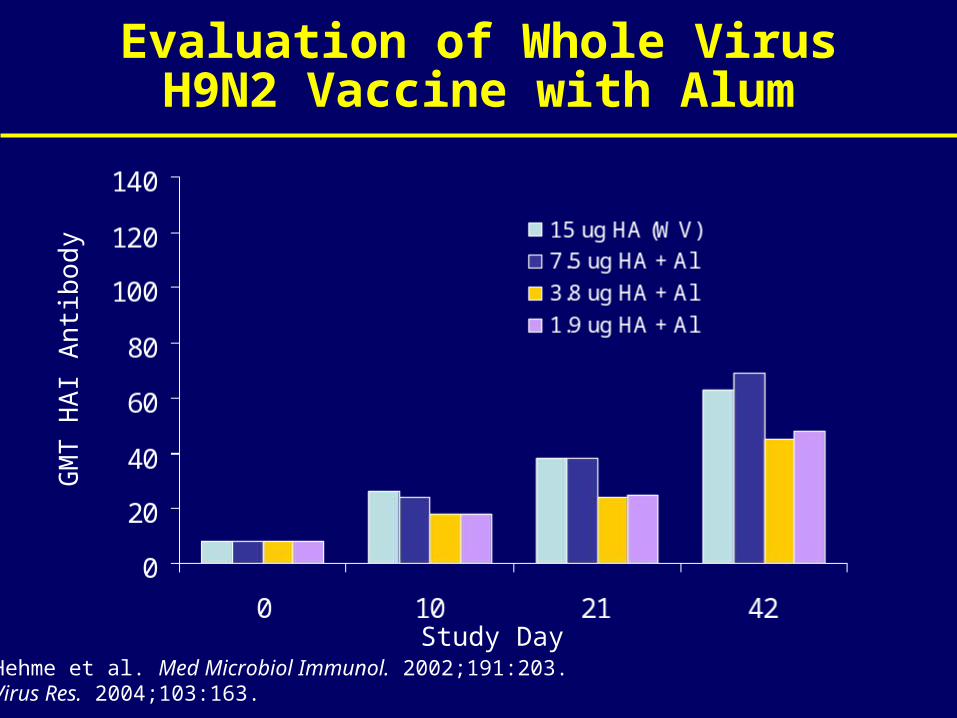
Evaluation of Whole Virus H9N2 Vaccine with Alum
Study Day
GM
T H
AI A
ntib
ody
Hehme et al. Med Microbiol Immunol. 2002;191:203. Virus Res. 2004;103:163.
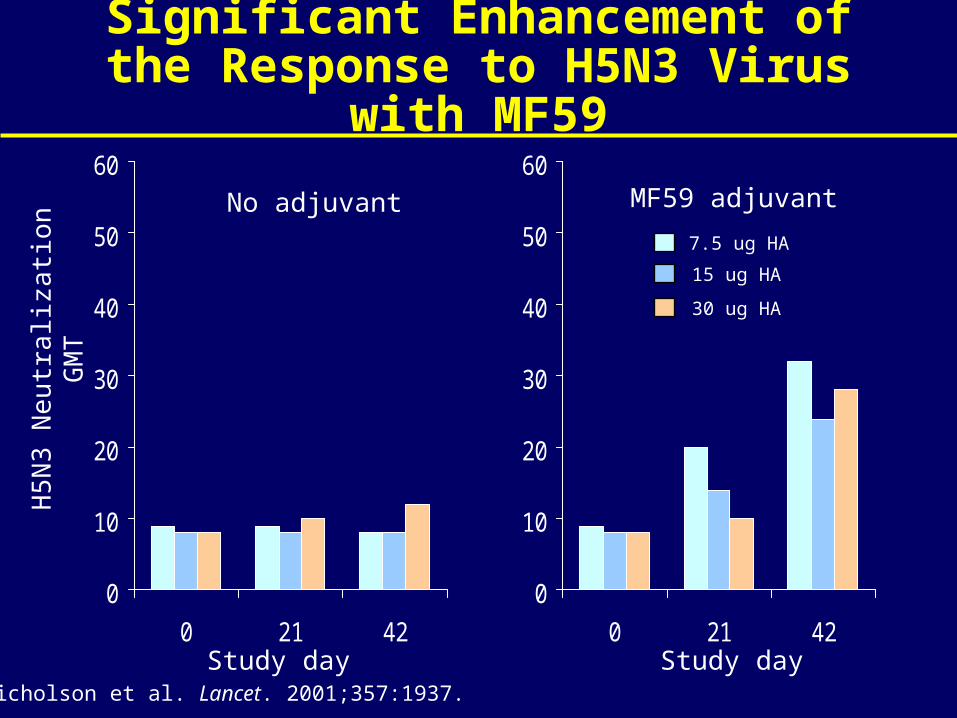
Significant Enhancement of the Response to H5N3 Virus with MF59
0
10
20
30
40
50
60
0 21 42
0
10
20
30
40
50
60
0 21 42
Nicholson et al. Lancet. 2001;357:1937.
No adjuvant MF59 adjuvant
Study day Study day
H5
N3
Ne
utra
lizat
ion
GM
T
7.5 ug HA
15 ug HA
30 ug HA
Adjuvant Strategies
• Alum– H5 formulation – 30 mcg dose met EMEA criteria
– H1, H3 vaccines – little enhancement seen in either pandemic or non-pandemic setting
– Study – DMID 05-0127 dose ranging H5 on constant alum in healthy adults
• MF59– Modest enhancement with TIV
– Promising results with H5 vaccines, no obvious dose-response relationship, ? Stochiometry
– DMID 04-019: significant enhancement of H9 response
– Issues: availablility, intellectual property
• Others: MPL, CPG
Strategies to Overcome Poor Responsiveness
• Booster strategies – include vaccine in annual vaccination, prime population
• Adjuvant strategies – add adjuvants with dose sparing potential
• Alternative routes of administration strategies
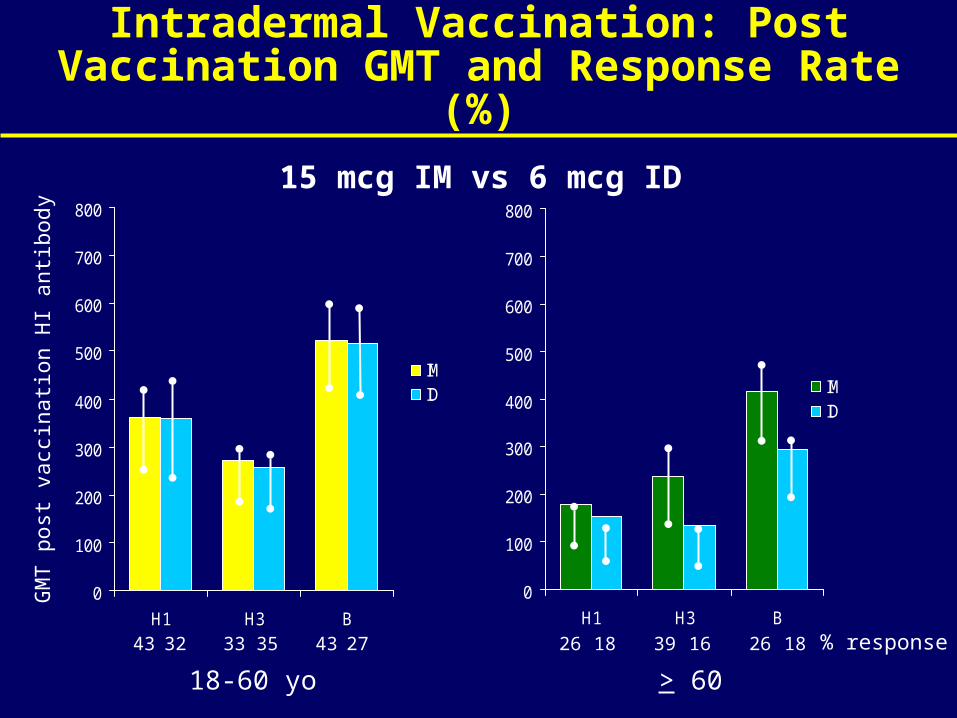
Intradermal Vaccination: Post Vaccination GMT and Response Rate (%)
0
100
200
300
400
500
600
700
800
H1 H3 B
IMID
0
100
200
300
400
500
600
700
800
H1 H3 B
IMID
GM
T p
ost v
acci
natio
n H
I ant
ibod
y
18-60 yo > 60
43 32 33 35 43 27 26 18 39 16 26 18 % response
15 mcg IM vs 6 mcg ID

Evaluation of Live Attenuated Vaccines (CAIV)
• H9 and H5 candidates generated, in clinical trials
• Highly immunogenic in susceptible populations
– Critical need to define correlates of immunity
• Potential use of low doses
– Studies should evaluate full range
• Induction of mucosal immunity might reduce transmission
– Development of challenge models
Evaluation of Live Attenuated Vaccines (CAIV)
• Potential cross protection
– Evaluate responses to range of antigenic variants
• Not licensed in all populations
– Critical need to expand safety database
– Define correlates of immunity that could be extended to elderly
• Concerns regarding transmission and reassortment
– Clearly define conditions of deployment, expected shedding patterns, and biologic behavior of reassortants
Experimental Approaches
• Nasal inactivated vaccines
• Cross protective peptides/epitopes
• Virus-like particles
• Alternative live vaccines
• Vectored approaches
• DNA Vaccines
Considerations for Alternate Approaches
• Validation in clinical studies
• Extensive safety evaluation
• Specific markers of efficacy
• Individualized development strategy
• Need for early determination of potential advantages against conventional approaches
Critical Issues
• Is the H5 HA intrinsically less immunogenic?
– Mechanism unclear
• Can cross-protective immune responses be generated?
– M2 based immunity
– Cross protective epitopes
– CTL approaches