Embed Size (px)
Citation preview
Journal of the American College of Cardiology Vol. 63, No. 19, 2014� 2014 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2014.02.581
Heart Valve Disease
B-Type Natriuretic PeptideClinical Activation in Aortic Stenosis
Impact on Long-Term SurvivalMarie-Annick Clavel, DVM, PHD, Joseph Malouf, MD, Hector I. Michelena, MD,
Rakesh M. Suri, MD, DPHIL, Allan S. Jaffe, MD, Douglas W. Mahoney, MS,
Maurice Enriquez-Sarano, MD
Rochester, Minnesota
From the D
Rochester,
Canadian I
Diagnostics
and the Sor
Edwards Lif
Objectives T
ivision of Cardiovascular
Minnesota. Dr. Clavel
nstitute of Health Resea
and St. Jude Medical; ha
in Group; and has receiv
esciences, St. Jude Medica
his study was conducted to define the association between serum B-type natriuretic peptide (BNP) activationand survival after the diagnosis of aortic stenosis (AS).
Background In
AS, the link between BNP levels and clinical outcome is in dispute. Failure to account for the normal shiftingof BNP ranges with aging in men and women, not using hard endpoints (survival), and not enrolling large seriesof patients have contributed to the uncertainty.Methods A
program of prospective measurement of BNP levels with Doppler echocardiographic AS assessment during thesame episode of care was conducted. BNP ratio (measured BNP/maximal normal BNP value specific to age andsex) >1 defined BNP clinical activation.Results In
1,953 consecutive patients with at least moderate AS (aortic valve area 1.03 � 0.26 cm2; mean gradient36 � 19 mm Hg), median BNP level was 252 pg/ml (interquartile range: 98 to 592 pg/ml); BNP ratio 2.46(interquartile range 1.03 to 5.66); ejection fraction (EF) 57% � 15%, and symptoms present in 60% of patients.After adjustment for all survival determinants, BNP clinical activation (BNP ratio >1) independently predictedmortality after diagnosis (p < 0.0001; hazard ratio [HR]: 1.91; 95% CI: 1.55 to 2.35) and provided incrementalpower to the survival predictive model (p < 0.0001). Eight-year survival was 62 � 3% with normal BNP levels, 44 �3% with BNP ratio of 1 to 2 (adjusted HR: 1.49; 95% CI: 1.17 to 1.90), 25 � 4% with BNP ratio of 2 to 3 (adjustedHR: 2.12; 95% CI: 1.63 to 2.75), and 15 � 2% with BNP ratio of �3 (adjusted HR: 2.43; 95% CI: 1.94 to 3.05). Thisstrong link to survival was confirmed in asymptomatic patients with normal EF (adjusted HR: 2.35 [95% CI: 1.57 to3.56] for BNP clinical activation and 2.10 [95% CI: 1.32 to 3.36] for BNP ratio of 1 to 2, 2.25 [95% CI: 1.31 to 3.87]for BNP ratio of 2 to 3, 3.93 [95% CI: 2.40 to 6.43] for BNP ratio of �3). Aortic valve replacement was associatedwith survival improved by a similarly high margin (p ¼ 0.54) with BNP ratio of <2 (HR: 0.68; 95% CI: 0.52 to 0.89;p ¼ 0.003) or BNP ratio of >2 (HR: 0.56; 95% CI: 0.47 to 0.66; p < 0.0001).Conclusions In
this large series of patients with AS, BNP clinical activation was associated with excess long-term mortalityincrementally and independently of all baseline characteristics. Higher mortality with higher BNP clinical activation,even in asymptomatic patients, emphasizes the importance of appropriate clinical interpretation of BNP levels inmanaging patients with AS. (J Am Coll Cardiol 2014;63:2016–25) ª 2014 by the American College of CardiologyFoundationSee page 2026
Plasma levels of B-type natriuretic peptide (BNP) havebeen shown to be predictive of outcome and to be clinicallyuseful in diagnosis, management, and risk stratificationof cardiovascular diseases such as heart failure and acutecoronary syndromes (1–4). In aortic stenosis (AS), pilotstudies have suggested that BNP levels may be related to
Diseases and Internal Medicine, Mayo Clinic,
holds a post-doctoral fellowship grant from
rch. Dr. Suri is a board member of Abbott
s served as a consultant for Abbott Diagnostics
ed research funding from Abbott Diagnostics,
l, and the Sorin Group. Dr. Jaffe presently or in
disease severity, symptoms, and mixed measures of outcome(5–10), but a recent prospective analysis raised a concernthat these presumptive outcome implications may have been
the past has served as a consultant for Abbott Diagnostics, Alere Diagnostic Systems,
Amgen, Beckman Coulter, Critical Diagnostics, Heart.org, Ortho Diagnostics,
Radiometer Medical, and Trinity Biotech. All other authors have reported that they
have no relationships relevant to the contents of this paper to disclose.
Manuscript received November 6, 2013; revised manuscript received February 15,
2014, accepted February 25, 2014.

Abbreviationsand Acronyms
AS = aortic stenosis
AVA = aortic valve area
AVR = aortic valve
replacement
BNP = B-type natriuretic
peptide
LVEF = left ventricular
ejection fraction
JACC Vol. 63, No. 19, 2014 Clavel et al.May 20, 2014:2016–25 BNP and Survival in Aortic Stenosis
2017
overemphasized (11). Survival association with BNP levelswas analyzed in very small sets of mostly symptomatic pa-tients (9,12,13) and thus remains undefined. Another sourceof uncertainty is that these pilot studies used different assaysand forms of BNP that are not well harmonized (6–9).Considerably different absolute thresholds proposed in thesestudies to stratify risk may reflect low power in small, variablyselected patient populations with short follow-up or mayreflect the instability of soft outcome endpoints (aortic valvereplacement, symptom onset, or combined endpointof variable cardiac events). Furthermore, normal values ofBNP for age and sex were not taken into account to affirmBNP clinical activation in excess of the normal range. Thus,the use of BNP as a marker of AS outcome has not beenadequately validated for use in clinical practice and is notrecommended in guidelines (14,15).
Obtaining objective markers of outcome is crucial in AS.Indeed, AS is frequent (16) and is the most common valvulardisease referred for valve replacement (17), which is the onlyeffective AS treatment (14,15), including transcutaneousinsertion (15). The role of symptom onset has been empha-sized (18,19), but epidemiological changes, with the currentpredominance of degenerative AS, are characterized byelderly patients being predominantly affected and in whomevaluation and interpretation of symptoms is challenging(20). Therefore, objective markers of risk are crucial in thatenvironment; as such, BNP could play an essential role in riskstratification. For that purpose, it is essential to account forthe shifting normal BNP range with aging and specific toeach sex and to assess a hard endpoint, particularly mortality,requiring a large cohort of patients diagnosed with AS.
Thus, the objectives of our study were to assess the linkbetween BNP values measured at diagnosis, particularlyBNP clinical activation (accounting for the normal BNPrange specific to each patient) and mortality followingthe diagnosis of moderate or severe AS, and to examinethe hypothesis that BNP clinical activation independentlypredicts excess mortality after adjustment for all baselinecharacteristics, even in asymptomatic patients. A secondaryhypothesis examined was that higher levels of activation areassociated with more severe outcomes.
Methods
Following a pilot study of natriuretic peptides in valvularheart diseases (21,22), we initiated a program of prospectiveand systematic measurement of BNP levels with compre-hensive Doppler echocardiographic evaluation of valve dis-eases performed during the same episode of care. For thepurpose of the present study, we gathered 1,953 consecutivepatients who were diagnosed with moderate or severe ASbased on aortic valve area (AVA) of �1.5 cm2 by Dopplerechocardiography and who underwent this combined clin-ical, hormonal, and Doppler echocardiographic assessment.Patients with known rheumatic valve disease (clinically and/or echocardiographically); congenital heart disease (except
overt or unknown bicuspid valveor patent foramen ovale); previ-ous valvular surgery; acute myo-cardial infarction within 8 weekspreceding AS diagnosis; atrialfibrillation with rapid ventricularresponse; history or current en-docarditis; pericarditis with orwithout tamponade; sepsis; se-vere liver, kidney, or brain diseaseexcept old stroke; hyperparathy-roidism; or Cushing disease were
excluded. Non-U.S. citizens were excluded to ensure ho-mogeneous Social Security death data. The study wasapproved by our institutional review board.Clinical data. Clinical data were collected by the patients’personal physicians during the same episode of care as theDoppler echocardiographic and hormonal assessment. TheCharlson score index was calculated as previously published(23). Symptomatic patients presented with syncope or nearsyncope, dyspnea, and/or probable or classic angina.Doppler echocardiography. All patients underwentcomprehensive Doppler echocardiography using standardultrasound systems, including interrogation from all possiblewindows (24). All measurements and calculations were per-formed as recommended by echocardiographic societies’recommendations (25). After measurement in systole ofaortic annulus diameter, flow velocity and time velocity in-tegral of left ventricular outflow tract by pulsed-waveDoppler, and AS jet by continuous-wave Doppler, wemeasured peak jet velocity and mean gradient and calculatedAVA by continuity equation as an absolute value and indexedto body surface area. AS severity was graded according tocurrent guidelines (14) and recent community studies (20)as moderate AS with AVA of 1.0 to 1.5 cm2 or severe ASwith AVA of �1.0 cm2.Laboratory data. Venous blood samples were drawn froman antecubital vein into chilled ethylenediaminetetraaceticacid Vacutainer test tubes (Becton, Dickinson and Com-pany, Franklin Lakes, New Jersey). Plasma separation wasimmediately performed at �4�C, and plasma samples werefrozen at �70�C until assay. Plasma BNP levels weredetermined by immunoenzymatic assay (Triage, Biosite Inc.,San Diego, California) within 3 days. The ratio betweenmeasured serum BNP level and maximal normal BNP levelfor age and sex (BNP ratio) was calculated for each patient(26). The maximal normal values of BNP specific to age andsex were derived from Mayo Clinic laboratory procedures.Patients with elevated BNP levels (i.e., BNP ratio >1) wereconsidered as displaying BNP clinical activation.Endpoints. The primary endpoint of this study was theoverall mortality after diagnosis, and the secondary endpointwas mortality under medical treatment. This secondaryendpoint was assessed in the whole cohort with censoring atthe time of aortic valve replacement (AVR) if performed.Due to the large size of our series, we elected to follow up
Table 1 Baselines Characteristics of the Population
Whole Cohort(n ¼ 1,953)
AsymptomaticIsolated AS Group*
(n ¼ 565)
Clinical data
Age, yrs 76 � 12 74 � 13
Male 1,081 (55) 310 (55)
Body mass index, kg/m2 28.9 � 6.4 28.0 � 5.8
Body surface area, m2 1.91 � 0.25 1.89 � 0.23
Diastolic blood pressure, mm Hg 68.6 � 11.8 68.8 � 10.4
Systolic blood pressure, mm Hg 127.0 � 20.6 128.6 � 19.3
Heart rate, beat/min 71 � 14 68 � 13
Atrial fibrillation 365 (20) 62 (11)
Diabetes 595 (30) 141 (25)
Hypertension 1,355 (70) 357 (63)
Old myocardial infarction 398 (20) 0
Chronic pulmonary disease 629 (32) 130 (23)
Chronic kidney disease 699 (36) 137 (24)
Previous open-heart surgery 132 (7) 23 (4)
Charlson comorbidity index 4.2 � 3.6 3.1 � 3.2
Symptoms 1165 (60) 0
Blood sample data
BNP, pg/ml 252 (98–592) 138 (58–324)
BNP ratio 2.46 (1.03–5.66) 1.42 (0.63–3.1)
Activated BNP 1472 (75) 347 (61)
Creatinine, mg/dl 1.2 (1.0–1.4) 1.1 (0.9–1.3)
Hemoglobin, g/dl 12.8 (11.4–14.1) 13.4 (12.0–14.5)
Echocardiographic data
LV end-diastolic diameter, mm 49.9 � 7.2 47.7 � 5.4
LV end-systolic diameter, mm 33.2 � 9.1 29.3 � 4.9
Peak aortic jet velocity, m/s 3.78 � 0.95 3.94 � 0.95
Mean gradient, mm Hg 36 � 19 39 � 19
AVA, cm2 1.03 � 0.26 1.04 � 0.26
AVAi, cm2/m2 0.55 � 0.15 0.55 � 0.14
LV ejection fraction, % 57 � 15 65 � 7
LV ejection fraction <50% 414 (22) 0
Values are mean � SD, n (%), or median (interquartile range). *Asymptomatic isolated AS groupwas defined as asymptomatic AS with normal ejection fraction and no previous myocardialinfarction.AS ¼ aortic stenosis; AVA ¼ aortic valve area; AVAi ¼ indexed aortic valve area; BNP ¼ B-type
natriuretic peptide; LV ¼ left ventricular.
Clavel et al. JACC Vol. 63, No. 19, 2014BNP and Survival in Aortic Stenosis May 20, 2014:2016–25
2018
on patients using electronic records of events from internalcomputerized databases and from the Social Security DeathIndex. For maximizing interrogation of the central SocialSecurity Death Index database, a multiple demographiclist (such as first and last name, date of birth, and SocialSecurity number) and a delay of 1 year between interrogationand closing follow-up date were used (27,28).Statistical analysis. Results are expressed as mean � SD,median with interquartile range, or percentage when appro-priate. Continuous variables were tested for distributionnormality with the Shapiro-Wilk test. Because BNP absolutevalues and BNP ratio were not normally distributed, naturallog transformations of BNP and BNP ratio were used forBNP continuous variable analyses (unless otherwise specified).BNP ratio was also categorically analyzed. Analysis of survivalused patients with normal BNP levels as reference comparedwith those with BNP clinical activation overall or stratifiedinto 3 groups (1 to 2, 2 to 3, or �3), or quintiles of elevatedBNP ratio distribution.
Univariable and multivariable models used Cox propor-tional hazards for survival analysis. To analyze BNP incre-mental value, we defined a background model to predictmortality including age, sex, body surface area, atrial fibril-lation, Charlson score index, symptoms, creatinine level,hemoglobin level, systolic blood pressure, indexed AVA, andleft ventricular ejection fraction (LVEF). All variables in theCox models verified the proportional hazards assumption onthe basis of inspection of trends in the Schoenfeld residuals(all p > 0.15). AVR was used as a time-dependent covariatein the multivariable Cox proportional hazards models. Thetime between diagnosis and AVR was considered as medicaltreatment follow-up. Using age, sex, creatinine level, he-moglobin level, LVEF, mean gradient, indexed AVA, atrialfibrillation, systolic blood pressure, body surface area, coro-nary artery disease, previous myocardial infarction, hyper-tension, previous open heart surgery, diabetes, renal disease,and symptoms, we calculated case-weight estimation with alogistic regression model to predict the inverse probability ofhaving an AVR. With this inverse probability of treatmentweighting, baseline characteristics were compared betweenpatients with and without AVR during follow-up with theuse of weighted Student t test or weighted Wilcoxon rank-sum test for continuous variables and weighted chi-squaretest or Fisher exact test for categorical variables, as appro-priate. Inverse probability-weighted Cox multivariablemodels were used to analyze potential impact of AVR overalland stratified by BNP ratio <2 or �2.
BNP additional impact on survival after diagnosis wasanalyzed by adding BNP (expressed as a continuous orcategorical variable) to the background survival model andassessing model incremental power using the likelihood ratiotest. Survival models are presented with BNP hazard ratio(HR) and 95% CI.
A p value <0.05 was considered statistically significant.Statistical analyses were performed with JMP 9.1 and SPSS20.0 software.
Results
Baseline characteristics. The baseline characteristics ofthe entire cohort are presented in Table 1, left column.Consistent with typical characteristics of patients diag-nosed with moderate to severe AS, age was 76 � 12 yearsand 1081 (55%) patients were male. With LVEF of 57 �15%, the AS characteristics were coherent with AVA was1.03 � 0.26 cm2, mean gradient 36 � 19 mm Hg andpeak velocity 3.78 � 0.95 m/s. In term of comorbidity,prevalence of hypertension (70%), atrial fibrillation (20%),diabetes (30%), chronic pulmonary disease (32%), andchronic kidney disease (36%) were as expected in a popu-lation of that age. Median (interquartile range) of BNPwas 252 (98 to 592) pg/ml and that of BNP ratio was2.46 (1.03 to 5.66), with BNP clinical activation notedin 75.4% of patients (20.0% having BNP ratio of 1 to 2,
JACC Vol. 63, No. 19, 2014 Clavel et al.May 20, 2014:2016–25 BNP and Survival in Aortic Stenosis
2019
11.6% 2 to 3, and 43.8% >3). The distribution in quintilesof patients with BNP ratio >1 corresponds to thresholdsof BNP ratio of 1.71, 2.87, 4.78, and 9.28. Among the1,953 patients, 565 (29%) were asymptomatic with pre-served LVEF (i.e., >50%) and no history of myocardialinfarction (Table 1).Clinical activation of BNP and overall survival in thewhole cohort. During a mean follow-up of 3.8 � 2.4years, there were 828 AVRs (1,125 patients had onlyfollow-up under medical management) and 1,070 deaths.Overall survival at 2, 5, and 8 years was 73% � 1%, 49% �1%, and 34% � 2%. In univariable analysis, expressed ascontinuous variables, ln BNP and ln BNP ratio wereassociated with increased overall mortality (HR: 1.68 [95%CI: 1.60 to 1.77; p < 0.0001] and HR: 1.54 [95% CI: 1.47to 1.62; p < 0.0001], respectively). After adjustment for thebackground model, ln BNP (HR: 1.40; 95% CI: 1.31 to1.50; p < 0.0001) or ln BNP ratio (HR: 1.40; 95% CI: 1.31to 1.50; p < 0.0001) was an independent predictor ofmortality after diagnosis. BNP clinical activation as a cat-egorical variable was independently associated with excessmortality (HR: 1.91; 95% CI: 1.55 to 2.35; p < 0.0001).The addition of BNP clinical activation (or the BNP ratioas continuous variable) to the background comprehensivemodel of survival determinants, showed that BNP consid-erably increased model predictive power (p < 0.0001).Moreover, with a higher degree of BNP clinical activation,excess mortality increased markedly. Indeed, analyzed asquintiles of activated BNP, each quintile of abnormal BNPratio was associated with excess mortality versus normalBNP reference group (Fig. 1A) but also showed 40% to60% additional risk of mortality compared with each pre-vious quintile of abnormal BNP ratio (all p � 0.004)(Fig. 2A). Furthermore, upon examination of specificthresholds of BNP clinical activation (Table 2), all activatedsubgroups incurred excess mortality, but the risk increasedfrom BNP ratio 1 to 2 to 2 to 3 to >3 (Figs. 1B and 2B).The adjusted HRs of 1.49 to 2.12 to 2.43 signified that,compared with patients with BNP ratio within the normalrange, those with elevated BNP ratio lower than twicenormal had a 49% increased mortality risk independent ofother baseline characteristics, those with elevated BNP ratio2 to 3 times normal had 112% increased mortality risk,and those with BNP ratio higher than 3 times normal had143% increased mortality risk (Table 2 and Fig. 1B). Sur-vival 8 years after diagnosis was 62 � 3% in patients withBNP ratio within normal range versus 24 � 2% for thosewith BNP clinical activation (p < 0.0001), and survivaldecreased proportionately with higher thresholds of BNPactivation (Fig. 3A). In estimating the therapeutic effect ofAVR, the inverse probability weight was effective at abol-ishing the differences in baseline characteristics betweenpatients who underwent an AVR during follow-up andthose who did not. Within that process, after adjusting forbaseline characteristics, we found that the HR estimate ofAVR benefit (time dependent) was similar in patients with
BNP ratio �2 and those with BNP ratio <2 (HR: 0.56[95% CI: 0.47 to 0.66] vs. HR: 0.68 [95% CI: 0.52 to0.88]; p ¼ 0.54) (Fig. 4), demonstrating that the mortalityincrease in those with markedly elevated BNP ratio wassimilarly palliated by AVR and thus in all likelihood isindeed related to AS.Survival under medical management. When survival un-der medical management was analyzed, the results weresimilar. During a mean follow-up of 2.1 � 2.2 years undermedical management, there were 791 deaths. Overall survivalunder medical management at 2, 5, and 8 years was 68� 1%,38 � 2%, and 21 � 2%. As continuous variables, adjustedfor the background model, ln BNP (HR: 1.41; 95% CI: 1.30to 1.54; p < 0.0001) or ln BNP ratio (HR: 1.41; 1.30-1.54;p < 0.0001) was independently predictive of mortality(Table 2). BNP clinical activation was associated with asimilarly increased mortality under medical management(as overall survival), with adjusted HR of 1.84 (95% CI: 1.44to 2.35; p < 0.0001), and the addition of BNP ratio to themodel markedly increased its predictive power (p < 0.0001).Survival under medical management 8 years after diagnosiswas 49 � 5% in patients without BNP clinical activationversus 13 � 2% for those with BNP clinical activation(p < 0.0001). Strata of clinical activation of BNP manifestedthe same trend for higher mortality risk with medical treat-ment when higher levels of BNP clinical activation werepresent (Table 2).Survival of isolated AS. Patients with isolated AS wereasymptomatic, had no history of myocardial infarction,and had normal LVEF at diagnosis. For these 565 patientswith isolated AS, baseline characteristics were morefavorable than those of the entire series (Table 1), but theresults in terms of link between BNP clinical activationand mortality were similar to those observed in the entireseries. During a mean follow-up of 4.3 � 2.4 years, therewere 265 AVRs and 227 deaths and overall survival at 2, 5,and 8 years was 80 � 2%, 62 � 2%, and 54 � 3%. ln BNPand ln BNP ratio were independent predictors of mortality(both p < 0.0001) (Table 2). BNP clinical activation wasindependently associated with excess mortality (adjustedHR: 2.35; 95% CI: 1.57 to 3.56; p < 0.0001), and additionof BNP clinical activation to the survival model markedlyincreased its predictive power (p < 0.0001). The survival ofisolated AS 8 years after diagnosis was 75 � 4% withoutversus 38 � 4% with BNP clinical activation (p < 0.0001).Survival after diagnosis in the 4 defined strata of BNP clin-ical activation shown in Figure 3B demonstrates widelydivergent survival rates. Adjusted in comprehensive multi-variable models, the degree of BNP clinical activation washighly and progressively associated with survival, as shownin Table 2 (right column), with mortality risk approximatelydoubled versus normal BNP with BNP ratio of 1 to 2,whereas the risk of death approximately quadrupled withBNP ratio �3 (Table 2). When this analysis was restrictedto severe AS (mean gradient >40 mm Hg, peak aortic jetvelocity >4 m/s, or AVA <1.0 cm2), the excess mortality
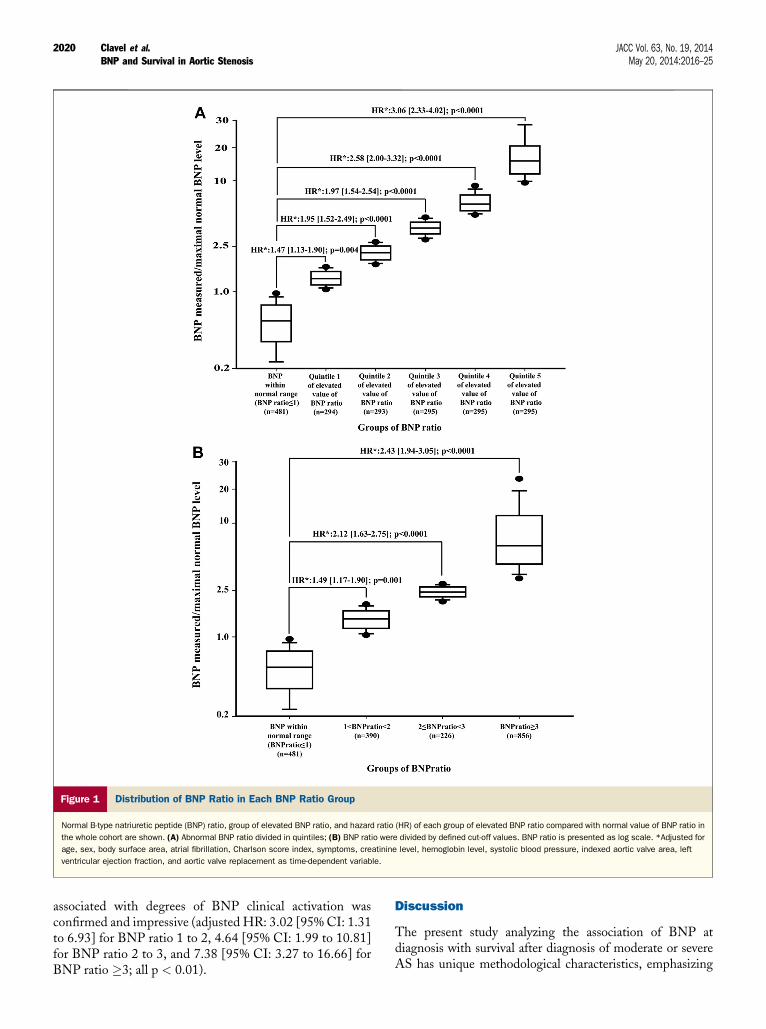
Figure 1 Distribution of BNP Ratio in Each BNP Ratio Group
Normal B-type natriuretic peptide (BNP) ratio, group of elevated BNP ratio, and hazard ratio (HR) of each group of elevated BNP ratio compared with normal value of BNP ratio in
the whole cohort are shown. (A) Abnormal BNP ratio divided in quintiles; (B) BNP ratio were divided by defined cut-off values. BNP ratio is presented as log scale. *Adjusted for
age, sex, body surface area, atrial fibrillation, Charlson score index, symptoms, creatinine level, hemoglobin level, systolic blood pressure, indexed aortic valve area, left
ventricular ejection fraction, and aortic valve replacement as time-dependent variable.
Clavel et al. JACC Vol. 63, No. 19, 2014BNP and Survival in Aortic Stenosis May 20, 2014:2016–25
2020
associated with degrees of BNP clinical activation wasconfirmed and impressive (adjusted HR: 3.02 [95% CI: 1.31to 6.93] for BNP ratio 1 to 2, 4.64 [95% CI: 1.99 to 10.81]for BNP ratio 2 to 3, and 7.38 [95% CI: 3.27 to 16.66] forBNP ratio �3; all p < 0.01).
Discussion
The present study analyzing the association of BNP atdiagnosis with survival after diagnosis of moderate or severeAS has unique methodological characteristics, emphasizing
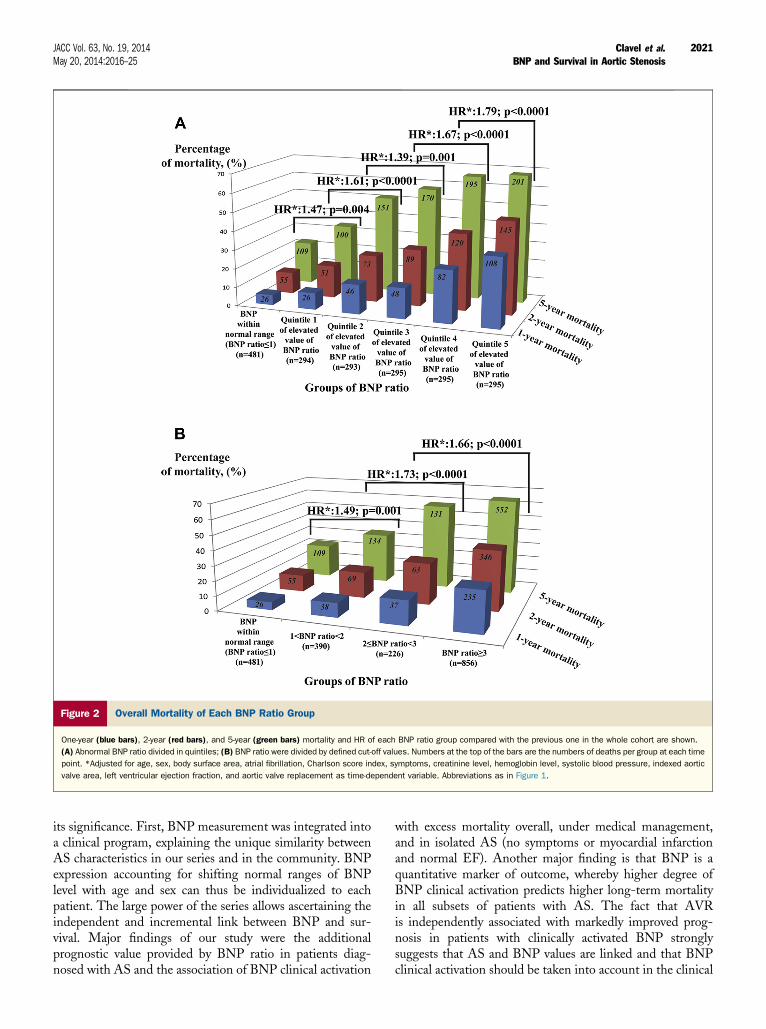
Figure 2 Overall Mortality of Each BNP Ratio Group
One-year (blue bars), 2-year (red bars), and 5-year (green bars) mortality and HR of each BNP ratio group compared with the previous one in the whole cohort are shown.
(A) Abnormal BNP ratio divided in quintiles; (B) BNP ratio were divided by defined cut-off values. Numbers at the top of the bars are the numbers of deaths per group at each time
point. *Adjusted for age, sex, body surface area, atrial fibrillation, Charlson score index, symptoms, creatinine level, hemoglobin level, systolic blood pressure, indexed aortic
valve area, left ventricular ejection fraction, and aortic valve replacement as time-dependent variable. Abbreviations as in Figure 1.
JACC Vol. 63, No. 19, 2014 Clavel et al.May 20, 2014:2016–25 BNP and Survival in Aortic Stenosis
2021
its significance. First, BNP measurement was integrated intoa clinical program, explaining the unique similarity betweenAS characteristics in our series and in the community. BNPexpression accounting for shifting normal ranges of BNPlevel with age and sex can thus be individualized to eachpatient. The large power of the series allows ascertaining theindependent and incremental link between BNP and sur-vival. Major findings of our study were the additionalprognostic value provided by BNP ratio in patients diag-nosed with AS and the association of BNP clinical activation
with excess mortality overall, under medical management,and in isolated AS (no symptoms or myocardial infarctionand normal EF). Another major finding is that BNP is aquantitative marker of outcome, whereby higher degree ofBNP clinical activation predicts higher long-term mortalityin all subsets of patients with AS. The fact that AVRis independently associated with markedly improved prog-nosis in patients with clinically activated BNP stronglysuggests that AS and BNP values are linked and that BNPclinical activation should be taken into account in the clinical
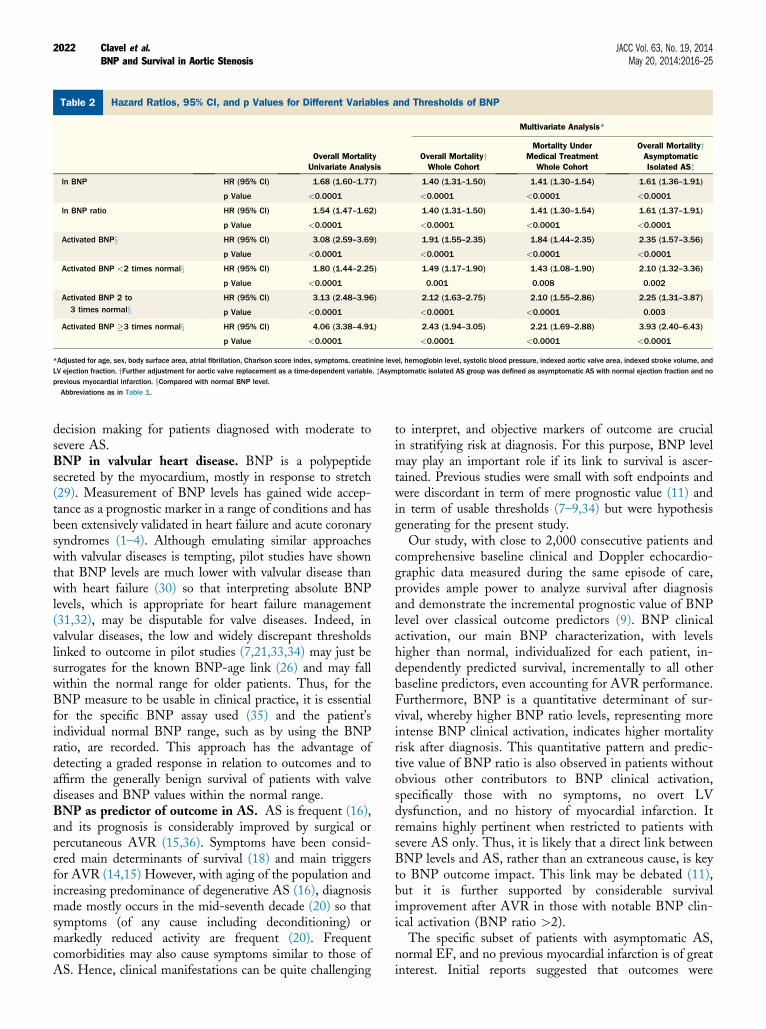
Table 2 Hazard Ratios, 95% CI, and p Values for Different Variables and Thresholds of BNP
Overall MortalityUnivariate Analysis
Multivariate Analysis*
Overall MortalityyWhole Cohort
Mortality UnderMedical Treatment
Whole Cohort
Overall MortalityyAsymptomaticIsolated ASz
ln BNP HR (95% CI) 1.68 (1.60–1.77) 1.40 (1.31–1.50) 1.41 (1.30–1.54) 1.61 (1.36–1.91)
p Value <0.0001 <0.0001 <0.0001 <0.0001
ln BNP ratio HR (95% CI) 1.54 (1.47–1.62) 1.40 (1.31–1.50) 1.41 (1.30–1.54) 1.61 (1.37–1.91)
p Value <0.0001 <0.0001 <0.0001 <0.0001
Activated BNPx HR (95% CI) 3.08 (2.59–3.69) 1.91 (1.55–2.35) 1.84 (1.44–2.35) 2.35 (1.57–3.56)
p Value <0.0001 <0.0001 <0.0001 <0.0001
Activated BNP <2 times normalx HR (95% CI) 1.80 (1.44–2.25) 1.49 (1.17–1.90) 1.43 (1.08–1.90) 2.10 (1.32–3.36)
p Value <0.0001 0.001 0.008 0.002
Activated BNP 2 to3 times normalx
HR (95% CI) 3.13 (2.48–3.96) 2.12 (1.63–2.75) 2.10 (1.55–2.86) 2.25 (1.31–3.87)
p Value <0.0001 <0.0001 <0.0001 0.003
Activated BNP �3 times normalx HR (95% CI) 4.06 (3.38–4.91) 2.43 (1.94–3.05) 2.21 (1.69–2.88) 3.93 (2.40–6.43)
p Value <0.0001 <0.0001 <0.0001 <0.0001
*Adjusted for age, sex, body surface area, atrial fibrillation, Charlson score index, symptoms, creatinine level, hemoglobin level, systolic blood pressure, indexed aortic valve area, indexed stroke volume, andLV ejection fraction. yFurther adjustment for aortic valve replacement as a time-dependent variable. zAsymptomatic isolated AS group was defined as asymptomatic AS with normal ejection fraction and noprevious myocardial infarction. xCompared with normal BNP level.Abbreviations as in Table 1.
Clavel et al. JACC Vol. 63, No. 19, 2014BNP and Survival in Aortic Stenosis May 20, 2014:2016–25
2022
decision making for patients diagnosed with moderate tosevere AS.BNP in valvular heart disease. BNP is a polypeptidesecreted by the myocardium, mostly in response to stretch(29). Measurement of BNP levels has gained wide accep-tance as a prognostic marker in a range of conditions and hasbeen extensively validated in heart failure and acute coronarysyndromes (1–4). Although emulating similar approacheswith valvular diseases is tempting, pilot studies have shownthat BNP levels are much lower with valvular disease thanwith heart failure (30) so that interpreting absolute BNPlevels, which is appropriate for heart failure management(31,32), may be disputable for valve diseases. Indeed, invalvular diseases, the low and widely discrepant thresholdslinked to outcome in pilot studies (7,21,33,34) may just besurrogates for the known BNP-age link (26) and may fallwithin the normal range for older patients. Thus, for theBNP measure to be usable in clinical practice, it is essentialfor the specific BNP assay used (35) and the patient’sindividual normal BNP range, such as by using the BNPratio, are recorded. This approach has the advantage ofdetecting a graded response in relation to outcomes and toaffirm the generally benign survival of patients with valvediseases and BNP values within the normal range.BNP as predictor of outcome in AS. AS is frequent (16),and its prognosis is considerably improved by surgical orpercutaneous AVR (15,36). Symptoms have been consid-ered main determinants of survival (18) and main triggersfor AVR (14,15) However, with aging of the population andincreasing predominance of degenerative AS (16), diagnosismade mostly occurs in the mid-seventh decade (20) so thatsymptoms (of any cause including deconditioning) ormarkedly reduced activity are frequent (20). Frequentcomorbidities may also cause symptoms similar to those ofAS. Hence, clinical manifestations can be quite challenging
to interpret, and objective markers of outcome are crucialin stratifying risk at diagnosis. For this purpose, BNP levelmay play an important role if its link to survival is ascer-tained. Previous studies were small with soft endpoints andwere discordant in term of mere prognostic value (11) andin term of usable thresholds (7–9,34) but were hypothesisgenerating for the present study.
Our study, with close to 2,000 consecutive patients andcomprehensive baseline clinical and Doppler echocardio-graphic data measured during the same episode of care,provides ample power to analyze survival after diagnosisand demonstrate the incremental prognostic value of BNPlevel over classical outcome predictors (9). BNP clinicalactivation, our main BNP characterization, with levelshigher than normal, individualized for each patient, in-dependently predicted survival, incrementally to all otherbaseline predictors, even accounting for AVR performance.Furthermore, BNP is a quantitative determinant of sur-vival, whereby higher BNP ratio levels, representing moreintense BNP clinical activation, indicates higher mortalityrisk after diagnosis. This quantitative pattern and predic-tive value of BNP ratio is also observed in patients withoutobvious other contributors to BNP clinical activation,specifically those with no symptoms, no overt LVdysfunction, and no history of myocardial infarction. Itremains highly pertinent when restricted to patients withsevere AS only. Thus, it is likely that a direct link betweenBNP levels and AS, rather than an extraneous cause, is keyto BNP outcome impact. This link may be debated (11),but it is further supported by considerable survivalimprovement after AVR in those with notable BNP clin-ical activation (BNP ratio >2).
The specific subset of patients with asymptomatic AS,normal EF, and no previous myocardial infarction is of greatinterest. Initial reports suggested that outcomes were
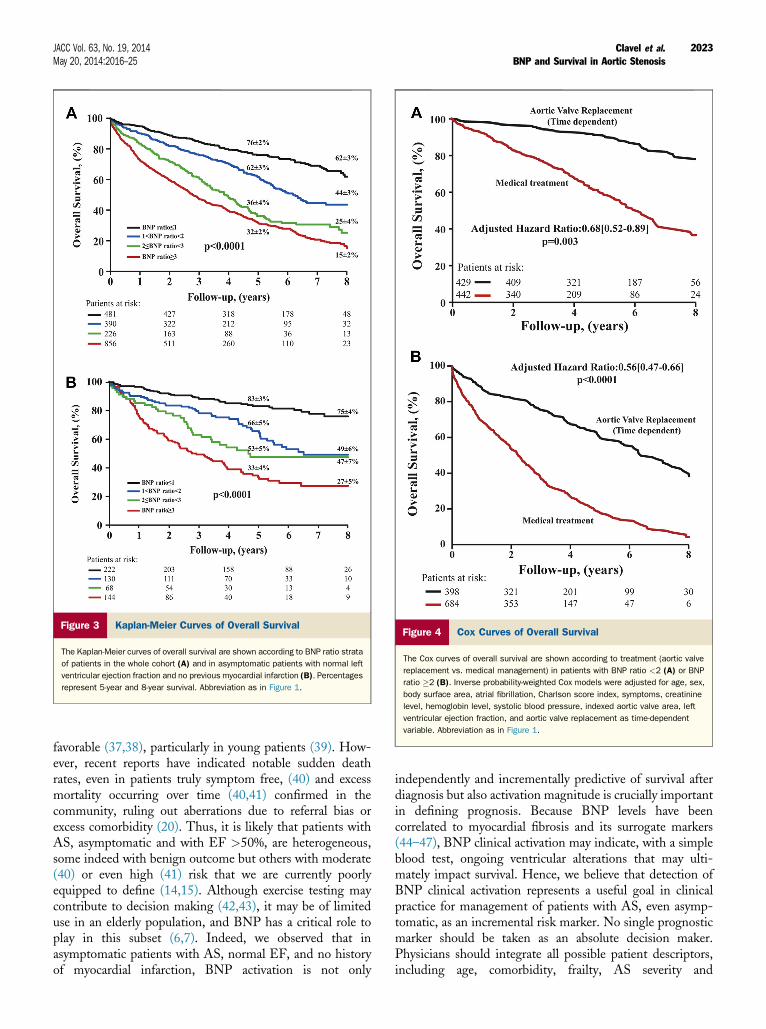
Figure 3 Kaplan-Meier Curves of Overall Survival
The Kaplan-Meier curves of overall survival are shown according to BNP ratio strata
of patients in the whole cohort (A) and in asymptomatic patients with normal left
ventricular ejection fraction and no previous myocardial infarction (B). Percentages
represent 5-year and 8-year survival. Abbreviation as in Figure 1.
Figure 4 Cox Curves of Overall Survival
The Cox curves of overall survival are shown according to treatment (aortic valve
replacement vs. medical management) in patients with BNP ratio <2 (A) or BNP
ratio �2 (B). Inverse probability-weighted Cox models were adjusted for age, sex,
body surface area, atrial fibrillation, Charlson score index, symptoms, creatinine
level, hemoglobin level, systolic blood pressure, indexed aortic valve area, left
ventricular ejection fraction, and aortic valve replacement as time-dependent
variable. Abbreviation as in Figure 1.
JACC Vol. 63, No. 19, 2014 Clavel et al.May 20, 2014:2016–25 BNP and Survival in Aortic Stenosis
2023
favorable (37,38), particularly in young patients (39). How-ever, recent reports have indicated notable sudden deathrates, even in patients truly symptom free, (40) and excessmortality occurring over time (40,41) confirmed in thecommunity, ruling out aberrations due to referral bias orexcess comorbidity (20). Thus, it is likely that patients withAS, asymptomatic and with EF >50%, are heterogeneous,some indeed with benign outcome but others with moderate(40) or even high (41) risk that we are currently poorlyequipped to define (14,15). Although exercise testing maycontribute to decision making (42,43), it may be of limiteduse in an elderly population, and BNP has a critical role toplay in this subset (6,7). Indeed, we observed that inasymptomatic patients with AS, normal EF, and no historyof myocardial infarction, BNP activation is not only
independently and incrementally predictive of survival afterdiagnosis but also activation magnitude is crucially importantin defining prognosis. Because BNP levels have beencorrelated to myocardial fibrosis and its surrogate markers(44–47), BNP clinical activation may indicate, with a simpleblood test, ongoing ventricular alterations that may ulti-mately impact survival. Hence, we believe that detection ofBNP clinical activation represents a useful goal in clinicalpractice for management of patients with AS, even asymp-tomatic, as an incremental risk marker. No single prognosticmarker should be taken as an absolute decision maker.Physicians should integrate all possible patient descriptors,including age, comorbidity, frailty, AS severity and

Clavel et al. JACC Vol. 63, No. 19, 2014BNP and Survival in Aortic Stenosis May 20, 2014:2016–25
2024
consequences, and patient desires into each clinical decision.Our data clearly showed that BNP activation should be oneof the elements that participate in this comprehensiveassessment of patients with AS.Study limitations. Our design, routine clinical practicecohort with hormonal levels, clinical, and Doppler echo-cardiographic data collected prospectively, but with nomandate to arrange follow-up with investigators, maintainedthe central role of the personal physician. The disadvantageof this design is that strict plans of care by investigatorscannot be enforced; therefore, ultimate decisions are madeby patients and personal physicians. The notable advantageof this design is the large number of patients participating,demonstrating unique statistical power, and the limitedenrollment bias demonstrated by the similarity of the currentenrolled population with patients diagnosed with AS in thecommunity (20). We did not evaluate serial values of BNP;however, now that the link of BNP to survival has beenestablished, future studies with serial measurements maydemonstrate additional prognostic power.
We could not secure funding to perform systematic mul-tiple testing simultaneously, such as computed tomography,magnetic resonance imaging, and measurement of multipleblood markers simultaneously to calculate BNP levels.We also did not measure NT-pro-BNP to compare predic-tive values of these 2 assays, which may not be equivalentprognostically in valve diseases, potentially explaining dis-cordances in the literature (11). We believe that futuremechanistic studies should be conducted in that regard, nowthat the present series has demonstrated the critical role ofBNP as a marker of survival after AS diagnosis. Comor-bidities may influence BNP activation but were accountedfor by exclusion criteria, by adjusting for specific baselinecharacteristics, and by analysis of subsets when there wasno other identified cause of BNP activation. Mild kidney orliver disease or atrial fibrillation with controlled heart ratewere included but did not affect the BNP-survival link.Despite our large sample size and event numbers, power wasnot sufficient to analyze all possible subgroups in multiplecomparisons and should be addressed by future largecollaborative studies. Our study raises the question of po-tential benefit of AVR in AS with elevated BNP levels forwhich a randomized control trial would be warranted.
Conclusions
In this large cohort of patients with moderate or severe AS,BNP clinical activation, defined as levels higher than theupper limit of normal for each individual patient, was apowerful predictor of long-term mortality, incrementallyand independently of all baseline characteristics. MoreoverBNP was a quantitative marker of outcome, whereby higheractivation predicted higher mortality, and was particularlyeffective in the important subset of asymptomatic patientswith normal EF and no history of myocardial infarction.Thus, BNP measurement and BNP ratio calculation should
be included for risk stratification in clinical practice and forconsideration of AVR, which is associated with considerablereduction of mortality, even in patients with marked BNPclinical activation.
Reprint requests and correspondence: Dr. Maurice Enriquez-Sarano, Division of Cardiovascular Diseases and Internal Medi-cine, Mayo Clinic, 200 First Street SW, Rochester, Minnesota55905. E-mail: [email protected].
REFERENCES
1. Shapiro BP, Chen HH, Burnett JC Jr., Redfield MM. Use of plasmabrain natriuretic peptide concentration to aid in the diagnosis of heartfailure. Mayo Clin Proc 2003;78:481–6.
2. Khan SQ, Dhillon O, Kelly D, et al. Plasma N-terminal B-typenatriuretic peptide as an indicator of long-term survival after acutemyocardial infarction: comparison with plasma midregional pro-atrialnatriuretic peptide: the LAMP (Leicester Acute Myocardial Infarc-tion Peptide) study. J Am Coll Cardiol 2008;51:1857–64.
3. Di Angelantonio E, Chowdhury R, Sarwar N, et al. B-type natriureticpeptides and cardiovascular risk: systematic review and meta-analysis of40 prospective studies. Circulation 2009;120:2177–87.
4. Pu DR, Chiong JR, Zhou QC. Clinical applications of N-terminal proB-type natriuretic peptide in heart failure and other cardiovasculardiseases. Heart Fail Rev 2010;15:293–304.
5. Ray SG. Natriuretic peptides in heart valve disease. Heart 2006;92:1194–7.
6. Gerber IL, Stewart RA, Legget ME, et al. Increased plasma natriureticpeptide levels reflect symptom onset in aortic stenosis. Circulation2003;107:1884–90.
7. Bergler-Klein J, Klaar U, Heger M, et al. Natriuretic peptides predictsymptom-free survival and postoperative outcome in severe aortic ste-nosis. Circulation 2004;109:2302–8.
8. Iwahashi N, Nakatani S, Umemura S, Kimura K, Kitakaze M. Use-fulness of plasma B-type natriuretic peptide in the assessment of diseaseseverity and prediction of outcome after aortic valve replacement inpatients with severe aortic stenosis. J Am Soc Echocardiogr 2011;24:984–91.
9. Katz M, Tarasoutchi F, Pesaro AE, et al. Natriuretic peptides andlong-term mortality in patients with severe aortic stenosis. J HeartValve Dis 2012;21:331–6.
10. Bergler-Klein J, Mundigler G, Pibarot P, et al. B-type natriureticpeptide in low-flow, low-gradient aortic stenosis: relationship to he-modynamics and clinical outcome: results from the Multicenter Trulyor Pseudo-Severe Aortic Stenosis (TOPAS) study. Circulation 2007;115:2848–55.
11. Cimadevilla C, Cueff C, Hekimian G, et al. Prognostic value of B-typenatriuretic peptide in elderly patients with aortic valve stenosis: theCOFRASA-GENERAC study. Heart 2013;99:461–7.
12. Lim P, Monin JL, Monchi M, et al. Predictors of outcome in patientswith severe aortic stenosis and normal left ventricular function: role ofB-type natriuretic peptide. Eur Heart J 2004;25:2048–53.
13. Nessmith MG, Fukuta H, Brucks S, Little WC. Usefulness of anelevated B-type natriuretic peptide in predicting survival in patientswith aortic stenosis treated without surgery. Am J Cardiol 2005;96:1445–8.
14. Bonow RO, Carabello BA, Kanu C, et al. ACC/AHA 2006 guidelinesfor the management of patients with valvular heart disease: a report ofthe American College of Cardiology/American Heart Association TaskForce on Practice Guidelines (writing committee to revise the 1998Guidelines for the Management of Patients With Valvular HeartDisease): developed in collaboration with the Society of CardiovascularAnesthesiologists: endorsed by the Society for Cardiovascular Angi-ography and Interventions and the Society of Thoracic Surgeons. J AmColl Cardiol 2006;48:e1–148.
15. Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the man-agement of valvular heart disease (version 2012). Eur Heart J 2012;33:2451–96.
JACC Vol. 63, No. 19, 2014 Clavel et al.May 20, 2014:2016–25 BNP and Survival in Aortic Stenosis
2025
16. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG,Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005–11.
17. Iung B, Baron G, Butchart EG, et al. A prospective survey of patientswith valvular heart disease in Europe: the Euro Heart Survey onValvular Heart Disease. Eur Heart J 2003;24:1231–43.
18. Ross J Jr., Braunwald E. Aortic stenosis. Circulation 1968;38:61–7.19. Otto CM. Calcific aortic valve disease: outflow obstruction is the end
stage of a systemic disease process. Eur Heart J 2009;30:1940–2.20. Malouf J, Le Tourneau T, Pellikka P, et al. Aortic valve stenosis in
community medical practice: determinants of outcome and implicationsfor aortic valve replacement. J Thorac Cardiovasc Surg 2012;144:1421–7.
21. Detaint D, Messika-Zeitoun D, Avierinos JF, et al. B-type natriureticpeptide in organic mitral regurgitation: determinants and impact onoutcome. Circulation 2005;111:2391–7.
22. Rossi A, Enriquez-Sarano M, Burnett JC Jr., Lerman A, Abel MD,Seward JB. Natriuretic peptide levels in atrial fibrillation: a prospectivehormonal and Doppler-echocardiographic study. J Am Coll Cardiol2000;35:1256–62.
23. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method ofclassifying prognostic comorbidity in longitudinal studies: developmentand validation. J Chronic Dis 1987;40:373–83.
24. Nishimura RA, Miller FA Jr., Callahan MJ, Benassi RC, Seward JB,Tajik AJ. Doppler echocardiography: theory, instrumentation, tech-nique, and application. Mayo Clin Proc 1985;60:321–43.
25. Baumgartner H, Hung J, Bermejo J, et al. Echocardiographic assess-ment of valve stenosis: EAE/ASE recommendations for clinical prac-tice. J Am Soc Echocardiogr 2009;22:1–23.
26. Redfield MM, Rodeheffer RJ, Jacobsen SJ, Mahoney DW, Bailey KR,Burnett JC Jr. Plasma brain natriuretic peptide concentration: impact ofage and gender. J Am Coll Cardiol 2002;40:976–82.
27. Devivo MJ, Underhill AT, Fine PR. Accuracy of world-wide-webdeath searches for persons with traumatic brain injury. Brain Inj2004;18:1155–62.
28. Quinn J, Kramer N, McDermott D. Validation of the Social SecurityDeath Index (SSDI): an important readily-available outcomes databasefor researchers. West J Emerg Med 2008;9:6–8.
29. Wei CM, Heublein DM, Perrella MA, et al. Natriuretic peptide sys-tem in human heart failure. Circulation 1993;88:1004–9.
30. Detaint D, Messika-Zeitoun D, Chen HH, et al. Association of B-typenatriuretic peptide activation to left ventricular end-systolic remodelingin organic and functional mitral regurgitation. Am J Cardiol 2006;97:1029–34.
31. Kociol RD, Horton JR, Fonarow GC, et al. Admission, discharge, orchange in B-type natriuretic peptide and long-term outcomes: datafrom Organized Program to Initiate Lifesaving Treatment in Hospi-talized Patients With Heart Failure (OPTIMIZE-HF) linked toMedicare claims. Circ Heart Fail 2011;4:628–36.
32. McMurray JJ, Adamopoulos S, Anker SD, et al. ESC guidelines forthe diagnosis and treatment of acute and chronic heart failure 2012:the Task Force for the Diagnosis and Treatment of Acute and Chronic
Heart Failure 2012 of the European Society of Cardiology. Developedin collaboration with the Heart Failure Association (HFA) of the ESC.Eur Heart J 2012;33:1787–847.
33. Pizarro R, Bazzino OO, Oberti PF, et al. Prospective validation of theprognostic usefulness of brain natriuretic peptide in asymptomatic pa-tients with chronic severe mitral regurgitation. J Am Coll Cardiol 2009;54:1099–106.
34. Monin JL, Lancellotti P, Monchi M, et al. Risk score for predictingoutcome in patients with asymptomatic aortic stenosis. Circulation2009;120:69–75.
35. Apple FS, Panteghini M, Ravkilde J, et al. Quality specifications forB-type natriuretic peptide assays. Clin Chem 2005;51:486–93.
36. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve im-plantation for aortic stenosis in patients who cannot undergo surgery.N Engl J Med 2010;363:1597–607.
37. Pellikka PA, Nishimura RA, Bailey KR, Tajik AJ. The natural historyof adults with asymptomatic, hemodynamically significant aortic ste-nosis. J Am Coll Cardiol 1990;15:1012–7.
38. Otto CM, Burwash IG, Legget ME, et al. Prospective study ofasymptomatic valvular aortic stenosis. Clinical, echocardiographic, andexercise predictors of outcome. Circulation 1997;95:2262–70.
39. Rosenhek R, Binder T, Porenta G, et al. Predictors of outcome insevere, asymptomatic aortic stenosis. N Engl J Med 2000;343:611–7.
40. Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adultswith asymptomatic, hemodynamically significant aortic stenosis duringprolonged follow-up. Circulation 2005;111:3290–5.
41. Pai RG, Kapoor N, Bansal RC, Varadarajan P. Malignant naturalhistory of asymptomatic severe aortic stenosis: benefit of aortic valvereplacement. Ann Thorac Surg 2006;82:2116–22.
42. Das P, Rimington H, Chambers J. Exercise testing to stratify risk inaortic stenosis. Eur Heart J 2005;26:1309–13.
43. Dhoble A, Sarano ME, Kopecky SL, Thomas RJ, Hayes CL,Allison TG. Safety of symptom-limited cardiopulmonary exercisetesting in patients with aortic stenosis. Am J Med 2012;125:704–8.
44. Weidemann F, Herrmann S, Stork S, et al. Impact of myocardialfibrosis in patients with symptomatic severe aortic stenosis. Circulation2009;120:577–84.
45. Lancellotti P, Moonen M, Magne J, et al. Prognostic effect of long-axisleft ventricular dysfunction and B-type natriuretic peptide levels inasymptomatic aortic stenosis. Am J Cardiol 2010;105:383–8.
46. Herrmann S, Stork S, Niemann M, et al. Low-gradient aortic valvestenosis myocardial fibrosis and its influence on function and outcome.J Am Coll Cardiol 2011;58:402–12.
47. Poulsen SH, Sogaard P, Nielsen-Kudsk JE, Egeblad H. Recovery ofleft ventricular systolic longitudinal strain after valve replacement inaortic stenosis and relation to natriuretic peptides. J Am Soc Echo-cardiogr 2007;20:877–84.
Key Words: valvular heart disease - aortic stenosis -
Doppler echocardiography - natriuretic peptide.