Embed Size (px)
Citation preview

Lymphoma is a type of blood cancer that occurs when lymphocytes--white blood cells that help protect the body from infection and disease--begin behaving abnormally. Abnormal lymphocytes may divide faster than normal cells or they may live longer than they are supposed to.
Lymphoma may develop in many parts of the body, including the lymph nodes, spleen, bone marrow, blood or other organs.
There are two main types of lymphomas:
• Hodgkin lymphoma (HL) (formerly referred to as Hodgkin's lymphoma) - There are six types of HL, an uncommon form of lymphoma that involves the Reed-Sternberg cells.
• Non-Hodgkin lymphoma (NHL) (formerly referred to as non-Hodgkin's lymphoma) - There are more than 61 types of NHL, some of which are more common than others. Any lymphoma that does not involve Reed-Sternberg cells is classified as non-Hodgkin lymphoma.
Signs and Symptoms
Certain symptoms are not specific to lymphoma and are, in fact, similar to those of many other illnesses. People often first go to the doctor because they think they have a cold, the flu or some other respiratory infection that does not go away.
Common symptoms include:
• Swelling of lymph nodes, which may or may not be painless• Fever • Unexplained weight loss • Sweating (often at night) • Chills • Lack of energy • Itching
Most people who have these non-specific symptoms will not have lymphoma. However, it is important that anyone with persistent symptoms be examined by a doctor to make sure lymphoma is not present.
Lymphoma Treatment
Some form of chemotherapy, radiation therapy, or a combination of the two is typically used to treat Hodgkin lymphoma. Bone marrow or stem cell transplantation may also sometimes be done under special circumstances. Most patients with Hodgkin lymphoma live long and healthy lives following successful treatment.
Many people treated for non-Hodgkin lymphoma will receive some form of chemotherapy, radiation therapy, biologic therapy, or a combination of these. Bone marrow or stem cell transplantation may sometimes be used. Surgery may be used under special circumstances,

but primarily to obtain a biopsy for diagnostic purposes.
Although "indolent" forms of non-Hodgkin lymphoma are not currently curable, the prognosis is still very good. Patients may live for 20 years or more following an initial diagnosis. In certain patients with an indolent form of the disease, treatment may not be necessary until there are signs of progression. Response to treatment can also change over time. Treatment that worked initially may be ineffective the next time, making it necessary to always keep abreast of the latest information on new or experimental treatment options.
Approximately 30 to 60 percent of patients with an aggressive form of non-Hodgkin lymphoma can be cured.
http://www.lymphoma.org/site/pp.asp?c=bkLTKaOQLmK8E&b=6299689&gclid=CImEps_G7rsCFesl4godEnIAKA
Hodgkin http://emedicine.medscape.com/article/201886-overview
Practice Essentials
Hodgkin lymphoma (formerly Hodgkin disease) is a potentially curable lymphoma with distinct histology, biologic behavior, and clinical characteristics. It is classified by the World Health Organization (WHO) into 5 types. Of these, 4—nodular sclerosis, mixed cellularity, lymphocyte depleted, and lymphocyte rich—are referred to as classic Hodgkin lymphoma; the fifth type, nodular lymphocyte predominant Hodgkin disease (NLPHD), is a distinct entity with unique clinical features and a different treatment paradigm.
Essential update: Hodgkin lymphoma treatment increases risk of stomach cancer
People treated for Hodgkin lymphoma could face an increased risk for the subsequent development of stomach cancer, according to recent case-control study in which a dose-dependent increase in the risk for stomach cancer was seen in patients who received subdiaphragmatic radiotherapy and a chemotherapy regimen containing high-dose procarbazine.[1, 2]
Morton and colleagues evaluated data on 19,882 survivors of Hodgkin's lymphoma, of whom 89 developed stomach cancer. These patients were matched with 190 control subjects. The risk for stomach cancer rose with increasing doses of radiation to the stomach (P for trend < .001) and with an increasing number of chemotherapy cycles containing alkylating agents (P for trend = .02). Patients who received 25 Gy of radiation or more to the stomach and procarbazine (≥5600 mg/m²) had a 77.5-fold higher risk of developing stomach cancer. However, for patients who received any dose of procarbazine but less than 25 Gy of abdominal radiation, there was no increased risk. For patients who received less than 5600 mg/m² of procarbazine and abdominal radiation of 25 Gy or more, the risk for stomach cancer jumped 2.8-fold. For those who received less than 25 Gy of abdominal radiation and dacarbazine, the risk was increased 5.4-fold.[1, 2]

Signs and symptoms
Features of Hodgkin lymphoma include the following:
Asymptomatic lymphadenopathy (above the diaphragm in 80% of patients) Constitutional symptoms (40% of cases; collectively known as “B symptoms”) Intermittent fever (~35% of cases); classic Pel-Ebstein fever (infrequent) Chest pain, cough, shortness of breath, or a combination thereof; hemoptysis (rare) Pruritus Pain at nodal disease sites, precipitated by drinking alcohol (< 10% of cases but specific for
Hodgkin lymphoma) Back or bone pain (rare)
Physical findings in Hodgkin lymphoma are as follows:
Palpable, painless lymphadenopathy (rubbery adenopathy) in the neck (60-80%), axilla (6-20%), or groin (6-20%)
Involvement of the Waldeyer ring or occipital or epitrochlear areas (infrequent) Splenomegaly or hepatomegaly Superior vena cava syndrome (in patients with massive mediastinal lymphadenopathy) Central nervous system (CNS) signs due to paraneoplastic syndromes
See Presentation for more detail.
Diagnosis
Imaging studies to be considered include the following:
Anteroposterior and lateral chest radiography Computed tomography (CT) of the chest, abdomen, and pelvis Positron emission tomography (PET) – Essential to initial staging of Hodgkin lymphoma and
often performed in conjunction with CT Magnetic resonance imaging (MRI) for CNS evaluation
Tissue sampling procedures to be considered are as follows:
Excisional lymph node biopsy (recommended), sometimes preceded by fine-needle aspiration (FNA)
Bone marrow biopsy (indicated in some cases) Sampling of a pleural effusion by thoracentesis and examination of cells CNS evaluation by lumbar puncture and cerebrospinal fluid (CSF) analysis
Blood studies may include the following:
Complete blood count (CBC) Erythrocyte sedimentation rate (ESR) Lactate dehydrogenase (LDH) Creatinine Alkaline phosphatase (ALP) Electrolytes Glucose HIV

Cytokines (usually only in special situations or in the context of a clinical trial)
The Ann Arbor classification for staging Hodgkin lymphoma is as follows:
Stage I - Single lymph node area or single extranodal site Stage II - 2 or more lymph node areas on the same side of the diaphragm Stage III - Lymph node areas on both sides of the diaphragm Stage IV - Disseminated or multiple involvement of the extranodal organs
Descriptive suffixes that may be added to the stages include the following:
S – Splenic involvement B – Presence of B symptoms (temperature >38°C, drenching night sweats, unexplained loss
of >10% of body weight in the preceding 6 months) A – Absence of B symptoms X – Presence of bulky disease E – Contiguous involvement of extranodal sites
In patients with stage I or II disease, the following factors are considered unfavorable:
Bulky disease ESR ≥50 mm/hr if the patient is otherwise asymptomatic >3 sites of disease involvement Presence of B symptoms Presence of extranodal disease
In patients with advanced disease, the following factors are considered unfavorable:
Serum albumin < 4 g/dL Hemoglobin < 10.5 g/dL Male sex Stage IV disease Age ≥45 years White blood cell (WBC) count >15,000/μL Lymphocyte count < 600/μL or < 8% of total WBC count
See Workup for more detail.
Management
Treatment of Hodgkin lymphoma is tailored to disease type, disease stage, and an assessment of the risk of resistant disease. The primary goal is to induce a complete remission (CR), defined as the disappearance of all evidence of disease. A partial remission (PR) is defined as “regression of measurable disease and no new sites” of disease.
In classic Hodgkin lymphoma, radiation therapy is generally administered in combination with chemotherapy; in NLPHD, involved-field radiation therapy may be recommended for stage IA and IIA disease. The radiation dose is tailored to the specific clinical scenario as follows:

Combined-modality therapy, bulky disease sites – 30-36 Gy Combined-modality therapy, nonbulky disease sites – 20-30 Gy Radiotherapy alone – 30-44 Gy
The following induction regimens are given as initial treatment for Hodgkin lymphoma:
MOPP (mechlorethamine, vincristine, procarbazine, prednisone) ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) Stanford V (doxorubicin, vinblastine, mustard, bleomycin, vincristine, etoposide, prednisone) BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine,
prednisone)
When induction chemotherapy fails or patients experience relapse, salvage chemotherapy is generally given. Commonly used salvage regimens include the following:
ICE (ifosfamide, carboplatin, etoposide) DHAP (cisplatin, cytarabine, prednisone) ESHAP (etoposide, methylprednisolone, cytarabine, cisplatin) EPOCH (etoposide, vincristine, doxorubicin, cyclophosphamide, prednisone)
Therapeutic approaches to different stages of Hodgkin lymphoma are as follows:
Early-stage, low-risk disease – 2-4 cycles of ABVD or 8 weeks of Stanford V, followed by involved-field radiation therapy; if radiation therapy is contraindicated or not possible, chemotherapy should continue for 2 additional cycles after CR
Early-stage disease with unfavorable factors – Chemotherapy (eg, ABVD or Stanford V) plus involved-field radiation therapy; in general, 2 cycles beyond best response (≤6 cycles of ABVD) is used
Advanced disease – Chemotherapy (NCCN: 4 cycles of ABVD or 12 weeks of Stanford V; EMSO: 8 cycles of ABVD or standard BEACOPP), with radiation reserved for initial bulky sites or residual disease
NLPHD – For early-stage disease, local excision, involved-field radiation therapy, or expectant management; advanced-stage disease may represent histologic transformation to types of non-Hodgkin lymphoma; addition of ABVD to radiotherapy for limited-stage NLPHD may improve outcome
Advanced disease with HIV infection – Addition of highly active antiretroviral therapy (HAART) to standard chemotherapy
Refractory or relapsed disease – High-dose chemotherapy with autologous stem cell transplantation; alternatively, allogeneic stem cell transplantation

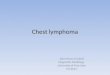
This image depicts a computed tomography (CT) scan, positron-emission tomography (PET) scan, and maximum intensity projection (MIP) PET scan from a patient with histologically proven Hodgkin lymphoma.

This computed tomography scan is from a 46-year patient with Hodgkin lymphoma at the level of the neck. Enlarged lymph nodes are visible on the left side of the neck (red-shaded region).
A computed tomography (CT) scan showing bulk disease in a patient with Hodgkin lymphoma.

A positron emission tomography (PET) scan obtained with fluorodeoxyglucose (FDG) that shows increased FDG uptake in a mediastinal lymph node.

Mixed cellularity Hodgkin lymphoma showing both mononucleate and binucleate Reed-Sternberg cells in a background of inflammatory cells (hematoxylin and eosin, original magnification ×200).
Background
Hodgkin lymphoma (formerly, Hodgkin disease) is a potentially curable lymphoma with distinct histology, biologic behavior, and clinical characteristics. Thomas Hodgkin first described the disorder in 1832; in the 20th century, realization that the disease is a lymphoid malignancy led to it being renamed Hodgkin lymphoma. The disease is defined in terms of its microscopic appearance (histology) and the expression of cell surface markers (immunophenotype). (See Pathophysiology.)
To diagnose Hodgkin lymphoma a histologic evaluation is always required, and an excisional lymph node biopsy is recommended for this purpose (see Workup). Various imaging studies are used to stage the patient.
Treatment for Hodgkin lymphoma is with multiagent chemotherapy, with or without radiation therapy. Treatment seeks to balance the risk of treatment failure with the risk of treatment side effects (see Treatment).
Pathophysiology
As classified by the World Health Organization (WHO), Hodgkin lymphoma exists in 5 types.[3] Four of these—nodular sclerosis, mixed cellularity, lymphocyte depleted, and lymphocyte rich—are referred to as classic Hodgkin lymphoma. The fifth type, nodular lymphocyte predominant Hodgkin disease (NLPHD), is a distinct entity with unique clinical features and a different treatment paradigm.
In classic Hodgkin lymphoma, the neoplastic cell is the Reed-Sternberg (RS) cell.[4, 5] Reed-Sternberg cells comprise only 1-2% of the total tumor cell mass. The remainder is composed of a variety of reactive, mixed inflammatory cells consisting of lymphocytes, plasma cells, neutrophils, eosinophils, and histiocytes.
Most Reed-Sternberg cells are of B-cell origin, derived from lymph node germinal centers but no longer able to produce antibodies. Some Hodgkin lymphoma cases have been identified in which the Reed-Sternberg cell is of T-cell origin but these are rare, accounting for 1-2% of classic Hodgkin lymphoma.
The Reed-Sternberg cells consistently express the CD30 (Ki-1) and CD15 (Leu-M1) antigens. CD30 is a marker of lymphocyte activation that is expressed by reactive and malignant lymphoid cells and was originally identified as a cell surface antigen on Reed-Sternberg cells. CD15 is a marker of late granulocytes, monocytes, and activated T cells that is not normally expressed by cells of B lineage.
Nodular sclerosis Hodgkin disease
In nodular sclerosis Hodgkin disease (NSHD), which constitutes 60-80% of all cases of Hodgkin lymphoma, the morphology shows a nodular pattern. Broad bands of fibrosis divide the node into nodules. The capsule is thickened. The characteristic cell is the lacunar-type

Reed-Sternberg cell, which has a monolobated or multilobated nucleus, a small nucleolus, and abundant pale cytoplasm.
NSHD is frequently observed in adolescents and young adults. It usually involves the mediastinum and other supradiaphragmatic sites.
Mixed-cellularity Hodgkin disease
In mixed-cellularity Hodgkin disease (MCHD), which constitutes 15-30% of cases, the infiltrate is usually diffuse. Reed-Sternberg cells are of the classic type (large, with bilobate, double or multiple nuclei, and a large, eosinophilic nucleolus). MCHD commonly affects the abdominal lymph nodes and spleen. Patients with this histology typically have advanced-stage disease with systemic symptoms. MCHD is the histologic type most commonly observed in patients with human immunodeficiency virus (HIV) infection.
Lymphocyte-depleted Hodgkin disease
Lymphocyte-depleted Hodgkin disease (LDHD) constitutes less than 1% of cases. The infiltrate in LDHD is diffuse and often appears hypocellular. Large numbers of Reed-Sternberg cells and bizarre sarcomatous variants are present.
LDHD is associated with older age and HIV-positive status. Patients usually present with advanced-stage disease. Epstein-Barr virus (EBV) proteins are expressed in many of these tumors. Many cases of LDHD diagnosed in the past were actually were non-Hodgkin lymphomas, often of the anaplastic large-cell type.
Lymphocyte-rich classic Hodgkin disease
Lymphocyte-rich classic Hodgkin disease (LRHD) constitutes 5% of cases. In LRHD, Reed-Sternberg cells of the classic or lacunar type are observed, with a background infiltrate of lymphocytes. It requires immunohistochemical diagnosis. Some cases may have a nodular pattern. Clinically, the presentation and survival patterns are similar to those for MCHD.
Nodular lymphocyte-predominant Hodgkin disease
Nodular lymphocyte-predominant Hodgkin disease (NLPHD) constitutes 5% of cases. In contrast to the other histologic subtypes, the typical Reed-Sternberg cells are either infrequent or absent in NLPHD. Instead, lymphocytic and histiocytic (L&H) cells, or "popcorn cells" (their nuclei resemble an exploded kernel of corn), are seen within a background of inflammatory cells, which are predominantly benign lymphocytes. Unlike Reed-Sternberg cells, L&H cells are positive for B-cell antigens, such as CD19 and CD20, and are negative for CD15 and CD30.
A diagnosis of NLPHD needs to be supported by immunohistochemical studies, because it can appear similar to LRHD or even some non-Hodgkin lymphomas.
Etiology

The etiology of Hodgkin lymphoma is unknown. Infectious agents, particularly EBV, may be involved in the pathogenesis. In as many as 50% of cases, the tumor cells are EBV-positive; EBV positivity is higher with MCHD (60-70%) than with NSHD (15-30%). Almost 100% of HIV-associated cases are EBV-positive.
An epidemiologic study from Denmark and Sweden showed an increased risk of EBV-positive Hodgkin lymphoma in patients with a self-reported history of infectious mononucleosis (IM) in adolescence.[6] The average incubation time from IM to symptoms of Hodgkin lymphoma was 2.9 years.
Patients with HIV infection have a higher incidence of Hodgkin lymphoma compared with the population without HIV infection. However, Hodgkin lymphoma is not considered an acquired immunodeficiency syndrome (AIDS)-defining neoplasm.
Genetic predisposition may play a role in the pathogenesis of Hodgkin lymphoma. Approximately 1% of patients with Hodgkin lymphoma have a family history of the disease. Siblings of an affected individual have a 3- to 7-fold increased risk for developing Hodgkin lymphoma. This risk is higher in monozygotic twins. Human leukocyte antigen (HLA)-DP alleles are more common in Hodgkin lymphoma.
A study by Chang et al found that routine residential UV radiation exposure may have a protective effect against lymphomagenesis through mechanisms that may be independent of vitamin D.[7]
Epidemiology
United States statistics
Information regarding the incidence and mortality of Hodgkin lymphoma in the United States can be found at the National Cancer Institute (NCI) Surveillance Epidemiology and End Results (SEER) database Website (www.seer.cancer.gov). Data are also collected by the American Cancer Society (ACS).[8] The NCI estimated that 8,830 new cases and 1,300 deaths from Hodgkin lymphoma would occur in 2011. The age-adjusted incidence of Hodgkin lymphoma is 2.8 cases per 100,000 individuals.
International statistics
Hodgkin lymphoma had a worldwide incidence of 62,000 cases in 2002. Compared with North America and Europe, Hodgkin lymphoma is relatively rare in Japan (age-adjusted incidence of 0.3 per 100,000 males) and China (age-adjusted incidence of 0.2 per 100,000 males). In developing countries, the incidence of the mixed-cellularity (MCHD) and lymphocyte-depleted (LDHD) subtypes is higher. In contrast, the nodular-sclerosis (NSHD) subtype is most frequent in developed countries.
Race-, sex-, and age-related differences in incidence
Hodgkin lymphoma incidence rates in the United States vary by race and sex. The US incidence in cases per 100,000 individuals is 3.3 for white males, 2.8 for white females, 3.2 for black males, 2.4 for black females, 1.5 for Asian/Pacific Islander males, and 1.0 for

Asian/Pacific Islander females. Overall, Hodgkin lymphoma is somewhat more common in males than in females. The observed male predominance is particularly evident in children, in whom 85% of the cases are in males.
Age-specific incidence rates of Hodgkin lymphoma have a bimodal distribution in both sexes, peaking in young adults (aged 15-34 y) and older individuals (>55 y). In the United States, young adults typically have NSHD, whereas children (aged 0-14 y) and older individuals more commonly have the MCHD subtype.
Prognosis
The 5-year disease-specific survival rates for patients with Hodgkin lymphoma are as follows[9] :
Stages I and II - 90% Stage III - 84% Stage IV - 65%
In addition to the stage of the disease, many factors contribute to the likelihood of survival from Hodgkin lymphoma (see Staging). These are considered in order to best match each patient to the correct type and intensity of therapy.
Survivors of Hodgkin lymphoma may have long-term sequelae from their therapy, including cardiac disease, pulmonary disease, secondary cancers, infertility, and infectious complications.[10] With the current widespread use of nonleukemogenic chemotherapy (ABVD) and the use of smaller radiation fields and doses, the rate of treatment-related deaths is expected to decrease. See Complications of Therapy in Treatment.
Patient Education
Before the initiation of treatment, patients with Hodgkin lymphoma should be counseled about the potential complications of Hodgkin lymphoma therapy, including the risk of cardiac disease, lung toxicity, and secondary cancers. Patients should also be apprised of the potential loss of fertility that may arise from MOPP chemotherapy, escalated BEACOPP chemotherapy, pelvic irradiation, or HDC, so that they may explore fertility-preserving options such as sperm banking, oral contraceptive use, or oophoropexy.
Female patients who have received chest radiation therapy should be encouraged to perform regular breast self-examinations. All patients should be counseled on health habits that may help reduce the risk of cancer and cardiovascular disease, including avoidance of smoking, control of lipids, and the use of sunscreen.
Patients should also be advised about the long-term risk of infection after undergoing splenectomy and the importance of calling their physician if they experience a fever.
Patients should understand the risk of psychosocial problems that may affect survivors of Hodgkin lymphoma. Consultations with social workers, psychologists, and psychiatrists may be helpful to manage some of these issues.

For patient education information, see the Blood and Lymphatic System Center, as well as Lymphoma.
History
Features of Hodgkin lymphoma include the following:
Asymptomatic lymphadenopathy may be present (above the diaphragm in 80% of patients)
Constitutional symptoms (eg, unexplained weight loss, fever, night sweats) are present in 40% of patients. Collectively, these are known as "B symptoms."
Intermittent fever is observed in approximately 35% of cases; infrequently, the classic Pel-Ebstein fever is observed (high fever for 1-2 wk followed by an afebrile period of 1-2 wk)
Chest pain, cough, shortness of breath, or a combination of these things may be present due to a large mediastinal mass or lung involvement; rarely, hemoptysis occurs
Patients may present with pruritus Pain at sites of nodal disease, precipitated by drinking alcohol, occurs in less than
10% of patients but is specific for Hodgkin lymphoma Back or bone pain may rarely occur
Physical Examination
Physical examination findings in Hodgkin lymphoma are as follows:
Palpable, painless lymphadenopathy can be seen in the cervical area (neck, 60-80%), axilla (armpit, 6-20%), and, less commonly, in the inguinal area (groin, 6-20%); it is described as rubbery adenopathy
Involvement of the Waldeyer ring (back of the throat, including the tonsils) or occipital (lower rear of the head) or epitrochlear (inside the upper arm near the elbow) areas is infrequently observed
Splenomegaly and/or hepatomegaly may be present Superior vena cava syndrome may develop in patients with massive mediastinal
lymphadenopathy Central nervous system (CNS) symptoms or signs may be due to paraneoplastic
syndromes, including cerebellar degeneration, neuropathy, Guillain-Barre syndrome, or multifocal leukoencephalopathy.
Diagnostic Considerations
Other diseases to be considered in the differential diagnosis of Hodgkin lymphoma include the following:
Any disease presenting with lymphadenopathy and constitutional symptoms HIV infection Hypersensitivity reaction Other solid tumors

Because Hodgkin lymphoma is considered a curable malignancy and the differential diagnosis is broad, medicolegal problems may arise from failure to diagnose the disease in a timely manner, possibly due to the following factors:
The misinterpretation of B symptoms A lack of follow-up for abnormal chest radiographs or physical examination findings A missed pathologic diagnosis because a needle biopsy was obtained rather than an
excisional lymph node biopsy
Occasionally, Hodgkin lymphoma can present as hemophagocytic syndrome (hemophagocytic lymphohistiocytosis).[11] Hemophagocytic syndrome is associated with Epstein-Barr virus antigen expression by Reed-Sternberg cells and has the following clinical and laboratory characteristics:
Pancytopenia Fever Hepatosplenomegaly with liver function test abnormalities Elevated serum levels of ferritin and triglycerides Phagocytosis of hematopoietic lineage cells by benign macrophages
Differential Diagnoses
Cytomegalovirus Infectious Mononucleosis Lung Cancer, Oat Cell (Small Cell) Lymphoma, Non-Hodgkin Sarcoidosis Serum Sickness Syphilis Systemic Lupus Erythematosus Toxoplasmosis Tuberculosis
Approach Considerations
The foundation for determining the ideal Hodgkin lymphoma treatment is accurate staging, which requires a comprehensive evaluation of possible sites of disease by imaging and sampling (biopsy), as well as an assessment of prognostic factors
Imaging
For imaging studies, anteroposterior and lateral chest radiography is performed to assess the bulk of the mediastinal mass, which has prognostic importance. On computed tomography (CT) scans of the chest, abdomen, and pelvis, possible abnormal findings include enlarged lymph nodes, hepatomegaly and/or splenomegaly (with or without focal parenchymal abnormalities), lung nodules or infiltrates, and pleural effusions. Positron emission tomography (PET) scanning is now considered essential to the initial staging of Hodgkin lymphoma, and this is often performed in conjunction with CT scanning.[12] A mediastinal

mass, representing mediastinal lymphadenopathy, is a very common finding in classic Hodgkin lymphoma, although it is uncommon in nodular lymphocyte-predominant Hodgkin disease (NLPHD).
Biopsy
A histologic diagnosis of Hodgkin lymphoma is always required. An excisional lymph node biopsy is recommended because the lymph node architecture is important for histologic classification. When a patient presents with neck lymphadenopathy and risk factors for a head and neck cancer, a fine-needle aspiration (FNA) is usually advised as the initial diagnostic step, followed by excisional biopsy if squamous cell histology is excluded.
Bone marrow biopsies are indicated in some cases. Bone marrow involvement is more common in patients who are elderly or have advanced-stage disease, systemic symptoms, or a high-risk histology. Because Hodgkin lymphoma in the bone marrow is often patchy, bilateral bone marrow biopsies are advised to improve yield. A bone marrow biopsy can be omitted in patients with stage I Hodgkin lymphoma and some patients with stage II disease without hematologic abnormalities.
Sampling of a pleural effusion by thoracentesis and examination of the cells obtained may be useful in the evaluation of Hodgkin lymphoma. The pleural fluid may be an exudate or transudate, or it may be chylous.
CNS evaluation by lumbar puncture and magnetic resonance imaging (MRI) should be performed if symptoms or signs of CNS involvement are present. CNS involvement with Hodgkin lymphoma is exceedingly rare, but it has been reported.
Blood Studies
Hematological (complete blood cell [CBC] count) and blood chemistry studies may reveal nonspecific findings in patients with Hodgkin lymphoma that may be associated with disease extent. Several of these findings have been used as prognostic factors.
CBC count studies for anemia (low red blood cell count), lymphopenia (low white blood cell count), excess neutrophils (neutrophilia), or eosinophils (eosinophilia) should be performed. Hodgkin lymphoma–associated anemia is most commonly the anemia of chronic disease. However, it may result from bone marrow involvement by tumor or from the presence of an autoantibody (as indicated by a positive warm-agglutinin on a Coombs test). Platelet counts may be increased or decreased.
The erythrocyte sedimentation rate (ESR)—a general marker of inflammation—may be elevated in Hodgkin lymphoma. An elevated ESR has been associated with worse prognosis. However, the ESR is a nonspecific test that should not be used for Hodgkin lymphoma screening.
Lactate dehydrogenase (LDH) may be increased. LDH may correlate with the bulk of disease.

Serum creatinine may be elevated, in the rare cases of nephrotic syndrome associated with Hodgkin lymphoma. Alkaline phosphatase (ALP) may be increased due to the presence of liver or bone involvement. Other uncommon laboratory findings include hypercalcemia, hypernatremia, and hypoglycemia (due to the presence of insulin autoantibodies).
An HIV test is important in the workup of Hodgkin lymphoma, because antiviral therapies can improve disease outcomes in HIV-positive patients.[13]
Serum levels of cytokines (interleukin [IL]-6, IL-10) and soluble CD25 (IL-2 receptor) correlate with tumor burden, systemic symptoms, and prognosis, but these studies are generally obtained only in special situations or in the context of a clinical trial.
Staging Laparotomy
A staging laparotomy is a surgical procedure that includes splenectomy with biopsies of the liver and lymph nodes in the para-aortic, mesenteric, portal, and splenic hilar regions. At present, a staging laparotomy procedure is very rarely indicated, because even early-stage Hodgkin lymphoma is most often treated with combination chemotherapy.
The procedure can be helpful in rare cases in which radiation therapy is under consideration as the sole treatment of early-stage Hodgkin lymphoma.
Staging
Clinical staging involves assessment of disease extent by clinical examination, history, and imaging techniques. When staging laparotomies are used as part of staging, the disease extent is designated as pathologic staging.[14]
The Ann Arbor classification (1971) is used most often for Hodgkin lymphoma. It classifies cases into the following 4 stages, principally on the basis of lymph node involvement:
Stage I - a single lymph node area or single extranodal site Stage II - 2 or more lymph node areas on the same side of the diaphragm Stage III - denotes lymph node areas on both sides of the diaphragm Stage IV - disseminated or multiple involvement of the extranodal organs
Involvement of the liver or the bone marrow is considered stage IV disease. For staging classifications, the spleen is considered to be a lymph node area. Involvement of the spleen is denoted with the S suffix (ie, IIBS).
A or B designations denote the absence or presence of B symptoms. A "B" designation includes the presence of 1 or more of the following:
Fever (temperature >38°C) Drenching night sweats Unexplained loss of more than 10% of body weight within the preceding 6 months
An "A" designation is the absence of the above.

An "X" designation is sometimes used to indicate the presence of bulky disease.
Approximately one third of new patients have splenic involvement based on laparotomy data. However, this depends on the histologic subtype. Two thirds of patients with the mixed cellularity subtype have splenic involvement, compared with only one third of patients with the lymphocyte-depleted or nodular sclerosis histology. When liver or bone marrow involvement is present, the spleen is likely to be involved.
Spread of Hodgkin lymphoma takes place via the lymphatics, hematogenous routes, and direct extension. Contiguous involvement of extranodal sites (eg, involvement of the lung parenchyma due to direct extension of large mediastinal lymphadenopathy) is not considered stage IV disease. Rather, it is designated with the E suffix (ie, IIBE).
Unfavorable factors in limited-stage Hodgkin lymphoma
Many factors that can be assessed at the time of diagnosis can help to determine whether a patient's Hodgkin lymphoma has a high or low risk of proving resistant to therapy. Such an estimate is important for treatment planning. In addition, it can help identify patients who would potentially benefit from participating in clinical trials that seek to either minimize therapy in low-risk patients or intensify therapy in high-risk patients.
In patients with stage I or II disease, the following factors are considered unfavorable and, if present, will increase the intensity of the recommended initial therapy:
Bulky disease An ESR of 50 mm/h or higher, if the patient is otherwise asymptomatic More than 3 sites of disease involvement The presence of B symptoms The presence of extranodal disease
For this purpose, bulky disease is defined as a mediastinal mass greater than one third of the intrathoracic diameter on a chest radiograph or greater than 35% of the thoracic diameter at vertebral level T5-6. Hodgkin lymphoma also qualifies as bulky disease if it is greater than 10 cm in diameter on a CT scan.
Unfavorable factors in advanced Hodgkin lymphoma
The International Prognostics Factors Project (IPFP) was a survey of the characteristics at diagnosis and outcomes of 5,141 patients with Hodgkin lymphoma with either advanced disease, defined as either stage III or IV disease, or earlier-stage disease with systemic symptoms or bulky features. The following characteristics were determined to each contribute independently to an increased relative risk for Hodgkin lymphoma progression despite therapy:
Serum albumin less than 4 g/dL Hemoglobin less than 10.5 g/dL Male sex Stage IV disease Age 45 years or older White blood cell (WBC) count greater than 15,000/μL

Lymphocyte count less than 600/μL or less than 8% of the total WBC count
The International Prognostic Score (IPS) is considered to be the number of features that are present at diagnosis for Hodgkin lymphoma.[15] The IPS correlates with the rate of freedom from disease progression and overall survival. Patients with 0-1 of these factors would be predicted to have a 90% overall survival. In contrast, patients with 4 or more of these factors may have an overall survival rate of only 59%.
One limitation of this scoring method is its inability to clearly identify the highest-risk subgroup of patients with Hodgkin lymphoma—that is, those who may benefit from up-front high-dose therapy. Analysis of cytokines and other serum markers may help to identify these patients in the future.
Approach Considerations
Treatment of Hodgkin lymphoma is tailored to disease type, disease stage, and an assessment of the risk of resistant disease. Hodgkin lymphoma is considered to be a curable malignancy, but therapies for this disease can have significant long-term toxicity. Therefore, advances in treatment protocols have sought to (1) minimize the treatment given to patients with early-stage, low-risk disease and (2) safely maximize the treatment given to patients with disease that is likely to be refractory to standard therapies.
This is particularly important in the elderly. As noted above, the elderly are at increased risk of not only developing Hodgkin lymphoma but also of developing toxicity from Hodgkin lymphoma treatment.[16] Interest in decreasing the toxicity of therapy in the elderly is leading to newer regimens being developed, which have shown some early promising results but have not been directly compared with the existing standard regimens. One such regimen is procarbazine, vinblastine, doxorubicin, and gentamicin (PVAG), which showed excellent response rates and good tolerability in a phase 2 trial.[17]
Because of the limited number of patients with Hodgkin lymphoma and the importance of the clinical questions that remain about optimal disease management, patient involvement in clinical trials is strongly encouraged.
Published guidelines from the National Comprehensive Cancer Network (NCCN),[18] the European Society of Medical Oncology (ESMO),[19] and the International Harmonization Project[20] provide consensus opinions from leading experts on evidence-based approaches to the diagnosis and treatment of Hodgkin lymphoma.
Combined-modality therapy (radiation therapy [XRT] and chemotherapy) is frequently the preferred approach in for most patients. In early-stage disease, combined-modality therapy provides a synergistic effect while limiting the total exposure to any particular agent.[21]
However, some randomized trials have suggested that radiation may not be necessary in early stage disease and adds considerable toxicity. A study by Meyer et al that was performed before the use of limited field radiation, causing some problems with its interpretation provides the first evidence that radiation can safely be omitted in early stage Hodgkin lymphoma.[22]

In patients with advanced Hodgkin lymphoma, involved-field XRT can be used for sites of persistent disease following chemotherapy. XRT to sites of disease that were bulky at diagnosis is a standard feature of the Stanford V regimen.
Despite the high rate of cure for this disease, many cases Hodgkin lymphoma do relapse. In most of these cases, salvage chemotherapy followed by high-dose chemotherapy (HDC) with autologous hematopoietic stem cell support is indicated.[23] The role of allogeneic hematopoietic stem cell transplantation for Hodgkin lymphoma is being explored.[24] This form of treatment should ideally be pursued only in the context of a clinical trial.
Nodular lymphocyte predominant Hodgkin disease (NLPHD) is clinically distinct from classic Hodgkin lymphoma in that it generally presents as early- stage disease that can be treated with local measures (surgery, radiation) or followed expectantly. However, some cases of NLPHD can transform to aggressive non-Hodgkin lymphomas that are treated using standard protocols.
Consultations
The following consultations should be sought in cases of Hodgkin lymphoma:
Hematologist/oncologist Radiation oncologist Social worker Tertiary care center for consideration of clinical trial enrollment
Guidelines
Two sets of consensus guidelines, written by the NCCN and the ESMO, currently help guide the standard of care for Hodgkin lymphoma. The guidelines are very similar, but the NCCN guidelines have more specific recommendations for response evaluation and follow-up.
In addition, a set of revised response criteria for malignant lymphoma, including Hodgkin lymphoma, and recommendations for using positron-emission tomography (PET) scanning to monitor Hodgkin lymphoma were published by the International Harmonization Project. Together, these 3 guidelines provide specific guidance for evaluating the response of disease therapy.
Goals of Therapy
The primary goal of therapy is to induce a complete remission (CR), which is defined as the disappearance of all evidence of disease, as evaluated by PET/CT scanning, physical examination, and bone marrow examination (if appropriate).[20] PET/CT scanning should be obtained at least 3 weeks and preferably 6-8 weeks following the last therapy in order to lessen the risk of false-positive scans resulting from nonmalignant inflammatory responses.
A partial remission (PR) is defined as "regression of measurable disease and no new sites" of disease. A failure to achieve a CR with initial therapy or a relapse after having attained a CR

is an indication for additional HDC and/or XRT, often with autologous hematopoietic stem cell support.
Assessment of Treatment Response
The high sensitivity of positron emission tomography (PET) scanning for classic Hodgkin lymphoma has won this imaging modality a prominent role in the assessment of treatment response in affected patients. A positive PET scan following therapy correlates strongly with a high risk of relapse. An early attainment of a negative PET scan during therapy is a positive prognostic indicator, but studies have not yet provided information on whether a course of therapy can be safely shortened in this situation.[25, 26]
PET/CT scans should be obtained at least 3 weeks, and preferably 6-8 weeks following the last therapy in order to lessen the risk of false-positive scans resulting from nonmalignant inflammatory responses.[27] Biopsies of PET-positive lesions are typically done in order to test for persistent Hodgkin lymphoma.
Radiation Therapy
For treatment of classic Hodgkin lymphoma, radiation therapy is generally administered in combination with chemotherapy. Radiation fields and doses are selected to minimizing the potential side effects of therapy, while maximizing the potential for long-term disease-free survival. Involved-field therapy encompasses only the areas of observed disease. Regional-field therapy extends the involved field to include adjacent lymph regions.
Other fields that have been used historically and may be used in exceptional clinical circumstances include the mantle field, covering the mediastinal, cervical, and axillary nodes; and the inverted Y field, covering the para-aortic, pelvic, and inguinal nodes. Subtotal nodal irradiation involves the mantle field plus the para-aortic nodes.
The mantle field is shaped in order to reduce radiation exposure to the heart and lungs. Careful avoidance of the spinal cord can reduce the risk of myelitis. Shielding the testes and oophoropexy (temporary surgical suspension of the ovaries [eg, outside of a radiation field]) are important during the reproductive years.
The dose of radiation to be administered is tailored to the specific clinical scenario. Doses used in combined modality therapy are 30-36 Gy for bulky disease sites and 20-30 Gy for nonbulky disease sites. When radiation therapy is used alone, doses may range from 30-44 Gy.
In the NLPHD subtype of Hodgkin lymphoma, involved-field radiation therapy may be recommended for stage IA and IIA disease.
Induction Chemotherapy Regimens
The following induction regimens are given as initial treatment for Hodgkin lymphoma:
MOPP (mechlorethamine, vincristine, procarbazine, prednisone)

ABVD (Adriamycin [doxorubicin], bleomycin, vinblastine, dacarbazine) Stanford V (doxorubicin, vinblastine, mustard, bleomycin, vincristine, etoposide, prednisone) BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine,
prednisone)
All the medications in these regimens are given intravenously, except for prednisone and procarbazine, which are given orally.
The MOPP regimen was the first effective combination chemotherapy for Hodgkin lymphoma. It is a 4-drug regimen developed by Vincent DeVita and colleagues at the National Cancer Institute in the mid 1960s and is primarily of historical importance.
The ABVD regimen was designed in Italy by Gianni Bonadonna and his colleagues in the early 1970s. This combination has now become the standard chemotherapy regimen for Hodgkin lymphoma. ABVD is superior to MOPP in terms of DFS and has a lower incidence of sterility and secondary leukemia.[28]
The Stanford V regimen is a multidrug regimen created at Stanford University by Sandra Horning and colleagues.[29] The drugs are administered weekly, alternating myelosuppressive and nonmyelosuppressive agents, for 12 weeks. Involved-field XRT at the conclusion of the 12-week regimen is an important part of this regimen. A potential advantage of the Stanford V regimen is that its use of a broad spectrum of chemotherapy drugs can limit the exposure (and potential side-effects) of any single drug.
The BEACOPP regimen was developed in Germany by Volker Diehl and colleagues.[30] A dose-intensified version of BEACOPP (escalated BEACOPP), with higher doses of etoposide, doxorubicin, and cyclophosphamide and the addition of granulocyte colony-stimulating factor (G-CSF) for neutrophil support, has also been developed and may be useful for unfavorable, advanced-stage Hodgkin lymphoma. However, escalated BEACOPP is associated with greater hematologic toxicity and a higher incidence of secondary malignancies, including acute myelogenous leukemia (AML).
In a 10-year follow-up of the German Hodgkin Study Group HD9 trial, Engert et al reported that escalated BEACOPP significantly improved freedom from treatment failure (82% vs 70%) and overall survival (86% vs 80%) compared with baseline BEACOPP.[31] The study compared the 2 doses of BEACOPP with COPP alternating with ABVD; COPP/ABVD has been the standard of care for this patient population, but freedom from treatment failure was only 64% and overall survival was only 75% in this group.
A study by Viviani et al demonstrated that BEACOPP produced better initial outcomes in patients with advanced Hodgkin disease than treatment with ABVD but found no significant long-term differences between the regimens.[32]
Ongoing clinical trials will directly compare the ABVD regimen to the Stanford V and escalated BEACOPP regimens.
A meta-analysis of 14 trials involving 9993 patients with Hodgkin lymphoma found that intense chemotherapy with BEACOPP conferred a 10% survival advantage at 5 years over treatment with ABVD. Overall survival was highest in patients who received 6 cycles of escalated BEACOPP: the 5-year survival was 95%, compared with 88% for ABDV.

Escalated BEACOPP was associated with more acute hematologic toxicity than ABDV was, and also with secondary malignancies and late cardiovascular effects.[33, 34, 35]
A study by Bauer et al found that patients aged 16-60 years with early unfavorable or advanced stage disease benefitted from escalated BEACOPP in terms of progression-free survival; however, no significant difference was noted in overall survival.[36]
While in general Hodgkin lymphoma curable for most patients, continued interest in the use of novel agents has led to the development of newer treatment regimens using newer targeted agents. For example, the monoclonal antibody Rituximab, directed at the B cell marker CD20 has been combined with standard ABVD in two early phase II trials with interesting results. While CD20 is most often not expressed on the malignant cell (i.e. the HRS cell) anti-CD20 therapy appears to improve on the efficacy of ABVD in this disease. This may occur through changes in the tumor microenvironment by affecting associated non-malignant lymphocytes. These data, while intriguing, will require confirmation in phase III studies before they can become part of routine clinical practice. These studies are on going.
Induction chemotherapy schedules
The MOPP regimen is given every 28 days for 6 or more cycles, as follows:
Mechlorethamine: 6 mg/m2, days 1 and 8 Vincristine: 1.4 mg/m2, days 1 and 8 Procarbazine: 100 mg/m2, days 1-14 Prednisone: 40 mg/m2, days 1-14, cycles 1 and 4 only
The ABVD regimen is given every 28 days for 6 or more cycles, as follows:
Adriamycin: 25 mg/m2, days 1, 15 Bleomycin: 10 mg/m2, days 1, 15 Vinblastine: 6 mg/m2, days 1, 15 Dacarbazine: 375 mg/m2, days 1, 15
The Stanford V regimen is given as follows[37] :
Vinblastine: 6 mg/m2, weeks 1, 3, 5, 7, 9, 11 Doxorubicin: 25 mg/m2, weeks 1, 3, 5, 9, 11 Vincristine: 1.4 mg/m2, weeks 2, 4, 6, 8, 10, 12 Bleomycin: 5 units/m2, weeks 2, 4, 8, 10, 12 Mechlorethamine: 6 mg/m2, weeks 1, 5, 9 Etoposide: 60 mg/m2 twice daily, weeks 3, 7, 11 Prednisone: 40 mg/m2, every other day, weeks 1-10, tapered weeks 11, 12 XRT to bulky sites 2-4 weeks following the end of chemotherapy
The escalated BEACOPP regimen is given every 3 weeks for 8 cycles, as follows:
Bleomycin: 10 mg/m2, day 8 Etoposide: 200 mg/m2, days 1-3 Doxorubicin: 35 mg/m2, day 1 Cyclophosphamide: 1,250 mg/m2, day 1

Vincristine: 1.4 mg/m2, day 8 Procarbazine: 100 mg/m2, days 1-7 Prednisone: 40 mg/m2, days 1-14
Salvage Chemotherapy Regimens
When induction chemotherapy fails, or patients experience relapse, salvage chemotherapy is generally given. Salvage regimens incorporate drugs that are complementary to those that failed during induction therapy. Commonly used salvage regimens include the following:
ICE (ifosfamide, carboplatin, etoposide) DHAP (cisplatin, cytarabine, prednisone) ESHAP (etoposide, methylprednisolone, cytarabine, cisplatin)
Salvage chemotherapy schedules
The ICE regimen is given as follows:
Ifosfamide: 5 g/m2, day 2 Mesna: g/m2, day 2 Carboplatin: AUC 5, day 2 Etoposide: 100 mg/m2, days 1-3
The DHAP regimen is given as follows:
Cisplatin: 100 mg/m2, day 1 Cytarabine: 2 g/m2, given twice on day 2 Dexamethasone: 40 mg, days 1-4
In the EPOCH regimen, etoposide, vincristine, and doxorubicin are given together over a total of 96 hours in a continuous intravenous infusion, as follows:
Etoposide: 50 mg/m2, days 1-4 Vincristine: 0.4 mg/m2, days 1-4 Doxorubicin: 10 mg/m2, days 1-4 Cyclophosphamide: 750 mg/m2, day 5 Prednisone: 60 mg/m2, days 1-6
Hematopoietic Stem Cell Transplantation
High-dose chemotherapy (HDC) at doses that ablate the bone marrow is feasible with reinfusion of the patient's previously collected hematopoietic stem cells (autologous transplantation) or infusion of stem cells from a donor source (allogeneic transplantation). Patients with refractory or relapsed Hodgkin lymphoma should be promptly referred to centers capable of HDC with hematopoietic stem cell support.
Historically, hematopoietic stem cells have been obtained from bone marrow, but they are now typically obtained by pheresis of peripheral blood lymphocytes. A validated and

relatively safe conditioning regimen for autologous transplantation is the BEAM regimen (carmustine [BCNU], etoposide, cytarabine, melphalan).[23]
Myeloablative chemotherapy
High-dose therapy, which requires hematopoietic stem cell support for recovery, is given according to the BEAM regimen. Different schedules for BEAM exist that vary primarily in the dose of etoposide administered. The following is the version used by Schmitz et al in a key randomized, prospective clinical trial[23] :
BCNU 300 mg/m2, day –7 Etoposide 150 mg/m2, every 12 hours, total of 8 doses, days –7 to –4 Cytarabine 200 mg/m2, every 12 hours, total of 8 doses, days –7 to –4 Melphalan 140 mg/m2, day –3
Following this chemotherapy regimen, autologous hematopoietic stem cells are administered on day 0.
Treatment of Early-Stage, Low-Risk Disease
Patients with clinical stages IA or IIA classic Hodgkin lymphoma who do not have unfavorable factors (ie, bulky disease, elevated ESR, >3 sites of involvement, B symptoms, extranodal disease) are categorized as having early-stage, low-risk disease.[21, 38] These patients generally should receive 2-4 cycles of the ABVD regimen or 8 weeks of the Stanford V regimen, followed by involved-field XRT.
Radiation alone has been shown to be inferior to the combined modality approach in early stage, low-risk disease. If XRT is contraindicated or not possible, then chemotherapy should continue for 2 additional cycles following the attainment of a CR.
In a multicenter, randomized trial, Engert et al determined that 2 cycles of ABVD followed by 20 Gy of involved-field radiation therapy (IFRT) is as effective as 4 cycles of ABVD followed by 30 Gy of involved-field radiation in patients with early-stage Hodgkin lymphoma who had a favorable prognosis. Toxic effects and adverse events were more common in the group who received the 4 cycles of ABVD and higher dose level of radiation.[39] This study has led most investigators to recommend 2 cycles of ABVD and 20 Gy of IFRT for patients with early-stage, low-risk disease; however, some studies looking at chemotherapy alone have been published, showing no difference in outcomes when chemotherapy with ABVD was compared with ABVD without radiation in early stage Hodgkin lymphoma.[22] A study by Barbaro et al is limited by the use of outdated expanded fields, but taken together, the data suggest that either 2 cycles of ABVD with 20 Gy IFRT or 4-6 cycles of ABVD alone are appropriate forearlystageHodgkin lymphoma.
Treatment of Early-Stage Disease with Unfavorable Factors
Patients with clinical stages I or II with bulky disease, with or without unfavorable factors (ie, elevated ESR, >3 sites of involvement, B symptoms, extranodal disease), are classified as

having early-stage disease with unfavorable factors. Chemotherapy plus involved-field XRT is indicated for these patients. The German Hodgkin Study Group HD11 trial demonstrated that ABVD was equivalent to BEACOPP in this setting, so the lower-toxicity regimen (ABVD) is preferred.[40] Stanford V with involved-field XRT is another reasonable option.
In general, these patients would be treated with 2 cycles of ABVD and have an interim PET scan, the results of which will dictate further therapy. In general, 2 cycles beyond best response (or maximum of 6 cycles of ABVD) is used. Patients with residual disease should always have repeat biopsies to determine therapy. Those with initial bulky disease should have IFRT.
Treatment of Advanced Disease
Patients are considered to have advanced disease if they are stage III or IV. Chemotherapy is the mainstay of therapy, with radiation reserved for initial bulky sites or residual PET activity. The NCCN recommends either 4 cycles of the ABVD regimen or 12 weeks of the Stanford V regimen, followed by restaging with PET/CT scanning. If a patient has positive results on PET scans following the ABVD regimen, an additional 2 cycles are administered.
Once a CR has been achieved, involved-field XRT is given to sites of intial bulky disease. If, after 12 weeks of the Stanford V regimen, a patient is in a CR or PR has been attained, then involved-field XRT is standard.
EMSO recommends that patients with this category of disease receive either 8 cycles of the ABVD regimen or the standard-dose BEACOPP regimen, with involved-field XRT applied only to tumors initially more than 7.5 cm or to sites of residual disease following chemotherapy. For patients with advanced-stage disease, the use of the escalated BEACOPP regimen has support in the literature.
However, a recent study by Viviani et al calls the use of escalated BEACOPP into question. In this study, while initial disease control was better with BEACOPP than with ABVD, long-term survival was no different because nonresponding patients were effectively salvaged with high-dose chemotherapy and stem cell transplantation. These data suggest that ABVD should be the initial treatment of choice for the majority of advanced stage patients.[41]
Treatment of Nodular Lymphocyte Predominant Hodgkin Disease
Early-stage NLPHD can be treated with local excision, involved-field XRT, or expectant management (close observation).[42] Advanced-stage disease may represent histologic transformation to T-cell rich B-cell lymphoma (TCR-BCL) or diffuse large cell B-cell lymphoma (DLCBL). These are types of non-Hodgkin lymphoma that should be treated with a typical non-Hodgkin regimen, such as R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone).
Rituximab is a humanized monoclonal antibody that is specific for CD20, a cell-surface antigen expressed by the malignant lymphocytic and histiocytic (L&H) cells in NLPHD. It has shown activity as a single agent in NLPHD. On long-term follow-up, the German

Hodgkin Lymphoma Study Group observed a 94% overall response rate, with 8 complete remissions, from their population of 15 patients treated with rituximab for relapsed/refractory NLPHD.[43]
Therefore, rituximab is a promising agent for advanced NLPHD. Nevertheless, the use of rituximab in NLPHD, especially in early-stage disease, should ideally be pursued in the context of a clinical trial.
A phase 2 study by Eichenauer et al found that results with rituximab appear inferior when compared with radiotherapy and combined-modality treatment in patients with early stage NLPHD. However, the authors concluded that investigation of anti-CD20 antibody–based combinations in patients with NLPHD is indicated.[44]
An era-to-era comparison between ABVD treatment and radiotherapy alone found that treating limited-stage NLPHD similar to classical Hodgkin lymphoma may improve outcome compared with the use of radiation alone.[45]
Treatment in HIV-Infected Patients
In patients with advanced Hodgkin lymphoma and HIV infection, the results with standard chemotherapy (eg, ABVD, BEACOPP) can be dramatically improved by simultaneous treatment with highly active antiretroviral therapy (HAART). Such therapy generally involves 3 drugs: 2 nucleoside reverse transcriptase inhibitors combined with a protease inhibitor, a nonnucleoside reverse transcriptase inhibitor, or a viral fusion inhibitor.
Treatment of Refractory or Relapsed Disease
Patients with Hodgkin lymphoma who have never entered a CR, or whose disease has relapsed after the attainment of a CR, have a very poor prognosis when treated with standard chemotherapy and radiation. Therefore, high-dose chemotherapy with autologous stem cell transplantation is recommended for these patients.[46]
In this procedure, salvage chemotherapy is first administered to help reduce the size of the persistent disease and obtain a CR, if possible. The number of cycles to be administered depends on how well the disease is responding to therapy. An optimal situation is one in which the disease enters a CR with negative PET scan findings, although one study demonstrated that patients may achieve long-term disease-free survival even if their condition has little or no response.[47]
Following one of the cycles of salvage chemotherapy, hematopoietic stem cells are collected from the peripheral blood by leukapheresis and are stored frozen. Following the administration of myeloablative chemotherapy (eg, BEAM), the stored hematopoietic stem cells are thawed and reinfused into the patient to facilitate hematopoietic recovery. HDC with autologous stem cell transplantation can provide better than 50% long-term, progression-free survival for patients with relapses, although specific predicted outcomes vary widely depending on patient-specific risk factors.

Many questions relating to salvage and HDC therapy for patients with Hodgkin lymphoma need to be addressed and are the subject of ongoing clinical trials. These include the following:
The optimal salvage regimen or regimens The ideal conditioning regimen or regimens The potential benefits of twin transplants compared with single transplants How to prospectively identify those patients who are unlikely to benefit from HDC
and how to best manage their disease
In some cases in which HDC fails, allogeneic stem cell transplantation may be a viable option. In this method, myeloablative therapy (chemotherapy and sometimes XRT) is followed by the infusion of hematopoietic stem cells from a genetically matched donor.[24]
This offers the potential for an immunologic antitumor effect from T cells provided by the hematopoietic stem cell donor, which may improve the chances for cure of the disease.
Historically, allogeneic stem cell transplantation for Hodgkin lymphoma has been considered too high-risk for most patients, due high transplant-related mortality. However, new transplant protocols use less toxic conditioning regimens and may be safer and more effective for patients with refractory Hodgkin lymphoma.[48]
Brentuximab vedotin was approved by the US Food and Drug Administration (FDA) in August 2011. It is a CD30-directed antibody-drug conjugate consisting of IgG1 antibody cAC10, specific for human CD30, and the microtubule disrupting agent, monomethyl auristatin E (MMAE, or vedotin).[49] Results from a study of patients with Hodgkin lymphoma in whom autologous stem cell transplantation and a median of 4 chemotherapy regimens had failed (n = 102) showed that 73% (95% confidence interval [CI], 65-83%) achieved an objective response to brentuximab vedotin therapy, including 32% with complete remission (95% CI, 23-42%) and 40% with partial remission (95% CI, 32-49%). Response duration averaged 6.7 months (range, 1.3-21.9 mo).[50]
A phase 2 study by Witzig et al found that the oral farnesyltransferase inhibitor tipifarnib has activity in refractory or relapsed lymphoma, particularly in heavily pretreated T-cel and Hodgkin lymphoma groups, with little activity in non-Hodgkin lymphoma. Further studies are warranted.[51]
Immunotherapy
Targeted immunotherapeutic agents are currently being evaluated for potential use in Hodgkin lymphoma.[25] The CD30 cell surface antigen, which is expressed at high levels on Reed-Sternberg cells, is a target of 2 monoclonal antibodies, SGN-30 and MDX-60.[52, 53, 54] In August 2011, the US Food and Drug Adminisration (FDA) granted fast-track approval to brentuximab, a CD30 antibody–drug condjugate, for the treatment of relapsed/refractory Hodgkin lymphoma that has progressed on 2 other lines of multiagent chemotherapy. This agent was approved based on early clinical trials suggesting a complete response rate of 34% and an objective response rate of 74%.[55]
Complications of Therapy

Cardiac disease
Mantle radiotherapy increases the risk the risk of coronary artery disease, chronic pericarditis, pancarditis, valvular heart disease, and defects in the conduction system.[56, 57] Patients with history of mediastinal radiation have a 3-fold increase in their risk of cardiac death.
A study of patients who had previously undergone mediastinal irradiation for Hodgkin lymphoma but who had no clinical evidence of heart disease demonstrated a significant incidence of silent coronary artery obstruction and previous ventricular damage.[58] Based on these results, it is reasonable to initiate functional screening 5 years after XRT in patients with Hodgkin lymphoma.
Pulmonary disease
The ABVD regimen contains bleomycin, a drug associated with dose-related pulmonary toxicity, mainly interstitial pneumonitis, which may lead to fibrosis. The addition of mantle irradiation enhances lung injury. Pulmonary symptoms, such as cough or dyspnea on exertion, are observed in 50% of patients, and declining pulmonary function is observed in approximately one third of patients during ABVD chemotherapy, with or without radiation therapy. This may necessitate dose reductions or even discontinuation of bleomycin.
Although acute toxicity is common, the incidence of severe long-term pulmonary toxicity is low. Fatal pulmonary toxicity has been reported in up to 2-3% of patients treated with the ABVD regimen.
Secondary cancers
Secondary leukemias and solid tumors are significant causes of morbidity and mortality for patients who have received early therapies, including the MOPP regimen and mantle radiation therapy. With modern therapies that emphasize the widespread use of the ABVD and Stanford V regimens and the application of radiation to involved fields only, the incidence of secondary cancers is expected to be much lower.
The most common secondary malignancy following treatment for Hodgkin lymphoma is lung cancer. Both chemotherapy with alkylating agents and irradiation are associated with a 10-fold increased relative risk of lung cancer. Smoking can further increase the risk.
In addition, retrospective data have suggested that survival is worse in Hodgkin lymphoma survivors who develop lung cancer compared with matched cohorts with de novo lung cancer.[59]
Myelodysplastic syndromes/acute myelogenous leukemia (MDS/AML) is a particular concern. In the Stanford case series, the projected risk for developing MDS/AML over a follow-up period of 35 years was 2%, and the relative risk compared with matched controls was 38%. The MOPP regimen is associated with an approximately 5% incidence of MDS/AML. With the ABVD regimen the risk is lower, less than 1%.
MDS/AML is usually seen in the first 3-8 years following treatment for Hodgkin lymphoma; subsequently, the risk appears to decline. These findings are consistent with the biology of secondary leukemias following alkylator therapy. MDS/AML usually develops in the context

of an MDS with cytogenetic abnormalities in chromosomes 5 and/or 7. Exposure to alkylating agents (eg, the mechlorethamine used in the MOPP regimen) has been implicated.
Exposure to epipodophyllotoxins (etoposide and teniposide) may also result in AML, which generally develops within 3 years and is associated with chromosomal abnormalities at band 11q23.
Breast cancer is 19 times more likely to occur in patients treated with mantle radiation therapy when they are younger than 30 years. If female patients are exposed to chest radiation therapy when they are younger than 15 years, this relative risk increases to 136. MOPP chemotherapy also produces an increased risk for breast cancer when combined with XRT.
Patients in the Stanford case series were also found to have increased risks of developing a variety of other cancers. These include melanoma, non-Hodgkin lymphoma, soft-tissue sarcoma, salivary gland cancers, pancreatic cancers, and thyroid cancers.
A study by Swerdlow et al found that the risk of second malignancy from chemotherapy alone is lower and affects fewer anatomic sites than combined treatment modalities. The authors concluded the risk of second malignancy was slight after 15 years.[60]
Taken in aggregate, these trial results suggest that altering the treatment paradigms of Hodgkin lymphoma to maximize curability while preventing long-term complications should be a focus of ongoing research. Using the least amount of therapy required to cure the disease and minimize complications should be the goal. Early results have suggested that modification of treatment is feasible and have shown some decreased rates of secondary cancers.[61]
Infertility
The degree of infertility widely varies with the regimen used. MOPP chemotherapy causes permanent infertility in at least 80% of males and approximately 50% of females.[60] The escalated BEACOPP results in infertility in nearly 100% of patients treated.[61] The ABVD and Stanford V regimens pose a lower risk of permanent sterility than regimens that contain an alkylating agent (eg, MOPP chemotherapy).[62]
The EORTC Lymphoma Group reported an 82% rate of recovery of fertility in male patients who were treated without alkylating agents. Given the overall excellent prognosis of this disease and the early age of onset, fertility preservation must be kept in mind when designing treatment plans for these patients. Options include sperm banking for men and various pharmacologic treatments for women including gonadotropin-releasing hormone agonists, ovarian stimulation, and egg preservation.
Infectious complications
Patients who have undergone splenectomy are predisposed to bacterial sepsis secondary to encapsulated microorganisms (especially Streptococcus pneumoniae). Empiric antibiotic therapy should be instituted promptly in patients who have undergone splenectomy and present with fever. Pneumococcal vaccination before splenectomy and every 5-7 years thereafter is also recommended.

Influenza vaccination annually may help to reduce the incidence and/or complications of influenza in patients who have received bleomycin or chest radiation therapy.
Herpes zoster usually appears in previously irradiated dermatomes, but this condition may also occur in patients who have not been irradiated.
Other complications
Lhermitte syndrome(an electric-shock sensation that radiates along the back and legs upon flexion of the neck) can occur in approximately 15% of patients after mantle irradiation. Lhermitte syndrome is not associated with the development of radiation myelitis, and it does not require treatment. This syndrome may last for many months, but it will eventually resolve without long-term sequelae.
Elevation of thyroid stimulating hormone (TSH) occurs in one third of adult patients after neck/mediastinal radiation therapy.
Survivors of Hodgkin lymphoma have an increased incidence of fatigue, psychiatric distress (anxiety, depression), employment problems, family issues, and sexual functioning problems, as compared with individuals without this disease or relative to survivors of acute leukemia.[63, 64]
Long-Term Monitoring
Both the NCCN and the ESMO guidelines provide recommendations for the long-term follow-up of treated patients with Hodgkin lymphoma who are in complete remission.[18, 19]
Most relapses occur in the first 3 years after therapy. Follow-up visits are recommended every 2-4 months for the first 1-2 years and every 3-6 months for the next 3-5 years.
Follow-up examinations include the following:
History and physical examination Complete blood cell count and chemistry panel, including lactate dehydrogenase
(LDH), erythrocyte sedimentation rate (ESR), glucose, and lipid levels Thyroid-stimulating hormone (TSH) levels (at least annually if the patient has had
neck XRT) Chest x-ray or CT scans of the chest every 6-12 months in the first 2-5 years Abdominal and pelvic CT scans may be added every 6-12 months in the first 2-3
years, especially if the disease originally occurred below the diaphragm Spiral chest CT scans may be appropriate annually, starting 5 years after therapy, to
screen patients at increased risk for lung cancer Female patients who have received chest irradiation should be screened annually with
mammography, starting at age 40 years or 5-8 years following the XRT
Use of PET scans for surveillance in patients with complete remission is specifically not encouraged by the NCCN, due to the possibility of false-positive results.

Vaccinations against pneumococcus (especially in patients who have had splenectomy), Haemophilus influenzae, meningococcus, and influenza (annually, especially in patients who have received bleomycin or chest XRT), should be maintained.
Lung injury may result from mantle irradiation or ABVD chemotherapy. Baseline tests and follow-up evaluation with pulmonary function tests are recommended. The best parameter to follow is the carbon monoxide diffusion capacity.
Prominent goals in the follow-up of survivors of Hodgkin lymphoma include the following:
Identify secondary cancers in a timely manner Consider sepsis as a possible cause for fever in a splenectomized patient Diagnose and treat predictable complications of Hodgkin lymphoma treatment, such
as coronary artery, pulmonary, or thyroid disease
Medication Summary
Several chemotherapeutic agents in various combinations are used to treat Hodgkin lymphoma. The combinations vary by the stage of disease and by the treating institution. In patients with relapsing or unresponsive disease, hematopoietic stem-cell transplantation significantly prolongs disease-free survival. Various drug combinations have been used with stem-cell rescue.
Although the intended target is the malignant cells of Hodgkin lymphoma, the effects of chemotherapy on normal cells of the body are considerable and account for the adverse effects observed with these agents. Because most patients with Hodgkin lymphoma are long-term survivors, one of the goals of current therapy is to decrease the long-term adverse effects while maintaining excellent cure rates. The use of different therapeutic agents with nonoverlapping toxicities is one way to achieve this goal. Various combinations of the drugs presented below are used to treat Hodgkin lymphoma (see Treatment).
Although adverse effects vary with each drug, some are common to many drugs. These adverse effects include nausea, vomiting, alopecia, bone marrow suppression, and, less commonly, secondary malignancies.
Antineoplastic Agents
Class Summary
Cancer chemotherapy is based on an understanding of tumor cell growth and of how drugs affect this growth. After cells divide, they enter a period of growth (ie, phase G1), followed by DNA synthesis (ie, phase S). The next phase is a premitotic phase (ie, G2), then finally a mitotic cell division (ie, phase M).
Cell-division rates vary for different tumors. Most common cancers grow slowly compared with normal tissues, and the growth rate may be decreased in large tumors. This difference allows normal cells to recover more quickly than malignant ones after chemotherapy and is the rationale behind current cyclic dosage schedules.

Antineoplastic agents interfere with cell reproduction. Some agents are specific to phases of the cell cycle, whereas others (eg, alkylating agents, anthracyclines, cisplatin) are not. Cellular apoptosis (ie, programmed cell death) is another potential mechanism of many antineoplastic agents.
View full drug information
Mechlorethamine (Mustargen)
This alkylating agent is a component of the MOPP (mechlorethamine, vincristine, procarbazine, prednisone) regimen.
View full drug information
Bleomycin
Classified as antibiotic, bleomycin induces free radical–mediated breaks in strands of DNA. This agent is part of the ABVD (Adriamycin [doxorubicin], bleomycin, vinblastine, dacarbazine) regimen.
View full drug information
Vinblastine
Vinblastine is a vinca alkaloid that inhibits mitosis because of interactions with tubulin.
View full drug information
Dacarbazine
Dacarbazine is an alkylating agent that inhibits DNA, RNA, and protein synthesis. It inhibits cell replication in all phases of the cell cycle.
View full drug information
Etoposide (Toposar)
Etoposide is an epipodophyllotoxin that induces DNA strand breaks by disrupting topoisomerase II activity.
View full drug information
Vincristine (Vincasar PFS)

Vincristine is a vinca alkaloid with a mechanism of action similar to that of vinblastine.
View full drug information
Procarbazine (Matulane)
Procarbazine is an alkylating agent with mechanism of action similar to that of dacarbazine.
View full drug information
Prednisone
Prednisone is a corticosteroid used to treat leukemias and lymphomas because of its lympholytic activity.
View full drug information
Cyclophosphamide
Cyclophosphamide is an alkylating agent that is chemically related to nitrogen mustards. The mechanism of action of its active metabolites may involve cross-linking of DNA, which may interfere with growth of normal and neoplastic cells.
View full drug information
Methotrexate (Rheumatrex, Trexall)
Methotrexate is an antimetabolite that inhibits dihydrofolate reductase, which is necessary for conversion of folate to biologically active tetrahydrofolate.
View full drug information
Doxorubicin (Adriamycin)
An anthracycline that functions as a DNA intercalator, doxorubicin inhibits topoisomerase II and produces free radicals, which may destroy DNA. The combination of these 2 events can inhibit the growth of neoplastic cells.
View full drug information
Brentuximab vedotin (Adcetris)
CD30-directed antibody-drug conjugate (ADC) consisting of chimeric IgG1 antibody cAC10, specific for human CD30 and the microtubule disrupting agent, monomethyl auristatin E

(MMAE, or vedotin). Indicated for treatment of Hodgkin lymphoma (HL) after failure of autologous stem cell transplant (ASCT) or after failure of at least 2 prior multiagent chemotherapy regimens in patients who are not ASCT candidates.
Non-Hodgkin Lymphoma http://emedicine.medscape.com/article/203399-overview
Practice Essentials
Non-Hodgkin lymphomas (NHLs) are tumors originating from lymphoid tissues, mainly of lymph nodes. These tumors may result from chromosomal translocations, infections, environmental factors, immunodeficiency states, and chronic inflammation.
Essential update: Tumor-absorbed dose predicts PFS in NHL patients undergoing radioimmunotherapy
In a study of 39 patients with 130 tumors (tumor dose, 94-711 cGy; mean, 295 cGy), the findings from which were reported at the 2013 annual meeting of the Society of Nuclear Medicine and Molecular Imaging, tumor-absorbed dose predicted progression-free survival (PFS) in patients undergoing I-131 radioimmunotherapy for non-Hodgkin lymphoma.[1]
Besides PFS, study endpoints included tumor shrinkage at 2 months and overall response at 6 months.
The researchers used computed tomography (CT)/single-photon emission CT (SPECT) imaging and Monte Carlo simulation of radiation transport to estimate 3-dimensional dosimetric parameters and calculated the equivalent biologic effect to determine the biologic influences of the nonuniform absorbed dose and the cold antibody, proliferation, and radiosensitivity.[1] They used biopsy samples, baseline tumor burden, and treatment history to determine nondosimetric parameters.
Logistic regression revealed that dosimetric parameters and equivalent biologic effect had correlations with overall response and PFS (P < .05), whereas the only nondosimetric parameter that correlated with overall response and progression-free survival was tumor burden (P = .0146).[1] Each 50-cGy increase in tumor-absorbed dose led to a 25% reduction in risk for progression; the optimal dose for differentiating PFS was 200 cGy.
Signs and symptoms
The clinical manifestations of NHL vary with such factors as the location of the lymphomatous process, the rate of tumor growth, and the function of the organ being compromised or displaced by the malignant process.
Signs and symptoms of low-grade lymphomas include the following:
Peripheral adenopathy: Painless and slowly progressive; can spontaneously regress Primary extranodal involvement and B symptoms: Uncommon at presentation; however,
common with advanced, malignant transformation or end-stage disease

Bone marrow: Frequent involvement; may be associated with cytopenias(s)[2] ; fatigue/weakness more common in advanced-stage disease
Intermediate- and high-grade lymphomas have a more varied clinical presentation, including the following:
Adenopathy: Most patients Extranodal involvement: More than one third of patients; most common sites are GI/GU
tracts (including Waldeyer ring), skin, bone marrow, sinuses, thyroid, CNS B symptoms: Temperature >38°C, night sweats, weight loss >10% from baseline within 6
months; in approximately 30-40% of patients
See Clinical Presentation for more detail.
Diagnosis
Examination in patients with low-grade lymphomas may demonstrate peripheral adenopathy, splenomegaly, and hepatomegaly.
Intermediate- and high-grade lymphomas may result in the following examination findings:
Rapidly growing and bulky lymphadenopathy Splenomegaly Hepatomegaly Large abdominal mass: Usually in Burkitt lymphoma Testicular mass Skin lesions: Associated with cutaneous T-cell lymphoma (mycosis fungoides), anaplastic
large-cell lymphoma, and angioimmunoblastic lymphoma[3]
Testing
Laboratory studies in a patient with suspected NHL should include the following:
CBC count: May be normal in early-stage disease; in more advanced stages, may demonstrate anemia, thrombocytopenia/leukopenia/pancytopenia, lymphocytosis, thrombocytosis
Serum chemistry studies: May show elevated LDH and calcium levels, abnormal liver function tests
Serum beta2-microglobulin level: May be elevated HIV serology: Especially in patients with diffuse large cell immunoblastic or small noncleaved
histologies Human T-cell lymphotropic virus-1 serology: For patients with adult T-cell
leukemia/lymphoma Hepatitis B testing: In patients in whom rituximab therapy is planned because reactivation
has been reported
Other tests that may be helpful in evaluating suspected NHL include the following:
Immunophenotypic analysis of lymph node, bone marrow, peripheral blood Cytogenetic studies: NHL occasionally associated with monoclonal gammopathy; possible
positive Coombs test; maybe hypogammaglobulinemia

Imaging tests
The following imaging studies should be obtained in a patient suspected of having NHL:
Chest radiography Upper GI series with small bowel follow-through: In patients with head and neck
involvement and those with a GI primary lesion CT scanning of the neck, chest, abdomen, and pelvis PET scanning Bone scanning: Only in patients with bone pain, elevated alkaline phosphatase, or both Testicular ultrasonography: For opposite testis in male patients with a testicular primary
lesion Multiple gated acquisition (MUGA) scanning: For patients being considered for treatment
with anthracyclines MRI of brain/spinal cord: For suspected primary CNS lymphoma, lymphomatous meningitis,
paraspinal lymphoma, or vertebral body involvement by lymphoma
Procedures
The diagnosis of NHL relies on pathologic confirmation following appropriate tissue biopsy. The following are procedures in cases of suspected NHL:
Bone marrow aspiration and biopsy: For staging rather than diagnostic purposes Excisional lymph node biopsy (extranodal biopsy): For lymphoma protocol studies
Perform lumbar puncture for CSF analysis in patients with the following conditions:
Diffuse aggressive NHL with bone marrow, epidural, testicular, paranasal sinus, or nasopharyngeal involvement, or 2 or more extranodal sites of disease
High-grade lymphoblastic lymphoma High-grade small noncleaved cell lymphomas HIV-related lymphoma Primary CNS lymphoma Neurologic signs and symptoms
See Workup for more detail.
Management
The treatment of NHL varies greatly, depending on various factors. Common therapies include the following:
Chemotherapy: Most common; usually combination regimens
Radiation therapy Rituximab administration Bone marrow transplantation: Possible role in relapsed high-risk disease Radioimmunotherapy Transfusions of blood products Antibiotics

Pharmacotherapy
Medications used in the management of NHL include the following:
Cytotoxic agents (eg, chlorambucil, cyclophosphamide, doxorubicin, vincristine, fludarabine, pralatrexate, nelarabine, etoposide, mitoxantrone, cytarabine, bendamustine, carboplatin, cisplatin, gemcitabine, denileukin diftitox, bleomycin)
Histone deacetylase inhibitors (eg, vorinostat, romidepsin) Colony-stimulating factor growth factors (eg, epoetin alfa, darbepoetin alfa, filgrastim,
pegfilgrastim) Monoclonal antibodies (eg, rituximab, ibritumomab tiuxetan, tositumomab and I131,
alemtuzumab, ofatumumab) mTOR (mammalian target of rapamycin) kinase inhibitors (eg, temsirolimus) Proteasome inhibitors (eg, bortezomib) Immunomodulators (eg, interferon alfa-2a or alfa-2b) Corticosteroids (eg, dexamethasone, prednisone)
Surgery
Surgical intervention in NHL is limited but can be useful in selected situations (eg, GI lymphoma), particularly in localized disease or in the presence of risk of perforation, obstruction, and massive bleeding. Orchiectomy is part of the initial management of testicular lymphoma.
Posteroanterior (PA) chest radiograph in a man with thoracic non-Hodgkin lymphoma (NHL) shows mediastinal widening due to grossly enlarged right paratracheal and left paratracheal nodes.

Posteroanterior (PA) chest radiograph in a 16-year-old male adolescent with thoracic non-Hodgkin lymphoma (NHL) shows subtle enlargement of the lower paratracheal lymph nodes.
Nonenhanced CT scan through the mediastinum shows multiple enlarged lymph nodes in the prevascular space, in the right and left paratracheal region. Nodes in the left paratracheal region

cause the trachea to be indented and narrowed on the left side. Note the small, bilateral pleural effusion
Nonenhanced CT scan through the mediastinum at the level of the carina shows enlarged tracheobronchial and subcarinal nodes. Note the small bilateral pleural effusion.

Contrast-enhanced axial CT scan in a child shows hypoattenuating, enlarged, subcarinal lymph nodes with splaying of the tracheal bifurcation.
Posteroanterior (PA) chest radiograph shows a large mass in the right parahilar region extending into the right upper and middle zones, with silhouetting of the right pulmonary artery. Smaller mass is

seen in the periphery of the right lower zone. The masses did not respond to a trial of antibiotics. Core-needle biopsy of the larger lesion revealed NHL deposits in the lung.
Lateral image shows a large mass in the anterior aspect of the right upper lobe of the lung.

Posterior bone scan shows no abnormally increased uptake in the thoracic vertebrae. Image shows an unusual pattern of non-Hodgkin lymphoma (NHL) of the upper thoracic vertebra.

This 28-year-old man was being evaluated for fever of unknown origin. Gallium-67 study shows extensive uptake in the mediastinal lymph nodes due to non-Hodgkin lymphoma (NHL).

T1-weighted coronal MRIs of the thorax in a 55-year-old woman with lower dorsal pain. Note the signal-intensity changes in the body of D12; these are associated with a right-sided, large, paravertebral soft-tissue mass involving the psoas muscle. Biopsy confirmed non-Hodgkin lymphoma (NHL).

T1-weighted coronal MRIs of the thorax in a 55-year-old woman with lower dorsal pain (same patient as in the previous image). Note the signal-intensity changes in the body of D12; these are associated with a right-sided, large, paravertebral soft-tissue mass involving the psoas muscle. Biopsy confirmed non-Hodgkin lymphoma (NHL).

Positron emission tomography (PET) CT in an 80-year-old woman with diffuse, large B-cell NHL of the skin and subcutaneous tissues that recently transformed from prior low-grade non-Hodgkin lymphoma (NHL). CT scan of the lower neck shows several subcutaneous nodules of varying size with variable uptake on PET (arrows).

Positron emission tomography (PET) CT in an 80-year-old woman with diffuse, large B-cell NHL of the skin and subcutaneous tissues that recently transformed from previous low-grade non-Hodgkin lymphoma (NHL) in the same patient as in the previous image. PET shows high level of uptake in the anterior subcutaneous nodule in the chest (white arrows). CT scan of similar nodules (arrowheads) on the anterior left chest does not show PET uptake; these may represent regions of lower-grade NHL. PET image of posterior lesions shows only mild uptake (gray arrow).
Gallium-67 (67Ga) scan shows the intrathoracic lymphoma to be 67Ga avid.
Non-Hodgkin lymphoma of the terminal ileum. Note the doughnut sign, ie, intraluminal contrast material surrounded by a grossly thickened bowel wall. This appearance is highly suggestive of small noncleaved cell lymphoma (Burkitt type).

Computed tomography of the throat in highly-malignant non-hodgkin lymphoma present as lymph node swelling in a child (transverse section with contrast). DE: Computertomographie des Halses bei einem hoch-malignen Non-Hodgkin

Malignant lymphoma high grade_B_cell

Ultrasound throat lymphadenopathy non-hodgkin-lymphoma
Background
The term lymphoma describes a heterogeneous group of malignancies with different biology and prognosis. In general, lymphomas are divided into 2 large groups of neoplasms, namely non-Hodgkin lymphoma (NHL) and Hodgkin disease. About 85% of all malignant lymphomas are NHLs. The median age at diagnosis is the sixth decade of life, although Burkitt lymphoma and lymphoblastic lymphoma occur in younger patients. NHL includes many clinicopathologic subtypes, each with distinct epidemiologies; etiologies; morphologic, immunophenotypic, genetic, and clinical features; and responses to therapy.
Currently, several NHL classification schemas exist, reflecting the growing understanding of the complex diversity of the NHL subtypes. The Working Formulation, originally proposed in 1982, classified and grouped lymphomas by morphology and clinical behavior (ie, low, intermediate, or high grade). In the 1990s, the Revised European-American Lymphoma (REAL) classification attempted to apply immunophenotypic and genetic features in identifying distinct clinicopathologic NHL entities. The World Health Organization (WHO) classification further elaborates upon the REAL approach. This classification divides NHL into those of B-cell origin and those of T-cell and natural killer (NK)–cell origin.
A study by Shustik et al found that within the WHO classification, the subdivisions of grade 3A and 3B had no difference in outcome or curability with anthracycline-based therapy.[4]
For clinical oncologists, the most practical way of sorting the currently recognized types of NHL is according to their predicted clinical behavior. Each classification schema contributes to a greater understanding of the disease, which dictates prognosis and treatment.
Although a variety of laboratory and imaging studies are used in the evaluation and staging of suspected NHL (see Workup), a well-processed hematoxylin and eosin (H&E)–stained section of an excised lymph node is the mainstay of pathologic diagnosis. The treatment of non-Hodgkin lymphoma (NHL) varies greatly, depending on tumor stage, grade, and type and various patient factors (eg, symptoms, age, performance status; see Treatment and Management).
For discussion of individual subtypes of NHL, see the following:
Anaplastic Large Cell Lymphoma Follicular Lymphoma B Cell Lymphoma Diffuse Large Cell Lymphoma Diffuse Mixed Lymphoma Lymphoblastic Lymphoma Mantle Cell Lymphoma Mycosis Fungoides Primary CNS Lymphoma Cutaneous T-Cell Lymphoma
Pathophysiology

NHLs are tumors originating from lymphoid tissues, mainly of lymph nodes. Various neoplastic tumor cell lines correspond to each of the cellular components of antigen-stimulated lymphoid follicles.
NHL represents a progressive clonal expansion of B cells or T cells and/or NK cells arising from an accumulation of lesions affecting proto-oncogenes or tumor suppressor genes, resulting in cell immortalization. These oncogenes can be activated by chromosomal translocations (ie, the genetic hallmark of lymphoid malignancies), or tumor suppressor loci can be inactivated by chromosomal deletion or mutation. In addition, the genome of certain lymphoma subtypes can be altered with the introduction of exogenous genes by various oncogenic viruses. Several cytogenetic lesions are associated with specific NHLs, reflecting the presence of specific markers of diagnostic significance in subclassifying various NHL subtypes.
Almost 85% of NHLs are of B-cell origin; only 15% are derived from T/NK cells, and the small remainder stem from macrophages. These tumors are characterized by the level of differentiation, the size of the cell of origin, the origin cell's rate of proliferation, and the histologic pattern of growth.
For many of the B-cell NHL subtypes, the pattern of growth and cell size may be important determinants of tumor aggressiveness. Tumors that grow in a nodular pattern, which vaguely recapitulate normal B-cell lymphoid follicular structures, are generally less aggressive than lymphomas that proliferate in a diffuse pattern. Lymphomas of small lymphocytes generally have a more indolent course than those of large lymphocytes, which may have intermediate-grade or high-grade aggressiveness. However, some subtypes of high-grade lymphomas are characterized by small cell morphology.
Etiology
NHLs may result from chromosomal translocations, infections, environmental factors, immunodeficiency states, and chronic inflammation.
Chromosomal translocations
Chromosomal translocations and molecular rearrangements play an important role in the pathogenesis of many lymphomas and correlate with histology and immunophenotype.
The t(14;18)(q32;q21) translocation is the most common chromosomal abnormality associated with NHL. This translocation occurs in 85% of follicular lymphomas and 28% of higher-grade NHLs. This translocation results in the juxtaposition of the bcl -2 apoptotic inhibitor oncogene at chromosome band 18q21 to the heavy chain region of the immunoglobulin (Ig) locus within chromosome band 14q32.
The t(11;14)(q13;q32 translocation has a diagnostic nonrandom association with mantle cell lymphoma. This translocation results in the overexpression of bcl -1 (cyclin D1/PRAD 1), a cell-cycle regulator on chromosome band 11q13.

The 8q24 translocations lead to c-myc dysregulation. This is frequently observed in high-grade small noncleaved lymphomas (Burkitt and non-Burkitt types), including those associated with HIV infection.
The t(2;5)(p23;q35) translocation occurs between the nucleophosmin (NPM) gene and the anaplastic lymphoma kinase (ALK1) gene. It results in the expression of an aberrant fusion protein found in a majority of anaplastic large cell lymphomas.
Two chromosomal translocations, t(11;18)(q21;q21) and t(1;14)(p22;132), are associated with mucosa-associated lymphoid tissue (MALT) lymphomas. The more common (ie, t[11;18][q21;q21]) translocates the apoptosis inhibitor AP12 gene with the MALT1 gene, resulting in the expression of an aberrant fusion protein. The other translocation, t(1;14)(p22;132), involves the translocation of the bcl -10 gene to the immunoglobulin gene enhancer region.
Infection
Some viruses are implicated in the pathogenesis of NHL, probably because of their ability to induce chronic antigenic stimulation and cytokine dysregulation, which leads to uncontrolled B- or T-cell stimulation, proliferation, and lymphomagenesis. Epstein-Barr virus (EBV) is a DNA virus that is associated with Burkitt lymphoma (especially the endemic form in Africa), Hodgkin disease, lymphomas in immunocompromised patients (eg, from HIV infection,[5]
organ transplantation), and sinonasal lymphoma.
Human T-cell leukemia virus type 1 (HTLV-1) causes a latent infection via reverse transcription in activated T-helper cells. This virus is endemic in certain areas of Japan and the Caribbean islands, and approximately 5% of carriers develop adult T-cell leukemia or lymphoma.
Hepatitis C virus (HCV) is associated with the development of clonal B-cell expansions and certain subtypes of NHL (ie, lymphoplasmacytic lymphoma, Waldenström macroglobulinemia), especially in the setting of essential (type II) mixed cryoglobulinemia.
Kaposi sarcoma–associated herpesvirus (KSHV) is associated with body cavity–based lymphomas in patients with HIV infection and in patients with multicentric Castleman disease.
Helicobacter pylori infection is associated with the development of primary gastrointestinal (GI) lymphomas, particularly gastric mucosa-associated lymphoid tissue (MALT) lymphomas.
Environmental factors
Environmental factors linked to the development of NHL include chemicals (eg, pesticides, herbicides, solvents, organic chemicals, wood preservatives, dusts, hair dye), chemotherapy, and radiation exposure.

Immunodeficiency states
Congenital immunodeficiency states (eg, severe combined immunodeficiency disease [SCID], Wiskott-Aldrich syndrome), acquired immunodeficiency states (eg, AIDS), and induced immunodeficiency states (eg, immunosuppression) are associated with increased incidence of NHL and are characterized by a relatively high incidence of extranodal involvement, particularly of the GI tract, and with aggressive histology. Primary CNS lymphomas can be observed in about 6% of patients with AIDS.
Celiac disease has been associated with an increased risk of malignant lymphomas. The risk of lymphoproliferative malignancy in individuals with celiac disease depends on small intestinal histopathology; no increased risk is observed in those with latent celiac disease.[6]
Chronic inflammation
The chronic inflammation observed in patients with autoimmune disorders, such as Sjögren syndrome and Hashimoto thyroiditis, promotes the development of MALT and predisposes patients to subsequent lymphoid malignancies. Hashimoto thyroiditis is a preexisting condition in 23-56% of patients with primary thyroid lymphomas.
Epidemiology
The American Cancer Society estimated that approximately 65,540 new cases of NHL would be diagnosed in 2010.[7] Since the early 1970s, the incidence rates of NHL have nearly doubled. Although some of this increase may be attributable to earlier detection (resulting from improved diagnostic techniques and access to medical care), or possibly to HIV-associated lymphomas, for the most part the rise is unexplained.
NHL is the most prevalent hematopoietic neoplasm, representing approximately 4% of all cancer diagnoses and ranking seventh in frequency among all cancers. NHL is more than 5 times as common as Hodgkin disease.
Incidence varies with race; white people have a higher risk than black and Asian American people. In general, the incidence of NHL is slightly higher in men than in women, with a male-to-female ratio of approximately 1.4:1. The ratio may vary depending on the subtype of NHL, however; for example, primary mediastinal diffuse large B-cell lymphoma occurs more frequently in females than in males.
The median age at presentation for most subtypes of NHL is older than 50 years. The exceptions are high-grade lymphoblastic and small noncleaved lymphomas, which are the most common types of NHL observed in children and young adults. At diagnosis, low-grade lymphomas account for 37% of NHLs in patients aged 35-64 years but account for only 16% of cases in patients younger than 35 years. Low-grade lymphomas are extremely rare in children.
Prognosis
The 5-year relative survival rate of patients with NHL is approximately 63%. The survival rate has steadily improved over the last 2 decades, thanks to improvements in medical and

nursing care, the advent of novel therapeutic strategies (ie, monoclonal antibodies), validation of biomarkers of response, and the implementation of tailored treatment.
The prognosis for patients with NHL depends on the following factors:
Tumor histology (based on Working Formulation classification) Tumor stage Patient age Tumor bulk Performance status Serum lactate dehydrogenase (LDH) level Beta2-microglobulin level Presence or absence of extranodal disease
In general, these clinical characteristics are thought to reflect the following host or tumor characteristics:
Tumor growth and invasive potential (eg, LDH, stage, tumor size, beta2-microglobulin level, number of nodal and extranodal sites, bone marrow involvement)
Patient's response to tumor (eg, performance status, B symptoms) Patient's tolerance of intensive therapy (eg, performance status, patient age, bone
marrow involvement)
The International Prognostic Index (IPI), which was originally designed as a prognostic factor model for aggressive NHL, also appears to be useful for predicting the outcome of patients with low-grade lymphoma and mantle cell lymphoma. This index is also used to identify patients at high risk of relapse, based on specific sites of involvement, including bone marrow, CNS, liver, testis, lung, and spleen. These patients may be considered for clinical trials that aim at improving the current treatment standard.
An age-adjusted model for patients younger than 60 years has been proposed. In younger patients, stage III or IV disease, high LDH levels, and nonambulatory performance status are independently associated with decreased survival rates.
Pediatric and adolescent patients have better outcome than adults with CNS lymphoma.[8] An ECOG performance status score of 0-1 is associated with improved survival. Higher dose methotrexate is associated with slightly better response.
Clinical features included in the IPI that are independently predictive of survival include the following:
Age - Younger than 60 years versus older than 60 years LDH level - Within the reference range versus elevated Performance status -Eastern Cooperative Oncology Group (ECOG) grade 0-1 versus
2-4 Ann Arbor stage - Stage I-II versus III-IV Number of extranodal sites - Zero to 1 versus more than 1
With this model, relapse-free and overall survival rates at 5 years are as follows:

0-1 risk factors - 75% 2-3 risk factors - 50% 4-5 risk factors - 25%
For patients with follicular lymphoma—the second most common subtype of NHL—the Follicular Lymphoma International Prognostic Index (FLIPI) score appears to be more discriminating than the IPI.[9] The FLIPI score is calculated on the basis of 5 adverse prognostic factors, as follows:
Age (>60 y) Ann Arbor stage (III-IV) Hemoglobin level (< 12 g/dL) Number of nodal areas (>4) Serum LDH level (above normal)
Three risk groups are defined: low risk (0-1 adverse factor), intermediate risk (2 factors), and poor risk (3 or more adverse factors).
A study by Antonopoulos et al found that maternal smoking during pregnancy may have a modest increase in the risk for childhood NHL but not HL.[10]
Biomarkers in tumor cells such as the expression of bcl- 2 or bcl- 6 proteins and cDNA microarray provide useful prognostic information.
Patients with congenital or acquired immunodeficiency have an increased risk of lymphoma and respond poorly to therapy.
Time to achieve complete remission (CR) and response duration has prognostic significance. Patients who do not achieve CR by the third cycle of chemotherapy have a worse prognosis than those who achieve rapid CR.
Immunophenotype is also a factor. Patients with aggressive T- or NK-cell lymphomas generally have worse prognoses than those with B-cell lymphomas, except the Ki-1 anaplastic large T- or null-cell lymphomas.
Cytogenetic abnormalities and oncogene expression affect prognosis. Patients with lymphomas with 1, 7, and 17 chromosomal abnormalities have worse prognoses than those with lymphomas without these changes.
Low-grade lymphomas have indolent clinical behavior and are associated with a comparatively prolonged survival (median survival is 6-10 y), but they have little potential for cure when the disease manifests in more advanced stages. They also have the tendency to transform to high-grade lymphomas.
Approximately 70% of all patients with intermediate- and high-grade NHL relapse or never respond to initial therapy. Most recurrences are within the first 2 years after therapy completion. Patients with relapsed or resistant NHL have a very poor prognosis (< 5-10% are alive at 2 years with conventional salvage chemotherapy regimens).

Drake et al found that low levels of vitamin D were associated with a decrease in clinical end points (event-free survival and overall survival) in subsets of patients with aggressive B-cell lymphoma (ie, diffuse large B-cell lymphoma or T-cell lymphoma).[11] Although the results of this study suggest an association between vitamin D levels and its metabolism with the biology of some aggressive lymphomas, further studies are needed before conclusions can be drawn.
A study by Change et al also found a protective effect associated with vitamin D and also concluded that routine residential UV radiation exposure may have a protective effect against lymphomagenesis through mechanisms possibly independent of vitamin D.[12]
Patient Education
Patients should receive a clear and detailed explanation of all the available treatment options, prognosis, and adverse effects of chemotherapy. Advise patients to call their oncologists as necessary and educate patients about oncologic emergencies that require an immediate emergency department visit. Suggest psychosocial counseling.
For patient education information, see the Blood and Lymphatic System Center, as well as Lymphoma.
History
The clinical manifestations of non-Hodgkin lymphoma (NHL) vary with such factors as the location of the lymphomatous process, the rate of tumor growth, and the function of the organ being compromised or displaced by the malignant process.
The Working Formulation classification groups the subtypes of NHL by clinical behavior—that is, low-grade, intermediate-grade, and high-grade. Because the Working Formulation is limited to classification based upon morphology, it cannot encompass the complex spectrum of NHL disease, excluding important subtypes such as mantle cell lymphoma or T cell/natural killer cell lymphomas. However, it continues to serve as a basis for understanding the clinical behavior of groups of NHLs.
Low-grade lymphomas
Peripheral adenopathy that is painless and slowly progressive is the most common clinical presentation in these patients. Spontaneous regression of enlarged lymph nodes can occur in low-grade lymphoma, potentially causing confusion with an infectious condition.
Primary extranodal involvement and B symptoms (ie, temperature >38°C, night sweats, weight loss >10% from baseline within 6 mo) are not common at presentation, but they are common in patients with advanced, malignant transformation (ie, evolution from a low-grade to an intermediate- or high-grade lymphoma) or end-stage disease.
Bone marrow is frequently involved and may be associated with cytopenia or cytopenias.[2]
Fatigue and weakness are more common in patients with advanced-stage disease.

Intermediate- and high-grade lymphomas
These types of lymphomas cause a more varied clinical presentation. Most patients present with adenopathy. More than one third of patients present with extranodal involvement; the most common sites are the gastrointestinal (GI) tract (including the Waldeyer ring), skin, bone marrow, sinuses, genitourinary (GU) tract, thyroid, and central nervous system (CNS). B-symptoms are more common, occurring in approximately 30-40% of patients.
Lymphoblastic lymphoma, a high-grade lymphoma, often manifests with an anterior superior mediastinal mass, superior vena cava (SVC) syndrome, and leptomeningeal disease with cranial nerve palsies.
Patients with Burkitt lymphoma (occurring in the United States) often present with a large abdominal mass and symptoms of bowel obstruction. Obstructive hydronephrosis secondary to bulky retroperitoneal lymphadenopathy obstructing the ureters can also be observed in these patients.
Primary CNS lymphomas are high-grade neoplasms of B-cell origin. Most lymphomas originating in the CNS are large cell lymphomas or immunoblastomas, and they account for 1% of all intracranial neoplasms. These lymphomas are more commonly observed in patients who are immunodeficient because of conditions such as Wiskott-Aldrich syndrome, transplantation, or AIDS (see HIV-Associated Opportunistic Neoplasms-CNS Lymphoma for more information on this topic).[5]
Fernberg et al examined time trends in risk and risk determinants in posttransplant patients with lymphoma and found that posttransplant NHL risk decreased during the 2000s compared with the 1990s among patients who underwent nonkidney transplants.[13]
Physical Examination
Low-grade lymphomas may produce peripheral adenopathy, splenomegaly, and hepatomegaly. Splenomegaly is observed in approximately 40% of patients; the spleen is rarely the only involved site at presentation.
Intermediate- and high-grade lymphomas may produce the following physical examination findings:
Rapidly growing and bulky lymphadenopathy Splenomegaly Hepatomegaly Large abdominal mass : this usually occurs in Burkitt lymphoma Testicular mass Skin lesions: lesions are associated with cutaneous T-cell lymphoma (mycosis
fungoides), anaplastic large-cell lymphoma, and angioimmunoblastic lymphoma [3]
Complications
Potential disease-related complications include the following:

Cytopenias (ie, neutropenia, anemia, thrombocytopenia) secondary to bone marrow infiltration; alternatively, autoimmune hemolytic anemia is observed in some types of NHL (eg, small lymphocytic lymphoma /chronic lymphocytic leukemia [SLL/CLL])
Bleeding secondary to thrombocytopenia, disseminated intravascular coagulation (DIC), or vascular invasion by the tumor
Infection secondary to leukopenia, especially neutropenia Cardiac problems secondary to large pericardial effusion or arrhythmias secondary to
cardiac metastases Respiratory problems secondary to pleural effusion and/or parenchymal lesions Superior vena cava (SVC) syndrome secondary to a large mediastinal tumor Spinal cord compression secondary to vertebral metastases Neurologic problems secondary to primary CNS lymphoma or lymphomatous
meningitis GI obstruction, perforation, and bleeding in a patient with GI lymphoma (may also be
caused by chemotherapy) Pain secondary to tumor invasion Leukocytosis (lymphocytosis) in leukemic phase of disease
Diagnostic Considerations
A significant number of medical disorders can produce local or generalized lymph node enlargement. Thus, the diagnosis of NHL relies on pathological confirmation following appropriate tissue biopsy.
The following are some of the conditions that can result in clinical manifestations similar to those observed in lymphoma patients:
Solid tumor malignancies: metastatic disease to lymph nodes secondary to carcinoma, melanoma, or sarcoma
Other hematologic malignancies or lymphoproliferative disorders: granulocytic sarcoma, multicentric Castleman disease
Benign lymph node infiltration or reactive follicular hyperplasia secondary to infection (eg, tuberculosis; other bacterial, fungal, and, rarely, viral infections), and collagen-vascular diseases
Hodgkin lymphoma, which requires a different treatment strategy than NHL
If the diagnosis of NHL is doubtful, acquire a second or third opinion from an expert hematopathologist before instituting therapy. Flow cytometry and cytogenetics should also be performed and can be especially helpful in difficult situations.
Differential Diagnoses
Hodgkin Disease Infectious Mononucleosis
Approach Considerations

The workup in a patient with suspected non-Hodgkin lymphoma (NHL) should include the following:
Complete blood cell (CBC) count Serum chemistry studies, including lactate dehydrogenase (LDH) Serum beta2-microglobulin level HIV serology Chest radiography Computed tomography (CT) scan of the neck, chest, abdomen, and pelvis Positron emission tomography (PET) scan Excisional lymph node biopsy Bone marrow aspirate and biopsy Hepatitis B testing in patients in whom rituximab therapy is planned because
reactivation has been reported
Other studies may be indicated, depending on the clinical presentation.
CBC Count
In the early stage of disease, patients with NHL may have blood counts within the reference range. As the disease progresses, a CBC count with differential and platelet count in patients with NHL may show the following:
Anemia secondary to bone marrow infiltration, autoimmune hemolysis (particularly associated with small lymphocytic lymphoma [SLL]/chronic lymphocytic leukemia [CLL]), bleeding, anemia of chronic disease
Thrombocytopenia, leukopenia, or pancytopenia secondary to bone marrow infiltration or autoimmune cytopenias
Lymphocytosis with circulating malignant cells (common in patients with low-grade lymphomas)
Thrombocytosis (paraneoplastic syndrome associated with lymphomas or reactive secondary to blood loss)
Serum Chemistry Studies
Serum chemistry studies may show the following:
Elevated lactate dehydrogenase (LDH): indicates poor prognosis; correlates with increased tumor burden
Abnormal liver function test (LFT) results: secondary to hepatic involvement, hypermetabolic tumor growth, chronic inflammation
Hypercalcemia: in patients with acute form of adult T-cell lymphoma-leukemia (ATLL)
Other Laboratory Studies
An elevated beta2-microglobulin level may be seen. Elevated levels correlate with a poor prognosis.

Occasionally, NHL is associated with monoclonal gammopathy. A Coombs test may be positive result (especially in SLL/CLL). Hypogammaglobulinemia may be present.
HIV serology should be obtained, especially in patients with diffuse large cell immunoblastic or small noncleaved histologies. HTLV-1 serology should be obtained in patients with ATLL.
In a February 2013 study, researchers measured serum levels of the chemokine CXCL13 in 179 men diagnosed with HIV-associated non-Hodgkin B-cell lymphoma (AIDS-NHL) and 179 male controls to determine whether levels are elevated before an AIDS-NHL diagnosis. Results showed that CXCL13 levels were elevated for more than 3 years, 1 to 3 years, and 0 to 1 year before diagnosis, suggesting CXCL13 may serve as a biomarker for early AIDS-NHL detection.[14]
Radiography
A chest radiograph yields positive information in approximately one fourth of patients with NHLs. It may identify hilar or mediastinal adenopathy, pleural or pericardial effusions, and parenchymal involvement. The chest radiograph may demonstrate a bulky mediastinal mass, which is associated with primary mediastinal large B-cell lymphoma or lymphoblastic lymphoma.
Obtain an upper GI series with small bowel follow-through in patients with head and neck involvement (eg, tonsil, base of tongue, nasopharynx, Waldeyer ring) and those with a GI primary lesion.
CT, Bone Scan, and Gallium Scan
A CT scan of the neck, chest, abdomen, and pelvis is used to detect enlarged lymph nodes, hepatosplenomegaly, or filling defects in the liver and spleen. Currently, it is the most widely used test for initial staging, assessing treatment response, and conducting follow-up care.[15]
A bone scan is ordered only in patients with bone pain, elevated alkaline phosphatase, or both. Bone lesions are particularly associated with the acute form of ATLL and diffuse large B-cell lymphomas.
Gallium scans are an option in selected cases of NHL. These scans can detect initial sites of disease, reflect therapy response, and detect early recurrences. This scan is positive in nearly all patients with aggressive and highly aggressive lymphomas and in approximately 50% of patients with indolent lymphomas at diagnosis.
Positron Emission Tomography and Ultrasonography
Whole body F-18 2-deoxyglucose (FDG) positron emission tomography (PET) scan can be used for the initial evaluation of patients with NHL; however, this scan is more useful for posttreatment evaluation to differentiate early recurrences or residual disease from fibrosis or necrosis. This PET scan has a higher predictive value for relapse than classic CT scan imaging.[16] A study by Zinzani et al determined that midtreatment scanning using PET allowed physicians to better make crucial decisions on further treatment.[17]

A study by Terezakis found that incorporating FDG-PET into CT-based treatment planning in patients with lymphoma resulted in beneficial changes in management, volume definition, and normal tissue dosimetry for a significant amount of patients.[18]
In a study of 130 patients with diffuse large B-cell lymphoma, Khan et al found PET-CT scanning to be highly accurate in identifying marrow disease.[19] PET-CT scanning identified 33 of 35 patients found to have marrow involvement, compared with 14 cases identified by marrow histology. The investigators found that PET scanning had a sensitivity of 94% and a specificity of 100%, whereas iliac crest biopsy had a sensitivity of 40% and a specificity of 100%.
Obtain an ultrasound image of the opposite testis in male patients with a testicular primary lesion.
Multiple Gated Acquisition Scanning
A multiple gated acquisition (MUGA) scan should be performed to measure the left ventricular ejection fraction (LVEF) of patients who are being considered for treatment with anthracyclines.
In general, anthracyclines should not be administered to those patients with LVEF of less than 50%.
Magnetic Resonance Imaging
Obtain an MRI of the brain and spinal cord of patients who are suspected of having primary CNS lymphoma, lymphomatous meningitis, paraspinal lymphoma, or vertebral body involvement by lymphoma. An MRI scan can also be performed to identify focal areas of marrow involvement in those patients suspected to have bone marrow involvement but in whom random bone marrow biopsy findings have been negative.
Biopsy
A well-processed hematoxylin and eosin (H&E)–stained section of an excised lymph node is the mainstay of pathologic diagnosis. Excisional lymph node biopsy is required because lymphoma diagnosis relies heavily on careful assessment of altered nodal architecture accompanying lymphomatous infiltrates. Fine-needle aspiration (FNA) is insufficient for establishing a diagnosis; needle-core biopsies have a limited role in establishing a diagnosis of NHL.
Bone marrow aspirate and biopsy
Perform this procedure for staging rather than diagnostic purposes. Bilateral bone marrow aspirate and biopsy should be performed because bone marrow involvement is usually patchy. In bone marrow sections, the neoplastic cells may infiltrate in a focal (ie, paratrabecular or nonparatrabecular, depending on the type of lymphoma), interstitial, or diffuse pattern.

Biopsy of extranodal sites
In approximately 30-35% of adult patients with NHL, the extranodal sites are the primary presenting sites. The most common site is the GI tract.
Processing extranodal biopsy material for lymphoma protocol studies is important whenever suspicion of a hematolymphoid neoplasm exists.
Lumbar Puncture
Lumbar puncture for cerebrospinal fluid (CSF) examination should be performed in patients with the following conditions:
Diffuse aggressive NHL with bone marrow, epidural, testicular, paranasal sinus, or nasopharyngeal involvement, or two or more extranodal sites of disease
High-grade lymphoblastic lymphoma High-grade small noncleaved cell lymphomas (eg, Burkitt and non-Burkitt types) HIV-related lymphoma Primary CNS lymphoma Neurologic signs and symptoms
Histologic Findings
NHLs are a heterogeneous group of lymphoproliferative malignancies, with varying morphologic features depending on the specific subtype. The abnormal lymphocytes in the lymph node, bone marrow, or extranodal sites can be small cleaved or noncleaved, intermediate, or large cell and can have a follicular or diffuse pattern. In contrast with reactive follicular hyperplasia, lymphomas usually alter the lymph node architecture, and the capsule is usually involved.
Immunophenotypic Analysis
Immunophenotypic analysis of lymph node, bone marrow, peripheral blood (if positive for neoplastic cells), or a combination of these complements and confirms the results of routine tissue section and may be useful in resolving a diagnostic dilemma in patients with an atypical morphology.
This analysis provides information about lineage and clonality, which are complementary to the histology of a given case. Analysis is also useful for subclassifying certain lymphoma subtypes, which has therapeutic and prognostic importance.
Immunophenotypic analysis helps to distinguish reactive from neoplastic lymphoid infiltrates, lymphoid from nonlymphoid malignancies, and specific lymphoid neoplasms. Although bcl -2 expression distinguishes follicular lymphoma from reactive follicular hyperplasia, bcl -1 expression strongly favors a diagnosis of mantle cell lymphoma. CD30 expression is important for the recognition of anaplastic large cell lymphoma, and it can also be found in the majority of Hodgkin lymphomas.

Cytogenetic Studies
These studies have contributed to the understanding of the biology and prognosis of lymphoma. Cytogenetic studies are critical to the discovery of oncogene abnormalities that now are known to be intimately involved in the pathogenesis of NHL.
Staging
Staging is important in selecting a treatment and determining prognosis. CT scans of the neck, chest, abdomen, and pelvis, as well as bilateral bone marrow aspirate and biopsy, are necessary to stage the lymphoma. Noncontiguous lymph node involvement, uncommon in Hodgkin disease, is more common among patients with NHL.
The Ann Arbor staging system is the most commonly used staging system for patients with NHL. This system divides NHL into 4 stages, as follows:
Stage I NHL involves a single lymph node region (I) or localized involvement of a single extralymphatic organ or site (IE)
Stage II NHL involves 2 or more lymph node regions on the same side of the diaphragm (II) or localized involvement of a single associated extralymphatic organ in addition to criteria for stage II (IIE)
Stage III involves lymph node regions on both sides of the diaphragm (III) that also may be accompanied by localized involvement of an extralymphatic organ or site (IIIE), spleen (IIIS), or both (IIISE)
Stage IV represents disseminated or multifocal involvement of one or more extralymphatic sites with or without associated lymph node involvement or isolated extralymphatic organ involvement with distant (nonregional) nodal involvement
In addition to the 4 stage designations, subscript letters designate involvement of extralymphatic organs, as follows:
L - lung H - Liver P - Pleura B - Bone M - Bone marrow D - Skin E - Extranodal lymphoid malignancies in tissues that are separate from but near the major
lymphatic aggregates
The stages can also be appended by A or B designations. Patients with A disease do not have systemic symptoms. The B designation is applied in patients with any of the following symptoms:
Unexplained loss of more than 10% of body weight in the 6 months before diagnosis Unexplained fever with temperature above 38°C Drenching night sweats

Risk stratification scoring systems
In addition to staging, risk stratification is important in patients with NHL. Prospectively validated scoring systems that can be used to determine prognosis include the International Prognostic Index (IPI) for patients with diffuse large B-cell lymphoma and the Follicular Lymphoma International Prognostic Index, (FLIPI) for patients with follicular B-cell lymphomas. The greater the number of risk factors present, the higher the risk.
The IPI for NHL is as follows:
Age older than 60 years ECOG grade greater than or equal to 2 Elevated LDH value Two or more extranodal sties Ann Arbor stage III or IV
The FLIPI score is as follows:
Number of nodal sites of 5 or more Elevated LDH value Age 60 years or older Ann Arbor stage III–IV Hemoglobin value less than 12 g/dL
Approach Considerations
The treatment of non-Hodgkin lymphoma (NHL) varies greatly, depending on the following factors:
Tumor stage Phenotype (B-cell, T-cell or natural killer (NK) cell/null-cell) Histology (ie, low-, intermediate-, or high-grade) Symptoms Performance status Patient age Comorbidities
Most of the chemotherapy for NHL, whether combination or single-drug, can be administered in an outpatient setting, at an infusion clinic. In the infusion clinic, specially trained oncology nurses, who are supervised by oncologists, administer the chemotherapy. Growth factor support (eg, GCSF, GM-CSF, erythropoietin) is also administered in an outpatient treatment setting.
Infusional chemotherapy (eg, infusional cyclophosphamide, doxorubicin, and etoposide [CDE], which should be administered continuously for 4 days) should be administered as inpatient treatment. High-dose chemotherapy and bone marrow and/or stem cell transplantation are administered in an inpatient setting of a tertiary hospital with an approved transplant center.

For the initial treatment of patients with intermediate- or high-grade lymphoma and patients with bulky disease, an inpatient setting is recommended in order to monitor for tumor lysis syndrome and to manage appropriately.
Admit patients with NHL for complications of disease progression (eg, pain control for intractable pain) or adverse effects from chemotherapy (eg, dehydration secondary to diarrhea, vomiting requiring IV hydration, severe mucositis). Patients with fever during neutropenia should be admitted for broad-spectrum antibiotic therapy.
Ensure that patients understand their diagnosis, treatment options, and prognosis and complications of therapy, which, in rare occasions, may result in a fatal event (eg, death secondary to severe infection unresponsive to antimicrobial therapy, in a patient with severe neutropenia). Start the treatment only after the patient has signed an informed consent form.
Management of Indolent NHL
Follicular lymphoma (grade I-IIIa) comprises 70% of this group. Other entities in this group include small lymphocytic lymphoma (SLL), lymphoplasmacytoid lymphoma, and marginal zone lymphomas (MZL, nodal or extranodal).
Indolent stage I and contiguous stage II NHL
Standard management consists of radiotherapy alone. Forty percent of patients with limited-stage disease remained disease-free at 10 years after radiation in a study done by Mac Manus and Hoppe.[20] No randomized study has shown combined chemotherapy and radiation to be better than radiation alone.
A study by Rossier et al found that low-dose involved-field radiotherapy is effective in treating patients with recurrent low-grade lymphoma.[21]
Radiation therapy (2500-4000 cGy) produces a 10-year failure-free survival (FFS) rate of 50-60%, with an overall survival (OS) rate of 60-80%. Offering adjuvant chemotherapy to selected patients with stage I-II NHL who have unfavorable prognostic factors (eg, B symptoms, >2 nodal sites), and to those with follicular mixed histology is not unreasonable. Early treatment in asymptomatic patients has not been shown to improve survival.
Indolent noncontiguous stage II, III, and IV NHL
The treatment of indolent B-cell lymphomas continues to evolve as new therapies with potent antitumor activity and limited toxicity are becoming available. Monoclonal antibodies are changing the treatment paradigm of patients with B-cell lymphomas. However, controversies persist regarding the best treatment strategy and the best time to initiate treatment.
The disease course of indolent lymphomas is characterized by a continuous decrease in the quality and the duration of response with each subsequent treatment or treatments. This effect is primarily due to the acquisition of chemotherapy resistance.

Advanced indolent lymphomas have been accepted to be not curable with currently available therapies. However, sustained complete remissions can be achieved with various treatment modalities.
The use of rituximab, a monoclonal antibody targeting CD20 antigen present in benign and malignant B-cells, in combination with systemic chemotherapy, has resulted in an improved duration of remission and survival for patients with indolent B-cell lymphomas when compared to chemotherapy. Prospective studies and 2 meta-analyses suggest that the rituximab-chemotherapy, also known as chemo-immunotherapy, may be changing the natural progression of indolent lymphomas.
Asymptomatic patients, especially older patients and patients with concomitant medical problems, deferred therapy with careful observation is an option. Early intervention in asymptomatic patients does not appear to prolong survival. The median time to progression is 4-6 years, and OS is 6-10 years.
The treatment of symptomatic patients with indolent lymphomas should be focused on achieving the best possible quality of response without producing excessive toxicity. Single-agent treatment with chlorambucil or cyclophosphamide (with or without prednisone) is useful in elderly patients with significant comorbidities. However, only a few achieve remission; most achieve palliation.
Combination chemotherapies are used in younger patients with the goal of achieving a complete remission. Frequently used combination regimens are CHOP (cyclophosphamide, hydroxydaunomycin [Adriamycin], vincristine [Oncovin], and prednisone), CVP (cyclophosphamide, vincristine, and prednisone), and fludarabine alone or in combination (eg, with cyclophosphamide or mitoxantrone). Combination agents are useful in bulky and rapidly progressive disease and have higher response rates than single agents, but there is no improvement in overall survival.[22, 23, 24]
As presented by Czuczman and Rummel, new treatment options for NHL are comparing traditional chemotherapy with high-dose regimens. The efficacy of bendamustine plus rituximab for the first-line treatment of advanced follicular, indolent, and mantle cell lymphomas is the most important recent development.[25, 26] In 2011, the NCCN upgraded the combination of rituximab and bendamustine to a category 1 recommendation for suggested first-line therapy of follicular lymphoma.[27] Other important results include the lack of superiority of high-dose chemotherapy plus rituximab compared with traditional chemotherapy plus rituximab for high-risk patients with aggressive B-cell lymphomas. Promising outcomes have been seen with the combination of lenalidomide plus rituximab for both rituximab-refractory and non–rituximab-refractory indolent NHL.[28]
Randomized trials have shown that adding rituximab to chemotherapy regimens results in higher response rates, longer time to progression, and longer survival than chemotherapy. For example, Czuczman et al reported a 95% overall response rate and increase in time to progression with addition of rituximab to CHOP chemotherapy.[29] Rituximab as a single agent is also useful in patients who are unable to tolerate chemotherapy or those patients who elect to undergo treatment in the absence of high tumor burden.
A study by Gaulard et al found that rituximab plus low-dose CHOP (R-miniCHOP) offered a good compromise between efficacy and safety in patients older than 80 years. The authors

concluded that R-miniCHOP should be considered the new standard of treatment in these patients.[30]
Bone marrow transplantation may have a role in patients with relapsed high-risk disease. Allogeneic transplants have lower relapse rates but higher transplant-related mortality than autologous transplants.[31] The precise role of transplantation in indolent lymphomas is still being investigated.
A study by Watanabe et al found that a denser dose R-CHOP strategy was not associated with improved progression-free survival in patients with untreated indolent B-cell lymphoma.[32]
Management of Aggressive NHL
Diffuse large B-cell lymphoma is the most common type of NHL. Other distinct entities in this group include immunoblastic, anaplastic, lymphoblastic, large-cell, Burkitt, and Burkitt-like lymphomas (high-grade lymphomas). Mantle cell lymphomas also behave aggressively.
Aggressive stage I and contiguous stage II (nonbulky or < 10 cm) NHL
Based on 2 large randomized trials (ie, Southwest Oncology Group [SWOG], Eastern Cooperative Oncology Group [ECOG]), the preferred treatment option for patients with intermediate-grade NHL is combination chemotherapy (3 cycles of CHOP) plus involved-field radiation therapy.
According to SWOG data, patients who are treated with chemotherapy and involved-field radiation therapy have significantly better progression-free survival rates (ie, 77% versus 66%) and 5-year overall survival (OS) rates (ie, 82% versus 72%) compared with patients surviving 8 cycles of chemotherapy (ie, CHOP) alone. Patients with high-grade disease should be strongly considered for treatment with more aggressive regimens beyond CHOP.
Aggressive noncontiguous stage II, III, and IV NHL
Approximately 40-50% of these patients are cured with standard therapy, approximately 35-40% will respond but ultimately progress or relapse, and the remainder will be have disease that is refractory to primary treatment. Scoring systems such the IPI score have been developed and validated to estimate the response rate or survival rate of a given patient with aggressive lymphomas.
For many years, the treatment of aggressive lymphomas consisted of chemotherapy regimens using multiple drugs. Initial clinical studies were focused on investigating the use of more toxic regimens (higher doses or more drugs).
A prospective randomized trial in patients with diffuse large-cell lymphoma showed no difference in response rate (RR), OS, or time to treatment failure (TTF) at 3 years with any of the following regimens[33] :
CHOP

Prednisone, methotrexate, leucovorin, doxorubicin, cyclophosphamide, and etoposide—cyclophosphamide, etoposide, Adriamycin, cytarabine, bleomycin, Oncovin, methotrexate, leucovorin, and prednisone (ProMACE-CytaBOM)
Methotrexate, bleomycin, doxorubicin (Adriamycin), cyclophosphamide, Oncovin, and dexamethasone (m-BACOD)
Methotrexate-leucovorin, Adriamycin, cyclophosphamide, Oncovin, prednisone, and bleomycin (MACOP-B)
Hyper-CVAD (cyclophosphamide, vincristine, doxorubicin, dexamethasone, alternating with methotrexate and cytarabine) plus rituximab has been shown to achieve a high rate of durable remission in patients with mantle cell lymphoma. It is a toxic regimen and is typically used in patients with good performance status, who can tolerate it; otherwise, R-CHOP is used.[34]
Bendamustine and rituximab combination has been successfully used in patients with mantle cell lymphoma in the first and second-line setting.[35] A study by Weidmann et al found that bendamustine in combination with rituximab may be an alternative treatment for aggressive lymphomas in elderly patients who are not eligible for R-CHOP because of its efficacy and low toxicity.[36]
Bortezomib has also been used in patients with relapsed or refractory mantle cell lymphoma.[37]
ProMACE-CytaBOM, m-BACOD, and MACOP-B all proved more toxic than CHOP. However, non-CHOP regimens such as MACOP-B are used as first-line therapies in some subtypes of NHL such as primary mediastinal large B-cell NHL.
After more than 2 decades of scientific investigations, the treatment of aggressive lymphomas was changed by the clinical development of rituximab. Currently, 6-8 cycles of CHOP chemotherapy in combination with rituximab is the standard of care in patients with advanced disease.
The GELA (Groupe d'Etude des Lymphomes de l'Adulte) study was the first phase III trial to demonstrate the efficacy of combining rituximab with standard doses of CHOP chemotherapy for elderly (older than 60 y) patients with diffuse large B-cell lymphoma. At 5-year follow-up, OS was 58% with rituximab and CHOP versus 46% with CHOP alone.[38] The results of this study were further validated by other international randomized studies favoring the use of rituximab and chemotherapy in elderly patients with aggressive B-cell lymphomas.
Studies in younger patients also showed the benefit of combining rituximab and CHOP chemotherapy. A large international study, the MabThera International Trial (MInT,) supported the role of rituximab-chemotherapy in young patients with aggressive B-cell lymphomas.[39] The study, which has been presented only in an abstract form, was a phase III trial in which 823 patients (ages 18-60 y) with diffuse large B-cell, CD20+ NHL (DLBCL).
These patients were randomized to receive either rituximab plus a standard anthracycline-containing chemotherapy regimen (standard chemotherapy) or standard chemotherapy alone as induction therapy. The rituximab plus standard chemotherapy regimens increased 2-year overall survival (OS) from 86% to 95% compared with standard chemotherapy alone and resulted in significant improvement in time to treatment failure and projected overall survival.[39]

Ongoing research is being focused on identifying patients at risk for treatment failure and developing tailored treatment for patients with aggressive lymphoma based on clinical scores (IPI score) or gene profiles. Patients at high risk of relapse (IPI intermediate or poor risk groups) might have an improved 5-year event-free survival/overall survival from autologous and allogeneic bone marrow or peripheral stem cell transplantation following chemotherapy.
CNS prophylaxis, usually with 4-6 injections of methotrexate intrathecally, is recommended for patients with paranasal sinus or testicular involvement, diffuse small noncleaved cell or Burkitt lymphoma, or lymphoblastic lymphoma. CNS prophylaxis for bone marrow involvement is controversial.
Treatment of acute lymphoblastic lymphoma, a very aggressive form of NHL, is usually patterned after acute lymphoblastic leukemia (ALL) therapy. Other subtypes of high-grade lymphomas are usually treated with more aggressive variations of CHOP chemotherapy, including the addition of high-dose methotrexate or other chemotherapy drugs and higher doses of cyclophosphamide.
Management of Indolent Recurrent NHL
In general, treatment with standard agents rarely produces a cure in patients who have relapsed. Sustained remissions after relapse can often be obtained in patients with indolent lymphomas, but relapse usually ensues. Favorable survival after relapse has been associated with age younger than 60 years, prior complete remission rather than partial remission, and duration of response longer than 1 year. For relapse that remains low grade, the following are possible treatment options:
Single alkylating agents (chlorambucil or bendamustine) Novel biological agents and small molecule inhibitors showing promising results in
patients with indolent lymphomas include ofatumumab, lenalidomide, and temsirolimus[40]
Combination chemotherapy - CVP, CHOP, and others Purine analogues - Fludarabine, 2-CDA Rituximab (results in a 40-50% RR in patients with relapsed/refractory indolent B-cell
lymphomas) in standard or extended schedules of administration Radioimmunotherapy
131 Iodine-rituximab radioimmunotherapy of relapsed or refractory indolent NHL achieves high overall response rates and complete response rates with minimal toxicity.[41]
Tositumomab (a murine IgG2a lambda monoclonal antibody directed against CD20 antigen) plus131 I (Bexxar) has been approved by the US Food and Drug Administration for relapsed or refractory, low-grade, follicular, or transformed NHL.[42, 43]
Ibritumomab tiuxetan plus90 Yttrium (Zevalin) also has been approved for use in relapsed indolent lymphoma. These radioimmunotherapy agents typically are used only in patients with less than 25% bone marrow involvement with lymphoma and in patients refractory to rituximab.

Local relapse can be treated with radiotherapy. High-dose chemotherapy plus stem cell transplantation is being investigated to determine whether it can produce significantly better survival rates compared with conventional chemotherapy.[44]
Management of Aggressive Recurrent Adult NHL
High-dose chemotherapy plus stem-cell transplantation is the treatment of choice for patients who have recurrent aggressive lymphomas. Preliminary studies indicate that approximately 20-40% of patients have a long-term disease-free status, but the precise percentage depends on patient selection and specific treatment used.
Second-line chemotherapy regimens such as ICE (ifosfamide, carboplatin, etoposide), DHAP (dexamethasone, high-dose cytarabine, cisplatin), or EPOCH (etoposide, vincristine, doxorubicin, cyclophosphamide, prednisone) are usually used with rituximab if the tumor is CD20 positive.
Gemcitabine and navelbine are also being attempted in these relapsed patients. Chemotherapy is usually followed by stem-cell transplantation.
In the PARMA trial, patients with relapsed NHL who were randomized to autologous bone marrow transplantation followed by involved-field radiation therapy did better than those randomized to conventional chemotherapy and involved-field radiation therapy.[45, 46] After a 5-year median follow-up study, the event-free survival (EFS) rate was significantly better with transplantation (46% versus 12%), and the OS rate was also better (53% versus 32%).
In general, patients who respond to initial therapy and who respond to conventional salvage therapy prior to bone marrow transplantation have better survival outcomes. Patients who relapse late (>12 mo after diagnosis) have better OS than patients who relapse earlier. Patients who are not candidates for transplantation can be treated with chemotherapy with or without monoclonal antibodies. If possible, these patients should be enrolled into clinical trials.
Tumor vaccines are still being investigated for use in patients with lymphoma. Novel biological and small agents showing promising results in ongoing clinical trials include CMC-544, lenalidomide, bortezomib, and temsirolimus.[40]
A study by Witzig et al concluded that lenalidomide is well tolerated and produces durable responses in patients with relapsed or refractory aggressive NHL.[47]
Management of T-cell Lymphomas
The treatment of T-cell lymphomas continues to be challenging. T-cell lymphomas are divided into 2 subgroups: cutaneous or systemic T-cell disorders. Typically, cutaneous T-cell lymphomas (CTCL) are managed with topical agents and oral disease modifiers during the early stage of the disease. See Cutaneous T-Cell Lymphoma for more information on this topic. Systemic chemotherapy is usually incorporated late in the course of the disease with modest activity. Systemic T-cell lymphomas represent a challenge to the practicing oncologist.

The complexity of each subtype of T-cell lymphomas, the low incidence, and poor response to standard therapies are important factors that contribute to the poor clinical outcomes of this group of neoplasms. Most patients with T-cell lymphomas are better served by participating in clinical trials exploring dose-intense regimens, early bone marrow transplantation, and/or novel chemotherapeutic agents. Treatment options for T-cell lymphoma can be categorized as follows:
Combination chemotherapy regimens - CHOP, CHOP plus etoposide, gemcitabine based-regimens
Single chemotherapy agents - Pralatrexate Monoclonal antibodies - Alemtuzumab (effective in prolymphocytic T-cell leukemia
and hepatosplenic gamma-delta T-cell lymphoma) Immunotoxin - Denileukin diftitox Novel biological agents and small molecule inhibitors - Histone deacetylase inhibitors
(vorinostat, panobinostat, romidepsin), lenalidomide, and bortezomib
The US Food and Drug Administration (FDA) granted accelerated approval for pralatrexate injection (Folotyn) as a single agent for the treatment of patients with relapsed or refractory peripheral T-cell lymphoma (PTCL).[48]
In June 2011, the FDA granted accelerated approval for romidepsin (Istodax) for treatment of PTCL in patients who have received at least 1 prior therapy.[49]
Jacobsen et al concluded that hematopoietic stem cell transplantation (HSCT) can result in long-term remissions in patients with relapsed or refractory T-cell lymphoma, especially those with nodal histologies.[50]
Surgical Care
The role of surgery in the treatment of patients with NHL is limited. Surgery is useful in selected situations (eg, GI lymphoma), particularly if the disease is localized or if risk of perforation, obstruction, and massive bleeding is present. Orchiectomy is part of the initial management of testicular lymphoma.
Complications of Therapy
Potential chemotherapy and other treatment-related complications include the following:
Cytopenias (ie, neutropenia, anemia, thrombocytopenia) Nausea or vomiting Infection Fatigue Neuropathy Dehydration after diarrhea or vomiting Cardiac toxicity from doxorubicin Catheter-related sepsis Catheter-related thrombosis Secondary malignancies Tumor lysis syndrome

Atherosclerosis
Tumor lysis syndrome
This syndrome commonly occurs after treatment of high-grade bulky NHLs because of their exquisite sensitivity to therapy, which is caused by their high proliferative capacity. Tumor lysis syndrome is characterized by hyperuricemia, hyperkalemia, hyperphosphatemia, hypocalcemia, and renal failure. Death from cardiac asystole can occur from hyperkalemia.
Measures to prevent this complication include aggressive hydration, allopurinol administration, and urine alkalinization. Frequent monitoring of input and output, electrolytes, uric acid, and creatinine is necessary. Dialysis is sometimes required.
Atherosclerosis
In a 3-year study, Bilora et al found evidence that patients receiving radiotherapy and chemotherapy for lymphoma (either NHL or Hodgkin lymphoma) are predisposed to early development of atherosclerosis.[51] In 96 patients, the investigators found increased intima-media thickness at 1-year follow-up; thickness had decreased at 3-year follow-up, but reduction in flow-mediated dilatation measured in the patients at 1 year had not improved by the 3-year examination.[51]
Dietary Modification
Usually, a regular diet is adequate, except when the patient is neutropenic. Patients with neutropenia should not eat raw fruits or vegetables.
Transplant patients who have severe mucositis, decreasing albumin levels, or both may be administered total parenteral nutrition (TPN) until they can tolerate oral feedings.
Activity Restriction
The following restrictions apply to patients who are neutropenic, thrombocytopenic, or both:
Avoid exposure to or contact with other patients with communicable or infectious diseases
Use a soft toothbrush during episodes of neutropenia and thrombocytopenia Do not shave with a razor
Ideally, patients with neutropenia should be admitted directly to a private room and should not stay long in the emergency department for evaluation. All medical personnel should wash hands before and after examining these patients
Management of NHL in Special Populations
Children
Pediatric patients with NHL are best treated by pediatric oncologists.

Pregnant women
NHL during pregnancy is uncommon, but it presents an ethical dilemma. Remission may be obtained with chemotherapy, but chemotherapy has potentially harmful effects to the fetus. Consider fetal exposure to transplacental chemotherapy when evaluating therapy options and carefully evaluate the timing of delivery.
For patients diagnosed with NHL during the second or third trimester of pregnancy, few literature reports suggest that they can be treated with chemotherapy without significant toxicity to the fetus. If possible, alkylating agents should be avoided. If the fetus can be delivered safely prior to administration of chemotherapy and a short wait will not affect the treatment outcome and prognosis of the patient, starting the treatment after the birth of the baby is better.
If the patient has high-grade NHL (eg, Burkitt or lymphoblastic lymphoma) diagnosed during the first trimester of pregnancy, immediate institution of therapy is necessary; otherwise, the condition could be fatal. Discuss at length with the patient and family that chemotherapy treatment at this period of pregnancy is very risky for the fetus, and whether therapeutic termination of pregnancy should be performed before the patient is treated should be decided. Consultation with the ethical committee of the hospital should be obtained in these very difficult situations.
Consultations
A hematologist-oncologist should treat patients with NHL.
Consult a radiation oncologist for treatment of patients with localized or limited-stage low-grade lymphoma and for palliative radiation therapy (eg, for treatment of SVC syndrome, treatment of painful metastases [especially to bone] as an adjunctive treatment for CNS lymphomas).
Consult an infectious disease specialist for the management of patients with neutropenic fever who are not responding to the usual broad-spectrum antibiotics.
Surgical consultation is needed for lymph node biopsy, palliative procedures, or placement of a venous access device (eg, Port-a-Cath, Hickman catheter) for blood drawing and chemotherapy access.
Long-Term Monitoring
Treatment and follow-up care of patients with NHL are usually performed on an outpatient basis. Monitoring patients’ blood cell counts while they are receiving chemotherapy (eg, prior to each treatment cycle and 10-14 d after each treatment cycle) is important.
Monitor adverse effects of chemotherapy with a detailed patient history, an examination, a CBC, and serum chemistries (especially liver function tests, electrolytes, lactate dehydrogenase, and blood urea nitrogen [BUN]/creatinine).

Treat symptomatic adverse effects such as nausea, vomiting, diarrhea, mucositis, anorexia, pain, and fatigue. Administer packed red blood cell (PRBC) transfusions for patients with symptomatic anemia and provide platelet transfusions for patients with a platelet count less than 10,000- 20,000/mm3. Provide growth factor (eg, granulocyte colony-stimulating factor [GCSF], granulocyte-macrophage colony-stimulating factor [GM-CSF], erythropoietin) support as necessary.
Perform a disease and response to treatment evaluation by obtaining patient history, physical examination (at intervals q2-3mo), and imaging studies (eg, CT scans at intervals q4-12mo).
Provide psychosocial support for the patient and family.
Medication Summary
Multiple chemotherapeutic agents are active against non-Hodgkin lymphoma (NHL) and can be used alone or in combination, depending on the histology and stage of the disease and whether the patient can tolerate chemotherapy. In addition, several biological therapies are currently available for these patients, including interferons, rituximab, and radiolabeled antibodies (the newest biological therapy).
Alkylating agents impair cell function by forming covalent bonds with DNA, ribonucleic acid (RNA), and proteins. These agents are not cell cycle phase–specific and are used for hematologic and nonhematologic malignancies.
Anthracycline antibiotics bind to nucleic acids by intercalation with base pairs of the DNA double helix, interfering with the DNA synthesis. They cause inhibition of DNA topoisomerases I and II.
Vinca alkaloids inhibit microtubule assembly, causing metaphase arrest in dividing cells. Vinca alkaloids are also cell cycle phase–specific at the M and S phase.
Glucocorticoids cause lysis of lymphoid cells, which led to their use against acute lymphoblastic leukemia (ALL), multiple myeloma, and NHL. These agents are also used as adjunctive antiemetic agents, to decrease vasogenic edema associated with tumors, and as prophylactic medication to prevent hypersensitivity reactions associated with some chemotherapeutic drugs.
Antimetabolites cause tumor cell death by inhibiting enzymes that are important in DNA synthesis.
Biological response modulators control the response of the patient's immune system to tumor cells, infecting organisms, or both.
Cytotoxic agents
Class Summary
These agents inhibit cell growth and proliferation.

View full drug information
Chlorambucil (Leukeran)
Chlorambucil alkylates and cross-links strands of DNA, inhibiting DNA replication and RNA transcription. It is used mainly to treat indolent lymphomas, particularly chronic lymphocytic leukemia (CLL) and Waldenstrom macroglobulinemia. This agent may be preferable for elderly patients with serious comorbid medical problems who require treatment for lymphoma. It is well absorbed orally.
View full drug information
Cyclophosphamide (Cytoxan)
Cyclophosphamide is chemically related to nitrogen mustards. As an alkylating agent, the mechanism of action of the active metabolites may involve cross-linking of DNA, which may interfere with growth of normal and neoplastic cells. This agent can be used alone but is mostly used as a component of multiple combination chemotherapy regimens.
View full drug information
Doxorubicin (Adriamycin)
An anthracycline antibiotic that can intercalate with DNA, doxorubicin affects many of the functions of DNA, including synthesis. It forms DNA-cleavable complexes by interaction with topoisomerase II, which is responsible for the cytocidal activity of the drug. Doxorubicin is administered IV and distributes widely into bodily tissues, including the heart, kidneys, lungs, liver, and spleen. It does not cross the blood-brain barrier and is excreted primarily in bile. It forms an important part of multiple chemotherapeutic regimens for lymphomas, including cyclophosphamide, hydroxydaunomycin (doxorubicin), vincristine (Oncovin), and prednisone (CHOP).
View full drug information
Vincristine (Oncovin)
The mechanism of action of vincristine is uncertain. It may involve a decrease in reticuloendothelial cell function or an increase in platelet production; however, neither of these mechanisms fully explains the effect in thrombocytopenic purpura and hemolytic-uremic syndrome. Vincristine is used in hematologic and nonhematologic malignancies. It is a component of CHOP and other regimens for lymphoma.
View full drug information
Fludarabine (Fludara)

Fludarabine is a purine analogue that interferes with DNA synthesis by inhibiting ribonucleotide reductase. It is also incorporated into RNA, causing inhibition of RNA and protein synthesis; however, its primary effect may result from activation of apoptosis.
View full drug information
Pralatrexate (Folotyn)
This agent is a folate inhibitor. It is indicated for relapsed or refractory peripheral T-cell lymphoma.
View full drug information
Nelarabine (Arranon)
Nelarabine is a prodrug of the deoxyguanosine analogue 9-beta-D-arabinofuranosylguanine (ara-G). It is converted to the active 5'-triphosphate, ara-GTP, a T-cell–selective nucleoside analog. Leukemic blast cells accumulate ara-GTP. This allows for incorporation into DNA, leading to inhibition of DNA synthesis and cell death.
View full drug information
Etoposide (Toposar)
Etoposide is a glycosidic derivative of podophyllotoxin that exerts its cytotoxic effect through stabilization of the normally transient covalent intermediates formed between DNA substrate and topoisomerase II, leading to single- and double-strand DNA breaks. This causes cell proliferation to arrest in the late S or early G2 portion of the cell cycle.
View full drug information
Mitoxantrone (Novantrone)
Mitoxantrone inhibits cell proliferation by intercalating DNA and inhibiting topoisomerase II.
View full drug information
Cytarabine
Cytarabine is converted intracellularly to the active compound cytarabine-5'-triphosphate, which inhibits DNA polymerase. It is cell cycle S phase specific and it blocks the progression from the G1 to the S phase, in turn killing cells that undergo DNA synthesis in the S phase of the cell proliferation cycle.
View full drug information

Bendamustine (Treanda)
Bendamustine is an alkylating agent that is a bifunctional mechlorethamine derivative. It forms covalent bonds with electron-rich nucleophilic moieties that can lead to cell death. It is active against both quiescent and dividing cells and is indicated for chronic lymphocytic leukemia (CLL).
View full drug information
Carboplatin
Carboplatin is an analog of cisplatin. This is a heavy metal coordination complex that exerts its cytotoxic effect by platination of DNA, a mechanism analogous to alkylation, leading to interstrand and intrastrand DNA cross-links and inhibition of DNA replication. It binds to protein and other compounds containing the SH group. Cytotoxicity can occur at any stage of the cell cycle, but the cell is most vulnerable to action of these drugs in the G1 and S phases. It has same efficacy as cisplatin, but with a better toxicity profile. The main advantages over cisplatin include less nephrotoxicity and ototoxicity, the lack of a need for extensive prehydration, and a smaller likelihood of inducing nausea and vomiting; however, it is more likely to induce myelotoxicity.
View full drug information
Cisplatin
Cisplatin is a platinum-containing compound that exerts its antineoplastic effect by covalently binding to DNA, with preferential binding to the N-7 position of guanine and adenosine. It can react with 2 different sites on DNA to cause cross-links. The platinum complex also can bind to the nucleus and to cytoplasmic protein. A bifunctional alkylating agent, once cisplatin is activated to the aquated form in the cell, it binds to DNA, resulting in interstrand and intrastrand cross-linking and denaturation of the double helix.
View full drug information
Gemcitabine
Gemcitabine is a cytidine analog. It is metabolized intracellularly to an active nucleotide. It inhibits ribonucleotide reductase and competes with deoxycytidine triphosphate for incorporation into DNA. It is cell-cycle specific for the S phase. Gemcitabine is indicated as first-line treatment for locally advanced (nonresectable stage II or stage III) or metastatic (stage IV) pancreatic adenocarcinoma.
View full drug information
Denileukin Diftitox (Ontak)

Denileukin diftitox is a molecule in which the diphtheria toxin and the receptor-binding domain of human interleukin 2 (IL-2) are fused. This fusion protein selectively delivers the cytotoxic activity of diphtheria toxin to targeted cells. It is used only in T-cell lymphoma in which malignant cells express the CD25 component of the IL-2 receptor. The drug binds to the IL-2 receptor (measured by CD25), is internalized by receptor-mediated endocytosis, and then inhibits protein synthesis by translocation of the active portion of diphtheria toxin into the cytosol. This, in turn, causes cell death.
View full drug information
Bleomycin
This agent is composed of a group of glycopeptides extracted from Streptomyces species. Each molecule has a planar end and an amine end; different glycopeptides of the group differ in their terminal amine moieties. The planar end intercalates with DNA, while the amine end facilitates oxidation of bound ferrous ions to ferric ions, thereby generating free radicals, which subsequently cleave DNA, acting specifically at purine-G-C-pyrimidine sequences.
Antineoplastic Agents, Histone Deacetylase Inhibitors
Class Summary
These agents can induce the termination of cell growth, which, in turn, leads to cell death. Agents include vorinostat and romidepsin.
View full drug information
Vorinostat (Zolinza)
Vorinostat is a histone deacetylase (HDAC) inhibitor. HDAC inhibition results in hypoacetylation of core nucleosomal histones, it condenses the chromatin structure, and it represses gene transcription. It is indicated for the treatment of progressive, persistent, or recurrent cutaneous T-cell lymphoma.
View full drug information
Romidepsin (Istodax)
This agent inhibits HDAC, which results in the accumulation of acetyl groups. This leads to alterations in chromatin structure and transcription factor activation, causing the termination of cell growth, which, in turn, leads to cell death. Indicated for CTCL and PTCL in patients who have received at least 1 prior therapy.
Colony-Stimulating Factor Growth Factors

Class Summary
These agents can induce an increase in reticulocyte counts, with a subsequent increase in hematocrit and hemoglobin levels.
View full drug information
Epoetin alfa (Epogen, Procrit)
This agent is a purified glycoprotein produced from mammalian cells modified with gene coding for human erythropoietin (EPO). Its amino acid sequence is identical to that of endogenous EPO. The biological activity of epoetin alfa mimics human urinary EPO, which stimulates division and differentiation of committed erythroid progenitor cells and induces the release of reticulocytes from bone marrow into the blood stream.
View full drug information
Darbepoetin alfa (Aranesp)
This is an erythropoiesis-stimulating protein closely related to EPO, a primary growth factor produced in the kidney that stimulates the development of erythroid progenitor cells. Its mechanism of action is similar to that of endogenous EPO, which interacts with stem cells to increase red blood cell production. It differs from epoetin alfa (recombinant human EPO) in that it contains 5 N-linked oligosaccharide chains, whereas epoetin alfa contains 3. Darbepoetin alfa has a longer half-life than epoetin alfa and can be administered weekly or biweekly.
View full drug information
Filgrastim (Neupogen)
Filgrastim is a recombinant methionyl human granulocyte colony-stimulating factor (r-metHuG-CSF) consisting of a 175–amino acid protein with a molecular weight of 18,800 d. It is produced by Escherichia coli bacteria into which the human G-CSF gene is inserted. This protein has an amino acid sequence identical to the natural sequence predicted from human DNA sequence analysis, except for the addition of an N-terminal methionine necessary for expression in E coli. Because it is produced in E coli, the product is nonglycosylated and thus differs from G-CSF isolated from human cells.
View full drug information
Pegfilgrastim (Neulasta)
Pegfilgrastim is a long-acting filgrastim created by the covalent conjugate of recombinant granulocyte colony-stimulating factor (ie, filgrastim) and monomethoxypolyethylene glycol. As with filgrastim, it acts on hematopoietic cells by binding to specific cell surface receptors,

thereby activating and stimulating the production, maturation, migration, and cytotoxicity of neutrophils.
Monoclonal Antibodies
Class Summary
The agents in this class target specific antigens in carcinoma cells and induce cytotoxicity.
View full drug information
Rituximab (Rituxan)
Rituximab is a genetically engineered chimeric murine/human monoclonal antibody directed against the CD20 antigen found on the surface of normal and malignant B lymphocytes. The antibody is an immunoglobulin G1 (IgG1) kappa immunoglobulin containing murine light- and heavy-chain variable region sequences and human constant region sequences.
View full drug information
Ibritumomab tiuxetan (Zevalin)
A murine monoclonal antibody that targets the CD20 antigen, ibritumomab tiuxetan is chelated to the radioisotopes indium-111 or yttrium-90. It is used in conjunction with rituximab to treat B-cell NHL or rituximab-refractory follicular NHL. The regimen consists of 2 low doses of rituximab, an imaging dose, 2-3 whole body scans, and a therapeutic dose, all of which are delivered in an outpatient setting over 8 days.
View full drug information
Tositumomab and iodine I131 (BEXXAR)
Tositumomab is a murine IgG2a lambda monoclonal antibody directed against the CD20 antigen, which is found on the surface of normal and malignant B lymphocytes. The radiolabeled tositumomab (ie, iodine I131 tositumomab) is administered following the nonradiotherapeutic version to direct treatment precisely to the malignancy. Possible mechanisms of action include apoptosis, complement-dependent cytotoxicity, antibody-dependent cytotoxicity, and ionizing radiation. Indicated for CD20-positive non-Hodgkin lymphoma that has recurred following chemotherapy and is refractory to rituximab.
View full drug information
Alemtuzumab (Campath)

Alemtuzumab is a monoclonal antibody against CD52, an antigen found on B cells, T cells, and almost all chronic lymphocytic leukemia cells. It binds to the CD52 receptor of the lymphocytes, which slows the proliferation of leukocytes.
View full drug information
Ofatumumab (Arzerra)
Ofatumumab is an anti-CD20 human monoclonal antibody that inhibits B-cell activation in early stages. It is indicated for chronic lymphocytic leukemia refractory to fludarabine and alemtuzumab.
Antineoplastic Agents, mTOR Kinase Inhibitors
Class Summary
Agents in this class halt the cell cycle at the G1 phase in tumor cells.
View full drug information
Temsirolimus (Torisel)
Temsirolimus is a water-soluble ester of sirolimus. It binds with high affinity to immunophilin FKBP (FK506-binding protein). This complex inhibits mammalian target of rapamycin (mTOR) kinase, a key protein in cells that regulate the gene translation responsible for cell-cycle regulation. mTOR also reduces the cell growth factors (eg, vascular endothelial growth factor) involved in new blood vessel development.
Antineoplastic Agents, Proteasome Inhibitors
Class Summary
Agents in this class may cause cell-cycle arrest and apoptosis.
View full drug information
Bortezomib (Velcade)
This is the first drug approved of the anticancer agents known as proteasome inhibitors. The proteasome pathway is an enzyme complex existing in all cells. This complex degrades ubiquitinated proteins that control the cell cycle and cellular processes and maintains cellular homeostasis. Reversible proteasome inhibition disrupts the pathways supporting cell growth, thus decreases cancer cell survival.
mmunomodulators

Class Summary
These drugs regulate key events responsible for immune reactions.
View full drug information
Interferon alfa-2a (Roferon-A) or alfa-2b (Intron A)
These drugs regulate key events responsible for immune reactions
Corticosteroids
Class Summary
These drugs have anti-inflammatory properties and cause profound and varied metabolic effects. Corticosteroids modify the body's immune response to diverse stimuli.
View full drug information
Dexamethasone (Decadron, AK-Dex, Alba-Dex, Baldex)
A component of the m-BACOD (methotrexate, bleomycin, doxorubicin [Adriamycin], cyclophosphamide, Oncovin, and dexamethasone) regimen, dexamethasone is a glucocorticoid that acts as an immunosuppressant by stimulating the synthesis of enzymes needed to decrease the inflammatory response. It also acts as an anti-inflammatory agent by inhibiting the recruitment of leukocytes and monocyte-macrophages into affected areas via inhibition of chemotactic factors and factors that increase capillary permeability.
Dexamethasone is readily absorbed via the GI tract and metabolized in the liver. Inactive metabolites are excreted via the kidneys. Most of the adverse effects of corticosteroids are dose dependent or duration dependent.
View full drug information
Prednisone (Deltasone, Orasone, Meticorten)
A component of several regimens, such as CHOP, prednisone is a glucocorticoid that acts as an immunosuppressant by stimulating the synthesis of enzymes needed to decrease the inflammatory response. It also acts as an anti-inflammatory agent by inhibiting the recruitment of leukocytes and monocyte-macrophages into affected areas via inhibition of chemotactic factors and factors that increase capillary permeability.
Prednisone is readily absorbed via the GI tract and metabolized in the liver. Inactive metabolites are excreted via the kidneys. Most of the adverse effects of corticosteroids are dose dependent or duration dependent.

Sumber
- Harrison- Wintrobe