Embed Size (px)
Citation preview

Basic and Clinical Cardiac Electrophysiology of Encainide
JAY W. MASON, MD
Encainide is a potent sodium channel antagonist. It dissociates slowly from blocked, repolarized channels (time constant of recovery >20 seconds). It markedly slows myocardial and His Purkinje conduction in vitro, in animal models and in humans. In vitro the parent compound and its major metabolites, 0-demethyl and 3-methoxy-0-demethyl encainide, have variable effects on action potential duration and refractoriness. In man the parent compound has relatively little effect on refractoriness and QT interval, but its metabolites may increase refractoriness moderately. Encainide has no significant effect on the normal sinoatrial node, and
only its metabolites significantly depress atrioventricular nodal conduction and refractoriness. In models of ischemia, all of encainide’s actions are more pronounced in ischemic than in normal tissue. Encainide is similar in its basic and clinical electrophysiologic profile to flecainide and lorcainide although its constellation of electrophysiologic properties is unique. It differs from quinidine, procainamide and disopyramide by slowing conduction more and affecting refractoriness less, and by absence of anticholinergic side effects.
(Am J Cardiol 1988;58:18C-24C)
E ncainide is a cardiac sodium channel blocker with proven clinical antiarrhythmic efficacy. It has diverse effects on electrophysiologic properties of normal and abnormal myocardium and cardiac conduction tissue. Its identified electrophysiologic effects appear to ac- count for its clinical efficacy as well as its undesirable cardiac effects. This article reviews both basic and clinical electrophysiologic effects of encainide. It will also draw parallels between encainide’s basic and clinical electrophysiological effects and compare them with other antiarrhythmic drugs. Encainide’s antiar- rhythmic or antifibrillatory effects will not be dis- cussed, as these topics are adequately covered else- where in this issue.
Cellular Electrophysiology of Encainide In 1978 Gibson et all demonstrated a concentration-
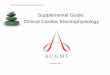
dependent reduction in maximum first time derivative of the upstroke of the action potential (V,,,) of canine Purkinje fibers by encainide. This depression of the fast sodium current was accompanied by an expected decrease in myocardial conduction velocity (Fig. 1). Gibson et al found a decrease in action potential dura- tion but no change in myocardial effective refractory period. They observed a decrease in spontaneous automaticity. In this preparation encainide did not
From the Cardiology Division, University of Utah Medical Cen- ter, Salt Lake City, Utah.
Address for reprints: Jay W. Mason, MD, Cardiology Division, University of Utah Medical Center, 50 North Medical Drive, Salt Lake City, Utah 84132.
prevent ouabain-induced increased automaticity. In general, the findings of Gibson and colleagues are consistent with clinical reports of increased QRS com- plex duration and His Purkinje conduction time, and absence of QT prolongation by acute exposure to en- cainide (which will be discussed].
Carmeliet2 studied encainide in guinea pig myocar- dium, sheep Purkinje fiber, cow Purkinje fiber and guinea pig Langendorf preparation. He also demon- strated sodium channel blockade by encainide as in- ferred from its reduction of Vi,,,. In the 3 species he studied action potential duration was either un- changed or decreased. Depolarization-induced auto- maticity and abnormal automaticity induced by oua- bain administration were blocked by encainide. In the Langendorf preparation His Purkinje conduction was markedly depressed while AV nodal conduction was only modestly depressed. Carmeliet found no effect of encainide on calcium-dependent action potentials in- duced by high potassium concentration and isoproter- enol.
Elharrar and Zipes3 studied the effects of encainide and compared them to its 2 major metabolites, O-de- methyl encainide (ODE) and 3-methoxy+hydroxy-O- demethyl encainide in canine Purkinj e tissue and ven- tricular muscle. In general, all 3 compounds exerted effects similar to those found for encainide by previ- ous investigators. ODE was markedly more potent than encainide and its methoxy metabolite. In this study only ODE depressed depolarization-induced automaticity. Encainide and its metabolites depressed calcium-mediated action potential while in the study

August 29, 1986 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 58 19c
of Carmeliet2 the parent compound had no effect on calcium-dependent action potentials. Elharrar and Zipes3 found that encainide and its metabolites short- ened action potential duration significantly in canine Purkinje tissue, while it had no significant effect on action potential duration in myocardium (Fig. 2).
The greater potency of ODE compared with the other 2 compounds demonstrated by Elharrar and Zipes probably has clinical significance, because this metabolite achieves a high concentration in patients and has a longer elimination half-life than the parent drug.
Two studies have been published concerning the effects of encainide in ischemic tissue compared with normal tissue. Wong et al4 showed that encainide’s electrophysiologic effects were more marked and oc- curred at a lower concentration of the drug in acutely
>
B l-i=
ischemic rabbit ventricular myocardium. Unlike find- ings in most other studies, these investigators demon- strated a prolongation of the action potential in normal cells and found this effect to be more pronounced in ischemic areas. King and Man5 studied encainide’s effects on canine subendocardial Purkinje fibers sur- viving in areas of experimental infarction. They also found ischemic tissue to be more sensitive to encain- ide. In their experiment action potential duration was decreased. They found no additional influence of de- creased pH on encainide’s electrophysiologic effects. Spontaneous depolarization of surviving Purkinje fi- bers was slowed.
Campbell6 has published the most complete data regarding kinetics of sodium channel depression by encainide. He studied the rate-dependence of sodium channel blockade and the recovery of sodium chan- nels from this blockade in guinea pig papillary muscle. He found that V,,, diminished progressively during rate trains with nearly equal decreases from 1 beat to the next until steady state was approached. The time constant for recovery from use-dependent block for encainide was extremely long: 20.3 f 0.9 seconds. Val- ues for other drugs are mexiletine 0.5 second,6 amio- darone 1.6 seconds7 and disopyramide 12.2 seconds.6 Campbell speculated that this slow recovery process accounts for the reduced His Purkinje and myocardial conduction seen in patients with physiologic heart rates, and is due to persistence of drug effect despite the rest period provided by diastole. He also suggested that encainide might be expected to work equally well in suppressing tachycardias with fast or slow rates compared with other agents.
ENCAINIDE MJ14030 MJ 9444
\ Comv- 2 1 2 J --’ -J -
_I 40mV
2 m5ec
FIGURE 1. B, encainide, 10p5M, is shown to increase conduction time between 2 microelectrodes in dog Purkinje fiber compared with A, control and C, washout. Reproduced with permission from Eur J Pharmacol.’
FIGURE 2. The effects of encainide, 3-methoxy-4-hydroxy-o-de- methyl encainide (MJ14030) and 0-demethyl encainide (MJ9444) on action potential duration are shown in dog Purkinje fiber (A, control [arrow] and drug superimposed) and ventricular muscle (B, control, and C, drug). In Purkinje fiber all 3 compounds caused a statistically significant decrease in action potential duration. In muscle the first 2 increased and the last decreased action potential duration insignificantly. Reproduced with permission from J Phar- macol Exp Ther.3

2oc A SYMPOSIUM: ENCAINIDE
TABLE I Effects of Encainide and Metabolites on Normal Myocardial and Purkinje Action Potential Duration and Refractoriness
Species Reference Purkinje Myocardial
Dog (in vitro) 1 Sheep (in vitro) 2 Cow (in vitro) 2 Guinea pig (in vitro) 2 Dog (in vitro) . 3 Rabbit (in vitro) 4 Dog (in vitro) 5 Sheep (in vitro) 7 Dog (in viva) a Dog (in viva) 9 Dog (in vivo) 10 Dog (in vivo) 11 Dog (in vivo) 12 Dog (in vivo) 13 Dog (in viva) 14 Man (in vivo) 15 Man (in vivo) 16 Man (in vivo) 17 Man (in viva) 21
APD ERP
i 0 0
J- 1 E,OD;MODE 4 E,ODE,MODE
- -
0 1 -
0
- - - - - 0’ E,ODE,MODE
- -
APD or QT -
-
0 0 E,ODE,MODE
t - -
0
t 0 ODE
- -
t E,ODyMODE
1: oc
ERP - - - -
? - -
0
t ODE
t ODE OE
0* E,ODE,MODE 7 E,ODE,MODE
t: 0, tc
-
* Reported changes in ERP in this study are too complex to summarize here: the net effect of high doses was no change. ADP = action potential duration; C = chronic oral encainide; E = encainide; ERP = effective refractory period; MODE = 3-methoxy-4 hydroxy-O-demethyl en-
cainide; ODE = 0-demethyl encainide; QT = electrocardiographic QT interval; 1 = decreased by drug; 1 = increased by drug; 0 = no statistically significant ef- fect of drug: - = not studied.
Statistically significant effects in normal tissue only are given. Unless otherwise indicated, the agent under study was encainide given acutely, not chronically.
In the most recent full publication of electrophysio- logic effects of encainide Arnsdorf et al8 studied myo- cardial excitability in sheep Purkinje fibers. They found multiphasic responses in the several determi- nants of cardiac excitability that they studied. They showed that encainide is capable not only of reducing excitability, as can be inferred from previous studies, but also of increasing excitability, which they speculat- ed could account in part for encainide’s proarrhythmic effect. At this time there are no reports that determine with certainty the exact nature of encainide’s sodium
60 , I
I - HV ** cn El QRS T
ki 3” -
g 6 40-
5 y 30- a e 5 20 -
E 10 -
(n=4) (n=4) (n=7)
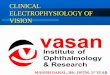
FIGURE 3. Mean percent change in QRS duration (stippled bars) and HV interval (so/id bars) are shown at the end of a ll-minute infusion of 3 doses of encainide (L = 0.3 mgfkg in 4 dogs, M = 0.9 mg/kg in 4 dogs, H = 2.7 mg/kg in 7 dogs). Both variables in- creased, and the increase was statistically significant afler the higher doses. Reproduced with permission from Am J Cardiol.g
channel blockade. It does seem clear that it interacts little if any with the rested sodium channel. Whether it interacts predominantly with the open or inactivated channel is not known. Studies are also lacking in which encainide is directly compared with new anti- arrhythmic agents, especially those most similar to it, such as flecainide and lorcainide.
Electrophysiology of Encainide in Intact Animals Sami et al9 reported in 1979 on the effects of encain-
ide on conduction and refractoriness in the intact ca- nine heart. They assessed the short-term effects of 3 doses of encainide administered intravenously. QRS complex duration and HV interval were increased by all 3 doses and the extent of change was dose related [Fig. 3). The medium dose (0.9 mg/kg given over 15 minutes) increased the HV interval by 48 f 12% and the QRS by 29 f 7%. Encainide had no significant effect at any dose level on heart rate, sinus node recov- ery time, atrioventricular (AV) nodal conduction, and refractoriness of the atrium, AV node and ventricular myocardium. Encainide did not prolong the QT inter- val, This was a short-term study of intravenously ad- ministered encainide, and thus could not assess affects of encainide’s metabolites.
In 1981 Samuelsson and HarrisonlO recorded atria1 and ventricular monophasic action potentials after 2 intravenous infusions of 2.7 mg/kg of encainide sepa- rated by 1 hour. Unlike the previous study from the same laboratory,g this study showed a statistically sig- nificant increase in QT interval and refractory periods of atrium and ventricle. These changes were relatively small (though statistically significant) after the first dose and much more marked after the second dose of encainide. The duration of the monophasic action po-

August 29, 1986 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 58 21c
tential of both right atrium and right ventricle was also significantly increased at both dose levels. The reason for the difference between the 2 studies cannot be explained by differences in plasma encainide concen- tration, as they were quite similar for the initial en- cainide dose. The 2 studies considered together dem- onstrate that encainide has a striking depressant effect on conduction in His Purkinje system and myocardi- urn and a much less marked effect on refractoriness of atrium and ventricle, which increases with larger dose and time. Accumulation of encainide’s metabolites could account for the latter finding. In 1981 Duff et all1 reported on the electrophysiologic effects of ODE compared with placebo in a canine model. They found a significant increase in ventricular refractoriness and a decrease in AV nodal conduction velocity. They not- ed that these effects are not seen with infusions of the parent compound and concluded that the ODE metab- olite has electrophysiologic effects distinctly different from those of encainide. In a later report the same group evaluated electrophysiologic effects in normal and infarcted tissue as well as inducibility of ventricu- lar tachycardia after infusion of ODE in a canine in- farction model.12 The metabolite did not consistently affect arrhythmia inducibility, but did affect both con- duction and refractoriness more markedly in the infarcted than the normal ventricular tissue. Enhance- ment of the drug’s effect in ischemic tissue is reminis- cent of the previously mentioned cellular electro- physiologic effects.
Ro et all3 evaluated encainide’s effects in a canine model of acute myocardial infarction. Encainide pro- duced the expected depression of conduction in both normal and ischemic zones. The effect, was more marked in the ischemic zone. Further, in the ischemic zone only, encainide prolonged refractoriness.
Dresel14 studied encainide and its 2 major metabo- lites in perfused rabbit heart and in the in situ dog heart. The metabolites were found to be far more po- tent than the parent compound in slowing conduction in the rabbit heart. This investigator found that encain- ide and its metabolites had inconsistent effects on His Purkinje and myocardial refractory periods in the dog heart.
Capos et all5 recently compared the refractory peri- od effects of encainide and its 2 major metabolites. They also found that all 3 compounds acutely prolong refractoriness. Thus, the reported effects of encainide and its metabolites on refractoriness and repolariza- tion time vary considerably in vitro and in vivo. These actions are summarized in Table I. These data show either no change or a decrease in Purkinje tissue re- fractoriness and action potential duration by encain- ide and its metabolites, while no change or an increase is demonstrated in myocardium.
Clinical Electrophysiologic Effects of Encainide Clinical electrophysiologic effects of encainide and
its metabolites are summarized in Table II. Sami et al16 produced the initial report of encainide’s cardiac con- duction system effects in man (Fig. 4 and 51. The proto- col and findings were similar to those of their earlier
TABLE II Clinical Electraphysiologic Effects of Enceinide
Acute Oral or IV Therapy Chronic Therapy
Electrocardiographic variables
Heart rate 0 0 PR interval 0% duration rrt I QT interval 0 0, f * JT interval 0 0, t *
Electrophysiologic variables
SNRT 0 0 AH interval HV interval R k AVN ERP 0 HPS ERP -
RV ERP 0 i
* Reports differ. AVN = atrioventricular node: HPS = His Purkinje system; RV = right
ventricle; SNRT = sinus node recovery time; ft = markedly increased by drug: other abbreviations as in Table I.
study in dogs. Encainide prolonged HV conduction and QRS duration. It produced a statistically signifi- cant but clinically insignificant increase in QT interval (+2%). AV nodal conduction and refractoriness, right ventricular refractoriness, sinus rate and recovery time and blood pressure were unaffected by encain- ide. Like the canine study, this one examined only acute effects of the parent compound.
Jackman et all7 studied the electrophysiologic ef- fects of chronic orally administered encainide. En- cainide not only lengthened the HV interval and QRS duration, but also increased AV nodal conduction time, QT interval and refractory periods of right atri- um and right ventricle. The sinus node was not affect- ed. They concluded that encainide’s metabolites exert AV nodal and myocardial repolarization effects that are not seen after a brief exposure to the parent compound.
DiBianco et alI8 studied encainide’s electrophysio- logic effects after short-term intravenous exposure, longer term intravenous exposure and chronic oral therapy. In all conditions the HV interval was marked- ly prolonged. After brief intravenous exposure AV nodal properties and ventricular refractory period were unchanged. There was a trend toward greater AV nodal effect during more protracted intravenous infusion. AV nodal and ventricular refractory period effects were still more marked during chronic therapy. More recently Libersa et all9 performed serial electro- physiologic study and plasma concentration determi- nation of encainide and its metabolites for up to 1 hour after an intravenous infusion of encainide. Although they did not show a change in refractory periods, they did demonstrate that AV nodal conduction properties were not affected early, but were depressed at later time periods in the study. This effect was positively correlated with increasing plasma concentrations of ODE.

22c A SYMPOSIUM: ENCAINIDE
Schwartz et alzo studied the conduction system ef- fects of encainide in 6 patients with bundle branch block and concluded that patients with preexisting infranodal conduction disease were more susceptible to depression of His Purkinje conduction by encain- ide. Narulazl studied the effects of chronically admin- istered encainide on reentry in the His Purkinje sys- tem in 8 patients. He found that the echo zone was widened by encainide, and considered this a potential adverse effect.
A number of reports (for example, DiBianco,18 Mason,2z Morganrothz3 and their co-workers) have demonstrated efficacy of encainide in suppressing spontaneous ventricular premature complexes and ventricular tachycardia. These antiarrhythmic effects are discussed in more detail elsewhere in this issue.
Comparison of Encainide’s Electrophysiologic Effects with Other Antiarrhythmic Agents
The prominent and characteristic electrophysiolog- ic effect of encainide is marked slowing of ventricular and His Purkinje conduction, a result of potent sodium channel blockade. In this regard, encainide is similar to other recently developed antiarrhythmic drugs that markedly prolong conduction, including flecainide and lorcainide. Although the conventional antiar- rhythmic agents quinidine, procainamide and disopyr- amide are also capable of markedly prolonging myo- cardial and His Purkinje conduction, they can only do so at clinically intolerable dosages.
Encainide also differs from quinidine, procaina- mide and disopyramide by having a much smaller effect on repolarization. The final major difference in electrophysiology of encainide compared with quini- dine, procainamide and disopyramide is absence of an anticholinergic effect in the former drug. This differ- ence not only affects significantly the net sinoatrial and AV nodal effects of the former compared with the latter 3 drugs, but also importantly influences their side effect profiles.
Encainide’s electrophysiologic effects are marked- ly different from those of lidocaine and its congeners,
tocainide and mexiletine. The latter 3 drugs do not significantly affect myocardial and His Purkinje con- duction velocities at physiologic sinus rates. Encainide does. While none of the 4 exert significant tonic block, recovery from phasic block by encainide is much slow- er than from lidocaine and its congeners. There has been insufficient direct comparison of encainide with other antiarrhythmic agents in isolated tissue or in intact animals to draw additional firm comparisons.
Comparison of the clinical electrophysiologic ef- fects of encainide with those of flecainide is of special interest because both agents are new and possess many similarities. The most important similarities are their ability to depress conduction and eliminate pre- mature ventricular complexes in humans.
Unlike encainide, flecainide is not metabolized to compounds with important clinical activity. Thus, its electrophysiologic effects after both intravenous and oral administration are similar.
In the tissue bath flecainide has been shown to markedly depress V,,, in myocardium and Purkinje tissue.24-26 In 1 studyz5 flecainide was shown to have a variable effect on myocardial action potential duration depending on concentration. In another it was shown to increase duration in myocardium but to decrease it in Purkinj e tissue,26 which is similar to encainide.
In a third study flecainide decreased the action potential duration at 50% repolarization but prolonged it at 96% repolarization, although not significantly.26 Encainide has a similar effect on the shape of the action potential.
Olson and Edvardssonz7 studied the intraventricu- lar conduction time, ventricular effective refractory period and ventricular monophasic action potential in humans. Flecainide significantly increased intraven- tricular conduction time and caused a modest increase in ventricular effective refractory period and mono- phasic action potential duration. Hellestrand et a128 studied the effects of intravenous flecainide in 47 pa- tients. All conduction intervals were significantly in- creased. Repolarization, measured from the J point to the end of the T wave, however, was not altered. A
H” 4s , “Y 50 , H” 55 H” BO
bl I (
IllllllIllllllIIlillIlll IlillIIlllIIIllIIlllIIlI lIIIIlllllllIIIllllllIII IllIIlIllllIIIIlIl’lllIlI FIGURE 4. Conduction system effects of encainide in man are illustrated. Three surface electrocardiographic leads (I, aVF, V,), an atrial electrogram (AE) and a His bundle electrogram (HE) are displayed with aortic pressure (Ao) and a zero baseline (bl). Leff panel was re- corded during atrial pacing (arrows) before encainide administration. The subsequent 3 panels were recorded at 5, IO and 15 minutes dur- ing a 15minute infusion of encainide, 0.9 mg/kg, during atrial pacing at the same rate. The measured AH and HV intervals are noted at the bottom of each panel. There was a marked, progressive increase in HV interval. AH changed minimally. Widening of the QRS complexes can also be appreciated by comparison of lead I in the leftmost and rightmost panels. Reproduced with permission from Am J Cardiol.16

August 29, 1986 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 58 23C
statistically significant but small increase in ventricu- lar refractoriness occurred (+9 ms). Vik-Mo et alzg studied the drug’s effects after intravenous infusion in patients with sinus node disease. Sinus node recovery was significantly depressed in these patients. All con- duction intervals increased. Ventricular refractory pe- riods were not reported, but the QT interval increased significantly although modestly. Anderson et a130 stud- ied the electrophysiologic effects of flecainide in 15 patients with recurrent ventricular tachyarrhythmias.
TIME (minutes)
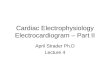
FIGURE 5. Serially determined mean plasma concentration (Cp), aortic pressure (BP) and electrophysiologic variables (heart rate [HR], AH interval, HV interval, QRS complex duration and QT inter- val) are displayed during 0 to 15 minutes, (stippled portion) and immediately after infusion of 0.6 mg/kg (0) or 0.9 mg/kg (0) of encainide in 10 patients. Only HV and QRS intervals were signifl- cantly affected. Although the QT interval increased modestly, this was entirely due to prolongation of the QRS portion of the QT interval. Reproduced with permission from Am J Cardiol.9
TABLE ill Average increase in Electrocardiographic Intervals
@=I*
Flecainide Encainide
PR 39 30 QRS 17 18 QT+ 28 20 JT 11 1
* Data summarized from references 23 and 32, with permission of authors and publishers.
t QT used in case of flecainide, QT, in case of encainide; QT values for encainide would be expected to be less than QT, values by approximately 10% to 15%.
It caused a significant increase in all conduction inter- vals and a small (lo%), although statistically signifi- cant, increase in ventricular refractory period. In pa- tients with AV reentrant tachycardias Bexton et a131 showed that flecainide prolonged total anterograde and retrograde conduction time and that the extent of prolongation was equivalent whether the acute intra- venous or chronic oral route was used.
In separate multicenter studies coordinated through the Likoff Cardiovascular Institute of Hahne- mann University, flecainide32 and encainide23 were compared with quinidine. Electrocardiographic data 1 were obtained. Flecainide increased electrocardio- graphic intervals to the same extent that encainide did, except that the former had a greater effect on repolari- zation [Table III).
Thus, the basic and clinical electrophysiologic ef- fects of encainide and flecainide are very similar. They differ in that encainide’s depressant effects on AV nodal conduction and ventricular refractory peri- ods are only seen after chronic therapy, and chronic encainide exerts a smaller effect than chronic flecain- ide on ventricular repolarization.
In summary, encainide has distinct electrophysio- logic properties. It is a potent sodium channel blocker, and in this regard is similar to flecainide and lorcain- ide, among a number of newly developed potent so- dium channel-blocking agents. It differs from the conventional sodium channel antagonists (quinidine, procainamide and disopyramide) in that it affects ven- tricular refractory period to a much lesser extent.
Encainide demonstrates the probability that pure (or nearly pure) sodium channel blockade is a potent and independently sufficient ventricular antiarrhyth- mic property, as encainide is among the most effective known suppressors of ventricular ectopic beats.
Encainide stands alone as a clinical antiarrhythmic agent whose major metabolites are not only electro- physiologically active, but have electrophysiologic ef- fects distinctly different from those of the parent com- pound. Encainide’s constellation of electrophysiologic effects, including its long time constant of recovery from sodium channel block, is unique.
References 1. Gibson JK, Somani P, Bassett AL. Electrophysiologic effects of encainide (A41 9067] on canine Purkinje fibers. Eur f PharmacoI1978:52:161-169.

24C A SYMPOSIUM: ENCAINIDE
2. Carmeliet E. Electrophysiolagicai effects of encainide on isolated cardiac muscle and Purkinje fibers and on the Langendorff-perfused guinea-pig heart. Eur J PharmacoI1980;61:247-262. 3. Elharrar V, Zipes DP. Effects of encoinide and metabolites (MJ14030 and Mj9444] on canine cardiac Purkinje and ventricular fibers. J Pharmacol Exp Ther 1982;220:440-447. 4. Wong SS, Myerburg RJ, Ezrin AM, Gelband H, Bassett AL. Electrophysio- logic effects of encainide on acutely ischemic rabbit myocardial cells. Em J PharmacoI~982;80:323-329. 5. King BW, Man RYK. Electrophysiological effects of encainide (MJ9067) on canine subendocardial Purkinje fibers surviving infarction. J Cardiovasc PharmacoI1984;6:547-554. 6. Campbell TJ. Resting and rate-dependent depression of maximum rate of depolarisation (VmOx) in guinea pig ventricular action potentials by mexile- tine, disopyramide, and encainide. J Cardiovasc PharmacoI1983;5:291-296. 7. Mason JW, Hondeghem LM, Katzung BG. Block of inactivated sodium channels and of depolarization-induced automaticity in guinea pig papillary muscle by amiodarone. Circ Res 1984;55:277-285. 8. Arnsdorf MF, Schmidt GA, Sawicki GJ. Effects of encainide on the deter- minants of cardiac excitability in sheep Purkinje fibers. j Pharmacol Exp Ther 1985;232:40-48. 9. Sami M, Mason JW, Harrison DC. Canine electrophysiology of encainide, a new antiarrhythmic drug. Am J CardioI1979;43:1149-1254. 10. Samuelsson RG, Harrison DC. Electrophysiologic evaluation of encainide with use of monophasic action potential recording. Am J CardioI2981;48:871- 876. 11. Duff HJ. Dawson AK, Carey EL, Roden DM, Oates JA, Smith RF, Woosley RL. The electrophysiologic actions of 0-demethyl encainide: an active metab- elite (abstr). CIin Res 1981;29:27OA\. 12. Roden DM, Dawson AK, Duff HJ, Woosley RL, Smith RF. Electrophysiol- ogy of 0-demethyl encainide in a canine model of sustained ventricular tachycardia. J Cardiovasc Pharmacol1984;6:588-595. 13. Ro JH, Gillon J, Kupersmith J. Electrophysiologic effects of encainide following acute coronary occlusion in dogs, J Cardiovasc Pharmacol 1981;3:532-540. 14. Dresel PE. Effect of encainide and its two major metabolites on cardiac conduction. J Phormacol Exp Ther 1984;228:180-186. 15. Capos NJ, Samuelsson RG, Harrison DC. Influence of encainide and two metabolites on the ratio of refractory period to action potential duration in the atrium and ventricle in dogs (abstr). PACE 3984;1:466. 16. Sami M, Mason JW, Peters F, Harrison DC. Clinical electrophysiologic effects of encainide, a newly developed antiarrhythmic agent. Am j Cardiol 1979;44:526-532. 17. Jackman WM. Zipes DP, Naccarelli GV, Rinkenberger RL, Heger JJ, Prystowsky EN. Electrophysioiogy of oral encainide. Am J Cardiol 1982;49: 1270-1277.
18. DiBianco R, Fletcher RD, Cohen AI, Gottdiener JS, Singh SN, Katz RJ, Bates HR, Sauerbrunn B. Treatment of frequent ventricular arrhythmia with encainide: assessment using serial ambulatory electrocardiograms, intracar- diac electrophysiologic studies, treadmill exercise tests, and radionuclide cineangiographic studies. Circulation 1982;65:1134-1147, 19. Libersa CC, Lekieffre JP, Caron JF, Poirier JM, Pladys AM, Kacei S, Kher A. Electrophysiological effects of encainide and its metabohtes in 11 patients (abstr). Eur Heart I 1984;5:suppI 1:290. 20. Schwartz AB, Shapiro WA, Same MJ, Shen EN, Bhandari A, Morady F, Scheinman MM. Adverse electrophysiologic effects of encainide in patients with bundle branch block (abstr]. Clin Res 1984;32:1. 21. Narula OS, Cassagneau B, Marin T. Effect of encainide [E) on re-entry in the His Purkinje system (HPS) (abstr]. Circulation 1981;64:suppI IV:135. 22. Mason JW, Peters FA. Antiarrhythmic efficacy of encainide in patients with refractory recurrent ventricular tachycardia. Circulation 1981;63:670- 675. 23. Morganroth J, Somberg JC. Pool PE, Hsu PH, Lee IK, Durkee J. Compara- tive study of encainide and quinidine in the treatment of ventricular arrhyth- mias. jACC 1986:7:9-X 24. Cowan JC, Williams MV. Characterization of a new oral antiarrhythmic drug, flecainide [R818]. Em J PharmacoI1981;73:333-342. 25. Borchard U, Boisten M. Effect of flecainide on action potentials and alternating current-induced arrhythmias in mammalian myocardium. J Car- diovasc PharmacoI1982;4:205-212. 26. Ikeda N, Singh BN, Davis LD, Hauswirth 0. Effects of flecainide on the efectrophysiologic properties of isolated canine and rabbit myocardial fibers. jACC 1985;5,2:303-310, 27. Olsson SB, Edvardsson N. Clinical efectrophysiologic study of antiar- rhythmic properties of flecainide: acute intraventricular delayed conduction and prolonged repolarization in regular paced and premature beats using intracardiac monophasic action potentials with programmed stimulation, Am Heart J 1981;102:864-871. 28. Hellestrand KJ, Bexton RS, Nathan AW, Spurrell RA, Camm AJ. Acute electrophysiological effects of flecainide acetate on cardiac conduction and refractoriness in man. Br Heart j 19822;48:140-148. 2% Vik-Mo H, Ohm OJ, Lund-Johansen P. Electrophysiologic effects of fle- cainide acetate in patients with sinus nodal dysfunction. Am J Cardiol 1982;50:1090-1094. 30. Anderson IL, Lutz IR, Allison SB. Electronhvsioloeic and antiarrhvthmic
., u
effects of oral flecainide in patients with inducible ventricular tachycardia. TACC 1983:2:105-114. 81. Bexton RS, Hellestrand KJ, Nathan AW, Spurrell RAJ, Camm AJ. A comparison of the antiarrhythmic effects on AV junctional re-entrant tachy- cardia of oral and intravenous flecainide acetate. Em Heart J 1983;4:92-102. 32. Flecainide-Quinidine Research Group. Flecainide versus quinidine for treatment of chronic ventricular arrhythmias. Circulation 1983;67:1117-1123.