Embed Size (px)
Citation preview

BASIC CONCEPT ON NEUROANESTHESIA
Tatang Bisri

Objective
To understand technique and anesthetic effect to reach slack brain.
To understand technique and anesthetic effect to CBF, ICP, CO2 reactivity, CMRO2.
To understand perioperative management. To understand mechanism of brain
protection and how to give brain protection.

Cotrell J.E. : Anesthesia for Neurosurgery, 1994
New diagnostic equipment
New monitoring equipment
New anesthetics
New understanding common drugs for neuroanesthesia.
Will be improve outcome in patient with intracranial disorder.

Anesthesiologist target in neurosurgery
Control ICP and brain volume.
Brain protection from ischemia and injury.
Less bleeding
Nancye Edwards : Principles and Practice of Neuro anaesthesia, 1991

The relation ICP and mortality in brain injury
Mean ICP (mm Hg) Mortality (%)
0 - 20 19
21 - 40 28
41 - 80 79
Miller JD : Head injury and brain ischemia implication for therapy Br. J Anaesth. 57 : 120 - 129 , 1985

Methods of brain protection
Basic methods Hypothermia - low normothermia Pharmacology Intravenous Anesthetic : pentothal Inhalation anesthetics: Sevoflurane Lidocaine Mannitol, Magnesium Erythropoietin Alpha 2 agonists dexmedetomidine

Basic methods Control airway, adequate oxygenation, avoidance
hypoxia, hypercapnia (keep normocapnia). Hyperventilation only if herniation present. Control of BP/Maintenance of CPP
normotension or induce hypertension 10-20%. CPP >70 mmHg.
Control ICP (CPP = MAP – ICP). Therapy if ICP 20 mmHg.
Correction of acidosis, electrolyte imbalance,control plasma glucose concentration

Intravenous anesthetics
Barbiturate Ca influx Block Na channel Free radicals inhibition formation. Extracellular lactate, glutamate, aspartat
Propofol: glutamate excotoxicity neuronal damage. propofol infus syndrome

Mortality:
Head injury with :
Hypoxia : 56%
Hypovolemia : 64%
Hypoxia + Hypovolemia : 76%
Without hypoxia+Hypovolemia : 27%Asean Congress of Anaesthesiologist, Singapore, 1995.


Figure: Idealized intracranial pressure volume relationships. From: Shapiro, H.M. Intracranial hypertension: Therapeutic and anaesthetic considerations. Anesthesiology 43: 445-471, 1975

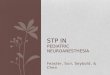
FIG 2 - 4.
Representation of brain function related to two measures of oxygenation ( arterial oxygen partial pressure ( Pa O2 ) and delivered oxygen ( D O2 ) ) and two measures of perfusions (cerebral blood flow ( CBF ) and cerebral perfusions pressures ( CVP ) ).


Anesthesia management : b
A = Clear airway
B = Control ventilation, normocapnia at TBI and slight hypocapnia at brain tumor.
C = Avoid high increase or decrease of BP avoid increase of cerebral venous pressure. normovolemia, iso-osmoler.
D = Avoid drugs & anesthesia technique will increase ICP, give drugs with brain protection effect.
E = environment (temperature control) target 35 degree C in OR

Airway
Clear airway at all the operation and anesthesia.
Non kinking ETT hypoxia or hypercarbia dangerous to
patient.

Ventilation to reach :
PaO2 : 100 - 200 mmHg
PaCO2 : 25 - 30 mmHg for brain tumor surgery
PaCO2 : Normocapnia in brain injury
Avoid PaCO2 < 20 mmHg
Control ventilation

Regulation BP
Hypotension :
CPP = MAP - ICP prefer systolic 90 - 100 mmHg
(tumor)
Normotension (trauma)
Hypertension :
- increase CBV, ICP, edema, blood loss.
- during laringoscopy/intubation, inserting head pin, skin incision, extubation

Mechanical factor which increase
cerebral venous pressure
Coughing, bucking Trendelenburg Neck large vein obstruction Abdominal pressure PEEP v. jugularis interna/v. subclavia
canulation

Preoperative evaluation
similar with routine assessment
add : - evaluation ICP, side effect therapy
- CT Scan, MRI
Premedication :
- avoid narcotic - diazepam 0,15 mg/kg po midazolam 0,025 - 0,05 mg/kg im - children : midazolam 0,75 mg/kg po

Intraoperative anesthetics
1. Monitoring
2. Induction of anesthesia
3. Maintenance of anesthesia :
- inhalation anesthetics (Sevoflurane,
isoflurane)
- intra venous anesthetics (pentothal)
- brain relaxation
- Fluid management
4. Emergence and immediate postoperative

Monitoring
Routine monitoring
ECG, non invasive BP, CVP, invasive BP (artery line), FiO2, pulse oximetry, temperature, peripheral nerve stimulator, catheter urine.

Indication for inserting artery line
Rapid changes of BP
Risk of rapid blood loss.
Hypotension technique
Pathologic condition
Need postoperative ventilation.

Indication for CVP monitoring
Severe blood loss
Measurement status volume
Sitting position / fossa posterior surgery
vasoactive drugs route

ICP Monitoring
still controversial
tumor > 3 cm Need ICP moni -
Edema toring

Target induction of anesthesia Control of PaCO2
Control of BP
Avoid drainage obstruction of cerebral vein
Adequate oxygenation & ventilation
Avoid awareness

Induction of anesthesia O2 100% Fentanyl 1 - 3 ug/kg Pentothal 5 mg/kg 2,5 mg/kg Lidocaine 1 - 1,5 mg/kg Norcuron 0,1 - 0,15 mg/kg oropharyngeal airway eye ointment; paper tape.

Technique to avoid increase BP
Deeper anesthesia: Pentothal
Narcotic : Fentanyl, Sufentanil
Nitroprusside ?
Glyseril trinitrat ?
Lidocaine 1-1,5 mg/kg iv
Alpha 2 agonist dexmedetomidine

Hypotension during induction of anesthesia :
Elevation extremities, not trendelenburg
Give crystalloid colloid
Vasopressor : if under lower limit of autoregulation

Choice of induction agent
Smooth induction more important than really drugs combination
Pentothal 3 - 4 mg/kg
Fentanyl 3 - 5 ug/kg
Vecuronium 0,1 - 0,15 mg/kg
or Rocuronium 0,6 - 0,8 mg/kg
or Atracurium 0,5 mg/kg

Maintenance of anesthesia
Less effect to cerebral autoregulation and response to CO2
Stable cardiovascular
Capable to decrease ICP and increase CPP
One of choice : pentothal, O2 + Sevoflurane, fentanyl, relaxant.

Choice of inhalation anesthetics
Inhalation anesthetic should be evaluated effect on ICP and cerebral vasculature.
All inhalation anesthetic has cerebral vasodilatation effect, will increase CBF, CBV and ICP.
Must be know the effect on cerebral autoregulation, response to CO2 reactivity and CMRO2, brain protection effect.

Variable Halothane Enflurane Isoflurane Sevoflurane
BP
Vascular resistance
Cardiac output
Cardiac contraction
CVP
Heart rate
Sensitization of the heart to epinephrine
0
0
0
0
0
0?
0
0
0
0 0
Cardiovascular effect of volatile inhalation anesthetics at 1-1,5 MAC
0 = no change (<10%)
= 10-20% decrease
= 20-40% decrease = increase

60% N2O : CBF 100% CMR O2 20%
Can decrease by Pentothal, Opioid, Hypocapnia.
Frequent of emesis 90%
Avoid in aerocele, until 5 days after pneumoencephalography, risk of air embolism, redo craniotomy < 3 weeks.
Don’t use N2O (Cottrell, 2001,2002)
N2O

N2O
Increases neurotoxicity of NMDA in rats Potentiated the NMDA damage Adding ketamine worsens damaged neuron. Cottrell. ESA 2004 Adding a nontoxic dose of N2O to
midazolam/isoflurane anesthetic resulted in a robust neurodegenerative reaction more severe in the thalamus and parietal cortex
Jevtovic et al. J neuroscience 2003

Halothane :
Smallest decrease CMR O2 CBF increase 3 x isoflurane With N2O, CBF increase 300%
Autoregulation loss at > 1 MAC and persistent until post operative period.
CSF : production and absorption increase ICP increase whereas hypocarbia BBB & B-CSF barierre : destroyed Increase brain water, permeability BBB, edema concentration 2% mitochondria destroyed myocardium sensitization to catecholamine
Stone DJ et al : The Neuroanaesthesia Hand Book, 1996 Cottrell JE : Anesthesia and Neurosurgery, 1994

Enflurane :
Can produce EEG seizure at moderate dose (1,5 - 2 MAC) and hypocapnia.
CMR O2 decrease
CSF : increase production, decrease absorption
cerebral ischemia protection better than halothane but less than isoflurane.
Loss autoregulation : 1 MAC
Not advised for neuroanesthesia

Isoflurane :
concentration 0,5% CBF decrease 0,95% CBF increase
Increased ICP with Isoflurane 1% easy reduce with hypocapnia / pentothal
Autoregulation intact until 1,5 MAC CO2 Response intact until 2,8 MAC
CSF : production : no change absorption increase
Increase ICP caused by Isoflurane : 30 minutes
Enflurane/halothane : 3 hours
Stone D.J et al : The Neuroanaesthesia Hand Book, 1996
Cottrell : Anesthesia and Neurosurgery, 1994

Isoflurane
Isoflurane only transient protective against a severe focal ischemic insult.
Isoflurane did not inhibit postischemic neuronal apoptosis.
Conclusion: Isoflurane have not brain protection effect.
Werner C. AOSRA Nov 2003, WCA 2004, ESA 2004. Cottrell JE: WCA 2004, ESA June 2004 Kawaguchi et al. Anesth Analg 2004 Warner DS.Anesth Analg 2004

sevoflurane
Sevoflurane improves neurological outcome following incomplete cerebral ischemia in rat.
Werner C et al.Br J Anesth 1995;83
Isoflurane delay but does not prevent cerebral infarction in rats subjected to focal ischemia.
Kawaguchi et al. Anesthesiology 2000;92
Sevoflurane provides sustained anti necrotic and anti apoptotic effect.
Engelhard et al. ASA Annual meeting 2003. Abstract A 740

Sevoflurane:
Have advantages performance for Neuroanesthesi.
Faster recovery Sevoflurane than Isoflurane faster neurologis evaluation post operative period.
Cerebral vasodilatation effect less than halothane, isoflurane.
Effect to blood circulation less than isoflurane More advantages than TIVA. Nathanson, WCA-Montreal, 2000

Autoregulation:
Keep until 1,5 MAC Sevoflurane Gupta et al, Br.J.Anaeth,1997 Summors et al, Anesth Analg , 1999. Autoregulation loss at 1,5 MAC
Isofluran. Matta et al, Anesth Analg,
1999. One of reasoning: effect dilatation Sevo
< Iso

Anoxia NMDA/AMPA
ProtectResponse
ImproveNA+
ImproveATP
ImproveCa+
ProtectResponse
Thiopental (600 μM) Yes Yes No/Yes1 Yes Yes
Midazolam (100 μM) Yes - Yes Yes -
Propofol (20 μg/ml) No Yes Yes Yes No
Lidocaine (10 μM) Yes Yes Yes No -
Isoflurane (1,5%) No No No No -
Sevoflurane (4%) Yes Yes Yes Yes -
Etomidate
3 μg/ml No No No - -
30 μg/ml No Yes No - -
Nitrous oxide (50%) No No No No -
1Worsens ATP after 3.5 minutes of anoxia: improves ATP after 10 minutes of anoxia.
Effect of Anesthetics on Physiological Responses Effect of Anesthetics on Physiological Responses and Ion and Metabolite Levelsand Ion and Metabolite Levels
Cottrell JE. ESA, 2004,Lisbon

Maintenance of anesthesia :
First choice : Sevoflurane Second choice : Isoflurane TOF : 0 fluid : 2/3 diuresis Mannitol : 0,25 - 1 gr/kg Lasix : 0,5 - 1 mg/kg

Fluid
Stable circulation
To avoid : hypovolemia, hypervolemia, hypoosmoler, hyperglycaemia
First choice NaCl 0,9%, avoid RL, no dextrose: 1-1,5 ml/kg/h or 2/3 diuresis.
Dextrose : only for therapy hypoglycaemia (blood sugar < 60 mg%)

Extubation
Be carefully : increase of BP, leading to hyperaemia, oedema, increase of ICP.
Lidocaine 1 - 1,5 mg/kg, alpha 2 agonist dexmedetomidine.
End of surgery increase TOF = 1
Et CO2 normal
Difficult to make decision criteria when extubation.

Tabel 4. Kondisi untuk Early Emergence (11).
Homeostasis Sistemik Homeostasis Otak
Normotermi (>36oC)Normovolemia, normotensi (70 mmHg <MAP<120 mmHg)Hipokapni ringan/Normokapnia (PaCO2 35 mmHg)
Normoglikemia (glukose 4-8 mmol/l)Tidak ada hipoosmoler (285 ± 5 mOsm/kg)Hematokrit > 25%Tidak ada gangguan koagulasi
Metabolisme otak dan aliran darah otak : normalTekanan intrakranial normal diakhir operasiProfilaksis antiepilepsiPosisi kepala head-up adekuatSaraf kranial untuk proteksi jalan nafas intack

Tabel 6. Check-list sebelum dilakukan ekstubasi segera (11):
No Parameter
1.2.3.4.5.6.7.8.
Kesadaran prabedah adekuat Operasi otak terbatasTidak ada laserasi otak yang luas Bukan operasi fossa posterior yang luas yang mengenai saraf IX dan XII Bukan reseksi AVM yang besar (resiko terjadinya edema pascabedah malignan)Temperatur normalOksigenasi normal Kardiovakuler stabil.

Tabel 7. Kondisi sistemik dan serebral yang menyebabkan pasien lambat bangun (11):
Sistemik Serebral
Hipotermi (<35,5oC)Hipertensi (tekanan sistolik > 150 mmHg)Hipotensi-hipovolemiaHematokrit < 25%Hipoksia atau hiperkapniaNafas spontan tidak efektifHipoosmoler < 280 mOsm/kg)Gangguan koagulasiAda residu obat pelumpuh otot
Perubahan kesadaran prabedahReseksi tumor besar dengan mid line shiftOperasi > 6 jamAda pembengkakan otak selama operasiCedera pada saraf IX, X, XIIKejang saat bangun dari anestesi

Postoperative periode
Avoid coughing, bucking, stretching, increase BP.
Neurological evaluation immediately.
Mostly extubated at OR
Lidocaine 1,5 mg/kg, dexmedetomidine, vasodilator, esmolol to avoid increase BP.
Analgetics : avoid ketorolac

Summary
1. Avoiding secondary brain injury will decrease morbidity and mortality.
2. Choice of anesthetics and technique of anesthesia will improve outcome.
3. knowledge neurophysiology and neuropharmacology fully help in patient management.

Tatang Bisri, 2005