Embed Size (px)
DESCRIPTION
Benign Thyroid Diseases. History. Goiter Fist described in China in 2700 BC Thyroid Function Da Vinci – thyroid is designed to fill empty spaces in the neck Parry – thyroid works as a buffer to protect the brain from surges in blood flow - PowerPoint PPT Presentation
Citation preview

Benign Thyroid Benign Thyroid DiseasesDiseases

HistoryHistory GoiterGoiter
– Fist described in China in 2700 BCFist described in China in 2700 BC
Thyroid FunctionThyroid Function– Da Vinci – thyroid is designed to fill empty spaces in the Da Vinci – thyroid is designed to fill empty spaces in the
neckneck– Parry – thyroid works as a buffer to protect the brain Parry – thyroid works as a buffer to protect the brain
from surges in blood flowfrom surges in blood flow– Roman physicians – thyroid enlargement is a sign of Roman physicians – thyroid enlargement is a sign of
pubertypuberty
CuresCures– ““application of toad’s blood to the neck” application of toad’s blood to the neck” – ““stroking of the thyroid gland with a cadaverous hand”stroking of the thyroid gland with a cadaverous hand”

Surgical advancesSurgical advances 500 AD500 AD
– Abdul Kasan Kelebis Abis performed the first goiter excision in Abdul Kasan Kelebis Abis performed the first goiter excision in Baghdad.Baghdad.
– Procedure: unknownProcedure: unknown 1200’s AD1200’s AD
– Advancements in goiter procedures included applying hot irons Advancements in goiter procedures included applying hot irons through the skin and slowly withdrawing them at right angles. through the skin and slowly withdrawing them at right angles. The remaining mass or pedicled tissue was excised.The remaining mass or pedicled tissue was excised.
– Patients were tied to the table and held down to prevent Patients were tied to the table and held down to prevent unwanted movement.unwanted movement.
– Most died from hemorhage or sepsisMost died from hemorhage or sepsis.. 1646 AD1646 AD
– Wilhelm Fabricus performed a thyroidectomy with standard Wilhelm Fabricus performed a thyroidectomy with standard surgical scalpels.surgical scalpels.
– The 10 y/o girl died, and he was imprisonedThe 10 y/o girl died, and he was imprisoned 1808 AD1808 AD
– Guillaume Dupuytren performed a total thyroidectomy.Guillaume Dupuytren performed a total thyroidectomy.– The patient died postoperatively of “shockThe patient died postoperatively of “shock””

Surgical advancesSurgical advances
18661866
– ““If a surgeon should be so foolhardy as to If a surgeon should be so foolhardy as to undertake it [thyroidectomy] … every step of undertake it [thyroidectomy] … every step of the way will be environed with difficulty, every the way will be environed with difficulty, every stroke of his knife will be followed by a torrent stroke of his knife will be followed by a torrent of blood, and lucky will it be for him if his of blood, and lucky will it be for him if his victim lives long enough to enable him to finish victim lives long enough to enable him to finish his horrid butchery.” his horrid butchery.”
– – Samuel David GrossSamuel David Gross

Surgical advancesSurgical advances
18831883
Kocher’s performs a retrospective reviewKocher’s performs a retrospective review 5000 career thyroidectomies5000 career thyroidectomies Mortality rates decreasedMortality rates decreased
– 40% in 1850 (pre-Kocher & Bilroth)40% in 1850 (pre-Kocher & Bilroth)– 12.6% in 1870’s (Kocher begins practice)12.6% in 1870’s (Kocher begins practice)– 0.2% in 1898 (end of Kocher’s career)0.2% in 1898 (end of Kocher’s career)
Many patients developed cretinism or myxedemaMany patients developed cretinism or myxedema
His conclusions ….His conclusions ….

Surgical advancesSurgical advances
In presentation to the German Surgical In presentation to the German Surgical Congress …Congress …
“ … “ …the thyroid gland in fact had a the thyroid gland in fact had a function….”function….”
- Theodor Kocher, - Theodor Kocher, 18831883

Medical AdvancesMedical Advances
1820 AD1820 AD– Johann Straub and Francois Coindet found that Johann Straub and Francois Coindet found that
use of seaweed (iodine) reduced goiter size use of seaweed (iodine) reduced goiter size and vascularityand vascularity
1830 AD1830 AD– Graves and von Basedow describe a toxic Graves and von Basedow describe a toxic
goiter condition they referred to as “Merseburg goiter condition they referred to as “Merseburg Triad” – goiter, exopthalmos, palpitations.Triad” – goiter, exopthalmos, palpitations.

Thyroid PhysiologyThyroid Physiology

Iodine transportIodine transport
NaNa++/I/I-- symport symport protein controls protein controls serum Iserum I-- uptake uptake
Based on NaBased on Na++/K/K++ antiport potentialantiport potential
Stimulated by TSHStimulated by TSH
Inhibited by Inhibited by PerchloratePerchlorate

Thyroid hormone formationThyroid hormone formation Thyroid Peroxidase (TPO)Thyroid Peroxidase (TPO)
– Apical membrane proteinApical membrane protein– Catalyzes Iodine organification to tyrosine Catalyzes Iodine organification to tyrosine
residues of thyroglobulinresidues of thyroglobulin– Antagonized by methimazole, PTUAntagonized by methimazole, PTU
Iodine coupled to ThyroglobulinIodine coupled to Thyroglobulin– Monoiodotyrosine (Tg + one IMonoiodotyrosine (Tg + one I--))– Diiodotyrosine (Tg + two IDiiodotyrosine (Tg + two I--))
Pre-hormones secreted into follicular Pre-hormones secreted into follicular spacespace


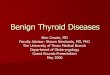
Wolff-Chaikoff EffectWolff-Chaikoff Effect
Increasing doses of IIncreasing doses of I-- increase hormone increase hormone synthesis initiallysynthesis initially
Higher doses cause Higher doses cause cessation of hormone cessation of hormone formation.formation.
This effect is countered This effect is countered by the Iodide leak from by the Iodide leak from normal thyroid tissue.normal thyroid tissue.
Patients with Patients with autoimmune thyroiditis autoimmune thyroiditis may fail to adapt and may fail to adapt and become become hypohypothyroid.thyroid.

Jod-Basedow EffectJod-Basedow Effect Opposite of the Wolff-Chaikoff effectOpposite of the Wolff-Chaikoff effect Excessive iodine loads induce Excessive iodine loads induce hyperhyperthyroidismthyroidism Observed in hyperthyroid disease processesObserved in hyperthyroid disease processes
– Graves’ diseaseGraves’ disease– Toxic multinodular goiterToxic multinodular goiter– Toxic adenomaToxic adenoma
This effect may lead to symptomatic This effect may lead to symptomatic thyrotoxicosis in patients who receive large thyrotoxicosis in patients who receive large iodine doses fromiodine doses from– Dietary changes Dietary changes – Contrast administrationContrast administration– Iodine containing medication (Amiodarone)Iodine containing medication (Amiodarone)

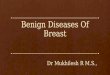
Thyroid Hormone ControlThyroid Hormone Control

TRHTRH
Produced by HypothalamusProduced by Hypothalamus Release is pulsatile, circadianRelease is pulsatile, circadian Downregulated by TDownregulated by T33
Travels through portal venous Travels through portal venous system to adenohypophysissystem to adenohypophysis
Stimulates TSH formationStimulates TSH formation

TSHTSH
Produced by Adenohypophysis ThyrotrophsProduced by Adenohypophysis Thyrotrophs Upregulated by TRH Upregulated by TRH Downregulated by TDownregulated by T44, T, T33
Travels through portal venous system to Travels through portal venous system to cavernous sinus, body.cavernous sinus, body.
Stimulates several processesStimulates several processes– Iodine uptakeIodine uptake– Colloid endocytosisColloid endocytosis– Growth of thyroid gland Growth of thyroid gland

TSH ResponseTSH Response

Thyroid HormoneThyroid Hormone Majority of circulating hormone is TMajority of circulating hormone is T44
– 98.5% T98.5% T44– 1.5% T1.5% T33
Total Hormone load is influenced by serum Total Hormone load is influenced by serum binding proteinsbinding proteins– Albumin 15%Albumin 15%– Thyroid Binding Globulin 70%Thyroid Binding Globulin 70%– Transthyretin 10%Transthyretin 10%
Regulation is based on the free component of Regulation is based on the free component of thyroid hormonethyroid hormone

Hormone Binding FactorsHormone Binding Factors
Increased TBGIncreased TBG– High estrogen states (pregnancy, OCP, HRT, High estrogen states (pregnancy, OCP, HRT,
Tamoxifen)Tamoxifen)– Liver disease (early)Liver disease (early)
Decreased TBGDecreased TBG– Androgens or anabolic steroidsAndrogens or anabolic steroids– Liver disease (late)Liver disease (late)
Binding Site CompetitionBinding Site Competition– NSAID’sNSAID’s– Furosemide IVFurosemide IV– Anticonvulsants (Phenytoin, Carbamazepine)Anticonvulsants (Phenytoin, Carbamazepine)

Thyroid EvaluationThyroid Evaluation
TRHTRH TSHTSH Total TTotal T33, T, T44
Free TFree T33, T, T44
RAIURAIU ThyroglobulinThyroglobulin Antibodies: Anti-TPO, Anti-TSHrAntibodies: Anti-TPO, Anti-TSHr

Thyroid EvaluationThyroid Evaluation

RAIURAIU Scintillation counter measures radioactivity after Scintillation counter measures radioactivity after
II123123 administration. administration. Uptake varies greatly by iodine statusUptake varies greatly by iodine status
– Indigenous diet (normal uptake 10% vs. 90%)Indigenous diet (normal uptake 10% vs. 90%)– Amiodarone, Contrast study, Topical betadineAmiodarone, Contrast study, Topical betadine
Elevated RAIU with hyperthyroid symptomsElevated RAIU with hyperthyroid symptoms– Graves’Graves’– Toxic goiterToxic goiter
Low RAIU with hyperthyroid symptomsLow RAIU with hyperthyroid symptoms– Thyroiditis (Subacute, Active Hashimoto’s)Thyroiditis (Subacute, Active Hashimoto’s)– Hormone ingestion (Thyrotoxicosis factitia, Hamburger Hormone ingestion (Thyrotoxicosis factitia, Hamburger
Thyrotoxicosis)Thyrotoxicosis)– Excess IExcess I-- intake in Graves’ (Jod-Basedow effect) intake in Graves’ (Jod-Basedow effect)– Ectopic thyroid carcinoma (Struma ovarii)Ectopic thyroid carcinoma (Struma ovarii)

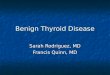
Iodine statesIodine states
Normal ThyroidNormal Thyroid
Inactive ThyroidInactive Thyroid
Hyperactive ThyroidHyperactive Thyroid

Common Thyroid Common Thyroid DisordersDisorders

GoiterGoiter GoiterGoiter: Chronic enlargement of the thyroid gland : Chronic enlargement of the thyroid gland
not due to neoplasmnot due to neoplasm Endemic goiterEndemic goiter
– Areas where > 5% of children 6-12 years of age have Areas where > 5% of children 6-12 years of age have goitergoiter
– Common in China and central AfricaCommon in China and central Africa Sporadic goiter Sporadic goiter
– Areas where < 5% of children 6-12 years of age have Areas where < 5% of children 6-12 years of age have goitergoiter
– MultinodularMultinodular goitergoiter in sporatic areas often denotes the in sporatic areas often denotes the presence of multiple nodules rather than gross gland presence of multiple nodules rather than gross gland enlargementenlargement
FamilialFamilial

GoiterGoiter EtiologyEtiology
– Hashimoto’s thyroiditis Hashimoto’s thyroiditis Early stages only, late stages show atrophic changesEarly stages only, late stages show atrophic changes May present with hypo, hyper, or euthyroid statesMay present with hypo, hyper, or euthyroid states
– Graves’ diseaseGraves’ disease Due to chronic stimulation of TSH receptorDue to chronic stimulation of TSH receptor
– Diet Diet Brassica (cabbage, turnips, cauliflower, broccoli)Brassica (cabbage, turnips, cauliflower, broccoli) CassavaCassava
– Chronic Iodine excessChronic Iodine excess Iodine excess leads to increased colloid formation and can prevent Iodine excess leads to increased colloid formation and can prevent
hormone releasehormone release If a patient does not develop iodine leak, excess iodine can lead to If a patient does not develop iodine leak, excess iodine can lead to
goitergoiter– MedicationsMedications
Lithium prevents release of hormone, causes goiter in 6% of chronic Lithium prevents release of hormone, causes goiter in 6% of chronic usersusers
– NeoplasmNeoplasm

GoiterGoiter Pathogenesis Pathogenesis
– Iodine deficient areasIodine deficient areas Heterogeneous response to TSHHeterogeneous response to TSH Chronic stimulation leads to multiple nodulesChronic stimulation leads to multiple nodules
– Iodine replete areas Iodine replete areas Thyroid follicles are heterogeneous in their growth and Thyroid follicles are heterogeneous in their growth and
activity potentialactivity potential Autopsy series show MNG >30%.Autopsy series show MNG >30%.
Thyroid function evaluationThyroid function evaluation– TSH, T4, T3TSH, T4, T3– Overt hyperthyroidism (TSH low, T3/T4 high)Overt hyperthyroidism (TSH low, T3/T4 high)– Subclinical hyperthyroidism (TSH low, T3/T4 normal)Subclinical hyperthyroidism (TSH low, T3/T4 normal)
Determination of thyroid state is key in determining Determination of thyroid state is key in determining treatmenttreatment

Non-Toxic GoiterNon-Toxic Goiter
Cancer screening in non-toxic MNGCancer screening in non-toxic MNG– Longstanding MNG has a risk of malignancy identical to Longstanding MNG has a risk of malignancy identical to
solitary nodules (<5%)solitary nodules (<5%)– MNG with nodules < 1.5 cm may be followed clinicallyMNG with nodules < 1.5 cm may be followed clinically– MNG with non-functioning nodules > 4cm should be MNG with non-functioning nodules > 4cm should be
excisedexcised No FNA needed due to poor sensitivityNo FNA needed due to poor sensitivity Incidence of cancer (up to 40%)Incidence of cancer (up to 40%)
– FNA in MNGFNA in MNG Sensitivity 85% - 95%Sensitivity 85% - 95% Specificity 95%Specificity 95% Negative FNA can be followed with annual USNegative FNA can be followed with annual US Insufficient FNA’s should be repeatedInsufficient FNA’s should be repeated Incoclusive FNA or papillary cytology warrants excisionIncoclusive FNA or papillary cytology warrants excision
– Hyperfunctioning nodules may mimic follicular neoplasm Hyperfunctioning nodules may mimic follicular neoplasm on on FNAFNA

Non-Toxic GoiterNon-Toxic Goiter Treatment options Treatment options (no compressive symptoms)(no compressive symptoms)
– US follow-up to monitor for progressionUS follow-up to monitor for progression
– Thyroid suppression therapyThyroid suppression therapy May be used for progressive growthMay be used for progressive growth May reduce gland volume up to 50%May reduce gland volume up to 50% Goiter regrowth occurs rapidly following therapy cessationGoiter regrowth occurs rapidly following therapy cessation
– SurgerySurgery Suspicious neck lymphadenopathySuspicious neck lymphadenopathy History of radiation to the cervical regionHistory of radiation to the cervical region Rapid enlargement of nodulesRapid enlargement of nodules Papillary histologyPapillary histology Microfollicular histology (?)Microfollicular histology (?)

Non-Toxic GoiterNon-Toxic Goiter
Treatment options Treatment options (compressive symptoms)(compressive symptoms)
– RAI ablationRAI ablation Volume reduction 33% - 66% in 80% of patientsVolume reduction 33% - 66% in 80% of patients Improvement of dysphagia or dyspnea in 70% - 90%Improvement of dysphagia or dyspnea in 70% - 90% Post RAI hypothyroidism 60% in 8 yearsPost RAI hypothyroidism 60% in 8 years Post RAI Graves’ disease 10%Post RAI Graves’ disease 10% Post RAI lifetime cancer risk 1.6%Post RAI lifetime cancer risk 1.6%
– SurgerySurgery Most commonly recommended treatment for healthy Most commonly recommended treatment for healthy
individualsindividuals

Toxic GoiterToxic Goiter Evaluate forEvaluate for
– Graves’ disease Graves’ disease Clinical findings (Pretibial myxedema, Opthalmopathy)Clinical findings (Pretibial myxedema, Opthalmopathy) Anti-TSH receptor AbAnti-TSH receptor Ab High RAUIHigh RAUI
– ThyroiditisThyroiditis Clinical findings (painful thyroid in Subacute thyroiditis)Clinical findings (painful thyroid in Subacute thyroiditis) Low RAUILow RAUI
– Recent Iodine administrationRecent Iodine administration AmiodaroneAmiodarone IV contrastIV contrast Change in dietChange in diet
FNA evaluationFNA evaluation– Not indicated in hyperthyroid nodules due to low incidence of Not indicated in hyperthyroid nodules due to low incidence of
malignancymalignancy– FNA of hyperthyroid nodules can mimic follicular neoplasmsFNA of hyperthyroid nodules can mimic follicular neoplasms

Toxic GoiterToxic Goiter Risks of hyperthyroidism Risks of hyperthyroidism
– Atrial fibrillationAtrial fibrillation– Congestive Heart FailureCongestive Heart Failure– Loss of bone mineral densityLoss of bone mineral density– Risks exist for both clinical or subclinical diseaseRisks exist for both clinical or subclinical disease
Toxic GoiterToxic Goiter– Toxicity is usually longstandingToxicity is usually longstanding– Acute toxicity may occur in hyperthyroid states (Jod Acute toxicity may occur in hyperthyroid states (Jod
Basedow effect) with Basedow effect) with Relocation to iodine replete areaRelocation to iodine replete area Contrast administrationContrast administration Amiodarone (37% iodine)Amiodarone (37% iodine)

Toxic GoiterToxic Goiter Treatment for Toxic MNGTreatment for Toxic MNG
– Thionamide medicationsThionamide medications Not indicated for long-term use due to complicationsNot indicated for long-term use due to complications May be used for symptomatic individuals until definitive May be used for symptomatic individuals until definitive
treatmenttreatment..– RadioiodineRadioiodine
Primary treatment for toxic MNGPrimary treatment for toxic MNG Large ILarge I131131 dose required due to gland size dose required due to gland size Goiter size reduction by 40% within 1 yearGoiter size reduction by 40% within 1 year Risk of hypothyroidismRisk of hypothyroidism 11% - 24% 11% - 24% May require second doseMay require second dose
– SurgerySurgery Used for compressive symptomsUsed for compressive symptoms Hypothyroidism occurs in up to 70% of subtotal Hypothyroidism occurs in up to 70% of subtotal
thyroidectomy patientsthyroidectomy patients Pre-surgical stabilization with thionamide medicationsPre-surgical stabilization with thionamide medications Avoid SSKI due to risk for acute toxic symptomsAvoid SSKI due to risk for acute toxic symptoms

Graves’ DiseaseGraves’ Disease
Most common cause of thyrotoxicosis in the industrialized Most common cause of thyrotoxicosis in the industrialized worldworld
Autoimmune condition with anti-TSHr antibodiesAutoimmune condition with anti-TSHr antibodies Onset of disease may be related to severe stress which Onset of disease may be related to severe stress which
alters the immune responsealters the immune response DiagnosisDiagnosis
– TSH, TTSH, T44, T, T33 to establish toxicosis to establish toxicosis– RAIU scan to differentiate toxic conditionsRAIU scan to differentiate toxic conditions– Anti-TPO, Anti-TSAb, fTAnti-TPO, Anti-TSAb, fT33 if indicated if indicated
RAIU in Hyperthyroid StatesRAIU in Hyperthyroid StatesHigh UptakeHigh Uptake Low UptakeLow Uptake
Graves’Graves’ Subacute ThyroiditisSubacute Thyroiditis
Toxic MNGToxic MNG Iodine ToxicosisIodine Toxicosis
Toxic AdenomaToxic Adenoma Thyrotoxicosis factitiaThyrotoxicosis factitia

Graves’ DiseaseGraves’ Disease TreatmentTreatment
– Beta blockers for symptomsBeta blockers for symptoms
– Thionamide medicationsThionamide medications May re-establish euthyroidism in 6-8 weeksMay re-establish euthyroidism in 6-8 weeks 40% - 60% incidence of disease remission40% - 60% incidence of disease remission 20% incidence of allergy (rash, itching)20% incidence of allergy (rash, itching) 0.5% incidence of potentially fatal agranulocytosis0.5% incidence of potentially fatal agranulocytosis
– Radioiodine ablationRadioiodine ablation 10% incidence of hypothyroidism at 1 year10% incidence of hypothyroidism at 1 year 55% - 75% incidence of hypothyroidism at 10 years55% - 75% incidence of hypothyroidism at 10 years Avoid RAI in children and pregancy Avoid RAI in children and pregancy
– SurgerySurgery Large goiters not amenable to RAILarge goiters not amenable to RAI Compressive symptomsCompressive symptoms Children, pregnancyChildren, pregnancy 50% - 60% incidence of hypothyroidism50% - 60% incidence of hypothyroidism

Toxic AdenomaToxic Adenoma ThyrotoxicosisThyrotoxicosis
– Hyperfunctioning nodules <2 cm rarely lead to Hyperfunctioning nodules <2 cm rarely lead to thyrotoxicosisthyrotoxicosis
– Most nodules leading to thyrotoxicosis are >3 Most nodules leading to thyrotoxicosis are >3 cm.cm.
Treatment IndicationsTreatment Indications– Post-menopausal femalePost-menopausal female
Due to increased risk of bone lossDue to increased risk of bone loss– Patients over 60 Patients over 60
Due to high risk of atrial fibrillationDue to high risk of atrial fibrillation– Adenomas greater than 3 cm (?)Adenomas greater than 3 cm (?)

Toxic AdenomaToxic Adenoma TreatmentsTreatments
– Antithyroid medicationsAntithyroid medications Not used due to complications of long-term treatmentNot used due to complications of long-term treatment
– RadioiodineRadioiodine Cure rate > 80% (20 mCi I131)Cure rate > 80% (20 mCi I131) Hypothyroidism risk 5% - 10%Hypothyroidism risk 5% - 10% Second dose of I131 needed in 10% - 20%Second dose of I131 needed in 10% - 20% Patients who are symptomatically toxic may require control Patients who are symptomatically toxic may require control
with thionamide medications before RAI to reduce risk of with thionamide medications before RAI to reduce risk of worsening toxicity.worsening toxicity.
– SurgerySurgery Preferred for children and adolescentsPreferred for children and adolescents Preferred for very large nodules when high I131 doses Preferred for very large nodules when high I131 doses
neededneeded Low risk of hypothyroidismLow risk of hypothyroidism
– Ethanol InjectionEthanol Injection Rarely done in the USRarely done in the US May achieve cure in 80%May achieve cure in 80%

HypothyroidismHypothyroidism
Symptoms – fatigability, coldness, weight gain, Symptoms – fatigability, coldness, weight gain, constipation, low voiceconstipation, low voice
Signs – Cool skin, dry skin, swelling of Signs – Cool skin, dry skin, swelling of face/hands/legs, slow reflexes, myxedemaface/hands/legs, slow reflexes, myxedema
Newborn – Retardation, short stature, swelling Newborn – Retardation, short stature, swelling of face/hands, possible deafnessof face/hands, possible deafness
Types of HypothyroidismTypes of Hypothyroidism– Primary – Thyroid gland failurePrimary – Thyroid gland failure– Secondary – Pituitary failureSecondary – Pituitary failure– Tertiary – Hypothalamic failureTertiary – Hypothalamic failure– Peripheral resistancePeripheral resistance

HypothyroidismHypothyroidism
Cause is determined by geographyCause is determined by geography– Hashimoto’s in industrialized countriesHashimoto’s in industrialized countries– May be due to iodine excess in some costal areasMay be due to iodine excess in some costal areas
DiagnosisDiagnosis– Low FTLow FT44, High TSH (Primary, check for antibodies), High TSH (Primary, check for antibodies)
– Low FTLow FT44, Low TSH (Secondary or Tertiary, TRH , Low TSH (Secondary or Tertiary, TRH
stimulation test, MRI)stimulation test, MRI) TreatmentTreatment
– Levothyroxine (TLevothyroxine (T44) due to longer half life) due to longer half life– Treatment prevents bone loss, cardiomyopathy, Treatment prevents bone loss, cardiomyopathy,
myxedemamyxedema

HypothyroidismHypothyroidism AgenesisAgenesis Thyroid destructionThyroid destruction
– Hashimoto’s thyroiditisHashimoto’s thyroiditis– SurgerySurgery– II131131 ablation ablation– Infiltrative diseasesInfiltrative diseases– Post-laryngectomyPost-laryngectomy
Inhibition of functionInhibition of function– Iodine deficiencyIodine deficiency– Iodine administrationIodine administration– Anti-thyroid medications (PTU, Methimazole, Lithium, Anti-thyroid medications (PTU, Methimazole, Lithium,
Interferon)Interferon)– Inherited defectsInherited defects
TransientTransient– PostpartumPostpartum– ThyroiditisThyroiditis

Hashimoto’sHashimoto’s(Chronic, Lymphocytic)(Chronic, Lymphocytic)
Most common cause of hypothyroidismMost common cause of hypothyroidism Result of antibodies to TPO, TBGResult of antibodies to TPO, TBG Commonly presents in females 30-50 yrs.Commonly presents in females 30-50 yrs. Usually non-tender and asymptomaticUsually non-tender and asymptomatic Lab valuesLab values
– High TSHHigh TSH
– Low TLow T44
– Anti-TPO AbAnti-TPO Ab– Anti-TBG AbAnti-TBG Ab
Treat with LevothyroxineTreat with Levothyroxine

ThyroiditisThyroiditis

Hashimoto’s ThyroiditisHashimoto’s Thyroiditis Most common cause of goiter and hypothyroidism in the U.S.Most common cause of goiter and hypothyroidism in the U.S. PhysicalPhysical
– Painless diffuse goiterPainless diffuse goiter Lab studiesLab studies
– HypothyroidismHypothyroidism– Anti TPO antibodies (90%)Anti TPO antibodies (90%)– Anti Thyroglobulin antibodies (20-50%)Anti Thyroglobulin antibodies (20-50%)– Acute Hyperthyroidism (5%)Acute Hyperthyroidism (5%)
TreatmentTreatment– Levothyroxine if hypothyroidLevothyroxine if hypothyroid– Triiodothyronine (for myxedema coma)Triiodothyronine (for myxedema coma)– Thyroid suppression (levothyroxine) to decrease goiter sizeThyroid suppression (levothyroxine) to decrease goiter size
ContraindicationsContraindications Stop therapy if no resolution notedStop therapy if no resolution noted
– Surgery for compression or pain.Surgery for compression or pain.

Silent ThyroiditisSilent ThyroiditisPost-partum ThyroiditisPost-partum Thyroiditis
Silent thyroiditis is termed post-partum thyroiditis if it Silent thyroiditis is termed post-partum thyroiditis if it occurs within one year of delivery.occurs within one year of delivery.
ClinicalClinical– Hyperthyroid symptoms at presentationHyperthyroid symptoms at presentation– Progression to euthyroidism followed by hypothyroidism for up Progression to euthyroidism followed by hypothyroidism for up
to 1 year.to 1 year.– Hypothyroidism generally resolvesHypothyroidism generally resolves
DiagnosisDiagnosis– May be confused with post-partum Graves’ relapseMay be confused with post-partum Graves’ relapse
TreatmentTreatment– Beta blockers during toxic phaseBeta blockers during toxic phase– No anti-thyroid medication indicatedNo anti-thyroid medication indicated– Iopanoic acid (Telopaque) for severe hyperthyroidismIopanoic acid (Telopaque) for severe hyperthyroidism– Thyroid hormone during hypothyroid phase. Must withdraw in Thyroid hormone during hypothyroid phase. Must withdraw in
6 months to check for resolution.6 months to check for resolution.

Subacute ThyroiditisSubacute ThyroiditisDeQuervain’s, GranulomatousDeQuervain’s, Granulomatous
Most common cause of Most common cause of painful thyroiditispainful thyroiditis
Often follows a URIOften follows a URI FNA may reveal FNA may reveal
multinuleated giant cells or multinuleated giant cells or granulomatous change.granulomatous change.
CourseCourse– Pain and thyrotoxicosis (3-Pain and thyrotoxicosis (3-
6 weeks)6 weeks)– Asymptomatic Asymptomatic
euthyroidismeuthyroidism– Hypothyroid period (weeks Hypothyroid period (weeks
to months)to months)– Recovery (complete in Recovery (complete in
95% after 4-6 months)95% after 4-6 months)

Subacute ThyroiditisSubacute ThyroiditisDeQuervain’s, GranulomatousDeQuervain’s, Granulomatous
DiagnosisDiagnosis– Elevated ESRElevated ESR– Anemia (normochromic, normocytic)Anemia (normochromic, normocytic)– Low TSH, Elevated T4 > T3, Low anti-TPO/TgbLow TSH, Elevated T4 > T3, Low anti-TPO/Tgb– Low RAI uptake (same as silent thyroiditis)Low RAI uptake (same as silent thyroiditis)
TreatmentTreatment– NSAID’s and salicylates.NSAID’s and salicylates.– Oral steroids in severe casesOral steroids in severe cases– Beta blockers for symptoms of hyperthyroidism, Iopanoic acid Beta blockers for symptoms of hyperthyroidism, Iopanoic acid
for severe symptomsfor severe symptoms– PTU not indicated since excess hormone results from leak PTU not indicated since excess hormone results from leak
instead of hyperfunctioninstead of hyperfunction– Symptoms can recur requiring repeat treatmentSymptoms can recur requiring repeat treatment– Graves’ disease may occasionally develop as a late sequellaeGraves’ disease may occasionally develop as a late sequellae

Acute ThyroiditisAcute Thyroiditis CausesCauses
– 68% Bacterial (S. aureus, S. pyogenes)68% Bacterial (S. aureus, S. pyogenes)– 15% Fungal15% Fungal– 9% Mycobacterial9% Mycobacterial
May occur secondary toMay occur secondary to– Pyriform sinus fistulaePyriform sinus fistulae– Pharyngeal space infectionsPharyngeal space infections– Persistent Thyroglossal remnantsPersistent Thyroglossal remnants– Thyroid surgery wound infections (rare)Thyroid surgery wound infections (rare)
More common in HIVMore common in HIV

Acute ThyroiditisAcute Thyroiditis DiagnosisDiagnosis
– Warm, tender, enlarged thyroidWarm, tender, enlarged thyroid– FNA to drain abscess, obtain cultureFNA to drain abscess, obtain culture– RAIU normal (versus decreased in DeQuervain’s)RAIU normal (versus decreased in DeQuervain’s)– CT or US if infected TGDC suspectedCT or US if infected TGDC suspected
TreatmentTreatment– High mortality without prompt treatmentHigh mortality without prompt treatment– IV Antibiotics IV Antibiotics
Nafcillin / Gentamycin or Rocephin for empiric therapyNafcillin / Gentamycin or Rocephin for empiric therapy– Search for pyriform fistulae (BA swallow, endoscopy)Search for pyriform fistulae (BA swallow, endoscopy)– Recovery is usually completeRecovery is usually complete

Riedel’s ThyroiditisRiedel’s Thyroiditis Rare disease involving fibrosis of the thyroid glandRare disease involving fibrosis of the thyroid gland
DiagnosisDiagnosis– Thyroid antibodies are present in 2/3Thyroid antibodies are present in 2/3– Painless goiter “woody”Painless goiter “woody”– Open biopsy often needed to diagnoseOpen biopsy often needed to diagnose– Associated with focal sclerosis syndromes Associated with focal sclerosis syndromes
(retroperitoneal, mediastinal, retroorbital, and sclerosing (retroperitoneal, mediastinal, retroorbital, and sclerosing cholangitis)cholangitis)
TreatmentTreatment– Resection for compressive symptomsResection for compressive symptoms– Chemotherapy with Tamoxifen, Methotrexate, or steroids Chemotherapy with Tamoxifen, Methotrexate, or steroids
may be effectivemay be effective– Thyroid hormone only for symptoms of hypothyroidismThyroid hormone only for symptoms of hypothyroidism