Embed Size (px)
Citation preview
Bermuda Health Strategy SymposiumBermuda Underwater Exploration Institute
16th Jan 2016 . 8:30am - 12:00pm

2

8:30 am Breakfast and Registration9:00 am Opening Remarks Chairman, Bermuda Medical Council Master of Ceremonies - Dr George Shaw9:05 am Feature Address and Formal OpeningBermuda Health Strategy Minister of Health, Seniors and EnvironmentHon Jeanne J Atherden CA, CPA, JP, MP9:20 am Bermuda Health Action Plan Acting CEO, Bermuda Health CouncilTawanna Wedderburn9:30 am Reducing Chronic Non-communicable Diseases Dr Cheryl Peek-Ball9:40 am Quality and sustainability through modernization and innovation Chief of Staff, BHBDr Michael Weitekamp9:50 am Insurance coverage access initiatives Clinical Care Manager Consultant, HIDDiana Liacos10:00 am Care Quality initiatives Acting CEO, Bermuda Health CouncilTawanna Wedderburn10:10 am Questions and Comments (about initiatives) Chairman, Bermuda Medical Council Master of Ceremonies - Dr George Shaw10:30 am BREAK10:45 am Panel Session:• Provider perspectives on cost savings Chief of General & Family Medicine, KEMHDr Fiona Ross• Insurance perspectives on quality/costs Executive Vice President, Group Insurance, ArgusMichelle Jackson• NGOs perspectives on care and affordability Executive Director, The Family CentreMartha Dismont• Public health and health promotion perspectives Director, Department of HealthDavid Kendell11:00 am Panel discussion Chairman, Bermuda Medical CouncilModerator - Dr George Shaw11:50 am Closing remarks and next steps Minister of Health, Seniors and EnvironmentHon Jeanne J Atherden JP, MP, CA, CPA12:00 pm Lunch on participant's own: 10% discount offered at Harbourfront Restaurant3
4
5
1
BERMUDAHEALTHREFORMSTRATEGY2014‐ 2019FromVisiontoAction
The Hon. Jeanne J. Atherden, CA, CPA, JP, MP
16th January 2016
OurVision:“HealthyPeopleinHealthyCommunities”
FromVisiontoAction
Vision • Health Reform Strategy
Action • Health Action Plan(s)
Results • Measured outcomes
ComplementaryStrategiestotacklevarioushealthsystemcomponents
Health Reform Strategy
DOH Strategic Plan
Bermuda Health Action
Plan
BHB Modernization
Plan
Well BermudaPAHO/MOH
Biennial Work Plan
Mental Health Plan
BMDA Cost Containment
Plan
Ageing Plan
HealthReformStrategy
What
WhyHow
Healthsystemcomponents
2
BermudaHealthStrategyOverview
VISIONHealthy People in Healthy
Communities
MISSIONTo provide affordable and sustainable healthcare for
all Bermuda residents
COREVALUESQuality
Equity
Sustainability
GOALS14 health sector goals address
specific deficiencies in the health system that lead to high cost and
poor value
REFORM
FocusonQuality
Right Care
Right Time
Right Setting
Best Value
The14GoalsoftheReformStrategy
EquitableAccess
QualityStandards
Sustainability&Efficiency
• 1. Access to basic insurance• 2. Smarter basic coverage• 3. Affordable contributions• 4. Appropriate overseas care
• 5. Pay for quality• 6. Electronic health record• 7. Address Long Term Care• 8. Standards of care
• 9. Financing efficiency• 10. Regulate health technology• 11. More health promotion• 12. Coordinate healthcare delivery• 13. Tackle NDCs• 14. Subsidize the vulnerable
GovernanceStructure
Lead Agencies
Develop Action Plans Consult stakeholders Implement initiatives
Bermuda Health Council
Coordinates Action Plan Development Assures Consultation Drives Strategy
Ministry of Health, Seniors and Environment
Sets Strategy & Approves Action Plans Communicates Updates & Progress
THANKYOU
1
Bermuda Health Action Plan 2014 - 2019
Tawanna WedderburnActing Chief Executive Officer
16th January 2016Presentation for Bermuda Health Strategy Symposium
Overview
About the Action Plan
1. Quality Care
2. Collaboration
Action Plan Goals
Capacity Building
Systems Strengthening
Disease Control & Prevention
About the Action Plan – Quality Care
Chronic kidney disease
Asthma
Diabetes
Hypertension
Heart disease
Other NCDs
About the Action Plan ‐ Collaboration
Residents
Providers
&
Professionals
Health Agencies
Regulators Solution
Action Plan Goals
Systems strengthening
Disease control & prevention
Capacity building
Goal # 1 – Capacity Building
System strengthening
Disease control & prevention
Capacity building
2
Capacity building
Strengthen and develop human resources (5 actions)
• Maintaining independence as we age (BHB, ADS)
Long‐term care
• Medical workforce planning (OCMO)
• Enhancing registration and complaints handling (OCMO)
Health Professionals
• Enhancing business practices and facility standards (BHeC)
Health Providers
Goal #2 – Systems strengthening
Systems strengthening
Disease control & prevention
Capacity building
Systems strengthening
Improving infrastructure and technology to support quality care (5 actions)
•Financing reforms to achieve insurance coverage for all (BHeC)
•Screening using evidence based clinical guidelines (BHeC)
Care Access
•Ensuring appropriate referrals and testing (BHeC)
•Managing health system planning and technology (BHeC)
•Monitoring population health and implementing UPI (OCMO/BHeC)
Health technology
Goal #3 – Disease Control & Prevention
System strengthening
Disease control & prevention
Capacity building
Disease control & prevention
Effective disease control (10 actions)
Chronic disease registers (OCMO)
Diabetes education (BHB)
Obesity and diabetes rates (DOH)
Disease control & prevention
Effective disease control (10 actions)
Monitoring CKD to prevent progression to ESRD (OCMO/BHeC)
Adding benefits to promote wellness (HID)
Improving access to quality, specialty medical care (BHB)
3
Disease control & prevention
Effective disease control (10 actions)
Post‐acute care programmes (HID)
Primary care pilot (HID)
Reducing NCD risk factors (OCMO/DOH)
Reducing risk factors associated with violence and injuries (DOH)
Summary
Systems strengthening
Disease control & prevention
Capacity building
1
Symposium opportunity
Office of CMO Vision: bird’s eye view and from the trees
PAHO‐WHO priorities and guidance
Office of Chief Medical Office– focus areas
Additional recommendations
Overview
Confirm we all have the same Vision
Answer relevant Question(s): • What are we trying to achieve in the health system?
• What changes are required?
• Are wewilling to make the necessary changes?
• Who’s best positioned to lead the changes?
• What is my role/contribution in the process of change?
Symposium opportunities
2
Bermuda’s Vision: Healthy people in healthy communities
Bermuda’s “…first concerted effort to create a joined-up approach to the promotion of health on our island, and to create a shared vision for health promoters across all sectors.”Well Bermuda: National Health Promotion Strategy, Dept of Health, 2008, 2nd edition.
• 3 Themes: Healthy People, Families and Communities
• 18 health goals, many objectives
• Approx. 40 Well Bermudacommunity partners with Action Plans
Cradle to grave positive health outcomes: low rates of avoidable health complications across life span
Equal access to high quality primary health care
Financial risk protection Optimal social outcomes: eliminate poverty, economic
stability and opportunity, high education rates, full employment, strong family structures, social cohesion, social justice…
(supported by family‐friendly policies addressing the social determinants of health)
Safe, health‐promoting environments
Healthy people in healthy communities
International Guidance: World Health Organization
• NCDs well understood; vast body of knowledge and experience exists to guide steps
• Refers to UN declaration on NCD’s (2012) and urgent need for multi-sectorial policies and plans
• Endorsed by World Health Assembly (2013): roadmap to progress on 9 global NCD targets by 2025
Governments must :• Set NCD targets• Develop multi-sectorial plans to
reduce exposure to risk factors• Measure results
2
“Enjoyment of the highest attainable level of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition” (WHO constitution, 1948)
Universal Health Coverage (UHC):2005WHO member states endorsed UHC as central goal in order to guarantee access to necessary services while providing protection against financial risk
2012 UN General Assembly adopted resolution emphasizing governments’ responsibility to “urgently and significantly scale up efforts to accelerate…transition towards universal access to affordable and quality health‐care services.”
Must: expand priority services, include more people (esp low‐income) and reduce out‐of‐pocket payments
UHC is “single most powerful concept that public health has to offer” (Margaret Chan, WHO Director‐General)
International Guidance…Health for Development
International guidance
NCD Control…5 priority strategies
Forum of Key Stakeholders on NCDs: Advancing the NCD agenda in the Caribbean, Barbados, June 2015 • Universal access to health
• Universal health coverage
• Appropriate human resources for population needs
• Sustainable financing of health system
• Enabling environments
• Health‐promoting public policies
• Multi‐sectorial , collaborative problem‐solving
• Political will
International Guidance (requirements for “Healthy people in healthy communities”)
5 Functional Areas:
1‐ Registration and Regulation of healthcare professionals and healthcare facilities
2‐ Drugs and Pharmaceutical product control– controlled drug monitoring & reporting
3‐ Epidemiology & Surveillance Unit‐ outbreak prevention and control, research, community assessment
4‐ Statutory functions‐ Customs, Burials, SMB, Ex‐officio role on BHB, BMC, BHeC
5‐ Public health focal point for international communications, reporting (PAHO‐WHO, IHR Focal Point) and public health leadership
Office of the Chief Medical Officer
Assure competent health work force (enhancing registration criteria and health workforce planning)
Advocate for health‐promoting policies
o Collaborate with Health Promotion Office (focus on NCD Risk Factor reduction)
Collaboration with providers to assure high clinical care quality and standards in community (adoption of evidence‐based clinical guidelines where possible)
Strengthen Surveillance of NCDs (creation of NCD registers)
OFFICE of CMO focus on NCDs
3
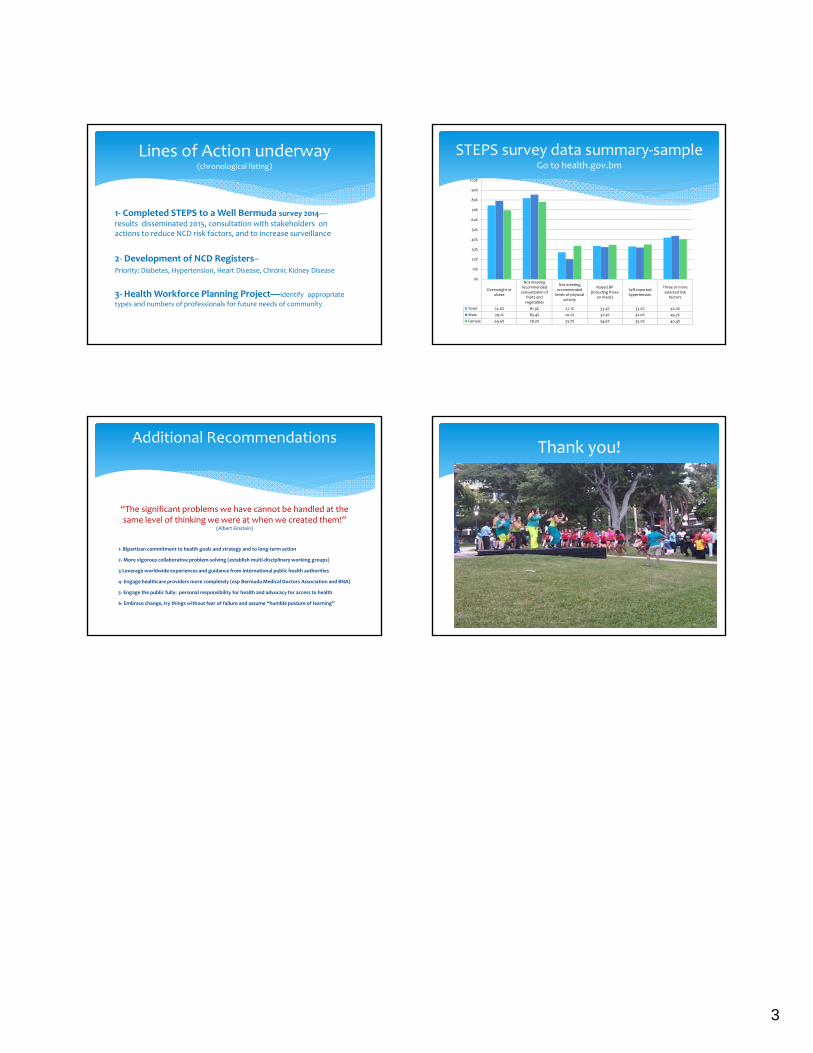
1‐ Completed STEPS to a Well Bermuda survey 2014—results disseminated 2015, consultation with stakeholders on actions to reduce NCD risk factors, and to increase surveillance
2‐ Development of NCD Registers–Priority: Diabetes, Hypertension, Heart Disease, Chronic Kidney Disease
3‐ Health Workforce Planning Project—identify appropriate
types and numbers of professionals for future needs of community
Lines of Action underway(chronological listing)
STEPS survey data summary‐sampleGo to health.gov.bm
Overweight orobese
Not meetingrecommendedconsumption of
fruits andvegetables
Not meetingrecommendedlevels of physical
activity
Raised BP(including those
on meds)
Self‐reportedhypertension
Three or moreselected risk
factors
Total 74.6% 81.9% 27.1% 33.4% 33.0% 42.0%
Male 79.1% 85.4% 20.2% 32.3% 32.0% 43.7%
Female 69.6% 78.0% 33.7% 34.6% 35.0% 40.4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
“The significant problems we have cannot be handled at the same level of thinking we were at when we created them!”
(Albert Einstein)
1‐ Bipartisan commitment to health goals and strategy and to long‐term action
2‐More vigorous collaborative problem‐solving (establish multi‐disciplinary working groups)
3‐Leverage worldwide experiences and guidance from international public health authorities
4‐ Engage healthcare providers more completely (esp Bermuda Medical Doctors Association and BNA)
5‐ Engage the public fully: personal responsibility for health and advocacy for access to health
6‐ Embrace change, try things without fear of failure and assume “humble posture of learning”
Additional RecommendationsThank you!
1
Quality & Sustainability Through Modernization
and Innovation
Bermuda Health Strategy Symposium
16th January 2016Michael R Weitekamp MD, MHA, FACP
Chief of Staff
Bermuda Hospitals Board
By Way of Background
BHB serves as a critical medical and social safety net for Bermuda, each year providing more complex and uncompensated care 24/7
BHB is also a robust component of the economy in its own right, as well as a key component of the enabling infrastructure supporting Bermuda’s international business and tourism
By necessity and strategic intent the current scope of services exceeds legislative mandate of Hospitals Act 1970, but would cause significant disruption and potential harm to the community if curtailed abruptly with no alternatives in place
Healthcare spend is determined by the volume & intensity of services & price
Cost are exacerbated by unwarranted duplication, volume‐based incentives, fragmentation, administrative inefficiency & limited regulation
By Way of Background
90 acute care beds should be more than adequate for population of 65,000
Yet beds are filled too often with patients who have preventable illness and trauma, unstable social supports, psychiatric co‐morbidity, are hospitalized as the default venue, or some combination of all the above
Similar challenge exists at MWI ‐ too often admission is a default and/or discharges are significantly delayed due to a lack of available social, behavioral or forensic resources within the community
Unnecessary hospitalization is bad for your health – risking rapid de‐conditioning, hospital acquired conditions such as infection, adverse drug reactions or falls, and immune suppression contributing to secondary illness after discharge
By Way of Background
Unnecessary hospitalization is also bad for the economy, as the hospital is the most expensive venue in the continuum of healthcare services
When viewed through a holistic lens of population wellness, the opportunity costs of acute healthcare expenditures are enormous
Healthcare competes for resources with education and health literacy, socio‐economic security, programmes to influence behavioral choices, infrastructure and the environment
YET SIMPLY TAKING MONEY OUT OF BHB WITHOUT SOLVING THE SYSTEMATIC ISSUES WILL ONLY DESTABILIZE THE SYSTEM

2
Concentration of Healthcare Spending in the US Population, 2012
21.0%
49.5%
65.2%
75.0%81.7%
97.3%
2.7%
0%
20%
40%
60%
80%
100%
Top1% Top5% Top10% Top15% Top20% Top50% Bottom50%
PercentofPopulation,RankedbyHealthCareSpending
NOTE: Dollar amounts in parentheses are the mean annual expenses per person in each percentile. Population is the civilian noninstitutionalized population, including those without any healthcare spending. Healthcare spending is total payments from all sources (including direct payments from individuals and families, private insurance, Medicare, Medicaid, and miscellaneous other sources) to hospitals, physicians, other providers (including dental care), and pharmacies; health insurance premiums are not included.
SOURCE: Kaiser Family Foundation calculations using data from U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey (MEPS), Household Component, 2010 and 2012 Health Care Transformation Task Force Report
Percent o
f Total H
ealthcare Spending
($97,859) ($43,038 ($28,452) ($12,951) (≥$829) (<$829)
Bermuda Hospitals Board Commitment
BHB is working diligently to modernize and improve safety, quality and efficiency of acute care services and can also assist Bermuda in rationalizing the use of overseas providers, but this requires time, fiscal stability, political will and regulatory assistance
BHB is well positioned in terms of governance, facilities and expertise to continuously evolve in support of secondary prevention/chronic disease management, as well as coordinating key elements of post‐acute, long‐term and palliative care
Partnering with government on well‐designed primary prevention strategies can have tremendous ROI – both from the prospective of a healthy and productive society as well as a responsive & financially sustainable healthcare system
Thank you
1
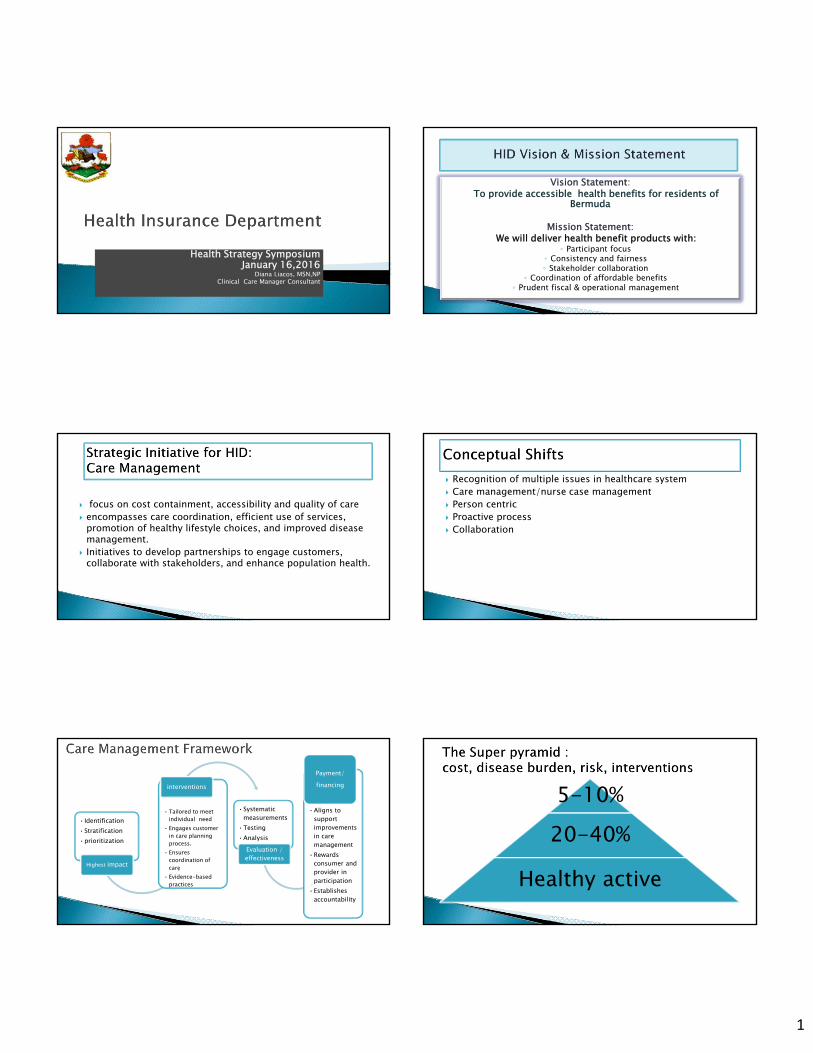
Health Strategy SymposiumJanuary 16,2016
Diana Liacos, MSN,NP Clinical Care Manager Consultant
Vision Statement: To provide accessible health benefits for residents of
Bermuda
Mission Statement: We will deliver health benefit products with:
◦ Participant focus◦ Consistency and fairness◦ Stakeholder collaboration
◦ Coordination of affordable benefits◦ Prudent fiscal & operational management
focus on cost containment, accessibility and quality of care encompasses care coordination, efficient use of services,
promotion of healthy lifestyle choices, and improved disease management.
Initiatives to develop partnerships to engage customers, collaborate with stakeholders, and enhance population health.
Recognition of multiple issues in healthcare system Care management/nurse case management Person centric Proactive process Collaboration
•Identification•Stratification•prioritization
Highest impact
• Tailored to meet individual need
• Engages customer in care planning process.
• Ensures coordination of care
• Evidence-based practices
interventions
•Systematic measurements
•Testing•Analysis
Evaluation / effectiveness
•Aligns to support improvements in care management
•Rewards consumer and provider in participation
•Establishes accountability
Payment/financing 5-10%
20-40%
Healthy active
2
Targeting individuals most likely to benefit from the intervention.Comprehensive assessment of the patient’s health conditions, treatments, behaviors, risks, supports, resources, values, and preferences Evidence-based care planning in accordance to patient’s goals and priorities and routine monitoring to meet the patient’s health-related needs and preferences. Promotion and coaching of patients’ and family caregivers’ in self-care .Coordination and communication among the patient and the care team.Facilitation of the transitions from the hospital to post acute care and referral to community resources. Specially trained nurse case manager that builds rapport with face to face contact with patient and collaborative relationship w/physician.
Re-evaluation of benefits to improve basic coverage Collaborations
Discharge planning Overseas referrals Chronic disease and long term care Case management software with patient engaging platform
Benefit Changes: HIP and FutureCarePromotes Quality of Care and LifeEnhances System Sustainability
Personal Home Care Services
Increased Number of Specialist Visits & Reimbursement Rates
Wellness Benefit
Youth Coverage (birth to age 21) - HIP Only
Overseas Preferred Provider Network
When an individual reaches their optimum level of wellness, everyone benefits including: The individual Their support system The health care delivery
system The reimbursement source
CMSA, 2013
1
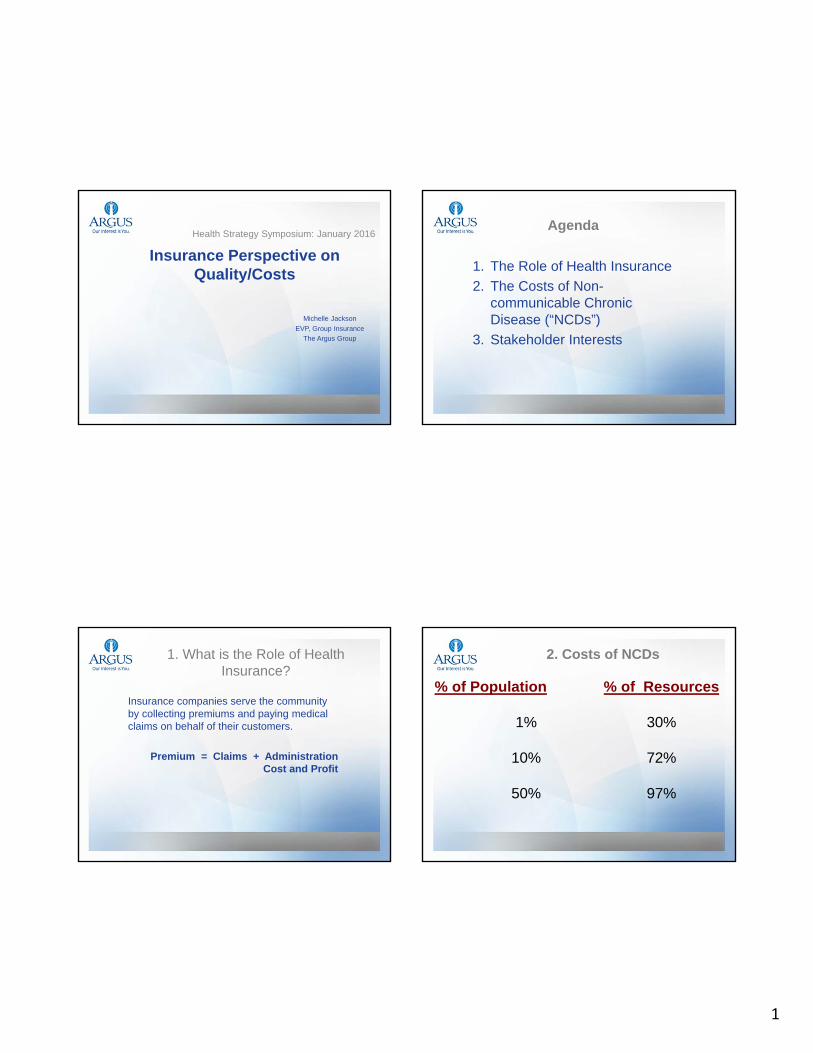
Insurance Perspective on Quality/Costs
Michelle Jackson
EVP, Group Insurance
The Argus Group
Health Strategy Symposium: January 2016Agenda
1. The Role of Health Insurance
2. The Costs of Non-communicable Chronic Disease (“NCDs”)
3. Stakeholder Interests
1. What is the Role of Health Insurance?
Insurance companies serve the community by collecting premiums and paying medical claims on behalf of their customers.
Premium = Claims + Administration Cost and Profit
2. Costs of NCDs
% of Population % of Resources
1% 30%
10% 72%
50% 97%
2
2. Costs of NCDs
1. Patients and providers often do not know the costs of care.
2. Treating chronic disease accounts for 86 percent of health care costs in the USA (Center for Disease Control and Prevention).
• Cardiovascular disease, Type 2 Diabetes, many cancers, kidney disease are among the most common, costly and preventable
• Example: $200,000 annually for one person on haemodialysis in Bermuda
3. Insurance payment model is “fee for service.” We pay for volume not value.
3. Stakeholder Interests
What can be done?
1. Initiatives focused on health literacy and empowerment
2. Non-communicable disease management (all stakeholders)
3. Payment reform
1/18/2016
1
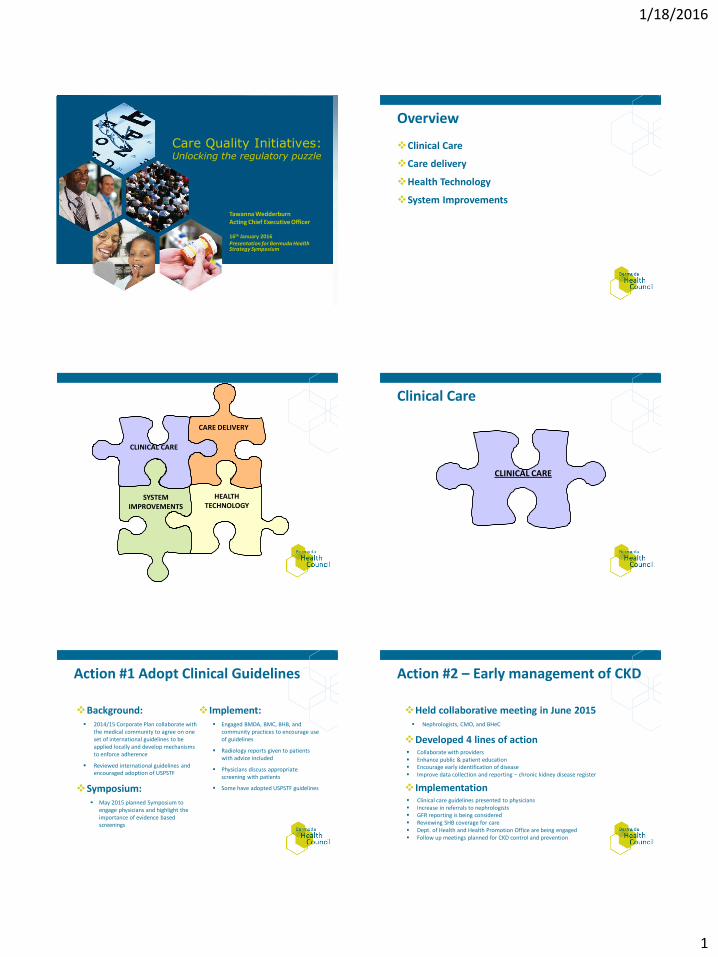
Care Quality Initiatives: Unlocking the regulatory puzzle
Tawanna Wedderburn Acting Chief Executive Officer 16th January 2016 Presentation for Bermuda Health Strategy Symposium
Overview
Clinical Care
Care delivery
Health Technology
System Improvements
CARE DELIVERY
HEALTH TECHNOLOGY
SYSTEM IMPROVEMENTS
CLINICAL CARE
Clinical Care
CLINICAL CARE
Action #1 Adopt Clinical Guidelines
Background: 2014/15 Corporate Plan collaborate with
the medical community to agree on one set of international guidelines to be applied locally and develop mechanisms to enforce adherence
Reviewed international guidelines and encouraged adoption of USPSTF
Symposium: May 2015 planned Symposium to
engage physicians and highlight the importance of evidence based screenings
Implement: Engaged BMDA, BMC, BHB, and
community practices to encourage use of guidelines
Radiology reports given to patients with advice included
Physicians discuss appropriate screening with patients
Some have adopted USPSTF guidelines
Action #2 – Early management of CKD
Held collaborative meeting in June 2015 Nephrologists, CMO, and BHeC
Developed 4 lines of action Collaborate with providers Enhance public & patient education Encourage early identification of disease Improve data collection and reporting – chronic kidney disease register
Implementation Clinical care guidelines presented to physicians Increase in referrals to nephrologists GFR reporting is being considered Reviewing SHB coverage for care Dept. of Health and Health Promotion Office are being engaged Follow up meetings planned for CKD control and prevention
1/18/2016
2
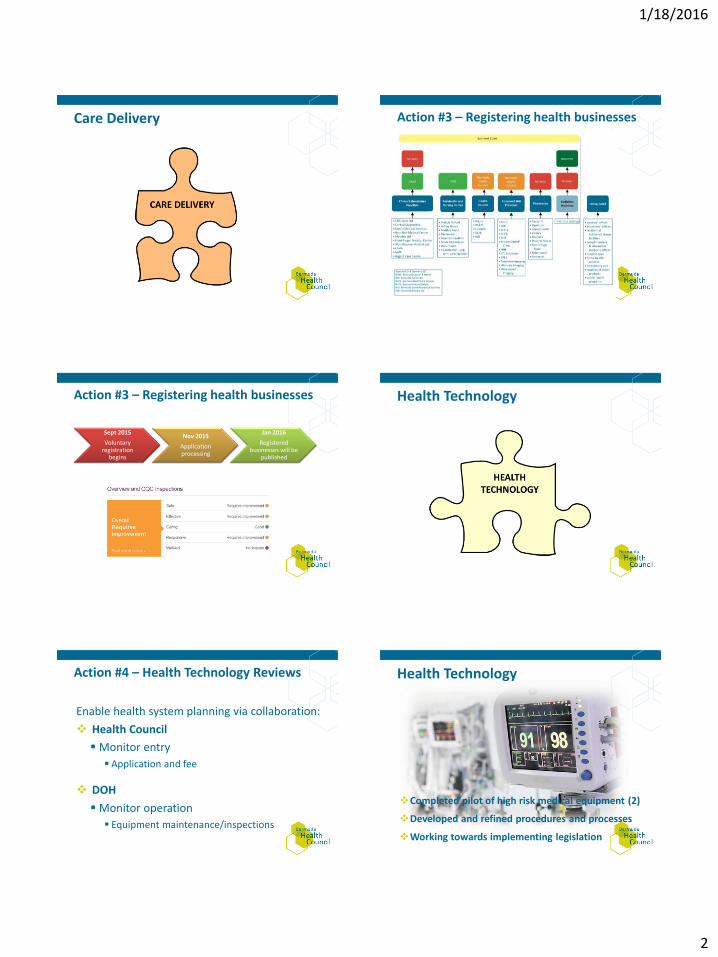
Care Delivery
Action #3 – Registering health businesses
Action #3 – Registering health businesses
Sept 2015
Voluntary registration
begins
Nov 2015
Application processing
Jan 2016
Registered businesses will be
published
Health Technology
Action #4 – Health Technology Reviews
Enable health system planning via collaboration:
Health Council
Monitor entry
Application and fee
DOH
Monitor operation
Equipment maintenance/inspections
Health Technology
Completed pilot of high risk medical equipment (2)
Developed and refined procedures and processes
Working towards implementing legislation
1/18/2016
3
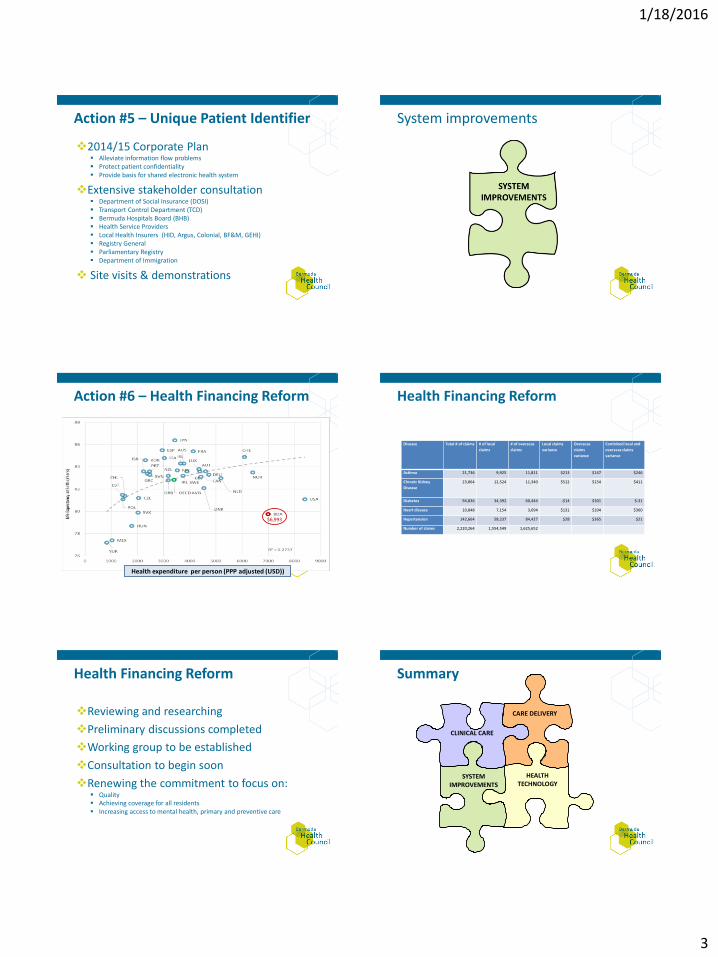
Action #5 – Unique Patient Identifier
2014/15 Corporate Plan Alleviate information flow problems Protect patient confidentiality Provide basis for shared electronic health system
Extensive stakeholder consultation Department of Social Insurance (DOSI) Transport Control Department (TCD) Bermuda Hospitals Board (BHB) Health Service Providers Local Health Insurers (HID, Argus, Colonial, BF&M, GEHI) Registry General Parliamentary Registry Department of Immigration
Site visits & demonstrations
System improvements
Action #6 – Health Financing Reform
Health expenditure per person (PPP adjusted (USD))
$6,993
Health Financing Reform
Disease Total # of claims # of local
claims
# of overseas
claims
Local claims
variance
Overseas
claims
variance
Combined local and
overseas claims
variance
Asthma 21,736 9,925 11,811 $213 $147 $246
Chronic Kidney
Disease
23,864 12,524 11,340 $512 $154 $411
Diabetes 94,836 34,392 60,444 -$14 $301 $-31
Heart disease 10,848 7,154 3,694 $131 $104 $360
Hypertension 142,664 58,237 84,427 $28 $365 $21
Number of claims 2,220,264 1,554,549 1,625,652
Health Financing Reform
Reviewing and researching
Preliminary discussions completed
Working group to be established
Consultation to begin soon
Renewing the commitment to focus on: Quality Achieving coverage for all residents Increasing access to mental health, primary and preventive care
Summary
CARE DELIVERY
HEALTH TECHNOLOGY
SYSTEM IMPROVEMENTS
CLINICAL CARE