Embed Size (px)
Citation preview

Beyond "DEATH and DYING" -
Managing Grief to Improve Occupancy

• Graduated Med School from Univ. of Zurich – 1957
• Psych Resident – NY & CO• Asst. Prof – U. of Chicago• Clinical Prof - UVA
Elisabeth Kubler-Ross, M.D.

Why You Should Study these Concepts
• Need to be a Grief Counselor for Residents
• Understanding your own fears of dying will help you deal with residents and their fears.
• Much of theory applies to other “losses” and concerns besides just death.
• Gain better understanding of how to support resident in their “last days” – w/o move-out!
• Learn how prospects go thru these same steps before making a move-in decision.

1. Increasing “speed” of move-ins Learn how the stages of “death & dying”
also apply to other “losses”; AND Learn how to use this psychology in
building relationships with prospective residents.
Improve Occupancy by:
Grief Management =
Learning to Accept Loss

2. Understanding more of the underlying needs & motivations of existing residents, Including:
Why some residents “complain all the time”; AND
AVOIDING MOVE-OUTS by better handling of these residents’ complaints!
Improve Occupancy by:

Improve Occupancy by:
3. Avoiding move-outs in a hospice situation Understand why why residents may move out; Learn why that may be the wrong decision;
AND Provide insights as to how you can help them
make the BESTBEST decision.

Kubler-Ross Theory
• All people go through 5 separate and distinct stages when faced with tragic news.
• Psychologically, these stages are different defense mechanisms enabling an individual to cope with an extremely difficult situation.
• The length of each stage will vary by person, but they must experience each stage.
• Had she written her book after computers became more prevalent, she might have portrayed this as a FLOW CHART, such as:

Denial anger
Bargaining
depression
ACCEPTANCE

Kubler-Ross 5 Stages of Acceptance
[Applies to all “losses” not only our own mortality]
• Death of spouse or other long-term companion• Loss of physical capability (e.g. failing
eyesight, suffered a fall with on-going limited mobility)
• Not permitted to drive anymore• Suffered some diminished mental capacity
and / or family expresses concern about forgetfulness
• Child / grandchild caregiver moved away• Spouse /friend experiences declining health
and unable to provide previous level of support

DENIAL
• “NO, Not me!”
• “There must be some mistake, the tests were mixed up somehow.”
• “That … (e.g. heart attack) was no big deal, I’ll be okay as soon as I get out of the hospital and back home!”
• “I don’t need any help, I’ve always done …”
• I just left the stove on that one time, normally I’m very safe.

DENIAL
• “Normal human emotion / reaction.
• Temporary state of shock.
• Serves as a buffer – gives time to continue with life and avoid becoming totally consumed with “bad news”.

DENIAL
•Often followed by ISOLATION.Easier to “fool yourself” if don’t also have to
try to fool other people!Can lead to living in a “fantasy world”.
EXAMPLE:• Resident that moves out because doesn’t want
to face all their friends in the building!

DENIAL
Patient (resident) can be quite selective in using this trait: Can be honest and discuss their
situation quite openly with one person; while
Pretending to “be fine” with others.May be more open with outsiders than own
family members!

DENIAL
Resident behaviors evidencing Denial of disease
• Diabetic refusing to eat diabetic desserts.
• Resident w COPD on O2 & still smoking
• Resident ignoring MD orders to exercise

STAGE 2: ANGER
• Feelings of anger, rage, envy & resentment.
• “Why me and not _________”
• “It was your fault that I left the stove on because you interrupted me by …”
• “You’re just saying that because you want to put me away.”
• “My daughter (son) doesn’t care, she/he just doesn’t want to be bothered”
• “Everybody here treats me like dirt.”

STAGE 2: ANGER
• Very difficult to deal with for both staff and family members.
• Anger is often displaced in all directions– Projected onto the environment– Appears to be directed at random

STAGE 2: ANGER
Often becomes cyclical in nature
• Visits from family & friends become painful
• Staff avoids the resident because “always complaining”
• Resident becomes more isolated and more angry about being ignored!
• Leads to further “acting out”, raising voice, making demands, complaining, etc.

How to AVOID MOVE-OUT1. Don’t take the anger personally (be
defensive) – understand that it generally has nothing to do with you!
2. Try to place yourself in resident’s “shoes” and understand what loss or “fear of loss” is precipitating the behavior.
Unresolved grief from loss of loved one Anger at medical diagnosis / prognosis Loss of physical or mental capabilities Loss of control – other people making decisions
for them

How to AVOID MOVE-OUT3. Don’t get into unnecessary arguments
No need to “defend your stand” Issue is most likely irrelevant Only feeds into hostile behavior
4. Understand that expressing anger (even if irrational) will help resident move thru the steps towards acceptance of their loss.
5. Show compassion, let the resident know that they are “still alive”, not forgotten and important to you.

How to AVOID MOVE-OUT6. Give assurances that they don’t have to
raise their voice to get your attention.
7. Encourage family members and staff to approach resident with cheerfulness and patience instead of AVOIDANCE.
8. Train staff to understand that, at times, anger will simply be because they still have physical and mental abilities that residents no longer possess. ENVY.

How to AVOID MOVE-OUT9. Encourage resident to retain independent
control of their decision making.10. Don’t ignore resident’s wishes and deal only
with the “children”.11. Respect the resident’s feelings, wishes, and
opinions – especially regarding his/her own care needs.
12. Remember that each resident wants to be “unique” but still loved and accepted.
13. Make sure you and your staff treat the resident as an individual and not a “thing”!

Denial anger
Bargaining

BARGAINING
• Looking for some type of agreement to postpone the inevitable!
• Not unlike a child: “If I am very good all week and do all my chores, then will you let me go?” (after being previously told NO)
• “I just want to stay here long enough to attend …”
• “I’ll only drive to my doctor’s, church and the grocery store”.

Marketing Opportunity1. When building relationships, identify
loss(es) that prospective residents have suffered:
• Loss of a Loved One
• Loss or diminishment of physical ability
• Declining mental capabilities
2. Determine which STAGE the senior is in dealing with their GRIEF over that loss.
3. In STAGE 3, Bargaining, offer them positive alternatives vs focus on disabilities.

DEPRESSION
Anger and rage replaced with a sense of a GREAT LOSS.
Effects both Current and Future ResidentsRealization that LIFE is GOING to CHANGE
Loss of Independence“Give up” their homeFinancial anxieties – “Will I run out of money?”“Life dreams” won’t be accomplished

What can You do to HELP?1. Recognize that the individual must go thru this
psychological stage and respect their concerns.
2. Be supportive. Allow them – at their time and pace – to share their sorrow and concerns with you. LISTEN!
3. Understand that this may be a time of quiet reflection and respect their need for privacy.
4. THIS IS NOT THE TIME FOR THE HARD SELL!
5. Become a problem-solver so that you are perceived as part of the “solution”, not a problem.
• e.g. Avoid move-out of current resident to a higher level of care by presenting them with a home-health / caregiver option.

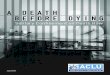
Use Maslow’s Hierarchy of Needs to Help with Depression
Demonstrate Alternatives that Meet Higher Level Needs

Apply Maslow’s Hierarchy of Needs1. Support self-esteem by complimenting them on some
positive aspect of appearance, personality, etc.
2. Help them focus on positive remembrances and CELEBRATE SUCCESSES!
3. Open new doors for future achievements and the creation of new precious memories.
4. Introduce them to existing residents who have suffered similar losses in the past.

5 Stages of Acceptance
Must achieve acceptance of their current situation before they will be willing to move-in.

Denial anger
Bargaining
depression
ACCEPTANCE

ACCEPTANCE
• Neither depressed nor angry about their “fate”.
• He/She will have mourned the loss AND moved towards a state of expectation for the next stage in their life.