Embed Size (px)
Citation preview

Bilateral pleural effusionsAn interesting case Authors: Dr Melissa Nagar (FY1)
Dr Patrick Liu (Consultant Respiratory Physician)Respiratory Dept., Victoria Hospital, Kirkcaldy
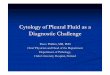
Left pleural effusion. Right hilar nodes
Ground glass, pleural effusions
Bibasal effusions, superior perihilar consolidation
INTRODUCTIONPleural effusions are a common finding in clinical practicewith a variety of causes1 and early identification aids inefficient treatment and symptomatic improvement inour patients.
It is caused by fluid accumulation for which thepathophysiology depends on the underlying cause. Swiftdiagnosis minimises further unnecessary investigationsand allows management plans to be implemented.1
CASE DESCRIPTIONA 52 year old female was admitted to acute medicaladmissions unit with a 5 week history of chest pain, newcough, increasing shortness of breath with new alteredsense of taste and pyrexia. She is a normally fit and wellnon-smoker with a past medical history of hypertension.
Blood tests revealed elevated d-dimer (2439) white cellcount (WCC) of 11.7 and C- reactive protein (CRP) of45. COVID PCR was negative. CXR was performed andshowed evidence of left pleural effusion and prominentright hilar nodes.
Given CXR findings and raised D-dimer, CT pulmonaryangiogram was performed and displayed bilateralgroundglass opacification, bilateral pleural effusions andmediastinal lymphadenopathy.
She was commenced on oral furosemide for cardiacfailure and amoxicillin to cover chest infection. Outpatientechocardiogram was arranged and the patient wasdeemed fit for discharge.
This lady re-presented 2 days after the above dischargewith ongoing symptoms of shortness of breath onexertion. CXR was carried out and was unchanged fromprevious. Furosemide dose was increased and she wasdeemed fit for discharge.
She had a final presentation around one month later withshortness of breath on exertion, persistent cough andchest tightness. Blood tests were carried out revealingelevated CRP to 44. CXR revealed bilateral pleuraleffusions and right perihilar consolidation thereforeantibiotics were commenced for atypical pneumonia.
Given worsening in pleural effusions, left pleural aspiratewas carried out. The results indicated it was an exudativeeffusion. CT chest/abdomen/pelvis showed similarfeatures as previous with mediastinal and supraclavicularlymphadenopathy, persistent groundglass opacificationand bilateral pleural effusions.
Echocardiogram was done as inpatient and revealednormal sized ventricle with dys-synchronous left
ventricular contraction and mild/moderate LV systolicimpairment.
Subsequently, EBUS-TBNA of mediastinal nodesshowed granulomatous inflammation in keeping with adiagnosis of sarcoidosis. Given LVSD on echocardiogram,cardiac MRI was arranged and showed evidence ofcardiac involvement.
She was then commenced on oral corticosteroids whichresulted in symptom improvement and radiographicchanges. She is now stable in the community on amaintenance dose of prednisolone.
DISCUSSIONSarcoidosis is a rare condition within the UK with annualincidence of 7 cases per 100,000 and lifetime prevalenceis 108,000 people.2 Although rare, diagnosis is importantto allow early treatment that will prevent complicationsof the disease.
Our case illustrates that cardiac sarcoidosis is a rare butimportant cause to consider in patients presenting withunexplained new-onset heart failure. Increased severityof heart failure in this patient group is a predictor ofsudden death.3 Furthermore, an American study of over300,000 inpatients found that nearly one fifth experiencedarrhythmias during hospitalisation.4 This is a complicationof sarcoidosis that requires prompt recognition andtreatment.
It further highlights how rapid improvement inrespiratory symptoms is observed once treatment iscommenced. The hope is that early treatment in this casewill have prevented long term irreversible impact on thepatient, for example, pulmonary fibrosis.5 It isdocumented that this complication is a risk factor formortality and a French study showed that “sarcodosispatients with pulmonary fibrosis have markedly decreasedsurvival compared to the general population” 3.
The above exhibits the potential substantial morbidityof the disease further emphasising the importance ofearly recognition and treatment. This aims to ensure thatcardiac and respiratory function (among others) ismaintained.
REFERENCES1. Hooper C, Lee YCG, Maskell N. Investigation of a unilateral pleural effusion in adults: British Thoracic
Society pleural disease guideline 2010. Thorax 201065: ii4-ii17.
2. Sarcoidosis statistics, Respiratory Health of the Nation Project, St Georges University London, Nottingham University and Imperial College London, British Lung Foundation
3. Gerke AK. Morbidity and Mortality in sarcoidosis. Current opinion in pulmonary medicine. Sep 2014.
4. Desai R, Kakumani K, Fong HK, et al. The burden of cardiac arrhythmias in sarcoidosis: a population basedinpatient analyis. Annals of translational medicine 2018.
Central predominant consolidation and ground glass attenuation with interlobular septal thickening and moderate bilateral pleural effusions
CXR prior to final discharge



























![Pleural Effusions [Read-Only] · An Update in Evaluation and Management Shruti Patel, MD Pulmonary & Critical Care PLEURAL EFFUSIONS](https://img.pdfslide.net/doc/110x75/5acddd407f8b9ab10a8e239f/pleural-effusions-read-only-update-in-evaluation-and-management-shruti-patel.jpg)