Embed Size (px)
Citation preview

BRIEF REPORT
Bilineal inheritance of PKD1 abnormalitiesmimicking autosomal recessive polycystic disease
Rodney D. Gilbert & Priya Sukhtankar &
Katherine Lachlan & Darren J. Fowler
Received: 21 December 2012 /Revised: 20 March 2013 /Accepted: 3 April 2013# IPNA 2013
AbstractBackground Dominant polycystic kidney disease is com-mon and usually presents clinically in adulthood. Recessivepolycystic kidney disease is much less common and fre-quently presents antenatally or in the neonatal period withsevere renal involvement. These are usually thought of asclinically distinct entities but diagnostic confusion is notinfrequent.Case-diagnosis/treatment We describe an infant withantenatally diagnosed massive renal enlargement andoligohydramnios with no resolvable cysts on ultrasound scan-ning. He underwent bilateral nephrectomy because of respira-tory compromise and poor renal function but died subsequentlyof overwhelming sepsis. Genetic analysis revealed that he hadbilineal inheritance of abnormalities of PKD1 and no demon-strable abnormalities of PKD2 or PKHD1.
Conclusions Biallelic inheritance of abnormalities of PKD1may cause extremely severe disease resembling autosomaldominant polycystic kidney disease (ADPKD) which canresult in diagnostic confusion. Accurate diagnosis is essen-tial for genetic counseling.
Keywords Autosomal dominant polycystic kidney disease .
Autosomal recessive polycystic kidney disease . Antenatal .
Hypomorphic allele
Introduction
Autosomal dominant (ADPKD) and recessive (ARPKD)polycystic kidney diseases are usually thought of as pheno-typically distinct entities but diagnostic confusion based onclinical findings is not unusual [1]. Although the majority ofpatients with ARPKD are diagnosed antenatally or in earlychildhood, there is wide phenotypic variability and some arenot diagnosed until adulthood [2, 3]. ADPKD is frequentlyasymptomatic until middle age but there is wide phenotypicvariation ranging from severe neonatal disease to individ-uals with adequate renal function into old age [4]. Wepresent a baby diagnosed in utero with severe fetal ADPKDmimicking ARPKD related to the inheritance of abnormalPKD1 genes from both parents.
Case report
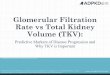
The male fetus of a primigravid 26-year-old was found tohave large, echogenic kidneys with no visible cysts, a smallbladder, and oligohydramnios on ultrasound scan at27 weeks of gestation. There was a maternal family historyof ADPKD (Fig. 1a) but both parents had normal renal
R. D. Gilbert (*) : P. SukhtankarRegional Paediatric Nephro-Urology Unit, University HospitalSouthampton, Tremona Road,Southampton SO16 6YD, UKe-mail: [email protected]
R. D. Gilbert : P. SukhtankarSchool of Medicine, University of Southampton,Southampton, UK
K. LachlanWessex Clinical Genetics Service, University HospitalSouthampton, Southampton, UK
K. LachlanHuman Genetics & Genomic Medicine, Faculty of Medicine,University of Southampton, Southampton, UK
D. J. FowlerCell Pathology Department, University HospitalSouthampton, Tremona Road,Southampton, UK
Pediatr NephrolDOI 10.1007/s00467-013-2484-x

ultrasound scans. There was no history of renal pathology inthe father’s family.
The child was born by Caesarian section at 34 weeksbecause of maternal pre-eclampsia. At birth, he requiredresuscitation for inadequate respiratory effort and bradycar-dia. He was intubated and surfactant was given. The birthweight was 3,470 g (>99.6th centile), heavier than expectedbecause of his enlarged kidneys.
Initially respiration was maintained on conventional venti-lation. On day 7 he was extubated and converted to nasalcontinuous positive airway pressure (CPAP). Initially he hadbrief episodes of apnea and bradycardia. These resolved withcaffeine, and were attributed to prematurity. Full enteral feedsof maternal breast milk via nasogastric tube were established.
Periodic apneas and desaturations became increasinglyfrequent and respiratory acidosis developed with poor gasexchange. Oliguria responded to furosemide administrationbut his respiratory status remained poor and he was re-intubated on day 11. Nasogastric feeds were stopped and he
received total parenteral nutrition (TPN). There was persistenthypertension despite treatment with amlodipine and hydral-azine. An echocardiogram showed a small patent ductusarteriosus and patent foramen ovale but good biventricularfunction. Respiratory function continued to deteriorate.
There was a prolonged discussion with the child’s parentsand the wider multidisciplinary team regarding withdrawalof care to allow natural death, as most neonates withARPKD who undergo bilateral nephrectomies do not sur-vive despite attempts at dialysis [5]. Despite the risks, bilat-eral nephrectomy was performed on day 17. Immediatelyprior to surgery, the plasma creatinine concentration was310 μmol/l. A peritoneal dialysis catheter and gastrostomywere also inserted. Ventilation immediately became verymuch easier and lung expansion improved significantly.Inotropic support with dopamine, noradrenaline, and adren-aline was required to maintain systolic blood pressure, pos-sibly because of the abrupt loss of renin production by thekidneys mimicking the severe hypotension seen in patients
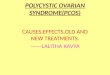
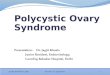
Fig. 1 a Family tree. The mother of the propositus had no renal cystsbut did have a clearly pathogenic mutation of PKD1. b Bisectedkidney. Both kidneys had similar macroscopic and microscopic ap-pearances. The left kidney measured 14×9×10 cm and weighed 430 g.The right kidney measured 14×8×8.5 cm and weighed 472 g. Onbisecting both kidneys, there was complete replacement of the normalparenchyma by multiple small cysts present in the cortex and medulla.c (H&E ×100)The histology of both kidneys showed large diametervariably shaped cysts arising from all parts of the nephron, includingglomerular cysts (in contrast to the multiple small diameter radially
arranged cysts arising from the collecting ducts expected in autosomalrecessive polycystic kidney disease ARPKD). Liver biopsy showed nohepatic fibrosis or ductal plate malformation. d DNA chromatogram.PKD1 Sanger DNA capillary sequencing traces (5′-3′) for the mater-nally inherited mutation (c.8362_8363ins34) (top DNA sequence) andpaternally transmitted unclassified variants (c.-67C>T, c.214C>T andc. 5848G>A). Deviation from wild-type sequence is denoted by un-derscore. *Neutral single-nucleotide polymorphism (dbSNP,rs137978188). HGVS recommended nomenclature applied with refer-ence to NCBI GenBank NM_001009944.2
Pediatr Nephrol

with renal tubular dysgenesis [6]. On day 19, metabolicacidosis with edema and ascites developed. Cultures ofblood and peritoneal fluid yielded Klebsiella pneumoniaeand Staphylococcus aureus. Despite intensive treatment, hedied on day 28.
Pathology
The kidneys were extremely large, weighing 430 g and472 g (Fig. 1b). Histological examination of the explantedkidneys was typical of ADPKD (Fig. 1c). Patients withARPKD usually have elongated cystic dilatation of thecollecting ducts but patients with cysts involving the entirenephron have been described [7].
A post-mortem liver biopsy showed no ductal plate mal-formation, which would have been consistent with ARPKDalthough it has been described in rare patients with ADPKD[8]. It was not possible to examine other organs because oflimited consent for post-mortem examination.
Genetics
Chromosome analysis (by conventional G-banding tech-nique) was normal, 46XY. Comparative genomic hybridiza-tion was also normal, excluding large deletions or insertions.Further analysis of PKD1 revealed a heterozygousc.8362_8363 ins34, (p.Ser2788fs) truncating mutation inexon 23 (Fig. 1d). This mutation has not been reported inADPKD previously, but is predicted to cause prematuretruncation of the protein product, and therefore is presumedto be pathogenic.
There were a further three previously unreported se-quence variants of unknown significance. These are c.-67C>T; c.214C>T (p.Leu72Leu) and c.5848G>A(p.Val1950Met). Genetic analysis of the parents showed thatthe truncating mutation was inherited from the mother, inkeeping with the family history. The three unreported vari-ants were inherited from the father and therefore in transwith the certain pathological mutation. Sequencing of thePKHD1 and PKD2 genes showed no abnormalities. Othergenes implicated in renal cystic disease such as VHL andHNF1-beta were not sequenced.
Discussion
ADPKD is the most common inherited renal disorder, withan incidence of one in 1,000 worldwide. It is caused bymutations in either PKD1 on chromosome 16 (85 % ofcases) or PKD2 on chromosome 4 (15 % of cases). Over500 mutations have been reported for PKD1 and 120 forPKD2. These genes encode the cell membrane proteinspolycystin 1 and polycystin 2, respectively. The polycystin
proteins are components of the primary cilium present oneach renal tubular cell. The role of the cilium is to senseflow within the tubule and thereby to orient the tubular cellto the long axis of the tubule. Polycystin 1 (PC1) is involvedin the detection of this shear stress. PC2 is a Ca2+-perme-able, non-selective cation channel. PC1 and PC2 interact viatheir C-terminal cytoplasmic tails and in response to flow-induced conformational change in PC1, PC2 allows influxof calcium ions from the extracellular fluid [9].
The highest level of PKD1 expression in renal tissue is inthe fetus from weeks 10 to 24. Thereafter, expression de-clines and it is not detectable in normal adult renal tubularcells [10]. Consistent with this is the observation that youngmice in whom the PKD1 gene is inactivated show massivecyst formation but adult mice develop a very mild cysticphenotype [11].
A model of cyst development that has gained widespreadsupport is that somatic mutation of the normal allele isrequired for cystogenesis. Evidence in support of this theoryincludes the demonstration of deletion or other inactivatingmutations in the remaining normal PKD1 or PKD2 gene inepithelial cells lining individual cysts [12]. There is alsoevidence for the clonal origin of cysts [13]. Total loss ofpolycystin 1 or 2 expression does not seem to be necessaryfor cyst development, however. In a murine model homo-zygous for a hypomorphic pkd1 allele that produces only13–20 % of normal transcript, affected animals were viablebut had enlarged, polycystic kidneys [14]. Similarly, pa-tients who inherit, in trans, two hypomorphic alleles whichdo not cause polycystic kidney disease, or a hypomorphicallele in trans with a pathogenic allele, develop severeneonatal disease reminiscent of ARPKD [15].
Our patient had in utero onset of disease in which thekidneys resembled those found in ARPKD. The most likelyexplanation for this is that he had very low expression ofpolycystin 1 in all tubule cells during the period when thegene is most actively expressed. This would imply that oneof the variants (or a combination of the variants) inheritedfrom the child’s father represents a hypomorphic allele,although we cannot exclude the possibility of an abnormal-ity in another cilium-related gene. This case adds furtherevidence that complete loss of polycystin 1 or 2 is notrequired for cystogenesis. It is also consistent with thenotion that a stimulus to cell division such as in uterogrowth, contralateral nephrectomy or acute kidney injurypromotes cyst formation and that high expression ofpolycystins during fetal development render the developingkidney particularly susceptible to low expression of theproteins during this period. Our patient illustrates the diag-nostic confusion that can arise with neonatal polycystickidney disease. Accurate diagnosis is essential for geneticcounseling and a concerted effort should be made to reachthe correct diagnosis.
Pediatr Nephrol

Acknowledgments Debbie Travis, Wendy Lewis, Rebecca Pollitt,Ann Dalton. Sheffield Diagnostic Genetic Service Sheffield Children’sNHS Foundation Trust, S10 2TH sheffieldchildrens.nhs.uk/SDGS
References
1. Guay-Woodford LM, Galliani CA, Musulman-Mroczek E, SpearGS, Guillot AP, Bernstein J (1998) Diffuse renal cystic disease inchildren: morphologic and genetic correlations. Pediatr Nephrol12:173–182
2. Sweeney WE, Avner ED (2011) Diagnosis and management ofchildhood polycystic kidney disease. Pediatr Nephrol 26:675–692
3. Bergmann C, Senderek J, Windelen E, Küpper F, Middeldorf I,Schneider F, Dornia C, Rudnik-Schöneborn S, Konrad M, SchmittCP, Seeman T, Neuhaus TJ, Vester U, Kirfel J, Büttner R, Zerres K(2005) Clinical consequences of PKHD1 mutations in 164 patientswith autosomal-recessive polycystic kidney disease (ARPKD).Kidney Int 67:829–848
4. Harris PC, Rosetti S (2010) Determinants of renal disease variabil-ity in ADPKD. Adv Chronic Kidney Dis 17:131–139
5. Guay-Woodford LM, Muecher G, Hopkins SD, Avner ED,Germino GG, Guillot AP, Herrin J, Holleman R, Irons DA,Primack W, Thomson PD, Waldo FB, Lunt PW, Zerres K (1995)The severe perinatal form of autosomal recessive polycystic kid-ney disease maps to chromosome 6p21.1-p12: implications forgenetic counseling. Am J Hum Genet 56:1101–1107
6. Gubler MC, Antignac C (2010) Renin-angiotensin system in kidneydevelopment: Renal tubular dysgenesis. Kidney Int 77:400–406
7. Bergmann C, Von Bothmer J, Bruchle NO, Venghaus A, Frank V,Fehrenbach H, Hampel T, Pape L, Buske A, Jonsson J, Sarioglu N,Santos A, Ferreira JC, Becker JU, Cremer R, Hoefele J, Benz MR,Weber LT, Buettner R, Zerres K (2011) Mutations in multiple PKD
genes may explain early and severe polycystic kidney disease. JAm Soc Nephrol 22:2047–2056
8. O’Brien K, Font-Montgomery E, Lukose L, Bryant J, Piwnica-Worms K, Edwards H, Riney L, Garcia A, Daryanani K, Choyke P,Mohan P, Heller T, Gahl WA, Gunay-Aygun M (2012) Congenitalhepatic fibrosis and portal hypertension in autosomal dominantpolycystic kidney disease. J Pediatr Gastroenterol Nutr 54:83–89
9. Chapin HC, Caplan MJ (2010) The cell biology of polycystickidney disease. J Cell Biol 191:701–710
10. Chauvet V, Qian F, Boute N, Cai Y, Phakdeekitacharoen B,Onuchic LF, Attie-Bitach T, Guicharnaud L, Devuyst O, GerminoGG, Gubler MC (2002) Expression of PKD1 and PKD2 transcriptsand proteins in human embryo and during normal kidney devel-opment. Am J Pathol 160:973–983
11. Lantinga-van Leeuwen IS, Leonhard WN, van der Wal A,Breuning MH, de Heer E, Peters DJ (2007) Kidney-specific inac-tivation of the Pkd1 gene induces rapid cyst formation in devel-oping kidneys and a slow onset of disease in adult mice. Hum MolGenet 16:3188–3196
12. Brasier JL, Henske EP (1997) Loss of the polycystic kidneydisease (PKD1) region of chromosome 16p13 in renal cyst cellssupports a loss-of-function model for cyst pathogenesis. J ClinInvest 99:194–199
13. Qian F, Watnick TJ, Onuchic LF, Germino GG (1996) The molec-ular basis of focal cyst formation in human autosomal dominantpolycystic kidney disease type I. Cell 87:979–987
14. Lantinga-van Leeuwen IS, Dauwerse JG, Baelde HJ, LeonhardWN, van de Wal A, Ward CJ, Verbeek S, Deruiter MC, BreuningMH, de Heer E, Peters DJ (2004) Lowering of Pkd1 expression issufficient to cause polycystic kidney disease. Hum Mol Genet13:3069–3077
15. Vujic M, Heyer CM, Ars E, Hopp K, Markoff A, Orndal C,Rudenhed B, Nasr SH, Torres VE, Torra R, Bogdanova N, HarrisPC (2010) Incompletely penetrant PKD1 alleles mimic the renalmanifestations of ARPKD. J Am Soc Nephrol 21:1097–1102
Pediatr Nephrol