Embed Size (px)
Citation preview

CLINICAL MICROBIOLOGY REVIEWS,0893-8512/97/$04.0010
Jan. 1997, p. 19–34 Vol. 10, No. 1
Copyright q 1997, American Society for Microbiology
Biology of Isospora spp. from Humans, Nonhuman Primates,and Domestic Animals
DAVID S. LINDSAY,1* J. P. DUBEY,2 AND BYRON L. BLAGBURN1
Department of Pathobiology, College of Veterinary Medicine, Auburn University, Auburn, Alabama 36849-5519,1 andParasite Biology and Epidemiology Laboratory, USDA Agricultural Research Service, Beltsville, Maryland 207052
INTRODUCTION .........................................................................................................................................................19TAXONOMIC PROBLEMS........................................................................................................................................20Isospora hominis.........................................................................................................................................................20Isospora bigemina .......................................................................................................................................................20
LIFE CYCLE .................................................................................................................................................................21Ultrastructure............................................................................................................................................................21Sporogony...................................................................................................................................................................21Excystation.................................................................................................................................................................21Endogenous Development ........................................................................................................................................21Extraintestinal Stages ..............................................................................................................................................21
DEVELOPMENT IN VITRO ......................................................................................................................................23DIAGNOSIS OF COCCIDIAL INFECTIONS .........................................................................................................23ISOSPORA INFECTIONS OF HUMANS..................................................................................................................23ISOSPORA BELLI INFECTIONS...............................................................................................................................23Life Cycle of I. belli ...................................................................................................................................................25Intestinal Infections in AIDS Patients...................................................................................................................25Extraintestinal Infections in AIDS Patients .........................................................................................................26Infections in Other Immunocompromised Hosts .................................................................................................27Infections in Immunocompetent Hosts..................................................................................................................27Microscopic Lesions Due to I. belli ........................................................................................................................27Diagnosis....................................................................................................................................................................27Treatment...................................................................................................................................................................27
ISOSPORA INFECTIONS OF NONHUMAN PRIMATES .....................................................................................28I. arctopitheci Infections............................................................................................................................................28Diagnosis and Treatment.........................................................................................................................................29
ISOSPORA INFECTIONS OF DOGS AND CATS...................................................................................................29Infections of Dogs .....................................................................................................................................................29I. canis infections ..................................................................................................................................................29The I. ohioensis complex.......................................................................................................................................29
Infections of Cats......................................................................................................................................................29I. rivolta infections.................................................................................................................................................29I. felis infections ....................................................................................................................................................29
Diagnosis....................................................................................................................................................................30Treatment...................................................................................................................................................................30
ISOSPORA SUIS INFECTIONS OF PIGS ................................................................................................................30Clinical Signs and Pathogenicity............................................................................................................................30Immunity....................................................................................................................................................................31Epidemiology .............................................................................................................................................................31Diagnosis....................................................................................................................................................................31Treatment and Control ............................................................................................................................................31
FUTURE DIRECTIONS ..............................................................................................................................................31REFERENCES ..............................................................................................................................................................31
INTRODUCTION
Isospora species are protozoan parasites that are in the phy-lum Apicomplexa. They are members of the group of organ-isms referred to as coccidia. The term “coccidia” was once usedto refer primarily to members of the genera Eimeria and Iso-
spora but is now used to include Cryptosporidium species, Tox-oplasma gondii, and other members of the suborder Eimerio-rina. Coccidia have complex life cycles. Members of the genusIsospora can complete their entire life cycle in a single host.Several have evolved the ability to use a paratenic host (trans-port host) in their developmental cycle.Coccidia are identified to the species level based on the
structure of their sporulated oocyst stage. The size, shape,color, texture, and type of internal contents are importantfeatures used in identifying coccidial oocysts. The oocyst stageis an environmentally resistant stage which is excreted in the
* Corresponding author. Mailing address: Department of Pathobi-ology, College of Veterinary Medicine, 166 Greene Hall, Auburn Uni-versity, Auburn, AL 36849-5519. Phone: (334) 844-2701. Fax: (334)844-2652. E-mail: [email protected].
19
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

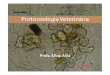
host feces. Most oocysts are excreted unsporulated and mustundergo a developmental period (sporulation) outside the hostbefore they are sporulated and become infectious. Sporulatedoocysts of Isospora species are characterized by having twosporocysts. Each sporocyst contains four sporozoites (Fig. 1a).The sporocyst may or may not have a Stieda body. A Stiedabody is a proteinaceous plug found at one end of the sporocyst.A sub-Stieda body may be present directly beneath the Stiedabody. Life cycle studies indicate that species of Isospora with aStieda body are generally monoxenous and confined to theintestines whereas species that lack a Stieda body often can useparatenic hosts, may have latent stages in the host, and may befacultatively heteroxenous. All important and valid species ofIsospora that infect humans, nonhuman primates, dogs, cats,and domesticated mammals lack a Stieda body in their sporo-cysts. Generic names of Levinia (34) and Cystoisospora (64)have been proposed for the Isospora species that utilizeparatenic hosts, but these generic names have not gained wide-spread acceptance.About 248 species of Isospora had been described prior to
1986 (95). Most of these species are known only from oocystsfound in the feces of the host animal. Until life cycle andcross-transmission studies are conducted to determine moreabout the biology of these species, the species validity of manyof these coccidians is questionable.
Isospora species can cause serious disease in humans andnursing pigs. Clinical disease is seldom seen in nonhumanprimates, dogs, or cats. Isospora species do not produce diseasein horses, domestic ruminants, rabbits, or domestic poultry,and reports of isosporan oocysts in the feces of these hostsprobably represent pseudoparasites that originated in feedcontaminated with wild-bird feces.
TAXONOMIC PROBLEMS
The sporulated oocysts of Isospora species resemble thesporulated oocysts of the related genera, Toxoplasma, Ham-mondia, Besnoitia, Frenkelia, and Sarcocystis. This resemblanceled to much confusion during the period from the late 1800s tothe mid-1970s, when the life cycle of these parasites was notknown. We will consider the two most notable examples inwhich these problems cause confusion.
Isospora hominis
Human isosporiasis is caused by Isospora belli, which is a truemember of the genus Isospora (187). Many early reports ofhuman coccidiosis refer to infection with a parasite describedas Isospora hominis. I. hominis is actually a species of Sarco-cystis, and the name is a synonym for Sarcocystis hominis or S.suihominis, species acquired by ingesting rare or raw infectedbeef or pork, respectively. There is no structural means ofdifferentiating these two species of Sarcocystis in human fecalsamples or in intestinal biopsy specimens. Intestinal sarcocys-tosis in humans can be a serious disease (18), unlike in otheranimals, which normally show no clinical signs. In many earlyreports, it is impossible to determine whether the authors aredescribing I. belli or a Sarcocystis species. An example of thisconfusion can be found in the pioneering work on coccidiosis,Coccidia and Coccidiosis of Domesticated, Game and Labora-tory Animals and of Man, by E. R. Becker, published in 1934(7). Becker includes line drawings that demonstrate sporula-tion of I. belli but refers to the parasite as I. hominis. The onlyway one can be certain if early authors are describing I. belli orI. hominis (Sarcocystis) is to examine the drawings or photomi-crographs if present. If none are included, a definitive identi-fication may not be possible.
Isospora bigemina
In the early and mid-1900s, it was thought that dogs and catsshared the same species of coccidia (7, 8). The name Coccid-ium bigemina had been given by Stiles in 1891 to a parasitedeveloping in the lamina propria of a dog (39). The organismwas placed in the genus Isospora in 1906. Based on the locationof the sporocysts, the parasite observed by Stiles was obviouslya species of Sarcocystis. Wenyon believed that there were two“races” of I. bigemina that could be differentiated based on sizeand called them the large and small races of I. bigemina (188).The large race developed in the lamina propria and was ex-creted as sporulated oocysts or sporocysts (i.e., a Sarcocystisspecies), whereas the small race developed in the epithelialcells of the small intestine and was excreted as unsporulatedoocysts. It is clear now that the small race of I. bigemina in dogsis actually Hammondia heydorni, an obligatorily heteroxenousparasite (81). It is impossible to determine what the small raceof I. bigemina in cats actually was because its oocysts are struc-turally indistinguishable from those of Toxoplasma gondii,Hammondia hammondi, and Besnoitia species. Reports of thelarge race of I. bigemina in cats, other animals, and humansalso actually refer to Sarcocystis species.
FIG. 1. Sporulated oocysts of I. belli. (a) Oocyst containing two sporocysts(arrows). Note the oocyst wall (open arrow), the sporozoites (S) in the sporo-cysts, and the nucleus of a sporozoite (arrowhead). (b) A Caryospora-like oocystof I. belli containing one sporocyst (arrow). Note the oocyst wall (open arrow), asporozoite (S), and sporocyst residuum (R). The oocysts are unstained. Magni-fication, 31,900. Courtesy of Donald Duszynski, University of New Mexico.
20 LINDSAY ET AL. CLIN. MICROBIOL. REV.
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

LIFE CYCLE
Coccidial life cycles are complex, with both exogenous andendogenous cycles present. Paratenic (transport) hosts mayalso be employed.
Ultrastructure
Transmission electron microscopy has been widely used toexamine the developmental stages of coccidial parasites. Theentire life cycle of I. suis in pigs has been described by usingTEM, and it was similar to that described for Eimeria species(123). Notable differences are present in the structure of thesporozoite stages of Isospora and Eimeria species. The sporo-zoites of mammalian Isospora species contain one or two in-clusions, termed crystalloid bodies, that are composed of par-ticles similar in appearance to beta-glycogen particles, whereasthe sporozoites of Eimeria species contain one or two inclu-sions, termed refractile bodies, that appear to be protein-aceous. These inclusions are generally lost in the process ofconversion from sporozoite to merozoite stage (59, 122) in vivobut may persist in parasites cultivated in vitro (107).
Sporogony
Sporogony is the production of infective sporozoites withinsporocysts inside the oocyst. Sporogony usually occurs outsidethe host and is the exogenous phase of the coccidial life cycle.Sporogony is dependent on moisture, temperature, and ade-quate oxygen. Several controlled studies have been conductedon the sporogony of Isospora oocysts from dogs (94, 117), cats(160), and pigs (108). These studies indicate that temperaturesgreater than 408C or less than 208C inhibit sporulation of theoocysts. Rapid sporulation (,16 h) of oocysts occurs at 30 or378C. Structural events that occur during sporogony are similarfor all species. Oocysts are excreted in the feces, and theyusually have a contracted sporont. A few oocysts will be ex-creted in the sporoblast stage (two-celled stage). As the nu-cleus of the sporont divides, a clear nuclear streak is formed,nuclear division occurs, and the sporont divides to form twouninucleate sporoblasts. Nuclear division occurs again, and thenuclei are visible as clear areas at the poles of the sporoblast.Nuclear pyramids may be seen at the poles of the sporoblasts.The sporoblasts become elongate and form the sporocyststage. Nuclear division occurs again, and the outline of devel-oping sporozoites soon becomes visible. When the sporozoitesare fully visible, the oocyst is considered to be sporulated. Asmall percentage (,2%) of oocysts are Caryospora-like andcontain one sporocyst which encloses eight sporozoites (96,108, 121, 193) (Fig. 1b). Heat treatment of unsporulated I.rivolta oocysts at 508C for 5 min increased the numbers ofCaryospora-like oocysts that were produced after sporulation(121). These Caryospora-like oocysts of I. rivolta were infec-tious for mice (paratenic hosts) and cats. Oocysts collectedfrom cats inoculated with Caryospora-like oocysts were Isospo-ra-like after sporulation, indicating that heat treatment did notinduce a stable mutation. The biological significance of theseCaryospora-like oocysts is unknown.
Excystation
Excystation is the process by which sporozoites are releasedfrom the sporocysts/oocysts. The process is basically the samefor all mammalian Isospora species studied to date (46, 47, 109,128, 165, 166) and is similar to what occurs in Sarcocystis spp.(15) and T. gondii (22). Studies have been conducted withintact oocysts or with sporocysts that have been mechanically
freed from the oocyst wall. Pretreatment of oocysts with so-dium hypochlorite solution (109, 165) or cystine hydrochloride(128) under CO2 enhances excystation of intact oocysts. Expo-sure of oocysts or sporocysts to sodium taurocholate solution(0.75%, wt/vol), bile (5%, vol/vol), or sodium taurocholate(0.75%, wt/vol) plus trypsin (0.25%, wt/vol) will cause activa-tion of sporozoites. If bile is used, the host animal from whichthe bile is obtained is of little importance (128). Sporozoitesbecome motile within the sporocysts and tumble or glidearound one another. This movement is not continuous but isinterrupted by periods of inactivity. Eventually, the sporocystwall opens along four plate-like junctions (148, 165, 166) andthe sporozoites will exit through the opening that is formed.Sporozoites exit oocysts through indentations or fractures thatform in one or both ends of the oocyst wall (128, 165).
Endogenous Development
The endogenous life cycle of mammalian Isospora species issomewhat different from that of typical Eimeria species (Fig.2). Sporozoites enter cells in the intestine but usually do notform rounded uninucleate trophozoites. Some sporozoitesand/or merozoites leave the intestine and form dormant cyststages (hypnozoites) in extraintestinal tissues (31, 40, 149).Intestinal sporozoites may retain their elongate sporozoiteshape, become binucleate, and divide by endodyogeny to formtwo daughter merozoites. These daughter merozoites divide byendodyogeny an indefinite number of times (27, 59, 107, 122,123). For this reason, the number of sequential asexual mer-ogonous cycles cannot be determined, and developmentalstages are referred to as structural types instead of generations.Eventually, multinucleate meronts are formed. These merontsare elongate and retain their merozoite shape. Several merontsmay occur in the same host cell, and, with time, sexual stagesare formed. Microgamonts are multinucleate and produce bi-flagellated microgametes (60). Macrogamonts lack the highlyeosinophilic wall-forming bodies found in most Eimeria spe-cies, and the oocyst wall is usually inconspicuous. Microga-monts and macrogamonts may coexist in the same host cell.The endogenous life cycles in animals that ingest oocysts and
in those that ingest paratenic hosts are similar (35, 38). Theprepatent period may be shortened in infections that are ini-tiated by consumption of paratenic hosts (35, 38, 43, 65).
Extraintestinal Stages
Extraintestinal stages occur in the tissues of the definitivehost in canine and feline Isospora species (31, 40) and I. belli ofhumans (130, 149) (Fig. 3 and 4). Instead of undergoing thenormal developmental cycle in the intestinal tract, some sporo-zoites (merozoites?) leave that site and invade extraintestinalsites in the host. Mesenteric lymph nodes are most often in-volved, but other tissues such as the liver, spleen, and tracheo-bronchial and mediastinal lymph nodes can be infected. Parasitesare usually found as single organisms resembling sporozoites, butsome divisionmay occur at these extraintestinal sites, and up to 15parasites have been observed in an infected cell (40). The infectedhost cells probably are macrophages.Mice, rats, hamsters, dogs, cats, cattle, sheep, and camels
have been shown to be paratenic hosts for several Isosporaspecies (31, 40, 42, 55, 65, 78, 82, 154, 192). Sporozoites excystfrom oocysts and invade extraintestinal tissues. Mesentericlymph nodes are most often infected; other tissues such as thespleen, liver, and skeletal muscles are sometimes parasitized.Parasites are most often found as single organisms; parasitedivision at these sites has not been confirmed (65). For this
VOL. 10, 1997 BIOLOGY OF ISOSPORA SPP. 21
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

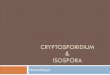
FIG. 2. Developmental stages of I. rivolta in cats and mice. (A, B, G to J, M, and N) Smears fixed in methanol and stained with Giemsa. (C to F) Sections stainedwith iron hematoxylin (C, D, F) and by the PAS reaction (E). (K and L) Smears not fixed or stained. (A and C) Division of meronts by endodyogeny (arrow). (B) Animmature meront with four nuclei. (D) Two multinucleated meronts (arrows) in the same parasitophorous vacuole. (E) PAS-positive granules (arrow) in merozoites.(F) Meronts with different-sized merozoites (arrows). (G) An immature microgamont with many nuclei (arrow). (H) Several mature microgametes (arrow). (I)Macrogamont with a large nucleus (arrow) and prominent nucleolus. (J) An unsporulated oocyst. (K) Unsporulated oocyst containing a contracted sporont. (L)Sporulated oocyst containing two sporocysts with sporozoites (arrows). (M) Extraintestinal zoites in the mesenteric lymph node of a cat. One zoite is in a host cell(arrow), and one has ruptured out of its host cell (arrowhead). (N) Extraintestinal tissue cyst containing a single zoite (arrow) in the mesenteric lymph node of a mouse.Magnifications, 32,300. Reprinted with permission of the publisher from reference 38.
22
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

reason, it is more accurate to refer to the host as a paratenicrather than an intermediate host.Transmission electron microscopy reveals that the sporozo-
ites are inside a parasitophorous vacuole (PV) (14, 42, 129)(Fig. 3). The appearance of the contents of the PV changesduring the course of infection. At 1 day postinoculation (p.i.)sporozoites are surrounded by a PV membrane that has a wavyappearance, and the PV contains numerous vesicles. By 7 daysp.i., there is an electron-dense granular layer immediately be-neath the PV membrane. Filaments or tubules may also bepresent in this layer. It is this granular layer that appears as athick wall by light microscopy. Membrane-bound, electron-dense granules, apparently of host cell origin, are present atthe margins of the PV membrane. The sporozoite lies in thecenter of the cyst. Sporozoites increase in size during thecourse of infection and accumulate polysaccharide granules intheir cytoplasm. It is because of the presence of these polysac-charide (amylopectin?) granules that the sporozoites stain pos-itively in the periodic acid-Schiff (PAS) reaction. The crystal-loid bodies of sporozoites remain intact during the course ofthe infection.Disease does not occur in paratenic hosts (38). Parasites
remain viable for at least 23 months in extraintestinal tissues ofmice (38). When the definitive host ingests a paratenic host,the subsequent prepatent period may be shorter than wheninfections are initiated by oocysts. The number of oocysts pro-duced by the definitive host and the patent period are similarto those in oocyst-induced infections (43). The tissues of paratenichosts are not infectious for other paratenic hosts (38).An interesting interaction occurs in mice experimentally in-
fected with I. felis and then challenged with Babesia microti. Miceinfected with I. felis 28 days before infection with B. microti do notdevelop B. microti antibodies but are completely resistant to in-fection with B. microti (176). Partial resistance to B. microti can beachieved by transfer of spleen cells frommice infected with I. felis.Treatment of I. felis-infected mice with a monoclonal antibody toL3T41 cells increases their susceptibility to B. microti infection(176). These results suggest that cell-mediated immunity is in-volved in the observed nonspecific resistance.
DEVELOPMENT IN VITRO
Several mammalian Isospora species have been grown in cellcultures (54, 56, 57, 58, 102, 107). Primary cell cultures fromthe host animal generally support the most numerous and mostchronologically advanced parasite stages. Sporozoites are ob-tained from excysted oocysts and used as an inoculum. Sporo-zoites penetrate host cells and undergo several divisions byendodyogeny. In primary porcine and bovine cell cultures,binucleate meronts and merozoites of I. suis were motile andwere observed to exit and enter host cells (102). No noticeableill effects were observed in the host cells. Only I. rivolta and I.suis have produced multinucleate meronts (with more than twonuclei) in cell cultures, and these meronts did not reach ma-turity (54, 102). Sexual stages and oocysts do not develop in cellcultures. Continuous cultivation of an Isospora species has notbeen achieved in cell culture.I. felis, I. rivolta, and I. suis will develop from sporozoites to
unsporulated oocysts in the chorioallantoic membrane of de-veloping chicken embryos (3, 71, 105). Development is usuallylimited to the tissues of the chorioallantoic membrane, butmeronts of I. felis have been seen in the livers and intestines ofchicken embryos that have been chemically immunosup-pressed (71). Although complete development has been ob-tained, the in ovo system has not gained widespread use be-cause few oocysts are obtained and they do not sporulate.
DIAGNOSIS OF COCCIDIAL INFECTIONS
Coccidia are often members of the normal fauna of animalhosts, and the mere presence of oocysts in the feces is notalways indicative of clinical infection (103). Demonstration ofoocysts in fecal samples is the method of choice for identifyingcoccidian infections in animals. Fecal flotation in Sheather’ssugar solution (500 g of sugar, 320 ml of water, 6.5 g of phenol)is most often used, but other flotation solutions such as zincsulfate or saturated sodium chloride can be used. If largeamounts of fecal fat are present, other concentration tech-niques such as formalin-ether or ethyl acetate sedimentationmay be more applicable because of the removal of fecal fat bythe solvents. No special stains are needed to observe the oo-cysts. However, special stains are often used to identify humaninfections with I. belli.The diagnosis of coccidiosis in animals is based on clinical
signs (diarrhea), history, evaluation for potential copathogens,and demonstration of coccidial oocysts of a pathogenic speciesin the animals’ feces. Knowing the actual numbers of oocystspresent in the feces is of little help in determining if clinicaldisease is present.Demonstration of parasite stages in tissue samples collected
at necropsy in animal infections or in intestinal biopsy speci-mens or samples collected at autopsy in human infections isalso suitable for obtaining a diagnosis. Special stains are oflittle value in identifying coccidial stages. Familiarity with theappearance of the stages is far more useful in locating them inhistological samples (Fig. 2).
ISOSPORA INFECTIONS OF HUMANS
I. natalensis has been reported in humans (48), but little isknown about this parasite. It was found in the feces of a21-year-old patient suffering from amebic dysentery and otherprotozoal and helminth infections. Oocysts of I. natalensis wereobserved on four consecutive days (after the patient had beentreated for amebic dysentery), and the I. natalensis infectionwas self-limiting. Infection with this parasite has apparently notbeen observed since 1953, when it was described. Its oocystsresemble those of the I. ohioensis complex seen in dogs, I.rivolta of cats, and I. suis of pigs, but they are slightly larger(Table 1).I. chilensis described from humans in South America is not
a valid name; it is a species of Sarcocystis. As mentioned above,I. hominis is also no longer considered a valid name because ittoo is a species of Sarcocystis.Three cases of infection with a coccidian species believed to
be an isosporan were reported from humans in Papua NewGuinea (4). The oocysts were excreted unsporulated, werespherical, and measured 8.5 mm in diameter. Sporulation wasslow, taking about 2 weeks, and the final proportion of oocyststhat sporulated was only about 10%. The sporocysts of thiscoccidium were illustrated in drawings with no Stieda body, butthere appears to be a Stieda body in the photomicrographs thataccompany the description. The parasite is probably a speciesof Cyclospora, a recently recognized coccidial pathogen of hu-mans that has two sporocysts with Stieda and sub-Stieda bodiesthat enclose two sporozoites (144).
ISOSPORA BELLI INFECTIONS
I. belli infections are essentially cosmopolitan in distributionbut are more common in tropical and subtropical regions,especially Haiti, Mexico, Brazil, El Salvador, tropical Africa,the Middle East, and Southeast Asia (53, 88, 164). Pigs, dogs,
VOL. 10, 1997 BIOLOGY OF ISOSPORA SPP. 23
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

24 LINDSAY ET AL. CLIN. MICROBIOL. REV.
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

mice, rats, rabbits, guinea pigs, and rhesus monkeys are notsuitable definitive hosts (61, 87); however, in one study, patentinfections were reported in two of three gibbons (193). Thislack of susceptibility has led some researchers to discountanimals as reservoirs (90). However, it is not known if these orother animals may serve as paratenic hosts for I. belli. The roleof paratenic hosts in the transmission of I. belli needs to beinvestigated to establish whether modes of transmission otherthan by contaminated food or water exist. The existence ofparatenic hosts may help explain infections occurring in areaswhere sanitation is adequate.
Life Cycle of I. belli
Oocysts are passed in feces unsporulated or partially sporu-lated (sporoblast stage). They can sporulate in less than 24 h(133). Oocysts are elongate and ellipsoidal with slightly ta-pered ends, or one end may be tapered and the other end blunt(Fig. 1; Table 1). The patent period is not known. It may be aslittle as 15 days in some patients (127). Chronic infectionsdevelop in some patients, and oocysts are excreted for severalmonths to years. In one case, an apparently immunocompetentindividual had symptoms that were present for 26 years andhad I. belli infection documented on several occasions over a10-year period.All life cycle stages typical of Isospora species have been
observed by light and transmission electron microscopy (16,149, 179). The number of asexual types present has not beendetermined. If the life cycle is similar to that of other carni-vore/omnivore Isospora species, the first asexual division wouldbe by endodyogeny. Division by endodyogeny probably occursrepeatedly. Endogenous stages are located in enterocytes lin-ing the villi of the small intestine and rarely in those in thelarge intestine (16, 149, 179). Endogenous stages are seldomfound in other locations such as enterocytes lining the crypts orin cells in the lamina propria. Extraintestinal infections havebeen observed in AIDS patients (see below) and probably alsooccur in immunocompetent patients.
Intestinal Infections in AIDS Patients
Diarrhea produced by I. belli in AIDS patients is often veryfluid and secretory-like and leads to dehydration requiringhospitalization. Fever and weight loss are also common find-ings. Other opportunistic pathogens are also common in thesepatients. Intestinal lesions induced by I. belli and the responsesto chemotherapy are usually similar to those in immunocom-petent patients.In an extensive 8-year surveillance program of AIDS pa-
tients in Los Angeles County (164), I. belli was found in 127(1%) of 16,351 patients. The prevalence of infection was high-est among foreign-born patients, especially patients from ElSalvador (7.4%) or Mexico (5.4%) or of other Hispanic eth-nicity (2.9%). Patients between the ages of 14 and 24 weremore likely to have I. belli infection than were older patients.Patients with a history of Pneumocystis carinii pneumonia wereless likely to have I. belli infection. The authors concluded thatisosporiasis among AIDS patients in Los Angeles may be re-
lated to travel exposure and/or recent immigration from LatinAmerican countries. Additionally, the use of trimethoprim(TMP)-sulfamethoxazole (SMX) for the treatment or preven-tion of P. carinii pneumonia may effectively prevent the acqui-sition of primary I. belli infection or the recrudescence ofexisting I. belli infection. It was recommended that physicianshave an increased index of suspicion for I. belli in AIDS pa-tients with diarrhea who have immigrated from or traveled toLatin America, are Hispanics born in the United States, areyoung adults, or have not received prophylaxis with TMP-SMXfor P. carinii. Additionally, it was suggested that AIDS patientstraveling to Latin America and other developing countries beadvised of the potential for food-borne and waterborne acqui-sition of I. belli infection and consider taking TMP-SMX che-moprophylaxis.I. belli infection was observed in 20 (15%) of 131 AIDS
patients with opportunistic infections at Port-au-Prince, Haiti(28). Stool samples collected from 170 siblings, friends, andsexual partners were negative. No demographic or laboratorycharacteristics distinguished patients with AIDS and I. bellifrom patients with AIDS and other opportunistic infections. Inanother study, three of three patients with I. belli infectionwere from Haiti and lived in the United States at the time ofthe study (190).Nine (19%) of 46 patients from Zaire with chronic diarrhea
and suspected of having AIDS had I. belli (80). Eight of thenine I. belli-positive patients were later confirmed to haveAIDS. I. belli was found in 13 (9.9%) of 81 AIDS patientsexamined at a reference center in Sao Paulo, Brazil (158).Stool samples from 81 immunocompetent individuals werenegative for I. belli. Three (5%) of 60 AIDS patients examinedin Catalinya, Spain, were positive for I. belli oocysts (155).A pregnant AIDS patient with I. belli diarrhea diagnosed at
5.5 months of pregnancy delivered a live human immunodefi-ciency virus-positive infant (147). Her sexual partner was also
TABLE 1. Measurements of oocysts of Isospora speciesfrom mammals
Species HostDimensions (mm) of:
Oocystsa Sporocystsa
I. belli Humans 23–36 by 12–17 12–14 by 7–9I. natalensis Humans 24–30 by 21–25 17 by 12I. arctopitheci NH primatesb 21–30 by 21–25 13–21 by 10–16I. callimico NH primates 13–21 by 12–17 10–13 by 7–9I. endocallimici NH primates 25–31 by 21–27 15–20 by 10–15I. scorzai NH primates 23 by 20 14 by 9I. canis Dogs 34–40 by 28–32 18–21 by 15–18I. ohioensis Dogs 19–27 by 18–23 15–19 by 10–13I. burrowsi Dogs 17–22 by 16–19 12–16 by 8–11I. rivolta Cats 18–28 by 16–23 14–16 by 10–13I. felis Cats 38–51 by 27–39 20–26 by 17–22I. suis Pigs 17–25 by 16–21 11–14 by 8–11
aMeasurements represent the range unless none was reported.b NH primates, nonhuman primates.
FIG. 3. Stages of I. ohioensis in lymphoid cells of the mesenteric lymph nodes of mice. (A) Zoite in a smear, 4 days after infection. Magnification, 31,650. (B)Electron micrograph of the crystalloid body 5 days after infection. Note the regular arrangement of units. Magnification, 371,300. (C) Electron micrograph of a zoitein the region of the nucleus 7 days after infection. The parasitophorous vacuole (PV) is filled nearly completely by granular material (GM). Magnification, 323,800.(D) Zoite in a smear of mesenteric lymph node, 4 days after infection. Giemsa stain was used. Magnification, 31,650. (E) Electron micrograph of a zoite 14 days afterinfection. The PV has an electron-lucent space (ES) and granular material (GM). Magnification, 323,800. Other abbreviations: A, amylopectin; CH, chromatin; CR,crystalloid body; DK, dark granules; HC, host cell; IT, intravacuolar tubules; LP, limiting membrane of the PV; NH, host cell nucleus; MN, micronemes; PA, zoite;PE, three-layered pellicle of zoite; R, rhoptries; SL, tissue cyst wall. Reprinted with permission of the publisher from reference 42.
VOL. 10, 1997 BIOLOGY OF ISOSPORA SPP. 25
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

positive for I. belli. Treatment with TMP-SMX never elimi-nated the I. belli infection.
Extraintestinal Infections in AIDS Patients
Two reports of disseminated extraintestinal isosporiasis inpatients with AIDS have been published (130, 149). The firstpatient was a 38-year-old white male homosexual who wasexamined at the National Institutes of Health, Bethesda, Md.(149). He initially presented to a local hospital with a history ofprogressive dyspnea and fever; he also complained of dyspha-gia, nausea, vomiting, and brown watery diarrhea (eight ornine episodes daily). He had lost 20 lb (9.17 kg) in 2 months(15% of his body weight). P. carinii pneumonia and oropha-ryngeal candidiasis were noted, and he was treated with TMP-SMX and pentamidine. His condition improved, and he wasdischarged 24 days after admission. He subsequently was re-admitted complaining of nausea, vomiting, and diarrhea. Hewas diagnosed as having Giardia lamblia infection and wastreated with metronidazole. Five months after his initial hos-pitalization, he was diagnosed as having I. belli and Entamoebahistolytica infection. He was treated with TMP-SMX, metroni-dazole, and diodoquin. Three months later he presented withdyspnea, fever, diarrhea, and generalized wasting. Cytomega-lovirus pneumonia was demonstrated at this time. Repeatedstool examinations were negative. He died 2 weeks later. Atautopsy, the body demonstrated severe cachexia, focally con-solidated lungs, multiple small intestinal foci of multifocal er-ythema and hemorrhage, ulcerated cecal lesions up to 5 mmacross, and enlarged mesenteric, periaortic, and mediastinallymph nodes. Microscopically, disseminated cytomegalovirusinfection involving the lungs, intestines, adrenal glands, mes-enteric lymph nodes, and, to a lesser extent, liver and pancreaswas observed. Mycobacterium kansasii was cultured from theliver and spleen, although no granulomas were observed intissue sections.Microscopic findings associated with I. belli infection were
observed in the lymph nodes and walls of both the small andlarge intestines. Marked lymphocytic depletion was observedin the lymph nodes, and foci of granuloma-like histiocytic pro-liferation were seen in the mesenteric, periaortic, and medias-tinal lymph nodes. Intracellular zoites were observed in thecytoplasm of histiocytes. The parasites were surrounded by athick eosinophilic cyst wall in hematoxylin-and-eosin-stainedsections. The cyst wall was PAS positive. Most of the infectedcells contained only one zoite; however, some contained two orthree. Examination of the intestinal tissues demonstrated in-traepithelial asexual and sexual stages of I. belli and occasion-ally merozoites that appeared to be in cells in the laminapropria. Numerous I. belli oocysts were observed in scrapingsobtained from the intestine.The second case was observed in a 30-year-old black woman
who was a native of Burkina Faso but had lived in France for2 years (130). She initially presented with fever, diarrhea, andweight loss. She was found to have esophageal candidiasis andI. belli infection. The I. belli infection was treated with TMP-SMX (200 mg/day), and the diarrhea resolved within a week.She was placed on maintenance therapy of 100 mg of TMP-SMX daily but suffered eight episodes of recurrent infectiondiagnosed by stool examination or duodenal biopsy over thenext 3 years. Examination of the biopsy specimens demon-strated severe villous atrophy and meronts, gamonts, and oo-cysts of I. belli within enterocytes. Gamonts and merozoite-likestages were observed in the lamina propria. No other patho-gens were observed in the biopsy specimens. An autopsy con-ducted after her death revealed cachexia. The abdominal cavity
contained 0.5 liter of serous ascitic fluid. The liver, spleen, andmesenteric lymph nodes were enlarged. The small intestineand colonic mucosa were pale and atrophic, but no ulcerationsor perforations were present. No gross lesions were observedin the omentum or other tissues. Examination of samples col-lected at autopsy revealed stages of I. belli in the intestine,mesenteric and mediastinal lymph nodes, liver, and spleen(Fig. 4). The extraintestinal stages were always observed assingle organisms that did not stain with acid-fast stains. Thetissue cyst wall was PAS negative, but the enclosed zoite con-tained PAS-positive granules. The tissue cyst wall did not stainby the Gomori-Grocott method. Massive infection was ob-served in the lymph nodes in association with plasmacytosisand some eosinophils but no granulomatous reaction. Parasiteswere usually grouped in clusters in the paracortical areas or thelumen of the sinus. Few parasites were observed in Kupffercells or within macrophages located in portal areas. No in-volvement of the biliary system was noted. A moderate steato-sis and cholestasis was also observed. The spleen had I. bellitissue cysts in the red and white pulp; the cysts were associatedwith congestion and atrophy of the white pulp.Notable differences in the light microscopic findings in these
two patients are the presence of more than one zoite within atissue cyst observed in the first patient and the lack of PASreactivity of the tissue cyst wall in the second. Additionally, nogranulomatous reaction was observed in the lymph nodes inthe second patient. It was believed that the concurrent cyto-megalovirus infection helped lead to dissemination of the parasitein the first patient. However, cytomegalovirus or other intestinalpathogens were not documented in the second patient.Transmission electron microscopy was used to examine por-
tions of lymph nodes in both patients, and the findings weresimilar. The zoites were in a PV within the cytoplasm of his-tiocytes. Organelles typical of coccidial sporozoites/merozoiteswith a crystalloid body and polysaccharide granules werepresent. An electron-dense granular layer was seen immedi-ately beneath the PV membrane. This layer probably com-posed the tissue cyst wall observed by light microscopy. Theultrastructural features of these tissue cysts observed in thelymph nodes of humans are similar to the tissue cysts observedin mice inoculated with I. felis and I. ohioensis.A recent study (23) examined the submicroscopic appear-
ance of I. belli infection in a 30-year-old white female intrave-nous drug user from Italy who had AIDS. Her symptoms were
FIG. 4. Tissue cysts of I. belli in the spleen of an AIDS patient. A longitudinalview and a cross-section of tissue cysts are present. Note the tissue cyst wall(arrows) and the nucleus (open arrow) of one zoite. Magnification, 31,000.
26 LINDSAY ET AL. CLIN. MICROBIOL. REV.
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

watery, nonbloody diarrhea and fever. She was treated withTMP-SMX, and her diarrhea stopped in 2 days. No otherclinical data were presented. Ultrastructural examination ofsmall intestinal biopsy specimens taken at the duodenojejunaljunction demonstrated trophozoites, merozoites, meronts, andmacrogamonts in epithelial cells. Occasionally, merozoiteswere observed in the intestinal lumen, in the lamina propria,and within lymphatic channels. The demonstration of merozo-ites in lymphatic channels documents a means of their dissem-ination to lymph nodes and to other tissues. The authors con-sidered that their findings of extracellular merozoites mightindicate that I. belli is not strictly an intracellular parasite. Thisconsideration is erroneous, because it is well documented thatmotile stages of Isospora can leave host cells and invade newhost cells (110). This movement is a normal part of the lifecycle, and these fortuitous observations of extracellular stagesare not indicative of extended extracellular survival by theseforms of the parasite. It is interesting that the photomicro-graph of a merozoite in a lymphatic channel (Fig. 6 in refer-ence 23) appears to be a tissue cyst. The merozoite is sur-rounded by electron-dense material identical to that seen intissue cysts in lymph nodes.Asexual and sexual stages and oocysts of I. belli have been
observed in the bile duct epithelium of an AIDS patient withacalculous cholecystitis (8a). No lymph nodes were examinedin this patient, and the relationship between bile duct infec-tions and disseminated infections with tissue cysts is presentlynot known.
Infections in Other Immunocompromised HostsClinical disease in I. belli infections is usually more severe in
immunocompromised patients than in immunocompetent pa-tients. I. belli has been observed in patients with concurrentHodgkin’s disease (16), non-Hodgkin’s lymphoproliferativedisease (72), human T-cell leukemia virus type 1-associatedadult T-cell leukemia (68), and acute lymphoblastic leukemia(189). These patients respond to specific anti-I. belli treatment(see below).It was suggested in one report that treatment with pred-
nisolone (60 mg/day for 13 days) led to transient immunosup-pression and severe I. belli infection in one patient (134). Thepatient recovered without specific treatment.
Infections in Immunocompetent HostsI. belli causes serious and sometimes fatal disease in immu-
nocompetent humans. Symptoms of I. belli infection includediarrhea, steatorrhea, headache, fever, malaise, abdominalpain, vomiting, dehydration, and weight loss (16, 75, 85, 98,179). Blood is not usually present in the feces. Eosinophilia isobserved in some patients. The disease is often chronic, withparasites present in the feces or biopsy specimens for severalmonths to years. Recurrences are common.Experimental infections demonstrate that fever begins 8
days after ingestion of oocysts and lasts for about 8 days (120).Nonbloody diarrhea begins 7 to 9 days after ingestion of oo-cysts. The prepatent period is 10 to 11 days, and oocysts areexcreted for 32 to 38 days. No oocysts were excreted when onevolunteer attempted to reinfect himself 33 days after ingestionof oocysts, indicating that immunity had developed.Disease is more severe in infants (98) and young children
(178) than in adults. A 6-month-old male infant in Californiahad I. belli infection that terminated fatally after 30 weeks ofcontinuous total parental nutrition (98). The disease was char-acterized by severe diarrhea (1 to 3 liters daily) due to cholera-like hypersecretion of intraluminal fluid. Little clinical re-
sponse to surgical, dietary, or antibiotic treatments wasobserved. An 18-month-old female in Thailand was admittedto hospital with severe dehydration, inappetence, and weak-ness (178). She had four or five diarrhetic bowel movementsdaily. She responded to treatment with electrolytes and TMP-SMX, and her diarrhea ceased within 5 days.
Microscopic Lesions Due to I. belli
The main microscopic changes are villous atrophy and crypthyperplasia (16, 149, 179). Eosinophils may be present in thelamina propria in large numbers approaching those seen ineosinophilic enteritis. Plasma cells, lymphocytes, and polymor-phonuclear leukocytes (PMNs) are present in increased num-bers. The lymphatics may be dilated.
Diagnosis
The Sheather sugar flotation method is an excellent methodfor detecting oocysts of I. belli (26, 115). The unsporulatedoocysts of I. belli are readily visible unstained by light micros-copy. Oocysts are in a slightly higher plane of focus than otherparasite cysts or ova (49). Flotation methods are superior todirect fecal smears for detecting oocysts (53). Sedimentationconcentration methods are also more sensitive than directsmears. Charcot-Leyden crystals may (70, 88, 131, 162) or maynot (163) be present in stool samples that contain I. bellioocysts.Stained fecal smears made from concentrated samples may
aid in the detection of I. belli oocysts (17, 92, 115, 137, 145).The modified acid-fast stain produces pink-staining oocyststhat contain bright red sporonts or sporoblasts (137). Oocystsstained by the auramine-rhodamine procedure fluoresce brightyellow (115). When the Giemsa stain is used, both the oocystsand sporoblasts stain pale blue. The heated safranin-methyleneblue technique produces oocysts that are orange-red (17). Thetrichrome stain is of little use (92).Duodenal aspirates (100, 179), the duodenal string test
(190), and small intestinal biopsies (179) are also useful insuspected cases in which oocysts are not found in stool sam-ples. I. belli oocysts are observed in duodenal aspirates and inmucus collected in the string test. Developmental stages of I.belli can be identified in enterocytes in small intestinal biopsyspecimens. Some biopsy samples may be negative for develop-mental stages but contain characteristic lesions. Likewise, oo-cysts may be present in stool samples from some biopsy-neg-ative patients (63). Routine histological staining methods aresatisfactory for demonstrating parasite stages. Many of theparasites will be in vacuoles, making them readily identifiable.I. belli can cause disease with relatively few stages of the par-asite present and can be missed on small intestinal biopsy.
Treatment
Many agents have been used to treat I. belli infections. Com-binations of protozoal dihydrofolate reductase/thymidylatesynthase inhibitors (TMP or pyrimethamine) with sulfon-amides (SMX, sulfadiazine, or sulfadioxine) have generallyproven effective. Treatment with TMP-SMX has been usedmost often (23, 28, 62, 88, 92, 147, 178, 189). One study exam-ined the TMP-SMX treatment of a group of 32 Haitian AIDSpatients. The patients ranged in age from 24 to 55 years old.They had a history of chronic intermittent diarrhea with amean duration of 7.9 months (range, 2 to 26 months). Thediarrhea was liquid, and 2 to 10 stools were excreted a day. Thepatients also had a history of diffuse, crampy abdominal pain,nausea, and intermittent fever. Of the 32 patients, 28 required
VOL. 10, 1997 BIOLOGY OF ISOSPORA SPP. 27
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

oral or intravenous rehydration before or during the first 3days of the study. The patients were treated with oral TMP(160 mg)-SMX (800 mg) four times a day for 10 days. Diarrheaand abdominal pain stopped 1 to 6 days (mean, 2.5 days) aftertreatment. All stool samples examined after the end of treat-ment were negative. At the end of the study, the prophylaxis ofI. belli infection was examined in these patients. Ten patientsreceived placebo orally three times a week, 10 received TMP(160 mg)-SMX (800 mg) orally three times a week, and 12received pyrimethamine (25 mg)-sulfadioxine (500 mg) orallyonce a week. Of the 10 patients given placebo, 5 developedrecurrent I. belli infection in 1 to 3.5 months and were re-treated with TMP-SMX for 10 days with favorable outcomes.None of the patients given pyrimethamine-sulfadioxine hadrelapses, and 1 of the patients given TMP-SMX developed anasymptomatic I. belli infection. Severe pruritus developed in 1patient in each drug treatment group, resulting in the termi-nation of treatment.Pyrimethamine-sulfadoxine has been used less frequently
than TMP-SMX but also gives prompt clinical response andeliminates the parasite when used (70, 133). Pyrimethamine-sulfadiazine is also effective in treating I. belli infection (132,179). Pyrimethamine used alone is also effective in patientswith sulfonamide allergies (186).Macrolide antibiotics have marginal efficacy in treating I.
belli enteritis. Sirimamycin given at 1.5 g twice daily initiallyprovided clinical improvement in a Haitian AIDS patient whodid not respond to TMP-SMX, furazolidone, or tetracyclinetreatments for I. belli enteritis (66). The response to treatmentlasted about a month, and then the patient relapsed. A treat-ment course with pyrimethamine-sulfadiazine was initiated af-ter the relapse, but little improvement was observed. Roxithro-mycin (2.5 mg/kg every 12 h) was used successfully to treat anAfrican AIDS patient who was suffering from chronic I. belli-induced diarrhea that did not respond to TMP-SMX or py-rimethamine treatments (136). Roxithromycin was given orallyfor 15 days, and the diarrhea became intermittent and lesssevere. Although diarrhea requiring hospitalization occurredtwice during the 2 months after treatment, no I. belli oocystswere observed in stool samples.Treatment with anti-giardial agents such as metronidazole,
tinidazole, quinacrine, and furazolidone is probably of littlevalue (19, 175, 179, 186). However, some cases of apparentlysuccessful treatment with metronidazole have been reported(62, 72).Administration of the antimalarial compounds primaquine
phosphate and chloroquine phosphate gave temporary relief ofchronic I. belli infection in an immunocompetent patient aftera 2-week treatment course (179). Intestinal biopsy specimensand duodenal aspirates were negative. The patient relapsed in1 month, and biopsy and aspirate specimens were positive forI. belli.Veterinary anticoccidial drugs have been used with some
success in treating I. belli infections in humans. Amprolium wasused in an AIDS patient in the Netherlands who was sufferingfrom severe diarrhea (181) and for whom treatment with py-rimethamine-sulfadiazine was stopped because of pancytope-nia. Spiramycin had been only partially effective. Amproliumwas given orally beginning at 10 mg/kg and increasing to 90mg/kg. The frequency of diarrhea lessened after 6 days oftreatment. Amprolium treatment was stopped on day 7 be-cause of polyneuropathy but was reinitiated on day 20 at areduced dose of 30 mg/kg. The stool became normal by day 28of treatment, and no oocysts were present after day 35. Dicla-zuril was used in a trial to treat eight AIDS patients with I. bellidiarrhea in Kinshasa, Zaire (89). Each patient received 200 mg
of diclazuril orally for 7 days. Oocysts were eliminated from thestools by 2 to 3 days. Diarrhea completely stopped in four ofthe eight patients, but severe diarrhea persisted in one patient.Oocysts were present in the stools of one of three patientsexamined more than 1 month later. Diarrhea and oocyst ex-cretion recurred at 47 days after treatment.
ISOSPORA INFECTIONS OF NONHUMAN PRIMATES
Little is known about the coccidial infections of nonhumanprimates. Most of the Isospora species recorded are knownonly by their oocyst structure (Table 1).I. callimico was isolated from the feces of a Goeldi’s mar-
moset (Callimico goeldi) at a laboratory animal facility in Bal-timore, Md. (Table 1) (84). The oocysts were excreted for 7days and sporulated in 2 days.I. endocallimici was isolated from the feces of five Goeldi’s
marmosets from the Tulane University Delta Regional Pri-mate Research Center in Louisiana (Table 1) (46). Two of theanimals were born at the center, and three were exported fromPeru. No transmission or life cycle studies have been con-ducted with these species.I. scorzai was isolated from the feces of a Uakari monkey
(Cacajao rubicundus) that was housed in the London Zoo, andthe parasite was transmitted to another monkey, Cebus nigrivit-tatus (2). The life cycle of I. scorzai is not known. Experimen-tally inoculated kittens did not excrete oocysts.I. cebi was isolated from the feces of a Cebus albifrons from
the Alto Magdalena region of Colombia (119). The sporocystsof this species have Stieda bodies, indicating that it is a pseu-doparasite of avian origin. A similar Isospora species was iso-lated from the feces of a Bonnet monkey (Macaca radiata) atthe Delhi Zoo in India but was not named (9).Isospora paponis was isolated from Chacma baboons (Papio
ursinus) (125). Oocysts sporulated endogenously in the smallintestines, indicating that this is a Sarcocystis species. Addition-ally, sporulated oocysts of this species have been seen in theskeletal muscles of Chacma baboons (126). Chimpanzees (Pantroglodytes) can also serve as definitive hosts for Sarcocystisspecies, and reports of Isospora sporocysts in their feces actu-ally describe Sarcocystis sporocysts.
I. arctopitheci Infections
I. arctopitheci has been studied more than the other coccidiaof nonhuman primates (76–78, 140). Hendricks conductedcross-transmission studies with this parasite and claimed tohave successfully transmitted it to members of six genera ofNew World nonhuman primates, four families of carnivores,and one marsupial species (77). This is an unusually large anddiverse definitive host range, and further experimental studiesare needed to confirm or deny these initial findings.The endogenous life cycle of I. arctopitheci occurs in the
small intestine (140). Developmental stages are located in en-terocytes on the distal two-thirds of the villi, and parasitedensities are greatest in the jejunum. Asexual multiplicationwas found to be exclusively by endodyogeny, and eosinophilicbodies were present in gamonts (140). The prepatent periodwas about 7 days, but the patent period was not reported.Extraintestinal stages were not seen in the definitive host.Experimental studies indicate that I. arctopitheci can be
pathogenic (140). Of 13 titi marmosets (Saguinus geoffroyi), 4died after being inoculated with 13 105 to 23 105 oocysts. Noclinical signs were seen in marmosets that died 3 and 5 days p.i.Bloody diarrhea was seen in two marmosets that died 7 daysp.i. All nine other marmosets remained normal. The micro-
28 LINDSAY ET AL. CLIN. MICROBIOL. REV.
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

scopic lesions observed were necrosis of apical enterocyteswith exposure of the lamina propria.
Diagnosis and Treatment
Diagnosis is made by finding the characteristic oocysts (Ta-ble 1) in fecal samples. Fecal flotation with Sheather’s sugarsolution is recommended as a reliable and sensitive technique.Sedimentation or other concentration techniques are also ad-equate.Most Isospora infections in nonhuman primates are subclin-
ical. We are unaware of any reports on the treatment of Iso-spora infections in nonhuman primates. Agents used in hu-mans or veterinary products may be of some value.
ISOSPORA INFECTIONS OF DOGS AND CATS
Infections of Dogs
Several species of Isospora infect dogs (Table 1). Cats arenot the definitive hosts for Isospora species found in dogs (32).Young dogs are more likely to be infected, and surveys indicatethat 3 to 38% of dogs are positive for coccidial oocysts (91).Stray dogs are more likely to be infected than are dogs withowners because stray dogs must hunt for food and thereforehave more exposure to infected paratenic hosts.It is unclear if coccidiosis is a serious problem in dogs (103,
146). Diarrhea associated with the presence of coccidial oo-cysts in young dogs occurs, but the clinical significance is notestablished because of the possibility of concurrent bacterial orviral infections. Published reports of naturally occurring caninecoccidiosis are few (24, 44, 141), and further studies on naturalcases are needed before firm conclusions can be made. Experi-mental infections have not usually been associated with disease.I. canis infections. I. canis has the largest oocysts of the
canine Isospora species and is the only species that can bediagnosed by microscopical examination of oocysts (Table 1).I. canis develops in cells in the lamina propria of the posteriorsmall intestine (93). Three asexual types are present, and thefirst asexual division is probably by endodyogeny. Theprepatent period is 9 days. The length of the patent period hasnot been determined.Disease was not produced in 25 6-week-old or 6 8-week-old
pups inoculated with 1 3 105 to 1.5 3 105 I. canis oocysts (93).Solid immunity follows primary infection, and no oocysts aredischarged after challenge (6). It has been suggested that thestress of weaning and shipping may enhance I. canis infections(93). This suggestion needs further investigation because theseoutbreaks of coccidially associated diarrhea may be related toa decrease in immunity and reactivation of latent extraintesti-nal stages with subsequent intestinal infection and clinical signsof disease.The I. ohioensis complex. Three Isospora species having
smaller oocysts than I. canis can be found in dogs: I. ohioensis,I. burrowsi (Table 1), and I. neorivolta. Because they cannot beseparated based on oocyst structure and because I. ohioensiswas the first named, these oocysts are often referred to as I.ohioensis-like (44) or members of the I. ohioensis complex.I. ohioensis develops in enterocytes in the small intestine,
cecum, and colon of dogs (35). Two asexual types are recog-nized, and division by endodyogeny is observed. The prepatentperiod is 5 days, and the length of the patent period is notknown. The parasite can cause disease in experimentally in-fected 7-day-old pups but not weaned pups or young dogs (36).Diarrhea was the major clinical sign seen in the 7-day-old pups.Microscopic changes were villous atrophy, necrosis of apical
enterocytes, and cryptitis. Dogs developed an immunity thatlasted for about 2 months.I. burrowsi develops in enterocytes and cells in the lamina
propria in the posterior small intestine (180). Two asexualtypes are present. Division by endodyogeny has not been re-corded but probably occurs. The prepatent period is 6 days,and oocysts are excreted for 9 to 15 days.I. neorivolta develops in cells in the lamina propria in the
posterior small intestine (41). Four asexual types are recog-nized, and division by endodyogeny is observed. The prepatentperiod is 6 days, and oocysts are excreted for 13 to 23 days.Little is known about the pathogenesis of I. burrowsi or I.
neorivolta infection in dogs. Neither caused disease in experi-mental infections of dogs (41, 116, 180).Because the significance of diarrhea caused by coccidia in
dogs is unclear, the treatment of the condition is also unclear.Suspected clinical cases can be treated with a variety of drugsused alone or in combination (see below).
Infections of Cats
I. rivolta and I. felis infect cats. Dogs do not serve as defin-itive hosts for these species (159). Both feline Isospora specieshave extraintestinal stages in the feline definitive host and in avariety of paratenic hosts. From 3 to 36% of cats examinedexcrete oocysts (91). Stray cats are more likely to excrete oo-cysts. Coccidiosis in cats is not thought to be a common prob-lem (191) and is usually seen only in naturally infected kittensin which other disease-causing agents may be present. Thedrugs used to treat dogs are used to treat kittens.I. rivolta infections. I. rivolta develops in enterocytes in the
small intestine (38). Three structural types of asexual stagesare present. The first asexual division is by endodyogeny. Theprepatent period is 4 to 7 days, and oocysts are excreted formore than 14 days.Experimentally, I. rivolta can cause disease in newborn kit-
tens (38). Diarrhea occurs 3 to 4 days after administration of1 3 105 or 1 3 106 sporocysts. Microscopic changes consist ofcongestion, erosion of enterocytes, villous atrophy, and crypti-tis. No disease was seen in 10- to 13-week-old kittens inocu-lated with up to 105 oocysts. Cats develop immunity to infec-tion, but it is not complete because some oocysts are shed afterchallenge (38).I. felis infections. I. felis develops in enterocytes in the small
intestine and occasionally the cecum (161). Three structuraltypes of asexual stages are recognized. The first asexual divi-sion is by endodyogeny. The prepatent period is 7 to 11 days,and oocysts are excreted for about 11 days.Experimental studies indicate that I. felis is not pathogenic
for cats over 1 month of age (83, 161). Few signs of disease areseen in 6- to 13-week-old cats given 1 3 105 to 1.5 3 105
oocysts. Mild microscopic changes consisting of congestion,erosion of superficial enterocytes, and neutrophil infiltrationmay be seen. Four-week-old kittens are the most susceptible,and enteritis, emaciation, and death can occur after inocula-tion of 105 oocysts (1).Cats develop immunity to I. felis, because after infection,
they have no or decreased oocyst production when challengedwith I. felis oocysts. Studies indicate that cats infected naturallywith I. felis develop lower antibody titers than do those exper-imentally inoculated with I. felis (142). If these cats are chal-lenged with Toxoplasma gondii, they will develop an antibodytiter to T. gondii and demonstrate an anamnestic response to I.felis antigen. A 22-kDa peptide on sporozoites is the major I.felis protein antigen recognized by immune feline serum (143).Peptides of 22, 45, 58, and 62 kDa on T. gondii tachyzoites or
VOL. 10, 1997 BIOLOGY OF ISOSPORA SPP. 29
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

sporozoites are recognized by I. felis immune feline serum.Absorption of I. felis immune serum with these T. gondii stagesremoves reactivity of the 45-, 58-, and 62-kDa peptides, imply-ing that the 22-kDa peptide is specific to I. felis.I. felis and T. gondii have evolved an unusual relationship in
the feline definitive host (20, 33, 37). Cats that have previouslyrecovered from a T. gondii infection will reexcrete T. gondiioocysts if they receive a primary challenge with I. felis oocysts.Cats that have a primary I. felis infection followed by a primaryT. gondii infection develop strong immunity to T. gondii andwill not reexcrete T. gondii oocysts if challenged with I. felisoocysts. The biological significance or mechanism of this rela-tionship is unknown.
Diagnosis
Fecal flotation with Sheather’s sugar solution is the recom-mended method. It is important to examine stools for bacterialand viral agents that cause disease in these animals becausecoccidiosis is usually asymptomatic. Dogs are coprophagic andoften will have oocysts from other animal feces in their sam-ples. It is important to recognize these pseudoparasites. Themost common of these are Eimeria species from ruminants,rabbits, or rodents. These oocysts will not be in the two-celledstage as is common for Isospora species. They often will haveornamentations, such as micropyle caps or dark thick walls,that are not found on Isospora oocysts. Isospora oocysts thatcontain sporocysts with Stieda bodies are also pseudoparasites.Cats may also have coccidial pseudoparasites in their fecesfrom the ingestion of prey.
Treatment
Sulfadimethoxine given at 50 mg/kg orally once a day for 10to 14 days will eliminate oocyst excretion in most dogs and cats(104, 191). The combination of ormetoprim (11 mg/kg) andsulfadimethoxine (55 mg/kg) given orally for up to 23 days hasbeen used effectively in dogs (45). Amprolium given orallyonce a day at 300 to 400 mg/kg for 5 days or 110 to 220 mg/kgfor 7 to 12 days is effective in treating coccidiosis in dogs. Otheragents such as furazolidone, quinacrine, and metronidazoleprobably are of little clinical value.
ISOSPORA SUIS INFECTIONS OF PIGS
The actual number of valid species of coccidia that infectswine is unknown because most are known only from thesporulated-oocyst stage. Levine and Ivens list 13 named speciesof Eimeria and 3 species of Isospora isolated from swine (97).I. suis, I. almataensis, and I. neyrai are the species of Isosporaisolated from swine. I. almataensis and I. neyrai are known onlyfrom oocysts in the feces. I. almataensis is most probably acombination of a bird Isospora sp. and I. suis.Biester and Murray described I. suis from pigs in 1934 (10–
12). However, it was not recognized as a major cause of diseasein nursing piglets until the early 1970s (167, 171). This probablyreflects the modernization of the swine production industryand the use of confinement facilities for the farrowing (birth-ing) of piglets.
Clinical Signs and Pathogenicity
Coccidiosis in pigs is a severe disease of nursing piglets (52,168). I. suis is the cause of neonatal porcine coccidiosis (167).There are no reports of coccidiosis caused by I. almataensis orI. neyrai. Eimeria species do not cause clinical coccidiosis innursing pigs (106). Neonatal porcine coccidiosis caused by I.
suis is ubiquitous where pigs are farrowed in confinement (21,25, 31, 51, 99, 139, 152, 156, 157) and is responsible for 15 to20% of the cases of piglet diarrhea seen at diagnostic labora-tories in the United States, Canada, and other countries. Out-breaks of coccidiosis occur year-round. I. suis can be seen innursing piglets suffering from other neonatal diarrheal dis-eases, and it increases the severity of disease caused by theseagents (135, 150, 151, 171).Infected piglets develop diarrhea at 7 to 14 days of age. The
diarrhea is yellowish to gray and initially pasty but becomesfluid after 2 to 3 days; blood is never present if I. suis is the onlyinfectious agent. If blood is present, other agents are involvedas primary or copathogens. Piglets become covered with diar-rhetic feces, causing them to stay damp and smell like souredmilk. They become lethargic but continue to nurse. Infectionsfail to respond to commonly used antibiotics. Piglets within alitter and all litters in the farrowing house are not equallyaffected by coccidiosis. Morbidity is high, and mortality is mod-erate. Microscopic changes consist of villous atrophy, villousfusion, necrotic enteritis, and crypt hyperplasia (52, 74, 173,183). Experimental studies indicate that the development ofclinical disease and microscopic lesions are dependent uponthe number of oocysts inoculated and the age at which pigletsare inoculated (13, 86, 112, 153, 172, 173). Doses of 5 3 104
oocysts or less generally produce diarrhea but no mortality inyoung (1- to 3-day-old) piglets, doses of 7 3 104 to 3 3 105
oocysts cause low to moderate mortality, and doses of 4 3 105
or greater cause high mortality in young piglets. Weight gainsof infected piglets are depressed (111).There is some evidence that I. suis may cause postweaning
diarrhea in 5- to 6-week-old piglets (138), with diarrhea begin-ning 4 to 7 days after the piglets are weaned. Morbidity is 80 to90%, but mortality is very low.Endogenous stages are found throughout the small intestine
and occasionally in the cecum and colon (73, 113, 123, 173).Parasite densities are highest in the jejunum and ileum. De-velopmental stages are found in enterocytes. Two types ofmeronts are produced (113). Type 1 meronts are binucleateand divide by endodyogeny (122, 123), whereas type 2 merontsare multinucleate. Both types of meronts are motile and canactively exit and penetrate host cells (110). The prepatentperiod is 4 to 5 days, and the patent period is 2 weeks or longer.Several peaks in oocyst numbers can occur during the patentperiod (21, 73, 184). Extraintestinal stages of I. suis have notbeen found by microscopic examination of tissues from in-fected piglets or in experimentally inoculated mice (73, 123,148, 170). Oral feeding of mouse or pig tissues was inconclusivein one study (170). Transmission occurred following intraper-itoneal inoculation of intestinal lymph node homogenates orhomogenates of pooled spleen and liver from pigs inoculated 1or 2 days previously with large numbers (5 3 107 and 1 3 107
oocysts, respectively) of I. suis oocysts (73). The prepatentperiod was 10 to 12 days in the recipient pigs.The role of viral and bacterial copathogens with I. suis has
been examined experimentally (5, 185). The responses of gno-tobiotic and conventional pigs to I. suis and rotavirus coinfec-tion are similar (185). The degree of observed clinical diseaseis more severe when the pathogens are administered concur-rently than when either is given singly. Both the virus and theparasite develop preferentially in the enterocytes of the centraland distal portion of the villi in the small intestine, and com-petition for a suitable host cell is believed to be the cause of theobserved increase in clinical disease and microscopic lesions.An established I. suis infection will interfere with the estab-lishment of a Salmonella typhimurium infection (5). The in-creased gut motility and destruction of host cells probably
30 LINDSAY ET AL. CLIN. MICROBIOL. REV.
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

interfere with the ability of the bacterium to colonize the in-testinal mucosa.
Immunity
Piglets that recover from I. suis infection exhibit a strongdegree of resistance to reinfection. No clinical signs developafter challenge, and few or no oocysts are excreted in the feces(174). Colostral antibodies against I. suis do not protect pigletsfrom developing clinical coccidiosis (177). Antibody levels inserum peak about 1 week after primary infection, and a sec-ondary antibody response occurs following challenge infection.Serum antibodies against I. suis do not recognize sporozoitesof Eimeria debliecki, E. neodebliecki, E. scabra, or E. porci in anindirect fluorescent-antibody test. Lymphocyte migration inhi-bition responses of pigs that are immune to I. suis are signifi-cantly lower than those of controls when soluble or particulateI. suis sporozoite antigens are used. Polymorphonuclear leu-kocyte (PMN) chemotactic factors were generated by lympho-cytes from piglets inoculated with I. suis and incubated withsoluble or particulate sporozoite antigens. Lymphocytes fromcontrol pigs did not produce chemotactic factors for PMNsafter incubation with I. suis sporozoite antigens, and the anti-gens alone were not chemotactic for PMNs.
Epidemiology
The epidemiology of neonatal porcine isosporiasis is puz-zling. Sows are often infected with Eimeria species, but theprevalence of I. suis is usually less than 5% (50, 69, 114, 182).The sow is a logical source of infection for newborn piglets, butstudies conducted in the United States have failed to demon-strate I. suis oocysts in a significant number of sows (50, 114,168). I. suis oocysts were not found in the feces of 77 sowsexamined from 7 farms with a problem of neonatal coccidiosiscaused by I. suis, and only 1 of 172 sows examined from 27farms without a history of neonatal coccidiosis was positive(114). Eimeria oocysts were found in 91% of these sows. Inanother study, sows from two farms with neonatal coccidiosisin piglets were examined on a daily basis for about 1 week priorto farrowing, at farrowing, and for about 2 weeks postfarrowing(168). I. suis oocysts were not found in these sows; however,piglets nursing from these sows developed coccidiosis and ex-creted I. suis oocysts at 4 to 8 days of age. Microscopic exam-ination of milk samples and placentas from these sows werenegative for parasites. Once I. suis is established on a farm, itis probably maintained by infection of piglets from the con-taminated farrowing crate.
Diagnosis
Diagnosis is based on a clinical history suggestive of coccid-iosis and the demonstration of I. suis oocysts in fecal samplesor the demonstration of developmental stages in mucosalsmears or histological sections obtained from necropsy speci-mens (101). Samples for oocyst identification should be takenfrom pigs that have had diarrhea for 2 days or more becauseclinical signs often appear before oocysts are excreted in thefeces (173). Pasty fecal samples are likely to contain moreoocysts than are liquid samples. Fecal fat makes identificationof oocysts in Sheather’s sugar flotation preparations difficult. Asolution of saturated sodium chloride and glucose has beenrecommended as an alternative flotation medium (79).The use of mucosal imprints stained with any Giemsa-type
stain is a reliable method for diagnosing porcine coccidiosis(101). Imprints should be taken from the jejunum or ileumbecause these are the sites where parasite densities are highest.
The presence of paired merozoites indicative of division byendodyogeny is characteristic for I. suis in pigs (101). Histo-logical sections taken from the jejunum or ileum also containdevelopmental stages in the enterocytes.
Treatment and Control
Anticoccidial treatment of piglets has generally proven un-rewarding. Nursing piglets do not eat or drink enough to makeantibiotics added to feed or water useful. Catching each pigletfor dosing is time-consuming and labor-intensive and probablypractical only on small farms. Controlled studies indicate thatamprolium, monensin, and furazolidone are not effective inpreventing coccidiosis in nursing piglets (29, 67). Toltrazurildoes show promise as an effective means of preventing coccidiosisin nursing piglets (30). When 20 to 30 mg of toltrazuril/kg wasgiven orally as a single dose to 3- to 6-day-old piglets, coccidiosiswas reduced from 71 to 22%. The severity of diarrhea and oocystexcretion was reduced in toltrazuril-treated piglets.Lasalocid and halofuginone have been evaluated in early-
weaned pigs experimentally infected with I. suis (118, 124).Lasalocid given at 150 mg/kg of feed prevented weight loss inpigs but did not prevent oocyst excretion. These pigs developedstrong immunity to reinfection. Halofuginone given at 6 mg/kgof feed inhibited oocyst production but caused reduced weightgains due to poor feed intake. The halofuginone-treated pigsdid not develop strong immunity to challenge infection.Improved sanitation is the best means of controlling neona-
tal coccidiosis (50). Feeding anticoccidial agents to sows is notrecommended because they are not the source of fecal oocystsfor their nursing piglets. Commercially available disinfectantsdo not inhibit the development of I. suis oocysts when used atthe concentrations recommended by the manufacturers (169).Once the oocysts sporulate, they are even more resistant todisinfectants. Steam cleaning is effective in killing sporulatedand unsporulated oocysts and is an effective means of decreas-ing piglet exposure to infective I. suis oocysts. Additional pre-ventive measures are for farm workers to limit their access toinfected piglets to prevent crate-to-crate spread of infection viatheir boots. Also, flies and other insects should be controlled toprevent them from mechanically carrying oocysts from crate tocrate. Supportive measures such as providing water or electro-lyte solutions in piglet waters may be of value in preventingdehydration in clinically infected piglets.
FUTURE DIRECTIONS
Future studies on human I. belli infections need to examinethe latent tissue cyst stage of the parasite. It is most probablyresponsible for the recrudescence of clinical disease which isobserved in AIDS and other patients. It is obvious that thetissue cyst stage is not killed by treatment with TMP-SMX. Anin vitro culture system needs to be developed to examine po-tential anticoccidial agents against I. belli and to study tissuecyst biology. Experimental inoculation of rodents with I. bellioocysts needs to be examined to determine whether latentinfections develop in these animals. If rodents are found to beparatenic hosts, potentially other food animals may also becapable of transmitting the infection.Additional studies on dog and cat Isospora spp. should be
conducted to determine if these coccidia are truly pathogenicin them. Studies with neonatal porcine coccidiosis should focuson identifying effective treatments and vaccines.
REFERENCES
1. Andrews, J. M. 1926. Coccidiosis in mammals. Am. J. Hyg. 6:784–794.2. Arcay, L. 1967. Coccidiosis en monos y su comparacion con la isosporosis
VOL. 10, 1997 BIOLOGY OF ISOSPORA SPP. 31
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

humana, con description de una nueva especie de Isospora en Cacajaorubicundus (Uakari monkey o mono chucuto). Acta Biol. Venez. 5:203–222.
3. Arcay, L. 1981. Nuevo coccidia de gato: Cystoisospora frenkeli sp. nova(Toxoplasmatinae) y su desarrollo en la membrana corioalantoidea deembrion de pollo. Acta Cient. Venez. 32:401–410.
4. Ashford, R. W. 1979. Occurrence of an undescribed coccidian in man inPapua New Guinea. Ann. Trop. Med. Parasitol. 73:497–500.
5. Baba, E., and S. M. Gaffer. 1985. Interfering effect of Isospora suis infec-tions on Salmonella typhimurium infection in swine. Vet. Parasitol. 17:271–278.
6. Becker, C., J. Heine, and J. Boch. 1981. Experimentelle Cystoisospora canis-und C. ohioensis-Infectionen beim Hund. Tieraerztl. Umsch. 36:1–8.
7. Becker, E. R. 1934. Coccidia and coccidiosis of domesticated, game andlaboratory animals and of man. Collegiate Press, Inc., Ames, Iowa.
8. Becker, E. R. 1954. The host affinities of Isospora bigemina-type coccidia.Iowa Acad. Sci. 61:463–467.
8a.Benator, D. A., A. L. French, L. M. Beaudet, C. S. Levy, and J. M. Oren-stein. 1994. Isospora belli infection associated with acalculous cholecystitisin a patient with AIDS. Ann. Int. Med. 121:633–634.
9. Bhattia, B. B., P. P. Chauhan, G. S. Arora, and R. D. Agrawal. 1972.Observations on some coccidian infections in birds and a mammal at theDelhi Zoo. Indian J. Anim. Sci. 42:625–628.
10. Biester, H. E. 1934. Isospora suis, N. sp. from the pig, p. 106–107. In E. R.Becker (ed.), Coccidia and coccidiosis of domesticated, game and labora-tory animals and of man. Collegiate Press, Inc., Ames, Iowa.
11. Biester, H. E., and C. Murray. 1934. The occurrence of Isospora suis N. sp.in swine. A preliminary note. J. Am. Vet. Med. Assoc. 84:294.
12. Biester, H. E., and C. Murray. 1934. Studies in infectious enteritis of swine.VII. Isospora suis n. sp. in swine. J. Am. Vet. Med. Assoc. 85:207–219.
13. Blagburn, B. L., T. R. Boosinger, and T. A. Powe. 1991. ExperimentalIsospora suis infections in miniature swine. Vet. Parasitol. 38:343–347.
14. Boch, J., E. Goebel, J. Heine, and M. Erber. 1981. Isospora-infektionen beiHund und Katze. Berl. Muench. Tieraertzl. Wochenschr. 94:384–391.
15. Box, E. D., A. A. Marchiondo, D. W. Duszynski, and C. P. Davis. 1980.Ultrastructure of Sarcocystis sporocysts from passerine birds and opossums:comments on classification of the genus Isospora. J. Parasitol. 66:68–74.
16. Brandborg, L. L., S. B. Goldberg, and W. C. Breidenbach. 1970. Humancoccidiosis—a possible cause of malabsorption: the life cycle in small-bowelmucosal biopsies as a diagnostic feature. N. Engl. J. Med. 283:1306–1313.
17. Bush, J. B., and M. B. Markus. 1987. Staining of Isospora belli oocysts.Trans. R. Soc. Trop. Med. Hyg. 81:244. (Letter.)
18. Bunyaratvej, S., P. Bunyawongwiroj, and P. Nitiyanant. 1982. Human in-testinal sarcosporidiosis: report of six cases. Am. J. Trop. Med. Hyg. 31:36–41.
19. Butler, T., and W. G. R. deBoer. 1981. Isospora belli infection in Australia.Pathology 13:593–595.
20. Chessum, B. S. 1972. Reactivation of Toxoplasma oocyst production in thecat infected with Isospora felis. Br. Vet. J. 128:33–36.
21. Christensen, J. P. B., and S. A. Henriksen. 1994. Shedding of oocysts inpiglets experimentally infected with Isospora suis. Acta Vet. Scand. 35:165–172.
22. Christie, E., P. W. Pappas, and J. P. Dubey. 1978. Ultrastructure of excyst-ment of Toxoplasma gondii oocysts. J. Protozool. 25:438–443.
23. Comin, C. E., and M. Santucci. 1994. Submicroscopic profile of Isosporabelli enteritis in a patient with acquired immune deficiency syndrome. Ul-trastruct. Pathol. 18:473–482.
24. Correa, W. M., C. N. M. Correa, H. Langoni, O. A. Volpato, and K.Tsunoda. 1983. Canine isoporosis. Canine Pract. 10:44–46.
25. Coussement, W., R. Ducatelle, G. Geeraerts, and P. Berghen. 1981. Babypig diarrhea caused by coccidiosis. Vet. Q. 3:57–60.
26. Current, W. L. 1990. Techniques and laboratory maintenance of Crypto-sporidium, p. 31–49. In J. P. Dubey, C. A. Speer, and R. Fayer (ed.),Cryptosporidiosis of man and animals. CRC Press, Inc., Boca Raton, Fla.
27. Daly, T. J. M., and M. Markus. 1981. Enteric multiplication of Isospora felisby endodyogeny. Proc. Electron Microsc. Soc. South. Afr. Proc. 11:99.
28. DeHovitz, J. A., J. Pape, M. Boncy, and W. D. Johnson. 1986. Clinicalmanifestations and therapy of Isospora belli infection in patients with theacquired immunodeficiency syndrome. N. Engl. J. Med. 315:87–90.
29. Dore, M., and M. Morin. 1987. Porcine neonatal coccidiosis: evaluation ofmonensin as preventive therapy. Can. Vet. J. 28:663–666.
30. Driesen, S. J., V. A. Fahy, and P. G. Carland. 1995. The use of toltrazurilfor the prevention of coccidiosis in piglets before weaning. Aust. Vet. J.72:139–141.
31. Dubey, J. P. 1975. Experimental Isospora canis and Isospora felis infectionin mice, cats, and dogs. J. Protozool. 22:416–417.
32. Dubey, J. P. 1975. Isospora ohioensis sp. n. proposed for I. rivolta of the dog.J. Parasitol. 61:462–465.
33. Dubey, J. P. 1976. Reshedding of Toxoplasma oocysts by chronically in-fected cats. Nature 262:213–214.
34. Dubey, J. P. 1977. Toxoplasma, Hammondia, Besnoitia, Sarcocystis, andother tissue cyst-forming coccidia of man and animals, p. 101–237. In J. P.Krier (ed.), Parasitic protozoa, vol. 3. Academic Press, Inc., New York,N.Y.
35. Dubey, J. P. 1978. Life cycle of Isospora ohioensis in dogs. Parasitology77:1–11.
36. Dubey, J. P. 1978. Pathogenicity of Isospora ohioensis infection in dogs. J.Am. Vet. Med. Assoc. 173:192–197.
37. Dubey, J. P. 1978. Effect of immunization of cats with Isospora felis andBCG on immunity to reexcretion of Toxoplasma gondii oocysts. J. Proto-zool. 25:380–382.
38. Dubey, J. P. 1979. Life cycle of Isospora rivolta (Grassi 1879) in cats andmice. J. Protozool. 26:433–443.
39. Dubey, J. P., and R. Fayer. 1976. Development of Isospora bigemina in dogsand other mammals. Parasitology 73:371–380.
40. Dubey, J. P., and J. K. Frenkel. 1972. Extra-intestinal stages of Isospora felisand I. rivolta (Protozoa: Eimeriidae) in cats. J. Protozool. 19:89–92.
41. Dubey, J. P., and J. L. Mahrt. 1978. Isospora neorivolta sp. n. from thedomestic dog. J. Parasitol. 64:1067–1073.
42. Dubey, J. P., and H. Mehlhorn. 1978. Extraintestinal stages of Isosporaohioensis from dogs in mice. J. Parasitol. 64:689–695.
43. Dubey, J. P., and R. H. Streitel. 1976. Isospora felis and I. rivolta infectionsin cats induced by mouse tissue or oocysts. Br. Vet. J. 132:649–651.
44. Dubey, J. P., S. E. Weisbrode, and W. A. Rogers. 1978. Canine coccidiosisattributed to an Isospora ohioensis-like organism: a case report. J. Am. Vet.Med. Assoc. 173:185–191.
45. Dunbar, M. R., and W. J. Foreyt. 1985. Prevention of coccidiosis in domes-tic dogs and captive coyotes (Canis latrans) with sulfadimethoxine-ormetoprim combination. Am. J. Vet. Res. 46:1899–1902.
46. Duszynski, D. W., and S. K. File. 1974. Structure of the oocyst and excys-tation of Isospora endocallimici n. sp., from the marmoset Callimico goeldii.Trans. Am. Microsc. Soc. 93:403–408.
47. Duszynski, D. W., and C. A. Speer. 1976. Excystation of Isospora arctopitheciRodhain, 1933 with notes on a similar process in Isospora bigemina (Stiles1891) Luhe 1906. Z. Parasitenkd. 48:191–197.
48. Elsdon-Dew, R. 1953. Isospora natalensis (sp. nov.) in man. J. Trop. Med.Hyg. 56:149–150.
49. Elsdon-Dew, R., and L. Freedman. 1953. Coccidiosis in man: experiences inNatal. Trans. R. Soc. Trop. Med. Hyg. 47:209–214.
50. Ernst, J. V., D. S. Lindsay, and W. L. Current. 1985. Control of Isosporasuis-induced coccidiosis on a swine farm. Am. J. Vet. Res. 46:643–645.
51. Eysker, M., G. A. Boerdam, W. Hollanders, and J. H. M. Verheijden. 1994.The prevalence of Isospora suis and Strongyloides ransomi in suckling pigletsin the Netherlands. Vet. Q. 16:203–205.
52. Eustis, S. L., and D. T. Nelson. 1981. Lesions associated with coccidiosis innursing piglets. Vet. Pathol. 18:21–28.
53. Faust, E. C., L. E. Giraldo, G. Giraldo, and R. Bonfante. 1961. Humancoccidiosis in the western hemisphere. Am. J. Trop. Med. Hyg. 10:343–350.
54. Fayer, R. 1972. Cultivation of feline Isospora rivolta in mammalian cells. J.Parasitol. 58:1207–1208.
55. Fayer, R., and J. K. Frenkel. 1979. Comparative infectivity for calves ofoocysts of feline coccidia: Besnoitia, Hammondia, Cystoisospora, Sarcocystis,and Toxoplasma. J. Parasitol. 65:756–762.
56. Fayer, R., and J. L. Mahrt. 1972. Development of Isospora canis (Protozoa:Sporozoa) in cell cultures. Z. Parasitenkd. 38:313–318.
57. Fayer, R., and D. E. Thompson. 1974. Isospora felis: development in cul-tured cells with some cytological observations. J. Parasitol. 60:160–168.
58. Fayer, R., H. R. Gamble, and J. V. Ernst. 1984. Isospora suis: developmentin cultured cells with some cytological observations. Proc. Helminthol. Soc.Wash. 51:154–159.
59. Ferguson, D. J. P., A. Birch-Anderson, W. M. Hutchinson, and J. C. Siim.1980. Ultrastructural observations on multiplication of Cystoisospora (Isos-pora) felis by endodyogeny. Z. Parasitenkd. 63:289–291.
60. Ferguson, D. J. P., A. Birch-Anderson, W. M. Hutchinson, and J. C. Siim.1980. Ultrastructural observations on microgametogenesis and the struc-ture of the microgamete of Isospora felis. Acta Pathol. Microbiol. Scand.Sect. B 88:151–159.
61. Foner, A. 1939. An attempt to infect animals with Isospora belli. Trans. R.Soc. Trop. Med. Hyg. 33:357–358.
62. Forthal, D., and S. S. Guest. 1984. Isospora belli enteritis in three homo-sexual men. Am. J. Trop. Med. Hyg. 33:1060–1064.
63. French, J. M., J. J. Whitby, and A. G. W. Whitfield. 1964. Steatorrhea in aman infected with coccidiosis (Isospora belli). Gastroenterology 47:642–648.
64. Frenkel, J. K. 1977. Besnoitia wallacei of cats and rodents: with a reclassi-fication of other cyst-forming isosporid coccidia. J. Parasitol. 63:611–628.
65. Frenkel, J. K., and J. P. Dubey. 1972. Rodents as vectors for the felinecoccidia, Isospora felis and Isospora rivolta. J. Infect. Dis. 125:69–72.
66. Gaska, J. A., K. J. Tietze, and E. M. Cosgrove. 1985. Unsuccessful treat-ment of enteritis due to Isospora belli with spiramycin: a case report. J. In-fect. Dis. 152:1336–1338.
67. Girard, C., and M. Morin. 1987. Amprolium and furazolidone as preventivetreatment for intestinal coccidiosis of piglets. Can. Vet. J. 28:667–669.
68. Greenberg, S. J., M. P. Davey, W. S. Zierdt, and T. A. Waldmann. 1988.Isospora belli infection in patients with human T-cell leukemia virus typeI-associated adult T-cell leukemia. Am. J. Med. 85:435–438.
69. Greiner, E. C., C. Taylor, W. B. Frankenberger, and R. C. Belden. 1982.
32 LINDSAY ET AL. CLIN. MICROBIOL. REV.
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

Coccidia of feral swine from Florida. J. Am. Vet. Med. Assoc. 181:1275–1277.70. Guisantes, J. A., S. Rull, M. F. Rubio, J. P. Tobalina, and E. de Landazuri.
1982. Human coccidiosis by Isospora belli and malabsorption. Rev. Iber.Parasitol. 42:223–230.
71. Gutierrez, F., and L. Arcay. 1987. Cultivo de Cystoisospora felis Frenkel,1977 (Isospora felis Wasielewski, 1904, Wenyon, 1923) en la membranacorioalantoidea de embrion de pollo. Acta Cient. Venez. 38:474–483.
72. Hallak, A., I. Yust, Y. Ratan, and U. Adar. 1982. Malabsorption syndrome,coccidiosis, combined immune deficiency, and fulminant lymphoprolifera-tive disease. Arch. Intern. Med. 142:196–197.
73. Harleman, J. H., and R. C. Meyer. 1984. Life cycle of Isospora suis ingnotobiotic and conventional piglets. Vet. Parasitol. 17:27–39.
74. Harleman, J. H., and R. C. Meyer. 1985. Pathogenicity of Isospora suis ingnotobiotic and conventional piglets. Vet. Rec. 116:561–565.
75. Henderson, H. E., G. W. Gillepsie, P. Kaplan, and M. Steber. 1963. Thehuman Isospora. Am. J. Hyg. 78:302–309.
76. Hendricks, L. D. 1974. A redescription of Isospora arctopitheci Rhodhain,1933 (Protozoa: Eimeriidae) from primates of Panama. Proc. Helminthol.Soc. Wash. 41:229–233.
77. Hendricks, L. D. 1977. Host range characteristics of the primate coccidian,Isospora arctopitheci Rodhain 1933 (Protozoa: Eimeriidae). J. Parasitol.63:32–35.
78. Hendricks, L. D., and B. C. Walton. 1974. Vertebrate intermediate hosts inthe life cycle of an isosporan from a non-human primate. Proc. Int. Congr.Parasitol. 1:96–97.
79. Henriksen, S. A., and J. P. B. Christensen. 1992. Demonstration of Isosporasuis oocysts in faecal samples. Vet. Rec. 131:443–444.
80. Henry, M. C., D. DeClercq, B. Lokombe, K. Kayembe, B. Kapita, K.Mamba, N. Mbendi, and P. Mazebo. 1986. Parasitological observations ofchronic diarrhoea in suspected AIDS adult patients in Kinshasa (Zaire).Trans. R. Soc. Trop. Med. Hyg. 80:309–310.
81. Heydorn, A. O., R. Gestrich, and V. Ipczynski. 1975. Zum Lebenszyklus derkleinen Form von Isospora bigemina des Hundes. II. Entwicklungsstadienim Darm des Hundes. Berl. Muench. Tieraerztl. Wochenschr. 88:449–453.
82. Hilali, M., A. M. Nassar, and A. El-Ghaysh. 1992. Camel (Camelus drom-edarius) and sheep (Ovis aries) meat as a source of dog infection with somecoccidian parasites. Vet. Parasitol. 43:37–43.
83. Hitchcock, D. J. 1955. The life cycle of Isospora felis in the kitten. J.Parasitol. 41:383–397.
84. Hsu, C., and E. C. Melby. 1974. Isospora callimico n sp, (Coccidia: Eimeri-idae) from Goeldi’s marmoset (Callimico goeldii). Lab. Anim. Sci. 24:476–477.
85. Jarpa Gana, A. 1966. Coccidiosis humana. Biologica (Santiago) 39:3–26.86. Jarvinen, J. A. C., G. L. Zimmerman, D. J. Schons, and C. Guenther. 1988.
Serum proteins of neonatal pigs orally inoculated with Isospora suis oocysts.Am. J. Vet. Res. 49:380–385.
87. Jeffery, G. M. 1956. Human coccidiosis in South Carolina. J. Parasitol.42:491–495.
88. Junod, C., M. Nault, and M. Copet. 1988. La coccidiosis a Isospora belli chezles sujets immuno-competents. Bull. Soc. Pathol. Exot. 81:317–325.
89. Kayembe, K., P. Desmet, M. C. Henery, and P. Stoffels. 1989. Diclazuril forIsospora belli infection in AIDS. Lancet i:1397–1398.
90. Kirkpatrick, C. E. 1988. Animal reservoirs of Cryptosporidium parvum andIsospora belli. J. Infect. Dis. 158:909. (Letter.)
91. Kirkpatrick, C. E., and J. P. Dubey. 1987. Enteric coccidial infectionsIsospora, Sarcocystis, Cryptosporidium, Besnoitia, and Hammondia. Vet.Clin. North Am. Small Anim. Pract. 17:1405–1420.
92. Kobayashi, L. M., M. P. Kort, O. G. W. Berlin, and D. A. Bruckner. 1985.Isospora infection in a homosexual man. Diagn. Microbiol. Infect. Dis.3:363–366.
93. Lepp, D. L., and K. S. Todd. 1974. Life cycle of Isospora canis Nemeseri,1959 in the dog. J. Protozool. 21:199–206.
94. Lepp, D. L., and K. S. Todd. 1976. Sporogony of the oocysts of Isosporacanis. Trans. Am. Microsc. Soc. 95:89–103.
95. Levine, N. D. 1988. The Protozoan Phylum Apicomplexa, vol. 1, CRC Press,Inc., Boca Raton, Fla.
96. Levine, N. D., and V. Ivens. 1965. Isospora species in the dog. J. Parasitol.51:859–864.
97. Levine, N. D., and V. Ivens. 1986. The coccidian parasites (Protozoa, Api-complexa) of artiodactyla. Ill. Biol. Monogr. 55:3–20.
98. Liebman, W. M., M. M. Thaler, A. DeLorimier, L. L. Brandborg, and J.Goodman. 1980. Intractable diarrhea of infancy due to intestinal coccidio-sis. Gastroenterology 78:579–584.
99. Lima, J. D., N. E. Martins, A. R. S. de Olivera, and L. P. Boretti. 1983.Coccidiose em Leitoes Lactentes de Minas Gerais. Arq. Bras. Med. Vet.Zootec. 35:33–40.
100. Limbos, P., G. VanRos, and A. DeMuynck. 1972. Deux noveaux cas decoccidiose a Isospora belli observes in Belgique. Bull. Soc. Pathol. Exot.65:288–292.
101. Lindsay, D. S. 1989. Diagnosing and controlling Isospora suis in nursingpigs. Vet. Med. 83:443–448.
102. Lindsay, D. S., and B. L. Blagburn. 1987. Development of Isospora suis
from pigs in primary porcine and bovine cell cultures. Vet. Parasitol. 24:301–304.
103. Lindsay, D. S., and B. L. Blagburn. 1991. Coccidial parasites of cats anddogs. Comp. Contin. Ed. Pract. Vet. 13:759–765.
104. Lindsay, D. S., and B. L. Blagburn. 1995. Practical treatment and control ofinfections caused by canine gastrointestinal parasites. Vet. Med. 89:441–455.
105. Lindsay, D. S., and W. L. Current. 1984. Complete development of Isosporasuis of swine in chicken embryos. J. Protozool. 31:152–155.
106. Lindsay, D. S., B. L. Blagburn, and T. R. Boosinger. 1987. ExperimentalEimeria debliecki infections in nursing and weaned pigs. Vet. Parasitol.25:39–45.
107. Lindsay, D. S., B. L. Blagburn, and M. A. Toivio-Kinnucan. 1991. Ultra-structure of developing Isospora suis in cultured cells. Am. J. Vet. Res.52:471–473.
108. Lindsay, D. S., W. L. Current, and J. V. Ernst. 1982. Sporogony of Isosporasuis Biester, 1934 of swine. J. Parasitol. 68:861–865.
109. Lindsay, D. S., W. L. Current, and J. V. Ernst. 1983. Excystation of Isosporasuis Biester, 1934 of swine. Z. Parasitenkd. 69:27–34.
110. Lindsay, D. S., W. L. Current, and J. V. Ernst. 1983. Motility of Isosporasuis meronts. J. Parasitol. 69:783–784.
111. Lindsay, D. S., W. L. Current, and J. R. Taylor. 1985. Effects of experi-mental Isospora suis infection on morbidity, mortality, and weight gains ofnursing pigs. Am. J. Vet. Res. 46:1511–1512.
112. Lindsay, D. S., B. L. Blagburn, J. V. Ernst, and W. L. Current. 1985.Experimental coccidiosis (Isospora suis) in a litter of feral piglets. J. Wildl.Dis. 21:309–310.
113. Lindsay, D. S., B. P. Stuart, B. E. Wheat, and J. V. Ernst. 1980. Endogenousdevelopment of the swine coccidium, Isospora suis Biester 1934. J. Parasitol.66:771–779.
114. Lindsay, D. S., J. V. Ernst, W. L. Current, B. P. Stuart, and T. B. Stewart.1984. Prevalence of oocysts of Isospora suis and Eimeria spp. from sows onfarms with and without a history of neonatal coccidiosis. J. Am. Vet. Med.Assoc. 185:419–421.
115. Ma, P., D. Kaufman, and J. Montana. 1984. Isospora belli diarrheal infec-tion in homosexual men. AIDS Res. 1:327–338.
116. Mahrt, J. L. 1967. Endogenous stages of the life cycle of Isospora rivolta inthe dog. J. Protozool. 14:754–759.
117. Mahrt, J. L. 1968. Sporogony of Isospora rivolta oocysts from the dog. J.Protozool. 15:308–312.
118. Manner, K., F. R. Matuschka, and J. Seehawer. 1981. Einflub einerMonoinfection mit Isospora suis und ihre Behandlung mit Halofuginon undLasalocid auf die Aufzuchtleistungen, Verdauungskoeffizienten und diestoffliche Zusammensetzung der Ganztierkorper fruhabgesetzter Ferkel.Berl. Muench. Tieraerztl. Wochenschr. 94:25–33.
119. Marinkelle, C. J. 1969. Isospora cebi sp. n. aislada de un mico de Colombia(Cebus albifronis). Rev. Bras. Biol. 29:35–40.
120. Matsubayashi, H., and T. Nozawa. 1948. Experimental infection of Isosporahominis in man. Am. J. Trop. Med. Hyg. 28:633–637.
121. Matsui, T., S. Ito, T. Fujinio, and T. Morii. 1993. Infectivity and sporogonyof Caryospora-type oocysts of Isospora rivolta obtained by heating. Parasitol.Res. 79:599–602.
122. Matuschka, F. R. 1982. Ultrastructural evidence of endodyogeny in Iso-spora suis from pigs. Z. Parasitenkd. 67:27–30.
123. Matuschka, F. R., and A. O. Heydorn. 1980. Die Entwicklung von Isosporasuis Biester 1934 (Sporozoa: Coccidia: Eimeriidae) im Schwein. Zool. Beitr.26:405–476.
124. Matuschka, F. R., and K. Manner. 1981. Die Entwicklung experimentellmit Isospora suis infizierter Absatzferkel als Modellfall fur die Wirksamkeitvon Lasalocid und Halofuginon auf Kokzidien. Zentralbl. Bakteriol. Mik-robiol. Hyg. 1 Abt Orig. A 248:565–574.
125. McConnell, E. E., A. J. De Vos, P. A. Basson, and V. De Vos. 1971. Isosporapapionis n. sp. (Eimeriidae) of the Chacma baboon Papio ursinus. J. Pro-tozool. 18:28–32.
126. McConnell, E. E., P. A. Basson, S. E. Thomas, and V. De Vos. 1972. Oocystsof Isospora papionis in the skeletal muscles of Chacma baboons. Onder-stepoort J. Vet. Res. 39:113–116.
127. McCracken, A. W. 1972. Natural and laboratory-acquired infection by Iso-spora belli. South. Med. J. 65:800–801.
128. McKenna, P. B., and W. A. G. Charleston. 1982. Activation and excystationof Isospora felis and Isospora rivolta sporozoites. J. Parasitol. 68:276–286.
129. Mehlhorn, H., and M. B. Markus. 1976. Electron microscopy of stages ofIsospora felis of the cat in the mesenteric lymph node of the mouse. Z.Parasitenkd. 51:15–24.
130. Michiels, J. F., P. Hofman, E. Bernard, M. C. St. Paul, C. Boissy, V.Mondain, Y. LeFichoux, and R. Loubiere. 1994. Intestinal and extraintes-tinal Isospora belli infection in an AIDS patient. Pathol. Res. Pract. 190:1089–1093.
131. Miller, F. H., A. V. Pizzuto, and H. McCauley. 1971. Human isosporosis:two cases. Am. J. Trop. Med. Hyg. 20:23–25.
132. Modigliani, R., C. Bories, Y. L. Charpenter, M. Salmerson, B. Messing, A.Galian, J. C. Rambaud, A. Lavergne, B. C. Priollet, and I. Desportes. 1985.Diarrhoea and malabsorption in acquired immune deficiency syndrome: a
VOL. 10, 1997 BIOLOGY OF ISOSPORA SPP. 33
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from

study of four cases with special emphasis on opportunistic protozoan infes-tations. Gut 26:179–187.
133. Mojon, M., J. Coudert, and E. O. de Landazuri. 1981. Serious isosporosisby Isospora belli: a case report treated by fansidar. Southeast Asian J. Trop.Med. Public Health 12:449–500.
134. Morakote, N., Y. Muangyimpong, P. Somboon, and C. Khamboonruang.1987. Acute human isosporiasis in Thailand: a case report. Southeast AsianJ. Trop. Med. Public Health 18:107–111.
135. Morin, M., D. Turgeon, J. Jolette, Y. Robinson, J. B. Phaneuf, R. Sau-vageau, M. Beauregard, E. Teuscher, R. Higgins, and S. Lariviere. 1983.Neonatal diarrhea of pigs in Quebec: infectious causes of significant out-breaks. Can. J. Comp. Med. 47:11–17.
136. Musey, K. L., C. Chidiac, G. Beaucaire, S. Houriez, and A. Fourrier. 1988.Effectiveness of roxithromycin for treating Isospora belli infection. J. Infect.Dis. 158:646. (Letter.)
137. Ng, E., E. K. Markell, R. L. Fleming, and M. Fried. 1984. Demonstration ofIsospora belli by acid-fast stain in a patient with acquired immune deficiencysyndrome. J. Clin. Microbiol. 20:384–386.
138. Nilsson, O. 1988. Isospora suis in pigs with post weaning diarrhoea. Vet.Rec. 122:310–311. (Letter.)
139. Nilsson, O., K. Martinsson, and E. Persson. 1984. Epidemiology of porcineneonatal steatorrhea in Sweden. 1. Prevalence and clinical significance ofcoccidial and rotaviral infections. Nord. Vet. Med. 36:103–110.
140. Olcott, A. T., C. A. Speer, and L. D. Hendricks. 1982. Endogenous devel-opment of Isospora arctopitheci Rodhain, 1933 in the marmoset Saguinusgeoffroyi. Proc. Helminthol. Soc. Wash. 49:118–126.
141. Olson, M. E. 1985. Coccidiosis caused by Isospora ohioensis-like organismsin three dogs. Can. Vet. J. 26:112–114.
142. Omata, Y., H. Oikawa, M. Kanda, K. Mikazuki, T. Takehara, C. Venturini,A. Saito, and N. Suzuki. 1991. Enhancement of humoral immune responseof Isospora felis-infected cats after inoculation with Toxoplasma gondii. J.Vet. Sci. 53:161–165.
143. Omata, Y., H. Oikawa, M. Kanda, K. Mikazuki, T. Takehara, C. Venturini,A. Saito, and N. Suzuki. 1991. Humoral immune response to Isospora felisand Toxoplasma gondii in cats experimentally inoculated with Isospora felis.J. Vet. Sci. 53:1071–1073.
144. Ortega, Y. R., R. H. Gilman, and C. R. Sterling. 1994. A new coccidianparasite (Apicomplexa: Eimeriidae) from humans. J. Parasitol. 80:625–629.
145. Pape, J. W., R. I. Verdier, and W. D. Johnson. 1989. Treatment and pro-phylaxis of Isospora belli infection in patients with the acquired immuno-deficiency syndrome. N. Engl. J. Med. 320:1044–1047.
146. Penzhorn, B. L., K. G. M. DeCramer, and L. M. Booth. 1992. Coccidialinfection in German shepherd dog pups in a breeding unit. J. S. Afr. Vet.Assoc. 63:27–29.
147. Peters, C. S., S. B. Kathpalia, A. L. Chittom-Swiatlo, C. A. Kallick, R.Sherer, and F. E. Kocka. 1987. Isospora belli and Cryptosporidium sp. froma patient not suspected of having acquired immunodeficiency syndrome.Diagn. Microbiol. Infect. Dis. 8:197–199.
148. Pinckney, R. D., D. S. Lindsay, M. A. Toivio-Kinnucan, and B. L. Blagburn.1993. Ultrastructure of Isospora suis during excystation and attempts todemonstrate extraintestinal stages in mice. Vet. Parasitol. 47:225–233.
149. Restrepo, C., A. M. Macher, and E. H. Radany. 1987. Disseminated ex-traintestinal isosporiasis in a patient with acquired immune deficiency syn-drome. Am. J. Clin. Pathol. 87:536–542.
150. Roberts, L., and E. J. Walker. 1982. Field study of coccidial and rotaviraldiarrhoea in unweaned piglets. Vet. Rec. 110:11–13.
151. Roberts, L., E. J. Walker, D. R. Snodgrass, and K. W. Angus. 1980. Diar-rhoea in unweaned piglets associated with rotavirus and coccidial infec-tions. Vet. Rec. 107:156–157.
152. Robinson, Y., and M. Morin. 1982. Porcine neonatal coccidiosis in Quebec.Can. Vet. J. 23:212–216.
153. Robinson, Y., M. Morin, C. Girard, and R. Higgins. 1983. Experimentaltransmission of intestinal coccidiosis to piglets: clinical, parasitological andpathological findings. Can. J. Comp. Med. 47:401–407.
154. Rommel, M., and B. Zielasko. 1981. Untersuchungen uber den Lebenszyk-lus von Isospora burrowsi (Trayser and Todd, 1978) aus dem Hund. Berl.Muench. Tieraerztl. Wochenschr. 94:87–90.
155. Ros, E., J. Fueyo, J. Llach, A. Moreno, and X. Latorre. 1987. Isospora belliinfections in patients with AIDS in Catalunya, Spain. N. Engl. J. Med.317:246–247. (Letter.)
156. Sanford, S. E., and G. K. A. Josephson. 1981. Porcine neonatal coccidiosis.Can. Vet. J. 22:282–285.
157. Sangster, L. T., B. P. Stuart, D. J. Williams, and D. M. Bedell. 1978.Coccidiosis associated with scours in baby pigs. Vet. Med. Small Anim.Clin. 73:1317–1319.
158. Sauda, F. C., L. A. Zamarioli, W. E. Filho, and L. B. Mello. 1993. Preva-lence of Cryptosporidium sp. and Isospora belli among AIDS patients at-tending Santos reference for AIDS, Sao Paulo, Brazil. J. Parasitol. 79:454–456.
159. Shah, H. L. 1970. Isospora species of the cat and attempted transmission ofI. felis Wenyon, 1923 from the cat to the dog. J. Protozool. 17:603–609.
160. Shah, H. L. 1970. Sporogony of the oocysts of Isospora felis Wenyon, 1923from the cat. J. Protozool. 17:609–614.
161. Shah, H. L. 1971. The life cycle of Isospora felisWenyon, 1923, a coccidiumof the cat. J. Protozool. 18:3–17.
162. Skinner, J. L. 1971. Human infection with Isospora belli in England: a casereport. J. Med. Microbiol. 5:271–273.
163. Smitskamp, H., and E. Oey-Muller. 1966. Geographical distribution andclinical significance of human coccidiosis. Trop. Geogr. Med. 18:133–136.
164. Sorvillo, F. J., L. E. Lieb, J. Seidel, P. Kerndt, J. Turner, and L. R. Ash.1995. Epidemiology of isosporiasis among persons with acquired immuno-deficiency syndrome in Los Angeles County. Am. J. Trop. Med. Hyg.53:656–659.
165. Speer, C. A., D. M. Hammond, J. L. Mahrt, and W. L. Roberts. 1973.Structure of the oocyst and oocyst walls and excystation of sporozoites ofIsospora canis. J. Parasitol. 59:35–40.
166. Speer, C. A., A. A. Marchiondo, D. W. Duszynski, and S. K. File. 1976.Ultrastructure of the sporocyst wall during excystation of Isospora endocal-limici. J. Parasitol. 62:984–987.
167. Stuart, B. P., and D. S. Lindsay. 1979. Coccidial diarrhea in swine. J. Am.Vet. Med. Assoc. 175:328–329. (Letter.)
168. Stuart, B. P., and D. S. Lindsay. 1988. Coccidiosis in swine. Vet. Clin. NorthAm. Food Anim. Pract. 2:455–468.
169. Stuart, B. P., D. M. Bedell, and D. S. Lindsay. 1981. Coccidiosis in swine:effect of disinfectants on in vitro sporulation of Isospora suis oocysts. Vet.Med. Small Anim. Clin. 76:1185–1186.
170. Stuart, B. P., D. M. Bedell, and D. S. Lindsay. 1982. Coccidiosis in swine:a search for extraintestinal sages of Isospora suis. Vet. Rec. 110:82–83.
171. Stuart, B. P., D. S. Lindsay, and J. V. Ernst. 1978. Coccidiosis as a cause ofscours in baby pigs. Proc. Int. Symp. Neonatal Diarrhea 2:371–382.
172. Stuart, B. P., H. S. Gosser, C. B. Allen, and D. M. Bedell. 1982. Coccidiosisin swine: dose and age response to Isospora suis. Can. J. Comp. Med.46:317–320.
173. Stuart, B. P., D. S. Lindsay, J. V. Ernst, and H. S. Gosser. 1980. Isosporasuis enteritis in piglets. Vet. Pathol. 17:84–93.
174. Stuart, B. P., D. B. Sisk, D. M. Bedell, and H. S. Gosser. 1982. Demon-stration of immunity against Isospora suis in swine. Vet. Parasitol. 9:185–191.
175. Syrkis, I., M. Fried, I. Elian, D. Pietrushka, and J. Lengy. 1975. A case ofsevere human coccidiosis in Israel. Isr. J. Med. Sci. 11:373–377.
176. Takahashi, M., Y. Omata, H. Oikawa, F. Claveria, I. Igarashi, A. Saito, andN. Suzuki. 1993. Protective immune response of Isospora felis-infected miceagainst Babesia microti infection. J. Vet. Med. Sci. 55:587–590.
177. Taylor, J. R. 1984. Ph.D. thesis. Auburn University, Auburn, Ala.178. Teschareon, S., P. Jariya, and C. Tipayadarapanich. 1983. Isospora belli
infection as a cause of diarrhoea. Southeast Asian J. Trop. Med. PublicHealth 14:528–530.
179. Trier, J. S., P. C. Moxey, E. M. Schimmel, and E. Robles. 1974. Chronicintestinal coccidiosis in man: intestinal morphology and response to treat-ment. Gastroenterology 66:923–935.
180. Trayser, C. V., and K. S. Todd. 1978. Life cycle of Isospora burrowsi n sp(Protozoa: Eimeriidae) from the dog Canis familiaris. Am. J. Vet. Res.39:95–98.
181. Veldhuyzen vanZanten, S. J. O., J. M. A. Lange, H. P. Sauerwein, A. C.Rijpstra, J. J. Laarman, P. J. G. M. Rietra, and S. A. Danner. 1984.Amprolium for coccidiosis in AIDS. Lancet ii:345–346. (Letter.)
182. Vetterling, J. M. 1966. Prevalence of coccidia in swine from six localities inthe United States. Cornell Vet. 56:155–166.
183. Vitovec, J., and B. Koudela. 1987. Pathology of natural isosporosis in nurs-ing piglets. Folia Parasitol. 34:199–204.
184. Vitovec, J., and B. Koudela. 1990. Double alteration of the small intestinein conventional and gnotobiotic piglets experimentally infected with thecoccidium Isospora suis (Apicomplexa, Eimeriidae). Folia Parasitol. 37:21–33.
185. Vitovec, J., B. Koudela, M. Kudweis, J. Stepanek, B. Smid, and R. Dvorak.1991. Pathogenesis of experimental combined infections with Isospora suisand rotavirus in conventional and gnotobiotic pigs. J. Vet. Med. Ser. B38:215–226.
186. Weiss, L. M., D. C. Perlman, J. Sherman, H. Tanowitz, and M. Wittner.1988. Isospora belli infection: treatment with pyrimethamine. Ann. Intern.Med. 109:474–475.
187. Wenyon, C. M. 1923. Coccidiosis of cats and dogs and the status of theIsospora of man. Ann. Trop. Med. Parasitol. 17:231–288.
188. Wenyon, C. M. 1926. Coccidia of the genus Isospora in cats, dogs, and man.Parasitology 18:253–266.
189. Westerman, E. L., and R. P. Christensen. 1979. Chronic Isospora belliinfection treated with co-trimoxazole. Ann. Intern. Med. 91:413–414.
190. Whiteside, M. E., J. S. Barkin, R. G. May, S. D. Weiss, M. A. Fischl, and C.MacLeod. 1984. Enteric coccidiosis among patients with the acquired im-munodeficiency syndrome. Am. J. Trop. Med. Hyg. 33:1065–1072.
191. Wilkinson, G. T. 1977. Coccidial infection in a cat colony. Vet. Rec. 100:156–157.
192. Wolters, E., A. O. Heydorn, and C. Laudahn. 1980. Das Rind als Zwisch-enwirt von Cystoisopora felis. Berl. Munch. Tieraerztl. Wochenschr. 93:207–210.
193. Zaman, V. 1968. Observations on human Isospora. Trans. R. Soc. Trop.Med. Hyg. 62:556–557.
34 LINDSAY ET AL. CLIN. MICROBIOL. REV.
on May 26, 2020 by guest
http://cmr.asm
.org/D
ownloaded from