Embed Size (px)
Citation preview

Gutl993;34:1581-1586
Biomechanical wall properties of the human rectum.
A study with impedance planimetry
F H Dall, C S J0rgensen, D Houe, H Gregersen, J C Djurhuus
AbstractBiomechanical properties of the rectal wallwere studied in 17 healthy adult volunteers(nine men and eight women). With impedanceplanimetry it is possible to obtain simultaneousmeasurements of pressure and rectal crosssectional area (CSA) during balloon inflations.Rectal distensions were done with an intra-luminal balloon using specified pressures upto 40 cmH2O above baseline rectal pressure.Balloon inflation elicited a phase of rapidincrease in rectal CSA followed by a phase ofslow increase until a steady state was reached.Steady state occurred within 67 to 140 secondswith the shortest period at the highest disten-sion pressures. Steady state rectal CSA valueshad a non-linear relation to increasing disten-sion pressure. Rectal CSA values in womenshowed a tendency of being slightly higherthan male values at all pressure steps with asignificant difference at 3 and 5 cm H20.Biomechanical parameters were calculatedfrom rectal CSA pressure relations. Circum-ferential wall tension increased in a linear way.Rectal compliance decreased in a non-linearway with no further decline between 30 and40 cmH2O. The pressure elastic modulusincreased steeply until a distension pressureof 35 cmH2O with no further increase to40 cmH20. This suggests that rectal tone isreduced as the muscle fails to resist furtherdistension at 35 cmH20 and higher pressures.Impedance planimetry offers new possibilitiesfor investigation of anorectal physiologythrough the study of segmental biomechanicalwall properties of the human rectum.(Gut 1993; 34: 1581-1586)
Institute of ExperimentalClinical Research,University ofAarhus,DenmarkF H DallD HoueJ C Djurhuus
Department of SurgicalGastroenterology L,Aarhus UniversityHospital, DenmarkC S J0rgensen
Department of MedicalGastroenterology -Hepatology V, AarhusUniversity Hospital,DenmarkH GregersenCorrespondence to:Dr F H Dall, Institute ofExperimental ClinicalResearch, Skeiby UniversityHospital, DK-8200 Aarhus N,Denmark.Accepted for publication8 April 1993
Changed anorectal function and innervation are
commonly studied by pressure-volume relationsby balloon distension, reflex investigations,characterisation of sphincter function, and regis-tration of rectal sensation. '"
Balloon distension elucidates the reservoirmechanism from a sensory point of view. Itprovides some information on biomechanicalproperties of the rectal wall. Commonly, rectaldistensibility is determined as rectal complianceand calculated as the changes of volume andintrarectal pressure (AV/AP). Radial expan-sion, however, is not necessarily related to thevolume infused because of the multidirectionalexpansion of the volume. Longitudinal exten-sion of a compliant balloon is likely to occur
during distension. This happens when tension,which has developed in the rectal wall, impedesfurther radial expansion.7-9 The value of suchcompliance measurements is disputed.7 '0 To
characterise segmental biomechanical propertiesof the rectal wall and regional thresholds ofsensation new methods have to be introduced.
This study concerns a method named imped-ance planimetry by which it is possible to obtainsegmental information on biomechanical proper-ties at one specific circumference of the rectalwall. The aim was to describe these properties bymeasuring rectal cross sectional area (CSA) at thesite ofdistension upon graded isobaric distensionin healthy volunteers. We have used the tech-nique in human and animal studies of intestinalwall properties."
Methods
SUBJECTSWe studied 17 healthy volunteers without anyhistory of bowel disease. The volunteers werenine men (age 28 (27-29) years, height 185 (179-187) cm, weight 80 (75-85) kg) and eight women(26 (23-29) years, 169 (166-172) cm, 58 (53-63)kg). Before the study we obtained informedconsent from all subjects. The study was per-formed according to the second declaration ofHelsinki and approved by the Ethical Committeeof Aarhus county.The study was conducted between 8 00 am
and 1 00 pm. There was a period of at least 12hours of fasting before the investigations. Nolaxative was used and subjects were asked toempty the rectum and bladder. Before theinvestigation a digital examination confirmed anempty rectum.
TECHNIQUE AND EXPERIMENTAL PROBE DESIGNWe used a specially constructed four electrodeimpedance measuring system located inside aballoon on a 20 cm long probe with an 8 mmexternal diameter (Fig 1). Two outer ring elec-trodes for excitation were placed with an inter-electrode distance of 6 cm. A generator delivereda constant alternating current of 100 micro-amperes at 5 kHz for excitation.9 5 Midwaybetween the excitation electrodes we placed tworing electrodes with an interelectrode distance of0-2 cm for measurement of impedance. We usedcopper electrodes wound around the probe in 0 5mm wide grooves to ensure a smooth surface.The distance between the excitation and detec-tion electrodes was chosen on the basis that theCSA can be measured up to a diameter of 4 to 5times the interelectrode distance. 3We measured CSA according to the field
gradient principle from the measurement ofimpedance of the fluid inside the balloon.'3'I_8Rise time for measurement of CSA was 0-02
1581
on 4 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.34.11.1581 on 1 Novem
ber 1993. Dow
nloaded from

Dall,frnrgensen, Houe, Gregersen, Djurhuus
Sensing system
tainer was cylindrical with a surface area of 363cm ensuring a maximum reduction of the waterlevel in the container of 0 55 cm in case ofmaximum balloon inflation. With a digitallycontrolled heating device (microprocessor HT50, temperature sensor Pt 100, and heating tapeBD 1194, Horst, Germany) we secured thetemperature stability of the infusion fluid. A sidehole for balloon pressure measurements wasplaced between the detection electrodes. Thelumen and the side hole had diameters of 0 7mm. We measured pressure with a low compli-ance perfusion system connected to an externaltransducer (strain gauge MX860, Medex Inc)with a perfusion rate of 0 16 to 0-20 ml min-'.Rise time for measurement of pressure was 0 09(0-08 to 0 10) seconds.'9
Signal processing system
Seensing
Figure 1: Upper drawing isa schematic diagram ofthesensing system including theprobefor measurement ofrectal CSA. D=electrodefordetection, E=electrodeforexitation, I=infusionchannels, and P=side holefor pressure measurement.Lower drawing shows thesignal processing system forsignals recording and onlinestoring. T=pressuretransducer.
(0-02-0-03) seconds.'9 We calibrated the CSAmeasuring system in PVC tubes with holes ofknown CSAs. Before the measurements we cali-brated the measurement system with a two pointminimum and maximum calibration.The latex balloon was 6-9 cm long. To prevent
longitudinal elongation of the balloon duringdistension we chose a balloon with a wall thick-ness of 0-2 mm. The balloon could be inflatedwith 37°C electrically conducting fluid (0-65 mMNaCl solution) through an infusion channel(diameter 4 5 mm) up to a CSA of 6361 mm2(diameter=90 mm and a volume of 200 ml)without stretching the balloon wall. The con-
7000
6000-
5000-
4000 -
E
3000-
2000 -
Figure 2: A diagram ofan 8point calibration. Thecalibration signals after theinitial two point calibration( ) and after thefinal 8point calibration ( ) areshown.
1000 -
0 1000 2000 3000 4000 5000 6000 7000
mm2
INVESTIGATIONAL PROCEDUREThe subjects were placed in the left lateralposition with hips and knees flexed to 900.20Calibration of the measuring system was donebefore the insertion of the probe into the rectum.We secured the position of the prove by tapeattached to the buttocks and measured the rectalCSA between 8-2 and 8 4 cm from the anal verge.The balloon was inflated to a pressure of 30
cmH2O to unfold the balloon before the mea-surements were recorded. There was a restingperiod of 20 minutes before the measurementswere taken. After this period we did a series ofrectal pressure distensions. We assessed thebaseline rectal pressure by increasing the pres-sure column in steps of 1 cm. We continued untilthe inflation of the balloon caused an increase inrectal CSA. Raising a pressure column of con-secutively increasing pressures at 3, 5, 10, 15, 20,25, 30, 35, and 40 cm above the baseline rectalpressure provided the distension stimulus. Eachdistension lasted at least 1-5 minutes and until asteady state rectal CSA value. Five minute restperiods separated each rectal distension. Wetested the in vivo reproducibility of the steadystate values with repeated measurements at thepressure steps 10, 20, 30, and 40 cm H20 in fivesubjects. After each rectal distension, the sub-jects described their sensation.
Records of rectal CSA and pressure were
amplified and analogue to digital converted witha sample frequency of 10 Hz and stored onlinewith software developed in our laboratory(Mingo).2'
DATA ANALYSISComputer analysis was applied to the data.2' Thecalibration curve was non-linear. Therefore wecalibrated the results with an 8 point calibrationcurve to obtain a final linear calibration (Fig 2).We determined the steady state rectal CSAvalues for further analysis of the biomechanicalparameters.
Definition ofbiomechanical parametersCircumferential wall tension=R Pt, where R is theintraluminal radius (R=square root of rectalCSA a- l) and Pt the transmural pressure differ-ence (law of LaPlace).
E00
15mmp
1582
on 4 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.34.11.1581 on 1 Novem
ber 1993. Dow
nloaded from
Biomechanical wallproperties ofthe human rectum. A study with impedance planimetry
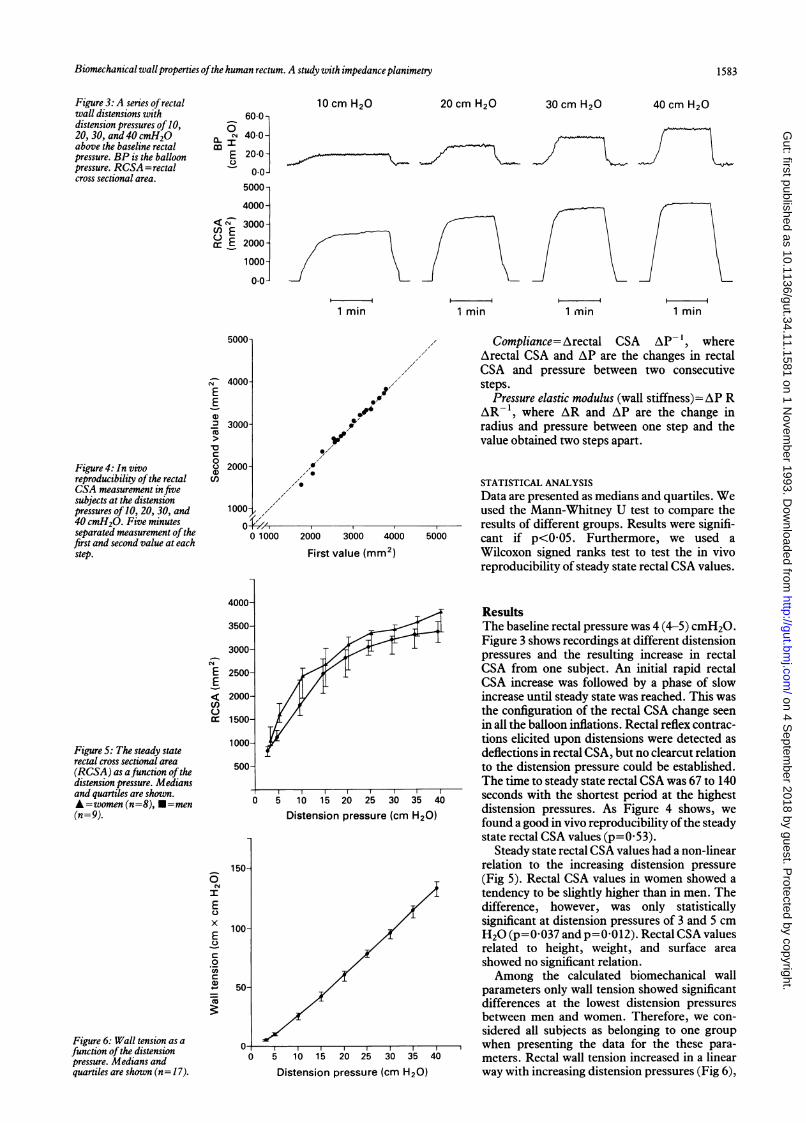
Figure 3: A series ofrectalwall distensions withdistension pressures of 10,20, 30, and 40 cmH2Oabove the baseline rectalpressure. BP is the balloonpressure. RCSA =rectalcross sectional area.
10 cm H20600
N 40-0--I
E 200-00
5000-
4000-
< NE 3000-
o E 2000-
1000-
0.0-
1 min
20 cm H20
1 min
30 cm H20
1 min
40 cm H20
1 min
5000-
Figure 4: In vivoreproducibility ofthe rectalCSA measurement in fivesubjects at the distensionpressures of 10, 20, 30, and40 cmH2O. Five minutesseparated measurement ofthefirst and second value at eachstep.
4000EE
.2 3000-
-0n 00
c 20001n
1 000- . ,
0 1000
I04.9.6
0I
I0
IV.
I,0
2000 3000 4000 5000
First value (mm2)
Compliance=Arectal CSA AP- ', whereArectal CSA and AP are the changes in rectalCSA and pressure between two consecutivesteps.
Pressure elastic modulus (wall stiffness)=AP RAR-1, where AR and AP are the change inradius and pressure between one step and thevalue obtained two steps apart.
STATISTICAL ANALYSISData are presented as medians and quartiles. Weused the Mann-Whitney U test to compare theresults of different groups. Results were signifi-cant if p<005. Furthermore, we used aWilcoxon signed ranks test to test the in vivoreproducibility of steady state rectal CSA values.
4000-
EE
cr
Figure 5: The steady staterectal cross sectional area(RCSA) as afunction ofthedistension pressure. Mediansand quartiles are shown.A=women(n=8), *=men(n= 9).
I
E0
x
E
C0
CAco
3500-
3000-
2500-
2000-
1500-
1000-
500-
150-
100-
50-
Figure 6: Wall tension as afunction ofthe distensionpressure. Medians andquartiles are shown (n= 17).
0
5 10 15 20 25 30 35 40Distension pressure (cm H20)
5 10 15 20 25 30 35 40
Distension pressure (cm H20)
ResultsThe baseline rectal pressure was 4 (4-5) cmH2O.Figure 3 shows recordings at different distensionpressures and the resulting increase in rectalCSA from one subject. An initial rapid rectalCSA increase was followed by a phase of slowincrease until steady state was reached. This wasthe configuration of the rectal CSA change seenin all the balloon inflations. Rectal reflex contrac-tions elicited upon distensions were detected asdeflections in rectal CSA, but no clearcut relationto the distension pressure could be established.The time to steady state rectal CSA was 67 to 140seconds with the shortest period at the highestdistension pressures. As Figure 4 shows, wefound a good in vivo reproducibility ofthe steadystate rectal CSA values (p=053).
Steady state rectal CSA values had a non-linearrelation to the increasing distension pressure(Fig 5). Rectal CSA values in women showed atendency to be slightly higher than in men. Thedifference, however, was only statisticallysignificant at distension pressures of 3 and 5 cmH20 (p=0 037 and p=0-012). Rectal CSA valuesrelated to height, weight, and surface areashowed no significant relation.Among the calculated biomechanical wall
parameters only wall tension showed significantdifferences at the lowest distension pressuresbetween men and women. Therefore, we con-sidered all subjects as belonging to one groupwhen presenting the data for the these para-meters. Rectal wall tension increased in a linearway with increasing distension pressures (Fig 6),
nJ e I} I
u,
1583
on 4 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.34.11.1581 on 1 Novem
ber 1993. Dow
nloaded from
Dall,Jsrgensen, Houe, Gregersen, Djurhuus
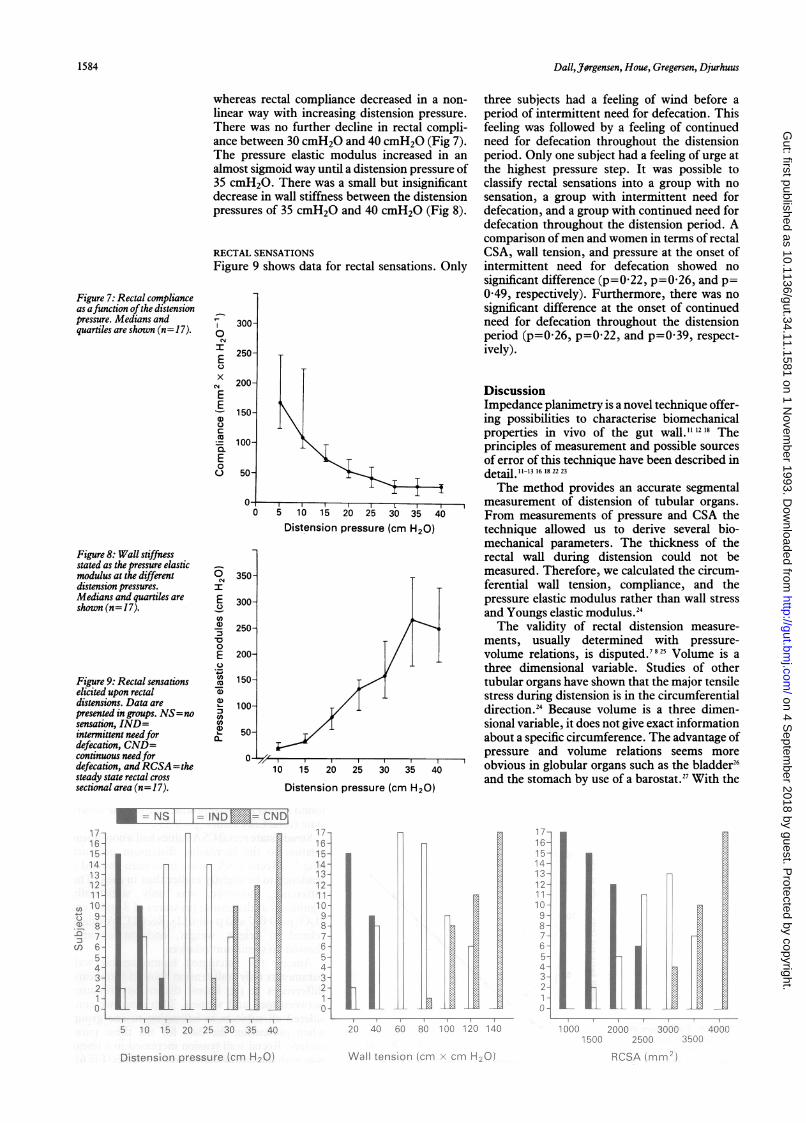
whereas rectal compliance decreased in a non-linear way with increasing distension pressure.There was no further decline in rectal compli-ance between 30 cmH2O and 40 cmH2O (Fig 7).The pressure elastic modulus increased in an
almost sigmoid way until a distension pressure of35 cmH2O. There was a small but insignificantdecrease in wall stiffness between the distensionpressures of 35 cmH2O and 40 cmH2O (Fig 8).
RECTAL SENSATIONSFigure 9 shows data for rectal sensations. Only
0
I
XE
x
E
E
a)
-._E0
u
300-
250-
200-
150-
100-
50-
0-1
0
Figure 8: Wall stiffnessstated as the pressure elasticmodulus at the differentdistension pressures.Medians and quartiles areshown (n= 17).
Figure 9: Rectal sensationselicited upon rectaldistensions. Data arepresented in groups. NS=nosensation, IND=intermittent needfordefecation, CND=continuous needfordefecation, andRCSA=thesteady state rectal crosssectional area (n= 17).
I
E
CA
')
0
E
.)
.4-CnCD
a)
a)
0~
350-
300-
250-
200-
150-
100-
50-
L.5 10 15 20 25 30 35 40
Distension pressure (cm H20)
a /III-
,,
10 15 20 25 30 35 40
Distension pressure (cm H20)
three subjects had a feeling of wind before aperiod of intermittent need for defecation. Thisfeeling was followed by a feeling of continuedneed for defecation throughout the distensionperiod. Only one subject had a feeling of urge atthe highest pressure step. It was possible toclassify rectal sensations into a group with nosensation, a group with intermittent need fordefecation, and a group with continued need fordefecation throughout the distension period. Acomparison ofmen and women in terms of rectalCSA, wall tension, and pressure at the onset ofintermittent need for defecation showed nosignificant difference (p=0-22, p=0-26, and p=0 49, respectively). Furthermore, there was nosignificant difference at the onset of continuedneed for defecation throughout the distensionperiod (p=0-26, p=0.22, and p=0 39, respect-ively).
DiscussionImpedance planimetry is a novel technique offer-ing possibilities to characterise biomechanicalproperties in vivo of the gut wall."'2'8 Theprinciples of measurement and possible sourcesof error of this technique have been described indetail.I 1-3 16 18 22 23
The method provides an accurate segmentalmeasurement of distension of tubular organs.From measurements of pressure and CSA thetechnique allowed us to derive several bio-mechanical parameters. The thickness of therectal wall during distension could not bemeasured. Therefore, we calculated the circum-ferential wall tension, compliance, and thepressure elastic modulus rather than wall stressand Youngs elastic modulus.24The validity of rectal distension measure-
ments, usually determined with pressure-volume relations, is disputed.7825 Volume is athree dimensional variable. Studies of othertubular organs have shown that the major tensilestress during distension is in the circumferentialdirection.24 Because volume is a three dimen-sional variable, it does not give exact informationabout a specific circumference. The advantage ofpressure and volume relations seems moreobvious in globular organs such as the bladder26and the stomach by use of a barostat.27 With the
17-16-15-14-13-12-11-
a 10U 9-
8-= 7-~co 6-
5-4.3.2-
0-
5 10 15 20 25 30 35 40
17-16-15-14-13-12-11-
10-9-
8-7-6.5-4-3-2-1-0- R ]
17-16-15-14-13-12-11-10-9-
8-7-6-5-4-3..
2-1-
°1I20 40 60 800I1 020 40 60 80 lOo t20o 140 1000
Distension pressure (cm H20)
2000 3000 40001500 2500 3500
RCSA (mm2)
Figure 7: Rectal complianceas afunction ofthe distensionpressure. Medians andquartiles are shown (n= 17).
in= NSI 1= IND = CNDI
n
----iv-
I
1584
Wall tension (cm x cm H20)
iL
on 4 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.34.11.1581 on 1 Novem
ber 1993. Dow
nloaded from

Biomechanical wall properties ofthe human rectum. A study with impedance planimetry 1585
rectal pressure as the zero pressure referencepoint, the applied distension pressure mostprobably equals the transmural pressure allow-ing the calculation of circumferential walltension according to the law of LaPlace. Thecalculation is valid for the innermost layer of thewall at a constant transmural pressure and atsteady state conditions. Furthermore, a uni-formly cylindrical lumen and wall contact at thesite of distension must be assumed during disten-sions. We achieved that in a previous study,9and before this study we showed these conditionswith a vaginal ultrasonic probe during distensionseries of the rectum (unpublished data).
In this study the rectal CSA curve at eachdistension pressure could be described by aninitial rapid phase followed by a slow phase offilling before reaching steady state. Previously,we have shown similar patterns in other intest-inal segments by use of impedance planimetry.'9It is a measure of viscoelastic properties, and notas previously stated a particular rectal phenome-non of accommodation to different volume load-ings.9 The rectal CSA values of men and womenwere significantly different at transmural pres-sures of 3 and 5 cmH20. This shows that therectal lumen is bigger and that the rectum ismore compliant at low induced pressures inwomen. We need further investigations, how-ever, including larger populations of men andwomen to confirm the tendency of higher lowpressure distensibility in women than in men.
Despite a non-linear increase of luminal rectalradius similar to the rectal CSA increase, theincrease of the circumferential wall tension withincreasing distension pressures was linear.This suggests a major influence ofthe transmuralpressure on this parameter calculated accordingto the Law of LaPlace. Calculation of stress-strain relations seems more appropriate toestimate the load of distension on a ratherthick walled human rectum.Compliance showed no linear relation to the
distension pressure (Fig 7). The rectum wasmost compliant at low pressures and declinedwith increasing distension pressure until nofurther progress in compliance between thepressures of 30 to 40 cmH20. Because non-linearity it is doubtful if rectal compliance shouldbe characterised by a single value. The pressureelastic modulus showed a similar non-linearpattern. This parameter is more appropriatethan compliance to describe biomechanicsbecause it measures the changes in rectal CSAand pressure and also considers the actual degreeof distension.
Variations in rectal tone as shown by Bell et almight change rectal distensibility upon disten-sion.21 The influence of smooth muscle cellswithin the wall of a tubular organ upon intra-luminar distensions is shown in studies ofvascular distensibility. Variations in vascularmuscle stiffness change arterial distensibility, forexample, when the arterial muscle contracts, thevessel is less distensible.24 In this study, the rectalpressure elastic modulus (wall stiffness),increased steeply until a distension pressure of35 cmH2O with no further increase to 40cmH2O. At 35 cmH2O and higher pressuresmuscle tone may be reduced as the muscle fails to
resist further distension. If only passive proper-ties determine the pressure elastic modulus, anexponential increase would have been expected.We showed this in a previous study of theisolated perfused porcine duodenum.'9 Studiesof the human oesophagus and duodenumshowed the same influence of intestinal toneupon the pressure elastic modulus during disten-sion." 30
Sensations elicited by rectal distensions are thesubject for research by several investigators.Volume is commonly the independent variable.Previously, another group performed isobaricdistensions with simultaneous registration of theinfused volume.3' In this study we classifiedrectal sensations elicited by isobaric distensionsaccording to the segmental steady state valuesobtained. Previous results have shown a higherthreshold of rectal sensation in men than inwomen.3233 This could not be confirmed by thisstudy. This may be caused by the use of differenttechniques, for example, continuous rectalfilling with a certain infusion rate up to themaximal tolerable volume.The method may be a future tool in studies
of rectal biomechanical wall properties andanorectal motility elicited by intraluminal dis-tensions. Furthermore, in combination with newtechniques, for example, high resolution ultra-sound systems, it permits the measurement ofand an estimation of stress-strain relations of therectal wall thickness during distensions.
This study was supported by grants from The Aarhus UniversityFoundation, The Institute of Experimental Clinical Research, andThe Danish Medical Research Council.
1 Denny-Brown DE, Robertson EG. An investigation of thenervous control of defaecation. Brain 1935; 58: 256-310.
2 Goligher JC, Hughes ESR. Sensibility of the rectum andcolon. Its role in the mechanism of anal continence. Lancet1951; i: 543-8.
3 Schuster MM, Hendrix TR, Mendeloff Al. The internal analsphincter response: manometric studies on its normalphysiology, neural pathways, and alteration in bowel dis-orders. J Clin Invest 1963; 42: 196-207.
4 Scharli AF, Kiesewetter WB. Defecation and continence:some new concepts. Dis Colon Rectum 1970; 13: 81-107.
5 Haynes WG, Read NW. Ano-rectal activity in man duringrectal infusion of saline: a dynamic assessment of the analcontinence mechanism. J Physiol 1982; 330: 45-56.
6 Arhan P, Faverdin C, Persoz B, Devroede G, Dubois B,Dornic C, et al. Relationship between viscoelastic propertiesof the rectum and anal pressure in man. J Appl Physiol 1976;41: 677-82.
7 Kendall GPN, Thompson DG, Day SJ, Lennard-Jones JE.Inter- and intraindividual variation in pressure-volumerelations of the rectum in normal subjects and patients withthe irritable bowel syndrome. Gut 1990; 31: 1062-8.
8 Sun WM, Read NW, Prior A, Daly JA, Cheah S, Grundy D.Sensory and motor responses to rectal distension varyaccording to rate and pattern of balloon inflation. Gastro-enterology 1990; 99: 1008-15.
9 Dall FH, J0rgensen CS, Djurhuus JC, Gregersen H. Bio-mechanical wall properties of the porcine rectum. A studyusing impedance planimetry. Dig Dis 1991; 9: 346-52.
10 Madoff RD, Orrom WJ, Rothenberger DA, Goldberg SM.Rectal compliance: a critical reappraisal. Int J Colorect Dis1990; 5:37-40.
11 Gregersen H, Jensen SL, Djurhuus JC. Changes in oesopha-geal wall biomechanics after portal vein banding and varicealsclerotherapy measured by a new technique. An experi-mental study in rabbits. Gut 1988; 29: 1699-704.
12 Gregersen H, Kraglund K, Djurhuus JC. Variations induodenal cross-sectional area during the interdigestivemotility complex. Am J Physiol 1990; 259 (GastrointestLiver Physiol 22): G2-3 1.
13 Gregersen H, Andersen MB. Impedance measuring system forquantification of cross-sectional area in the gastrointestinaltract. Med BiolEng Comput 1991; 29: 108-10.
14 Gregersen H, Djurhuus JC. Impedance planmetry. A newapproach to biomechanical wall properties in the intestine.DigDis 1991; 9: 332-40.
15 Gregersen H, J0rgensen CS, Dall FH, Jensen SL.Spontaneous and evoked motility in the isolated perfusedporcine duodenum.JZApplPhysiol 1992; 73 (1): 9-19.
on 4 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.34.11.1581 on 1 Novem
ber 1993. Dow
nloaded from

1586 Dall,Jorgensen, Houe, Gregersen, Djurhuus
16 Harris JH, Therkelsen EE, Zinner NR. Electrical measure-ment of ureteral flow. In: Boyarsky S, Tanagho EA,Gottschalk CW, Zimskind PD, eds. Urodynamics. London:Academic Press, 1971: 465-72.
17 Colstrup H, Mortensen SO, Kristensen JK. A probe formeasurements of related values of cross-sectional area andpressure in the resting female urethra. Urol Res 1983; 11:139-43.
18 Gregersen H, St0dkilde-J0rgensen H, Djurhuus JC,Mortensen SO. The four electrode impedance technique: amethod for investigation of compliance in luminal organs.Clin Phys PhysiolMeas 1988; 9 (suppl A): 61-4.
19 Gregersen H, J0rgensen CS, Dall FH. Biomechanical wallproperties in the isolated perfused procine duodenum.An experimental study using impedance planimetry.J GastrointestMotility 1992; 4: 125-35.
20 Akervall S, Fasth S, Nordgren S, Oresland T, Hulten L.Manovolumetry: a new method for investigation of anorectalfunction. Gut 1988; 29: 614-23.
21 Andersen MB, St0dkilde-J0rgensen H, Gregersen H.Versatile software system for analysis of gastrointestinalpressure recordings. Dig Dis 1991; 9: 382-8.
22 Lose G, Colstrup H, Saksager K, Kristensen JK. A new probefor measurement of related values of cross-sectional area andpressure in a biological tube. MedBiol Eng Comput 1986; 24:488-92.
23 Mortensen SO, Djurhuus JC, Rask-Andersen H. A system formeasurements of micturition urethral cross-sectional areas
and pressures. Med Biol EngComput 1983; 21: 482-8.24 Dobrin PB. Mechanical properties of arteries. Physiol Rev
1978; 58: 397-460.25 Varma JS, Smith AN. Reproducibility of the proctometro-
gram. Gut 1986; 27: 288-92.26 Coolsaet B. Bladder compliance and detrusor activity the
collection phase. Neurourology and Urodynamics 1985; 4:263-73.
27 Azpiroz F, Malagelada JR. Intestinal control of gastric tone.Am J Physiol 1985; 249 (Gastrointest Liver Physiol 12):G501-9.
28 Bell AM, Pemberton JH, Hanson RB, Zinsmeister AR.Variations in muscle tone of the human rectum: recordingswith an electromechanical barostat. AmJ3 Physiol 1991; 260(Gastrointest Liver Physiol 23): G17-25.
29 Orvar KB, Gregersen H, Christensen J. Biomechanicalcharacteristics of the human esophagus. Dig Dis Sci 1993;38: 197-205.
30 Gregersen H, Orvar KB, Christensen J. Biomechanicalproperties of the duodenal wall and tone during phase I andphase II of the MMC. AmJ7 Physiol 1992; 263: G795-801.
31 Akervall S, Fasth S, Nordgren S, Oresland T, Hulten L.Rectal reservoir and sensory function studied by gradedisobaric distension in normal man. Gut 1989; 30: 496-502.
32 Loening-Baucke V, Anuras S. Effects of age and sex onanorectal manometry. AmJ Gastroenterol 1985; 80: 50-3.
33 Sun WM, Read NW. Anorectal function in normal humansubjects: effect of gender. Int3J Colorect Dis 1989; 4: 188-96.
on 4 Septem
ber 2018 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.34.11.1581 on 1 Novem
ber 1993. Dow
nloaded from





























