Embed Size (px)
Citation preview
REVIEW
Clinical Applications of Biomedical Microdevicesfor Controlled Drug Delivery
Pablo Gurman, MD; Oscar R. Miranda, PhD; Kevin Clayton, BS; Yitzhak Rosen, MD;and Noel M. Elman, PhDAbstract
Miniaturization of devices to micrometer and nanometer scales, combined with the use of biocompatibleand functional materials, has created new opportunities for the implementation of drug delivery systems.Advances in biomedical microdevices for controlled drug delivery platforms promise a new generation ofcapabilities for the treatment of acute conditions and chronic illnesses, which require high adherence totreatment, in which temporal control over the pharmacokinetic profiles is critical. In addition, clinicalconditions that require a combination of drugs with specific pharmacodynamic profiles and local deliverywill benefit from drug delivery microdevices. This review provides a summary of various clinical appli-cations for state-of-the-art controlled drug delivery microdevices, including cancer, endocrine and oculardisorders, and acute conditions such as hemorrhagic shock. Regulatory considerations for clinicaltranslation of drug delivery microdevices are also discussed. Drug delivery microdevices promise aremarkable gain in clinical outcomes and a substantial social impact. A review of articles covering the fieldof microdevices for drug delivery was performed between January 1, 1990, and January 1, 2014, usingPubMed as a search engine.
ª 2014 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2014;nn(n):1-16
From the Institute forSoldier Nanotechnologies,Massachusetts Institute ofTechnology, Cambridge(P.G., O.R.M., K.C., Y.R.,N.M.E.); and Departmentof Materials Science,University of Texas atDallas, Richardson (P.G.).
B iomedical microdevices are fabricateddevices with critical features on the orderof 1 to 100mm. Thesemicrodevices range
in complexity from simple microstructures suchas microchannels to more sophisticated micro-functional parts such as microtransducers andmicroelectromechanical systems (MEMS).1
These devices integrate mechanisms thatactivate a variety of physical signals to achievea specific function. For example, MEMS-basedinertial sensors transduce a mechanical signalinput to an electrical signal response. Currenttransducers are able to combine multiplephysical inputs with multiple output signals.
Biomedical microdevices present a varietyof key advantages for applications in healthcare owing to their (1) extremely small sizesproviding minimally invasive procedures, (2)low power consumption, (3) batch fabricationprocesses with high reproducibility, and (4)low cost per device, in conjunction with theirmultiple functionalities and compatibility withvery large-scale integration electronics.
These novel technologies have acceleratedthe development of a variety of micromedicaldevices, such as catheter pressure sensors,microelectronic components for pacemakers,
Mayo Clin Proc. n XXX 2014;nn(n):1-16 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org n ª 2014 Mayo Foundation for M
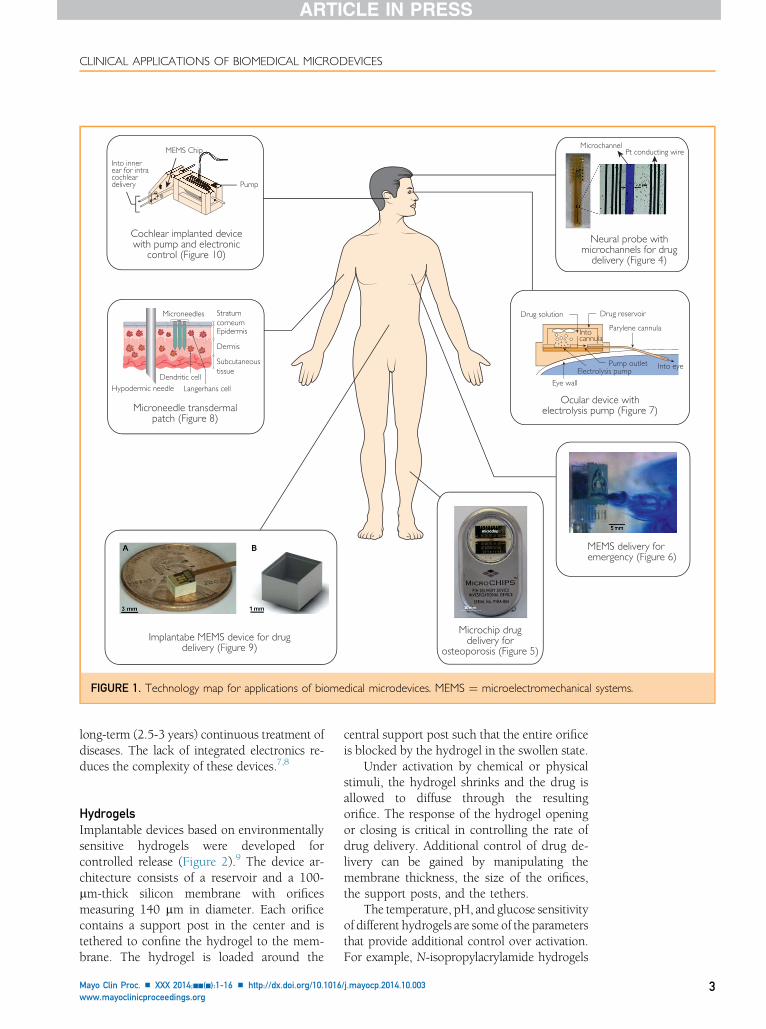
hand-held point-of-care diagnostic devices,and drug delivery systems, all of which haveprovided significant improvement over treat-ment possibilities for numerous chronic andnonchronic illnesses.1-4 Figure 1 shows a varietyof biomedical microdevices for several therapeu-tic applications.
Controlled drug delivery systems that arebased onmicrodevices contain structural micro-parts, such as microchannels and microreser-voirs, to store drugs. In addition, drug deliverysystems based on MEMS incorporate micro-transducers such as microactuators and micro-sensors, which improve the device capabilities.
Drug delivery devices based on MEMSprovide an opportunity for improved diag-nosis, monitoring, and treatment of numerousillnesses. The MEMS can deliver a variety ofdrugs, including drugs in combination, usinga single device. The MEMS drug delivery de-vices have the ability to control the rate ofdrug release to a target area. They can be pro-grammed for pulsatile or continuous deliveryand can release the drug locally, which in-creases treatment efficacy using a smalleramount of drug, reducing systemic concentra-tion levels1-6 and associated toxicity.
/j.mayocp.2014.10.003edical Education and Research
1
ARTICLE HIGHLIGHTS
n Drug delivery systems can be classified as passive and active.Passive devices do not incorporate sensors and actuators fordrug delivery.
n Active microdevices include microelectromechanical systems(MEMS), which comprise microparts such as microchannels andmicrovalves and transducers, including microsensors andmicroactuators, integrated into a singular microdevice.
n Advantages of MEMS drug delivery systems include miniaturization,integration with microelectronics, actively controlled, low cost,multiple pharmacologic therapies in a single device, controlled overrelease rate, and in vivo long-term storage of drugs.
n The MEMS are being used for a variety of clinical conditions,including diabetes, neurologic disorders, inner ear diseases, andcancer.
n Fluzone is an example of a Food and Drug Administrationeapproved drug delivery microdevice for vaccine delivery.
n The MEMS drug delivery devices can be considered combina-tion products. Many combination products are considereddrugs, requiring a New Drug Application for Food and DrugAdministration approval.
MAYO CLINIC PROCEEDINGS
2
Finally, the scope of novel materials forbiomedical devices has expanded the potentialuse of biocompatible platforms with high biolog-ical performance, eg, less toxic and nonreactivedevices, enabling new therapeutic applications.
This review provides a summary of currentstate-of-the-art biomedical microdevices forcontrolled drug delivery and their correspond-ing clinical applications. The following sectionsdescribe passive and active delivery devicesbased on MEMS technology. Each section pro-vides a technical description of a microdevicefollowed by its suggested clinical application.The review continues with a summary of theregulatory strategies for obtaining Food andDrug Administration (FDA) approval for suchmicrodevices. Finally, a perspective on thefuture of these novel devices is presented.
DATA SOURCES AND SEARCHESA PubMed search between January 1, 1990, andJanuary 1, 2014, was performed. The searchterms were drug delivery AND MEMS, implant-able devices AND MEMS, control release ANDmicrochip, controlled release AND BioMEMS,
Mayo Clin Proc. n XXX 20
neural probes AND drug delivery, vaccines ANDmicroneedles, diabetes AND microneedles, intraoc-ular AND drug delivery devices, and inner earAND drug delivery AND microfluidics. Paperswere selected following the definition of micro-devices and MEMS. Selection also was per-formed with the aim of having examples ofdifferent types of microdevices (passive andactive, actuationmechanism, andmaterials). Ex-amples of different clinical applications for drugdelivery microdevices assisted in selecting pa-pers more close to the clinical application thanthose focused solely on fundamental science.Diagnostic microdevices were specificallyexcluded from the search.
PASSIVE DEVICESPassive biomedical microdevices for drug deliv-ery do not rely on an actuation mechanism oron monitoring for feedback. These devices arereservoir based, relying on mass transfer acrossa permeable membrane to deliver pharmaceu-tical drugs, the biodegradation of a hermeticmembrane, or a unique reservoir structure toachieve controlled release. The rate of releasecan be controlled by taking into account thefollowing design parameters: (1) the effectivepermeability of the membranes by fine-tuningstructural dimensions and materials (poresize, thickness), (2) the rate of degradation ofthe polymer contained on the membrane orin the reservoir, (3) the diffusivity propertiesof the drug, and (4) the osmotic pressure. Pas-sive delivery of drugs cannot be modified afterimplementation. Other passive-release devicesoperate based on actuation resulting fromin vivo conditions inside the body, such as pHor temperature, to accelerate degradation ofthe materials that encapsulate the pharmaceu-tical drugs. Typically, the controlled release isachieved by considering the pharmacokineticsof the selected drug for delivery. Design and ma-terial parameters are thereafter adjusted andselected during the design process to provide aconstant and superior pharmacokinetic perfor-mance, such as an improvement in treatmentefficacy duration over the typical half-life ofthe pharmaceutical drug. Existing passive-release devices, such as the fentanyl transdermalsystem (DURAGESIC; Janssen PharmaceuticalsInc) and the fluocinolone acetonide intravitrealimplant (Retisert; Bausch & Lomb Inc),are used for either short-term (3 days) or
14;nn(n):1-16 n http://dx.doi.org/10.1016/j.mayocp.2014.10.003www.mayoclinicproceedings.org
MicrochannelPt conducting wire
Neural probe withmicrochannels for drug
delivery (Figure 4)
MEMS Chip
Pump
Into innerear for intracochleardelivery
Cochlear implanted devicewith pump and electronic
control (Figure 10)
StratumcorneumEpidermis
Dermis
Subcutaneoustissue
Microneedles
Hypodermic needleDendritic cell
Langerhans cell
Microneedle transdermalpatch (Figure 8)
Drug solution Drug reservoir
Parylene cannulaIntocannula
Into eye
Eye wall
Electrolysis pumpPump outlet
Ocular device withelectrolysis pump (Figure 7)
MEMS delivery foremergency (Figure 6)
Microchip drugdelivery for
osteoporosis (Figure 5)Implantabe MEMS device for drug
delivery (Figure 9)
FIGURE 1. Technology map for applications of biomedical microdevices. MEMS ¼ microelectromechanical systems.
CLINICAL APPLICATIONS OF BIOMEDICAL MICRODEVICES
long-term (2.5-3 years) continuous treatment ofdiseases. The lack of integrated electronics re-duces the complexity of these devices.7,8
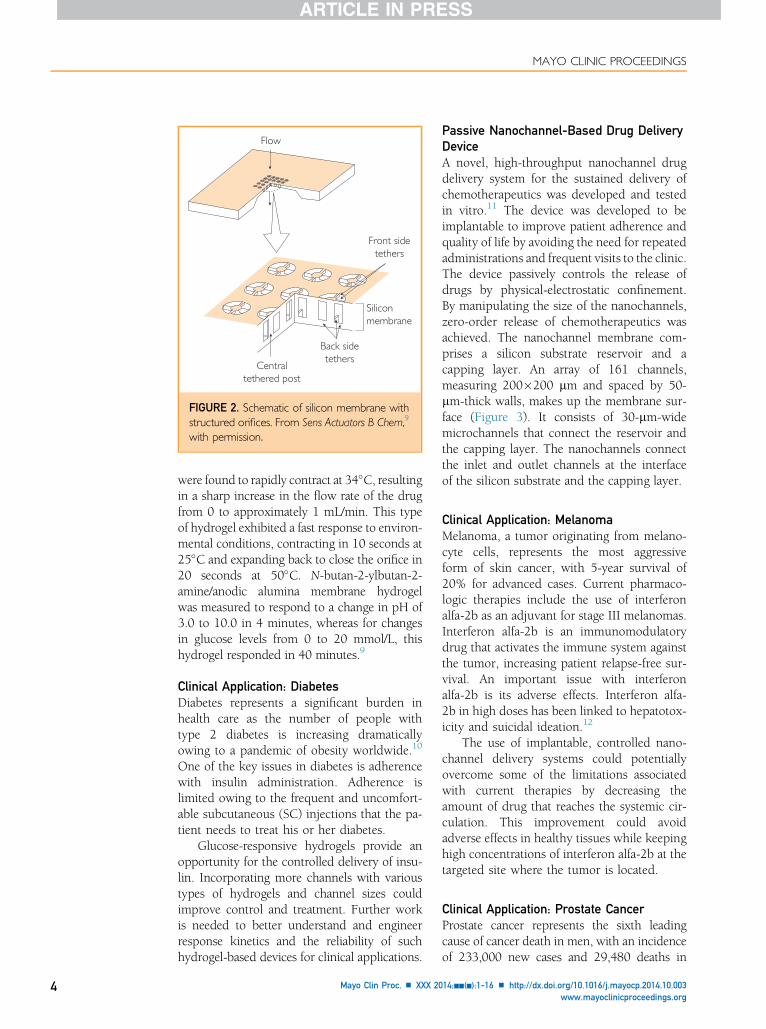
HydrogelsImplantable devices based on environmentallysensitive hydrogels were developed forcontrolled release (Figure 2).9 The device ar-chitecture consists of a reservoir and a 100-mm-thick silicon membrane with orificesmeasuring 140 mm in diameter. Each orificecontains a support post in the center and istethered to confine the hydrogel to the mem-brane. The hydrogel is loaded around the
Mayo Clin Proc. n XXX 2014;nn(n):1-16 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
central support post such that the entire orificeis blocked by the hydrogel in the swollen state.
Under activation by chemical or physicalstimuli, the hydrogel shrinks and the drug isallowed to diffuse through the resultingorifice. The response of the hydrogel openingor closing is critical in controlling the rate ofdrug delivery. Additional control of drug de-livery can be gained by manipulating themembrane thickness, the size of the orifices,the support posts, and the tethers.
The temperature, pH, and glucose sensitivityof different hydrogels are some of the parametersthat provide additional control over activation.For example, N-isopropylacrylamide hydrogels
/j.mayocp.2014.10.003 3
Front sidetethers
Centraltethered post
Back sidetethers
Flow
Siliconmembrane
FIGURE 2. Schematic of silicon membrane withstructured orifices. From Sens Actuators B Chem,9
with permission.
MAYO CLINIC PROCEEDINGS
4
were found to rapidly contract at 34�C, resultingin a sharp increase in the flow rate of the drugfrom 0 to approximately 1 mL/min. This typeof hydrogel exhibited a fast response to environ-mental conditions, contracting in 10 seconds at25�C and expanding back to close the orifice in20 seconds at 50�C. N-butan-2-ylbutan-2-amine/anodic alumina membrane hydrogelwas measured to respond to a change in pH of3.0 to 10.0 in 4 minutes, whereas for changesin glucose levels from 0 to 20 mmol/L, thishydrogel responded in 40 minutes.9
Clinical Application: DiabetesDiabetes represents a significant burden inhealth care as the number of people withtype 2 diabetes is increasing dramaticallyowing to a pandemic of obesity worldwide.10
One of the key issues in diabetes is adherencewith insulin administration. Adherence islimited owing to the frequent and uncomfort-able subcutaneous (SC) injections that the pa-tient needs to treat his or her diabetes.
Glucose-responsive hydrogels provide anopportunity for the controlled delivery of insu-lin. Incorporating more channels with varioustypes of hydrogels and channel sizes couldimprove control and treatment. Further workis needed to better understand and engineerresponse kinetics and the reliability of suchhydrogel-based devices for clinical applications.
Mayo Clin Proc. n XXX 20
Passive Nanochannel-Based Drug DeliveryDeviceA novel, high-throughput nanochannel drugdelivery system for the sustained delivery ofchemotherapeutics was developed and testedin vitro.11 The device was developed to beimplantable to improve patient adherence andquality of life by avoiding the need for repeatedadministrations and frequent visits to the clinic.The device passively controls the release ofdrugs by physical-electrostatic confinement.By manipulating the size of the nanochannels,zero-order release of chemotherapeutics wasachieved. The nanochannel membrane com-prises a silicon substrate reservoir and acapping layer. An array of 161 channels,measuring 200�200 mm and spaced by 50-mm-thick walls, makes up the membrane sur-face (Figure 3). It consists of 30-mm-widemicrochannels that connect the reservoir andthe capping layer. The nanochannels connectthe inlet and outlet channels at the interfaceof the silicon substrate and the capping layer.
Clinical Application: MelanomaMelanoma, a tumor originating from melano-cyte cells, represents the most aggressiveform of skin cancer, with 5-year survival of20% for advanced cases. Current pharmaco-logic therapies include the use of interferonalfa-2b as an adjuvant for stage III melanomas.Interferon alfa-2b is an immunomodulatorydrug that activates the immune system againstthe tumor, increasing patient relapse-free sur-vival. An important issue with interferonalfa-2b is its adverse effects. Interferon alfa-2b in high doses has been linked to hepatotox-icity and suicidal ideation.12
The use of implantable, controlled nano-channel delivery systems could potentiallyovercome some of the limitations associatedwith current therapies by decreasing theamount of drug that reaches the systemic cir-culation. This improvement could avoidadverse effects in healthy tissues while keepinghigh concentrations of interferon alfa-2b at thetargeted site where the tumor is located.
Clinical Application: Prostate CancerProstate cancer represents the sixth leadingcause of cancer death in men, with an incidenceof 233,000 new cases and 29,480 deaths in
14;nn(n):1-16 n http://dx.doi.org/10.1016/j.mayocp.2014.10.003www.mayoclinicproceedings.org
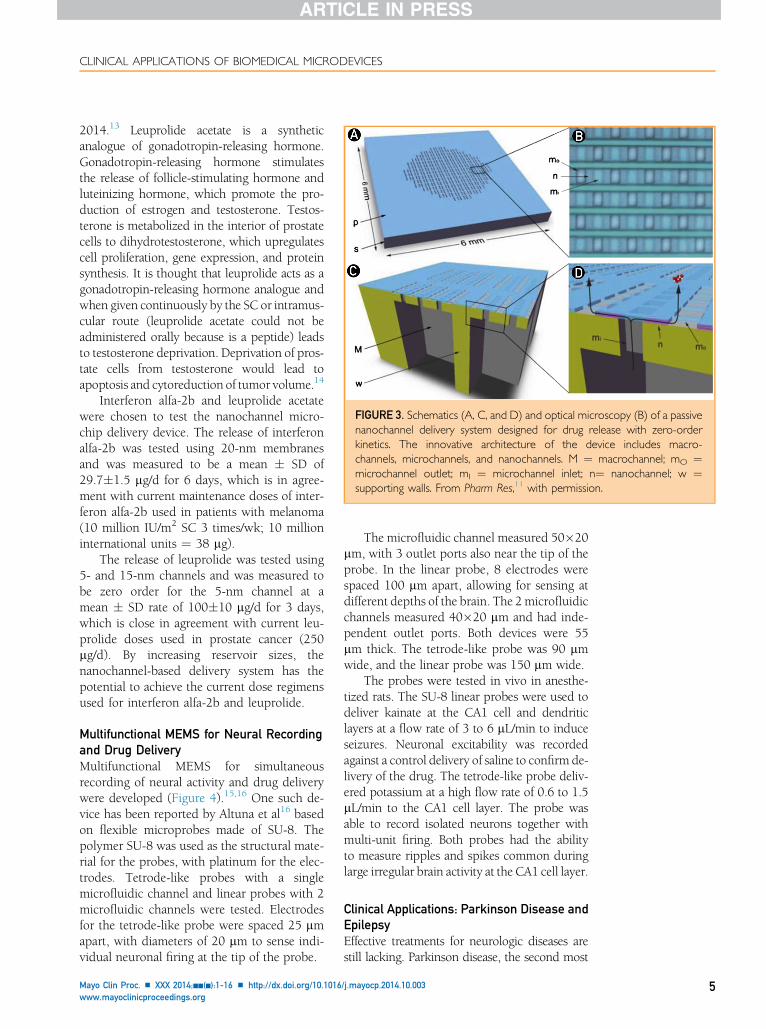
FIGURE 3. Schematics (A, C, and D) and optical microscopy (B) of a passivenanochannel delivery system designed for drug release with zero-orderkinetics. The innovative architecture of the device includes macro-channels, microchannels, and nanochannels. M ¼ macrochannel; mO ¼microchannel outlet; mI ¼ microchannel inlet; n¼ nanochannel; w ¼supporting walls. From Pharm Res,11 with permission.
CLINICAL APPLICATIONS OF BIOMEDICAL MICRODEVICES
2014.13 Leuprolide acetate is a syntheticanalogue of gonadotropin-releasing hormone.Gonadotropin-releasing hormone stimulatesthe release of follicle-stimulating hormone andluteinizing hormone, which promote the pro-duction of estrogen and testosterone. Testos-terone is metabolized in the interior of prostatecells to dihydrotestosterone, which upregulatescell proliferation, gene expression, and proteinsynthesis. It is thought that leuprolide acts as agonadotropin-releasing hormone analogue andwhen given continuously by the SC or intramus-cular route (leuprolide acetate could not beadministered orally because is a peptide) leadsto testosterone deprivation. Deprivation of pros-tate cells from testosterone would lead toapoptosis and cytoreduction of tumor volume.14
Interferon alfa-2b and leuprolide acetatewere chosen to test the nanochannel micro-chip delivery device. The release of interferonalfa-2b was tested using 20-nm membranesand was measured to be a mean � SD of29.7�1.5 mg/d for 6 days, which is in agree-ment with current maintenance doses of inter-feron alfa-2b used in patients with melanoma(10 million IU/m2 SC 3 times/wk; 10 millioninternational units ¼ 38 mg).
The release of leuprolide was tested using5- and 15-nm channels and was measured tobe zero order for the 5-nm channel at amean � SD rate of 100�10 mg/d for 3 days,which is close in agreement with current leu-prolide doses used in prostate cancer (250mg/d). By increasing reservoir sizes, thenanochannel-based delivery system has thepotential to achieve the current dose regimensused for interferon alfa-2b and leuprolide.
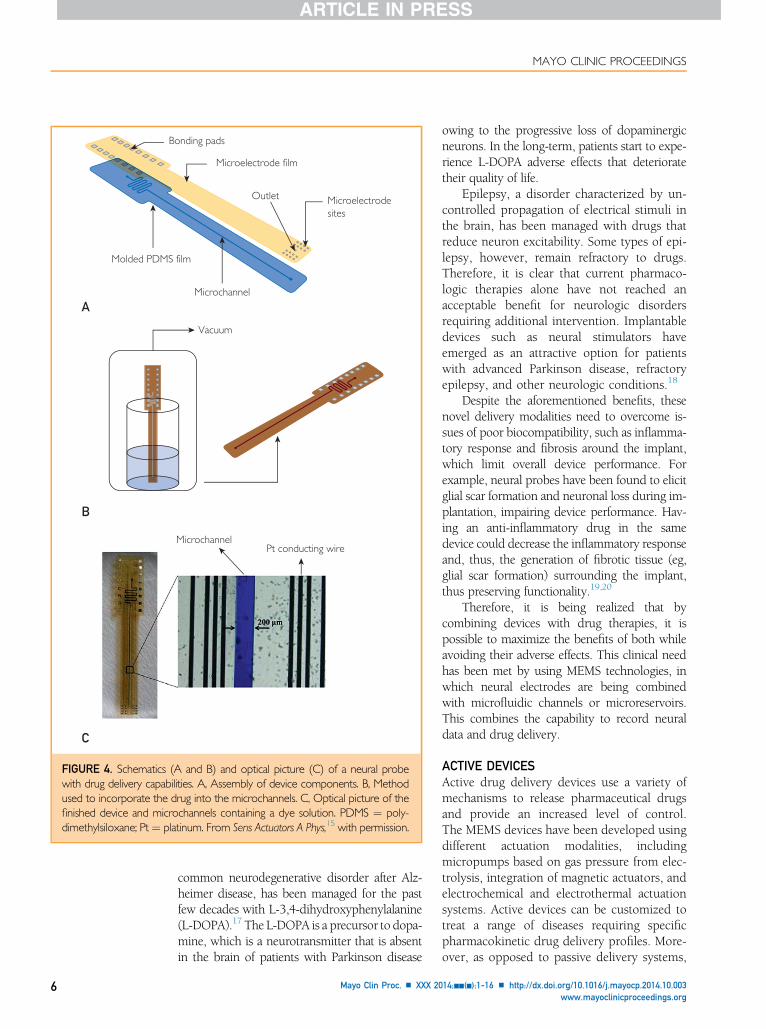
Multifunctional MEMS for Neural Recordingand Drug DeliveryMultifunctional MEMS for simultaneousrecording of neural activity and drug deliverywere developed (Figure 4).15,16 One such de-vice has been reported by Altuna et al16 basedon flexible microprobes made of SU-8. Thepolymer SU-8 was used as the structural mate-rial for the probes, with platinum for the elec-trodes. Tetrode-like probes with a singlemicrofluidic channel and linear probes with 2microfluidic channels were tested. Electrodesfor the tetrode-like probe were spaced 25 mmapart, with diameters of 20 mm to sense indi-vidual neuronal firing at the tip of the probe.
Mayo Clin Proc. n XXX 2014;nn(n):1-16 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
The microfluidic channel measured 50�20mm, with 3 outlet ports also near the tip of theprobe. In the linear probe, 8 electrodes werespaced 100 mm apart, allowing for sensing atdifferent depths of the brain. The 2microfluidicchannels measured 40�20 mm and had inde-pendent outlet ports. Both devices were 55mm thick. The tetrode-like probe was 90 mmwide, and the linear probe was 150 mm wide.
The probes were tested in vivo in anesthe-tized rats. The SU-8 linear probes were used todeliver kainate at the CA1 cell and dendriticlayers at a flow rate of 3 to 6 mL/min to induceseizures. Neuronal excitability was recordedagainst a control delivery of saline to confirm de-livery of the drug. The tetrode-like probe deliv-ered potassium at a high flow rate of 0.6 to 1.5mL/min to the CA1 cell layer. The probe wasable to record isolated neurons together withmulti-unit firing. Both probes had the abilityto measure ripples and spikes common duringlarge irregular brain activity at the CA1 cell layer.
Clinical Applications: Parkinson Disease andEpilepsyEffective treatments for neurologic diseases arestill lacking. Parkinson disease, the second most
/j.mayocp.2014.10.003 5
Bonding pads
Microelectrode film
Microelectrodesites
Outlet
Microchannel
Molded PDMS film
Vacuum
A
B
C
MicrochannelPt conducting wire
FIGURE 4. Schematics (A and B) and optical picture (C) of a neural probewith drug delivery capabilities. A, Assembly of device components. B, Methodused to incorporate the drug into the microchannels. C, Optical picture of thefinished device and microchannels containing a dye solution. PDMS ¼ poly-dimethylsiloxane; Pt¼ platinum. From Sens Actuators A Phys,15 with permission.
MAYO CLINIC PROCEEDINGS
6
common neurodegenerative disorder after Alz-heimer disease, has been managed for the pastfew decades with L-3,4-dihydroxyphenylalanine(L-DOPA).17 The L-DOPA is a precursor to dopa-mine, which is a neurotransmitter that is absentin the brain of patients with Parkinson disease
Mayo Clin Proc. n XXX 20
owing to the progressive loss of dopaminergicneurons. In the long-term, patients start to expe-rience L-DOPA adverse effects that deterioratetheir quality of life.
Epilepsy, a disorder characterized by un-controlled propagation of electrical stimuli inthe brain, has been managed with drugs thatreduce neuron excitability. Some types of epi-lepsy, however, remain refractory to drugs.Therefore, it is clear that current pharmaco-logic therapies alone have not reached anacceptable benefit for neurologic disordersrequiring additional intervention. Implantabledevices such as neural stimulators haveemerged as an attractive option for patientswith advanced Parkinson disease, refractoryepilepsy, and other neurologic conditions.18
Despite the aforementioned benefits, thesenovel delivery modalities need to overcome is-sues of poor biocompatibility, such as inflamma-tory response and fibrosis around the implant,which limit overall device performance. Forexample, neural probes have been found to elicitglial scar formation and neuronal loss during im-plantation, impairing device performance. Hav-ing an anti-inflammatory drug in the samedevice could decrease the inflammatory responseand, thus, the generation of fibrotic tissue (eg,glial scar formation) surrounding the implant,thus preserving functionality.19,20
Therefore, it is being realized that bycombining devices with drug therapies, it ispossible to maximize the benefits of both whileavoiding their adverse effects. This clinical needhas been met by using MEMS technologies, inwhich neural electrodes are being combinedwith microfluidic channels or microreservoirs.This combines the capability to record neuraldata and drug delivery.
ACTIVE DEVICESActive drug delivery devices use a variety ofmechanisms to release pharmaceutical drugsand provide an increased level of control.The MEMS devices have been developed usingdifferent actuation modalities, includingmicropumps based on gas pressure from elec-trolysis, integration of magnetic actuators, andelectrochemical and electrothermal actuationsystems. Active devices can be customized totreat a range of diseases requiring specificpharmacokinetic drug delivery profiles. More-over, as opposed to passive delivery systems,
14;nn(n):1-16 n http://dx.doi.org/10.1016/j.mayocp.2014.10.003www.mayoclinicproceedings.org
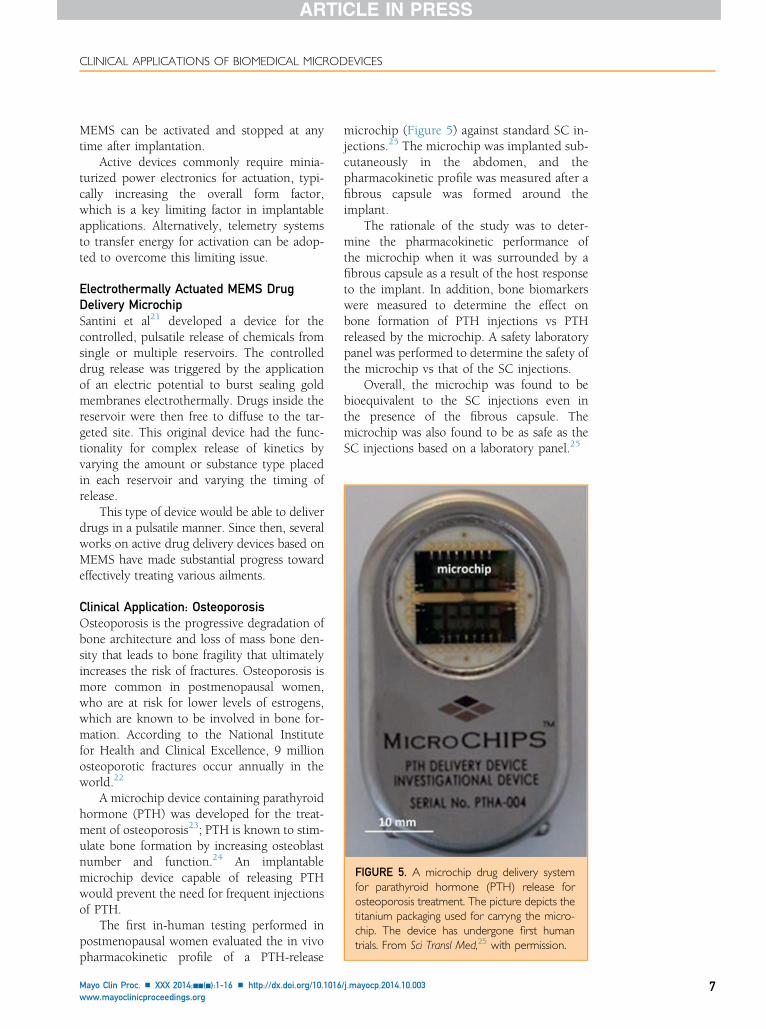
FIGURE 5. A microchip drug delivery systemfor parathyroid hormone (PTH) release forosteoporosis treatment. The picture depicts thetitanium packaging used for carryng the micro-chip. The device has undergone first humantrials. From Sci Transl Med,25 with permission.
CLINICAL APPLICATIONS OF BIOMEDICAL MICRODEVICES
MEMS can be activated and stopped at anytime after implantation.
Active devices commonly require minia-turized power electronics for actuation, typi-cally increasing the overall form factor,which is a key limiting factor in implantableapplications. Alternatively, telemetry systemsto transfer energy for activation can be adop-ted to overcome this limiting issue.
Electrothermally Actuated MEMS DrugDelivery MicrochipSantini et al21 developed a device for thecontrolled, pulsatile release of chemicals fromsingle or multiple reservoirs. The controlleddrug release was triggered by the applicationof an electric potential to burst sealing goldmembranes electrothermally. Drugs inside thereservoir were then free to diffuse to the tar-geted site. This original device had the func-tionality for complex release of kinetics byvarying the amount or substance type placedin each reservoir and varying the timing ofrelease.
This type of device would be able to deliverdrugs in a pulsatile manner. Since then, severalworks on active drug delivery devices based onMEMS have made substantial progress towardeffectively treating various ailments.
Clinical Application: OsteoporosisOsteoporosis is the progressive degradation ofbone architecture and loss of mass bone den-sity that leads to bone fragility that ultimatelyincreases the risk of fractures. Osteoporosis ismore common in postmenopausal women,who are at risk for lower levels of estrogens,which are known to be involved in bone for-mation. According to the National Institutefor Health and Clinical Excellence, 9 millionosteoporotic fractures occur annually in theworld.22
A microchip device containing parathyroidhormone (PTH) was developed for the treat-ment of osteoporosis23; PTH is known to stim-ulate bone formation by increasing osteoblastnumber and function.24 An implantablemicrochip device capable of releasing PTHwould prevent the need for frequent injectionsof PTH.
The first in-human testing performed inpostmenopausal women evaluated the in vivopharmacokinetic profile of a PTH-release
Mayo Clin Proc. n XXX 2014;nn(n):1-16 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
microchip (Figure 5) against standard SC in-jections.25 The microchip was implanted sub-cutaneously in the abdomen, and thepharmacokinetic profile was measured after afibrous capsule was formed around theimplant.
The rationale of the study was to deter-mine the pharmacokinetic performance ofthe microchip when it was surrounded by afibrous capsule as a result of the host responseto the implant. In addition, bone biomarkerswere measured to determine the effect onbone formation of PTH injections vs PTHreleased by the microchip. A safety laboratorypanel was performed to determine the safety ofthe microchip vs that of the SC injections.
Overall, the microchip was found to bebioequivalent to the SC injections even inthe presence of the fibrous capsule. Themicrochip was also found to be as safe as theSC injections based on a laboratory panel.25
/j.mayocp.2014.10.003 7

MAYO CLINIC PROCEEDINGS
8
A Rapid-Delivery Microchip for AcuteClinical ConditionsA microchip drug delivery system for rapid de-livery of vasopressin was developed by Elmanet al.26 The device consists of a membrane layer,an actuation layer, and a reservoir layer. Themembrane layer consists of a biocompatible sil-icon nitride film that serves as a hermetic seal forthe reservoirs. The actuation layer consists of 3microresistors. Heat is generated when a currentis passed through these microresistors. The heatserves to nucleate bubbles and dramatically in-crease internal pressure inside of the reservoir.This step leads to rupturing of the silicon nitridemembrane, followed by rapid release of thepharmaceutical drug, used as a bolus. A pictureof the device in action is shown in Figure 6.
Clinical Application: Hemorrhagic ShockHemorrhagic shock is an acute condition that canresult from severe traumatic injuries associatedwith massive bleeding loss, which if not treatedwithin seconds or minutes could result in perma-nent damage or death. In most cases, critical pa-tients do not have immediate access to a healthcare facility where basic measures to restore he-modynamic stability are available. These mea-sures include oxygenation; restoration ofintravascular volume with colloids, crystalloids,or blood products; and use of inotropic and vaso-pressor drugs. In settings with limited or no ac-cess to health care facilities, interventions toprevent massive hemorrhages include self-applied hemostatic dressings.
FIGURE 6. Pulsatile controlled delivery profileof a microelectromechanical systems devicewith a thermally induced actuator releasing drugout of a reservoir for emergency applications.From Biomed Microdevices,26 with permission.
Mayo Clin Proc. n XXX 20
This approach, however, does not accountfor internal bleeding sites, which occasionallyare themain cause of death. During hemorrhagicshock, the massive loss of blood compromisesvital organ activity in the brain, heart, and kid-neys, among others. The natural response ofthe body to avert vital organ damage is to pro-duce vasoconstriction to restore arterial bloodpressure and cardiac output to the level requiredtomaintain adequate oxygenation of vital organswhile avoiding further blood loss.27
Vasopressin and inotropic agents representan important tool in the management of hem-orrhagic shock.28-30 This biomedical microde-vice was designed to be implanted in high-riskpatients to deliver vasopressin for the manage-ment of hemorrhagic shock in emergency andambulatory settings. Finally, other potentialuses of the rapid-delivery microchip includeacute medical conditions that require immedi-ate intervention, such as cardiovascular andneurologic emergencies.
Magnetically Controlled MEMS Drug DeliveryA magnetic actuator MEMS drug delivery devicewas developed for the controlled release of achemotherapeutic agent. The device wasdesigned to avoid the use of batteries, improvingform factor. The device consists of a microreser-voir sealed by a thin magnetic membrane com-posite consisting of elastic polydimethylsiloxanematerial integrated with iron oxide nanoparticles.An external magnetic field applied by a neodym-ium iron boron permanentmagnet creates a forcethat allows the magnetic membrane to deflect.This process builds up pressure inside the reser-voir, enabling the drug to diffuse out through alaser-drilled micron-sized aperture.
On-demand release profiles can be createdfor optimal treatment using this device. Withno actuation, the mean � SD release of thedrug was measured to be 0.053�0.014 ng/min. With actuation of the membrane by appli-cation of a 255-mT magnetic field, the mean �SD release rate increased to 160�10.2 ng peractuation. The release rate exhibited sustaineddelivery for more than 35 days.31
Clinical Application: CancerDocetaxel was selected as a test drug to studythe device release profile. Docetaxel is an anti-neoplastic agent that disrupts the mitotic spin-dle, causing cell death; it is used for the
14;nn(n):1-16 n http://dx.doi.org/10.1016/j.mayocp.2014.10.003www.mayoclinicproceedings.org
Drug solution Drug reservoir
Parylene cannula
Intocannula
Into eye
Eye wall
Electrolysis pump
Pump outlet
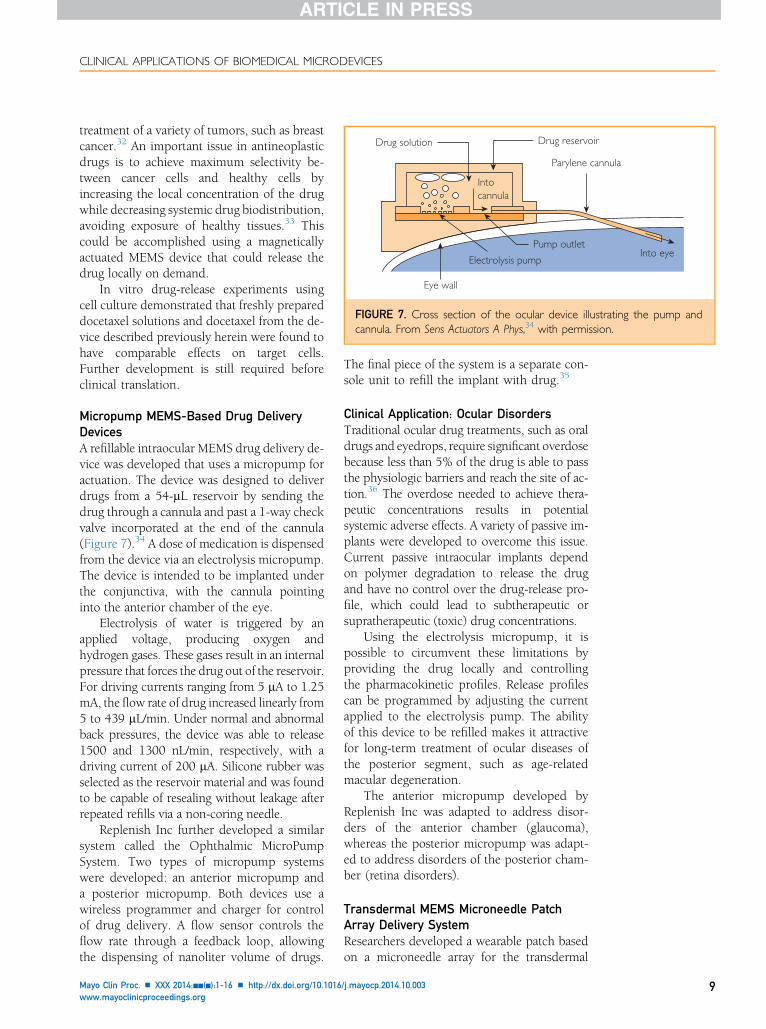
FIGURE 7. Cross section of the ocular device illustrating the pump andcannula. From Sens Actuators A Phys,34 with permission.
CLINICAL APPLICATIONS OF BIOMEDICAL MICRODEVICES
treatment of a variety of tumors, such as breastcancer.32 An important issue in antineoplasticdrugs is to achieve maximum selectivity be-tween cancer cells and healthy cells byincreasing the local concentration of the drugwhile decreasing systemic drug biodistribution,avoiding exposure of healthy tissues.33 Thiscould be accomplished using a magneticallyactuated MEMS device that could release thedrug locally on demand.
In vitro drug-release experiments usingcell culture demonstrated that freshly prepareddocetaxel solutions and docetaxel from the de-vice described previously herein were found tohave comparable effects on target cells.Further development is still required beforeclinical translation.
Micropump MEMS-Based Drug DeliveryDevicesA refillable intraocular MEMS drug delivery de-vice was developed that uses a micropump foractuation. The device was designed to deliverdrugs from a 54-mL reservoir by sending thedrug through a cannula and past a 1-way checkvalve incorporated at the end of the cannula(Figure 7).34 A dose of medication is dispensedfrom the device via an electrolysis micropump.The device is intended to be implanted underthe conjunctiva, with the cannula pointinginto the anterior chamber of the eye.
Electrolysis of water is triggered by anapplied voltage, producing oxygen andhydrogen gases. These gases result in an internalpressure that forces the drug out of the reservoir.For driving currents ranging from 5 mA to 1.25mA, the flow rate of drug increased linearly from5 to 439 mL/min. Under normal and abnormalback pressures, the device was able to release1500 and 1300 nL/min, respectively, with adriving current of 200 mA. Silicone rubber wasselected as the reservoir material and was foundto be capable of resealing without leakage afterrepeated refills via a non-coring needle.
Replenish Inc further developed a similarsystem called the Ophthalmic MicroPumpSystem. Two types of micropump systemswere developed: an anterior micropump anda posterior micropump. Both devices use awireless programmer and charger for controlof drug delivery. A flow sensor controls theflow rate through a feedback loop, allowingthe dispensing of nanoliter volume of drugs.
Mayo Clin Proc. n XXX 2014;nn(n):1-16 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
The final piece of the system is a separate con-sole unit to refill the implant with drug.35
Clinical Application: Ocular DisordersTraditional ocular drug treatments, such as oraldrugs and eyedrops, require significant overdosebecause less than 5% of the drug is able to passthe physiologic barriers and reach the site of ac-tion.36 The overdose needed to achieve thera-peutic concentrations results in potentialsystemic adverse effects. A variety of passive im-plants were developed to overcome this issue.Current passive intraocular implants dependon polymer degradation to release the drugand have no control over the drug-release pro-file, which could lead to subtherapeutic orsupratherapeutic (toxic) drug concentrations.
Using the electrolysis micropump, it ispossible to circumvent these limitations byproviding the drug locally and controllingthe pharmacokinetic profiles. Release profilescan be programmed by adjusting the currentapplied to the electrolysis pump. The abilityof this device to be refilled makes it attractivefor long-term treatment of ocular diseases ofthe posterior segment, such as age-relatedmacular degeneration.
The anterior micropump developed byReplenish Inc was adapted to address disor-ders of the anterior chamber (glaucoma),whereas the posterior micropump was adapt-ed to address disorders of the posterior cham-ber (retina disorders).
Transdermal MEMS Microneedle PatchArray Delivery SystemResearchers developed a wearable patch basedon a microneedle array for the transdermal
/j.mayocp.2014.10.003 9
Hypodermic nee
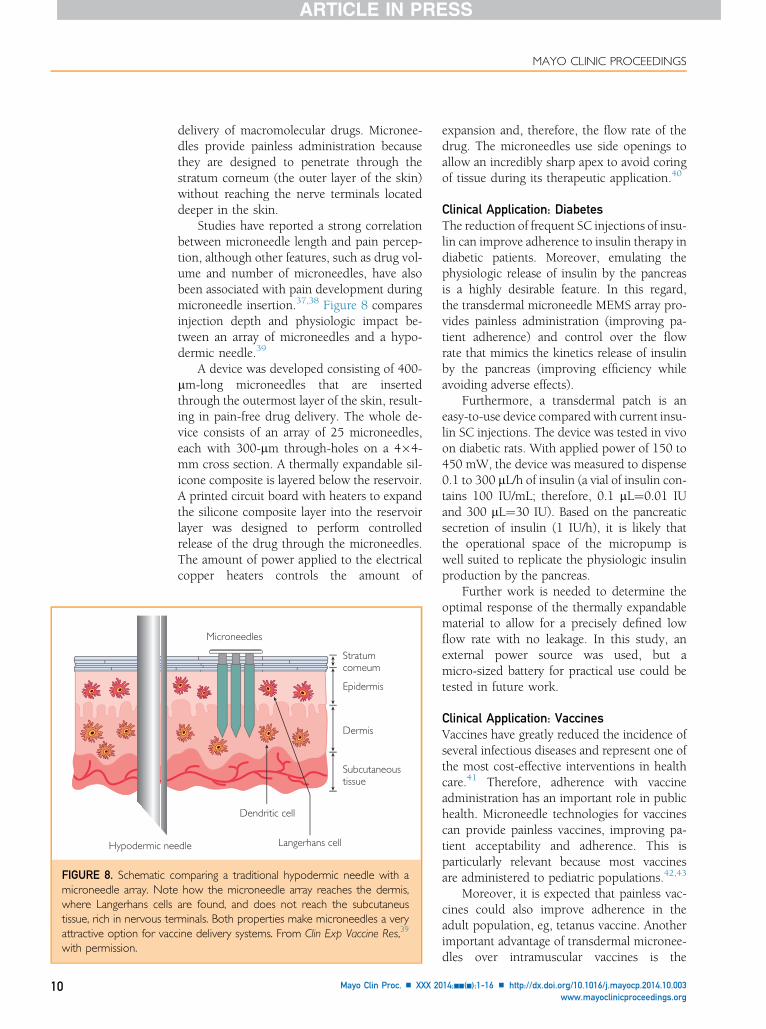
FIGURE 8. Schematic cmicroneedle array. Notewhere Langerhans cellstissue, rich in nervous terattractive option for vaccwith permission.
MAYO CLINIC PROCEEDINGS
10
delivery of macromolecular drugs. Micronee-dles provide painless administration becausethey are designed to penetrate through thestratum corneum (the outer layer of the skin)without reaching the nerve terminals locateddeeper in the skin.
Studies have reported a strong correlationbetween microneedle length and pain percep-tion, although other features, such as drug vol-ume and number of microneedles, have alsobeen associated with pain development duringmicroneedle insertion.37,38 Figure 8 comparesinjection depth and physiologic impact be-tween an array of microneedles and a hypo-dermic needle.39
A device was developed consisting of 400-mm-long microneedles that are insertedthrough the outermost layer of the skin, result-ing in pain-free drug delivery. The whole de-vice consists of an array of 25 microneedles,each with 300-mm through-holes on a 4�4-mm cross section. A thermally expandable sil-icone composite is layered below the reservoir.A printed circuit board with heaters to expandthe silicone composite layer into the reservoirlayer was designed to perform controlledrelease of the drug through the microneedles.The amount of power applied to the electricalcopper heaters controls the amount of
Stratumcorneum
Epidermis
Dermis
Subcutaneoustissue
Microneedles
dle
Dendritic cell
Langerhans cell
omparing a traditional hypodermic needle with ahow the microneedle array reaches the dermis,are found, and does not reach the subcutaneusminals. Both properties make microneedles a veryine delivery systems. From Clin Exp Vaccine Res,39
Mayo Clin Proc. n XXX 20
expansion and, therefore, the flow rate of thedrug. The microneedles use side openings toallow an incredibly sharp apex to avoid coringof tissue during its therapeutic application.40
Clinical Application: DiabetesThe reduction of frequent SC injections of insu-lin can improve adherence to insulin therapy indiabetic patients. Moreover, emulating thephysiologic release of insulin by the pancreasis a highly desirable feature. In this regard,the transdermal microneedle MEMS array pro-vides painless administration (improving pa-tient adherence) and control over the flowrate that mimics the kinetics release of insulinby the pancreas (improving efficiency whileavoiding adverse effects).
Furthermore, a transdermal patch is aneasy-to-use device compared with current insu-lin SC injections. The device was tested in vivoon diabetic rats. With applied power of 150 to450 mW, the device was measured to dispense0.1 to 300 mL/h of insulin (a vial of insulin con-tains 100 IU/mL; therefore, 0.1 mL¼0.01 IUand 300 mL¼30 IU). Based on the pancreaticsecretion of insulin (1 IU/h), it is likely thatthe operational space of the micropump iswell suited to replicate the physiologic insulinproduction by the pancreas.
Further work is needed to determine theoptimal response of the thermally expandablematerial to allow for a precisely defined lowflow rate with no leakage. In this study, anexternal power source was used, but amicro-sized battery for practical use could betested in future work.
Clinical Application: VaccinesVaccines have greatly reduced the incidence ofseveral infectious diseases and represent one ofthe most cost-effective interventions in healthcare.41 Therefore, adherence with vaccineadministration has an important role in publichealth. Microneedle technologies for vaccinescan provide painless vaccines, improving pa-tient acceptability and adherence. This isparticularly relevant because most vaccinesare administered to pediatric populations.42,43
Moreover, it is expected that painless vac-cines could also improve adherence in theadult population, eg, tetanus vaccine. Anotherimportant advantage of transdermal micronee-dles over intramuscular vaccines is the
14;nn(n):1-16 n http://dx.doi.org/10.1016/j.mayocp.2014.10.003www.mayoclinicproceedings.org
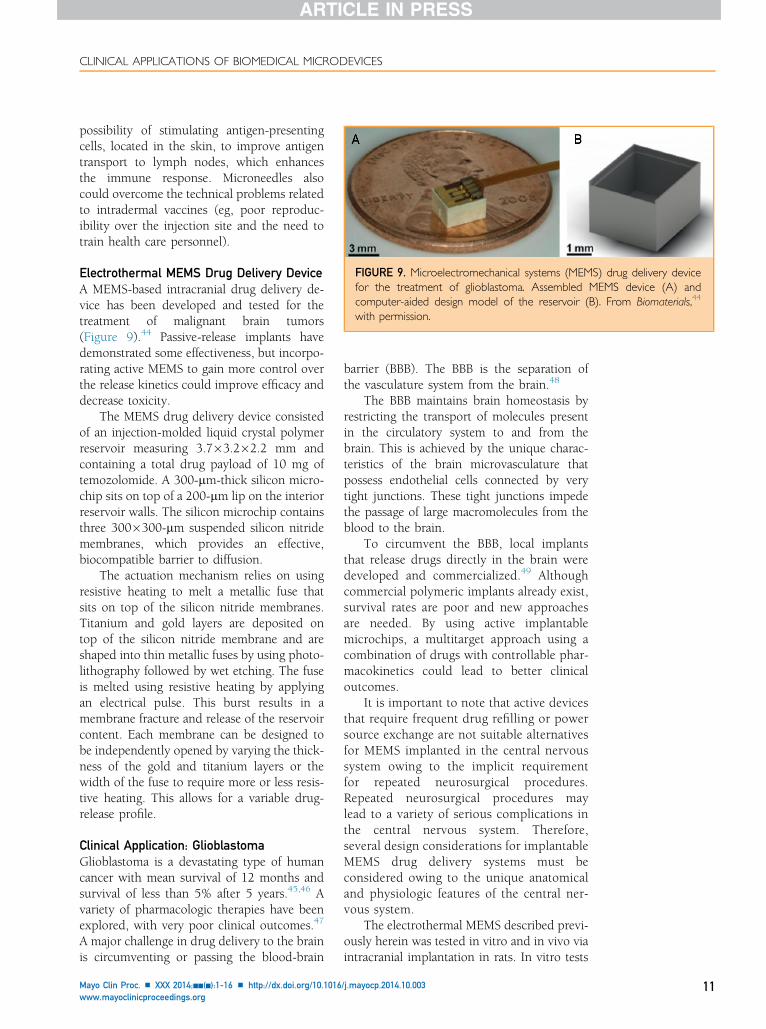
FIGURE 9. Microelectromechanical systems (MEMS) drug delivery devicefor the treatment of glioblastoma. Assembled MEMS device (A) andcomputer-aided design model of the reservoir (B). From Biomaterials,44
with permission.
CLINICAL APPLICATIONS OF BIOMEDICAL MICRODEVICES
possibility of stimulating antigen-presentingcells, located in the skin, to improve antigentransport to lymph nodes, which enhancesthe immune response. Microneedles alsocould overcome the technical problems relatedto intradermal vaccines (eg, poor reproduc-ibility over the injection site and the need totrain health care personnel).
Electrothermal MEMS Drug Delivery DeviceA MEMS-based intracranial drug delivery de-vice has been developed and tested for thetreatment of malignant brain tumors(Figure 9).44 Passive-release implants havedemonstrated some effectiveness, but incorpo-rating active MEMS to gain more control overthe release kinetics could improve efficacy anddecrease toxicity.
The MEMS drug delivery device consistedof an injection-molded liquid crystal polymerreservoir measuring 3.7�3.2�2.2 mm andcontaining a total drug payload of 10 mg oftemozolomide. A 300-mm-thick silicon micro-chip sits on top of a 200-mm lip on the interiorreservoir walls. The silicon microchip containsthree 300�300-mm suspended silicon nitridemembranes, which provides an effective,biocompatible barrier to diffusion.
The actuation mechanism relies on usingresistive heating to melt a metallic fuse thatsits on top of the silicon nitride membranes.Titanium and gold layers are deposited ontop of the silicon nitride membrane and areshaped into thin metallic fuses by using photo-lithography followed by wet etching. The fuseis melted using resistive heating by applyingan electrical pulse. This burst results in amembrane fracture and release of the reservoircontent. Each membrane can be designed tobe independently opened by varying the thick-ness of the gold and titanium layers or thewidth of the fuse to require more or less resis-tive heating. This allows for a variable drug-release profile.
Clinical Application: GlioblastomaGlioblastoma is a devastating type of humancancer with mean survival of 12 months andsurvival of less than 5% after 5 years.45,46 Avariety of pharmacologic therapies have beenexplored, with very poor clinical outcomes.47
A major challenge in drug delivery to the brainis circumventing or passing the blood-brain
Mayo Clin Proc. n XXX 2014;nn(n):1-16 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
barrier (BBB). The BBB is the separation ofthe vasculature system from the brain.48
The BBB maintains brain homeostasis byrestricting the transport of molecules presentin the circulatory system to and from thebrain. This is achieved by the unique charac-teristics of the brain microvasculature thatpossess endothelial cells connected by verytight junctions. These tight junctions impedethe passage of large macromolecules from theblood to the brain.
To circumvent the BBB, local implantsthat release drugs directly in the brain weredeveloped and commercialized.49 Althoughcommercial polymeric implants already exist,survival rates are poor and new approachesare needed. By using active implantablemicrochips, a multitarget approach using acombination of drugs with controllable phar-macokinetics could lead to better clinicaloutcomes.
It is important to note that active devicesthat require frequent drug refilling or powersource exchange are not suitable alternativesfor MEMS implanted in the central nervoussystem owing to the implicit requirementfor repeated neurosurgical procedures.Repeated neurosurgical procedures maylead to a variety of serious complications inthe central nervous system. Therefore,several design considerations for implantableMEMS drug delivery systems must beconsidered owing to the unique anatomicaland physiologic features of the central ner-vous system.
The electrothermal MEMS described previ-ously herein was tested in vitro and in vivo viaintracranial implantation in rats. In vitro tests
/j.mayocp.2014.10.003 11
MAYO CLINIC PROCEEDINGS
12
confirmed that more membranes beingopened leads to more rapid drug release.With 3 membranes activated, the release ratewas measured at 0.3 mg/h, and the mean �SD total release was 90%�3.2% in 30 hours.The release rate and mean � SD total releasedecreased to 0.136 mg/h and 82%�1.9%,respectively, in 60 hours for 2 membranesactivated; further decreases to 0.007 mg/hand 60%�12%, respectively, in 800 hourswas observed for 1 membrane activated.
Implantation and activation of the devicewas found to be effective in increasing survivaltime of 9-L glioblastoma rats. Activation of all3 membranes in the device on the day of im-plantation was the most effective. This deviceshowed improved efficacy via control of drugpharmacokinetics, but further studies areneeded to determine optimal release ratesand timing.
MEMS chip
Drug loa
Infusewithdra
MEMS chip
PuInto inner ear forintracochleardelivery
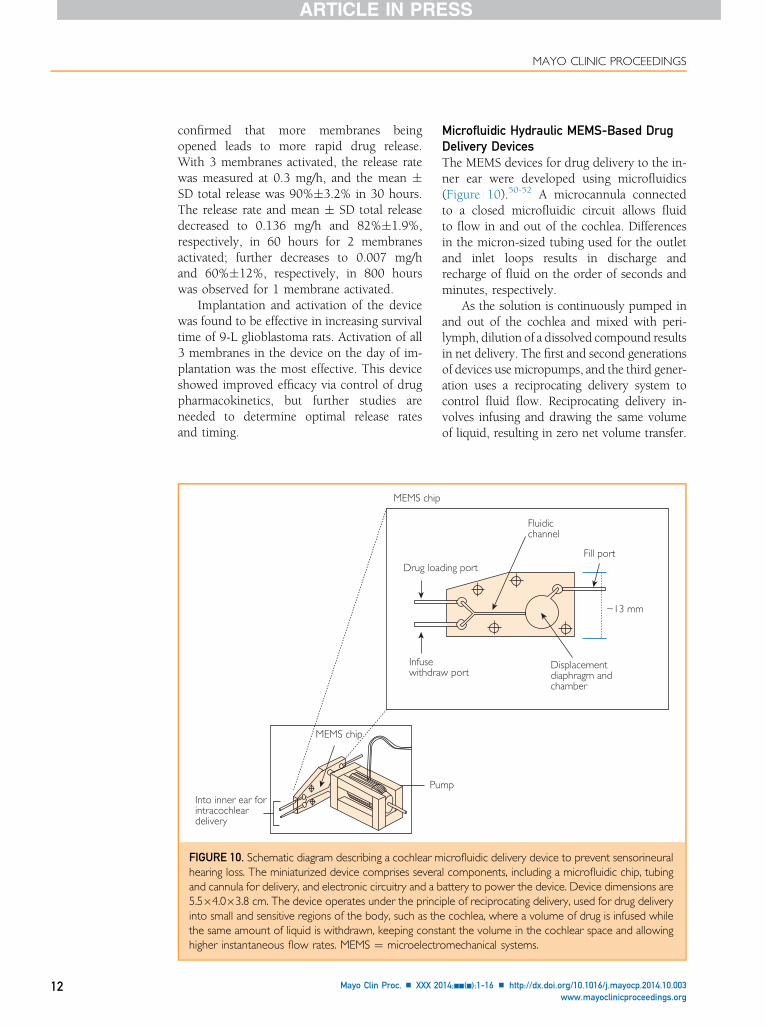
FIGURE 10. Schematic diagram describing a cochlear mhearing loss. The miniaturized device comprises severaand cannula for delivery, and electronic circuitry and a b5.5�4.0�3.8 cm. The device operates under the princinto small and sensitive regions of the body, such as ththe same amount of liquid is withdrawn, keeping consthigher instantaneous flow rates. MEMS ¼ microelectr
Mayo Clin Proc. n XXX 20
Microfluidic Hydraulic MEMS-Based DrugDelivery DevicesThe MEMS devices for drug delivery to the in-ner ear were developed using microfluidics(Figure 10).50-52 A microcannula connectedto a closed microfluidic circuit allows fluidto flow in and out of the cochlea. Differencesin the micron-sized tubing used for the outletand inlet loops results in discharge andrecharge of fluid on the order of seconds andminutes, respectively.
As the solution is continuously pumped inand out of the cochlea and mixed with peri-lymph, dilution of a dissolved compound resultsin net delivery. The first and second generationsof devices use micropumps, and the third gener-ation uses a reciprocating delivery system tocontrol fluid flow. Reciprocating delivery in-volves infusing and drawing the same volumeof liquid, resulting in zero net volume transfer.
Fluidicchannel
ding port
w portDisplacementdiaphragm andchamber
mp
Fill port
~13 mm
icrofluidic delivery device to prevent sensorineurall components, including a microfluidic chip, tubingattery to power the device. Device dimensions areiple of reciprocating delivery, used for drug deliverye cochlea, where a volume of drug is infused whileant the volume in the cochlear space and allowingomechanical systems.
14;nn(n):1-16 n http://dx.doi.org/10.1016/j.mayocp.2014.10.003www.mayoclinicproceedings.org

CLINICAL APPLICATIONS OF BIOMEDICAL MICRODEVICES
This technique is suitable for small spaces whereoverall volume is limited, such as delivery ofdrugs in the cochlea.
Biological back pressures in the cochlea wereconfirmed to have no noticeable effect ondischarge. The distribution of agents in the co-chlea was tested using 6,7-dinitroquinoxaline-2,3-dione to alter the generation of compoundaction potential. In vitro and in vivo studies inguinea pigs found increases in the compoundaction potential threshold, indicating effectivedrug penetration.
Clinical Application: Inner Ear DisordersInner ear disorders comprise a variety of clinicalconditions affecting the inner ear structure orthe auditory nerve. The inner ear anatomy in-volves the cochlea and the vestibular system.The cochlea is responsible for transducing soundwaves into electrical impulses that are trans-ported through the auditory nerve to the regionin the brain responsible for audition perception.
Disorders that affect either the sensing(cochlear) or transducing (auditory nerve)component of the auditory system are knownas sensorineural hearing loss (SNHL). It is esti-mated that SNHL affects nearly 250 millionpeople worldwide.52 Disorders affecting theinner ear include infectious diseases (eg,congenital rubella and congenital cytomegalo-virus), genetic disorders (such as mutations onthe gene for myosin VIIa, a protein found inthe stereocilia), and sensing elements of thehair cells located in the cochlea.
Other causes include trauma due to long-term exposure to loud sounds and drugs suchas aminoglycosides.53 The physiopathology ofSNHL involves damage to and death of thehair cells located in the corti organ (a region ofthe cochlea that contains hair cells and auditoryneurons). Hair cells are a specialized type of cellthat contain stereocilia, a type of organelle thatin response to acoustic waves opens ionic chan-nels, resulting in depolarization of hair cellmembranes. This leads to the release of neuro-transmitters, which transport action potentialsalong the auditory nerve to the regions of thebrain responsible for auditory function.
The development of the cochlear implanthas been a great achievement to restore hearingto people with deafness.54 Cochlear implantsaim to stimulate ganglion cells. With the contin-uous degeneration of these cells as a result of
Mayo Clin Proc. n XXX 2014;nn(n):1-16 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
infectious, traumatic, or genetic disorders,cochlear implants lose their efficacy. Therefore,drug delivery devices such as the reciprocatingmicropumps described previously herein repre-sent a novel and promising modality forrestoring auditory perception. These devicesmay allow delivery of neurotropic factors withzero net volume transfer, thus maintaining intra-cochlear pressure constant and preserving thesensing elements of the cochlea.55
REGULATORY PROCESS FOR CLINICALTRANSLATIONTo date, there are a few examples of MEMS formedical applications approved by the FDA,including the CardioMEMS wireless pressuresensor (St Jude Medical, Inc), the i-STATpoint-of-care blood analyzer device (AbbottLaboratories), and Fluzone (Sanofi PasteurInc), an influenza vaccine based on micronee-dles.56-60 Several of the MEMS drug deliverydevices described previously herein have notbeen approved by the FDA for clinical use. Itis possible, however, based on previous tech-nologies, such as prefilled syringes (a deviceprefilled with a drug) and the case of Fluzone(which was approved under a Biologics LicenseApplication), to describe a potential regulatorypathway for future drug delivery microdevices.
First, MEMS drug delivery systems involve atleast 2 components: a device and a drug. If theMEMS device incorporates the drug into the finalpackaged product (it is expected, owing to theirsmall size, that the device and the drug will becopackaged in a single product), they will beconsidered combination products.61,62 Second,according to the FDA Office of CombinationProducts, because the drug incorporated intothe device provides the main mechanism of ac-tion (the therapeutic effect is due to the drug;the device only releases the drug), the system isconsidered a drug. Drug products are subjectedto premarket approval through a New DrugApplication (NDA) submission or an AbbreviatedNDA (ANDA) submission.61,63 As mentionedpreviously, Fluzone was approved under a Bio-logics License Application, which is similar toan NDA.60
An NDA requires a complete descriptionof the manufacturing process and preclinicaland clinical studies with the device to establishsafety and effectiveness. When the drug beingused in the device has already been approved,
/j.mayocp.2014.10.003 13

MAYO CLINIC PROCEEDINGS
14
an ANDA might be required. An ANDA is lessstringent than an NDA, demanding only bio-equivalence studies to establish a similar phar-macokinetic profile with existing devices orformulations using the same drug.4
The future of drug delivery microdevices ispromising. Their novelty, their complexity,and the fact that they are implantable, however,will make regulatory approval a challengingendeavor.
PERSPECTIVEBiomedical microdevices for controlled drug de-livery represent the next generation of deliverymodalities that combine miniaturization, lowcost, batch manufacturability and reproduc-ibility, and integration with very large-scale inte-gration electronics, allowing programmabilityand active control over drug release. The currentdevelopment of drug delivery microdevices is atan early stage, and most of the technologies arestill in the proof-of-concept stage.
There are a few examples of successful clin-ical translation of biomedical microdevices, suchas the clinical use of vaccinemicroneedles. Thereare several reasons that some of themicrodevicesare still in the drug delivery pipeline.
From a clinical standpoint, there must be aclear and identified unmet clinical need wherecurrent solutions are still lacking. Even if theclinical need exists and is identified, many appli-cations (eg, infectious diseases) demand largedrug payloads that cannot be accommodatedwith microdevices or that would require peri-odic refilling. Moreover, bringing these devicesto the market entails a very high-risk endeavor.
Finally, regulatory issues could also pose asignificant barrier for bringing microedrugdelivery devices to the market. Some recentinitiatives at the FDA, such as the Center forDevices and Radiological Health Medical Inno-vation Initiative, potentially will help ensure afaster transition of novel biomedical microde-vices into the market.
CONCLUSIONRecent advances in drug delivery devices thatuse biomedical microdevices for controlled de-livery promise improved treatment for a vari-ety of acute and chronic illnesses. Passivedevices operate by releasing the pharmaceu-tical drugs from reservoirs through permeablestructures, which can also be degraded by
Mayo Clin Proc. n XXX 20
environmental triggers, such as pH and os-motic forces, to regulate the release rate.
Active devices require power to actuate apart that releases the drug after the device isdeployed. The release profile of the drug canbe actively controlled after the device has beenimplanted. Passive and active devices can beused as part of minimally invasive proceduresand have the ability to deliver drugs with a pre-cise pharmacokinetic profile, enhancing the effi-cacy and decreasing the toxicity of the drugbeing used.
These devices offer a range of clinical ap-plications in which tailored pharmacokinetics,local release, and high adherence are prerequi-sites. These clinical conditions include cancer,endocrine disorders, and ocular diseases,among many others. Drug delivery devicesrepresent a novel technology but face a varietyof regulatory challenges.
Further understanding of biocompatiblematerials, alternative techniques for drug releaseactuation, and closed-loop microdevices willenhance the capability of microdevices for clin-ical drug delivery. Microdevices for drug deliv-ery represent the next generation of platformsfor more accurate and efficient drug deliverysystems that will enable new therapeutic modal-ities. These novel platforms promise to increasepatient adherence and overall significantlyimprove treatment outcomes.
Abbreviations and Acronyms: ANDA = AbbreviatedNew Drug Application; BBB = blood-brain barrier; FDA =Food and Drug Administration; L-DOPA = L-3,4-dihydroxyphenylalanine; MEMS = microelectromechanicalsystems; NDA = New Drug Application; PTH = parathyroidhormone; SC = subcutaneous; SNHL = sensorineuralhearing loss
Grant Support: This work was supported by the US ArmyResearch Office via the Institute for Soldier Nanotechnol-ogies at Massachusetts Institute of Technology (contractW911NF-07-D-0004).
Correspondence: Address to Noel M. Elman, PhD, Institutefor Soldier Nanotechnologies, Massachusetts Institute ofTechnology, 500 Technology Square, Cambridge, MA02139 ([email protected]).
REFERENCES1. Madou MJ. Fundamentals of Microfabrication and Nanotech-
nology. 3rd ed. Boca Raton, FL: CRC Press; 2011.2. Huff MA. Medical applications of micro-electro mechanical sys-
tems technology. In: Rosen Y, Elman N, eds. Biomaterials Sci-ence: An Integrated Clinical and Engineering Approach. BocaRaton, FL: CRC Press; 2012.
14;nn(n):1-16 n http://dx.doi.org/10.1016/j.mayocp.2014.10.003www.mayoclinicproceedings.org
CLINICAL APPLICATIONS OF BIOMEDICAL MICRODEVICES
3. Polla DL, Erdman AG, Robbins WP, et al. Microdevices in med-icine. Annu Rev Biomed Eng. 2000;2:551-576.
4. Panescu D. MEMS in medicine and biology. IEEE Eng Med BiolMag. 2006;25(5):19-28.
5. Staples M, Daniel K, Cima MJ, Langer R. Application of micro-and nano-electromechanical devices to drug delivery. PharmRes. 2006;23(5):847-863.
6. Jain KK. Drug delivery systems: an overview. Methods Mol Biol.2008;437:1-50.
7. DURAGESIC website. http://www.duragesic.com. AccessedFebruary 5, 2014.
8. Posterior uveitis/Retisert. Psivida Corp website. http://www.psivida.com/products-retisert.html. Accessed February 5, 2014.
9. Baldi A, Lei M, Gu Y, Siegel RA, Ziaie B. A microstructuredsilicon membrane with entrapped hydrogels for environmen-tally sensitive fluid gating. Sens Actuators B Chem. 2006;114(1):9-18.
10. Ginter E, Simkon V. Type 2 diabetes mellitus, pandemic in 21stcentury. Adv Exp Med Biol. 2012;771:42-50.
11. Grattoni A, Shen H, Fine D, et al. Nanochannel technology forconstant delivery of chemotherapeutics: beyond metronomicadministration. Pharm Res. 2011;28(2):292-300.
12. Dieperink E, Ho SB, Tetrick L, Thuras P, Dua K, Willenbring ML.Suicidal ideation during interferon-alpha2b and ribavirin treat-ment of patients with chronic hepatitis C. Gen Hosp Psychiatry.2004;26(3):237-240.
13. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Can-cer J Clin. 2014;64(1):9-29.
14. Sethi R, Sanfilippo N. Six-month depot formulation of leupror-elin acetate in the treatment of prostate cancer. Clin Interv Aging.2009;4:259-267.
15. Gao K, Li G, Lia L, Cheng J, Zhao J, Xu Y. Fabrication of flexiblemicroelectrode arrays integrated with microfluidic channels forstable neural interfaces. Sens Actuators A Phys. 2013;197(1):9-14.
16. Altuna A, Bellistri E, Cid E. SU-8 based microprobes for simul-taneous neural depth recording and drug delivery in the brain.Lab Chip. 2013;13(7):1422-1430.
17. Khatri IA, Chaudhry US. Parkinson disease: a review. J Neurol Sci.2009;4(1):33-43.
18. Theodore WH, Fisher RS. Brain stimulation for epilepsy. LancetNeurol. 2004;3(2):111-118.
19. Retterer ST, Smith KL, Bjornsson CS, et al. Model neural pros-theses with integrated microfluidics: a potential interventionstrategy for controlling reactive cell and tissue responses. IEEETrans Biomed Eng. 2004;51(11):2063-2073.
20. Zhong Y, Bellamkonda RV. Dexamethasone-coated neuralprobes elicit attenuated inflammatory response and neuronalloss compared to uncoated neural probes. Brain Res. 2007;1148:15-27.
21. Santini JT Jr, Cima MJ, Langer R. A controlled-release microchip.Nature. 1999;397(6717):335-338.
22. National Insititute for Health and Care Excellence. Osteoporosis:Assesing the Risk of Fragility Fracture. Manchester, UK: NICE;2012:4-23:NICE clinical guideline 146.
23. Proos ER, Prescott JH, Staples MA. Long-term stability andin vitro release of hPTH(1e34) from a multi-reservoir array.Pharm Res. 2008;25(6):1387-1395.
24. Esbrit P, Alcaraz MJ. Current perspectives on parathyroidhormone (PTH) and PTH-related protein (PTHrP) as boneanabolic therapies. Biochem Pharmacol. 2013;85(10):1417-1423.
25. Farra R, Sheppard NF, McCabe L, et al. First-in-human testing ofa wirelessly controlled drug delivery microchip. Sci Transl Med.2012;4(122):1-12.
26. Elman NM, Ho Duc HL, Cima MJ. An implantable MEMS drugdelivery device for rapid delivery in ambulatory emergencycare. Biomed Microdevices. 2009;11(3):625-631.
27. Tintinally J, Kelen GD, Stapcszynsky JS. Emergency Medicine: AComprehensive Study Guide. 6th ed. New York, NY: McGraw-Hill Education; 2003.
Mayo Clin Proc. n XXX 2014;nn(n):1-16 n http://dx.doi.org/10.1016www.mayoclinicproceedings.org
28. Brunton L, Lazo J, Parker K, Lazo JS. Goodman and Gilman’s ThePharmacological Basis of Therapeutics. 11th ed. New York, NY:McGraw Hill Education; 2006.
29. Liu L, Tian K, Xue M, et al. Small doses of arginine vasopressin incombination with norepinephrine “buy” time for definitivetreatment for uncontrolled hemorrhagic shock in rats. Shock.2013;40(5):398-406.
30. Beloncle F, Meziani F, Lerolle N, Radermacher P, Asfar P. Doesvasopressor therapy have an indication in hemorrhagic shock?Ann Intensive Care. 2013;3(1):13.
31. Pirmoradi FN, Jackson J, Burt H, Chiao M. Delivery of an anti-cancer drug from a magnetically controlled MEMS deviceshows cytotoxicity in PC3 and HUVEC cells. In: Proceedingsfrom the 16th International Solid-State Sensors, Actuatorsand Microsystems Conference (TRANSDUCERS); June 5-9,2011; Beijing.
32. Alken S, Kelly MC. Benefit risk assessment and update on theuse of docetaxel in the management of breast cancer. CancerManag Res. 2013;5:357-365.
33. Wolinsky JB, Colson YL, Grinstaff MW. Local drug delivery stra-tegies for cancer treatment: gels, nanoparticles, polymeric films,rods, and wafers. J Control Release. 2012;159(1):14-26.
34. Li P-Y, Shih J, Lo R, et al. An electrochemical intraocular drugdelivery device. Sens Actuators A Phys. 2008;143:41-48.
35. Replesnish Inc website. http://www.replenishinc.com. AccesedSeptember 1, 2014.
36. Gaudana R, Ananthula HK, Parenky A, Mitra AK. Ocular drugdelivery. AAPS J. 2010;12(3):348-360.
37. Pierre MB, Rossetti FC. Microneedle-based drug delivery sys-tems for transdermal route. Curr Drug Targets. 2014;15(3):281-291.
38. Sachdeva V, Banga AK. Microneedles and their applications.Recent Pat Drug Deliv Formul. 2011;5(2):95-132.
39. Suh H, Shin J, Kim YC. Microneedle patches for vaccine deliv-ery. Clin Exp Vaccine Res. 2014;3(1):42-49.
40. Roxhed N, Samel B, Nordquist L, Griss P, Stemme G. Painlessdrug delivery though Microneedle-based transdermal patchesfeaturing active infusion. IEEE Trans Biomed Eng. 2008;55(3):1063-1071.
41. Greenwood B, Salisbury D, Hill AV. Vaccines and global health.Philos Trans R Soc Lond B Biol Sci. 2011;366(1579):2733-2742.
42. Prausnitz MR, Mikszta JA, Cormier M, Andrianov AK.Microneedle-based vaccines. Curr Top Microbiol Immunol.2009;333:369-393.
43. Kim YC, Park JH, Prausnitz MR. Microneedles for drug and vac-cine delivery. Adv Drug Deliv Rev. 2012;64(14):1547-1568.
44. Masi BC, Tyler BM, Bow H, et al. Intracranial MEMS basedtemozolomide delivery in a 9L gliosarcoma model. Biomaterials.2012;33(23):5768-5775.
45. Davis ME, Stoiber AM. Glioblastoma multiforme: enhancingsurvival and quality of life. Clin J Oncol Nurs. 2011;15(3):291-297.
46. Omuro A, DeAngelis LM. Glioblastoma and other malignantgliomas: a clinical review. JAMA. 2013;310(17):1842-1850.
47. Neyns B, D’haeseleer M, Rogiers A, et al. The role of cytotoxicdrugs in the treatment of central nervous system gliomas. ActaNeurol Belg. 2010;110(1):1-14.
48. Domb A, Maniar M, Bogdansky S, Chasin M. Drug delivery tothe brain using polymers. Crit Rev Ther Drug Carrier Syst. 1991;8(1):1-17.
49. Panigrahi M, Das PK, Parikh PM. Brain tumor and Gliadel wafertreatment. Indian J Cancer. 2011;48(1):11-17.
50. Fiering J. Local drug delivery with a self-contained, programma-ble, microfluidic system. Biomed Microdevices. 2008;11(3):571-578.
51. Pararas EE, Borkholder DA, Borenstein JT. Microsystems tech-nologies for drug delivery to the inner ear. Adv Drug Deliv Rev.2012;64(14):1650-1660.
52. Borestein JB. Intracochlear drug delivery systems. Expert OpinDrug Deliv. 2011;8(9):1161-1174.
/j.mayocp.2014.10.003 15
MAYO CLINIC PROCEEDINGS
16
53. Haddad J. The ear. In: Nelson Textbook of Pediatrics. 17th ed.Philadelphia, PA: Elsevier Health Sciences; 2003.
54. Lenarz T, Pau HW, Paasche G. Cochlear implants. Curr PharmBiotechnol. 2013;14(1):112-123.
55. Budenz CL, Pfingst BE, Raphael Y. The use of neurotrophintherapy in the inner ear to augment cochlear implantation out-comes. Anat Rec (Hoboken). 2012;295(11):1896-1908.
56. FDA approves first implantable wireless device with remotemonitoring to measure pulmonary artery pressure in certain heartfailure patients. Food and Drug Administration website. http://www.fda.gov/newsevents/newsroom/pressannouncements/ucm399024.htm. Published May 28, 2014. Accessed June 5, 2014.
57. St. Jude Medical acquires CardioMEMS and announces FDAapproval of heart failure (HF) monitoring technology. St JudeMedical website. http://www.sjm.com/cardiomems. AccessedFebruary 5, 2014.
58. The i-STAT� system: advanced handheld and test cartridgeblood analysis system that delivers lab-quality results. Abbott
Mayo Clin Proc. n XXX 20
Laboratories website. http://www.abbottpointofcare.com/Products-and-Services.aspx. Accessed February 5, 2014.
59. Icardi G, Orsi A, Ceravolo A, Ansaldi F. Current evidence on in-tradermal influenza vaccines administered by Soluvia� licensedmicro injection system. Hum Vaccin Immunother. 2012;8(1):67-75.
60. May 15, 2012 approval letter: Fluzone, Fluzone high-dose andFluzone intradermal. FDA website. http://www.fda.gov/biologicsbloodvaccines/vaccines/approvedproducts/ucm305015.htm. Accessed February 5, 2014.
61. Siegel EB, ed. Development and Approval of CombinationProducts: A Regulatory Perspective. Hoboken, NJ: John Wiley &Sons; 2008.
62. Gurman P, Chi A, Hood T, et al. Prefilled devices for parenteralapplications. Expert Rev Med Devices. 2014;11(2):205-223.
63. Gurman P, Rabinovitz O, Hunter TB. Regulatory challenges onbiomaterials: focus on medical devices. In: Rosen Y, Elman NM,eds. Biomaterials Science: a Clinical and Engineering Approach.Boca Raton, FL: CRC Press; 2012.
14;nn(n):1-16 n http://dx.doi.org/10.1016/j.mayocp.2014.10.003www.mayoclinicproceedings.org





























