Embed Size (px)
Citation preview

Can Respir J Vol 19 No 3 May/June 2012 193
Birt-Hogg-Dubé syndrome: Report of a new mutationHabib U Rehman FRCPI FRCP, FRCP(Glas) FACP
Regina Qu’Appelle Health Region, Regina, SaskatchewanCorrespondence: Dr Habib U Rehman, Regina Qu’Appelle Health Region, 1440-14th Avenue, Regina, Saskatchewan S4P 0W5.
Telephone 306-565-4120, fax 306-566-4150, e-mail [email protected]
Learning objectives• Recognizedifferentunderlyingfamilialcausesofspontaneous
pneumothorax.• UnderstandthegeneticbasisofBirt-Hogg-Dubésyndrome.• ComprehendthescreeningstrategiesinBirt-Hogg-Dubé
syndrome.
Pre-test
• WhataretheclinicalfeaturesofBirt-Hogg-Dubésyndrome?• Giveadifferentialdiagnosisoffamilialsyndromesof
pneumothorax.
CASE PRESENTATIONA47year-oldwomanofFrenchandItaliandescentpresentedtotheemergencyroomwithincreasingshortnessofbreathonexertionofafewdaysduration.Shedeniedanychestpain,cough,fevers,orthopneaorparoxysmalnocturnaldyspnea.Thepatientweighed121.5kg.Herheightwas165 cmandherbloodpressurewas126/88mmHg.Multiplepaleyellow-whitedome-shapednoduleswereseenonher face,neckanduppertrunk(Figure1).Shewastachypneic.Examinationofherchest revealedhyper-resonance and reduced breath sounds over therightlung.Nocracklesorwheezeswereaudible.Thetracheawasdevi-atedtotheleft.Anx-rayofthechestshowedalargerightpneumo-thorax,completecollapseoftherightlungandmediastinalshifttotheleft.Theremainderofthephysicalexaminationwasunremarkable.AHeimlich valve was placed, resulting in complete expansion of herrightlung.
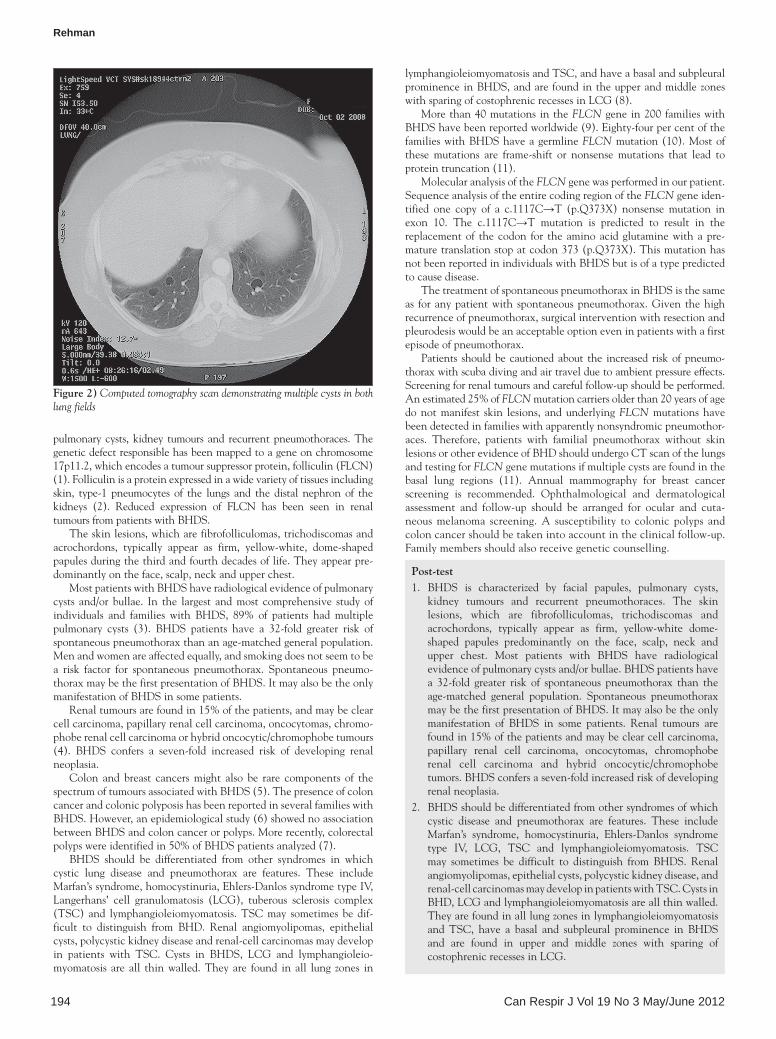
Thepatient’smedicalhistorywassignificantforrecurrentpneumo-thoraces.Sheexperiencedherfirstpneumothoraxontherightsideat41 years of age, whichwas treatedwith percutaneous drainage. Sixyearslater,sheexperiencedtwoadditionalpneumothoracesinvolvingthe right lung, which were treated with percutaneous drainage andplacement of a Heimlich valve. A previously performed computedtomography(CT)scanofthechestrevealedmultiplethin-walledcystsinboth lungsandacystalongthepleural surfaceof therightupperlobe(Figure2).Fibrofolliculomawasdiagnosedonthebasisofaskinbiopsysevenyearspreviously.Shewasnotasmoker.
Familyhistorywassignificantforfaciallesionsandpulmonarycystsinherfatherandapaternaluncle,andrecurrentpneumothoracesinapaternalaunt.Hersisterwasdiagnosedwithbreastcancerat44yearsofageandpassedawayat60yearsofage.Fourmaternalauntsandhermaternalgrandmotheralsohadbreastcancer.Onepaternalauntwhohad a history of recurrent pneumothoraces died of cancer of theadrenalgland,andapaternalunclediedofrenalcarcinoma.Herpater-nalgrandmotherhaddiedoflungcancer.
A clinical diagnosis of Birt-Hogg-Dubé syndrome (BHDS) wasmade. Further investigations revealed a normal CT scan of theabdomenandpelvis.Pulmonary function testsdemonstratednormalspirometry,lungvolumesanddiffusioncapacity.
Arightthoracotomywasperformedwithwedgeresectionofthreeblebsandpleurectomy.Microscopicexaminationofthesurgicalspeci-men showed neutrophilic infiltration of the blebwalls. The pleuralspecimenalsoshowedfocalactiveinflammation.
Sequencinganalysisofthefolliculin(FLCN)geneidentifiedonecopyofac.1117C→T(p.Q373X)nonsensemutation.
DISCuSSIONBHDS is an autosomal dominant genodermatosis caused by germlinemutations in the FLCN gene and characterized by facial papules,
clinico-patHologic confeRences
©2012 Pulsus Group Inc. All rights reserved
Hu Rehman. Birt-Hogg-Dubé syndrome: Report of a new mutation. Can Respir J 2012;19(3):193-195.
Birt-Hogg-Dubé syndrome is an autosomal dominant genodermatosiscausedbygermlinemutationsinthefolliculingeneandcharacterizedbyfacialpapules,pulmonarycysts,kidneytumoursandrecurrentpneumotho-races.Severaldistinctmutationsinthefolliculingeneresultinginatrun-cated protein have been described. The present report describes a newmutation, which has not been reported in individuals with Birt-Hogg-Dubésyndromebutisofatypepredictedtocausedisease.
Key Words: Fibrofolliculoma; Folliculin; Pneumothorax; Pulmonary cysts; Renal tumour
Le syndrome de Birt-Hogg-Dubé : rapport d’une nouvelle mutation
Le syndrome de Birt-Hogg-Dubé est une génodermatose autosomiquedominante causée par desmutations des cellules germinales du gène defolliculineetcaractériséepardespapulesfaciales,deskystespulmonaires,des tumeurs rénalesetdespneumothoraxrécurrents.Plusieursmutationsdistinctesdugènedefolliculineresponsabledelatroncationd’uneproté-ineontétédécrites.Leprésentrapportdécritunenouvellemutation,quin’a pas été signalée chez les personnes ayant le syndromedeBirt-Hogg-Dubé,maisquiestd’untypepréditcommeresponsabledelamaladie.
Figure 1) Facial nodules (fibrofolliculomas)
Rehman
Can Respir J Vol 19 No 3 May/June 2012194
pulmonary cysts, kidney tumours and recurrentpneumothoraces.Thegeneticdefectresponsiblehasbeenmappedtoageneonchromosome17p11.2,whichencodesatumoursuppressorprotein,folliculin(FLCN)(1).Folliculinisaproteinexpressedinawidevarietyoftissuesincludingskin, type-1 pneumocytes of the lungs and the distal nephron of thekidneys (2). Reduced expression of FLCN has been seen in renaltumoursfrompatientswithBHDS.
Theskinlesions,whicharefibrofolliculomas,trichodiscomasandacrochordons, typically appear as firm, yellow-white, dome-shapedpapulesduringthethirdandfourthdecadesoflife.Theyappearpre-dominantlyontheface,scalp,neckandupperchest.
MostpatientswithBHDShaveradiologicalevidenceofpulmonarycysts and/or bullae. In the largest andmost comprehensive study ofindividuals and families with BHDS, 89% of patients hadmultiplepulmonary cysts (3). BHDS patients have a 32-fold greater risk ofspontaneouspneumothoraxthananage-matchedgeneralpopulation.Menandwomenareaffectedequally,andsmokingdoesnotseemtobea risk factor for spontaneous pneumothorax. Spontaneous pneumo-thoraxmaybethefirstpresentationofBHDS.ItmayalsobetheonlymanifestationofBHDSinsomepatients.
Renaltumoursarefoundin15%ofthepatients,andmaybeclearcellcarcinoma,papillaryrenalcellcarcinoma,oncocytomas,chromo-phoberenalcellcarcinomaorhybridoncocytic/chromophobetumours(4). BHDS confers a seven-fold increased risk of developing renalneoplasia.
Colon and breast cancersmight also be rare components of thespectrumoftumoursassociatedwithBHDS(5).ThepresenceofcoloncancerandcolonicpolyposishasbeenreportedinseveralfamilieswithBHDS.However,anepidemiologicalstudy(6)showednoassociationbetweenBHDSandcoloncancerorpolyps.Morerecently,colorectalpolypswereidentifiedin50%ofBHDSpatientsanalyzed(7).
BHDS should be differentiated from other syndromes in whichcystic lung disease and pneumothorax are features. These includeMarfan’ssyndrome,homocystinuria,Ehlers-DanlossyndrometypeIV,Langerhans’ cell granulomatosis (LCG), tuberous sclerosis complex(TSC) and lymphangioleiomyomatosis.TSCmay sometimes be dif-ficult to distinguish from BHD. Renal angiomyolipomas, epithelialcysts,polycystickidneydiseaseandrenal-cellcarcinomasmaydevelopin patients with TSC. Cysts in BHDS, LCG and lymphangioleio-myomatosis are all thinwalled.They are found in all lung zones in
lymphangioleiomyomatosisandTSC,andhaveabasalandsubpleuralprominenceinBHDS,andare foundintheupperandmiddlezoneswithsparingofcostophrenicrecessesinLCG(8).
Morethan40mutations intheFLCNgene in200 familieswithBHDShavebeenreportedworldwide(9).Eighty-fourpercentofthefamilieswithBHDShaveagermlineFLCNmutation(10).Mostofthesemutations are frame-shift or nonsensemutations that lead toproteintruncation(11).
MolecularanalysisoftheFLCNgenewasperformedinourpatient.SequenceanalysisoftheentirecodingregionoftheFLCNgeneiden-tified one copy of a c.1117C→T (p.Q373X) nonsensemutation inexon 10. The c.1117C→T mutation is predicted to result in thereplacementof the codon for the aminoacid glutaminewith apre-maturetranslationstopatcodon373(p.Q373X).ThismutationhasnotbeenreportedinindividualswithBHDSbutisofatypepredictedtocausedisease.
ThetreatmentofspontaneouspneumothoraxinBHDSisthesameas for anypatientwith spontaneouspneumothorax.Given thehighrecurrenceofpneumothorax,surgicalinterventionwithresectionandpleurodesiswouldbeanacceptableoptioneveninpatientswithafirstepisodeofpneumothorax.
Patients shouldbe cautionedabout the increased riskofpneumo-thoraxwithscubadivingandairtravelduetoambientpressureeffects.Screeningforrenaltumoursandcarefulfollow-upshouldbeperformed.Anestimated25%ofFLCNmutationcarriersolderthan20yearsofagedonotmanifest skin lesions, andunderlyingFLCNmutationshavebeendetectedinfamilieswithapparentlynonsyndromicpneumothor-aces. Therefore, patients with familial pneumothorax without skinlesionsorotherevidenceofBHDshouldundergoCTscanofthelungsandtestingforFLCNgenemutationsifmultiplecystsarefoundinthebasal lung regions (11). Annual mammography for breast cancerscreening is recommended. Ophthalmological and dermatologicalassessment and follow-up should be arranged for ocular and cuta-neousmelanoma screening.A susceptibility to colonic polyps andcoloncancershouldbetakenintoaccountintheclinicalfollow-up.Familymembersshouldalsoreceivegeneticcounselling.
Figure 2) Computed tomography scan demonstrating multiple cysts in both lung fields
Post-test1. BHDS is characterized by facial papules, pulmonary cysts,
kidney tumours and recurrent pneumothoraces. The skinlesions, which are fibrofolliculomas, trichodiscomas andacrochordons, typically appear as firm, yellow-white dome-shaped papules predominantly on the face, scalp, neck andupper chest. Most patients with BHDS have radiologicalevidenceofpulmonarycystsand/orbullae.BHDSpatientshavea 32-fold greater risk of spontaneous pneumothorax than theage-matched general population. Spontaneous pneumothoraxmaybethefirstpresentationofBHDS.Itmayalsobetheonlymanifestation of BHDS in some patients. Renal tumours arefoundin15%ofthepatientsandmaybeclearcellcarcinoma,papillary renal cell carcinoma, oncocytomas, chromophoberenal cell carcinoma and hybrid oncocytic/chromophobetumors.BHDSconfersaseven-foldincreasedriskofdevelopingrenalneoplasia.
2. BHDSshouldbedifferentiatedfromothersyndromesofwhichcystic disease and pneumothorax are features. These includeMarfan’s syndrome, homocystinuria, Ehlers-Danlos syndrometype IV, LCG, TSC and lymphangioleiomyomatosis. TSCmay sometimes be difficult to distinguish from BHDS. Renalangiomyolipomas,epithelialcysts,polycystickidneydisease,andrenal-cellcarcinomasmaydevelopinpatientswithTSC.CystsinBHD,LCGandlymphangioleiomyomatosisareallthinwalled.Theyarefoundinalllungzonesinlymphangioleiomyomatosisand TSC, have a basal and subpleural prominence in BHDSand are found in upper and middle zones with sparing ofcostophrenicrecessesinLCG.

Birt-Hogg-Dubé syndrome
Can Respir J Vol 19 No 3 May/June 2012 195
TheCanadian Respiratory JournalisnowacceptingsubmissionsforanewClinico-PathologicConferencesseries.Thesewillbebasedoncasepresentationsthatillustrateimportantlearningissuesinvolvingdiagnosisand/ormanagementdecisions,andshouldbesupportedbyimagesfromappropriatelyapplieddiagnosticand/orprognostictestingwhichcouldinclude:1)Lungfunctiontests;2)Exercisetesting;3)X-raysorcomputedtomographyscans;4)Ultrasound(includingendobronchialultrasound);5)Positronemissiontomographyscans;or6)Bronchoscopy/thoracoscopy.
AllcasereportsappearingintheCanadian Respiratory JournalwillconformtothisformatandmanuscriptsshouldbestructuredasdescribedintheInstructionstoAuthors.Amaximumoffourimagescanbesubmittedandthenumberofreferencesshouldnotusuallyexceed10.Thesubmissionwillbepeerreviewedandmaybeeditedbyoureditorialteam.
REFERENCES1.SchmidtLS,WarrenMB,NickersonML,etal.Birt-Hogg-Dubesyndrome,agenodermatosesassociatedwithspontaneouspneumothoraxandkidneyneoplasia,mapstochromosome17p11.2.AmJHumGenet2001;69:876-82.
2.WarrenMB,Torres-CabalaCA,TurnerML.ExpressionofBirt-Hogg-DubegenemRNAinnormalandneoplastichumantissues.ModPathol2004;17:998-1011.
3.ToroJR,PautlerSE,StewartL,etal.Lungcysts,spontaneouspneumothorax,andgeneticassociationsin89familieswithBirt-Hogg-Dubésyndrome.AmJRespirCritCareMed2007;175:1044-53.
4.ZbarB,AlvordWG,GlennG,etal.RiskofrenalandcolonicneoplasmsandspontaneouspneumothoraxintheBirt-Hogg-Dubesyndrome.CancerEpidemiolBiomarkersPrev2002;11:393-400.
5.PalmirottaR,SavonarolaA,LudoviciG,etal.AssociationbetweenBirtHoggDubésyndromeandcancerpredisposition.AnticancerRes2010;30:751-7.
6.ZbarB,AlwordWG,GlennG,etal.RiskofrenalandcolonicneoplasmsandspontaneouspneumothoraxintheBirtHoggDubésyndrome.CancerEpidemiolBiomarkers2002;11:393-400.
7.KlugerN,GiraudS,CoupierI,etal.BirtHoggDubésyndrome:Clinicalandgeneticstudiesof10Frenchfamilies.BrJDermatol2010;162:527-37.
8.GrantLA,BabarJ,GriffinN.Cysts,cavitiesandhoneycombinginmultisystemdisorders:DifferentialdiagnosisandfindingsonthinsectionCT.ClinRadiol2009;64:439-48.
9.ToroJR,WeiM-H,GlennGM,etal.BHDmutations,clinicalandmoleculargeneticinvestigationsofBirt-Hogg-Dubésyndrome:Anewseriesof50familiesandareviewofpublishedreports.JMedGenet2008;45:321-31.
10. MenkoFH,vanSteenselMAM,GiraudS,etal;EuropeanBHDConsortium.Birt-Hogg-Dubésyndrome:Diagnosisandmanagement.LancetOncol2009;10:1199-206.
11. SchmidtLS,NickersonML,WarrenMB,etal.GermlineBHD-mutationspectrumandphenotypeanalysisofalargecohortoffamilieswithBirt-Hogg-Dubésyndrome.AmJHumGenet2005;76:1023-33.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com



![Birt-Hogg-Dubé syndrome in Korean: clinicora- diologic features … · 2019. 7. 1. · INTRODUCTION Birt-Hogg-Dubé (BHD) syndrome, initially described in 1977 [1], is a rare autosomal](https://img.pdfslide.net/doc/110x75/5fdc1f2a21c2bc7b72151d64/birt-hogg-dub-syndrome-in-korean-clinicora-diologic-features-2019-7-1-introduction.jpg)

























