Embed Size (px)
Citation preview

Bleeding DisordersBleeding Disorders
Jaya V Juturi, MDJaya V Juturi, MD
Texas Oncology, PATexas Oncology, PA

HEMOSTASISHEMOSTASISRegulating factorsRegulating factors
Vessel Wall IntegrityVessel Wall Integrity
Adequate Numbers of PlateletsAdequate Numbers of Platelets
Proper Functioning PlateletsProper Functioning Platelets
Adequate Levels of Clotting FactorsAdequate Levels of Clotting Factors
Proper Function of Fibrinolytic PathwayProper Function of Fibrinolytic Pathway

HEMOSTASIS
1. VASCULAR PHASE
2. PLATELET PHASE
3. COAGULATION PHASE
4. FIBRINOLYTIC PHASE

VASCULAR PHASEVASCULAR PHASE
WHEN A BLOOD VESSEL IS WHEN A BLOOD VESSEL IS DAMAGED, VASOCONSTRICTION DAMAGED, VASOCONSTRICTION
RESULTS.RESULTS.

Vascular wallVascular wall ( Endothelium) ( Endothelium)
AntithromboticAntithrombotic propertiesproperties
– Antiplatelet effectsAntiplatelet effects
– Anticoagulant propertiesAnticoagulant properties
– Fibrinolytic propertiesFibrinolytic properties
ProthromboticProthrombotic properties properties
– Von Willebrand factorVon Willebrand factor
– Tissue factorTissue factor
– Fibrinolysis inhibitorsFibrinolysis inhibitors

HEMOSTASIS
1. VASCULAR PHASE
2. PLATELET PHASE
3. COAGULATION PHASE
4. FIBRINOLYTIC PHASE

PLATELET PHASEPLATELET PHASE

PLATELET PHASEPLATELET PHASE


Glanzmann’s

From Henry’s Clinical Diagnosis and Management by Laboratory Methods, McPherson and Pincus, eds, Saunders Elsevier, 2006.
Platelet Activation MechanismsPlatelet Activation Mechanisms

Platelet PlugPlatelet Plug Initial hemostatic response at the site of injuryInitial hemostatic response at the site of injury
Adhesion – deposition of platelets on the subendothelial Adhesion – deposition of platelets on the subendothelial matrix with vWf. (GP Ib)matrix with vWf. (GP Ib)
Aggregation – platelet-platelet cohesion with GP IIb/IIIa Aggregation – platelet-platelet cohesion with GP IIb/IIIa (ADP mediated, calcium facilitated)(ADP mediated, calcium facilitated)
Secretion – release of granule proteinsSecretion – release of granule proteins
Procoagulant – enhancement of thrombin generationProcoagulant – enhancement of thrombin generation
PLATELETS ADHERE TO THE DAMAGED SURFACE AND FORM PLATELETS ADHERE TO THE DAMAGED SURFACE AND FORM A TEMPORARY PLUG.A TEMPORARY PLUG.

HEMOSTASIS
1.VASCULAR PHASE
2.PLATELET PHASE
3.COAGULATION PHASE
4. FIBRINOLYTIC PHASE

COAGULATION PHASECOAGULATION PHASE
THROUGH TWO SEPARATE PATHWAYS THROUGH TWO SEPARATE PATHWAYS THE CONVERSION OF FIBRINOGEN TO THE CONVERSION OF FIBRINOGEN TO
FIBRIN IS COMPLETE.FIBRIN IS COMPLETE.

THE CLOTTING MECHANISMINTRINSIC EXTRINSIC
PROTHROMBIN THROMBIN
FIBRINOGEN
FIBRIN(II) (III)
(I)V
X
Tissue Thromboplastin
Collagen
VII
XII
XI
IXVIII

Coagulation cascadeCoagulation cascade
Vitamin K dependant factorsVitamin K dependant factors
XIIaXIIa
IIa
Intrinsic system Intrinsic system (surface contact)(surface contact)
XIIXII
XIXI XIa
Tissue factorTissue factor
IXIX IXa VIIa VIIVII
VIIIVIII VIIIaVIIIa
Extrinsic system Extrinsic system (tissue damage)(tissue damage)
XX
VV VaVa
IIII
FibrinogenFibrinogen FibrinFibrin
(Thrombin)(Thrombin)IIa
Xa

Factors produced in the Factors produced in the liverliver
Prothrombin Factor XIProthrombin Factor XI Factor V Factor XIIFactor V Factor XII Factor VII PrekallikreinFactor VII Prekallikrein Factor IX HMWKFactor IX HMWK Factor X Factor XIIIFactor X Factor XIII Fibrinogen Protein CFibrinogen Protein C AT IIIAT III

HEMOSTASIS
1.VASCULAR PHASE
2.PLATELET PHASE
3.COAGULATION PHASE
4. FIBRINOLYTIC PHASE

FIBRINOLYTIC PHASEFIBRINOLYTIC PHASE
ANTICLOTTING MECHANISMS ARE ANTICLOTTING MECHANISMS ARE ACTIVATED TO ALLOW CLOT ACTIVATED TO ALLOW CLOT
DISINTEGRATION AND REPAIR OF DISINTEGRATION AND REPAIR OF THE DAMAGED VESSEL.THE DAMAGED VESSEL.

Approach to a bleeding Approach to a bleeding disorderdisorder
HistoryHistory– Very importantVery important– Duration of Duration of
symptomssymptoms– When do they occurWhen do they occur– Prior trauma/surgeryPrior trauma/surgery– Other medical Other medical
conditionsconditions– Family historyFamily history
Medication usageMedication usage
ExaminationExamination– PetechiaePetechiae– EcchymosisEcchymosis
LabsLabs– CBC with smearCBC with smear– PTPT– PTTPTT– Thrombin timeThrombin time– FibrinogenFibrinogen– Platelet function Platelet function
assayassay

REVIEW PATIENT’S MEDSREVIEW PATIENT’S MEDS
FIVE DRUGSFIVE DRUGS THAT INTERFERE WITH THAT INTERFERE WITH HEMOSTASISHEMOSTASIS
ASPIRINASPIRIN ANTICOAGULANTSANTICOAGULANTS ANTIBIOTICSANTIBIOTICS ALCOHOLALCOHOL ANTICANCERANTICANCER

Diagnosis of Bleeding Diagnosis of Bleeding DisorderDisorder
HistoryHistory Neonatal bleedingNeonatal bleeding Bleeding after circumscisionBleeding after circumscision Delayed bleeding from umbilical stump (factor XIII)Delayed bleeding from umbilical stump (factor XIII) Deep hamatoma after IM injectionsDeep hamatoma after IM injections Epistaxis Epistaxis Dental extraction, tonsils, adenoidsDental extraction, tonsils, adenoids Site of bleeding: skin, mucous membranes, jointsSite of bleeding: skin, mucous membranes, joints Family history of bleeding disordersFamily history of bleeding disorders Drug exposureDrug exposure The presence of conditions causing bleeding: SLE, The presence of conditions causing bleeding: SLE,
nephrosis, hypothyroidism, Ehler Danlosnephrosis, hypothyroidism, Ehler Danlos


Primary Vs Secondary Defect: Primary Vs Secondary Defect: Clinical Manifestations Clinical Manifestations

Normal Peripheral SmearNormal Peripheral Smear

From Henry’s Clinical Diagnosis and Management by Laboratory Methods, McPherson and Pincus, eds, Saunders Elsevier, 2006.
Platelet lumi-Platelet lumi-aggregation: aggregation: Examples of Examples of
Normal and of Normal and of Glanzmann Glanzmann
ThrombasthenThrombastheniaia

Overview of Common Coagulation Overview of Common Coagulation TestsTests
From Henry’s Clinical Diagnosis and Management by Laboratory Methods, McPherson and Pincus, eds, Saunders Elsevier, 2006.

PetechiaePetechiae
Do not blanch with Do not blanch with pressure, Not pressure, Not
palpablepalpable


ORAL MANIFESTATIONSORAL MANIFESTATIONS
Petechiae & Ecchymosis Petechiae & Ecchymosis
Gingival Hyperplasia Gingival Hyperplasia
Spontaneous Gingival BleedingSpontaneous Gingival Bleeding
Ulceration of Oral MucosaUlceration of Oral Mucosa
LymphadenopathyLymphadenopathy


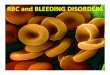
Copyright ©2008 American Society of Hematology. Copyright restrictions may apply.
Maslak, P. ASH Image Bank 2008;2008:8-00089
Figure 1. This picture demonstrates petechiae in dependent areas of a thrombocytopenic patient with AML

LABORATORY EVALUATIONLABORATORY EVALUATION
PLATELET COUNTPLATELET COUNT
PROTHROMBIN TIME (PT)PROTHROMBIN TIME (PT)
PARTIAL THROMBOPLASTIN TIME (PTT)PARTIAL THROMBOPLASTIN TIME (PTT)
THROMBIN TIME (TT)THROMBIN TIME (TT)
FIBRINOGENFIBRINOGEN


Copyright ©2004 American Society of Hematology. Copyright restrictions may apply.
Maslak, P. ASH Image Bank 2004;2004:101214
Figure 1. Review of the peripheral smear reveals a paucity of platelets

THROMBIN TIME
Time for Thrombin To Convert
Fibrinogen Fibrin A Measure of Fibrinolytic Pathway
NORMAL VALUENORMAL VALUE
9-13 SECS9-13 SECS

Initial Evaluation of a Bleeding Patient - 1Initial Evaluation of a Bleeding Patient - 1
Normal PTNormal PTT
Consider evaluating for: Mild factor deficiency Monoclonal gammopathy Abnormal fibrinolysis Platelet disorder (2 anti-plasmin def) Vascular disorder Elevated FDPs
Ureasolubility
Normal
Abnormal
Factor XIIIdeficiency

Normal PTAbnormal PTT
Test for factor deficiency: Isolated deficiency in intrinsic pathway (factors VIII, IX, XI) Multiple factor deficiencies (rare)
Repeatwith
50:50mix
50:50 mix is normal
50:50 mix is abnormal
Test for inhibitor activity: Specific factors: VIII,IX, XI Non-specific (anti-phospholipid Ab)

Initial Evaluation of a Bleeding Patient - 3Initial Evaluation of a Bleeding Patient - 3
Abnormal PTNormal PTT
Test for factor deficiency: Isolated deficiency of factor VII (rare) Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)
Repeatwith
50:50mix
50:50 mix is normal
50:50 mix is abnormal
Test for inhibitor activity: Specific: Factor VII (rare) Non-specific: Anti-phospholipid (rare)

Initial Evaluation of a Bleeding Patient - 4Initial Evaluation of a Bleeding Patient - 4
Abnormal PTAbnormal PTT
Test for factor deficiency: Isolated deficiency in common pathway: Factors V, X, Prothrombin, Fibrinogen Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)
Repeatwith
50:50mix
50:50 mix is normal
50:50 mix is abnormal
Test for inhibitor activity: Specific : Factors V, X, Prothrombin,
fibrinogen (rare) Non-specific: anti-phospholipid (common)

Coagulation factor deficienciesCoagulation factor deficienciesSummarySummary
Sex-linked recessiveSex-linked recessive Factors VIII and IX deficiencies cause bleedingFactors VIII and IX deficiencies cause bleeding
Prolonged Prolonged PTT; PTT; PT normalPT normal
Autosomal recessive Autosomal recessive (rare)(rare) Factors II, V, VII, X, XI, fibrinogen deficiencies cause bleedingFactors II, V, VII, X, XI, fibrinogen deficiencies cause bleeding
Prolonged Prolonged PTPT and/or and/or PTTPTT
Factor XIII deficiency is associated with bleeding andFactor XIII deficiency is associated with bleeding andimpaired wound healingimpaired wound healing
PT/ PTT normal; PT/ PTT normal; clot solubilityclot solubility abnormal abnormal
Factor XII, prekallikrein, HMWK deficienciesFactor XII, prekallikrein, HMWK deficienciesdo not cause bleedingdo not cause bleeding

Bleeding disorders
Vascular abnormalities
Platelet disordersClotting factorabnormalities
DIC
PathologyPathology

Vascular abnormalitiesVascular abnormalities CausesCauses
– InfectionsInfections Meningococcemia, Rickettsioses , Infective endocarditisMeningococcemia, Rickettsioses , Infective endocarditis
– Drug reactionsDrug reactions
– Hereditary hemorrhagic telangiectasiaHereditary hemorrhagic telangiectasia Autosomal dominant Autosomal dominant
– Cushing syndromeCushing syndrome
– Henoch - Schönlein PurpuraHenoch - Schönlein Purpura systemic hypersensitivity disease of unknown cause systemic hypersensitivity disease of unknown cause polyarthralgia, and acute Glomerulonephritis polyarthralgia, and acute Glomerulonephritis Palpable purpuric rash, colicky abdominal pain Palpable purpuric rash, colicky abdominal pain
– Scurvy and the Ehlers-Danlos syndromeScurvy and the Ehlers-Danlos syndrome
– Amyloid infiltration of blood vessels Amyloid infiltration of blood vessels

Bleeding disorders
Vascular abnormalities
***Platelet disorders
Clotting factorabnormalities
DIC

Bleeding disorders
Platelet disorders
↓production ↑destruction
SequestrationHypersplenism
Primary/IdiopathicITP
Acute/Chronic
SecondaryDrugs, HIV

Immune Thrombocytopenic Immune Thrombocytopenic Purpura (ITP)Purpura (ITP)
CauseCause– Antiplatelet antibodies Antiplatelet antibodies – Antigen - platelet membrane glycoprotein complexes IIb-IIIa Antigen - platelet membrane glycoprotein complexes IIb-IIIa
and Ib-IXand Ib-IX MorphologyMorphology
– Peripheral BloodPeripheral Blood thrombocytopenia, abnormally large platelets (megathrombocytes thrombocytopenia, abnormally large platelets (megathrombocytes
or Giant platelets),or Giant platelets),– MarrowMarrow
Normal or Increased magakaryocyte #Normal or Increased magakaryocyte # Diagnosis - by exclusion, normal PT and PTTDiagnosis - by exclusion, normal PT and PTT

DiagnosisDiagnosis
Exclude other causesExclude other causes Evaluate for other syndromesEvaluate for other syndromes
– SLESLE– APSAPS– LymphomasLymphomas– HIVHIV
Look at peripheral blood smearLook at peripheral blood smear– Pseudothrombocytopenia, hemolysis, Pseudothrombocytopenia, hemolysis,
large plateletslarge platelets

ITPITP
FeatureFeature AcuteAcute ChronicChronicAge / SexAge / Sex ChildrenChildren Adult/FemaleAdult/Female
OnsetOnset AbruptAbrupt GradualGradual
Predisposing Predisposing FactorsFactors
Viral infection/ Viral infection/ vaccinevaccine
--
DurationDuration <2 months<2 months >6mnoths>6mnoths
PathogenesisPathogenesis -- IgG against IgG against Platelet GPPlatelet GP
Peripheral Peripheral smearsmear
ThrombocytopenThrombocytopenia & Giant PLTSia & Giant PLTS
SameSame
Bone marrowBone marrow Normal or Normal or ↑Megakaryocyte↑Megakaryocytess
SameSame

ITPITP
FeatureFeature AcuteAcute ChronicChronicTestsTests Normal PT & Normal PT &
PTTPTTSameSame
Complication Complication (most (most dangerous)dangerous)
Intracranial Intracranial bleedbleed
SameSame
Clinical courseClinical course Spontaneous Spontaneous remissionremission
NoNo
TreatmentTreatment PLT. PLT. Transfusion/treatTransfusion/treat SplenectomySplenectomy
If <20,000If <20,000
NoNoIf <50,000If <50,000
Yes (refractory Yes (refractory cases)cases)

TreatmentTreatment
No need to treat if platelet count No need to treat if platelet count above 20-30k. above 20-30k.
Initial therapyInitial therapy– Prednisone 1 mg/kg divided bidPrednisone 1 mg/kg divided bid– Decadron 40 mg daily x 4 daysDecadron 40 mg daily x 4 days– High dose solumedrol High dose solumedrol
May increase platelet count fasterMay increase platelet count faster More side effectsMore side effects
– IVIG for serious presentationIVIG for serious presentation

TreatmentTreatment 50% relapse after initial therapy or remain steroid 50% relapse after initial therapy or remain steroid
dependentdependent Splenectomy especially for steroid responsive casesSplenectomy especially for steroid responsive cases
– 80% response rate80% response rate– Immunize priorImmunize prior
Anti-D immune globulin in Rh+ patientsAnti-D immune globulin in Rh+ patients RituxanRituxan DanazolDanazol DapsoneDapsone VincristineVincristine Immunosuppression with azathioprine, cytoxanImmunosuppression with azathioprine, cytoxan Thrombopoietan receptor agonists – Nplate and PromactaThrombopoietan receptor agonists – Nplate and Promacta
– ?rebound worsening when drugs stopped?rebound worsening when drugs stopped– Myelofibrosis Myelofibrosis

Drug induced thrombocytopeniaDrug induced thrombocytopeniaHeparin induced thrombocytopenia Heparin induced thrombocytopenia
(HIT)(HIT)
Seen inSeen in 3-5% of patients treated with3-5% of patients treated with unfractionatedunfractionated heparinheparin
thrombocytopenic after 1-2 weeks of Rxthrombocytopenic after 1-2 weeks of Rx Caused byCaused by IgG antibodies against IgG antibodies against platelet factor platelet factor
4/heparin complexes4/heparin complexes on platelet surfaces on platelet surfaces ExacerbatesExacerbates thrombosisthrombosis, both arterial and venous (in , both arterial and venous (in
setting of severe thrombocytopenia) setting of severe thrombocytopenia) – Antibody binding results in platelet activation and Antibody binding results in platelet activation and
aggregation.aggregation. Rx -Rx - cessation of heparincessation of heparin
Other drugs???

Thrombotic MicroangiopathiesThrombotic Microangiopathies
1.1. Thrombotic thrombocytopenic Purpura Thrombotic thrombocytopenic Purpura (TTP)(TTP) 2.2. Hemolytic-Uremic syndrome Hemolytic-Uremic syndrome (HUS)(HUS)

Thrombotic Thrombotic MicroangiopathiesMicroangiopathies
common for both disorderscommon for both disorders
Mechanism =Mechanism =***hyaline (platelets) thrombi in the ***hyaline (platelets) thrombi in the microcirculationmicrocirculation
Pathogenesis = Pathogenesis = Systemic endothelial cell damage Systemic endothelial cell damage Clinically =Clinically = Fever, Thrombocytopenia, Renal failure, Fever, Thrombocytopenia, Renal failure,
Hemolytic anemia, neurological symptomsHemolytic anemia, neurological symptoms
***How to differentiate them from DIC?

HEMOLYSIS/HEMOLYTIC ANEMIAS HEMOLYSIS/HEMOLYTIC ANEMIAS DUE TO RBC TRAUMADUE TO RBC TRAUMA
Mechanical heart valves Mechanical heart valves breaking RBC’sbreaking RBC’s
MICROANGIOPATHIES:MICROANGIOPATHIES:– TTPTTP– Hemolytic Uremic Hemolytic Uremic
SyndromeSyndrome

Schistocytes: Microangiopathic Schistocytes: Microangiopathic Hemolytic AnemiaHemolytic Anemia

Thrombotic Thrombotic MicroangiopathiesMicroangiopathies
HUS TTP
Absent Absent Neurological Neurological symptomssymptoms
Prominent Prominent
Prominent Prominent Acute Renal FailureAcute Renal Failure Less prominentLess prominent
Children Children Age Age Adults Adults
InfectionInfection
( E.coli O157 : H7)( E.coli O157 : H7)
CauseCause GeneticGenetic
(vWF (vWF metalloprotease- metalloprotease-
ADAMTS 13ADAMTS 13) ) deficiencydeficiency
SupportiveSupportive Rx.Rx. Plasma ExchangePlasma Exchange
Good in children Good in children
Bad in adultsBad in adults
Prognosis Prognosis Better with plasma Better with plasma exchangeexchange
Feature

Mannucci PM. Pathophysiol Haemost Thromb. 2006;35(1-2):89-97. Thrombotic thromboytopenic purpura: another example of immunomediated thrombosis.
In the absence of ADAMTS13 (or when the concentrations of ADAMTS13 are not sufficient to cleave the increased quantity of UL VWF multimers released by the activated endothelial cells), UL VWF aggregates the platelets within the vessels causing thrombi that block blood flow. The red cells passing through the thrombi become fragmented and form schistocytes.
Mechanisms of thrombocytopenia and anemia in TTP: Comparison with the normal physiological state

Platelet functional Platelet functional disordersdisorders

Copyright ©2009 American Society of Hematology. Copyright restrictions may apply.
Maslak, P. et al. ASH Image Bank 2009;2009:9-00008
Figure 1. Lumiaggregometry tracing demonstrates simultaneous platelet aggregation (red and blue curves) and ATP release (green and black curves) in response to collagen used as
an agonist

Bleeding disorders
Vascular abnormalities
Platelet disordersClotting factorabnormalities
DIC

Clotting factor Clotting factor abnormalitiesabnormalities
Congenital disordersCongenital disorders– Von Willebrand disease –MC with minimal bleedingVon Willebrand disease –MC with minimal bleeding
– Factor VIII Deficiency - Hemophilia A or Classic TypeFactor VIII Deficiency - Hemophilia A or Classic Type
– Factor IX Deficiency – Hemophilia BFactor IX Deficiency – Hemophilia B
Acquired disordersAcquired disorders– Vit. K deficiency =Due to deficient carboxylation of factors II, Vit. K deficiency =Due to deficient carboxylation of factors II,
VII, IX &XVII, IX &X
– Oral anti-coagulantsOral anti-coagulants Coumarin derivatives= warfarin – inhibit Vit. K factors Coumarin derivatives= warfarin – inhibit Vit. K factors Liver diseases Liver diseases ↓↓ synthesis of factors synthesis of factors

Von Willebrand DiseaseVon Willebrand Disease
MCMC inherited bleeding disorder with mild bleeding inherited bleeding disorder with mild bleeding Autosomal dominantAutosomal dominant TYPE I =Most commonTYPE I =Most common (70% of all cases) (70% of all cases) Prolonged Prolonged bleeding time but bleeding time but normal platelet countnormal platelet count ↓↓Plasma Plasma vWF vWF levelslevels Secondary Secondary ↓↓ in Factor in Factor VIII VIII levelslevels

von Willebrand Diseasevon Willebrand DiseaseClinical featuresClinical features
von Willebrand factorvon Willebrand factor Carrier of factor VIII Carrier of factor VIII anchors platelets to subendotheliumanchors platelets to subendothelium Bridge Bridge between plateletsbetween platelets
InheritanceInheritance Autosomal dominantAutosomal dominant
Incidence Incidence 1/10,0001/10,000
Clinical featuresClinical features Mucocutaneous bleedingMucocutaneous bleeding

Effect of blood group on Effect of blood group on plasma vWF levelplasma vWF level
Blood groupBlood group Plasma vWF Plasma vWF level level U/dIU/dI
OO 7575
AA 106106
BB 117117
ABAB 123123



Treatment of von Willebrand Treatment of von Willebrand diseasedisease
Varies by ClassificationVaries by Classification CryoprecipitateCryoprecipitate– Source of fibrinogen, factor VIII and VWFSource of fibrinogen, factor VIII and VWF– Only plasma fraction that consistently contains VWF Only plasma fraction that consistently contains VWF
multimersmultimers– Correction of bleeding time is variableCorrection of bleeding time is variable
DDAVP (Deamino-8-arginine vasopressin)DDAVP (Deamino-8-arginine vasopressin)– Increases plasma VWF levels by stimulating secretion from Increases plasma VWF levels by stimulating secretion from
endotheliumendothelium– Duration of response is variableDuration of response is variable– Used for type 1 diseaseUsed for type 1 disease– Dosage 0.3 µg/kg q 12 hr IVDosage 0.3 µg/kg q 12 hr IV
Factor VIII concentrate (Humate-P)Factor VIII concentrate (Humate-P)– Virally inactivated productVirally inactivated product– Used for type 2 and 3Used for type 2 and 3

******Hemophilia AHemophilia A MC MC hereditaryhereditary disease disease with serious bleedingwith serious bleeding
– X-linked recessiveX-linked recessive– In 30%In 30% No family historyNo family history (new mutations) (new mutations)– 15% of severe cases develop 15% of severe cases develop factor VIII inhibitorsfactor VIII inhibitors
↓↓ amount or activity of factor VIIIamount or activity of factor VIII
factor VIII = cofactor for activation of factor X in the coagulation factor VIII = cofactor for activation of factor X in the coagulation cascadecascade
Symptoms usually develop in Symptoms usually develop in severesevere cases (factor VIII cases (factor VIII <1% of <1% of normalnormal) – ) – hemoarthrosis, hemoarthrosis, bruising, hemorrhage after trauma or bruising, hemorrhage after trauma or surgerysurgery

Hemophilia BHemophilia B
Factor IX deficiencyFactor IX deficiency
X-linked recessiveX-linked recessive
Much less commonMuch less common
Clinically= Clinically= indistinguishableindistinguishable from Hemophilia A with from Hemophilia A with Similar Similar lab findingslab findings
Diagnosis by factor IX levelsDiagnosis by factor IX levels
Treat with recombinant IX Treat with recombinant IX

HemophiliaHemophilia
X-linked disorderX-linked disorder Factor VIII or IX Factor VIII or IX Females carriersFemales carriers
– SymptomsSymptoms New mutationNew mutation
– 30%30%– VIII gene hugeVIII gene huge
Infectious risksInfectious risks HemarthropathyHemarthropathy
MildMild ModerateModerate SevereSevere
Factor Factor levellevel
>5%>5% 1-5%1-5% <1%<1%
BleedingBleeding RareRare 3-4x/year3-4x/year MultipleMultiple
TreatmeTreatmentnt
SupportiveSupportive SupportiveSupportive prophylaxiprophylaxiss

Acquired HemophiliaAcquired Hemophilia
Occurs in malignancy, autoimmune Occurs in malignancy, autoimmune disorders, post-partumdisorders, post-partum
PTT prolongedPTT prolonged Mixing studies – immediate and delayedMixing studies – immediate and delayed Bethesda assay – measurement of Bethesda assay – measurement of
strength of the inhibitorstrength of the inhibitor Treatment is with alternative factor Treatment is with alternative factor
concentratesconcentrates Immunosuppression to clear inhibitorImmunosuppression to clear inhibitor

Fresh Frozen PlasmaFresh Frozen Plasma
Advantages:Advantages:• Availability.Availability.
Disadvantages:Disadvantages:• Volume problemsVolume problems• Infectious exosure: hep. C, HIV, hep. BInfectious exosure: hep. C, HIV, hep. B• Clotting activity by freezing and thawing (-15%)Clotting activity by freezing and thawing (-15%)
IndicationsIndications::• Deficiency of factors V, VII, IX, X and XIIIDeficiency of factors V, VII, IX, X and XIII• Multiple deficiencies: servere liver disease and DIC.Multiple deficiencies: servere liver disease and DIC.• Unknown cause.Unknown cause.

CryoprecipitateCryoprecipitate
Prepared form single units of donor plasma.Prepared form single units of donor plasma.
Contains 50% of VIII C, vW activity, fibrinogen, XIII.Contains 50% of VIII C, vW activity, fibrinogen, XIII.
= 100 units of factors vIII C.= 100 units of factors vIII C.
Main uses:Main uses: Treatment of choice of VW disease except type 1.Treatment of choice of VW disease except type 1. Hemophilia A, Hypo & dysfibrinogenemia.Hemophilia A, Hypo & dysfibrinogenemia.
Disadvantages:Disadvantages: Should be kept at deep freeze (-20 to -30 C).Should be kept at deep freeze (-20 to -30 C). Difficult to handle at home.Difficult to handle at home. Cryoprecipitate vary in factor VIII C content from bag to bag.Cryoprecipitate vary in factor VIII C content from bag to bag.
Dosages: similar to factor VIIIDosages: similar to factor VIII
1 bag 100 units1 bag 100 units

Commercially Prepared Factor Commercially Prepared Factor VIII ConcentratesVIII Concentrates
Advantages:Advantages: Easy storage, reconstitution and Easy storage, reconstitution and
infusion.infusion. Each bottle contains a fixed amount Each bottle contains a fixed amount
of factor VIII.of factor VIII. No volume problem.No volume problem.Disadvantages:Disadvantages: Infectious exposure HIV.Infectious exposure HIV. Hep C. Hep B and others.Hep C. Hep B and others.

Prothrombin complex Prothrombin complex concentratesconcentrates
Contains: vit. K dependent factors + protein C.Contains: vit. K dependent factors + protein C.Activated factors: hemophilia A & B.Activated factors: hemophilia A & B.Uses:Uses: Hemophilia B.Hemophilia B. Hemophilia A with inhibitors.Hemophilia A with inhibitors.Advantages:Advantages: Easy to store (-4C) and to administer.Easy to store (-4C) and to administer.Main problems:Main problems: Infection risk.Infection risk. DIC and thromboembolic phenomena.DIC and thromboembolic phenomena. Thromboembolic phenomena, this risk increase in:Thromboembolic phenomena, this risk increase in:
– Injury & high tissue thrompoblastin activity.Injury & high tissue thrompoblastin activity.– Liver disease because of low levels of antithrombin III.Liver disease because of low levels of antithrombin III.– Neonates.Neonates.

Recombinant concentratesRecombinant concentrates
Factors VII, VIII, IXFactors VII, VIII, IX
Effective in clinical trialsEffective in clinical trials
AdvantagesAdvantages No infectious risk.No infectious risk. No volume problems.No volume problems.

Bleeding disorders
Vascular abnormalities
Platelet disordersClotting factorabnormalities
DIC

Disseminated Intravascular CoagulationDisseminated Intravascular Coagulation
Characterized byCharacterized by = =activation of the coagulationactivation of the coagulation sequence sequence systemic micro- systemic micro- thrombi thrombi
SequelaeSequelae= = tissue hypoxiatissue hypoxia due to due to microinfarcts (Thrombotic) or bleedingmicroinfarcts (Thrombotic) or bleeding problemsproblems
Triggering PathwaysTriggering Pathways – Release of tissue factor / thromboplastic factors into circulation Release of tissue factor / thromboplastic factors into circulation – Widespread endothelial injuryWidespread endothelial injury
Mechanism=Activated monocytesMechanism=Activated monocytes release IL-1 and TNF release IL-1 and TNF αα ↑↑ expression of expression of tissue Thromboplastic factor on endothelial cells & decrease Thrombomodulintissue Thromboplastic factor on endothelial cells & decrease Thrombomodulin– Mechanism = Consumption Mechanism = Consumption of coagulation factors , platelets, and activation of coagulation factors , platelets, and activation
of fibrinolytic pathwaysof fibrinolytic pathways

Disseminated Intravascular CoagulationDisseminated Intravascular Coagulationcontd…contd…
Sources of thromboplastic substancesSources of thromboplastic substances::– Leukemic Leukemic cell granulescell granules– Placenta in Placenta in obstetric obstetric complicationscomplications– CarcinomasCarcinomas- (Mucin - secreting adenocarcinomas)- (Mucin - secreting adenocarcinomas)– Bacterial Bacterial endo and exotoxinsendo and exotoxins
Endothelial injury can also be Caused byEndothelial injury can also be Caused by– Antigen-antibodyAntigen-antibody complexes =S.L.E. complexes =S.L.E.– TemperatureTemperature extremes= Heat stroke or burns extremes= Heat stroke or burns– Microorganisms=Microorganisms=Rickettsae, meningococciRickettsae, meningococci

Disseminated Intravascular Disseminated Intravascular CoagulationCoagulation
contd…contd…
Plasmin Plasmin Fibrinolysis Fibrinolysis formation of fibrin degradation products formation of fibrin degradation products ((FDP)FDP)– D-Dimer most important of FDPsD-Dimer most important of FDPs
Organ damage due to Micro thrombiOrgan damage due to Micro thrombi – Kidney =Kidney =microinfarcts in the renal cortexmicroinfarcts in the renal cortex
In severe cases = In severe cases = bilateral renal cortical necrosisbilateral renal cortical necrosis– Adrenals Adrenals = bilateral adrenal hemorrhage= bilateral adrenal hemorrhage
resembles resembles waterhouse - Friderichsen syndromewaterhouse - Friderichsen syndrome– Brain= MicroinfarctsBrain= Microinfarcts surrounded by foci of hemorrhage surrounded by foci of hemorrhage– Heart and anterior pituitary= Heart and anterior pituitary= show Similar changesshow Similar changes

Disseminated Intravascular Disseminated Intravascular CoagulationCoagulation
contd…contd…
Clinically= Clinically= Bleeding tendency in presence of widespread Bleeding tendency in presence of widespread coagulationcoagulation– Acute Acute D.I.C.= dominated by a D.I.C.= dominated by a bleedingbleeding
seen in obstetrical complications and trauma seen in obstetrical complications and trauma – Chronic Chronic D.I.C.= presents with D.I.C.= presents with Thrombotic Thrombotic complicationscomplications
seen in cancersseen in cancers Manifestations =Manifestations = variable variable
– Minimal to profound shock, renal failure, dyspnea, cyanosis, Minimal to profound shock, renal failure, dyspnea, cyanosis, convulsions, and comaconvulsions, and coma
– Hypotension isHypotension is characteristic. characteristic.

Disseminated Intravascular CoagulationDisseminated Intravascular Coagulationcontd…contd…
Lab = Lab = PT And PTT Are typically prolonged.PT And PTT Are typically prolonged.– ThrombocytopeniaThrombocytopenia– low Fibrinogenlow Fibrinogen– Elevated plasma Fibrin split products Elevated plasma Fibrin split products
PrognosisPrognosis = = Highly variableHighly variable– Depends upon:Depends upon:
Underlying disorderUnderlying disorder Degree of intravascular clottingDegree of intravascular clotting Activity of mononuclear phagocytic systemActivity of mononuclear phagocytic system Amount of FibrinolysisAmount of Fibrinolysis
Treatment of the underlying disorder is most important!!Treatment of the underlying disorder is most important!!
How to differentiate DIC form HUS/TTP using lab parameters?


ALL CLL

Antithrombin III concentrateAntithrombin III concentrate
Neutralizes mainly thrombin.Neutralizes mainly thrombin. Inhibits activated factor xa.Inhibits activated factor xa.Also factor IXa, XIa, XIIa.Also factor IXa, XIa, XIIa. Uses:Uses:
1.1. Congenital deficiency states acute Congenital deficiency states acute thrombosis.thrombosis.
2.2. Congenital deficiency states before Congenital deficiency states before surgery.surgery.
3.3. Acquired deficiency states thrombosis Acquired deficiency states thrombosis or DIC.or DIC.

Antifibrinolytic therapyAntifibrinolytic therapy
Effective in controlling mucosal bleeding Effective in controlling mucosal bleeding especially the oral mucosa (prevent rebleeds)especially the oral mucosa (prevent rebleeds)
Not well studied for: nasal, urinary and GIT Not well studied for: nasal, urinary and GIT bleedingbleeding
EACA (Amicar) 500 mg tab, 250/mL elixirEACA (Amicar) 500 mg tab, 250/mL elixir Dose 100-200 mg/Kg (maximum 10 g initial)Dose 100-200 mg/Kg (maximum 10 g initial)
50-100 mg/kg/dose (max 5 g) every 6 hours50-100 mg/kg/dose (max 5 g) every 6 hours
Transexamic acid (cyclockapron) 500mg cap.Transexamic acid (cyclockapron) 500mg cap. 25 mg/kg/dose every 6 hours25 mg/kg/dose every 6 hours
tranexamic acid effective locally as mouth washtranexamic acid effective locally as mouth wash