Embed Size (px)
Citation preview

Blunt Abdominal Trauma and Interventional Radiology
Ri 高祥豐April 12, 2004

Outline of Presentation
Introduction of therapeutic embolization Embolization in different organ injury
Spleen, Liver, Kidney, Pelvis Indication or patient selection Outcome, survival rate Complication Current Protocol

Introduction Therapeutic Embolization

Spontaneous hemostasis
Vasoconstriction Formation of a clot Scar formation Vessel recanalization
Eur Radiol 2002;12:979-993

Principles of hemostatic embolization
Treatment should be derived from the physiological process of hemostasis
Resorbable material may be sufficient to initiate local thrombus
It should take place at the site of injury Minimal tissue loss Rebleeding should be avoided by formation of a
stable clot
Eur Radiol 2002;12:979-993

Agents for embolizations
Gelfoam Soaked in an antibiotic solution resorable Can be cut in variable size May result in too distal embolization Risks for tissue infarction or late abscess formation
Coils Have variable size, length, diameter Precise targeted delivery Expensive Need normal coagulation
Metal stents Large-caliber patent artery
Eur Radiol 2002;12:979-993

Techniques for embolization
Simple
SandwichLarge vesselpseudoaneurysm

Spleen Injury
Indications, Outcomes, Complications, and Protocols

Spleen trauma -- Grading
The American Association for the Surgery of Trauma Organ Injury Severity Scale Spleen grading system Grade I - Small subcapsular hematoma, less than 10% of surfac
e area Grade II - Moderate subcapsular hematoma on 10-50% of surfac
e area; intraparenchymal hematoma less than 5-cm diameter; capsular laceration less than 1-cm deep
Grade III - Large or expanding subcapsular hematoma on greater than 50% of surface area; intraparenchymal hematoma greater than 5-cm diameter; capsular laceration 1- to 3-cm deep
Grade IV - Laceration greater than 3-cm deep; laceration involving segmental or hilar vessels producing major devascularization (>25%)
Grade V - Shattered spleen; hilar injury that devascularizes the spleen

Spleen trauma
Treatment of choicesLaparotomy and splenectomyNon-operative managementEmbolization

Spleen trauma
Patient Selection Surgery vs Non-operative management
J Trauma 2000;49:177–189. EAST study Successful nonoperative management was associated with: Higher blood pressure and hematocrit Less severe injury based on ISS, Glasgow Coma Scale, grade
of splenic injury, and quantity of hemoperitoneum
Surgery vs non-operative vs embolization Lack of evidence….
Extravasation in CT or angiography Vascular injury Hemodynamically stable?

Spleen trauma
Outcomes of embolization J Trauma 2004;56;542-47
Multicenter, retrospective, 140 patients Patient selection: positive CT findings Spleen salvage rate: 87%, decreased with increasing ISS score. Embolization by Coils or subselective coils had similar successful ra
te Prognostic factors
AV fisfula: poor prognosis Hemoperitoneum, extravasation, pseudoaneurysm: silimar Old age: not significant Intraperitoneal hemorrhage: not significant

Spleen trauma
Outcomes of embolization J Trauma 2001;51;1161-65
Level I trauma center, retrospective, 126 patients Patient selections: positive CT finding, stable 68% had negative angiographic finding.
Splenic salvage rate: 92% 32% had positive angiographic finding, then embolized
Splenic salvage rate: 92% Salvage rate in Gr. IV and V injury: ~70% Compared with EAST non-operative management group: b
etter salvage rate CT is a predictive tool

Spleen trauma
Complications of spleen traumaJ Trauma 2004;56;542-47
Complication rate: ~20% Bleeding: 11%, abscess: 3%
Gastric wall infarctionPancreatic infarctionSplenic artery dissection

Liver Injury
Indications, Outcomes, Complications, and Protocols

Liver trauma: grading by CT
J Trauma 2002;52:1091–1096

Liver trauma: grading by angio
J Trauma 2002;52:1091–1096

Liver trauma: Outcomes
Low CT grading, stable hemodynamics, non-operative management Common complications
AV fistula Bile leaks Abscess, intrahepatic or extrahepatic Hemobilia or bilhemia (vascular-biliary fistula)
Early intervention of these complications does work in 85% of patients with complications
Embolization, CT-guided drainage, ERCP…
J Trauma 1999; 46(4):619-22

Liver trauma: Outcomes
CT grading Gr. IV and V: advantages Embolization can decrease the amount of resuscitatio
n fluid to maintain vital sign. J Trauma 1998;45:353-359; J Trauma. 2002;52:1097–1101; J Trauma. 2003;55:1077–1082
Embolization can decrease shock index AJR 1997, 169, 1151-1156
Operation with adjunct embolization can decrease the mortality rate.(65% 30%, p=0.02) J Trauma 2003;54:647–654
Early embolization may decrease the mortality rate J Trauma. 2003;55:1077–1082, J Trauma. 2002;52:1097–1101

Liver trauma: pitfalls and morbidity
CT grading: Gr. IV and VCT scan grade 4 or 5 lesion and the fluid requ
irements of more than 2,000 mL/h to maintain normotension indicated the absolute necessity of surgery. J Trauma 2002;52:1091–1096.
Morbidity rate: 58% Hepatic abscess, hepatic necrosis, bile leaks
J Trauma. 2003;55:1077–1082

Liver trauma: protocol
J Trauma 2002;52:1091–1096

Liver trauma: protocol
J Trauma 2002;52:1091–1096

Kidney Injury
Indications, Outcomes, Complications, and Protocols

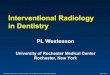
Kidney Trauma: grading by CT
J Trauma 2001;51:526-31

Kidney Trauma: grading by angio
Type A: variable degrees of avascularity and heterogeneity in the accumulation of contrast medium in the renal parenchyma or displacement of the renal arterial branches
Type B: disruption of renal artery branches Type C: extravasation of contrast medium from a renal ar
tery, or presence of an arteriovenous fistula Type D: complete occlusion of the main renal artery or inj
ury to a main renal vein.
J Trauma 2001;51:526-31

Kidney trauma: protocol
J Trauma 2001;51:526-31

Kidney trauma: protocol
J Trauma 2001;51:526-31

Pelvis Injury
Indications, Outcomes, Complications, and Protocols

Pelvic trauma
Pelvic trauma included: arterial, venous, or bones in origins
The instability of pelvic bone fractures is a good predictor of the need for hemostatic embolization
Pelvic fracture is responsible for 6-8% of death of all trauma patients
Rupture of a main pelvic artery carries a mortality of 50-75%
Eur Radiol 2002;12:979-993

Pelvic trauma: outcomes
In CGMH, retrospective100% to stop bleeding in patients with
unstable pelvic fracturesSurvival rate after successfully stopping
bleeding: 83%Predictors for mortality: rates for blood
transfusion The risk of dying increased by 62% for every 1
unit/h increase of transfusion rate.
J Trauma 2000; 49(1):71-5

Pelvic trauma: outcomes
In a center which places angiographic intervention in the first priority
100% to stop bleeding Survival rate: 87% Application of angiography may reduce the need for
surgery The predictors of death included
posterior pelvic arterial injury an elevated Acute Physiology and Chronic Health Evaluation II
score Need of fluids for resuscitation
J Trauma 2003;55(4):696-703

Pelvic trauma
Complications related to embolizationPelvic visceral necrosisFistulazation Ischemic neuropathy impotence
Eur Radiol 2002;12:979-993

Pelvic trauma
Indications for angiography
> 4 units transfused for pelvic bleeding in < 24hrs > 6 units transfused for pelvic bleeding in < 48hours Hemodynamic instability with a negative FAST or DPL Large pelvic hematoma on CT Pelvic pseudoaneurysm on helical CT
Large and/or expanded pelvic hematoma seen at the time of laparotomy
Trauma, Moore EE et al, 4th ed, P822

Pelvic trauma: protocols
For stable patients Evidence of solid visceral injury Large pelvic hematoma
For unstable patients FAST: if positive OP
Large hematoma + ongoing blood loss angio Negative FAST:
Able to stabilize angio Unable to stabilize DPL
Positive DPL OP Negative DPL angio
Trauma, Moore EE et al, 4th ed, P824-825

NTUH: indications for interventional radiology Hemodynamically unstable patients High risk for surgery Once performed, surgical intervention sho
uld be arranged later for debridement. Prophylactic antibiotics are optional.

Take Home Messages
Embolization is a promising way for stopping bleeding
Because of the lack of evidence, indications for therapeutic embolization are vague