Embed Size (px)
Citation preview

ww
w.s
om
at.org
.mx
Boletín
Año II. Vol. 2 No. 4 Julio-Agosto 2017 ISSN EN TRÁMITE
Sociedad Mexicana de Anestesiología en Trauma, A.C.
CONTENIDO
Editorial. Dra. María Elena Launizar García
Incidencia de recurrencia de los hematomas subdurales crónicos en el Hospital I .M.S.S. Traumatología “Dr. Victorio de la Fuente Narváez”. Dra. Alma Edith Gress Mendoza, Dr. Michael Herbas Rocha
Normas para los autores
Índice
PÁGINA
3
5
22
CONTENT PAGEEditorial 4
Incidence or recurrence of the chronic subdural hematomas at HospitalIMSS Traumatología “Dr. Victorio de la Fuente Narváez” 14
Guidelines for autor 24
CONSEJO DIRECTIVO 2016-2018PRESIDENTE
DR. JAIME VÁZQUEZ TORRES
VICEPRESIDENTEDR. JOSÉ F. FERNÁNDEZ LÓPEZ
SECRETARIODRA. MARÍA E. LAUNIZAR GARCÍA
SECRETARIO SUPLENTEDRA. LESLIAN J. MEJÍA GÓMEZ
TESORERODRA. ANA MA. DOMÍNGUEZ CRUZ
PROTESORERODR. MIGUEL Á. GARCÍA LARA
EDUCACIÓN MÉDICA CONTINUA (ENSEÑANZA E INVESTIGACIÓN)
COORDINADORDR. ALEJANDRO L. MARÍN GONZÁLEZ
COORDINADOR SUPLENTEDR. MOISÉS MANCINI GARCÍA
COMITÉS ESPECIALESADMISIÓN
DRA. PAULINA ESPITIA HUERTER'ODR. ARTURO ZARAGOZA GALVÁN
PTCDRA. MARÍA E. LAUNIZAR GARCÍA
DRA. ARIZBE RIVERA ORDÓÑEZDRA. MA. DE L. VALLEJO VILLALOBOS
DIFUSIÓNDR. JOSÉ A. AGUILAR RAMÓN
DR. ROSEMBERG ALBORES FIGUEROA DR. SALVADOR CASTILLO
DRA. YOLANDA M. MARTÍNEZ B.DR. MARIO MARTÍNEZ NAVA
DR. VICENTE MARTÍNEZ ROSETEDR. FILIBERTO MARTÍNEZ GONZÁLEZ
DR. JOSÉ L. MARTÍNEZ RODRÍGUEZ DRA. GLORIA MOLINA RODRÍGUEZ
DR. LUIS MOTTA AMÉZQUITADR. JORGE A. NAVA LÓPEZ
DRA. CLARA NÚÑEZ IÑÍGUEZ DR. LEANDRO GONZÁLEZ V.
HONOR Y JUSTICIADR. FERNANDO LEAL LEAL
DRA. MARÍA C. SERRATOS VÁZQUEZ
ÉTICADR. RUBÉN OMAR TAFOYA OLIVOS
CONSENSOS, GUÍAS, ALGORITMOSDR. JESÚS OJINO SOSA GARCÍA
ENLACES NACIONALES E INTERNACIONALES
ACAD. DR. JAIME RIVERA FLORESDR. JAIME VÁZQUEZ TORRES
PREHOSPITALARIODR. GERARDO J. ILLESCAS FERNÁNDEZ
SOCIOCULTURALDRA. MARÍA E. PINTO SEGURA
DRA. MARÍA ISABEL LUNA PALMILLA
PÁGINA WEB, REDES SOCIALESY BOLETÍN
ACAD. DR. JAIME RIVERA FLORES
CONSEJO CONSULTIVOACAD. DR. JAIME RIVERA FLORES
OMITÉ EDITORIAL
CEditor
Acad. Dr. Jaime Rivera Flores
Revisores Nacionales
Dr. José A. Aguilar Ramón Dr. Rosemberg Albores Figueroa Dr. Salvador Castillo Barón
Dra. Susana Cervantes Ceballos Dra. Marisela Correa Valdéz Dra. Ana Ma. Domínguez Cruz
Dra. Paulina Espitia Huerter’O Dr. José F. Fernández López Dr. Miguel Á. García Lara
Dr. Leandro González Villanueva Dra. Clara L. Gutiérrez Porras Dr. Saúl Hernández García
Dra. María E. Launizar García Dra. Leticia Leal Gudiño Dr. Moisés Mancini García
Dr. Alejandro L. Marín González Dra. Yolanda M. Martínez Barragán Dr. Filiberto Martínez González
Dr. José L. Martínez Rodríguez Dra. Leslián J. Mejía Gómez Dra. Gloria Molina Rodríguez
Dra. Minerva Moreno Ángeles Dra. Clara Núñez Íñiguez Dr. Joel Ortega Salas
Dra. Ana A. Peña Riverón
Dra. Arizbe Rivera Ordóñez Dra. María C. Serratos Vázquez Dr. Jesús O. Sosa García
Dr. Rubén O. Tafoya Olivos Dr. David Unzueta Navarro Dra. María M. Tun Martin
Dra. Emma G. Urías Romo de Vivar Dra. María de L. Vallejo Villalobos Dr. Jaime Vázquez Torres
Dr. José G. Velazco González Dra. Gabriel J. Vidaña Martínez Dr. Juan S. Vilchis Rentería
Revisores Internacionales
Dr. Becket Argüello (Nic.) Carlos Campos M.D. (USA) Dr. Samuel Galvagno (USA)
Dr. Aurelio Rodríguez (USA) Manuel Lorenzo MD (USA) María Fernanda Rojas (Col.)
Tanya Zackrison (USA)
Todos los trabajos publicados son originales y su propiedad literaria pertenece al bole�n.Los conceptos que aparecen en esta publicación son responsabilidad exclusiva de los autores.El contenido de la publicidad es responsabilidad de las empresas e ins�tuciones anunciantes.Se autoriza la reproducción parcial o total del contenido de la publicación, incluyendo el almacenamiento y redistribución por el mismo medio; siempre y cuando sea sin fines de lucro o para usos estrictamente académico, citando la fuente sin alteración del contenido y dando los créditos autorales.
Información Legal.Bole�n, Año 2, No. 4,Julio-Agosto 2017, es una publicación periódica electrónica, bimestral. Publicada y editada por la Sociedad Mexicana de Anestesiología en Trauma, A.C. (SOMAT), con domicilio en Fortunato Zuazua 48-106 Col. San Juan Tlihuaca. Del. Azcapotzalco C.P. 02400, Tel. 67983227, www.somat.org.mx, [email protected] responsable: Dr. Jaime Rivera FloresReserva de Derechos al Uso Exclusivo: 04-2017-110613014600-203, ISSN en trámite otorgado por el Ins�tuto Nacional de Derecho de Autor. Responsable de la úl�ma actualización de este Número, Unidad de Edición SOMAT, Dr. Jaime Rivera Flores calle Fortunato Zuazua 48-106 Col. San Juan Tlihuaca. Del Azcapotzalco C.P. 02400 Fecha de úl�ma modificación 12 de julio de 2019.
SOCIEDAD MEXICANA DE ANESTESIOLOGÍA EN TRAUMA, A.C.
DITORIALEl hematoma subdural crónico (CSDH) se caracteriza por sangre en el espacio subdural que evoca una reacción inflamatoria; es una forma Ecomún de hemorragia intracraneal con una tasa de recurrencia sustancial.
El HSC es común en la práctica neuroquirúrgica y frecuente en los ancianos; la tasa de recurrencia es entre el 2.3 y el 33%, en otros estudios tiene 1-2una incidencia de 58 / 100,000 personas al año en personas de 70 años de edad o mayores.
Aunque CSDH es uno de los más comunes condiciones en neurocirugía, aún no existe consenso sobre la técnica quirúrgica óptima para tratar la CSDH. La fuga de líquido cefalorraquídeo hacia el espacio subdural puede influenciar en la patogénesis y frecuencia de recurrencia del hematoma subdural crónico y el higroma subdural (SH).
Como lo indica la presencia de βTP en el líquido subdural, la fuga de LCR en el espacio subdural está presente en la gran mayoría de los pacientes con CSDH y SH.
La presencia de una colección de aire subdural postoperatorio se asocia con la recurrencia del hematoma. Los fármacos antiplaquetarios o anticoagulantes pueden facilitar el crecimiento de CSDH, la persistencia del efecto de masa y colección de aire subdural postoperatorios
3-5aumentan el riesgo de recurrencia; aunque no se han investigado ampliamente.
La clasificación de las CSDH según la arquitectura interna y la extensión intracraneal puede ser útil para predecir el riesgo de recurrencia postoperatoria.
El desplazamiento postoperatorio de la línea media (≥5 mm), la diabetes mellitus, la convulsión preoperatoria, el ancho preoperatorio del hematoma (≥20 mm) son predictores independientes de la recurrencia del CSDH. Según la arquitectura interna del hematoma, la tasa de
3-7recurrencia es significativamente menor en el tipo homogéneo y trabecular que en el tipo laminar y separado.
Para prevenirlo se han realizado varias estrategias como el drenaje del hematoma, dejar un drenaje después de la evacuación quirúrgica del hematoma.
Se ha demostrado el beneficio del drenaje postoperatorio después del tratamiento de CSDH, el uso de riego parece ser beneficioso, el trépano realizado el taladro helicoidal o por fresado parecen ser opciones de tratamiento confiables.
3-5La duración del drenaje no está bien establecida, así como la posición postoperatoria.
Bibliografía. 1) Kouchi T, Nobutake S, Kazumichi Y, Osamu N, Masaki C, Sen Y. Independent predictors for recurrence of chronic subdural hematoma: A
review of 343 consecutive surgical cases. Neurosurgery 2008;63(6): 1125–29 h�ps://doi.org/10.1227/01.NEU.0000335782.60059.172) Hiroshi N, Takeo T, Norio Y. Factors in the natural history of chronic sudural hematomas that influence their postoperative recurrence. J
Neurosurg 2001;95(2):256-62 DOI: h�ps://doi.org/10.3171/jns.2001.95.2.0256 3) Kristof RA, Grimm JM, Stoffel-Wagner B.Cerebrospinal fluid leakage into the subdural space: possible influence on the pathogenesis and
recurrence f requency of chronic subdural hematoma and subdural hygroma. J Neurosurg 2008;108(2) :275-80 h�ps://doi.org/10.3171/JNS/2008/108/2/0275
4) Ohba S, Kinoshita Y, Nakagawa T, Murakami H. The risk factors for recurrence of chronic subdural hematoma. Neurosurg Rev2013;36(1):145.50
5) Leroy HA, Aboukais R, Reyns N, Bourgeois P, Labreuche J, Duhamel A, Lejeune J-P. Predictors of functional outcomes and recurrence ofchronic subdural hematomas. J Clin Neuroscience 2015;22(12):1895-1900 h�ps://doi.org/10.1016/j.jocn.2015.03.064
6) Chon K-H, Lee J.M, Koh E-J, Choi H.H. Independent predictors for recurrence of chronic subdural hematoma. Acta Neurochir20112;154(9):1541-48
7) Weiming L, Bakker NA, Groen RJM. Chronic subdural hematoma: a systematic review and meta-analysis of surgical procedures A systematic review. J Neurosurg 2014;665:121:665–73 (http://thejns.org/doi/abs/10.3171/2014.5.JNS132715)
Dra. María Elena Launizar GarcíaAnestesióloga en Trauma
Hospital General Xoco, SEDESA
3
SOCIEDAD MEXICANA DE ANESTESIOLOGÍA EN TRAUMA, A.C.
DITORIALEhronic subdural hematoma (CSDH) is characterized by blood in the subdural space that evokes an inflammatory reaction; It's a common Cform of intracranial hemorrhage with a substantial recurrence rate.
CSDH is common in neurosurgical practice and frequent in the elderly; the recurrence rate is between 2.3 and 33%, in other studies it has an
1-2incidence of 58 / 100,000 people a year in people 70 years of age or older.Although CSDH is one of the most common conditions in neurosurgery, there is still no consensus on the optimal surgical technique to treat CSDH. Leaking cerebrospinal fluid into the subdural space can influence the pathogenesis and frequency of recurrence of chronic subdural hematoma and subdural hygroma (SH).As indicated by the presence of βTP in the subdural fluid, CSF leakage in the subdural space is present in the vast majority of patients with CSDH and SH.The presence of a postoperative subdural air collection is associated with hematoma recurrence. Antiplatelet or anticoagulant drugs can facilitate the growth of CSDH, the persistence of the effect of postoperative mass and subdural air collection increase the risk of recurrence; although they
3-5have not been extensively investigated. The classification of CSDH according to internal architecture and intracranial extension may be useful to predict the risk of postoperative recurrence.Postoperative displacement of the midline (≥5 mm), diabetes mellitus, preoperative seizure, preoperative hematoma width (≥20 mm) are independent predictors of CSDH recurrence. According to the internal architecture of the hematoma, the recurrence rate is significantly lower in
3-7the homogeneous and trabecular type than in the laminar and separated type.To prevent it, several strategies have been carried out, such as draining the hematoma, leaving a drain after the surgical evacuation of the hematoma.The benefit of postoperative drainage has been demonstrated after the CSDH treatment, the use of irrigation seems to be beneficial, the trephine drilled or by milling seems to be reliable treatment options.
3-5The drainage duration is not well established, as is the postoperative position.
Bibliography
1) Kouchi T, Nobutake S, Kazumichi Y, Osamu N, Masaki C, Sen Y. Independent predictors for recurrence of chronic subdural hematoma:
A review of 343 consecutive surgical cases. Neurosurgery 2008;63(6): 1125–29 h�ps://doi.org/10.1227/01.NEU.0000335782.60059.17 2) Hiroshi N, Takeo T, Norio Y. Factors in the natural history of chronic sudural hematomas that influence their postoperative recurrence. J
Neurosurg 2001;95(2):256-62 DOI: h�ps://doi.org/10.3171/jns.2001.95.2.0256 3) Kristof RA, Grimm JM, Stoffel-Wagner B.Cerebrospinal fluid leakage into the subdural space: possible influence on the pathogenesis and
recurrence f requency of chronic subdural hematoma and subdural hygroma. J Neurosurg 2008;108(2) :275-80 h�ps://doi.org/10.3171/JNS/2008/108/2/0275
4) Ohba S, Kinoshita Y, Nakagawa T, Murakami H. The risk factors for recurrence of chronic subdural hematoma. Neurosurg Rev2013;36(1):145.50
5) Leroy HA, Aboukais R, Reyns N, Bourgeois P, Labreuche J, Duhamel A, Lejeune J-P. Predictors of functional outcomes and recurrence ofchronic subdural hematomas. J Clin Neuroscience 2015;22(12):1895-1900 h�ps://doi.org/10.1016/j.jocn.2015.03.064
6) Chon K-H, Lee J.M, Koh E-J, Choi H.H. Independent predictors for recurrence of chronic subdural hematoma. Acta Neurochir20112;154(9):1541-48
7) Weiming L, Bakker NA, Groen RJM. Chronic subdural hematoma: a systematic review and meta-analysis of surgical procedures A systematic review. J Neurosurg 2014;665:121:665–73 (http://thejns.org/doi/abs/10.3171/2014.5.JNS132715)
Dra. María Elena Launizar GarcíaAnestesióloga en Trauma
Hospital General Xoco, SEDESA
4

INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS
SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
RESUMEN.La tasa de recurrencia en los hematomas subdurales crónicos, se estima puede ser amplia y variable de 5 a 30%, dependiendo de los criterios establecidos de recurrencia descritos a lo largo de los años.Generalmente los pacientes que padecen esta patología son mayores de 70 años, algunos con comorbilidades agregadas, una nueva exposición a procedimiento neuroquirúrgico y anestésico pueden ensombrecer el pronóstico de estos pacientes.Objetivo: El presente trabajo tiene como objetivo identificar la incidencia de recurrencia de los pacientes que fueron intervenidos quirúrgicamente por hematomas subdurales agudos, crónicos y epidurales y sus posibles causas desencadenantes en el Hospital de Traumatología IMSS “Dr. Victorio de la Fuente Narváez”.Material y Métodos: Se realizó una revisión retrospectiva de los procedimientos neuroquirúrgicos sometidos durante un año. Se seleccionaron los hematomas Subdurales Agudos y Crónicos, Epidurales y se identificaron aquellos pacientes que se diagnosticaron como Hematomas Subdurales Crónicos Recidivantes. Se revisó la Tomografía de Cráneo Simple (TC) prequirúrgica y posquirúrgica; y se midió el diámetro y espesor del hematoma, volumen, desplazamiento de la línea media, comorbilidades, edad, y técnica anestésica empleada.Resultados: Se obtuvieron un total de 424 procedimientos neuroquirúrgicos, de los cuales 306 pacientes corresponden al sexo masculino (72.16%) y 88 pacientes al sexo femenino (20.7%). Dentro de los procedimientos más frecuentes, se encuentran el Hematoma Subdural Crónico, con 250 pacientes, que corresponde al 59%, el Hematoma Subdural Agudo registró 60 pacientes con el 14.15%. La resolución neuroquirúrgica que predominó fue la evacuación por trépanos único o bilateral con un 72.6% (225) y en segundo lugar la craneotomía con un 27.4% (85 pacientes).Conclusiones: El estudio realizado, nos da como resultado que el predominio de los hematomas subdurales crónicos son la patología más frecuente en el Hospital de Traumatología IMSS “Dr. Victorio de la Fuente Narváez”; la tasa de recidiva es baja, incluso por debajo de los rangos descritos en otros países, sin embargo se habrá de trabajar sobre los hallazgos obtenidos para disminuir o incluso erradicar la aparición de hematomas subdurales crónicos recidivantes, principalmente por la disminución del pronóstico de estos pacientes que generalmente son adultos mayores. Palabras clave: Trauma craneoencefálico, hematoma subdural crónico, hematoma subdural crónico recidivante, paciente neuroquirúrgico.
SUMMARY.The recurrence rate in chronic subdural hematomas is estimated to be broad and variable from 5 to 30%, depending on the established recurrence criteria described over the years.Generally patients suffering from this pathology are older than 70 years, some with added comorbidities, a new exposure to neurosurgical and anesthetic procedures can overshadow the prognosis of these patients.Objective: The objective of this study is to identify the incidence of recurrence of patients who underwent surgery for acute, chronic and epidural subdural hematomas and their possible triggering causes at the Hospital de Traumatología IMSS "Dr. Victorio de la Fuente Narváez ".Material and Methods: A retrospective review of the neurosurgical procedures submitted during one year was conducted. Acute and Chronic and Epidural Subdural hematomas were selected and those patients who were diagnosed as Chronic Recurrent Subdural Hematomas were identified. The preoperative and postoperative Simple Skull Tomography (CT) was reviewed; and the diameter and thickness of the hematoma, volume, displacement of the midline, comorbidities, age, and anesthetic technique used were measured.Results: A total of 424 neurosurgical procedures were obtained, of which 306 patients correspond to the male sex (72.16%) and 88 female patients (20.7%). Among the most frequent procedures, are the Chronic Subdural Hematoma, with 250 patients, corresponding to 59%, the Acute Subdural Hematoma recorded 60 patients with 14.15%. The neurosurgical resolution that prevailed was single or bilateral trephine evacuation with 72.6% (225) and secondly the craniotomy with 27.4% (85 patients).Conclusions: The study carried out shows that the predominance of chronic subdural hematomas are the most frequent pathology in the Hospital Traumatología “Dr. Victorio de la Fuente Narvaez” IMSS, the rate of recurrence is low, even below the ranges described in other countries. However, we must work on the findings obtained to reduce or even eradicate the appearance of recurrent chronic subdural hematomas, mainly due to the decrease in the prognosis of these patients who are generally older adults.Palabras clave: Trauma craneoencefálico, hematoma subdural crónico, hematoma subdural crónico recidivante, paciente neuroquirúrgico.
5
Dra. Alma Edith Gress MendozaServicio de Anestesiología y Neuroanestesiología Hospital de Traumatología “Magdalena de las Salinas”Unidad Médica de Alta Especialidad “Dr. Victorio de la Fuente Narváez”Instituto Mexicano del Seguro [email protected]. Michael Herbas RochaMédico NeurocirujanoCirugía en Epilepsia y FuncionalHospital de Traumatología “Magdalena de las Salinas”Unidad Médica de Alta Especialidad
INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS
SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
I. INTRODUCCIÓN.El Trauma Craneoencefálico (TCE) actualmente representa un problema de salud grave y es la causa más común de muerte y discapacidad en la población pediátrica y adulto joven. Se clasifica según el nivel de conciencia, medido por la Escala de Coma de Glasgow (GCS): TCE leve puntaje de 15 a 13, moderado de 12 a 9, severo menor de 8.Según su fisiopatología pueden ser lesiones focales y difusas, dentro de estas se encuentran los hematomas subdurales, h e m a t o m a s e p i d u r a l e s , y / o h e m o r r a g i a s intraparenquimatosas. Las lesiones focales como el Hematoma Subdural son lesiones frecuentes, estos se encuentran entre la membrana subdural y la aracnoides y se pueden clasificar según su tiempo de aparición en agudo o crónico. En la persona joven suele ser un espacio virtual, pero existen algunas circunstancias en la evolución de las personas que condicionan que el espacio subdural sea más grande, como la atrofia cerebral secundaria a edad avanzada, alcoholismo crónico, demencia senil por Alzheimer, etc. Un golpe lo suficientemente fuerte puede condicionar el acúmulo del hematoma por ruptura de venas puente y mantener al paciente asintomático. El hematoma subdural se puede clasificar por el tiempo de evolución: los agudos son los que se presentan en las primeras 72 horas, los subagudos entre las 3 y 4 semanas y los crónicos
1después de las 3 semanas a 4 meses.El Hematoma Subdural Crónico tiene una tasa significante de recurrencia, los rangos oscilan de 5 a 30%. Por lo que se propone realizar el presente estudio con la finalidad de buscar la frecuencia de hematomas subdurales crónicos recidivantes en el Hospital de Traumatología IMSS “Dr. Victorio de la Fuente Narváez” y sus posibles causas.
II. ANTECEDENTES.El trauma craneoencefálico (TCE) es la lesión física o deterioro funcional del contenido craneal secundario a un intercambio
1repentino de energía mecánica.Se tiene el antecedente de realizar trepanación desde el Neolítico, que consistía en la retirada de secciones de hueso del cráneo trypanon (perforador), así como en Francia y Perú, 500 a.c. La evidencia más antigua se tiene del papiro de Edwin Smith, VII a.c. Hipócrates, 460 a 380 a.c.; hace descripciones sobre las heridas de la cabeza. Herófilo de Calcedonia, considerado padre la anatomía, estudió el cerebro y sus meninges; Celsus describe el hematoma epidural; Galeno de Pérgamo (129-210 d.c) describió las fracturas deprimidas y su manejo, así como las lesiones medulares. Pablo de Egina (625–690 d.c.), cambia el concepto por trauma craneal, clasifica las fracturas de cráneo y aconseja el uso de la trefina. Rhazes (875 d.c.) fue el primero en utilizar el término concusión y aconseja la cirugía para las heridas penetrantes del cráneo y levantamiento de las fracturas deprimidas.En Europa, Teodorico de Cervia (1205–1298), Jean Louis Petit (1674–1750) define la compresión del cerebro como causa de somnolencia. Victor Horsley (1857–1916) hipotetizó que las trepanaciones se llevaban a cabo para tratar la epilepsia focal secundaria en las fracturas conminutas y hundimientos que
2comprimían la corteza motora primaria. 1974 Bryan Jennett, describe la escala de coma de Glasgow
3(GCS).
Epidemiología.El Traumatismo Craneoencefálico (TCE); es una de las condiciones del trauma más frecuentes en cuanto a atención prehospitalaria y hospitalaria. A nivel mundial 1.2 millones de personas fallecen anualmente por TCE y 20 a 50 millones sufren TCE no mortal.Es la tercera causa de muerte (antes que los problemas cardiovasculares y el cáncer) que corresponden a muertes violentas y accidentes, para el 2008 en México se registraron 35,567 defunciones con mortalidad de 38.8 por 100 000 habitantes, con una relación 3 a 1 varón–mujer, afectando principalmente a la población de entre 15 a 45 años. Las causas más comunes en un 75% son los accidentes de tráfico, afectando a jóvenes menores de 25 años, motociclistas y en
4estado de ebriedad.Para el 2011; los accidentes por vehículo automotor corresponden a la 8ª causa de muerte, que corresponden a 16,615 muertes, con una tasa de mortalidad de 14.4 por cada 100,000 habitantes, con una tasa de letalidad de 40.3 por cada 1000 habitantes. La población de 15 a 29 años representa el
533% de muertes correspondientes a siniestros de tránsito.Un 53% de los pacientes admitidos en urgencias, en las unidades hospitalarias con diagnóstico de trauma severo de cráneo mueren dentro de los siguientes 6 meses; 17% evolucionan desfavorablemente y solo 24% tienen evolución y pronóstico favorable dentro de los 6 meses posteriores al
6trauma. Respecto a los traumatismos no mortales, un porcentaje importante de sobrevivientes presentan secuelas importantes que impedirán o dificultarán el retorno y readaptación a sus actividades anteriores. Solo el 40% de los sobrevivientes se
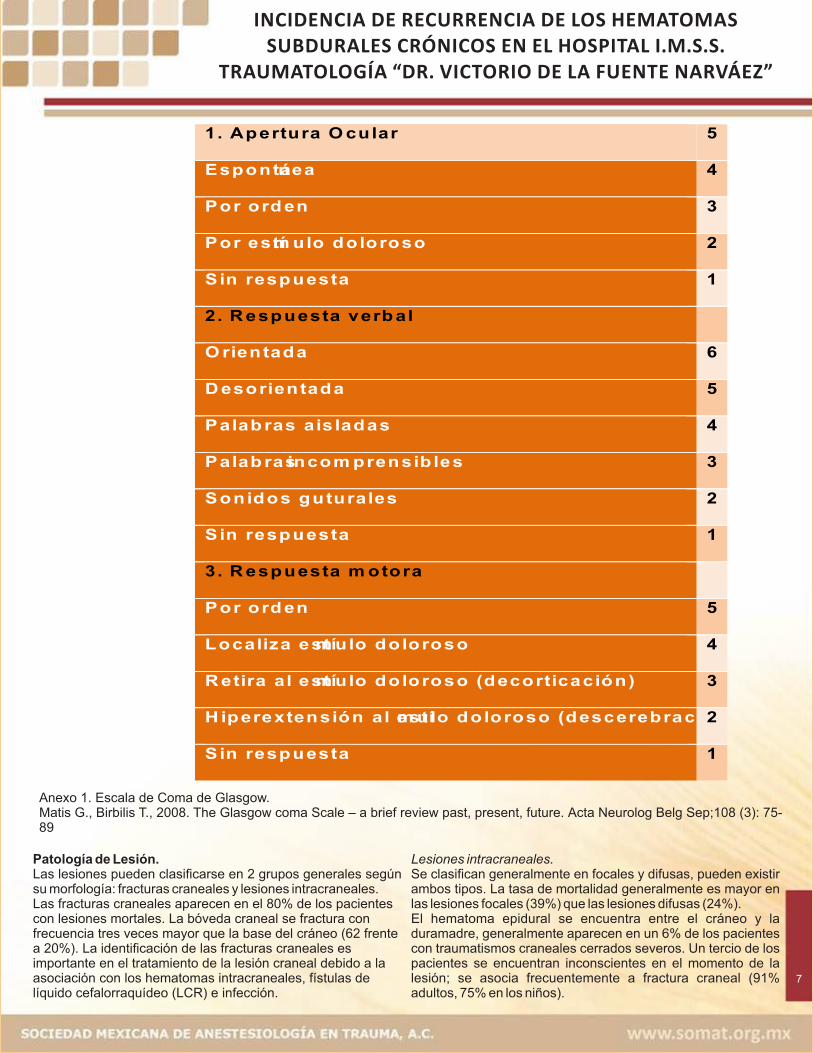
7reincorporan.El TCE se clasifica basándose en su mecanismo de lesión, gravedad, patología y hal lazgos en la Tomografía Computarizada (TC). Mecanismo de Lesión.Las lesiones craneales se dividen según el modo de lesión. Las lesiones craneales cerradas que se asocian a accidentes en vehículo de motor, caídas y agresiones. Las lesiones abiertas o penetrantes, o por proyectiles, son debidas frecuentemente a heridas por armas de fuego. Gravedad de la lesión.La Escala de Coma de Glasgow de (ECG) se utiliza para cuantificar la exploración neurológica. Se basa en 3 parámetros: apertura ocular, habla y función motora. ANEXO 1El paciente que obedece órdenes y está orientado, se otorgan 15 puntos; una puntuación de 13 a 15 puntos, se considera una lesión leve, una puntuación entre 9 y 12 puntos se considera una lesión moderada y una puntuación menor a 8 puntos,
3postreanimación ha sufrido una lesión craneal severa.Patología de Lesión.Las lesiones pueden clasificarse en 2 grupos generales según su morfología: fracturas craneales y lesiones intracraneales. Las fracturas craneales aparecen en el 80% de los pacientes con lesiones mortales. La bóveda craneal se fractura con frecuencia tres veces mayor que la base del cráneo (62 frente a 20%). La identificación de las fracturas craneales es importante en el tratamiento de la lesión craneal debido a la asociación con los hematomas intracraneales, f ís tu las de l íquido cefalorraquídeo (LCR) e infección.
6
INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
Anexo 1. Escala de Coma de Glasgow.Matis G., Birbilis T., 2008. The Glasgow coma Scale – a brief review past, present, future. Acta Neurolog Belg Sep;108 (3): 75-89
7
1. Apertura O cular 5
Espontánea 4
Por ord en 3
Por estím ulo doloroso 2
S in respuesta 1
2. R espuesta verb al
O rientada 6
D esorientada 5
Palab ras ais ladas 4
Palab ras incom prensib les 3
Sonidos guturales 2
S in respuesta 1
3. R espuesta m otora
Por ord en 5
Localiza estím ulo doloroso 4
R etira al estím ulo doloroso (decorticación) 3
H iperextensión al estím ulo doloroso (descerebración). 2
S in respuesta 1
Patología de Lesión.Las lesiones pueden clasificarse en 2 grupos generales según su morfología: fracturas craneales y lesiones intracraneales. Las fracturas craneales aparecen en el 80% de los pacientes con lesiones mortales. La bóveda craneal se fractura con frecuencia tres veces mayor que la base del cráneo (62 frente a 20%). La identificación de las fracturas craneales es importante en el tratamiento de la lesión craneal debido a la asociación con los hematomas intracraneales, fístulas de líquido cefalorraquídeo (LCR) e infección.
Lesiones intracraneales.Se clasifican generalmente en focales y difusas, pueden existir ambos tipos. La tasa de mortalidad generalmente es mayor en las lesiones focales (39%) que las lesiones difusas (24%).El hematoma epidural se encuentra entre el cráneo y la duramadre, generalmente aparecen en un 6% de los pacientes con traumatismos craneales cerrados severos. Un tercio de los pacientes se encuentran inconscientes en el momento de la lesión; se asocia frecuentemente a fractura craneal (91% adultos, 75% en los niños).
INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS
SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
Esta patología es detectada por tomografía (TC) en la mayoría de los pacientes (80%), la mayor parte de estos pacientes son
10asintomáticos y clínicamente insignificantes.La combinación de la edad de la población y el incremento en el uso de medicación antiplaquetaria y anticoagulante ha condicionado también el incremento de la incidencia de los hematomas subdurales crónicos, estos se ha ido incrementando substancialmente en los últimos 25 años.Los 3 métodos de evacuación de los hematomas son principalmente: agujero único por craneostomía, perforación helicoidal por craneostomía y craneotomía. Generalmente la técnica mínimamente invasiva por orificio helicoidal suele ser una técnica segura y eficaz. Sin embargo se debe seguir un
11estudio futuro de ésta.
Diseño del estudio:El objetivo general fue evaluar el curso posoperatorio de los pacientes con Hematoma subdural crónico del Hospital de Traumatología IMSS Victorio de la Fuente Narváez, durante un periodo de 1 año, de octubre del 2014 a septiembre del 2015, e identificar los casos que presentaron resangrado; considerando identificar la incidencia de recurrencia de hematomas subdurales crónicos en un periodo de 1 años, las posibles causas que condicionaron que pacientes posoperados de drenaje de hematoma subdural crónico, presentaron recurrencia de resangrado, la técnica quirúrgica que se utilizó durante el procedimiento neuroquirúrgico inicial, así como de la reintervención; que manejo anestésico se dio, las comorbilidades de los pacientes y la condición neurológica de ingreso del paciente y durante el procedimiento inicial y su reintervención mediante la escala de coma de Glasgow.Debido a que el Hematoma Subdural Crónico (HSC) es una patología que se presenta principalmente en pacientes adultos mayores y es una condición clínica grave que pone en peligro la vida, además de las diferentes comorbilidades que pueden padecer, hace que estos pacientes presenten un elevado riesgo anestésico–quirúrgico que podría desencadenar en un desenlace fatal, más aún el riesgo de requerir una nueva reintervención por presentar resangrado durante su evolución posoperatoria.Se justifica que se tiene la necesidad de investigar cual es la incidencia de resangrado en éste tipo de pacientes.Metodología.Previa autorización de la unidad de enseñanza e investigación y del comité de ética del hospital, se realizó el estudio de tipo retrospectivo, analítico, longitudinal, observacional.Se revisó de forma consecutiva desde octubre del 2014 a septiembre del año 2015 la base de datos registrada en el área de quirófano del Hospital de Traumatología IMSS Victorio de la Fuente Narváez; se identificaron los procedimientos neuroquirúrgicos realizados durante este periodo, se seleccionaron los diagnósticos de hematomas subdurales crónicos ingresados para drenaje de hematoma ya sea por técnica quirúrgica trepanación única o doble, y/o bilateral, craneotomía y /o craniectomía; se seleccionaron los pacientes que durante el transcurso posoperatorio se registraron como hematoma recurrente. 8
La sangre proviene de la sección de vasos durales, generalmente arteriales, del hueso craneal fracturado y ocasionalmente de los senos venosos seccionados. En la TC el hematoma epidural se caracteriza por una lesión biconvexa, hiperdensa. El hematoma subdural es la lesión intracraneal focal más frecuente. El hematoma se localiza entre la duramadre y el cerebro, siendo consecuencia generalmente de la sección de las venas puente, situadas entre la corteza y los senos de drenaje. El hematoma subdural agudo que se observa después de las 72 horas del TCE, se observa en la TC como una masa hiperdensa y homogénea en forma de media luna y paralela a la calota. La tasa de mortalidad es elevada; del 50%, dependiendo de varios factores como: edad, tiempo transcurrido entre la lesión y el tratamiento, alteraciones pupilares, puntuación de la ECG al ingreso, hallazgos de la TC, presión intracraneana (PIC) durante y posoperatoria y el tipo de cirugía.La TC puede arrojar datos predictivos pronósticos como: grosor del hematoma, desplazamiento de la línea media, tumefacción presente o concusión cerebral subyacente. La tasa de supervivencia es del 50% para un hematoma con grosor de 18 mm y desplazamiento de la línea media de 20 mm. La supervivencia es del 0% cuando el desplazamiento de la línea media es mayor a 25 mm.El hematoma subdural se puede clasificar por el tiempo de evolución: los agudos son los que se presentan en las primeras 72 horas, los subagudos entre las 3 y 4 semanas y los crónicos después de las 3 semanas a 4 meses.En los hematomas subdurales se ha observado una reducción del flujo sanguíneo cerebral, por debajo del umbral isquémico y
8una disminución marcada de la oxigenación cerebral.Los hematomas subdurales crónicos (CSDH) generalmente ocurren en la edad adulta, con un promedio de edad de 63 años. El trauma craneal es identificado en menos del 50% de los casos (muchas veces en relación a contusiones triviales). Otros factores de riesgo identificados son: abuso de alcohol, crisis convulsivas, derivaciones ventrículo peritoneal, coagulopatías (incluyendo anticoagulación terapéutica), y pacientes con riesgos de caída (por ejemplo hemiplejia previa por EVC). Los CSDHs son bilaterales en 20 a 25% de los casos.El espesor de los hematomas tienden a ser mayor en pacientes ancianos debido a que decrece el peso del cerebro e incrementa el espacio subdural.Generalmente el contenido del Hematoma Subdural Crónico es un fluido conocido como aceite de motor quemado. La sangre en el espacio subdural evoca la respuesta inflamatoria. Con el paso de los días, los fibroblastos invaden el coágulo y forman neomembranas sobre la cortical y la superficie dural. Esto es seguido por formación neocapilar, fibrinolisis enzimática y licuefacción del coágulo sanguíneo.Los pacientes suelen presentar síntomas de cefalea, confusión, dificultad en el lenguaje o síntomas de Ataque
9Isquémico Transitorio (TIA). La tasa de recurrencia es significante en los hematomas subdurales crónicos (HSC), varía de un rango de 5 a 30 %. Hay algunos criterios que definen la recurrencia de los
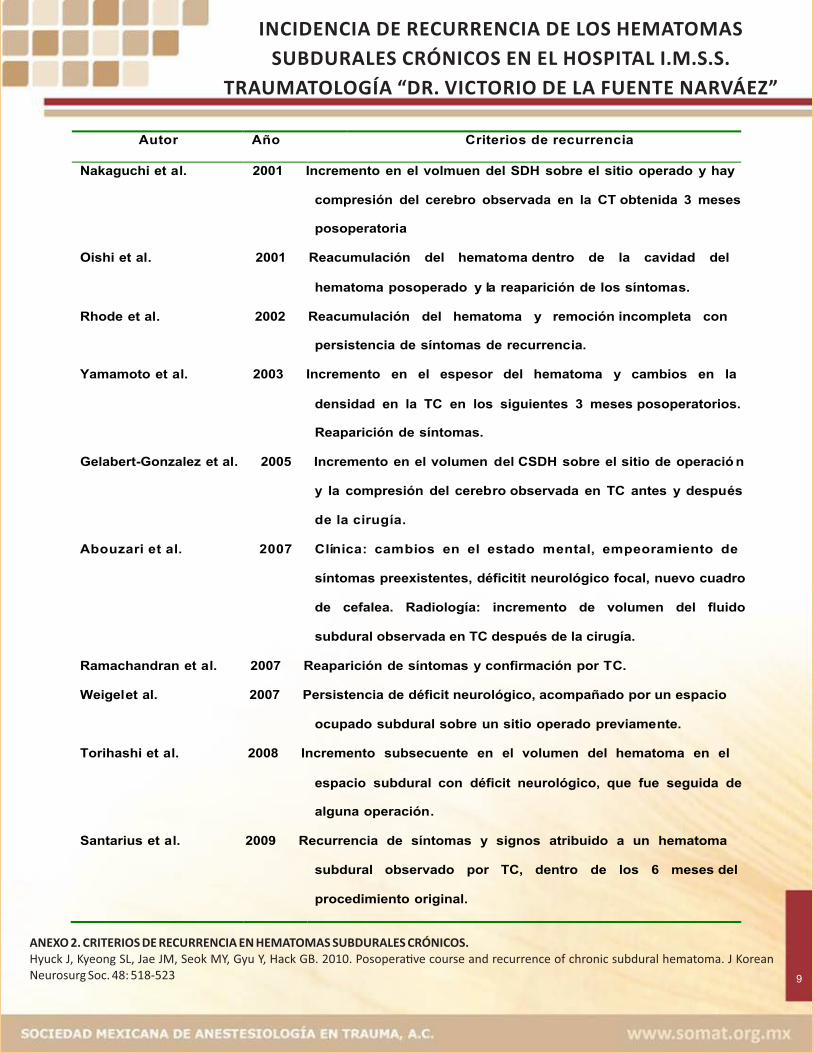
10hematomas subdurales crónicos. Anexo 2
INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS
SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
9
ANEXO 2. CRITERIOS DE RECURRENCIA EN HEMATOMAS SUBDURALES CRÓNICOS.Hyuck J, Kyeong SL, Jae JM, Seok MY, Gyu Y, Hack GB. 2010. Posopera�ve course and recurrence of chronic subdural hematoma. J Korean Neurosurg Soc. 48: 518-523
Autor Año Criterios de recurrencia
Nakaguchi et a l. 2001 Incremento en el volmuen del SDH sobre el sitio operado y hay y
compresión del cerebro observada en la CT obt enida 3 meses
posoperatori a
Oishi et al . 2001 Reacumulación del hemato ma dentro de la cavidad del l
hematoma posoperado y l a reaparición de los síntoma s.
Rhode et al . 2002 Reacumulación del hematoma y remoción incompleta con
persistencia de síntomas de recurrenc ia.
Yamamoto et a l. 2003 Incremento en el espesor del hematoma y cambios en la
densidad en la TC en los siguientes 3 meses posoperatorios.
Reaparición de síntomas.
Gelabert-Gonzalez et al . 2005 Incremento en el volumen d el CSDH sobre el sitio de operació n
y la compresión del cereb ro observada en TC antes y despu és
de la cirugía.
Abouzari et al. 2007 Clínica: cambios en el estado mental, empeoramiento de los
síntomas preexistentes, déficitit neurológico focal, nuevo cuadro
de cefalea. Radiología: incremento de volumen del fluido
subdural observada en TC después de la cirugía.
Ramachandran et a l. 2007 Reaparición de síntomas y confirmación por T C.
Weigel et al. 2007 Persistencia de déficit neurológico, acompañado por un espacio cio
ocupado subdural sobre un sitio operado previame nte.
Torihashi et a l. 2008 Incremento subsecuente en el volumen del hematoma en el
espacio subdural con déficit neurológico, que fue seguida de e
alguna operación .
Santarius et a l. 2009 Recurrencia de síntomas y signos atribuido a un hematoma a
delsubdural observado por TC, dentro de los 6 meses del
procedimiento original.
INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS
SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
10
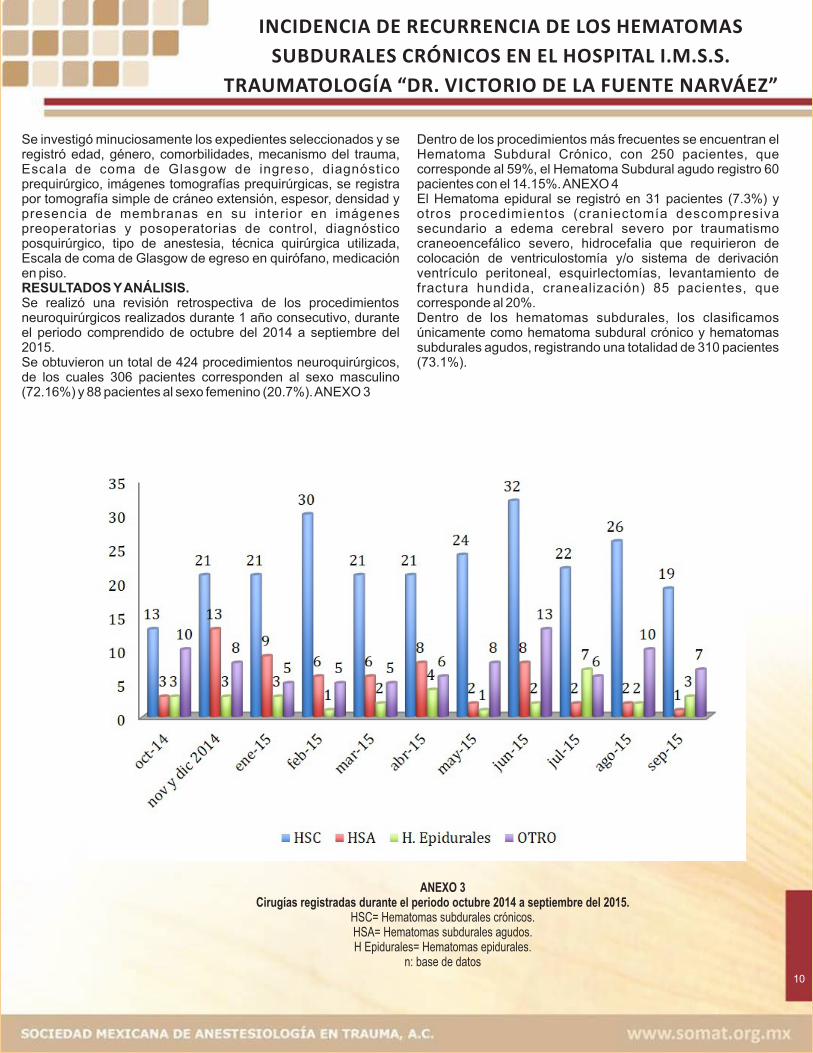
Se investigó minuciosamente los expedientes seleccionados y se registró edad, género, comorbilidades, mecanismo del trauma, Escala de coma de Glasgow de ingreso, diagnóstico prequirúrgico, imágenes tomografías prequirúrgicas, se registra por tomografía simple de cráneo extensión, espesor, densidad y presencia de membranas en su interior en imágenes preoperatorias y posoperatorias de control, diagnóstico posquirúrgico, tipo de anestesia, técnica quirúrgica utilizada, Escala de coma de Glasgow de egreso en quirófano, medicación en piso. RESULTADOS Y ANÁLISIS.Se realizó una revisión retrospectiva de los procedimientos neuroquirúrgicos realizados durante 1 año consecutivo, durante el periodo comprendido de octubre del 2014 a septiembre del 2015. Se obtuvieron un total de 424 procedimientos neuroquirúrgicos, de los cuales 306 pacientes corresponden al sexo masculino (72.16%) y 88 pacientes al sexo femenino (20.7%). ANEXO 3
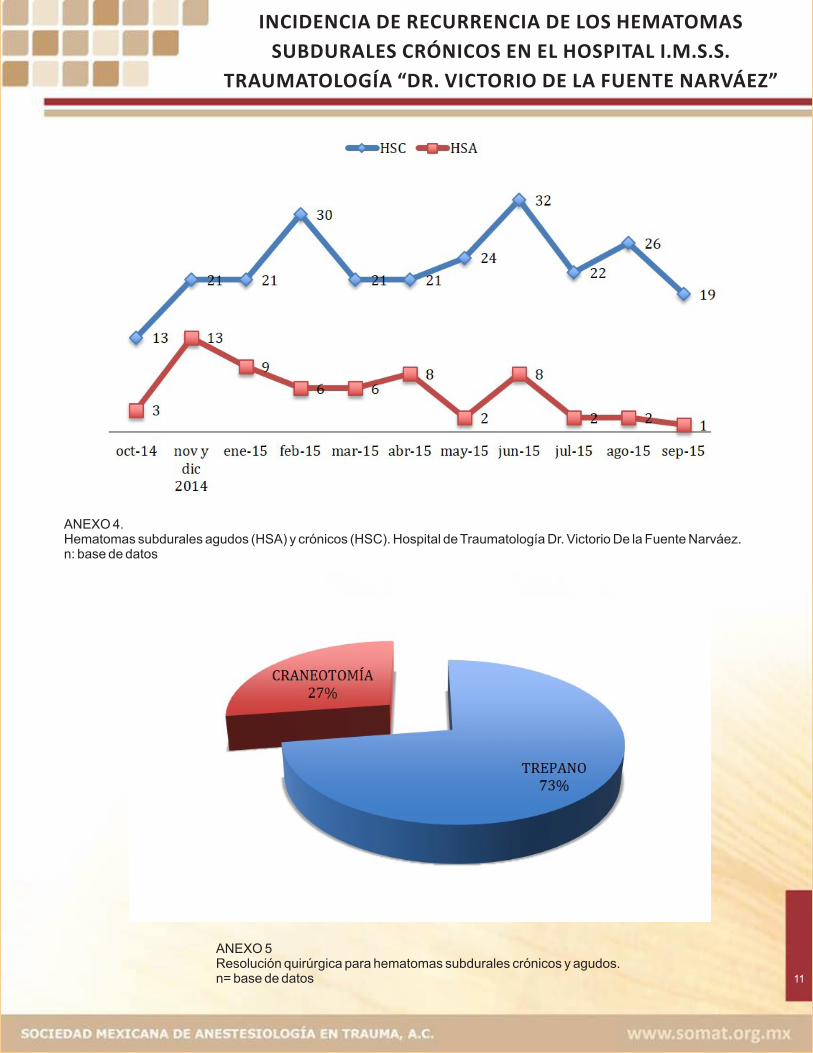
Dentro de los procedimientos más frecuentes se encuentran el Hematoma Subdural Crónico, con 250 pacientes, que corresponde al 59%, el Hematoma Subdural agudo registro 60 pacientes con el 14.15%. ANEXO 4El Hematoma epidural se registró en 31 pacientes (7.3%) y otros procedimientos (craniectomía descompresiva secundario a edema cerebral severo por traumatismo craneoencefálico severo, hidrocefalia que requirieron de colocación de ventriculostomía y/o sistema de derivación ventrículo peritoneal, esquirlectomías, levantamiento de fractura hundida, cranealización) 85 pacientes, que corresponde al 20%.Dentro de los hematomas subdurales, los clasificamos únicamente como hematoma subdural crónico y hematomas subdurales agudos, registrando una totalidad de 310 pacientes (73.1%).
ANEXO 3Cirugías registradas durante el periodo octubre 2014 a septiembre del 2015.
HSC= Hematomas subdurales crónicos. HSA= Hematomas subdurales agudos.H Epidurales= Hematomas epidurales.
n: base de datos
INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS
SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
ANEXO 5Resolución quirúrgica para hematomas subdurales crónicos y agudos.n= base de datos 11
ANEXO 4.Hematomas subdurales agudos (HSA) y crónicos (HSC). Hospital de Traumatología Dr. Victorio De la Fuente Narváez.n: base de datos
INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS
SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
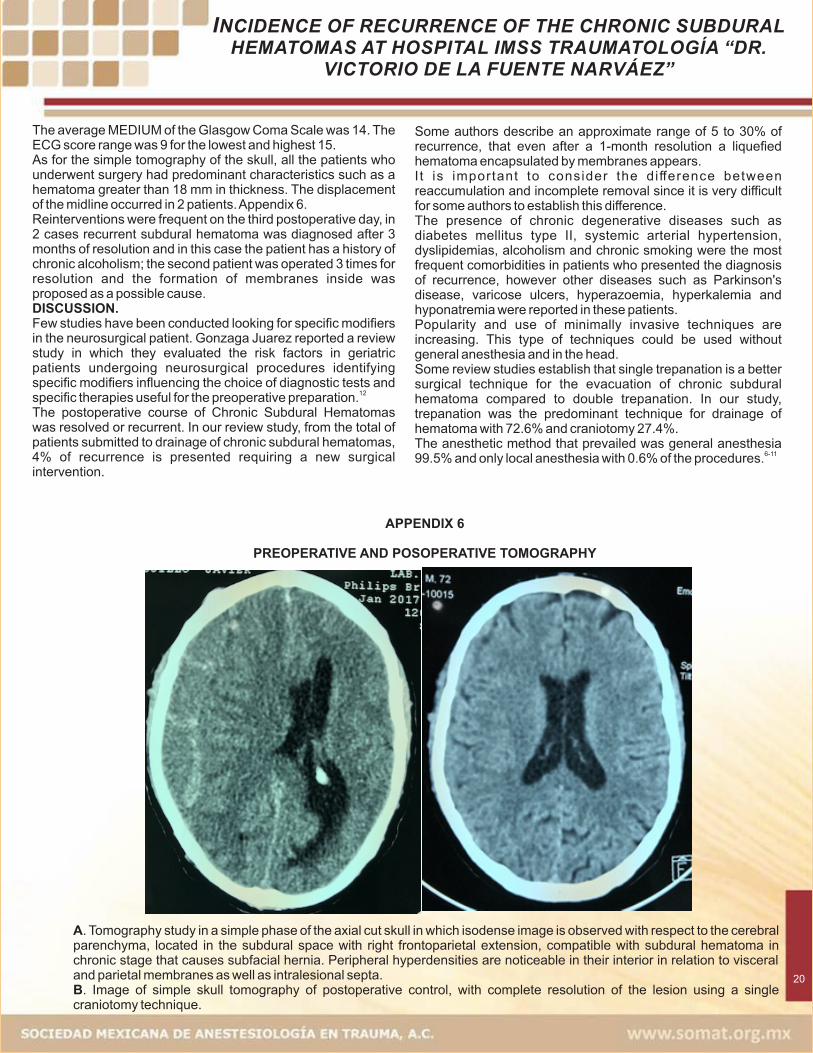
La MEDIANA promedio de la Escala de Coma de Glasgow fue 14. El rango de puntuación de la ECG fue 9 para el menor y el mayor 15. En cuanto a la tomografía simple de cráneo, todos los pacientes intervenidos presentaron características predominantes como hematoma mayor a 18 mm de espesor. El desplazamiento de la línea media se presentó en 2 pacientes. ANEXO 6Las reintervenciones fueron frecuentes al tercer día posquirúrgico, en 2 casos se diagnosticó hematoma subdural recidivante después de 3 meses de su resolución y en este caso el paciente cuenta con antecedente de alcoholismo crónico; el segundo paciente fue intervenido en 3 ocasiones para resolución y se propone como posible causa la formación de membranas en su interiorDISCUSIÓN.Pocos estudios se han realizado buscando modificadores específicos en el paciente neuroquirúrgico. Gonzaga Juárez reportan un estudio de revisión en el cual evalúan los factores de riesgo en el paciente geriátrico sometido a procedimientos neuroquirúrgicos identificando modificadores específicos que influyen en la elección de pruebas diagnósticas y terapias
12especificas útiles para la preparación preoperatoria.
12
El procedimiento quirúrgico de estos pacientes se registró de la siguiente forma: 225 pacientes fueron intervenidos quirúrgicamente por trepanación (72.6%), ya sea único o doble. 85 pacientes fueron resueltos por craneostomía (27.4%).Se registraron 10 pacientes que presentaron hematoma subdural crónico recidivante, lo que corresponde al 4% del total de hematomas subdurales crónicos. De estos pacientes, la mediana de edad fue 66.5 años, con un valor máximo de 92 años y el menor de 33 años.Las comorbilidades más frecuentes fueron alcoholismo 7%, diabetes mellitus tipo II (DMTII) con 4%, hipertensión arterial sistémica (HAS) 2%, tabaquismo 4% y otros como Parkinson, hiperazoemia, úlcera varicosa, etc. 3%. Todos los laboratorios se encontraban dentro de parámetros normales. El tiempo de evolución del diagnóstico inicial y la formación de un nuevo hematoma obtuvo un rango de 3 días a 120 días, con una MEDIA de 4 y MEDIA ARMONICA de 4.2. El tiempo menor fue de 3 días y el máximo de 120 días. Las resoluciones quirúrgicas iniciales en 9 procedimientos fue drenaje de hematoma por trépanos y uno de forma inicial por craneotomía; durante el segundo tiempo quirúrgico la técnica quirúrgica elegida fue craneotomía y en un caso se realizó una tercera intervención por craneotomía para membranectomía. ANEXO 5
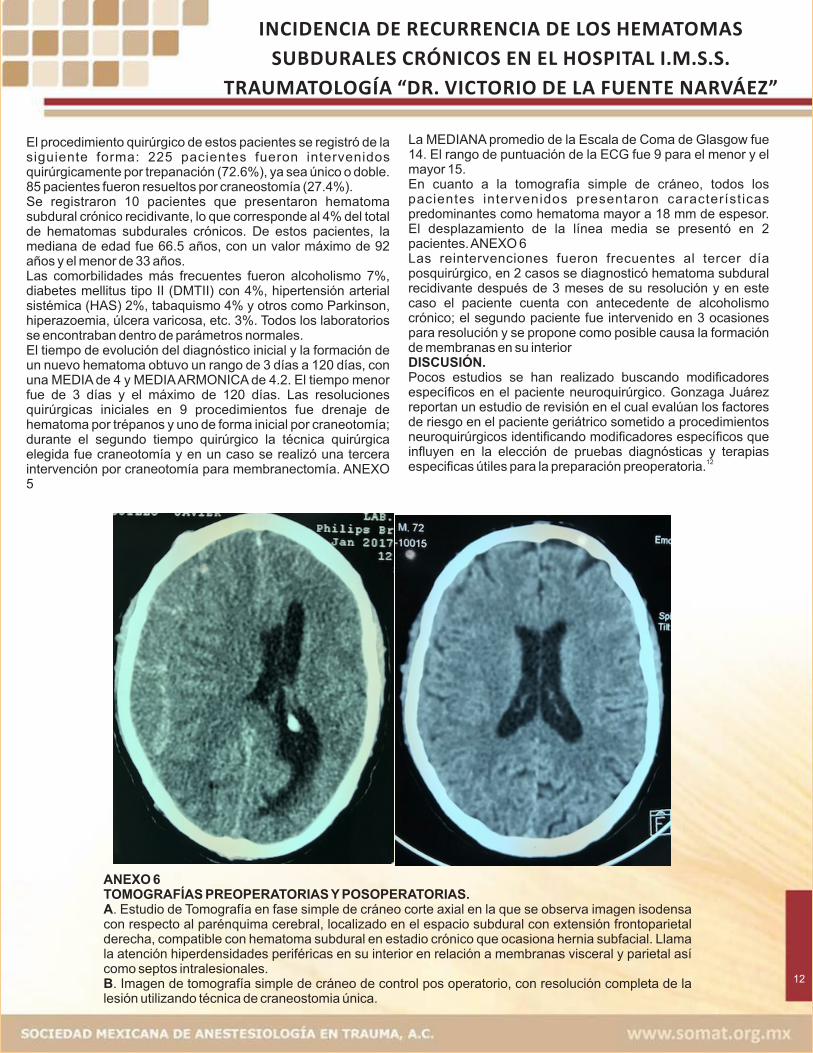
ANEXO 6TOMOGRAFÍAS PREOPERATORIAS Y POSOPERATORIAS.A. Estudio de Tomografía en fase simple de cráneo corte axial en la que se observa imagen isodensa con respecto al parénquima cerebral, localizado en el espacio subdural con extensión frontoparietal derecha, compatible con hematoma subdural en estadio crónico que ocasiona hernia subfacial. Llama la atención hiperdensidades periféricas en su interior en relación a membranas visceral y parietal así como septos intralesionales. B. Imagen de tomografía simple de cráneo de control pos operatorio, con resolución completa de la lesión utilizando técnica de craneostomia única.
INCIDENCIA DE RECURRENCIA DE LOS HEMATOMAS
SUBDURALES CRÓNICOS EN EL HOSPITAL I.M.S.S.
TRAUMATOLOGÍA “DR. VICTORIO DE LA FUENTE NARVÁEZ”
capturar un número mayor de muestra o bien iniciar un estudio prospectivo que nos permita vigilar estrechamente al paciente neuroquirúrgico y disminuir al máximo la posibilidad de recurrencia en hematomas subdurales crónicos.
BIBLIOGRAFÍA.1. Narayan RK; Michel ME; Ansell B; Baethmann A;
Biegon A; Bracken MB; Bullock MR. 2002. Clinicaltrials in head injury. J Neurotrauma;19 (5): 503-557
2. Rubiano A., Pérez R. 2008. Neurotrauma yneurointensivismo. En: Peña Q. Rubiano A. Reseñahistórica del trauma craneoencefálico. BogotáColombia. DISTRIBUNA. Cap 3.
3. Matis G., Birbilis T., 2008. The Glasgow coma Scale – abrief review past, present, future. Acta Neurolog BelgSep;108 (3): 75-89
4. Sistema Nacional de Vigilancia Epidemiológica. SSA,2014 No. 26, vol. 25
5 . http://www.cenetec.salud.gob.mx/descargas/gpc/CatalogoMaestro/016_GPC_TCEenelAdulto/SSA_016_08_EyR.pdf
6 . https://www.braintrauma.org/pdf/protected/Guidelines_Management_2007w_bookmarks.pdf
7. González Villavelázquez ML, García González A.Traumatismo craneoencefálico. Rev Mex Anest2013;;36(Supl. 1):S186-S193
8. Greenberg MS. 2010. Handbook of Neurosurgery. Ensu: Head trauma. Seventh Edition. Florida. THIEME.pag: 899-901.
9. Cottrel J. Young W. 2010. Cotrell and Young´sNeuroanesthesia. En: Bendo A. Perioperativemanagement of adult patients with severe head injury.5ta edición, Philadelphia. MOSBY ELSEVIER. pag:317-325.
10. Hyuck J, Kyeong SL, Jae JM, Seok MY, Gyu Y, HackGB. 2010. Posoperative course and recurrence ofchronic subdural hematoma. J Korean Neurosurg Soc.48: 518-523
11. Chari A, Kolias A, Santarius T, Bond S, Hutchinson P.2014. Twist-drill craniostomy with hollow screws forevacuation of chronic subdural hematoma. JNeurosurg. 121:176-183
12. Gonzaga R., Juárez. 2010. Factores de riesgo en el paciente geriátrico sometido a neurocirugía. Revista Mexicana de Anestesiología. 33 (1): S99-S100.
13
El curso posoperatorio de los Hematomas Subdurales Crónicos fue resuelto o recurrente. En nuestro estudio de revisión del total de pacientes sometidos a drenaje de hematomas subdurales crónicos, se presenta el 4% de recurrencia que requieren de nueva intervención quirúrgica. Algunos autores describen un rango aproximado de 5 a 30% de recurrencia, que incluso después de 1 mes de resolución se presenta un hematoma licuefacto encapsulado por membranas. Es importante tomar en cuenta la diferencia entre reacumulación y una remoción incompleta ya que es muy difícil para algunos autores establecer esta diferencia. La presencia de enfermedades crónicas degenerativas como diabetes mellitus tipo II, hipertensión arterial sistémica, dislipidemias, alcoholismo y tabaquismo crónico fueron las comorbilidades más frecuentes en los pacientes que presentaron el diagnóstico de recidiva, sin embargo otras enfermedades como Parkinson, úlceras varicosas, hiperazoemia, hiperkalemia e hiponatremia se hicieron presentes en estos pacientes.Las técnicas mínimamente invasivas se encuentran en incremento en su popularidad y uso. Este tipo de técnicas pueden ser utilizadas sin anestesia general y en la cabecera.Hay estudios de revisión que establecen que la trepanación única es una mejor técnica quirúrgica para la evacuación del hematoma subdural crónico en comparación con la trepanación doble. En nuestro estudio se encontró como predominante la trepanación como técnica de elección para drenaje de hematoma con un 72.6% y craneostomía 27.4%. El método anestésico que predominó fue anestesia general 99.5% y únicamente anestesia local con 0.6% de los
6-11procedimientos.CONCLUSIONES.Se evaluó el curso posoperatorio de los paciente sometidos a procedimiento neuroquirúrgico del Hospital de Traumatología IMSS Dr. Victorio de la Fuente Narváez durante un periodo de un año, hasta encontrar los hematomas subdurales crónicos que presentaron recurrencia. Se identificaron imágenes características que se presentaron en la mayoría de los pacientes con diagnóstico de hematoma subdural crónico recurrente por Tomografía Computada de Cráneo como son el espesor del hematoma y desplazamiento de la línea media, pero que sin embargo requiere una revisión más minuciosa de estos estudios para establecer posibles factores predisponentes de recurrencia en una revisión poblacional mayor a futuro. La técnica quirúrgica de elección para el tratamiento inicial fue mínima invasión por trepanación y como segunda opción craneotomía. En cuanto a procedimiento anestésico predominó la anestesia general balanceada. Aunque los hematomas subdurales crónicos son de predominio en paciente adultos mayores, pueden presentarse en menor medida en pacientes jóvenes y de la misma manera pueden ensombrecer el pronóstico según sus comorbilidades. El alcoholismo fue la comorbilidad más frecuente en estos pacientes.El estudio tiene limitantes por ser retrospectivo sin embargo se cumplieron algunos de los objetivos establecidos y el restante se propone realizar una revisión más amplia para

INCIDENCE OF RECURRENCE OF THE CHRONIC SUBDURAL HEMATOMAS AT HOSPITAL IMSS TRAUMATOLOGÍA “DR.
VICTORIO DE LA FUENTE NARVÁEZ”
INTRODUCTION.Cranioencephalic Trauma (TBI) currently represents a serious health problem and is the most common cause of death and disability in the pediatric and young adult population.It is classified according to the level of consciousness, as measured by the Glasgow Coma Scale (GCS): mild TCE score from 15 to 13, moderate from 12 to 9, severe under 8.Depending on their pathophysiology, they may be focal and diffuse lesions, including subdural hematomas, epidural hematomas, and / or intraparenchymal hemorrhages.Focal lesions such as Subdural Hematoma are frequent lesions, these are between the subdural membrane and the arachnoid and can be classified according to their time of onset in acute or chronic. In the young person there is usually a virtual space, however, some circumstances in their evolution condition a larger subdural space, such as brain atrophy secondary to old age, chronic alcoholism, senile dementia for Alzheimer's, etc. A blow strong enough could condition the accumulation of the hematoma by rupture of bridging veins and keep the patient asymptomatic.Subdural hematoma is classified by the time of evolution: the acute ones are those that appear in the first 72 hours, the subacute ones between 3 and 4 weeks and the chronic ones
1after the 3 weeks to 4 months.Chronic Subdural Hematoma has a significant rate of recurrence, they range from 5 to 30%. So, the present study aims to find the frequency of recurrent chronic subdural hematomas at Hospital de Traumatología IMSS “Dr. Victorio de la Fuente Narváez” and its possible causes.
I. BACKGROUND.Cranioencephalic trauma (TBI) is the physical injury or functional deterioration of the cranial content secondary to a
1sudden exchange of mechanical energy.History of trepanation comes from the Neolithic and consisted in the removal of bone sections of the skull trypanon (perforator), as well as in France and Peru, 500 a.c. The oldest evidence was taken from the papyrus of Edwin Smith, VII a.c. Hippocrates, 460 to 380 BC; makes descriptions about head injuries. Herophilus of Chalcedon, considered the father of anatomy, studied the brain and its meninges; Celsus described the epidural hematoma; Galen of Pergamon (129-210 AD) described depressed fractures and their management, as well as spinal cord injuries. Pablo de Egina (625-690 AD), changed the concept for cranial trauma, classified skull fractures and advised the use of trephine. Rhazes (875 AD) was the first to use the term concussion and advised surgery for penetrating wounds of the skull and removal of depressed fractures.In Europe, Teodorico de Cervia (1205-1298), Jean Louis Petit (1674-1750) defines the compression of the brain as a cause of drowsiness. Victor Horsley (1857-1916) hypothesized that trepanations were carried out to treat secondary focal epilepsy in comminuted fractures and subsidence that compressed the
2primary motor cortex.In 1974 Bryan Jennett, describes the Glasgow Coma Scale
3(GCS). Epidemiology.Cranioencephalic Trauma (TBI); it is one of the most frequent trauma conditions in prehospital and hospital care. Worldwide, 1.2 million people die annually from TBI and 20 to 50 million
14
SUMMARY.The recurrence rate in chronic subdural hematomas is estimated to be broad and variable from 5 to 30%, depending on the established recurrence criteria described over the years.Patients with this pathology are usually older than 70 years and some of them with other comorbidities. A new exposure to neurosurgical and anesthetic procedures could overshadow their prognosis.Objective: To identify the incidence of recurrence in patients who underwent surgery for acute, chronic and epidural subdural hematomas and their possible triggering causes at Hospital de Traumatología IMSS "Dr. Victorio de la Fuente Narváez", Instituto Mexicano del Seguro Social, Mexico City. Material and Methods: A retrospective review of neurosurgical procedures during one year was carried out. Acute and Chronic and Epidural Subdural hematomas were selected and those patients who were diagnosed as Chronic Recurrent Subdural Hematomas were identified. Preoperative and postoperative Simple Skull Tomography (CT) was reviewed; diameter and thickness of the hematoma, volume, displacement of the midline, comorbidities, age, and anesthetic technique used were measured.Results: A total of 424 neurosurgical procedures were obtained, of which 306 patients were male (72.16%) and 88 female patients (20.7%). Among the most frequent procedures were Chronic Subdural Hematoma, with 250 patients, corresponding to 59%, Acute Subdural Hematoma with 60 patients, 14.15%. The neurosurgical resolution that prevailed was single or bilateral trephine evacuation with 72.6% (225) and secondly the craniotomy with 27.4% (85 patients).Conclusions: The present study shows that chronic subdural hematomas are the most frequent pathology at Hospital Traumatología “Dr. Victorio de la Fuente Narvaez” IMSS, the rate of recurrence is low, even below the ranges described in other countries. However, work should be focused on the findings obtained in order to reduce or even eradicate the appearance of recurrent chronic subdural hematomas, mainly due to the decrease in the prognosis of these patients who are generally elderly adults.Key words: Cranioencephalic Trauma, chronic subdural hematomas, Chronic Recurrent Subdural Hematomas, neurosurgical patient.
Dra. Alma Edith Gress MendozaServicio de Anestesiología y Neuroanestesiología Hospital de Traumatología “Magdalena de las Salinas”Unidad Médica de Alta Especialidad “Dr. Victorio de la Fuente Narváez”Instituto Mexicano del Seguro [email protected]. Michael Herbas RochaMédico NeurocirujanoCirugía en Epilepsia y FuncionalHospital de Traumatología “Magdalena de las Salinas”Unidad Médica de Alta Especialidad“Dr. Victorio de la Fuente Narváez”Instituto Mexicano del Seguro Social
INCIDENCE OF RECURRENCE OF THE CHRONIC SUBDURAL
HEMATOMAS AT HOSPITAL IMSS TRAUMATOLOGÍA “DR.
VICTORIO DE LA FUENTE NARVÁEZ”
In regard to non-fatal injuries, a significant percentage of survivors have important consequences that will prevent or hinder their return and readjustment to their previous activities.
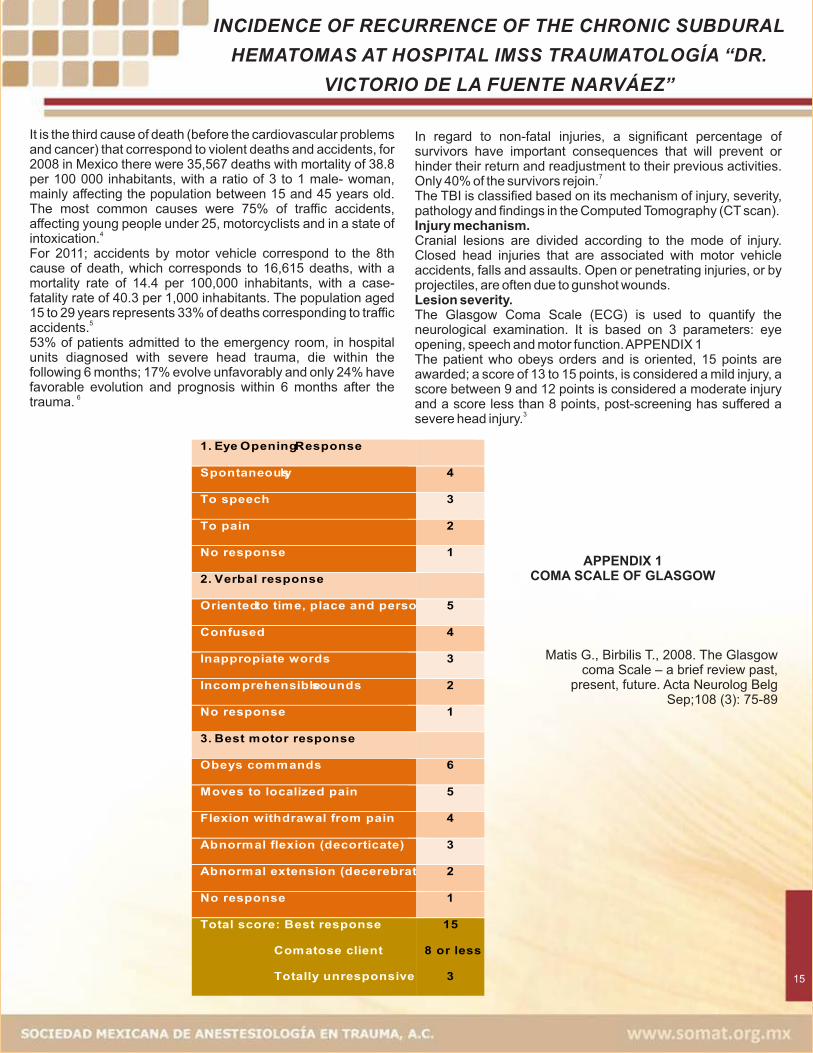
7Only 40% of the survivors rejoin.The TBI is classified based on its mechanism of injury, severity, pathology and findings in the Computed Tomography (CT scan). Injury mechanism.Cranial lesions are divided according to the mode of injury. Closed head injuries that are associated with motor vehicle accidents, falls and assaults. Open or penetrating injuries, or by projectiles, are often due to gunshot wounds.Lesion severity.The Glasgow Coma Scale (ECG) is used to quantify the neurological examination. It is based on 3 parameters: eye opening, speech and motor function. APPENDIX 1The patient who obeys orders and is oriented, 15 points are awarded; a score of 13 to 15 points, is considered a mild injury, a score between 9 and 12 points is considered a moderate injury and a score less than 8 points, post-screening has suffered a
3severe head injury.
15
It is the third cause of death (before the cardiovascular problems and cancer) that correspond to violent deaths and accidents, for 2008 in Mexico there were 35,567 deaths with mortality of 38.8 per 100 000 inhabitants, with a ratio of 3 to 1 male- woman, mainly affecting the population between 15 and 45 years old. The most common causes were 75% of traffic accidents, affecting young people under 25, motorcyclists and in a state of
4intoxication.For 2011; accidents by motor vehicle correspond to the 8th cause of death, which corresponds to 16,615 deaths, with a mortality rate of 14.4 per 100,000 inhabitants, with a case-fatality rate of 40.3 per 1,000 inhabitants. The population aged 15 to 29 years represents 33% of deaths corresponding to traffic
5accidents.53% of patients admitted to the emergency room, in hospital units diagnosed with severe head trauma, die within the following 6 months; 17% evolve unfavorably and only 24% have favorable evolution and prognosis within 6 months after the
6trauma.
APPENDIX 1COMA SCALE OF GLASGOW
1. Eye Opening Response
Spontaneously 4
To speech 3
To pain 2
No response 1
2. Verbal response
Oriented to time, place and person 5
Confused 4
Inappropiate words 3
Incomprehensible sounds 2
No response 1
3. Best motor response
Obeys commands 6
Moves to localized pain 5
Flexion withdrawal from pain 4
Abnormal flexion (decorticate) 3
Abnormal extension (decerebrate) 2
No response 1
Total score: Best response
Comatose client
Totally unresponsive
15
8 or less
3
Matis G., Birbilis T., 2008. The Glasgow coma Scale – a brief review past,
present, future. Acta Neurolog Belg Sep;108 (3): 75-89
INCIDENCE OF RECURRENCE OF THE CHRONIC SUBDURAL
HEMATOMAS AT HOSPITAL IMSS TRAUMATOLOGÍA “DR.
VICTORIO DE LA FUENTE NARVÁEZ”
known as burned motor oil. The blood within the subdural space evokes the inflammatory response. As the days go by, the fibroblasts invade the clot and form neomembranes on the cortical and dural surfaces. This is followed by neocapillary formation, enzymatic fibrinolysis and liquefaction of the blood clot.Patients usually present symptoms of headache, confusion, difficulty in language or symptoms of Transient Ischemic Attack
9(TIA). The recurrence rate is significant in chronic subdural hematomas (HSC), ranging from a range of 5 to 30%. There are some criteria that define the recurrence of chronic
10subdural hematomas. Appendix 2This pathology is detected by tomography (CT) in most patients (80%), most are asymptomatic and clinically
10insignificant.The combination of the age of the population and the increase in the use of antiplatelet and anticoagulant medication has also conditioned the increase in the incidence of chronic subdural hematomas, which has increased substantially in the last 25 years.The 3 methods of evacuation of bruises are mainly: single hole by craniotomy, helical perforation by craniotomy and craniotomy. Generally the minimally invasive technique by helical hole is usually a safe and effective technique. However, a
11future study of this must be followed.
II. Study design.The general objective was to evaluate the postoperative course of patients with chronic subdural hematoma at IMSS Victorio de la Fuente Narváez Traumatology Hospital, for a period of one year, from October 2014 to September 2015, and to identify cases that rebleed; considering the incidence of recurrence of chronic subdural hematomas in a period of 1 year, the possible causes that conditioned postoperative patients of drainage of chronic subdural hematoma, presented recurrence of rebleeding, the surgical technique that was used during the initial neurosurgical procedure, as well as of the reoperation; anesthetic management was given, the comorbidities of the patients and the neurological condition of the patient's admission and during the initial procedure and its reintervention using the Glasgow coma scale.Because Chronic Subdural Hematoma (HSC) is a pathology that occurs mainly in elderly patients and is a serious clinical condition that endangers life, in addition to the different comorbidities that might occur, these patients have a higher anesthetic-surgical risk that could trigger a fatal outcome, and even more, the risk of requiring a new reoperation due to rebleeding during its postoperative evolution.To investigate the incidence of rebleeding in this type of patients is necessary.
III. Methodology.After the authorization of the teaching and research unit and the ethics committee of the hospital, a retrospective, analytical, longitudinal, and observational study was carried out.
16
Pathology of the injury.Injuries could be classified into 2 general groups according to their morphology: cranial fractures and intracranial lesions.Cranial fractures appear in 80% of patients with fatal injuries. The cranial vault fractures are frequently three times greater than the base of the skull (62 versus 20%). The identification of cranial fractures is important in the treatment of cranial injury due to the association with intracranial hematomas, cerebrospinal fluid (CSF) fistulas and infection.Intracranial injuriesThey are generally classified as focal and diffuse, both types could exist. The mortality rate is generally higher in focal lesions (39%) than diffuse lesions (24%).The epidural hematoma is located between the skull and the dura mater, generally occurring in 6% of patients with severe closed head injuries. One third of patients are unconscious at the time of the injury; It is frequently associated with cranial fracture (91% adults, 75% in children).The blood comes from the section of dural vessels, usually arterial, fractured cranial bone and occasionally sectioned venous sinuses. In the CT the epidural hematoma is characterized by a biconvex, hyperdense lesion.Subdural hematoma is the most frequent focal intracranial lesion. The hematoma is located between the dura mater and the brain, being a consequence generally of the section of the bridge veins, located between the cortex and the drainage sinuses. The acute subdural hematoma that is observed after 72 hours of the TBI is seen in the CT as a hyperdense and homogeneous mass in the form of a half moon and parallel to the calotte. The mortality rate is high; 50%, depending on several factors such as age, time from injury and treatment time, pupillary abnormalities, score admission ECG, CT findings, intracranial pressure (ICP) during and postoperative and type of surgery.CT can yield predictive data such as thickness of the hematoma, displacement of the midline, present swelling or underlying cerebral concussion.The survival rate is 50% for a bruise with a thickness of 18 mm and a mean line displacement of 20 mm. The survival is 0% when the displacement of the median line is greater than 25 mm.Subdural hematoma could be sorted by time of evolution: acute are those presented in the first 72 hours, subacute between 3 and 4 weeks and chronic after 3 weeks to 4 months.In the subdural hematomas a reduction of the cerebral blood flow has been observed, below the ischemic threshold and a
8marked decrease of the cerebral oxygenation.Chronic subdural hematomas (CSDH) usually occur in adulthood, with an average age of 63 years. Cranial trauma is identified in less than 50% of cases (often in relation to trivial contusions). Other risk factors identified are: alcohol abuse, seizures, ventriculoperitoneal shunts, coagulopathies (including therapeutic anticoagulation), and patients with risk of falling (for example, previous hemiplegia due to EVC). CSDHs are bilateral in 20 to 25% of cases.The thickness of the bruises tend to be greater in elderly patients because the weight of the brain decreases and the subdural space increases.Generally, content of the Chronic Subdural Hematoma is a fluid
INCIDENCE OF RECURRENCE OF THE CHRONIC SUBDURAL
HEMATOMAS AT HOSPITAL IMSS TRAUMATOLOGÍA “DR.
VICTORIO DE LA FUENTE NARVÁEZ”
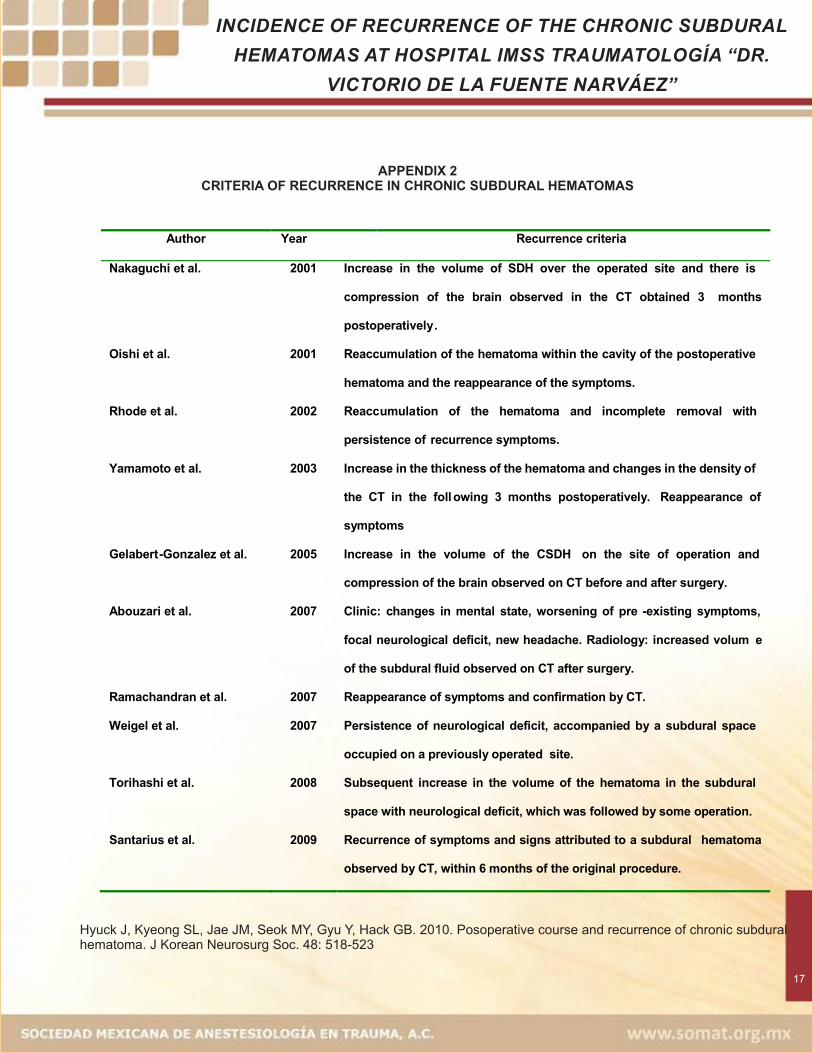
Hyuck J, Kyeong SL, Jae JM, Seok MY, Gyu Y, Hack GB. 2010. Posoperative course and recurrence of chronic subdural hematoma. J Korean Neurosurg Soc. 48: 518-523
17
APPENDIX 2CRITERIA OF RECURRENCE IN CHRONIC SUBDURAL HEMATOMAS
Author Year Recurrence criteria
Nakaguchi et al. 2001 Increase in the volume of SDH over the operated site and there is
compression of the brain observed in the CT obtained 3 months
postoperatively.
Oishi et al. 2001 Reaccumulation of the hematoma within the cavity of the postoperative
hematoma and the reappearance of the symptoms.
Rhode et al. 2002 Reaccumulation of the hematoma and incomplete removal with
persistence of recurrence symptoms.
Yamamoto et al. 2003 Increase in the thickness of the hematoma and changes in the density of
the CT in the foll owing 3 months postoperatively. Reappearance of
symptoms
Gelabert-Gonzalez et al. 2005 Increase in the volume of the CSDH on the site of operation and
compression of the brain observed on CT before and after surgery.
Abouzari et al. 2007 Clinic: changes in mental state, worsening of pre -existing symptoms,
focal neurological deficit, new headache. Radiology: increased volum e
of the subdural fluid observed on CT after surgery.
Ramachandran et al. 2007 Reappearance of symptoms and confirmation by CT.
Weigel et al. 2007 Persistence of neurological deficit, accompanied by a subdural space
occupied on a previously operated site.
Torihashi et al. 2008 Subsequent increase in the volume of the hematoma in the subdural
space with neurological deficit, which was followed by some operation.
Santarius et al. 2009 Recurrence of symptoms and signs attributed to a subdural hematoma
observed by CT, within 6 months of the original procedure.

INCIDENCE OF RECURRENCE OF THE CHRONIC SUBDURAL HEMATOMAS AT HOSPITAL IMSS TRAUMATOLOGÍA “DR.
VICTORIO DE LA FUENTE NARVÁEZ”
The database registered in the operating room area at IMSS Traumatology Hospital Victorio de la Fuente Narváez was reviewed consecutively from October 2014 to September 2015; the neurosurgical procedures performed during this period were identified, the diagnoses of chronic subdural hematomas admitted for drainage of hematoma were selected either by surgical technique single or double trepanation, and / or bilateral, craniotomy and / or craniectomy; patients who during the postoperative course were registered as a recurrent hematoma were selected.Selected records were thoroughly investigated and age, gender, comorbidities, trauma mechanism, Glasgow Coma Scale of admission, pre-surgical diagnosis, pre-surgical tomography images, recorded by simple tomography of the skull, thickness, density and presence of membranes were recorded. In its interior in preoperative and post-operative images of control, postoperative diagnosis, type of anesthesia, surgical technique used, Glasgow coma graduation scale, floor medication.
IV. Results and analysis.A retrospective review of the neurosurgical procedures performed during 1 consecutive year was carried out, during the period from October 2014 to September 2015.A total of 424 neurosurgical procedures were obtained, 306 of them corresponded to male (72.16%) and 88 to female patients (20.7%). Appendix 3
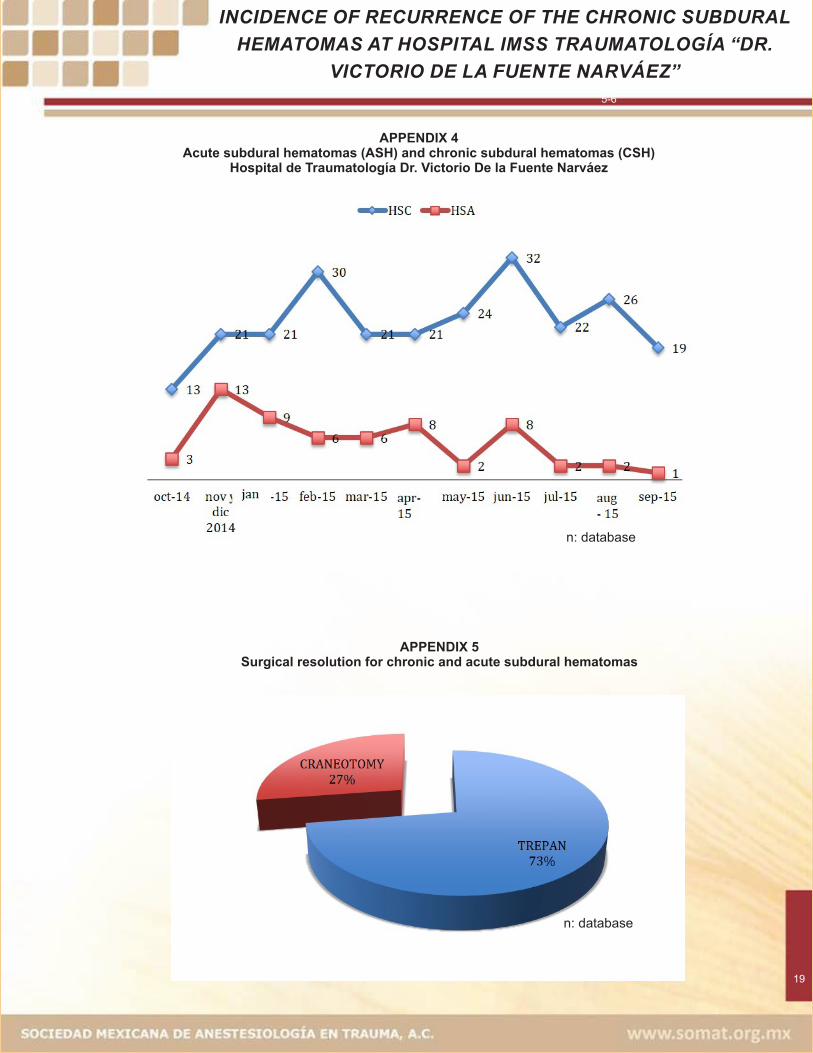
Among the most frequent procedures were the Chronic Subdural Hematoma, with 250 patients, corresponding to 59%, the acute Subdural Hematoma with 60 patients, i.e., 14.15%. Appendix 4.
Epidural Hematoma was recorded in 31 patients (7.3%) and other procedures (decompressive craniectomy secondary to severe cerebral edema due to severe head trauma, hydrocephalus requiring ventriculostomy placement and / or ventriculoperitoneal shunt system, esquislectomies, sunken fracture survey , cranialization) 85 patients, corresponding to 20%.Within the subdural hematomas, we classified them only as chronic subdural hematoma and acute subdural hematomas, registering a total of 310 patients (73.1%).The surgical procedure of these patients was recorded as follows: 225 patients underwent surgery by trepanation (72.6%), either single or double. 85 patients were solved by craniotomy (27.4%).Ten patients presented recurrent chronic subdural hematoma, which corresponded to 4% of the total of chronic subdural hematomas with median age of 66.5 years, and maximum value of 92 years and the lowest of 33 years.The most frequent comorbidities were alcoholism 7%, diabetes mellitus type II (DMTII) with 4%, hypertension systemic (HAS) 2%, smoking 4% and others such as Parkinson's, hyperazoemia, varicose ulcer, etc. 3%. All laboratories were within normal parameters.The time of evolution of the initial diagnosis and the formation of a new hematoma ranged from 3 to 120 days, with a MEDIA of 4 and HARMONIC MEDIA of 4.2. The shortest time was 3 days and the maximum time was 120 days. The initial surgical resolutions in 9 procedures were drainage of hematoma by trephines and one of initial form by craniotomy; during the second surgical time the surgical technique chosen was craniotomy and in one case a third intervention was performed by craniotomy for membranectomy. Appendix 5.
18
APPENDIX 3Surgeries registered during the period October 2014 to September 2015
n: database
CSH= Chronic subdural hematomas.ASH= Acute subdural hematomas.Epidural H= Epidural hematomas
INCIDENCE OF RECURRENCE OF THE CHRONIC SUBDURAL
HEMATOMAS AT HOSPITAL IMSS TRAUMATOLOGÍA “DR.
VICTORIO DE LA FUENTE NARVÁEZ”
19
6-75-6
APPENDIX 4Acute subdural hematomas (ASH) and chronic subdural hematomas (CSH)
Hospital de Traumatología Dr. Victorio De la Fuente Narváez
n: database
APPENDIX 5Surgical resolution for chronic and acute subdural hematomas
n: database
INCIDENCE OF RECURRENCE OF THE CHRONIC SUBDURAL HEMATOMAS AT HOSPITAL IMSS TRAUMATOLOGÍA “DR.
VICTORIO DE LA FUENTE NARVÁEZ”
The average MEDIUM of the Glasgow Coma Scale was 14. The ECG score range was 9 for the lowest and highest 15.As for the simple tomography of the skull, all the patients who underwent surgery had predominant characteristics such as a hematoma greater than 18 mm in thickness. The displacement of the midline occurred in 2 patients. Appendix 6.Reinterventions were frequent on the third postoperative day, in 2 cases recurrent subdural hematoma was diagnosed after 3 months of resolution and in this case the patient has a history of chronic alcoholism; the second patient was operated 3 times for resolution and the formation of membranes inside was proposed as a possible cause. DISCUSSION.Few studies have been conducted looking for specific modifiers in the neurosurgical patient. Gonzaga Juarez reported a review study in which they evaluated the risk factors in geriatric patients undergoing neurosurgical procedures identifying specific modifiers influencing the choice of diagnostic tests and
12specific therapies useful for the preoperative preparation.The postoperative course of Chronic Subdural Hematomas was resolved or recurrent. In our review study, from the total of patients submitted to drainage of chronic subdural hematomas, 4% of recurrence is presented requiring a new surgical intervention.
Some authors describe an approximate range of 5 to 30% of recurrence, that even after a 1-month resolution a liquefied hematoma encapsulated by membranes appears.I t is important to consider the difference between reaccumulation and incomplete removal since it is very difficult for some authors to establish this difference.The presence of chronic degenerative diseases such as diabetes mellitus type II, systemic arterial hypertension, dyslipidemias, alcoholism and chronic smoking were the most frequent comorbidities in patients who presented the diagnosis of recurrence, however other diseases such as Parkinson's disease, varicose ulcers, hyperazoemia, hyperkalemia and hyponatremia were reported in these patients.Popularity and use of minimally invasive techniques are increasing. This type of techniques could be used without general anesthesia and in the head.Some review studies establish that single trepanation is a better surgical technique for the evacuation of chronic subdural hematoma compared to double trepanation. In our study, trepanation was the predominant technique for drainage of hematoma with 72.6% and craniotomy 27.4%.The anesthetic method that prevailed was general anesthesia
6-1199.5% and only local anesthesia with 0.6% of the procedures.
20
APPENDIX 6
PREOPERATIVE AND POSOPERATIVE TOMOGRAPHY
A. Tomography study in a simple phase of the axial cut skull in which isodense image is observed with respect to the cerebral parenchyma, located in the subdural space with right frontoparietal extension, compatible with subdural hematoma in chronic stage that causes subfacial hernia. Peripheral hyperdensities are noticeable in their interior in relation to visceral and parietal membranes as well as intralesional septa. B. Image of simple skull tomography of postoperative control, with complete resolution of the lesion using a single craniotomy technique.

INCIDENCE OF RECURRENCE OF THE CHRONIC SUBDURAL HEMATOMAS AT HOSPITAL IMSS TRAUMATOLOGÍA “DR.
VICTORIO DE LA FUENTE NARVÁEZ”
CONCLUSIONS.The postoperative course of the patients submitted to the neurosurgical procedure at Hospital Traumatología IMSS, Dr. Victorio de la Fuente Narvaez, was evaluated over a period of one year, until chronic subdural hematomas recurred.Characteristic images were identified that were present in the majority of the patients with a diagnosis of recurrent chronic subdural hematoma by Computed Tomography of the Skull, such as the thickness of the hematoma and displacement of the midline, but which nevertheless require a more thorough review to establish possible predisposing factors of recurrence in a major population revision in the future.The surgical technique of choice for the initial treatment was minimal invasion by trepanation and, craniotomy as a second option. Balanced general anesthesia prevailed.Although chronic subdural hematomas are predominant in elderly patients, they could occur to a lesser extent in young patients and in the same way they might overshadow the prognosis according to their comorbidities. Alcoholism was the most common comorbidity in them.The study has limitations because it is retrospective; however, some of the established objectives were met and the rest is proposed to perform a more extensive review to capture a greater number of samples or to start a prospective study that could allow to closely monitor the neurosurgical patient and reduce at the maximum the possibility of recurrence in chronic subdural hematomas.
BIBLIOGRAPHY.1. Narayan RK; Michel ME; Ansell B; Baethmann A;
Biegon A; Bracken MB; Bullock MR. 2002. Clinical trialsin head injury. J Neurotrauma;19 (5): 503-557
2. Rubiano A., Pérez R. 2008. Neurotrauma yneurointensivismo. En: Peña Q. Rubiano A. Reseñahistórica del trauma craneoencefálico. BogotáColombia. DISTRIBUNA. Cap 3.
3. Matis G., Birbilis T., 2008. The Glasgow coma Scale – abrief review past, present, future. Acta Neurolog BelgSep;108 (3): 75-89
4. Sistema Nacional de Vigilancia Epidemiológica. SSA,2014 No. 26, vol. 25
5 . http://www.cenetec.salud.gob.mx/descargas/gpc/CatalogoMaestro/016_GPC_TCEenelAdulto/SSA_016_08_EyR.pdf
6 . https://www.braintrauma.org/pdf/protected/Guidelines_Management_2007w_bookmarks.pdf
7. González Villavelázquez ML, García González A.Traumatismo craneoencefálico. Rev Mex Anest2013;;36(Supl. 1):S186-S193
8. Greenberg MS. 2010. Handbook of Neurosurgery. Ensu: Head trauma. Seventh Edition. Florida. THIEME.pag: 899-901.
9. Cottrel J. Young W. 2010. Cotrell and Young´sNeuroanesthesia. En: Bendo A. Perioperativemanagement of adult patients with severe head injury.5ta edición, Philadelphia. MOSBY ELSEVIER. pag:317-325.
10. Hyuck J, Kyeong SL, Jae JM, Seok MY, Gyu Y, HackGB. 2010. Posoperative course and recurrence ofchronic subdural hematoma. J Korean Neurosurg Soc.48: 518-523
11. Chari A, Kolias A, Santarius T, Bond S, Hutchinson P.2014. Twist-drill craniostomy with hollow screws forevacuation of chronic subdural hematoma. JNeurosurg. 121:176-183
12. Gonzaga R., Juárez. 2010. Factores de riesgo en elpaciente geriátrico sometido a neurocirugía. RevistaMexicana de Anestesiología. 33 (1): S99-S100.
21
NORMAS PARA LOS AUTORES
El Boletın SOMAT es una publicacion de la Sociedad Mexicana de Anestesiologıa en Trauma, A.C. digital, bimensual.
Publicara contribuciones de las secciones que abajo se indican escritas en Arial 12 puntos, 1.5 espacio, margenes de 2.5 cm, sin sangrıa ni justi�icacion derecha. Todos los escritos seran evaluados por pares.I. Editoriales. Escrito por el editor o editores invitados.II. Trabajos cientı�icos (investigacion).III. Trabajos de revisionIV. Reporte de casos clınicosV. Perlas en el manejo del paciente con traumaVI. Evaluacion de casosVII. Aspectos legales, eticos-bioeticos, riesgos profesionales del profesional de la saludVIII. Historia, arte en la medicinaIX. Polıticas de saludX. Cartas al editor*** Originales en espanol e ingles en el ambito de las especialidades medicas (anestesiologıa , medicina crıtica, urgencias medico quirurgicas, trauma y ortopedia, cirugıa general, rehabilitacion, neurocirugıa, imagenologıa), enfermerıa, medicina prehospitalaria relacionadas al manejo del pacientetraumatizado y/o en estado crıt ico en particular y de otras areas en general.Todos los artıculos deberan contar con una pagina inicial:1. Tıtulo en espanol e ingles
2. Tıtulo breve en espanol e ingles
3. Nombre del autor (es) y cargos institucionales
4. Nombre, adscripcion, telefono, direccion postal, correo electronico del autor principal y contacto y para correspondencia
5. Resumen en espanol e ingles. Maximo media cuartilla.Palabras clave en espanol e ingles (se recomienda revisar Descripcion en Ciencias de la Salud (DECS,http://decs.bus.br/E/homepage.htm) y del MedicalS u b j e c t H e a d i n g s d e l I n d e x M e d i c u s(http://www.nlm.nih.gov/mesh/).
5.1 Trabajos cientı�icos de investigacion. El resumen contara con:* Antecedentes* Material y metodos* Resultados* Conclusiones
5.2 Trabajos de revision / Historia o Arte de laMedicina / Aspectos Legales, E� ticos-Bioeticos, Riesgos Profesionales del Profesional de la Salud.El resumen sera en extenso
5. 3 Casos clınicosEl resumen sera en extenso
6. Desarrollo del trabajo (artıculo)Posterior al resumen y palabras clave:
6.1 Cientı�icos / Investigacion- Introduccion o antecedentes- Material y Metodos- Resultados- Conclusiones- Bibliografıa
6.2 Trabajos de Revision- Cuadro de contenido- Cuerpo del manuscrito:--- Introduccion--- Antecedentes--- Desarrollo del tema- Bibliografıa
6.3 Caso Clın ico- Introduccion- Reporte o descripcion del caso- Discusion- Conclusiones- Bibliografıa
6.4 Evaluacion de Casos- Antecedentes- Datos clınicos del paciente- Preguntas diagnostico y manejo- Respuestas- Resumen patologıa , diagnostico y manejo- Bibliografıa
7. Fuentes de �inaciamiento en su caso
8. Posible con�licto de interes de los autores (en sucaso)
9. Bibliografıa.Las referencias de artıculos publicados de revistas, capıtulos de libros y libros completos se referiran deacuerdo al estilo Vancouver (www.icmje.org). 22
NORMAS PARA LOS AUTORES
Se indicara arabigamente y en forma consecutiva de acuerdo a la aparicion en el texto.a) Revistas periodicasKern SE, Xie G, White JL, Egan TD. A response surface analysis of propofol-remifentanyl pharmacodynamic interaction involunters. Anesthesliology 2004;100;1373-81 Referir el doi
b) Capıtulos de libros.Hoffman BB, Le antagonists. In: The Pharmacological Basis of Therapeutics. 8a Edition. Eds. Gilman AG, Rail TW, Nies AS. New York: Pergamon Press, 1990:229-43
c) Libros completos.Boiselle PM, McLoud TC, Abbot GF. Thoracic imaging: case review. Philadelphia: Elsevier Mosby, 2001d) Libros y artıculos en internet. Agregar la fechaconsultada, disponible en http://www..... y el doi...10. Cuadros y �igurasUna por pagina, poniendo pie del cuadro o �igura. Si es de alguna revista o libro poner de donde se tomo y pedir la autorizacion del autor o editorial para publicacion.E n v i a r t o d o s l o s a r t ı c u l o s d i r i g i d o s a [email protected] en atencion a Dr. Jaime Rivera Flores Editor del Boletın SOMAT.
23
GUIDELINES AUTHORS
SOMAT Newsle�er is a bimonthly digital publica�on of the
Sociedad Mexicana de Anestesiología en Trauma, A.C.
SOMAT Newsle�er accepts the following types of manuscripts, in
Arial font size 12 points, 1.5 spacing and 2.5 cm margins, with no
indenta�on or right jus�fica�on. All manuscripts will be peer
reviewed.
I. Editorials. Wri�en by the editor or guest editors.
II. Scien�fic works (research).
III. Review papers
IV. Clinical cases
V. Pearls in management of pa�ent with trauma
VI. Case evalua�on
VII. Legal, ethical-bioethical aspects, professional risks of the
health professional
VIII. History, art in medicine
IX. Health policies
X. Le�ers to the editor
*** Original texts in Spanish and English in medical special�es
(anesthesiology, cri�cal medicine, medical surgical emergencies,
trauma and orthopedics, general surgery, rehabilita�on,
neurosurgery, imaging), nursing, medicine prehospital care
related to pa�ent management trauma�zed and / or cri�cally ill in
par�cular and of other areas in general.
All manuscripts should have the following sec�ons:
Title page:
1. Original �tle in Spanish and English
2. Running �tle in Spanish and English
3. Authors' name and affilia�on
4. Correspondence author: Name, affilia�on, telephone, postal
address and e-mail.
5. Summary: in Spanish and English. Maximum half page.
Keywords: in Spanish and English (it is recommended to review the
D e s c r i p � o n i n H e a l t h S c i e n c e s ( D E C S ,
h�p://decs.bus.br/E/homepage.htm) and Medical Subject
H e a d i n g s f r o m i n d e x m e d i c u s
( ).h�p://www.nlm.nih.gov/mesh/
Summaries should follow the sequence of the main body of the
text:
5.1. Scien�fic research manuscripts:
* Background
* Material and methods
* Results
* Conclusions
5.2. Review manuscripts / History or Art of the
Medicine / Legal Aspects, Ethics-Bioethics, Professional Risks of the
Health Professional.
Summary should be in extenso.
5.3. Clinical cases
Summary should be in extenso.
6. Manuscript prepara�on
The following requirements should be fulfilled a�er the summary
and keywords:
6.1 Scien�fic / Research papers
- Introduc�on or background
- Material and methods
- Results
- Conclusions
- Bibliography
6.2 Review manuscripts
- Table of contents
- Manuscript:
--- Introduc�on
--- Background
--- Development
- Bibliography
6.3 Clinical Case
- Introduc�on
- Report or descrip�on of the case
- Discussion
- Conclusions
- Bibliography
6.4 Case Evalua�on
- Background
- Clinical data of the pa�ent
- Diagnos�c and management ques�ons
- Answers
- Summary pathology, diagnosis and management
- Bibliography
7. Funding sources and conflict of interest declara�ons.
8. Bibliography
References to ar�cles published in journals, book chapters and
complete books should follow the standards indicated by the
Interna�onal Commi�ee of Medical Journal Editors, Vancouver style
(www.icmje.org), each of them numbered and ordered
sequen�ally as they appear in the text with consecu�ve Arabic
numerals.
Example:
a) Periodical journals
Kern SE, Xie G, White JL, Egan TD. A response surface analysis of
propofol-remifentanyl pharmacodynamics involunters interac�on
Anesthesliology 2004;100;1373-81 Refer the doi
b) Book chapters.
Hoffman BB, Le antagonists. In: The Pharmacological Basis of
Therapeu�cs. 8th Edi�on. Eds. Gilman AG, Rail TW, Nies AS. New
York: Pergamon Press, 1990:229-43
24
GUIDELINES AUTHORS
c) Complete books.
Boiselle PM, McLoud TC, Abbot GF. Thoracic imaging: case review
Philadelphia: Elsevier Mosby, 2001
d) Books and ar�cles on the internet:
Kern SE, Xie G, White JL, Egan TD. A response surface analysis of
propofol-remifentanyl pharmacodynamics involunters interac�on
A n e st h e s l i o l o g y 2 0 0 4 ; 1 0 0 ; 1 3 7 3 - 8 . Ava i l a b l e f ro m :
h�p://anesthesiology.pubs.asahq.org/ar�cle.aspx?ar�cleid
=1943590
9. Artwork and figures
One figure per page and with a “descrip�ve legend” for each one is
required. If it was taken from another journal or book, a le�er of
approval for its use must be a�ached.
All submissions should be sent to SOMAT Newsle�er:
[email protected] in a�en�on to Jaime Rivera Flores
MD Editor.
25