Embed Size (px)
Citation preview
HEALTH FINANCING IN D.I. YOGYAKARTA PROVINCE, THE
ROLE OF PUBLIC AND PRIVATE SECTOR
BONDAN AGUS SURYANTO
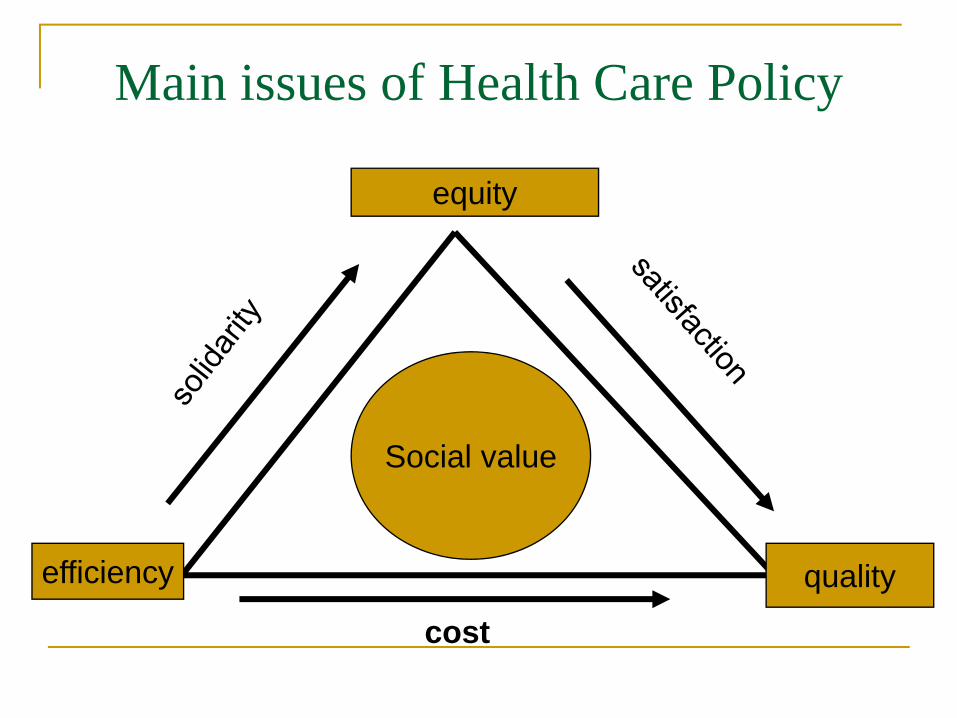
Main issues of Health Care Policy
equity
efficiency quality
cost
Social value
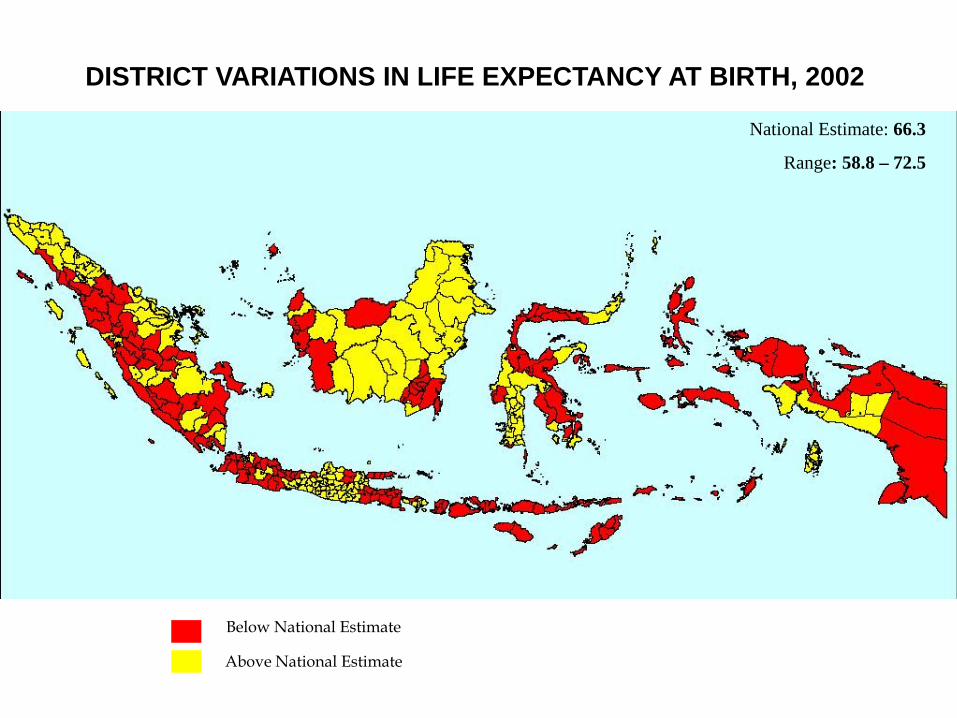
DISTRICT VARIATIONS IN LIFE EXPECTANCY AT BIRTH, 2002
Below National Estimate
Above National Estimate
National Estimate: 66.3
Range: 58.8 – 72.5
JAVA ISLAND
MAP OF YOGYAKARTA SPECIAL REGION
CENTRAL JAVA PROVINCE
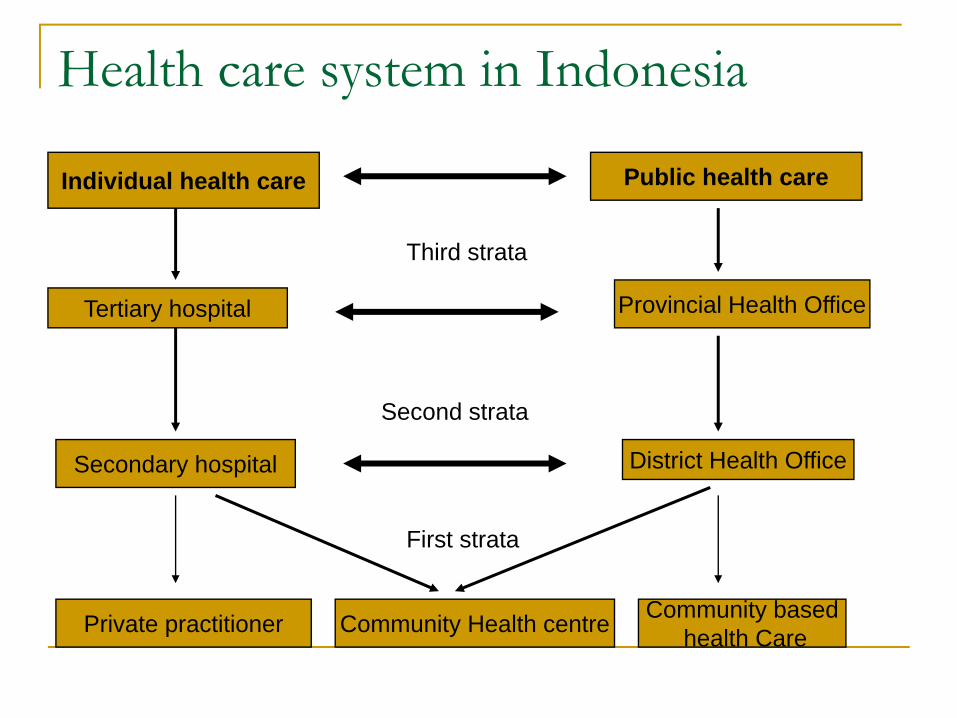
Health care system in Indonesia
Individual health care Public health care
Tertiary hospital
Secondary hospital
Private practitioner Community Health centre
Provincial Health Office
District Health Office
Third strata
Second strata
First strata
Community basedhealth Care
Which one will be dominant role in health care: the government or private sector ?
The availability of government resources: budget, Human resources, hospital, health center etc.Economic level of the population and the number of the poorThe number of Private Facilities and Private health workers. The coverage of health insurance: social and privateMarket system or wellfare system, Is it fit to overall national system?
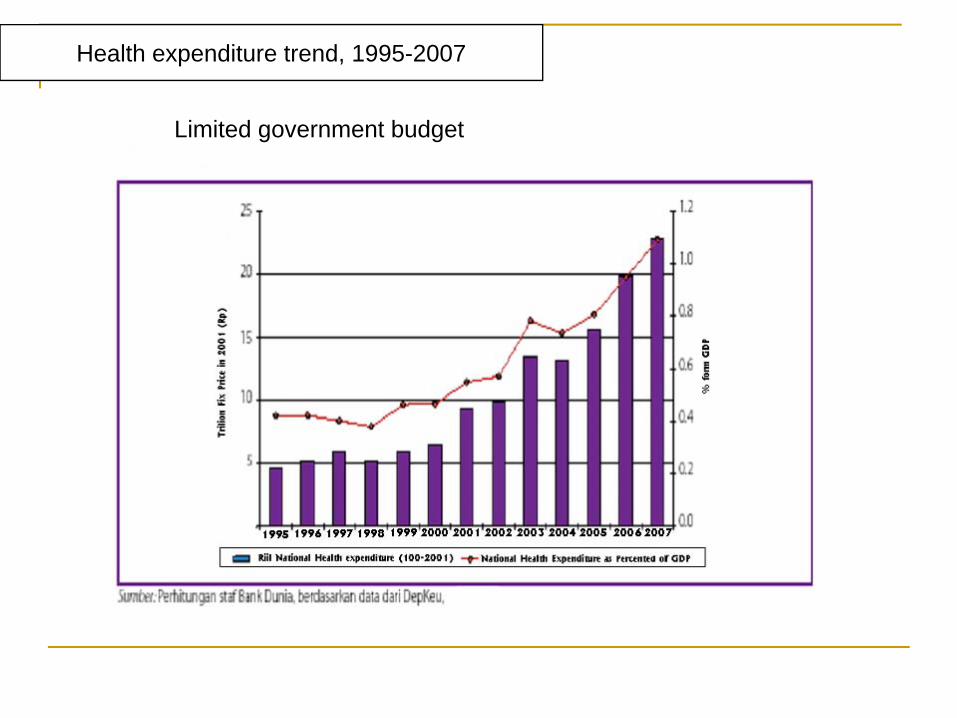
Health expenditure trend, 1995-2007
Limited government budget
2010 National Target
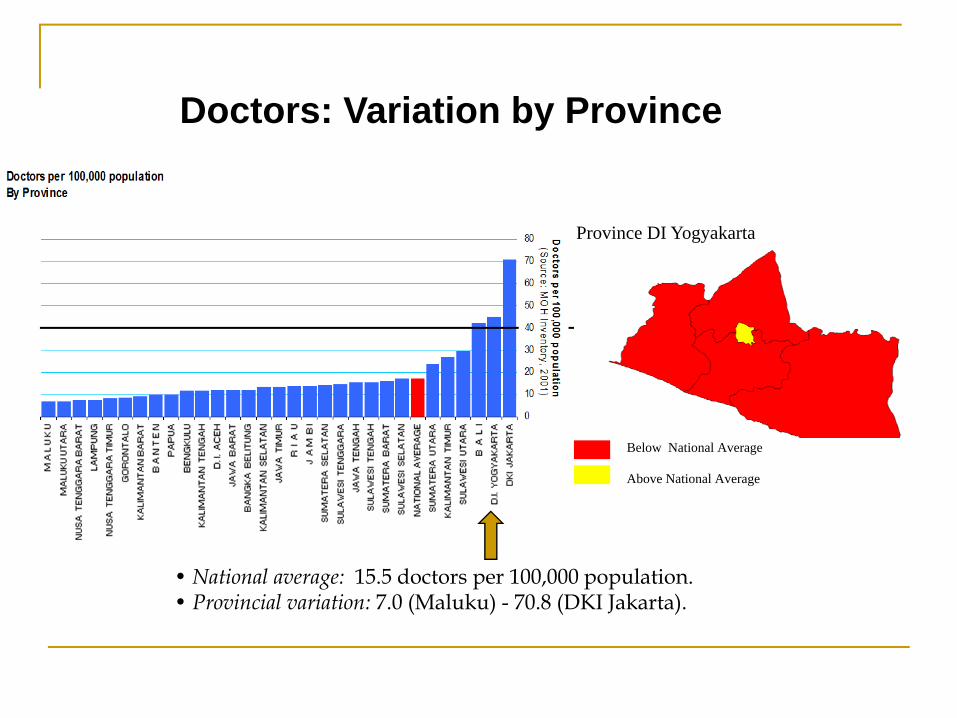
• National average: 15.5 doctors per 100,000 population.• Provincial variation: 7.0 (Maluku) - 70.8 (DKI Jakarta).
Doctors: Variation by Province
Province DI Yogyakarta
Below National Average
Above National Average
2010 National Target
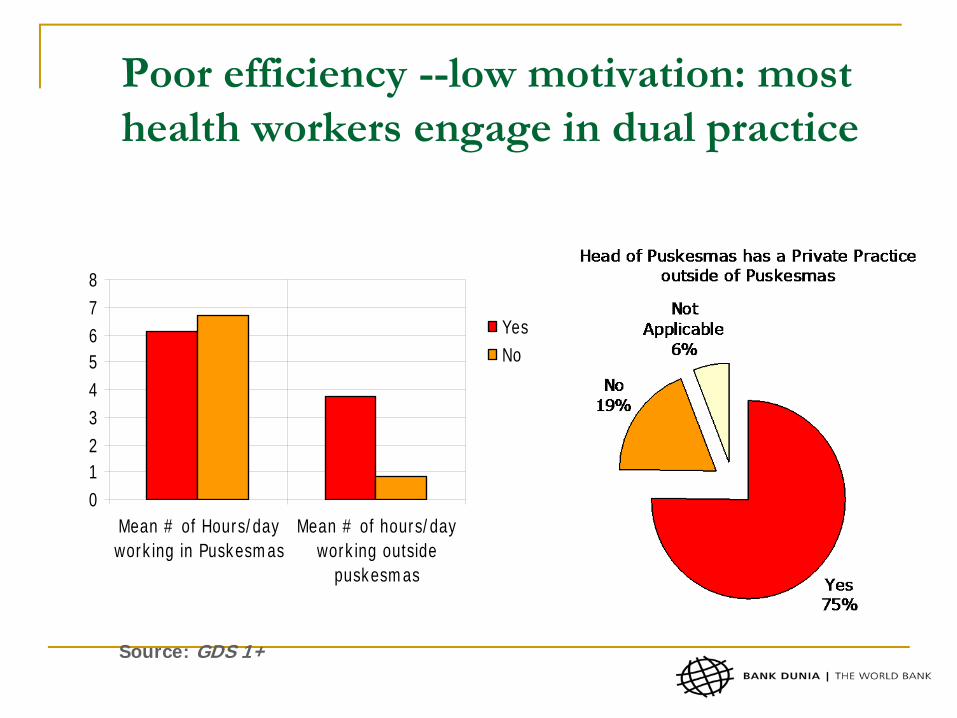
Poor efficiency --low motivation: most health workers engage in dual practice
012345678
Mean # of Hours/dayworking in Puskesmas
Mean # of hours/dayworking outside
puskesmas
YesNo
Source: GDS 1+
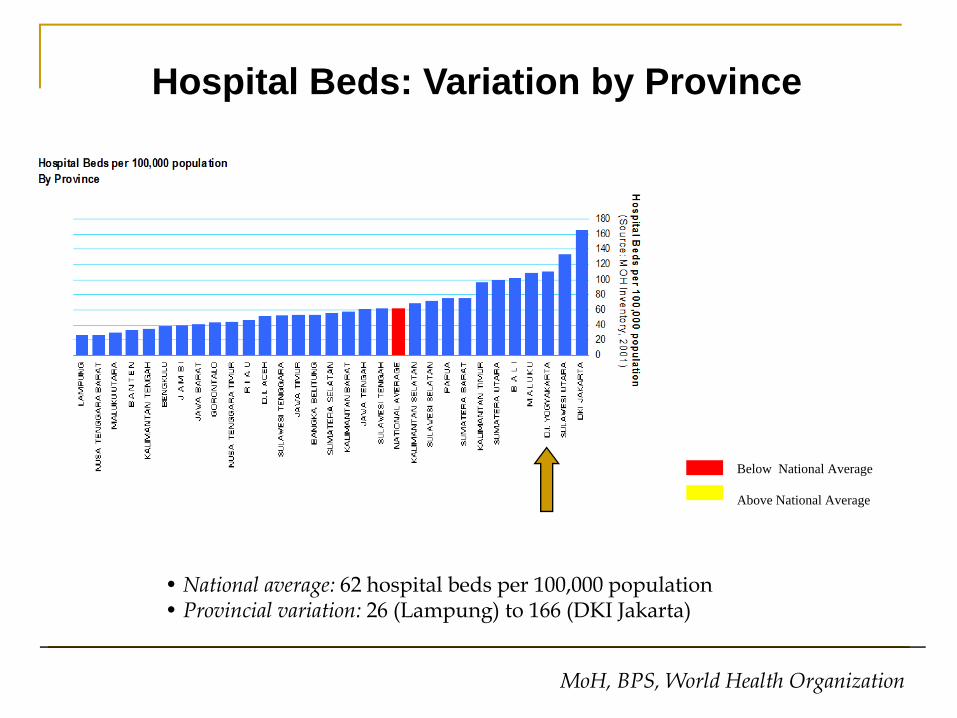
• National average: 62 hospital beds per 100,000 population• Provincial variation: 26 (Lampung) to 166 (DKI Jakarta)
Hospital Beds: Variation by Province
MoH, BPS, World Health Organization
Below National Average
Above National Average
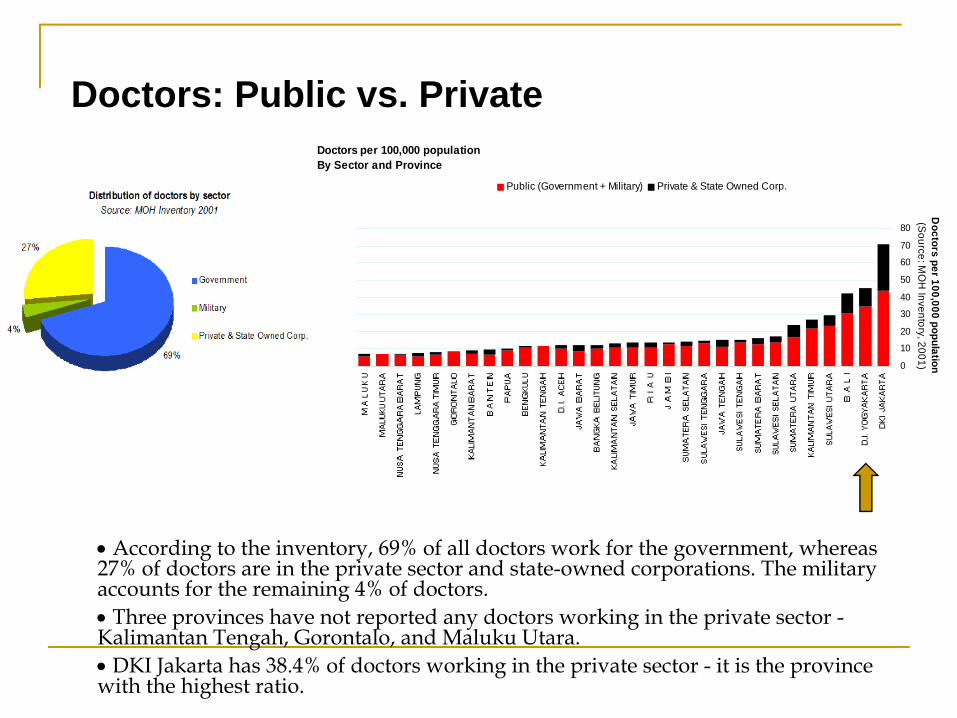
• According to the inventory, 69% of all doctors work for the government, whereas 27% of doctors are in the private sector and state-owned corporations. The military accounts for the remaining 4% of doctors.• Three provinces have not reported any doctors working in the private sector -Kalimantan Tengah, Gorontalo, and Maluku Utara.• DKI Jakarta has 38.4% of doctors working in the private sector - it is the province with the highest ratio.
Doctors: Public vs. PrivateDoctors per 100,000 populationBy Sector and Province
0
10
20
30
40
50
60
70
80
Doctors per 100,000 population(S
ource: MO
H Inventory, 2001)
Public (Government + Military) Private & State Owned Corp.
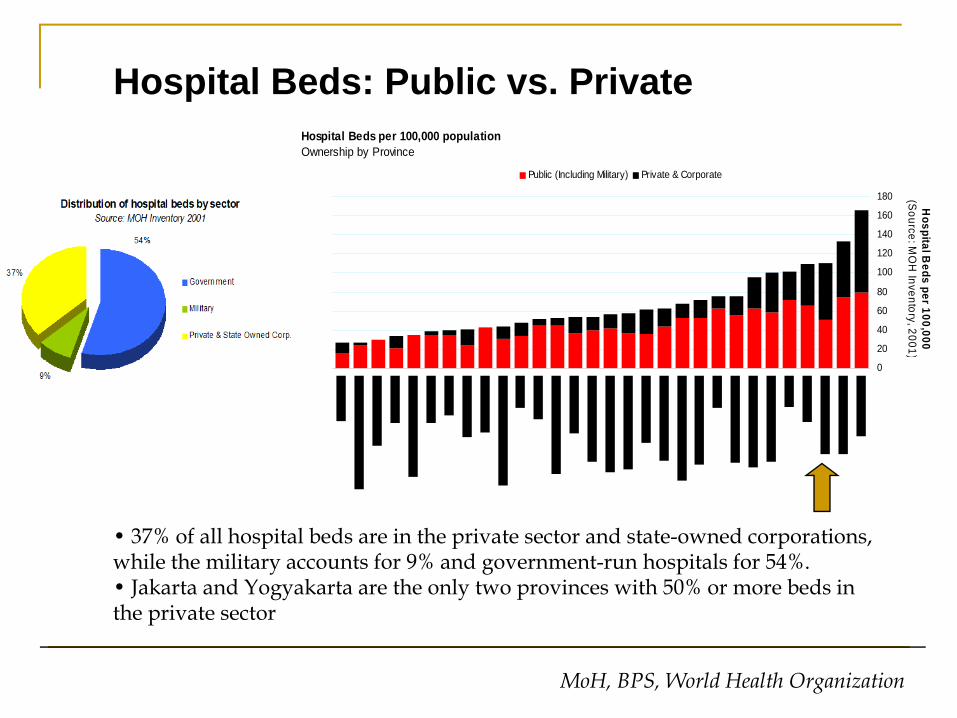
• 37% of all hospital beds are in the private sector and state-owned corporations, while the military accounts for 9% and government-run hospitals for 54%.• Jakarta and Yogyakarta are the only two provinces with 50% or more beds in the private sector
Hospital Beds: Public vs. Private
MoH, BPS, World Health Organization
Hospital Beds per 100,000 populationOwnership by Province
0
20
40
60
80
100
120
140
160
180
Hospital B
eds per 100,000(S
ource: MO
H Inventory, 2001)
Public (Including Military) Private & Corporate
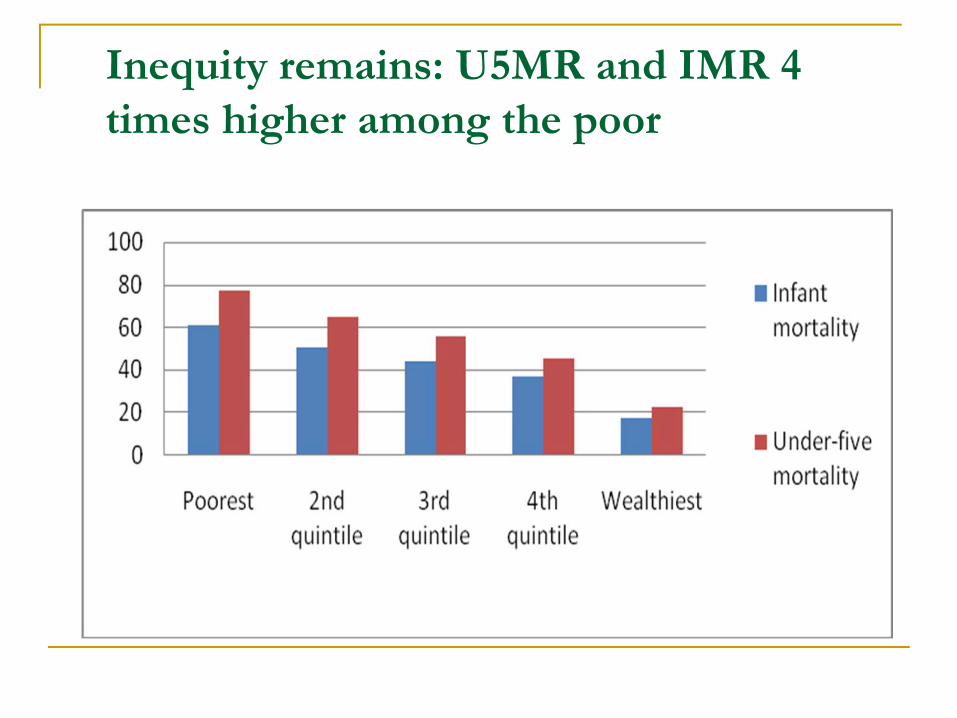
Inequity remains: U5MR and IMR 4 times higher among the poor
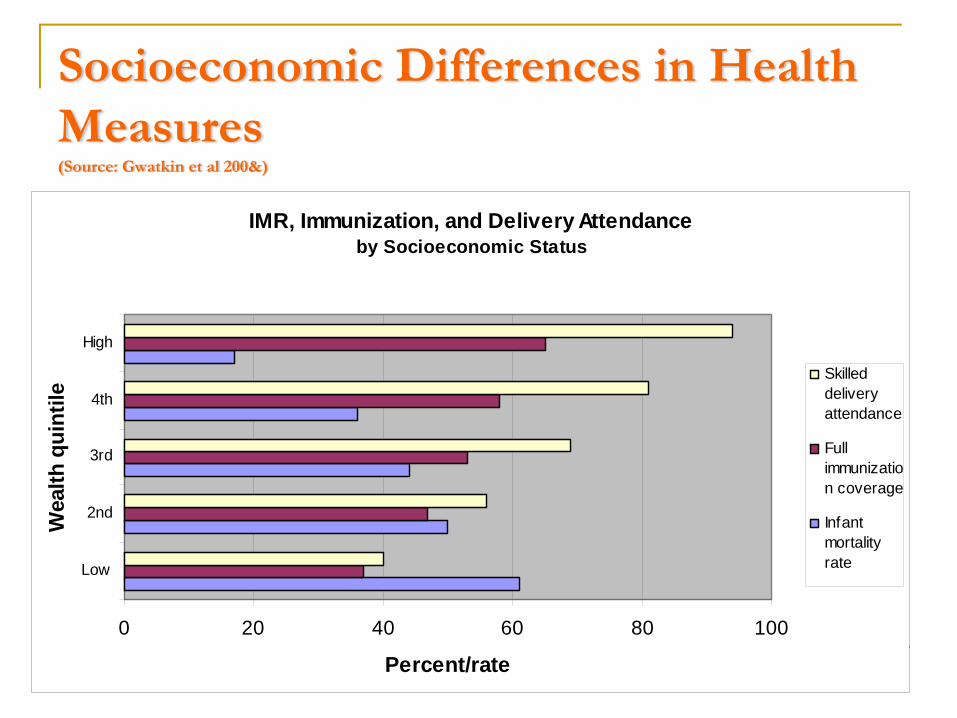
Socioeconomic Differences in Health Measures (Source: Gwatkin et al 200&)
IMR, Immunization, and Delivery Attendance by Socioeconomic Status
0 20 40 60 80 100
Low
2nd
3rd
4th
High
Wea
lth q
uint
ile
Percent/rate
Skilleddeliveryattendance
Fullimmunization coverage
Infantmortalityrate
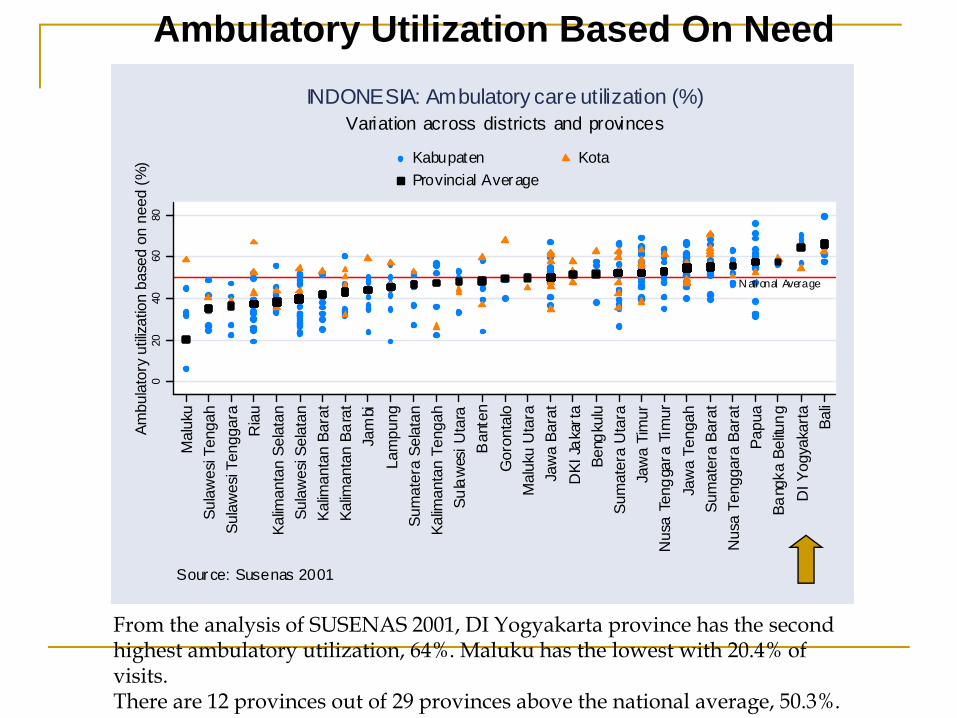
Ambulatory Utilization Based On Need
From the analysis of SUSENAS 2001, DI Yogyakarta province has the second highest ambulatory utilization, 64%. Maluku has the lowest with 20.4% of visits. There are 12 provinces out of 29 provinces above the national average, 50.3%.
N ati onal Average
020
4060
80Am
bula
tory
utili
zatio
n ba
sed
on n
eed
(%)
Mal
uku
Sula
wes
i Ten
gah
Sula
wes
i Ten
ggar
aR
iau
Kalim
anta
n Se
lata
nSu
law
esi S
elat
anKa
liman
tan
Bara
tKa
liman
tan
Bara
tJa
mbi
Lam
pung
Sum
ater
a Se
lata
nKa
liman
tan
Teng
ahSu
law
esi U
tara
Ban
ten
Gor
onta
loM
aluk
u U
tara
Jaw
a Ba
rat
DKI
Jak
arta
Beng
kulu
Sum
ater
a U
tara
Jaw
a Ti
mur
Nus
a Te
ngga
ra T
imur
Jaw
a Te
ngah
Sum
ater
a Ba
rat
Nus
a Te
ngga
ra B
arat
Papu
aBa
ngka
Bel
itung
DI Y
ogya
karta Ba
li
Kabupaten KotaProvincial Average
Source: Susenas 2001
Variation across districts and provincesINDONESIA: Ambulatory care utilization (%)
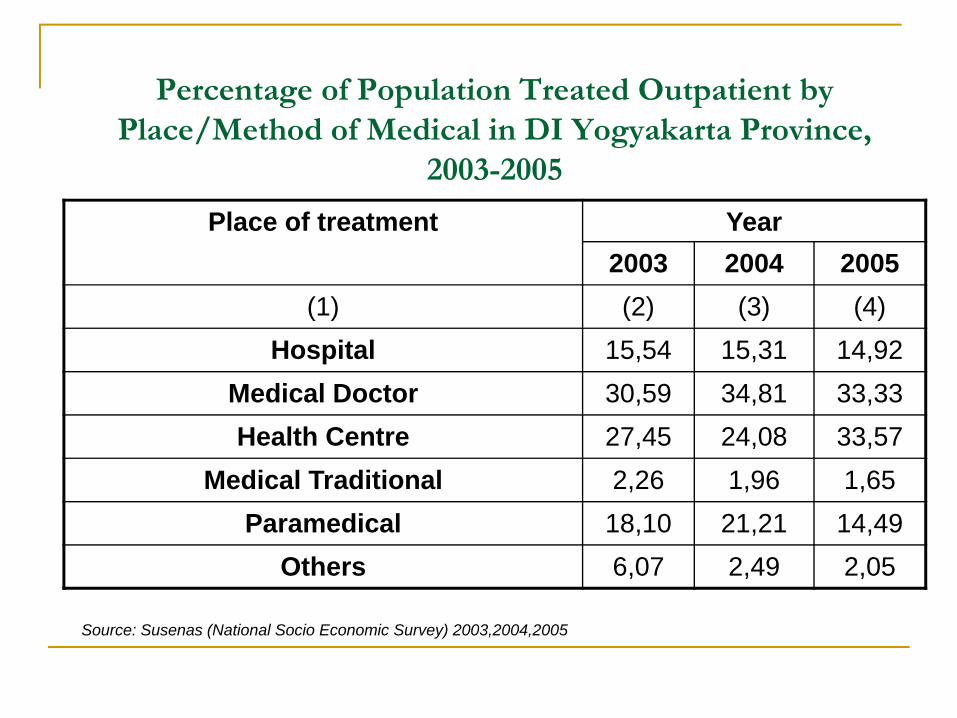
Percentage of Population Treated Outpatient by Place/Method of Medical in DI Yogyakarta Province,
2003-2005
Place of treatment Year2003 2004 2005
(1) (2) (3) (4)Hospital 15,54 15,31 14,92
Medical Doctor 30,59 34,81 33,33Health Centre 27,45 24,08 33,57
Medical Traditional 2,26 1,96 1,65Paramedical 18,10 21,21 14,49
Others 6,07 2,49 2,05
Source: Susenas (National Socio Economic Survey) 2003,2004,2005
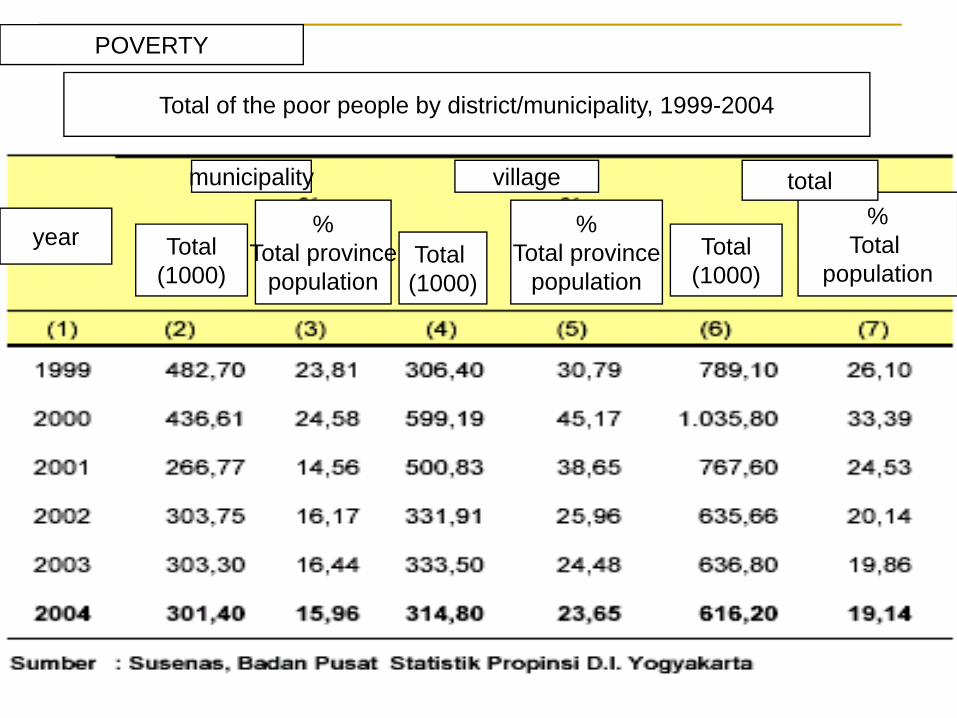
POVERTY
Total of the poor people by district/municipality, 1999-2004
year
municipality
Total(1000)
%Total province
populationTotal (1000)
%Total province
populationTotal
(1000)
%Total
population
village total
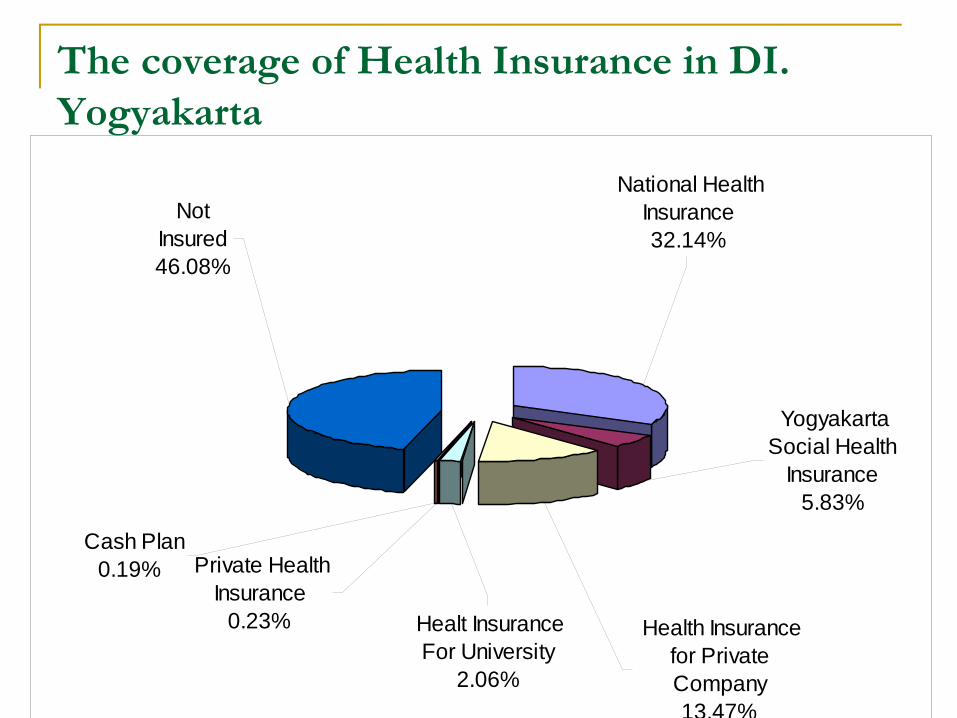
NotInsured46.08%
Cash Plan 0.19% Private Health
Insurance0.23% Healt Insurance
For University2.06%
National Health Insurance32.14%
YogyakartaSocial Health
Insurance5.83%
Health Insurance for Private Company13.47%
The coverage of Health Insurance in DI. Yogyakarta
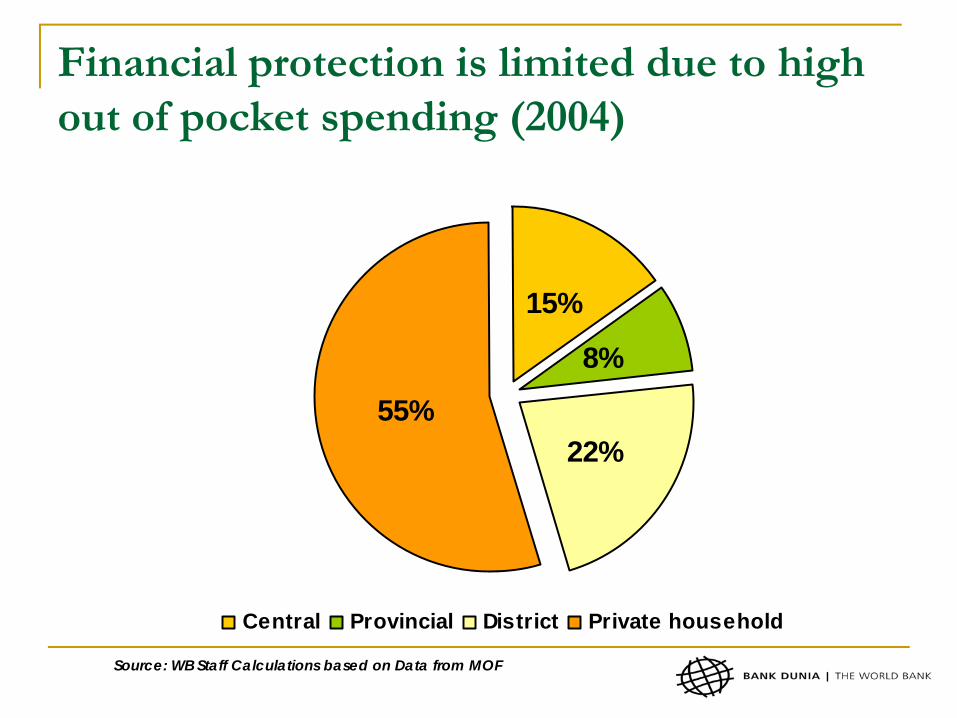
Financial protection is limited due to high out of pocket spending (2004)
15%
8%
22%55%
Central Provincial District Private household
Source: WB Staff Calculations based on Data from MOF
-
10,000,000,000
20,000,000,000
30,000,000,00040,000,000,000
50,000,000,000
60,000,000,000
70,000,000,00080,000,000,000
90,000,000,000
100,000,000,000
Rup
iah
2004 2005 2006 2007
Tahun
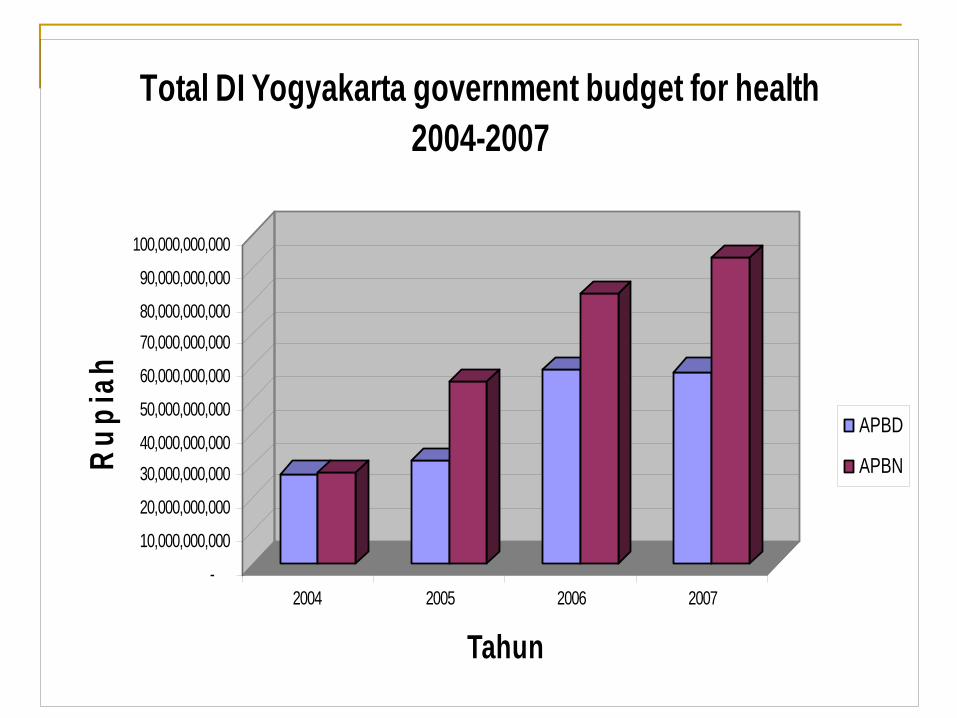
Total DI Yogyakarta government budget for health 2004-2007
APBD
APBN
Challenges in Health system
Health system faces problems of: under-funding, limited HI coverage and financial protection, income and geographic inequities, fragmentation, allocative and technical inefficiencies, low productivity, and financial sustainability
Weak stewardship of entire health system (public and private) and weak public health system
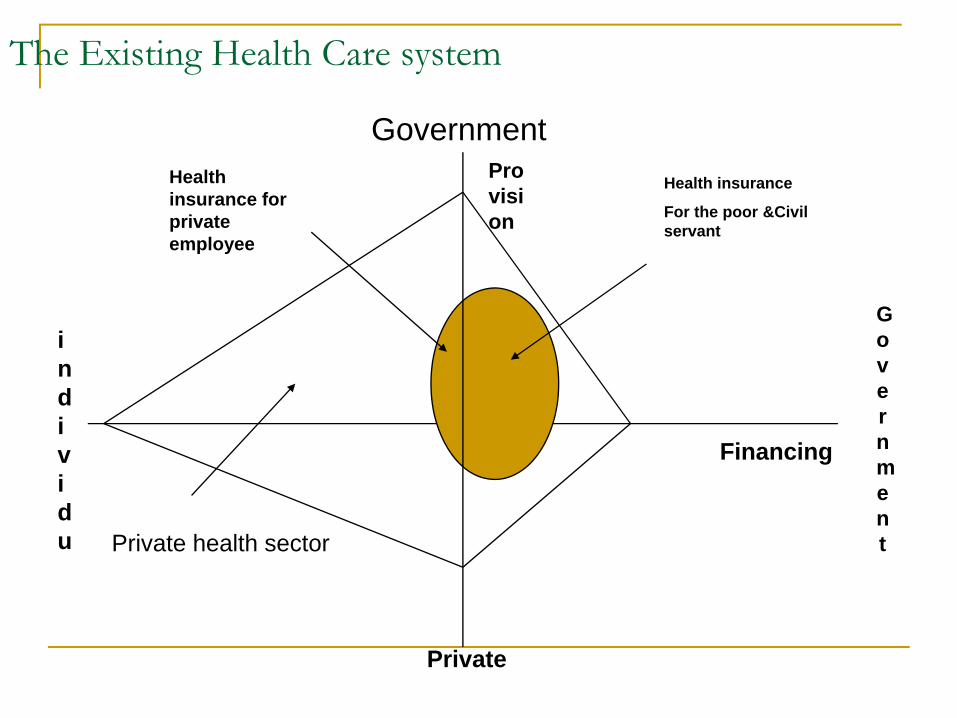
The Existing Health Care system
individu
Government
Private
Financing
Provision
Government
Health insurance
For the poor &Civil servant
Health insurance for private employee
Private health sector
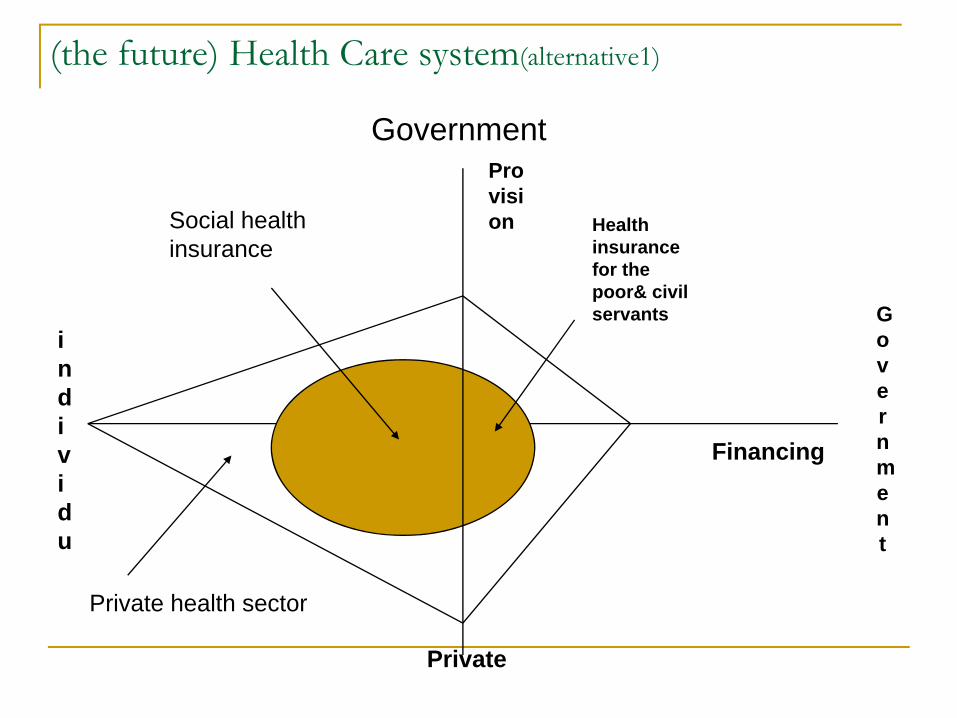
(the future) Health Care system(alternative1)
individu
Government
Private
Financing
Provision
Government
Health insurance for the poor& civil servants
Social health insurance
Private health sector
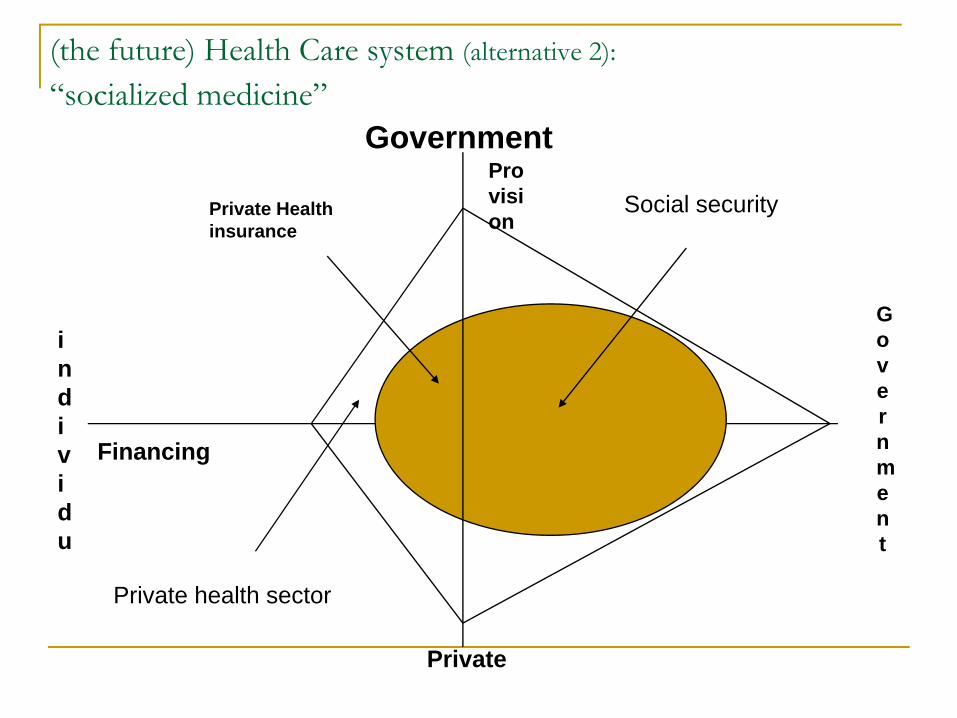
(the future) Health Care system (alternative 2):“socialized medicine”
individu
Government
Private
Financing
Provision
Government
Social securityPrivate Health insurance
Private health sector
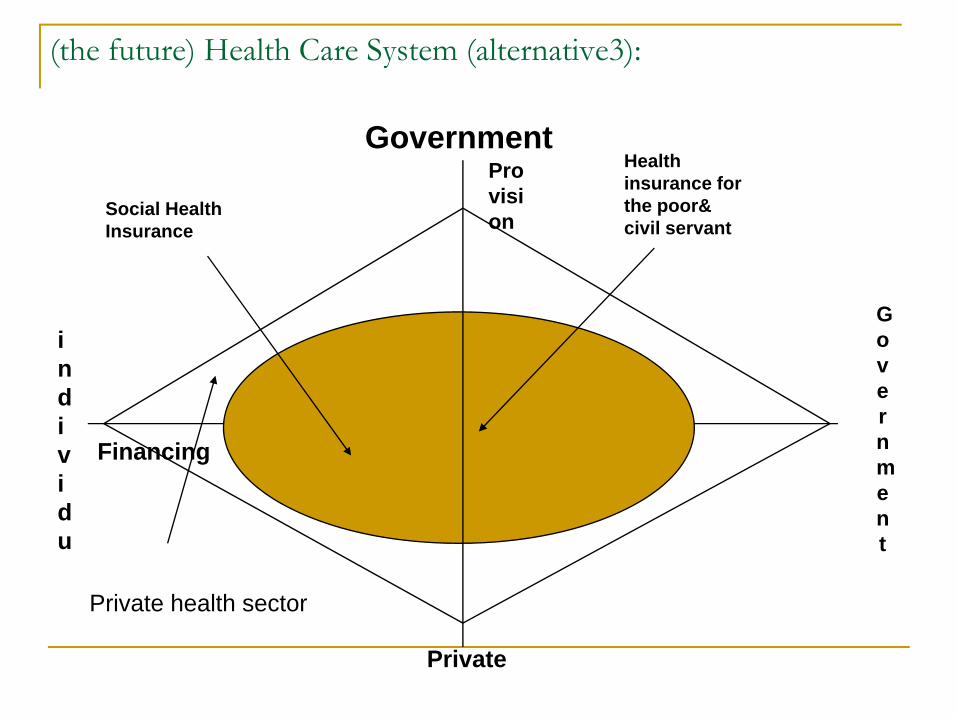
(the future) Health Care System (alternative3):
individu
Government
Private
Financing
Provision
Government
Social Health Insurance
Health insurance for the poor& civil servant
Private health sector
HEALTH FINANCING SYSTEM IN DI YOGYAKARTA PROVINCE
Predominantly role of the government in stewardship, financing and providing health care is necessary in order to assure access, equity, and affordability of health services.Preventive care like immunization, Community disease control mostly has to be the responsibility of the Government, The role of Private practice should be encouraged to substitute the weaknesses of public health services such as low quality. .Social Health Insurance should be developed, to increase access of medical services especially for the poor.Government strengthen its stewardship by set up regulation, standard and quality assurance Government has to provide free/ cheap health services to The Poor and vulnerable people
PUBLIC PRIVATE MIX ALTERNATIVES
Encourage Private and Public mix by:Appointing doctor practitioners as one of health provider in health insuranceUtilize Government health facilities by doctor practitioner in the evening servicesEncourage local health worker in the community to provide health services according to their competence Set up “village health post” to provide health services in collaboration between community and local government Collaboration among health authorities, Private and public hospital, health centre and community in disease control like TB control, dengue etc.Collaboration among all public and private hospitals, health centre and red cross in emergency and disaster.
SOCIAL HEALTH INSURANCE IN DI YOGYAKARTA PROVINCE
D.I. Yogyakarta province has already established local health Insurance: JAMKESOS, abbreviation of social health insurance, as quasi government company, which is now giving heath insurance for:Poor peopleNeglected and street ChildrenHealth volunteer (cadres)People with HIV-Aids and dengue fever
JAMKESOS contract public and Private Hospital and health centre and Family physician as health provider

Health Care Quality Council(BADAN MUTU PELAYANAN KESEHATAN)
A government partner in regulating health careA non-structural government body who is developing to be independentNot as a part of health office, health professionals organization, or health care institutionto give recommendations to government based on result of health institution surveyto accredit and certify medical institution, mostly privateEncourage setting up health worker competence standard