Embed Size (px)
DESCRIPTION
chapter 4 lecture
Citation preview

Chapter 4- Cerebrovascular
DiseaseBrant and Helms Lecture Series
Michael Bergen PGY-2

Stroke is a clinical term referring to a non-traumatic brain insult resulting in a sudden loss of neurologic function
Infarction represents about 75% and Hemorrhage about 25% of strokes
Radiologist plays a critical role in evaluation and triage of EVERY stroke patient

Ischemic StrokesThromboembolic events are the
principle causes of ischemic events
i.e. Large artery atherosclerosis
has a higher mortality than
lacunes and are amendable to
Carotid Endarectomy

Acute Ischemia FindingsIschemia = Increased Cellular water
content = Cytotoxic edema
Brain water content is the principle to understating CT and Brain MRI in stroke

More Subtle CT findings
r/o Hemorrhage is the most critical step in HEAD CT evaluation
Early signs of infarction can be evident: Insular Ribbon Sign, Sulcal effacement, Mass effect, edema

MRI SequencingDWI: Uses a strong gradient pair that sensitizes images to microscopic BROWNIAN WATER MOTION
Brain water diffusion rapidly falls during acute ischemia.
Early infarct = BRIGHT SIGNAL ON DWI
ADC: reflects pure diffusion behavior free of any shine through and appears = DARK SIGNAL
** DDX: pyogenic abscess and tumors

MR

Pattern Recognition in Ischemic
Stroke
Vascular anatomy to functional neuroanatomy is critical

Anterior Circulation
Internal Carotid Artery- atherosclerotic disease near the carotid bifurcation is responsible for majority ICA territory events

MRA of Circle Willis

ACARepresent 5% of infarcts
3 subgroups of Branches:
1. Medial Lenticulostriates
2. Hemispheric
3. pericallosal

MCA
Represents 2/3 of Infarcts
Branches:
1. Lateral Hemispheric
2. Lateral lenticulostirates

Posterior (Vertebrobasilar) Circulation

Acute Brainstem Infarction

Posterior Cerebral ArteryRepresent 10-15% of Infarcts
Major Branches : 1. thalamic perforators 2.Posterior Choroidal 3.Cortical (med. temporal and occ. lobes)
** Normal Variant of the Circle Willis is a fetal origin of the PCA ~20% population

Contralateral homonymous Hemiaponsia

Cerebellar StrokeOften Neurosurgical emergencies and require posterior fossa decompression
85% ischemic and 15% hemorrhagic
Presents with headache, vertigo, N/V, ipsilateral ataxia
Superior Cerebellar Artery
Anterior Inferior Cerebellar Artery
Posterior Inferior Cerebellar Artery


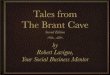
Small Vessel IschemiaLacunes ‘little lakes’ account for 15-20% of all strokes
Secondary to long-standing HTN
Affects subcortical regions i.e Lenticular nucleus (37%), pons (16%), thalamus (14%), caudate (10%), IC (10%)

1. multiple foci of deep white matter/basal ganglia lacunar infarcts (black arrow), typical in small vessel ischemic disease


Venous InfarctionUncommon, but affects younger, OCPS, dehydration, infections
Blockage of outflow leads to stasis--neuronal death
Lesions tend to spare cortex, don’t follow normal vascular territories
CT- Empty Delta Sign; Spin Echo and MRV best imaging modality

Venous Infarction

Hemorrhagic Transformation of infarction
Reperfusion injury and develops in 15-45% of infarcts
Confined to infarcted vessel territory and intraventricular extension is UNCOMMON
Peaks 1-2 weeks post infarction
Manifest as serpiginous line of petechial blood following gyral contours of the infarcted cortex
Catastrophic hemorrhagic transformation can follow TPA

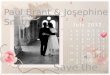
Subacute Infarction

Acute vs Subacute vs Chronic

Subacute InfarctionSubacute infarction approximately 2-14 days following initial ischemic event
Best diagnostic clue: Gyral edema and enhancement within basal ganglia and cortex
Typically wedge-shaped abnormality involving gray and white matter within vascular distribution
HT of initially ischemic infarction occurs in 15-20% of MCA occlusions, usually by 48-72 hours
"2-2-2" rule = enhancement begins at 2 days, peaks at 2 weeks, disappears by 2 months
• ↑ lactate, ↓ NAA within infarcted tissue

wedge-shaped abnormality involving gray and white matter within vascular distribution

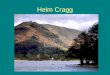
Gyriform Enhancement


Chronic Infarction• Volume loss with gliosis along affected margins
• Classic: Wedge-shaped area of encephalomalacia
• Wallerian degeneration may be present

Chronic Infarction


HemorrhagesDivided: Subarachnoid vs Intraparenchymal
CT presents as high attenuation and MR is based on iron oxidation state
MR is best for subacute and chronic blood
FLAIR very sensitive for SAH
Gradient T2 echo is sensitive for parenchymal bleed

Biochemical evolution of hemorrhage

MR pattern signal


Subarachnoid Hemorrhage

Parenchymal HemorrhageHemorrhage has a higher mortality than infarction but less deficits on recovery
Trauma excluded DDX considerations: hypertensive, drugs, AVM, amyloid, tumors

Cases

Case 1

Case 2

Case 3

Case 4

Case 5
1
2
3