Embed Size (px)
Citation preview

BY DR.HISHAM AHMED,M.D.
CONSULTANT PEDIATRIC SURGERY
PEDIATRIC SURGICAL PHYSIOLOGYPEDIATRIC SURGICAL PHYSIOLOGY
INTRODUCTION Pediatric patients include neonates (less than 30 days
of age), infants (1-12 months of age), and children (1-12 years of age) who are not merely small adults.
Their successful and safe surgical and anaesthetic management depends on an appreciation and clear understanding of the physiologic, anatomic, pharmacologic and psychologic differences between each group and adults.
The smaller size, immature organ systems, and differing volume capacities present unique challenges toward perioperative management. .
1- Respiratory Function 2- Cardio-circulatory Function
3- Fluid and Electrolyte Regulation 4- Thermal Regulation
5- Metabolic Problems
Key areas of concern in the newborn include:
6- Nutrition 7- Stress Response to Surgery 8- Infection in the newborns
9-Control of pain
10- Rate of deterioration
Key areas of concern in the newborn include:
1-Respiratory Function
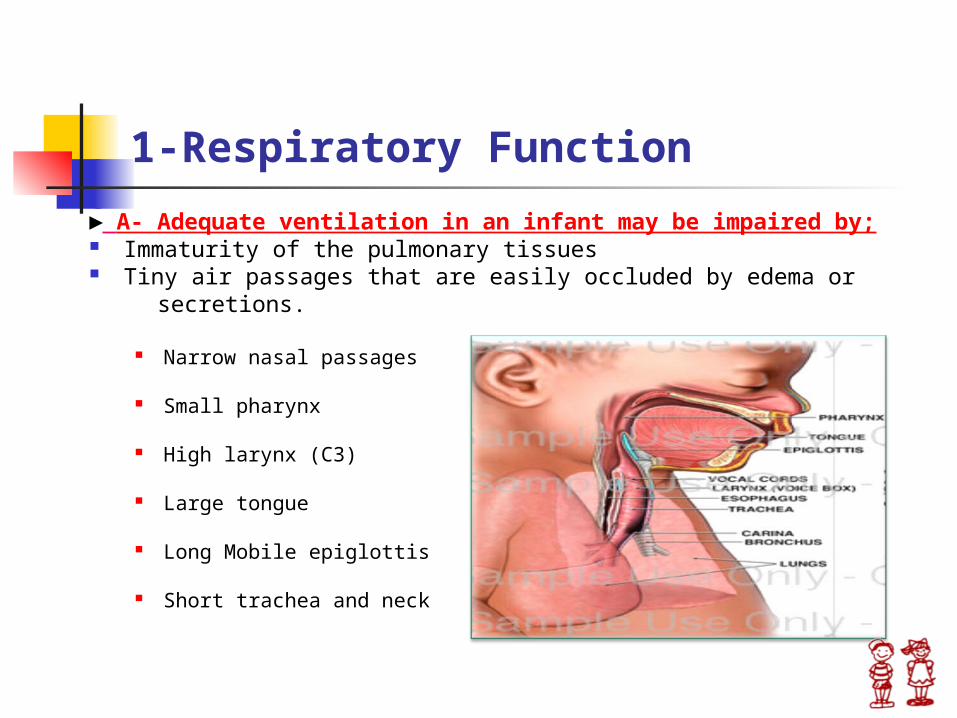
► A- Adequate ventilation in an infant may be impaired by; Immaturity of the pulmonary tissues Tiny air passages that are easily occluded by edema or secretions.
Narrow nasal passages
Small pharynx
High larynx (C3)
Large tongue
Long Mobile epiglottis
Short trachea and neck
1-Respiratory Function
► B- Increase Oxygen demand required for their relatively high metabolic rate;
Oxygen consumption in the neonate is 6 ml/Kg/min versus 3 ml/Kg/min in the adult.
The process of pulmonary alveolar maturation is not
complete until 8-10 years of age.
The number of saccules and primitive alveoli in the lung of a neonate is only 8% of the number of the alveoli in an adult.
Alveolar ventilation in a neonate is twice that of the adult ( 100-150 ml/Kg/min versus 60 ml/Kg/min).
1-Respiratory Function
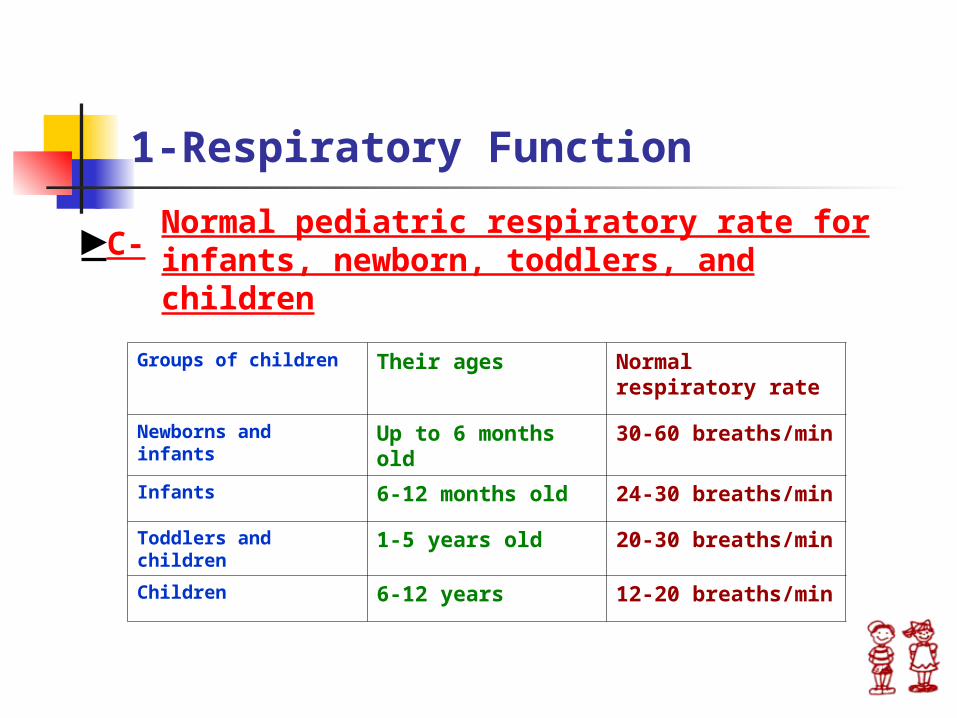
►C-Normal pediatric respiratory rate for infants, newborn, toddlers, and children
Groups of children Their ages Normal respiratory rate
Newborns and infants
Up to 6 months old
30-60 breaths/min
Infants 6-12 months old 24-30 breaths/min
Toddlers and children
1-5 years old 20-30 breaths/min
Children 6-12 years 12-20 breaths/min
2-Cardio-circulatory Function A satisfactory circulating blood volume is the most
important factor in determining whether an operation can be undertaken safely, and in the absence of cardiac failure.
The blood volume of a newborn infant is approximately 10% of the total body weight.
High hematocrit in the first few days of life (>50%) .
A minimal deficit of 25% can lead to acute hypovolemic shock.
2-Cardio-circulatory Function
A single surgical sponge may absorb as much as 20 ml of blood ( a few saturated sponges may prove sufficient to precipitate shock).
Transfusion of blood is given for losses >10% of the blood volume. A transfusion of 10 ml/Kg is approximately equivalent to the administration of a single unit of whole blood to a 70 Kg adult.
An infant can tolerate rapid infusion of 20-25 ml/Kg of whole blood or plasma without ill effect.
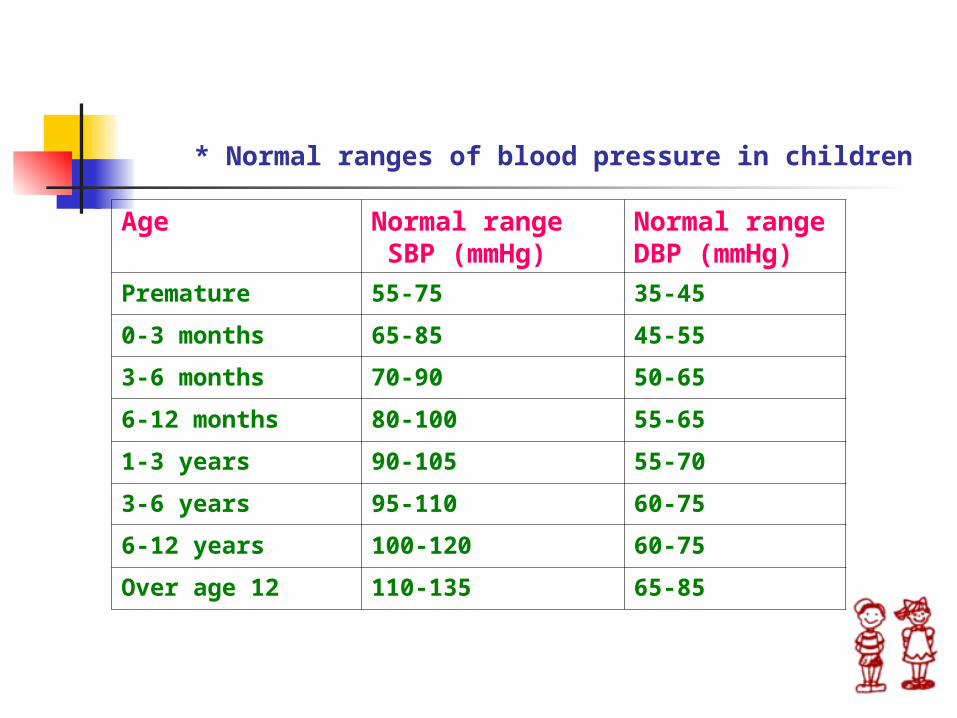
* Normal ranges of blood pressure in children
Age Normal range SBP (mmHg)
Normal range DBP (mmHg)
Premature 55-75 35-45
0-3 months 65-85 45-55
3-6 months 70-90 50-65
6-12 months 80-100 55-65
1-3 years 90-105 55-70
3-6 years 95-110 60-75
6-12 years 100-120 60-75
Over age 12 110-135 65-85
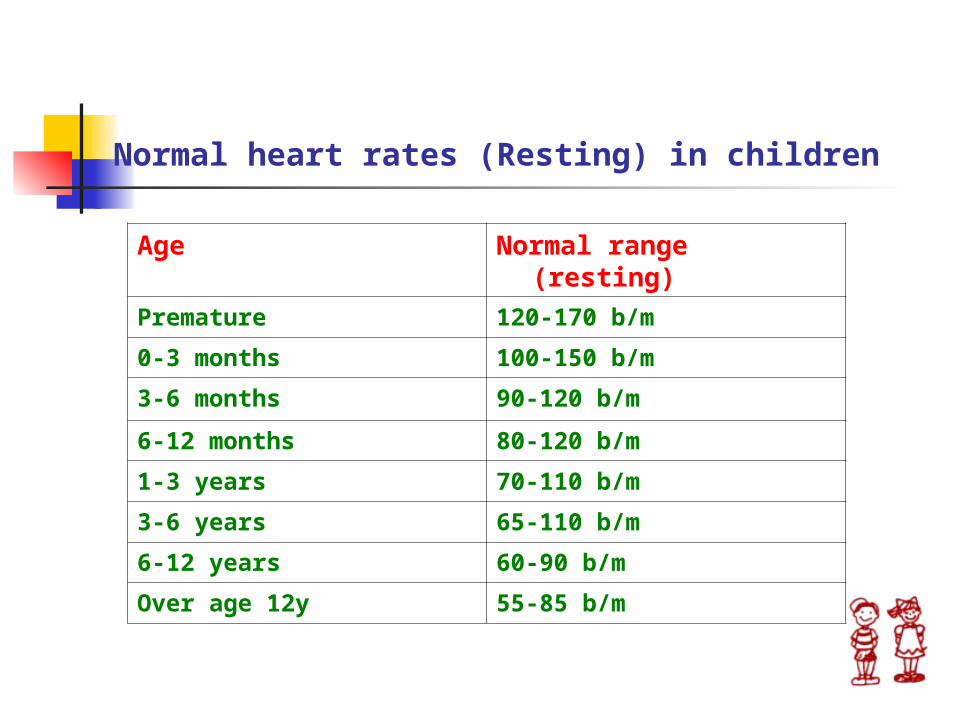
Normal heart rates (Resting) in children
Age Normal range (resting)
Premature 120-170 b/m
0-3 months 100-150 b/m
3-6 months 90-120 b/m
6-12 months 80-120 b/m
1-3 years 70-110 b/m
3-6 years 65-110 b/m
6-12 years 60-90 b/m
Over age 12y 55-85 b/m

3-Fluid and Electrolyte Regulation In managing the pediatric surgical patient, an understanding of fluid and
electrolyte balance is critical, as the margin between dehydration and fluid overload is small.
• The total body water (TBW) of a newborn is 75-80% at term gestation, decreased by 4-5% during the first week of life.
• The glomerular filtration rate (GFR) of the newborn is 25% that of the adult.
• The GFR rapidly rises during the first week of life and then slowly increases to adult levels by 2 years of age.
3-Fluid and Electrolyte Regulation
The immaturity of the newborn kidney contribute to the inability to concentrate and conserve fluid and electrolyte, and so rapid development of respiratory and metabolic acidosis or alkalosis.
The normal urinary output in adequately hydrated infant should approximate 1-2 ml/kg/hr.
♠ What is the maintenance IV fluid for children? D5 ¼ NS + 20 mEq KCL♠ How are maintenance fluid rates calculated in children? 4,2,1 per hour *4 cc/kg for the first 10 kg of Body weight *2 cc/kg for the second 10 kg of body weight *1 cc/kg for every kilogram over the first 20 kg.
4-Thermal Regulation
Newborn infants are potentially thermolabile as a consequence of;
Increased body surface area relative to weight.
Thinner layer of insulating S.C fat.
Immature thermal regulatory mechanisms.
Incomplete myelination of the heat regulating center in the hypothalamus
4-Thermal Regulation
Inadequate vasoconstriction of cutaneous vessels in response to cold.
Minimal shivering and sweating mechanisms.
All premature babies and most neonates will require incubators or at least wrapping of limbs and body with cotton wool to minimize heat loss.
4-Thermal Regulation
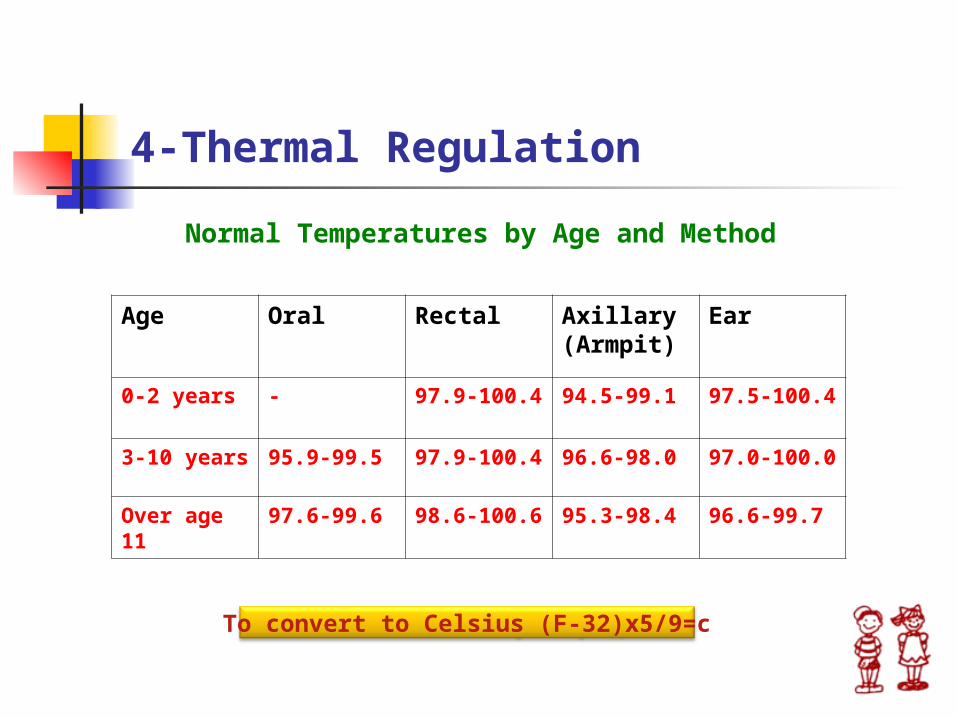
Normal Temperatures by Age and Method
Age Oral Rectal Axillary (Armpit)
Ear
0-2 years - 97.9-100.4
94.5-99.1 97.5-100.4
3-10 years 95.9-99.5 97.9-100.4
96.6-98.0 97.0-100.0
Over age 11
97.6-99.6 98.6-100.6
95.3-98.4 96.6-99.7
To convert to Celsius (F-32)x5/9=c
5-Metabolic Regulation
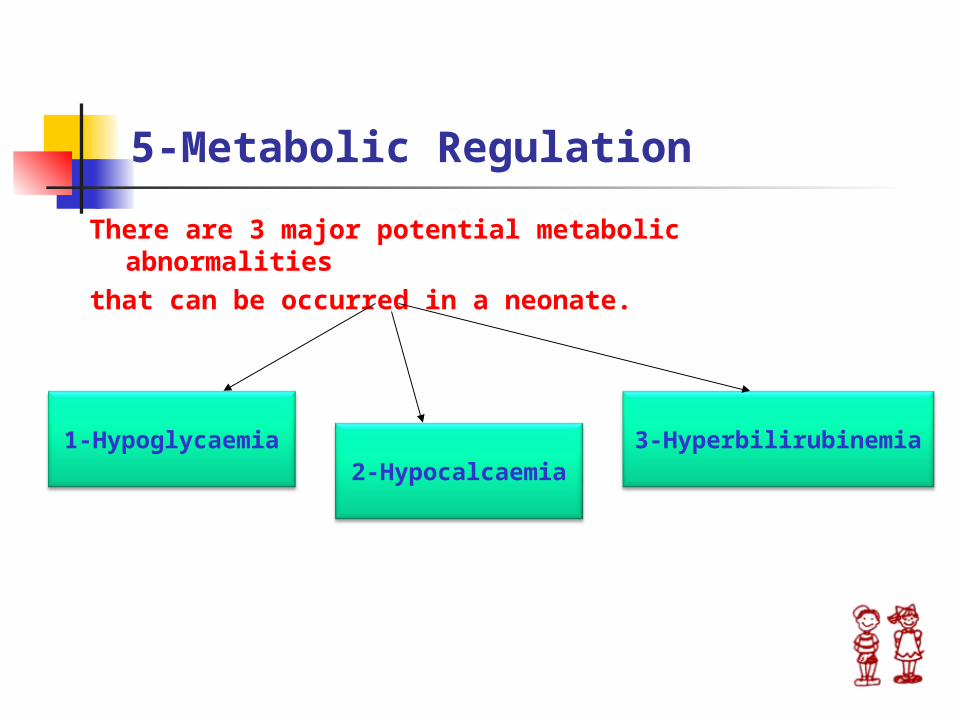
There are 3 major potential metabolic abnormalitiesthat can be occurred in a neonate.
2-Hypocalcaemia3-Hyperbilirubinemia1-Hypoglycaemia
5-Metabolic Problems
►1-Hypoglycaemia; It’s common and dangerous
complications in the newborn stressed by surgical trauma or disease .
It’s due to
♠ Deficiency of glycogen stores♠ Impaired gluconeogenesis♠ Difficulties with insulin regulation
►2-Hypocalcaemia;(especially in premature infants)Overall, one of the most common causes of hypocalcemia is renal failure because of inadequate 1-hydroxylation of 25-hydroxyvitamin D.
Other causes of hypocalcaemia:
♠ Prematurity ♠ Birth asphyxia ♠ Exogenous phosphate load ♠ Hypoparathyroidism ♠ Abnormal vitamin D production ♠ Intrauterine growth retardationN.B; The normal range of glucose
production in a newborn is about 5-8 mg/kg/min.
5-Metabolic Problems
►3-Hyperbilirubinaemia; (Neonatal Jaundice)
♦ It is virtually a normal physiological occurrence in almost all newborn especially in the first 3-7 days.
♦ It is the result of accumulation of unconjugated bilirubin in healthy neonates.
♦ In white and black infants the peak level of bilirubin is ~6 mg/dl at 72 hours of age. In Asian infants the bilirubin level peaks later(3-5days) at a higher level ~ 12 mg/dl.
♦ Bilirubin is neurotoxic and can cause death in newborns or Kernicterus which is a bilirubin staining of the basal ganglia, thalamus, cerebellum, hippocampus, and cranial nerve nuclei leading to long-term sequelae in children.
5-Metabolic Problems
Neonatal physiologic jaundice results from simultaneous occurrence of the following 2 phenomena;
♥ Increased bilirubin production because of increased breakdown of fetal erythrocytes.
♥ Hepatic excretory capacity is low both because of low concentrations of the binding protein and low activity of glucuronyl transferase enzyme
Jaundice in infants that persists longer than 2 weeks should not be considered Physiologic, especially if the predominant fraction is conjugated bilirubin.
6-Nutrition
♣ Because of limited caloric reserves and the high demands due to rapid growth and maturation, maintenance of adequate nutritional support is of paramount important.
♣ The best feed for infant is fresh maternal breast milk, if not possible, parentral feeding should be started, using solutions of amino acids (Vamin),fats (Intralipid 10% or 20%) and carbohydrates ( Dextrose) with electrolytes, vitamins and trace elements via a central venous or peripheral venous line.
6-Nutrition
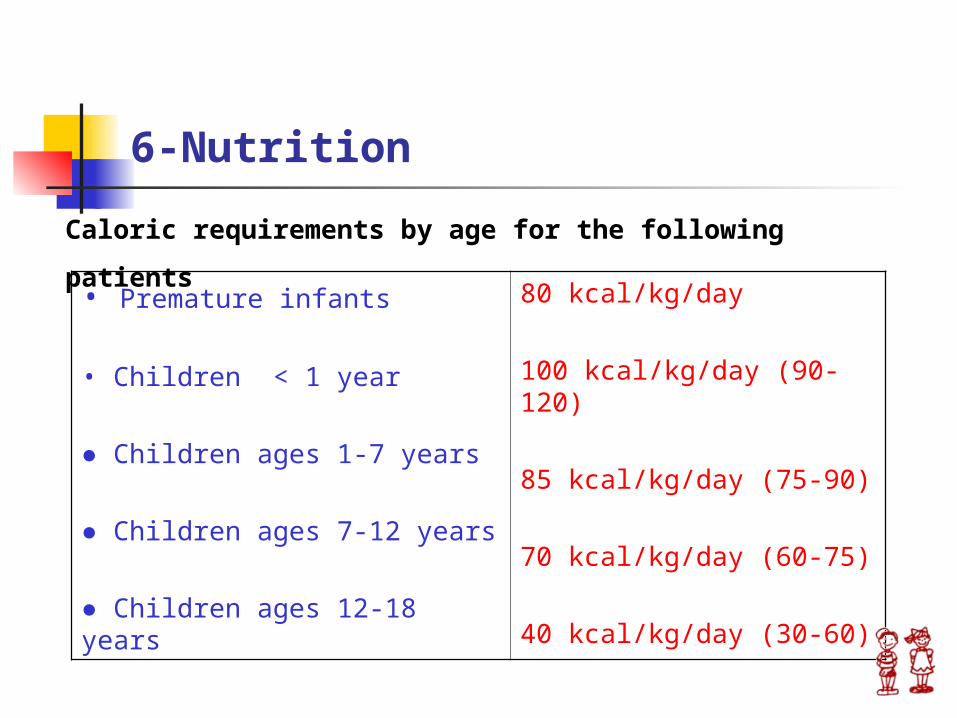
Caloric requirements by age for the following patients • Premature infants
• Children < 1 year
● Children ages 1-7 years
● Children ages 7-12 years
● Children ages 12-18 years
80 kcal/kg/day
100 kcal/kg/day (90-120)
85 kcal/kg/day (75-90)
70 kcal/kg/day (60-75)
40 kcal/kg/day (30-60)
7- Stress Response to Surgery
♣ The endocrine and metabolic response to surgical stress in newborn is characterized by catabolic metabolism.
♣ An initial elevation in catecholamines, cortisol and endorphins upon stimulation by noxious stimuli occurs.
♣ Responsiveness during the first week of life is diminished , due to immaturity of the adrenal gland.
♣ During surgical stress newborn release glucose, fatty acids, ketone bodies and amino acids necessary to meet body energy needs in time of increased metabolic demands.
♣ Early post-operative parenteral nutrition can result in significant rate of weight gain due to solid tissue and water accumulation.
7- Stress Response to Surgery
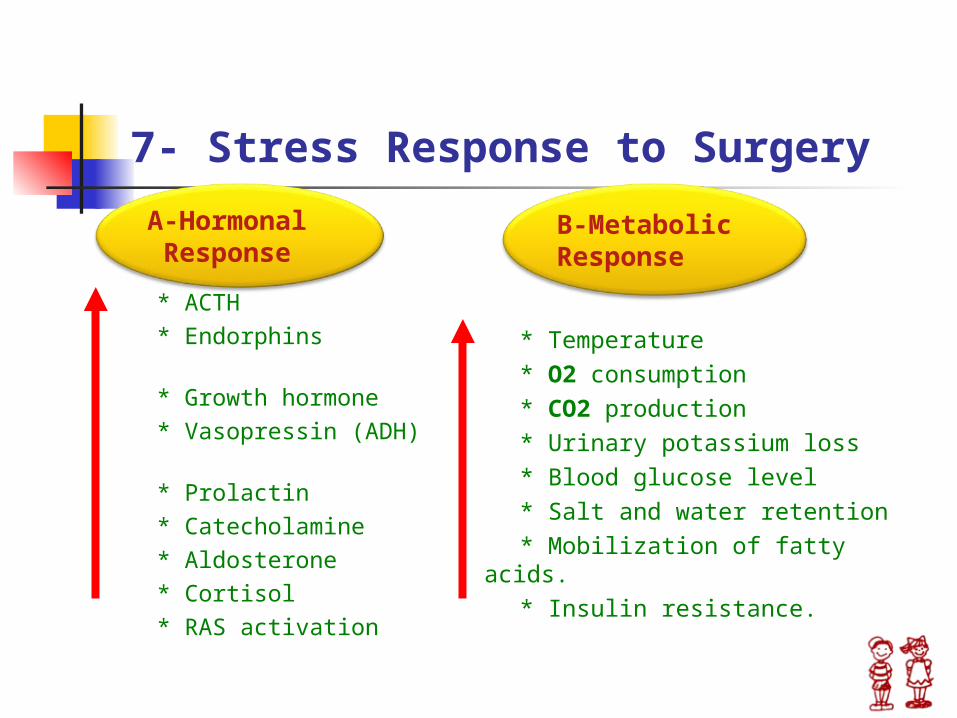
* ACTH * Endorphins * Growth hormone * Vasopressin (ADH) * Prolactin * Catecholamine * Aldosterone * Cortisol * RAS activation
* Temperature * O2 consumption * CO2 production * Urinary potassium loss * Blood glucose level * Salt and water retention * Mobilization of fatty acids. * Insulin resistance.
A-Hormonal Response
B-Metabolic Response
7- Stress Response to Surgery
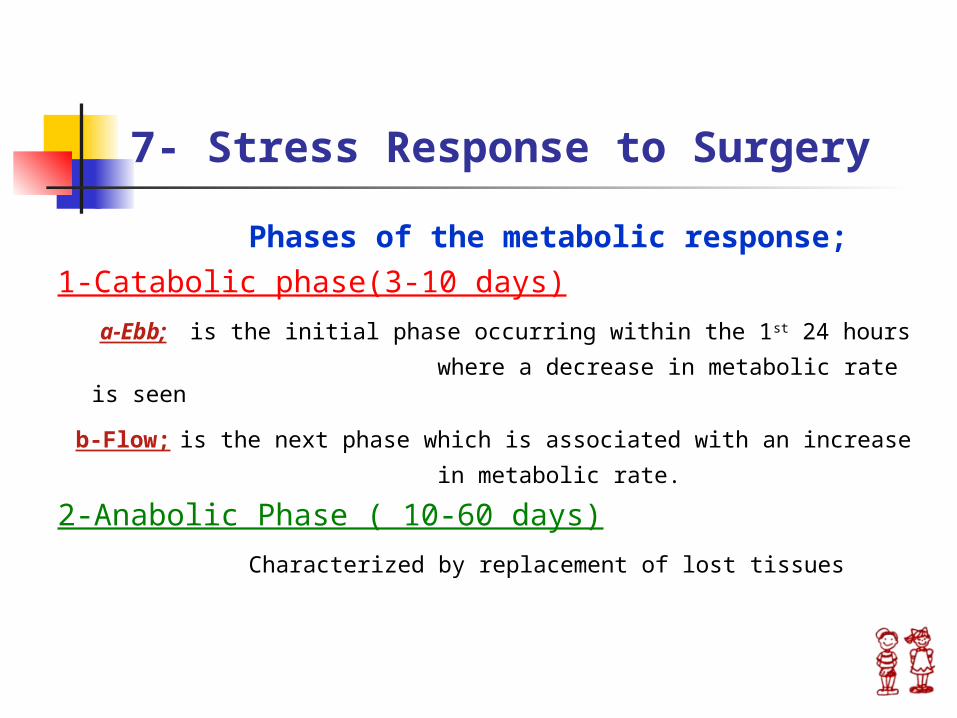
Phases of the metabolic response;
1-Catabolic phase(3-10 days)
a-Ebb; is the initial phase occurring within the 1st 24 hours
where a decrease in metabolic rate is seen
b-Flow; is the next phase which is associated with an increase
in metabolic rate.
2-Anabolic Phase ( 10-60 days)
Characterized by replacement of lost tissues
7-Stress Response to Surgery
Factors contributing to a prolonged catabolic response
Degree of neuro-endocrinal maturation Duration of operation General condition of the patient Amount of blood loss Type of surgical procedure Type of pathology Extent of surgical trauma Associated conditions ( hypothermia, prematurity, etc.).
8- Infection in Newborn
In stable newborn infants the intra-cellular phagocytosis-killing of bacteria is normal, but with the added stress of sepsis or operation there is a significant decrease in bactericidal activity as a result of the immunosuppressive effect of operation and anaesthesia.
Gram +ve ( staphylococcus aureus or albus) and gram –ve (E-coli) sepsis account for the major and most serious infections, that may lead to severe acidosis, hypothermia and circulatory collapse in late cases.
Broad spectrum antibiotics are indicated when complex surgical procedures are performed in neonates
9- Pain Control
♠ The past 20 years have seen many changes in the understanding and treatment of acute pain in infants and children.
♠ The first step was to disprove the previously held misconceptions that neonates, infants and children did not feel or react to pain like adults.
♠ This belief was based on the misconception of the immaturity of the CNS of infants made them less likely to perceive pain.
♠ This theory compounded by fears of addiction and adverse effects from opioids, resulted in the inadequate treatment of pain.
9- Pain Control
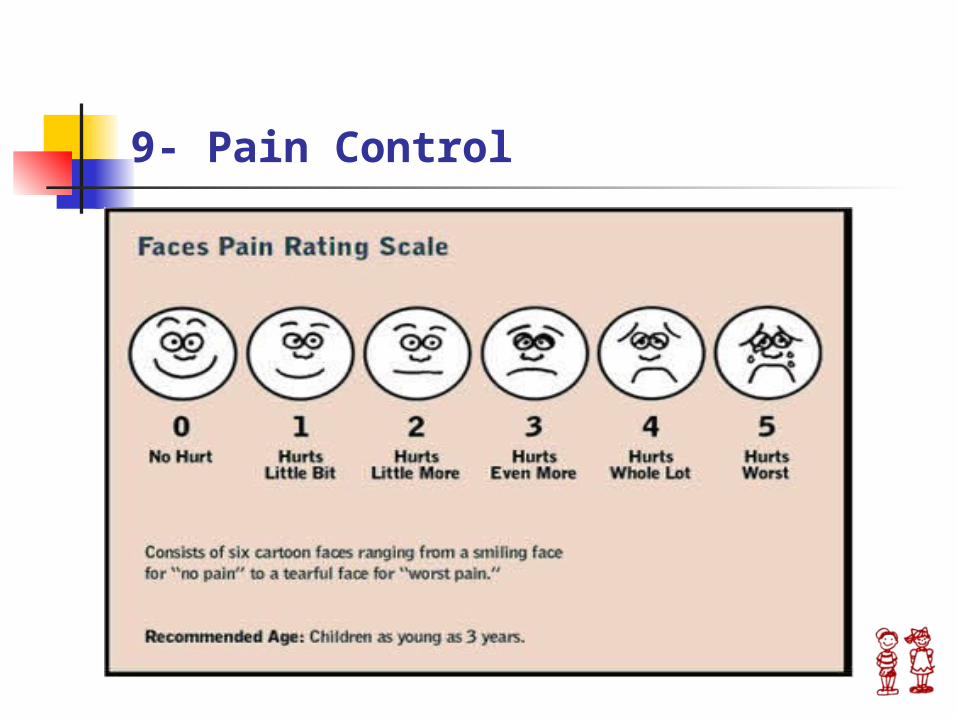
♠ Recent studies have shown that infants and children experience a severity of postoperative pain similar to adults and that even premature infants demonstrate alterations in heart rate, blood pressure, and oxygen saturation in response to painful stimuli.
♠ Considerations in the treatment of acute pain includes;
* The severity of pain
* The setting in which it is treated (inpatient Vs outpatient)
♠ One approach is to use a three step ladder, initially described by the World Health Organization for the treatment of cancer related pain.
9-Pain Control
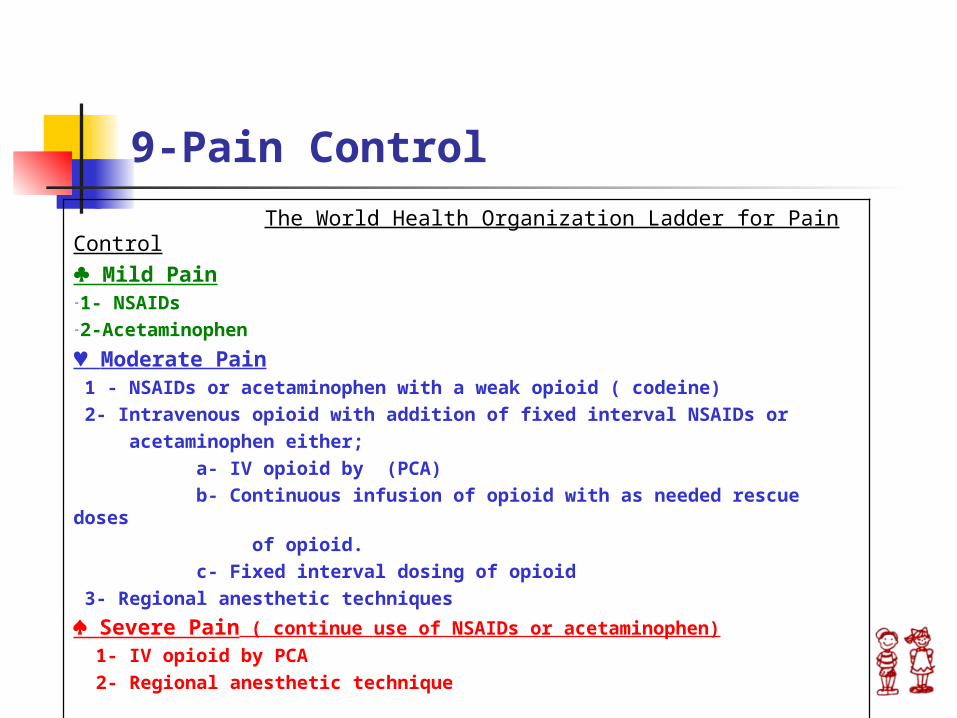
The World Health Organization Ladder for Pain Control♣ Mild Pain-1- NSAIDs-2-Acetaminophen
♥ Moderate Pain 1 - NSAIDs or acetaminophen with a weak opioid ( codeine)
2- Intravenous opioid with addition of fixed interval NSAIDs or
acetaminophen either;
a- IV opioid by (PCA)
b- Continuous infusion of opioid with as needed rescue doses
of opioid.
c- Fixed interval dosing of opioid
3- Regional anesthetic techniques
♠ Severe Pain ( continue use of NSAIDs or acetaminophen)
1- IV opioid by PCA
2- Regional anesthetic technique
9- Pain Control
10-Rate of Deterioration
♥ Newborns deteriorates rapidly than
adults.
♥ A child can become dehydrated from
gastroenteritis to the extent of peripheral circulatory failure in a day.