Embed Size (px)
Citation preview
PergamonInternational Journal for Quality in Health Care, Vol. 6, No. 4, pp. 389-395,1994
Copyright © 1994 Elsevier Science LtdPrinted in Great Britain. All rights reserved
1353-^505/94 $7.00+0.00
1353-4505(94)00023-9
Calculation and Administration of Drug Dosage bySwedish Nurses, Student Nurses and Physicians
INEZ D. KAPBORG
Dean of School of Nursing, S-721 89 Vaster&s,Sweden
A diagnostic test was used to assess the math-ematical knowledge and skills in 545 experiencednurses and 197 student nurses. The main pur-pose of this study was to investigate if studentnurses and registered nurses have adequateknowledge and skills in drug dosage calculation.Nine out of fourteen test items were solved accu-rately and no differences were found in theaverage performance between the two groups.To evaluate physicians' knowledge about statu-tory regulations on drug prescription and legalresponsibility, 36 physicians from differenthealth care areas answered a questionnaire. Theanswers revealed that the majority was not fam-iliar with these regulations.
The results are discussed in relation to nurseeducation and the physicians' legal responsibi-lity in connection with drug administration andprescription.
Key words: Nursing education, mathematical skills,drug dosage calculation, evaluation, quality assur-ance, statutory regulations on drug prescription.
INTRODUCTION
In a previous Swedish study, the mathemat-ical knowledge and skills of beginner studentnurses were investigated by Kapborg [1]. Thestudy included 997 subjects enrolled in a 2-yearnursing education programme and 188 subjectsattending a 3-year programme. Subjects calcu-lated 65 items comparable with the mathemat-ical knowledge of the 9-year compulsory schoolcurriculum. The results showed that a large
proportion of this sample lacked adequatemathematical knowledge and skills when theyentered the school of nursing. The studentsmanaged to solve about 50% of the items accu-rately. Items involving transformation of unitsand percentage calculations appeared to be themost difficult to solve.
Another study by the same author [2] investi-gated the students' educational background aswell as the amount of scheduled teaching timefor drug dosage calculation during the 2-yeareducation in 31 schools of nursing in Sweden.This time varied between 0 and 42 hours. Onaverage, students were offered 12 hours ofteacher-provided training. One reason for thisvariation in training may be that there are norules regulating the teaching of drug dosagecalculation in the curriculum for Swedish nurs-ing education programmes. Further, nursetutors are usually not qualified as teachers ofmathematics.
The accurate administration of drugsdepends not only on the nurses' knowledge andskills in drug dosage calculation, but also on thenurses' knowledge of pharmacology in order toexamine the relevance of prescribed drugs anddosages. Other factors may influence thenurses' administration of drugs. One of themost important is the physicians' responsibilityin prescribing drugs.
Swedish statutory regulations [3] state thatphysicians must prescribe drug dosages in writ-ing on a medicine card. Prescriptions, signed bya qualified physician, must follow these regu-lations, in order for the nurse to administer therequired drugs. This means that when the physi-cian has completed his written prescriptions,the nurse does not have to make any calcu-lations before administration of the drugs iscarried out.
Received 1 March 1994; accepted 9 June 1994.
389
at University of M
ichigan on October 19, 2014
http://intqhc.oxfordjournals.org/D
ownloaded from
390 I. D. Kapborg
From personal experience, a nurse can re-spond in two different ways to the physicians'decisions. First, some nurses think that it is thephysician's sole prerogative to make decisionsabout what should be done for a patient, whilethe nurse's function is to comply with thesedecisions. Secondly, other nurses feel com-petent and ask questions about the differentdecisions before they carry them out. Whennurses handle drugs they have the responsibilityof double-checking the dosage and possibletoxic effects or contraindications, i.e. to consulta suitable pharmacological textbook in uncer-tain cases before administering prescribeddrugs.
It is therefore of interest to investigate notonly the nurses' calculating ability, but also thephysicians' knowledge of the pertinent regu-lations in this area.
Purpose of the study
The main purpose of this study is to investi-gate whether student and registered nurses haveadequate knowledge and skills in drug dosagecalculation. The results from a diagnostics testare related to different background variables.An additional aim is to evaluate the physicians'knowledge about statutory regulations on drugprescription and their legal responsibilityregarding the proper prescription of drugs.
MATERIALS AND METHODS
Subjects
In order to achieve a representative sample ofexperienced nurses from various medical fields,the test was given to 545 nurses who wereenrolled in various supplementary nursing pro-grammes. Represented in the study were nursesin programmes for: Bachelor of Science inNursing Midwifery; Public Health Nursing;Anaesthetic Nursing and Intensive Care Nurs-ing; Psychiatric Nursing; Oncology Nursing;and Trainee Nursing Teachers. Work experi-ence for the subjects included in this groupranged from 1 to 33 years, the average timebeing 9 years. A large number of the subjects(51%) had completed the 2-year basic nursing
programme, while others (43%) had taken theirnursing education in a 2i-year programme. Aminority (6%) had qualified before 1966through a 3-year nursing programme. The meanage of all subjects was 35 years (range 21-56;SD=7.64).
The student nurse group consisted of 197subjects who were recruited from six differentschools of general nursing education (2-year)within a region in central Sweden. Their agesranged from 20 to 51 with a mean age of 29 years(SD=7.97). Both nurses and student nursegroups included 6% men.
Thirty-six physicians with an average workexperience of 15 years, in different health carefields including medical wards and children'swards, completed a questionnaire about statu-tory regulations on drug prescription. The posi-tions held by the physicians in the health caresystem varied from the head of a medical de-partment to an intern.
Procedure
Permission to perform the test was soughtand obtained from the directors of the schoolsof nursing in Sweden. Seven of the directorsanswered that it was not possible to administerthe test because of time and schedule restric-tions and declined to participate.
No individual was compelled to participate.There were 32 individuals (5%) who declined toparticipate and 75 individuals (12%) were ab-sent, due to illness or other causes, when thetest was performed. The length of the test wasset for 2 hours and the test was completed undersupervision. The use of calculators was notallowed.
The test consisted of 14 items* categorizedinto subgroups such as, calculation of percent-ages, dosage calculation of liquid and soliddrugs as well as tablets, transformation of units,and calculation of time for giving intravenousfluids and infusions. The instrument was basedon items from examples in textbooks and itemsthat had been used earlier in the further edu-cation of nurses. Thus, the test items were notconstructed specifically for this study. The max-imum score was 14 and each test item had thesame relative value in the scoring procedure.
* A copy of the test items is available from the author by request.
at University of M
ichigan on October 19, 2014
http://intqhc.oxfordjournals.org/D
ownloaded from
Skills in calculating drug dosage 391
Pwctntag* ol «nsw»racorracty solved „
10-
Nurses
Student nurses
1 2 3 « 5 6 7 8 9 1 0 1 1 1 2 1 3 1 4 Number ol items
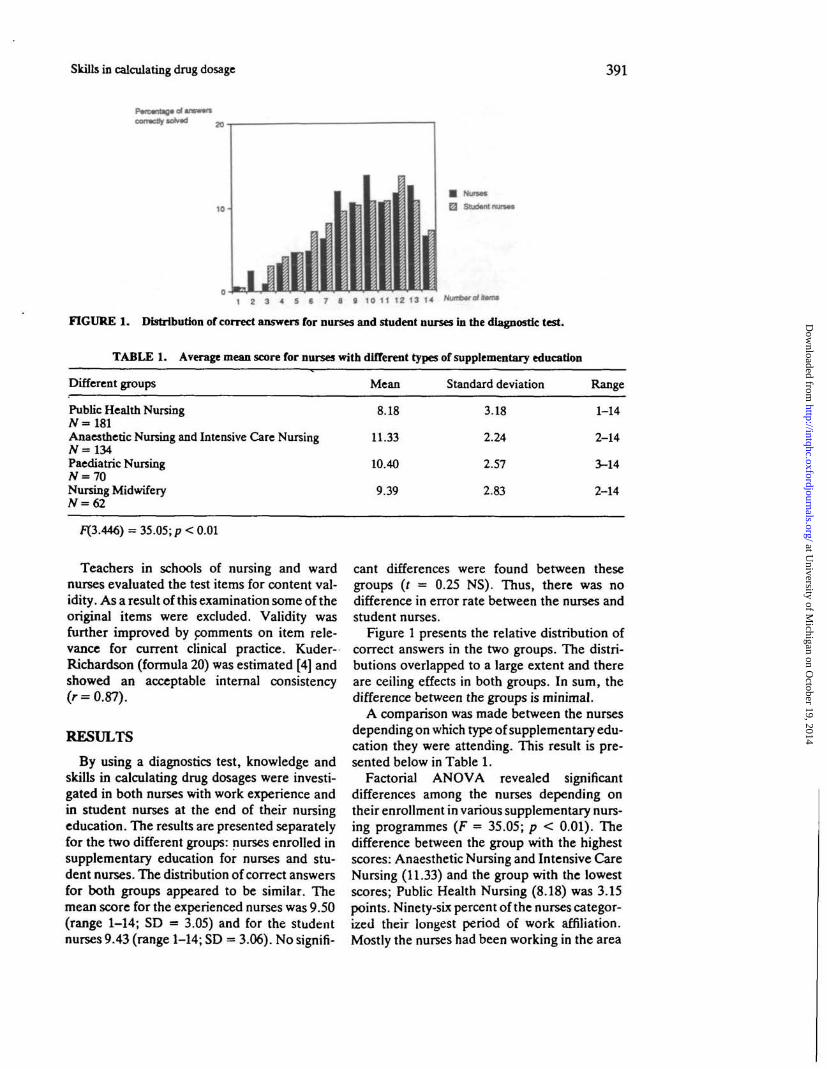
FIGURE 1. Distribution of correct answers for nurses and student nurses in the diagnostic test.
TABLE 1. Average mean score for nurses with different types of supplementary education
Different groups Mean Standard deviation Range
Public Health NursingTV =181Anaesthetic Nursing and Intensive Care Nursing
Paediatric NursingN = 70Nursing MidwiferyN=62
8.18
11.33
10.40
9.39
3.18
2.24
2.57
2.83
1-14
2-14
3-14
2-14
i=X3.446) = 35.05; p< 0.01
Teachers in schools of nursing and wardnurses evaluated the test items for content val-idity. As a result of this examination some of theoriginal items were excluded. Validity wasfurther improved by comments on item rele-vance for current clinical practice. Kuder-Richardson (formula 20) was estimated [4] andshowed an acceptable internal consistency(r = 0.87).
RESULTS
By using a diagnostics test, knowledge andskills in calculating drug dosages were investi-gated in both nurses with work experience andin student nurses at the end of their nursingeducation. The results are presented separatelyfor the two different groups: nurses enrolled insupplementary education for nurses and stu-dent nurses. The distribution of correct answersfor both groups appeared to be similar. Themean score for the experienced nurses was 9.50(range 1-14; SD = 3.05) and for the studentnurses 9.43 (range 1-14; SD = 3.06). No signifi-
cant differences were found between thesegroups (r = 0.25 NS). Thus, there was nodifference in error rate between the nurses andstudent nurses.
Figure 1 presents the relative distribution ofcorrect answers in the two groups. The distri-butions overlapped to a large extent and thereare ceiling effects in both groups. In sum, thedifference between the groups is minimal.
A comparison was made between the nursesdepending on which type of supplementary edu-cation they were attending. This result is pre-sented below in Table 1.
Factorial ANOVA revealed significantdifferences among the nurses depending ontheir enrollment in various supplementary nurs-ing programmes (F = 35.05; p < 0.01). Thedifference between the group with the highestscores: Anaesthetic Nursing and Intensive CareNursing (11.33) and the group with the lowestscores; Public Health Nursing (8.18) was 3.15points. Ninety-six percent of the nurses categor-ized their longest period of work affiliation.Mostly the nurses had been working in the area
at University of M
ichigan on October 19, 2014
http://intqhc.oxfordjournals.org/D
ownloaded from
392 I. D. Kapborg
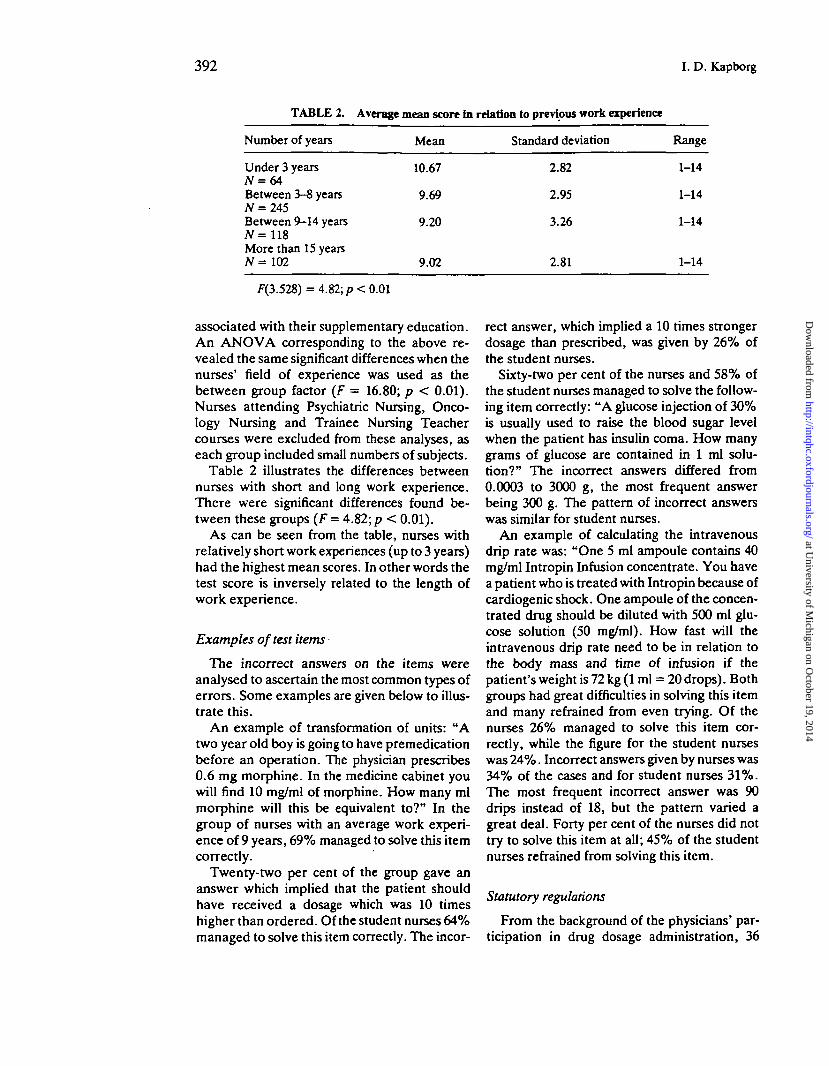
TABLE 2. Average mean score in relation to previous work experience
Number of years
Under 3 years
Between 3-S yearsN = 245Between 9-14 yearsN= 118More than 15 yearsN= 102
Mean
10.67
9.69
9.20
9.02
Standard deviation
2.82
2.95
3.26
2.81
Range
1-14
1-14
1-14
1-14
f(3.528) = 4.82; p< 0.01
associated with their supplementary education.An ANOVA corresponding to the above re-vealed the same significant differences when thenurses' field of experience was used as thebetween group factor (F = 16.80; p < 0.01).Nurses attending Psychiatric Nursing, Onco-logy Nursing and Trainee Nursing Teachercourses were excluded from these analyses, aseach group included small numbers of subjects.
Table 2 illustrates the differences betweennurses with short and long work experience.There were significant differences found be-tween these groups (F = 4.82; p < 0.01).
As can be seen from the table, nurses withrelatively short work experiences (up to 3 years)had the highest mean scores. In other words thetest score is inversely related to the length ofwork experience.
Examples of test items
The incorrect answers on the items wereanalysed to ascertain the most common types oferrors. Some examples are given below to illus-trate this.
An example of transformation of units: "Atwo year old boy is going to have premedicationbefore an operation. The physician prescribes0.6 mg morphine. In the medicine cabinet youwill find 10 mg/ml of morphine. How many mlmorphine will this be equivalent to?" In thegroup of nurses with an average work experi-ence of 9 years, 69% managed to solve this itemcorrectly.
Twenty-two per cent of the group gave ananswer which implied that the patient shouldhave received a dosage which was 10 timeshigher than ordered. Of the student nurses 64%managed to solve this item correctly. The incor-
rect answer, which implied a 10 times strongerdosage than prescribed, was given by 26% ofthe student nurses.
Sixty-two per cent of the nurses and 58% ofthe student nurses managed to solve the follow-ing item correctly: "A glucose injection of 30%is usually used to raise the blood sugar levelwhen the patient has insulin coma. How manygrams of glucose are contained in 1 ml solu-tion?" The incorrect answers differed from0.0003 to 3000 g, the most frequent answerbeing 300 g. The pattern of incorrect answerswas similar for student nurses.
An example of calculating the intravenousdrip rate was: "One 5 ml ampoule contains 40mg/ml Intropin Infusion concentrate. You havea patient who is treated with Intropin because ofcardiogenic shock. One ampoule of the concen-trated drug should be diluted with 500 ml glu-cose solution (50 mg/ml). How fast will theintravenous drip rate need to be in relation tothe body mass and time of infusion if thepatient's weight is 72 kg (1 ml = 20 drops). Bothgroups had great difficulties in solving this itemand many refrained from even trying. Of thenurses 26% managed to solve this item cor-rectly, while the figure for the student nurseswas 24%. Incorrect answers given by nurses was34% of the cases and for student nurses 31%.The most frequent incorrect answer was 90drips instead of 18, but the pattern varied agreat deal. Forty per cent of the nurses did nottry to solve this item at all; 45% of the studentnurses refrained from solving this item.
Statutory regulations
From the background of the physicians' par-ticipation in drug dosage administration, 36
at University of M
ichigan on October 19, 2014
http://intqhc.oxfordjournals.org/D
ownloaded from

Skills in calculating drug dosage 393
physicians answered a questionnaire about theirknowledge of statutory regulations concerningthe prescription of drugs. Only 19 out of 36physicians knew who is responsible for drugadministration. They also had difficulties indescribing the content of a correct prescriptionorder. In exceptional cases a physician can givea person, other than a nurse, the responsibilityof drug administration. Three subjects werefamiliar with these rules. Six physicians did notknow that they had the right to give prescrip-tions orally. Ten out of 36 physicians had pre-vious experience from situations with errone-ously administered drugs. Thus, the answersrevealed that physicians have an unacceptablelevel of knowledge in this area.
DISCUSSION
This study is based on the conclusions of anearlier study [1] which showed that studentnurses have severe difficulties in solving math-ematical items in areas essential to their work.Previous research has also found that nurses inclinical settings make errors when performingdrug dosage calculation [5,6]. The results in thisstudy revealed that approximately 90% ofnurses and student nurses who performed thetest failed to solve all items correctly. In gen-eral, both groups solved nine items out of four-teen correctly. It is somewhat surprising thatthere was no difference between the twogroups. However, this finding is supported byother studies. Two examples can be given.Laverty [5] suggested that "The poor perform-ance of trained staff in calculating drug dosescould be due to their forgetting the skills due tolack of recent practice." (p.36). Perlstein et al.[6] claimed that "It was somewhat surprising todiscover that experienced nurses did not havebetter computational skills than inexperiencednurses." (p.379).
The present study also investigated the per-formance of nurses' knowledge and skills incalculating drug dosages in relation to the num-ber of years of earlier work experiences. It wasfound that subjects with a longer work experi-ence performed worse than those with less ex-perience.
The results showed that there is a differencebetween the nurses, associated with the type ofsupplementary education they are attending.
The highest score was obtained by nursesenrolled in Anaesthetic Nursing and IntensiveCare Nursing education. The result also re-vealed that nurses with work experience in thefields of Anaesthetic Nursing and IntensiveCare Nursing had the highest mean score com-pared to nurses with work experiences fromother fields.
However, these nurses may have been betterprepared in mathematics before they enteredthe general nursing education. The lowest aver-age score was found for nurses in Public HealthNursing. The nurses enrolled in this educationhad the longest work experiences of all subjectsand they also were the oldest in age.
The physicians' answers to the questionnairerevealed that most of them were not entirelyfamiliar with the statutory regulations for drugprescription. Because of the physicians' prac-tice of prescribing an exactly stated drug dosageon the medicine card, there is a risk that nurseswill not take an active part in drug adminis-tration. If nurses do not understand the import-ance of their role, it might be hazardous for thepatients. Nurses must realize that they arelegally responsible for the drugs- they adminis-ter. It could be mentioned that one group ofnurses in Public Health Nursing educationwrote a letter to the investigator suggesting thatthis study is unnecessary because they did nothave to do any calculations in their work. In-stead they claimed that this is the sole responsi-bility of physicians.
Student nurses should gain a mastery level of100% in correctly solving drug dosage calcu-lations during their education before they canbe considered competent to administer drugs ontheir own. This is an example of quality assur-ance in nursing education, where the standardlevel is 100% correctly solved items. If this testhad been a regular examination for these stu-dent nurses, there would have been 93% of thesubjects who were required to retake the exam-ination. Thus, it is surprising to find that studentnurses just about to graduate have insufficientcompetence in calculation of drug dosages. Thismay be due to a variation in time spent oncalculating drug dosages during nursing edu-cation. The scheduled time has been investi-gated earlier [2] and it showed a large variationin this respect.
Unfortunately, data on scheduled teaching
at University of M
ichigan on October 19, 2014
http://intqhc.oxfordjournals.org/D
ownloaded from
394 I. D. Kapborg
time for training calculation has not been col-lected in the present study. However, it issuggestive that the nursing education in Swedenhas not been successful so far in preparingstudent nurses in this area for their work in thehealth care system.
If these results were applied to the practice ofhealth care it must be presumed that nursesadminister inappropriate dosages of drugs topatients. In addition there may be more press-ure on nurses in clinical settings than in a testsituation because of workload and the patients'conditions. The risk for incorrect calculationscould, therefore, increase in clinical settings.
Nurses are taught drug dosage calculationsduring their nursing studies, and they are conse-quently expected to be competent in this field.This study has shown that nurse education doesnot prepare all student nurses to perform drugdosage calculation accurately. Therefore, it isnecessary to study drug dosage calculation moreclosely in realistic work situations. The teachingmethods need to be changed emphasizingunderstanding. If student nurses understand theproblem underlying the figures, they will prob-ably be able to determine what is required andwill also recognize if the calculated dose isreasonable. The nursing teachers are importantas role models and must be competent in thisarea so that they are able to deepen and extendthe student nurses' knowledge.
Sometimes nurses claim that the use of calcu-lators will help them solve drug dosage items.However, Pieri [7] found that:
"The advent of the pocket calculator has not elimi-nated the need for mental arithmetical skills sincethere are many occasions in nursing when use of acalculator is inappropriate. Even when using acalculator the nurse should be able to judgewhether the answer to her calculation is reasonablebasing her decision either on past experience or onmathematical estimation." (p. 31).
It could also happen that the physician pres-cribes the correct drug doses but the nurse givesthe patient a wrong dose. Therefore the collab-oration between physicians and nurses is veryimportant. In some cases it could be crucial forthe patient's safety in the health care system.
In conclusion, the factors that may influencefaulty administration of drug dosages from themedicine cabinet to the patient are numerous.In this study the focus has been the calculation
ability of student nurses and nurses. All of themmust be aware of the need for accuracy incalculating drugs. Nursing education is one wayto ensure the nurses' knowledge in this area.Another important factor is the admissionrequirements to nursing education. If studentshave a good preparation in mathematics beforeentering their nursing education, it will prob-ably be easier for them to understand the calcu-lation of drug dosages. They must be able todeal with realistic situations, not only with idealones in classrooms.
Nurses cannot rely only on the physicians'written prescriptions and the figures shown onthe calculator. They must take the responsibi-lity for accurately, quickly and efficiently calcu-lating drug dosages. One way to accomplish thisis to take remedial courses continually.
Another way of improving these skills is touse a study guide or self study workbook whichcan be developed by the clinical units, focusingon the drug dosage calculation for a specificarea. Computer assisted learning can beanother aid for nurses. Feedback is an essentialcomponent of the learning situation. In the end,to secure a patient's safety, nurses must beaccurate in their use of mathematical conceptsto interpret data and their ability to use com-puters and other information technology com-petently in order to analyse problems. Takinginto account the results of this study, furtherresearch is needed on medication errors, thestatutory regulations on drug administrationand the capacity of physicians to apply theseregulations.
Acknowledgements: I would like to thank my per-sonal supervisor, Professor Siv Fischbein, for hergreat interest in and support of my work as well as herconstructive criticism.
REFERENCES1. Kapborg I, An evaluation of the mathematical
skills of beginner Swedish nurse students. Qual.Assurance in Health Care 4: 311,1992.
2. Kapborg I, An evaluation of Swedish nurse stu-dents' calculating ability in relation to their earliereducational background. (In Swedish: "SjukskS-terskestuderandes matematikkunskaper vid b6r-jan av sina studier med avseende pa olika utbildn-ingsbakgrund samt 15kemedelsrakningensutformning under utbildningstiden"). Report1993:6; VardhOgskolan, Vasteris, 1993.
at University of M
ichigan on October 19, 2014
http://intqhc.oxfordjournals.org/D
ownloaded from

Skills in calculating drug dosage 395
3. Willow K, (Ed.) Statutory Regulations Textbookfor Personnel in the Health Care System. (InSwedish: Fdrfattningshandbok, F6r personalinom halso- och sjukvarden). Almqvist & Wiksell,Uppsala, 1993.
4. Waltz C, Strickland O and Lenz E, Measurementin nursing research (2nd Edn). F.A. David Com-pany, Philadelphia, 1991.
5. Laverty D, Accuracy of nurses' calculations.Nursing Standard 3: 34, 1989.
6. Perlstein P, Callison C, White M, Barnes B andEdwards N, Error in drug computations duringnewborn intensive care. Am J Dis Children 133:376,1979.
7. Pieri S, Nurses and mathematics; deficiencies inbasic mathematical skills among nurses. Develop-ment and evaluation of methods of detection andtreatment. Whitefriars Press, London, 1987.
at University of M
ichigan on October 19, 2014
http://intqhc.oxfordjournals.org/D
ownloaded from