Embed Size (px)
Citation preview

A o t a P a t h . J a p . 29(2): 251-257, 1979
CARCINOMA IN HETEROTOPIC GASTRIC PANCREAS
Akira TANIMURA*, Hideo YAMAMOTO**, Hidenori SHIBATA**, and Eijiro SANO***
* Second Department of Pathology, Kurume University School of Medicine ** Second Department of Surgery, Kurume University School of Medicine
*** Second Department of Internal Medicine, Kurume University School of Medicine
(Received on June 29, 1978)
A case of a 55-year-old Japanese female who died of adenocarcinoma originating from heterotopic gastric pancreas is presented. The autopsy revealed, extensive metastases of bones. Though careful examination was done, other primary focus except that of the stomach could not be detected. In review of literatures, 11 malignant tumors originating from heterotopic gastric pancreas could be found including our case. ACTA PATH. JAP. 29: 251-257, 1979.
Introduction
Gastric carcinomas originate from gastric polyp, gastric ulcer, chronic gastritis and In these lesions, malignant transformation from heterotopic
Since the first report by GOLDFARB and associates4 in 1963
This paper reports a case of malignant transformation from heterotopic gastric
heterotopic pancreas. pancreas is extremely rare. we could find only a few cases in review of Japanese and English literatures.
pancreas (Heinrich I1 +III type) in the pyloric area with extensive bone metastasis.
Case Report
A 55 years old Japanese female entered the hospital because of hemorrhagic diathesis from the gum. One month before admission, an episode of continued bleeding from the gum occurred without any cause. Two months previously she had experienced severe lumbago, and subsequently she became unable to walk because of severe pain of the right leg. She had received appendectomy a t the age 45 years. She was troubled by gastric discomfort (gastritis) for the past 2 years and had received treatment.
Physical examination showed a thin, pale women, with few subcutaneous hemorrhages on both legs. Temperature was 37.1°C, pulse 92, and respiration 24. Blood pressure was 100 systolic, 50 diastolic.
Superficial lymph nodes were not palpable. X-ray h s of the upper gastrointes- tinal series showed figures of chronic gastritis. After admission, hemorrhagic diathesis and severe anemia continued and blood transfusion (2400 ml) was given. Malaise became progressively worse.
G';F.f #A, l4* %E, %63 wu, E% %=?a Directed by Prof. T. N A K A S ~ A .
251
252 CARCINOMA IK HETEROTOPIC GASTRIC PANCREAS Acta Path. Jap.
In spite of detailed gastrointestinal examination, no lesions were found in the G.I. series. Although sternal punctures were performed 3 times, bone marrow tissue could not be aspirated. However, the iliac bone marrow revealed PAS positive malignant tumor cells.
X-ray films of the scalp and lumbar vertebrae revealed many punctuated destructive bone lesions. One months after admission, lumbar pain became more marked, and she could no longer walk. Headache, nausea and stiffneck developed and sub- sequently she became comatose and died.
The origin of metastasis into bones could not be found.
Autopsy Finding
The patient was a poorly nourished, emaciated 55 years old Japanese female. An autopsy was done about 3 hours after death. No operative incision or other external skin change such as petechia was present.
Conj. pal. was anemic and C. bulbi was not icteric. Superficial lymphadenopathy was not present.
On opening the abdominal cavity there were few ml of light yellow colored ascites. The peritoneum and serosa of intestinal tract were smooth and shiny. The pericardial sac contained few ml of clear yellow fluid. Thoracic cavity: The left thoracic cavity was partially obliterated by fibrous tissue and contained no fluid. Stomach: The gastric
Both pupils were round and symmetric. The mouth, ear and nose were not remarkable.
Thorax was symmetrical.
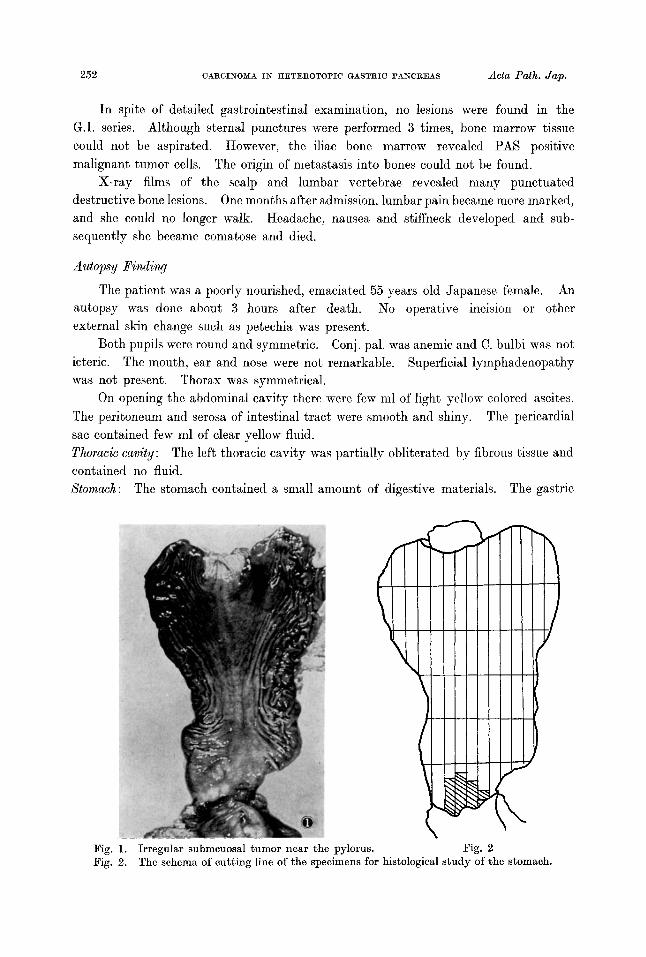
The stomach contained a small amount of digestive materials.
I
Big. 2 Pig. 1. Fig. 2.
Irregular submcuosal tumor near the pylorus. The schema of cutting line of the specimens for histological study of the stomach.
29(2): 1979 A. TANIMURA et ol. 253
mucosa was slightly atrophic, and an irregular-shaped submucosal tumor measuring 0.5 x 2 x 2 cm was present near the antrum to the pyloric ring (Figs. 1, 2). The overlying mucous membrane was uneven with no ulcer. The serosal surface of the above tumor showed an irregular protrusion. On cut-section, the tumor tissue was partially grayish-white and extended from the submucosal layer to the serosa. Further- more the blocks of No 5, No 6 were cut into serial sections. Heart (260 g) : The epicardium was normal and the myocardium was reddish brown in color. Lung (r; 210 1:180 g): The external surface of the left lung was covered by dense fibrous tissue. The pulmonary arteries were not remarkable. Liver (1070 g) : The cut-surface showed normal architecture. The gall bladder and common duct was not remarkable. Spleen (85 g): Multiple cross sections showed dark-red splenic tissue with fibrosis. Kidney (r. 130, 1.135 g): The capsule was stripped with ease revealing a smooth surface. The cut-surface showed a distinct cortico-medullary junction with the cortex measuring 5 mm in thickness. The cortex in the left kidney had a whitish-gray, round fibroma measuring 3.5 mm in diameter. The pelvis was not dilated and no focal lesions were found. Partereas: The parenchyma had a distinct lobular architecture. Multiple cross sections showed no focal lesions. Skeletal system : The sternum, scalp, ribs and lumbar vertebrae showed grayish-white osteolytic lesions measuring 1 N 10 mm in size. These nodular lesions were scattered throughout the medullary cavity without destruction of the bone trabeculae. Bone marrow tissue surrounding tumor nodules was dark-red in color which suggested a hyperplastic bone marrow. Brain. (weight 1100 g): Subcutaneous hemorrhage in the scalp was seen but not severe. Destruction of the skull as observed on X-ray film was not apparent macroscopically. A fresh subarachnoidal hemorrhage was seen and both hemispheres were markedly edematous but symmetric.
On the cut-surface through the mammillary body, there was a hemorrhagic lesion measuring 0.5 x 0.5 cm in diameter in the septum pellucidum. A focal hemorrhagic lesion (0 .5~1 .3 cm in diameter) was also found in the medulla of cerebellum. The basal nuclei, pontine, medulla oblongata and spinal cord revealed no focal lesions.
The duodenum was not involved.
The stomach was cut into step-sections a t intervals of 0.5 cm.
There was no scar or hemorrhage in the myocardium.
The cut-surface of all lobes was congested.
The external surface was smooth with no focal lesions. The intra-hepatic duct was not dilated.
The capsule was wrinkled and thickened.
The genitn-urinary system was not remarkable. The pancreas was normally located and normal in size.
Microscopic Examination
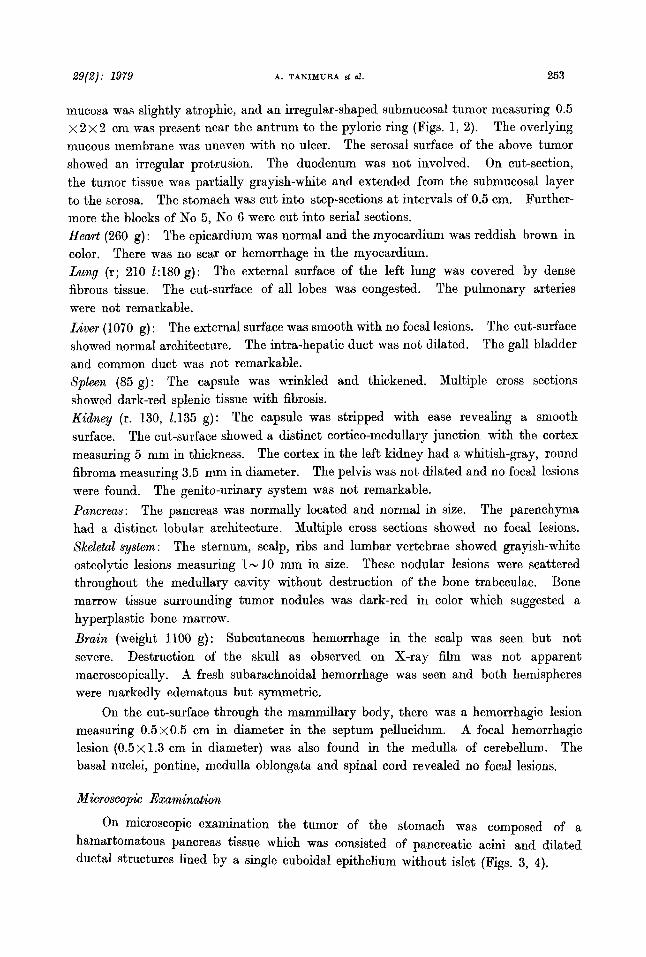
On microscopic examination the tumor of the stomach was composed of a hamartomatous pancreas tissue which was consisted of pancreatic acini and dilated ductal structures lined by a single cuboidal epithelium without islet (Figs. 3, 4).
254 Actu Path. Jap. CARCINOMA I N HETEROTOPIC GASTRIC PANCREAS
29(2): 1979 A. TANIMURA et al. 255
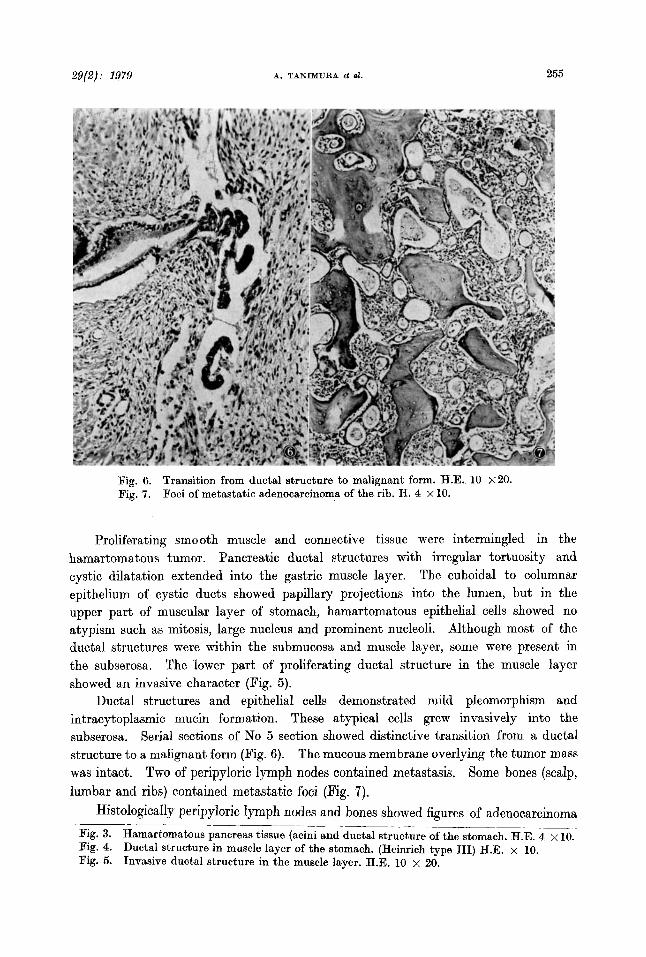
Fig. 6. Fig. 7.
Transition from ductal structure to malignant form. H.E. 10 X20. Foci of metastatic adenocarcinoma of the rib. H. 4 x 10.
Proliferating smo 0th muscle and connective tissue were intermingled in the hamartomatous tumor. Pancreatic ductal structures with irregular tortuosity and cystic dilatation extended into the gastric muscle layer. The cuboidal to columnar epithelium of cystic ducts showed papillary projections into the lumen, but in the upper part of muscular layer of stomach, hamartomatous epithelial cells showed no atypism such as mitosis, large nucleus and prominent nucleoli. Although most of the ductal structures were within the submucosa and muscle layer, some were present in the subserosa. The lower part of proliferating ductal structure in the muscle layer showed an invasive character (Fig. 5).
Ductal structures and epithelial cells demonstrated mild pleomorphism and intracytoplasmic mucin formation. These atypical cells grew invasively into the subserosa. Serial sections of No 5 section showed distinctive transition from a ductal structure t o a malignant form (Fig. 6). The mucous membrane overlying the tumor mass was intact. Two of peripyloric lymph nodes contained metastasis. Some bones (scalp, lumbar and ribs) contained metastatic foci (Fig. 7).
Histologically peripyloric lymph nodes and bones showed figures of adenocarcinoma
Fig. 3. Hamartomatous pancreas tissue (acini and ductal structure of the stomach. H.E. 4 x 10. Fig. 4. Ductal structure in muscle layer of the stomach. (Heinrich type 111) H.E. x 10. Fig. 5. Invasive ductal structure in the muscle layer. H.E. 10 x 20.
- - _ _ _ ~ __~___ ___-__

256 CARCINOMA I N RETEROTOPIC GASTRIC PANCERAS Acta Path. J q .
tubulare-mucocellulare similar to that of the stomach. Detailed studies of the gastrointestinal tract, genito-urinary system, etc. revealed no other primary lesion except that of the stomach. Microscopically, a few tumor emboli were seen in the pulmonal artery, but no metastatic lesions were found in any other organs.
Discussion
Heterotopic pancreatic tissue of the stomach is very common and its frequency varies from 0.6 to 5.6% of autopsy cases. The most common location is in the stomach, duodenum and jejunum, where the incidence is almost 70%223 In the majority of the cases reported as well as in our case most of the location was found near the antrum to pyloric area (82.2%). Heterotopic pancreatic tissue usually reveals itself as a single, firm lobulated, irregular node measuring up to 5 cm in diameter. A large mass over 5 cm may be found.
The histologic picture of heterotopic pancreatic tissue is the same as that of normal pancreas, with lobule-formation including glandular acini, ducts and islets of Langerhans. There may, however, be a lack of one or more histologic element of normal tissue such as acinar structure, duct and islet. HEINRICII (1909) classified heterotopic pancreas into 3 types; type I consists of normal pancreatic elements, type I1 of acini and ducts without islet of Langerhans, type I11 of proliferating smooth muscles and ductal structures but no acinar structure and islet.
Cyst formation, hemorrhage, and neoplastic change are found in heterotopic gastric pancreas. Though malignancy of heterotopic pancreas (gastric) is a very rare condition, there are 11 cases including doubtful cases in reviewing Japanese and English literatures1-'. According to the study of 400 cases of resected gastric carcinomas, INOUE et aL5 reported that malignant change from heterotopic pancreas of the stomach was found in only 3 cases (0.8%). It is very difficult to determine whether malignant change developed from pre-existing heterotopic pancreas or not. For the evidence that the malignant tumor has undoubtedly developed from heterotopic pancreas, one must ascertain the direct transition from heterotopic pancreastic tissue into carcinoma in serial sections. Malignant change of heterotopic pancreas can occur from incomplete ductal element (so-called adenomyoma) which shows atypical proliferation of ductal epithelium. In our case, the tumor revealed malignant transformation from adenomyomatous foci in serial sections. The extent of primary cancerous area in the stomach was small, as compared to the extent of bone metastases. Myelophthisic
anemia and hemorrhagic diathesis had occurred by extensive bone marrow metastases, and the patient died of subarachnoidal hemorrhage.
The ratio of male to female is 2 to 1.
Our case consisted of type I1 + I11 of Heinrich's classification.
Acknowledgement: The authors thank Prof. T. NAEASFEMA for his advice and criticism.
References
1. ACKERMAN, L.V.: Heterotopic Pancreas. Surgical Pathology. 4th Ed. p. 336, C.V. Mosby Co. St. Louis, 1968.
29(2): 1979 A. TANIMURA et al. 257
2.
3.
4. 5.
6.
7.
8.
BARBOSA, J.J. et al.: Pancreatic heterotopia. Review of the literature and reprots of authenticated surgical case, of which were clinically significant. Surg. Gynec & Obst. 28: 527, 1964. BRANCH, C.D. and GROSS, R.E. : Aberrant pancreatic tissue in the gastrointestinal tract. Arch. Surg. 31: 200, 1935. GOLDFARB, W.B. et al.: Carcinoma in heterotopic gastric pancreas Ann. Surg. 158: 56, 1963. INOUE, N. : Gastric carcinoma originated from heterotopio gastric pancreas, The Journal of Juzen Medical Society 56: 838, 1954. MIYAMOTO, S. : A case of gastric carcinoma arising heterotopic pancreas tissue in the stomach. Journal of Osaka Medical College. 27 : 44, 1968. MURATA T., et al.: Two cases of early carcinoma of the stomach, suspected of malignant change of aberrant pancreatic tissue in the gastric wall. Japan Journal of Cancer Clinics. 15: 815, 196 NAGAYO, T., et al.: Histopathological findings of the aberrant pancreas in the gastric wall. Stomach and Intestine 5: 1423, 1970.










![International Journal of Clinical EndocrinologyTh e heterotopic pancreas is histologically divided into three types, according to von Heinrich’s classifi cation [1]. Type I had ducts,](https://img.pdfslide.net/doc/110x75/5f4b2d8546fe527db76dd962/international-journal-of-clinical-endocrinology-th-e-heterotopic-pancreas-is-histologically.jpg)