Embed Size (px)
Citation preview
H A I N E S - - C A R C I N O M A OF H E A D OF P A N C R E A S W I T H O U T J A U N D I C E 683
will usually admit the prolonged use of cascara or one of the other cathar t ics .
Of the twelve cases observed, eight had taken cascara f requent ly and other laxatives, only one was quite emphat ic tha t none of the group had been used. The ages of the pa t i en t s ranged between 30 and 66. One was a colored male ; all the others were white. There were six males and six females. In one case, a man of 66 years of age, the condi t ion was associated wi th divert iculosis of the sigmoid.
There is little to be said so f a r as the t r e a t m e n t is concerned, except the wi thdrawal of an th racene ca- thar t ics and correction of the cons t ipa t ion usual ly will
be rewarded by d isappearance of the p igmenta t ion . I t has been es t imated t ha t three to six months is re- quired. This is approximate ly the period observed in our cases.
SUMMARY
Twelve cases of Melanosis Proctocoli have been re- ported. While the condi t ion is relat ively uncommon, it is by no means as i n f r e q u e n t as usual ly considered. The fact tha t it only can be visualized by sigmoido- scopy, aga in emphasizes the impor tance of a complete examina t ion of the rec tum and sigmoid in all cases coming unde r observat ion.
R E F E R E N C E S 1. Cruveilhier, $ . : Anatomle pathologique du corps. Paris, Humane, 14. Lignac, G. O. E. : Ueber sogenarinte "melanosis coll." Krank-
19:6, 1829. 2. Virchow, R.: Die pathologischen pigmente. Virchow's Archly.,
1, 1847. 3. Solger, F. B.: nickdarmmelanosc, Inaug. Diss Greifswald, 1898. 4. Pick, L. : Uber melanose der dickdarmschleimhaut. Berlin, kllnische
Wochenschrift, 19:840, May, 1911. 5. Yeomans, F. C.: Proctology. 2nd ed., p. 101. A. D. Appleton, N.
Y., 1935. 6. Stewart, N. J . and Hickman, E. M.: Melanosis Coli. Jour. Path.
and Bact., 34:61, Jan., 1931. 7. Battle, H. J . : Sigmoid; Anatomy, Physiology Examination and
Pathology. Med. Jour. and Record, 27:521, May 15, 1928. 8. Bockus, I t . L. : Willard, J. H. and Banks, J . : Melanosis Coli.
The Etiologic Significance of Anthracene Laxatives. Report cf 41 cases. J . A. M. A., 101:1, July 1, 1933.
9. ttueck, W.: Pigment studien. Beltr. z. path. anat., 54:160, 1912. 10. Synnott, M. J . : Melanosis coil Tr. Amer. Proc. Soc., p. 122, 1934. 11. Obendorfer, F. : Die pathologischen pigmente. Ergebn d. AUg.
Path. U. path. anat., 19:124, 1921. 12. Pitt, G. N.: Colon Pigmented Black Throughout with Lead. Tr.
Path. Soc., London, 42:109, 1891. 13. Rolleston, R. D.: Colon Pigmented with Mercury. Tr. Path. Soc.,
London, 43:69, 1892.
heitsyorshung, 2:162, Dec., 1925. 15. l~cFarland, W. L. : Pigmentation of the Hindgut a Pathological
and Experimental Study. J. A. M. A., 619:1946, Dee. 8, 1917. 16. Lynch, J . M.: Diseases of the Rectum. Leo & Febiger, Phila.,
p. 374, 1914. 17. Bockus, I t . L. : Discussion Melanosis Coll. Tr. Amer. Proc. Sot.,
p. 125, 1934. 18. Williams, C. T. : Black Deposit in Large Intestine from Presence
of Mercury. Tr. Path. Soe., London, 18:11, 1857. 19. noyd, W.: A Text Book of Pathology. 2nd ed., p. 42. Lea &
Febiger, Phila., 1934. 20. Bland-Sutton, J . : Tumors Innocent and Malignant. 7th, ed., p.
123. Cassel & Co., London, 1922. 21. Bland-Sutton, J . : Cancer of Duodenum and Small Intestine. Brlt.
Mcd. Jour.. 2:653, 1914. 22. Zobel, J . and Susnow, D. A. : Melanosis Coli Clinical Significance.
Arch. Surg.. 30:974, June, 1935. 23. Dalldorf, G. J . : Melanosis Coli. Beitr. z. path. anat. u. z. aUg.
path., 78:225, Aug., 1927. 24. ttenschen, F. and Bergstrand, H . : Studien uber die Melanose der
dickdarmschlcimhaut. Beltr. Path. Anat., 56:173, 1913. 25. Laidlaw, G. F. : Melanoma Studies. Amer. Jour. Path., 8:477,
Sept., 1932. 26. Wirth, E. H . : Pharmacogrosy. Lea & Febiger, Phila., 1936.
Carcinoma of Head of Pancreas Without Jaundice By
CHARLES HAINES, M.D. NEW YORK, NEW YORK
T H E most common symptom of an advanced carci- noma of the head of the pancreas is a deepening
jaundice . The carcinoma encroaches upon the common bile duct a t i ts ent rance into the duodenum d a m m i n g back the bile into the b i l i a ry system and caus ing jaundice . I t is safe to say tha t a diagnosis of carci- noma of the head of the pancreas would not be made unless the pa t i en t were jaundiced.
Thus i t seems tha t the following case repor t of a carc inoma of the head of the pancreas wi thout j aund ice may be of interest .
CASE R E P O R T M. W., 50 years of age, white, male, was first seen by
me October 12, 1934. According to the patient 's history he had been in good health until nine months previously. At that time he first noticed some discomfort in the upper abdomen which tended to come on after meals and which was not relieved by food. During these nine months the patient had had several attacks of nausea and vomiting. In spite of advice from his physician he had refused any satisfactory study of the gastro-intestinal tract.
About ten days before I first saw the patient, nausea and vomiting had become severe. The discomfort in the epigastrium became a constant pain. He was obliged to remain in bed. He could eat no solid foods and took only milk and cream.
At the time of my examination he was in acute distress.
During the half hour which I spent with him he vomited more than two quarts of dark green fluid.
Temperature was normal; pulse, 100 per minute. The tongue was dry and coated. The abdomen was markedly distended, especially across the epigastrium. There was no tenderness. No mass could be felt in the abdomen. No intestinal sounds were heard. Rectal examination showed no abnormality.
And there was no jaundice. I made a diagnosis of pyloric obstruction. The patient 's stomach was drained by means of a Wan-
gensteen tube. He was given large doses of 5% glucose intravenously and under the skin. He gradually improved.
A gastro-intestinal X-ray series was made. Films of the stomach and duodenum showed (1) a very large stomach; (2) a somewhat i rregular pyloric r ing; (3) considerable increase over the normal emptying time of the stomach; (4) a large six hour residue.
When the patient 's general condition had improved as much as possible under the treatment outlined above, I operated. At operation I found the glands along the greater and lesser curvatures of the stomach and along the vertebral column markedly enlarged and stony hard; they were obviously involved in a neoplastic process. The head of the pancreas was also enlarged and stony hard. It was impossible to ascertain definitely where the neo- plastic process had originated. The growth was pressing upon the duodenum in such a way as to cause a partial obstruction. I did a posterior gastro-enterostomy and re-
684 AMERICAN JOURNAL OF DIGESTIVE DISEASES
moved a lymph node which microscopically showed a metastatic carcinoma.
After operation progress was not satisfactory. X-ray treatments were tried but they caused marked nausea and vomiting and had to be discontinued. However, after some days the patient was able to be out of bed and was even able to shave himself.
During the next six weeks the patient grew steadily weaker, and he died January 1, 1935.
An autopsy showed that the original neoplasm had been in the head of the pancreas. It had encroached upon the duodenum and had caused an almost complete duodenal obstruction. It had also caused a complete obstruction of the common bile duct.
The fact that there had been no jaundice was explained as follows: at some time previous to his last illness, the patient had had a gall stone in the gall bladder. The stone had ulcerated into the duodenum and had established a sinus between the gall bladder and the duodenum. Bile
had drained through this sinus into the gastro-intestinal tract and was not dependent for a passageway on the common bile duct which was now occluded by the neoplasm. It had flowed freely into the duodenum distal to the ob- struction. Thus, a simple mechanical readjustment by Nature explains the phenomena of a Carcinoma of the Head of the Pancreas without Jaundice.
SUMMARY A patient with a very extensive and advanced carci-
noma of the head of the pancreas, which was proved by operation and autopsy, did not develop jaundice. Failure to develop jaundice was explained by the fact that at some previous time a sinus had formed between the gall bladder and the duodenum, thus allowing free drainage of the gall bladder into the duodenum, inde- pendently of the common bile duct which had been occluded by a carcinoma.
Calcium Gluconate and Kaolin in the Treatment of Bacillary Dysentery" By
BERNARD L. GREENE, M.D. ELGIN, ILLINOIS
and LOUIS H. BLOCK, M.D.
CHICAGO, ILLINOIS
O VER 1,000 cases of bacillary dysentery of Flexner type have been observed and treated by the
authors in the past two and one-half years. In a small percentage the acute phase became chronic, indis- tinguishable c l i n i c a l l y and proctoscopically from chronic ulcerative colitis, and as a rule persisted in spite of various treatments. In June, 1937, we decided to use the Haskell and Cantarow (1) method of calcium, kaolin and parathyroid extract treatment, first reported in 1931. However, before we were able to begin this study, our chronic cases had dwindled to two. We then proceeded to use this method in acute cases, modifying it by omitting belladonna and using our regular soft diet.
Since the patients under discussion are psychotic, it is usually impossible to obtain subjective information concerning the efficacy of treatment, and all conclu- sions were necessarily based upon objective findings. Fortunately, we had previously performed about four thousand proctoscopic examinations upon dysenteric cases and had observed the mucous membrane of the lower twenty-five centimeters of the large bowel in all phases of the disease. One of us, (L. H. B.) (2), had reported in a previous article that the infection ap- parently starts in the terminal ileum or cecum and travels downward, whereas when healing takes place it starts at the muco-cutaneous junction and always travels cephalad. Furthermore, the mucosal picttire invariably corresponds to the clinical picture, i.e. the more severe the infection, the more marked the mucosal change. We have graded the proctoscopic mucosal picture into four groups: One plus ( + ) where there is a mild hyperemia and no blood vessels visible; two plus ( + + ) where there is a moderate
* F r o m t h e " D ' e p a r t m e n t of Proctology, service of Dr. L. H. Block, Elgin Sta te Hospi ta l .
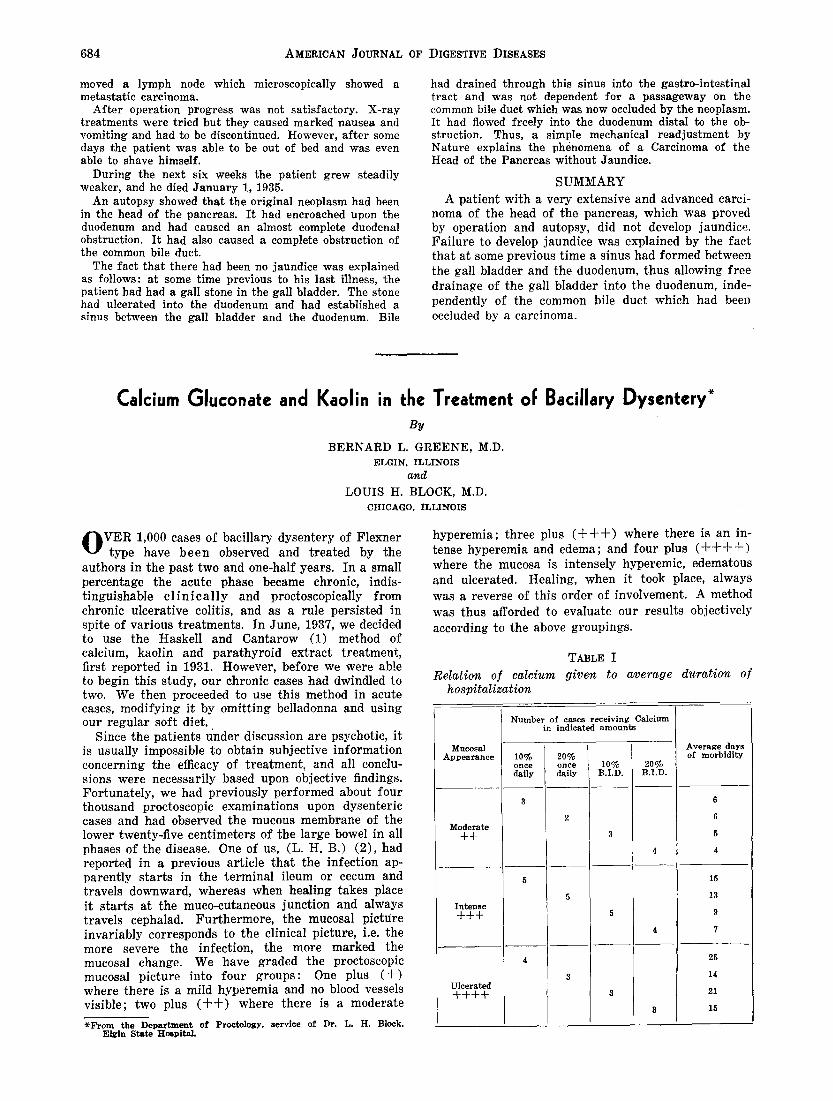
hyperemia; three plus ( + + + ) where there is an in- tense hyperemia and edema; and four plus ( + + - t - + ) where the mucosa is intensely hyperemic, edematous and ulcerated. Healing, when it took place, always was a reverse of this order of involvement. A method was thus afforded to evaluate our results objectively according to the above groupings.
TABLE I
Relation of calcium given to average hospitalization
duration of
Mucosal Appearance
Moderate ++
Intense + + +
Ulcerated +++-t-
Number of cases receiving Calcium in indicated amounts
10% 20% once once daily daily
10% B.I.D.
20% B.I.D.
Average days of morbidity
15
13
9
7
25
14
21
15