Embed Size (px)
Citation preview

Cardiac Effects of Acute Ethanol IngestionUnmasked by Autonomic Blockade
JOHN S. CHILD, M.D., RODNEY B. KOVICK, M.D.,
JORGE A. LEVISMAN, M.D., AND MORTON L. PEARCE, M.D.
SUMMARY We assessed the effects of ethanol and autonomic blockade on left ventricular function in ninenormal subjects, age 20-35 years, using M-mode echocardiography and systolic time intervals. On day 1, mea-surements were made of heart rate, mean velocity of circumferential fiber shortening, and left ventricular pre-ejection period and left ventricular ejection time ratio (PEP/LVET), during a control period and afterautonomic blockade. Autonomic blockade was produced with intravenous propranolol (0.2 mg/kg bodyweight) and atropine (0.04 mg/kg body weight). On day two, measurements were again made during a controlperiod, then with ethanol alone, followed by addition of autonomic blockade to ethanol. One hundred eightymilliliters of ethanol were ingested over 60 minutes, resulting in a mean blood ethanol level of 110 mg/dl (range77-135 mg/dl) at 60 minutes post-ingestion.
There were no significant differences between the control data on days 1 and 2. Blood pressure was un-changed throughout the study. On day 1, autonomic blockade alone resulted in the expected increase in heartrate (p < 0.001), with a proportional increase in mean velocity of circumferential fibr shortening (p < 0.01),and an increase in PEP/LVET (p < 0.01). On day 2, ethanol alone resulted in no significant changes exceptfor a slight increase in PEP/LVET (p < 0.02). Ethanol plus autonomic blockade, (day 2), compared withautonomic blockade alone (day 1), revealed a decrease in mean velocity of circumferential fiber shortening(p < 0.05), and an increase in PEP/LVET (p < 0.01), with a decrease in intrinsic heart rate (p < 0.001).We conclude that in normal subjects: 1) autonomic blockade does not directly affect contractility; 2) acute
ethanol ingestion alone does not produce important changes in cardiac function; and, 3) ethanol in theautonomic blockaded heart causes a significant decrease in contractility. Thus, we infer that ethanol has anegative inotropic effect which is masked by catecholamines and/or autonomic nervous system discharge.
CHRONIC INGESTION OF ETHANOL is knownto cause cardiac dysfunction, most notably as con-gestive cardiomyopathy.'-5 Cardiac function, as mea-sured by systolic time intervals, may be depressed evenin the clinically "normal" alcoholic.6 In addition, pa-tients with coronary heart disease have shown de-pressed hemodynamics,78 as well as decreased exer-cise tolerance with increased ischemic ST-segmentabnormalities and angina,9 after acute oral ingestionof moderate amounts of ethanol. Intravenous admin-istration of ethanol to dogs caused decreased coronaryflow and increased coronary resistance at all dosagelevels.10
However, the acute administration of ethanol todogs and to normal humans has resulted in conflict-ing reports of the effects on left ventricular (LV) func-tion.8' 11-22 Hemodynamic studies of dogs receivingintravenous ethanol infusions during autonomicblockade have shown myocardial depression.'2' 22Acute ethanol administration results in increased
hypothalamic activity23 and increased circulatingcatecholamines.24 26 Because catecholamines can in-crease cardiac contractility,27 they might "mask" in-trinsic myocardial depression by ethanol.12' 22
From the Division of Cardiology, Department of Medicine,University of California, Los Angeles, Los Angeles, California.
Supported in part by grant 490-IG2 from the American HeartAssociation, Greater Los Angeles Affiliate.
Address for reprints: John S. Child, M.D., Division of Car-diology, Department of Medicine, University of California at LosAngeles, Los Angeles, California 90024.
Received February 1, 1978; revision accepted August 30, 1978.Circulation 59, No. 1, 1979.
Autonomic blockade may therefore unmask myo-cardial dysfunction during ethanol ingestion.We therefore extended the study of the effects of
acute ethanol ingestion on LV function in normal sub-jects to include autonomic blockade.28' 29 Because ofvariations in vagal tone, we chose full autonomicblockade instead of g blockade alone. We used echo-cardiography as a tool for the evaluation of LV per-formance because it is a safe, reliable, and noninva-sive technique,30 38 which has been shown to bereproducible from day to day37 and to reflect ac-curately acute alterations in LV function.34 36
Systolic time intervals were also measured, usingthe ratio of the pre-ejection period to LV ejection time(PEP/LVET) as the most useful indicator (by thistechnique) of the function of the left ventricle.39 40This ratio is not significantly affected by changes inheart rate in the absence of changes in myocardialfunction.
MethodsSubjects
After detailed description of the study protocol,nine normal humans signed an informed consent formapproved by the University of California at LosAngeles Committee on Investigation InvolvingHuman Subjects. There were five men and fourwomen, with an age range of 20-35 years (mean 27.1years). All had normal medical histories, physical ex-aminations and baseline echocardiograms. They wereinfrequent users of alcohol, and were on nomedications. Each was studied after a 12-hour fast, in
120
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

ETHANOL AND AUTONOMIC BLOCKADE/Child et al.
the supine position, using M-mode echocardiographyand systolic time intervals.
Procedure
On day 1, control determinations of blood pressure(BP), heart rate (HR), mean velocity of circum-ferential fiber shortening (Vcf), and the PEP/LVETwere made after the subject had been resting supinefor at least 10 minutes.Autonomic blockade was then produced by the
method of Jose,28' 29 using a mixture of propranolol(0.2 mg/kg) and atropine (0.4 mg/kg) in a totalvolume of 20 ml, given intravenously over 2-3minutes. Five minutes after the end of this injection,the BP, HR, Vcf, and PEP/LVET were againrecorded, to be used as baseline information of theeffect of autonomic blockade alone on these param-eters. According to Jose and Taylor,29 completeblockade lasts 10-20 minutes, with essentially com-plete recovery by 100 minutes after injection. All sub-jects were closely observed for 2 hours after the pro-cedure. No complications developed.On day 2, 24 hours after autonomic blockade alone,
control measurements of BP, HR, Vcf, andPEP/LVET were performed as before. Upon com-pletion of these measurements, chilled ethanol(commercially available 80-proof Scotch whiskey;total 180 ml. 61.8 g of ethanol over 60 minutes) wasorally ingested in three doses at a rate of one doseevery 20 minutes. Sixty minutes after the ingestion ofthe first dose (20 minutes after the third dose), themean blood ethanol level was 110 mg/dl (range77-135 mg/dl), as measured by headspace gaschromatography.41' 42 Each subject appeared mildly
intoxicated. The BP, HR, Vcf and PEP/LVET wereagain recorded to determine the effect of ethanol alone(at a single blood level) on these parameters.Immediately upon completion of these measure-ments, autonomic blockade was again produced as onday 1, and the measurements repeated 5 minutes afterthe intravenous injection was completed.
Echocardiographic Measurements
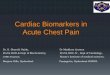
Echocardiograms were obtained with a Smith-KlineEkoline 20A Ultrasonoscope using a 10 cm focus 2.25MHz transducer with a repetition rate of 1000/sec.Tracings were made on a Honeywell 1856 recorder onKodak light sensitive paper at a speed of 50 mm/sec. Using standard techniques previously de-scribed, 30-38, 43-45 the transducer was placed in the third,fourth or fifth left parasternal intercostal space, andthe "standard interspace" was identified where thetransducer was perpendicular to the chest wall withoutinferior or superior angulation while being directedslightly medially to identify both mitral valve leaflets.The echoes of the interventricular septum and LVposterior wall were recorded at the level of the chor-dae tendineae, just below the tip of the anterior mitralleaflet. From the tracings, the following measure-ments were made: LV end-diastolic dimension (EDD)was taken as the distance between the left septal sur-face and the endocardium of the posterior wall belowthe mitral valve, at the R wave of the ECG (normalless than 5.4 cm); LV end-systolic dimension (ESD)was taken as the shortest simultaneous systolic dis-tance between the left interventricular septal andposterior LV wall endocardium (fig. 1). Two indepen-dent observers had excellent agreement of each
QRS
-----'-......... ..... ..... ............ .... ...
- ---
ol~~_~_
B- K
FIGURE 1. Representative baseline M-mode echocardiogram (unretouched) of theleft ventricle at the level of the tip of theanterior mitral valve leaflet and chordae ten-dineae. Using the end-diastolic (EDD) andend-systolic (ESD) dimensions of the leftventricle (as described in Methods) and us-ing the left ventricular ejection time (L VET)from a phonocardiogram, the mean veloc-ity of circumferential fiber shortening (Vef)may be calculated: VCF - (EDD EST)(EDD X LVET). Key: QRS = QRS of
the electrocardiogram; plvw = posteriorleft ventricular wall. A 10 mm distancecalibration is shown.
121
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 59, No 1, JANUARY 1979
measurement. All dimensions were measured to thenearest millimeter, and paper speed was carefully cali-brated at 50 mm/sec.Mean Vcf was derived from:32 33, 36 Vcf = (EDD-
ESD)/(EDD X LVET). Our normal values for themeasurements have been reported previously.44' 4
Systolic Time Intervals
Systolic time intervals39' 40 were measured fromsimultaneous recordings of the indirect carotid pulse,ECG, and phonocardiogram from the third left inter-costal space, using the Honeywell 3820 echocardiog-raphy-phonocardiography system and the Honeywell1856 fiberoptic recorder with a calibrated paper speedof 100 mm/sec with 40 msec time lines. We made thefollowing measurements: HR; electromechanicalsystole (QS2), measured from the onset of the Q waveof the ECG to the first high frequency positive deflec-tion of the aortic component of the second sound;LVET, from the onset of the rapid upstroke of thecarotid pulse to the incisura of the dicrotic notch;PEP = QS2 - LVET. They were combined to formthe ratio PEP/LVET. A mean value for 10 beats wastaken for each measurement, with the patient supine,during quiet respiration.
Statistics
We used a two-tailed t test for paired variables. Wechose a level of significance ofp < 0.05. Mean valueswere reported ± SD.48
Results
Control Measurements
Baseline measurements on day 1 and day 2, beforeany pharmacologic manipulation (table 1) of HR,mean Vcf, and PEP/LVET were virtually the same. Itis unclear why the mean PEP/LVET was at the upperlimits of the reported normal range.39' 40 7 However,each subject served as his or her own control for com-parison with subsequent measurements. BPs were un-changed throughout the study.
TABLE 1. Effects on Cardiac Function of Ethanol, AutonomicBlockade, and Autonomic Blockade Plus Ethanol in NineNormal Subjects
HR VCF PEP/LVET
C1 68.6 6.4 1.06 0.07 0.39 0.05
C2 66.8 - 13.6 1.07 - 0.14 0.40 0.03
B 105.8 - 20.1 1.27 - 0.15 0.43 - 0.05
E 71.5 - 13.9 1.04 0.17 0.42 0.07
BE 95.8 - 10.7 1.14 0.13 0.45 0.05
All values are mean SD.
Abbreviations: B = autonomic blockade; BE = autono-mic blockade and ethanol; C1 = control day 1; C2 = controlday 2; E = ethanol; HR = heart rate (beats/min); PEP/LVET = ratio of pre-ejection period to left ventricularejection time; VCF = mean velocity of left ventricularcircumferential fiber shortening (circ/sec).
Autonomic Blockade (tables 1 and 2)
On day 1, after control measurements of BP, HR,Vcf, and PEP/LVET were recorded, autonomicblockade was performed and measurements of BP,HR, Vcf and PEP/LVET were repeated to give infor-mation on 1) the effects of autonomic blockade onthese noninvasive parameters, and 2) a baseline forcomparison with combined blockade and ethanol. Asreported by Jose,29 the effects of autonomic blockadeare essentially gone by 2 hours. Thus, the controlvalues for day 2 were essentially the same as on day 1.Autonomic blockade resulted in no change in BP.
HR with blockade ("intrinsic heart rate," IHR) wasincreased by 54% (p < 0.001) from control values to105.8 ± 20.1 beats/min. This was not significantlydifferent from the age-predicted IHR (102.6beats/min) for the group.29 The Vcf increased by 20%(p < 0.01). In the absence of changes in afterload(BP), or in preload (ventricular filling), the change inVcf is probably related to the increase in HR.48PEP/LVET increased by 10% (p < 0.01), suggesting adecrease in LV performance compared with controlvalues; however, this undoubtedly reflects the basalLV function after removal of autonomic tone, ratherthan LV dysfunction.
Ethanol (tables 1 and 2)Alcohol is rapidly absorbed from the stomach,
small intestine, and colon. Many factors may modifythe rate of gastric absorption, and gastric emptying(e.g., volume, character, and dilution of the alcoholicbeverage, presence of food, period of time to ingest thedrink, individual differences). In our fasted subjects,60 minutes after ingestion of a total of 180 ml ethanol,the mean blood ethanol was 110 ± 17.8 mg/dl (range77-135 mg/dl). Each subject became mildly intoxi-cated. For the average person, 180 ml of distilled
TABLE 2. Comparison of the Cardiac Effects of Ethanol,Autonomic Blockade and Autonomic Blockade Plus Ethanolin Nine Normal Subjects
%A(X2-X1) HR VCF PEP/LVET%A(E-C2) + 7 - 3 + 4t%A(B-C1) +54§ +20f +10l%A(BE-C2) +43§ + 7 + 12k%A(BE-B) -10§ -10* + 4tValues are expressed as the percentage change from X1
x vwhere
XX 100 = %±X1. Plus (+) and minus (-)
signs denote the direction of change. Ethanol was not sig-nificantly different from control except for PEP/LVET. ForVCF, B versus Control had a 20c%o increase, and BE versusControl2 had a 7, increase, a difference of 13%, suggestingthat addition of ethanol to the autonomic blockaded heartresults in decreased myocardial performance (see text fordiscussion).
*p <0.05.tP <0.02.Tp <0.01.§P <0.001.Abbreviations: see table 1.
122 CIRCULATION
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

ETHANOL AND AUTONOMIC BLOCKADE/Child et al.
spirits on an empty stomach will produce a blood levelof approximately 100 mg/dl.49 Blood levels in usualsocial drinking situations average 50-75 mg/dl, withovert signs of intoxication in social (nontolerant)drinkers at levels between 100-200 mg/dl.49 50The cardiac measurements were lost in one subject
for this phase of the study, so mean values on onlyeight subjects are reported. HR increased only 7%,and Vcf decreased by 3%. PEP/LVET showed a slightincrease of 4% (p < 0.02). Thus, there was evidence ofa possible slight decrease in LV performance at amean blood ethanol level of 110 mg/dl.
Ethanol Plus Autonomic Blockade (tables 1 and 2)
Immediately after the ethanol (alone), cardiacmeasurements were made, autonomic blockade wasperformed, and the measurements were repeated.Compared to the control values on day 2, HR in-creased 43% (p < 0.001); however, this was a 10%decrease compared with autonomic blockade alone(p < 0.001) as determined on day 1. Also, Vcf rose 7%(NS), proportionately less than the increase in HR,and Vcf was decreased by 10% (p < 0.05), comparedwith autonomic blockade without ethanol. Thissuggested a decrease in LV performance in subjectsacutely ingesting ethanol and then undergoingautonomic blockade. This was confirmed by thePEP/LVET, which rose 12% (p < 0.01) over control,and also rose 4% (p < 0.01) over that seen withautonomic blockade alone.
DiscussionThe published accounts of the acute effects of ethanol
on the myocardium are somewhat inconsistent.'0-22, 51At least some of the discrepancy is probably due todifferences in experimental design. The major vari-able not controlled during most of the studies hasbeen the influence of autonomic tone and/orcatecholamines. Ethanol causes release of epinephrinefrom the adrenal medulla,24 26 and also causes cortico-hypothalamic stimulation.23 Moreover, acetaldehyde,a metabolite of ethanol, may cause release of myo-cardial norepinephrine, and thereby stimulate theheart.12' 52 Any study of the effect of ethanol on myo-cardial function will be modified by such factors.27To separate the postulated primary depressant
effects of ethanol from the secondary stimulant effects(evoked by release of circulating catecholamines) oncardiac function, Wong12 evaluated hemodynamicsbefore and during autonomic blockade in 20anesthesized dogs receiving intravenous infusions ofethanol. Blood ethanol levels were over 100 mg/dl by30 minutes and over 200 mg/dl by 2 hours. During theethanol infusions, cardiac index declined and LV end-diastolic pressure rose; these changes were even morepronounced during autonomic blockade plus ethanolinfusion. Autonomic blockade alone did notsignificantly affect cardiac function, except for an in-crease in HR. These findings could be interpreted asdisclosing a "masking" effect by catecholamines,presumably released by the ethanol, whose cardiac
stimulatory effects cancelled the myocardial depres-sion of ethanol. Our results in human subjects are inagreement.Horowitz and Atkins22 studied the effects of intra-
venous ethanol and autonomic blockade in six con-scious chronically instrumented dogs (to avoidanesthetic-induced myocardial depression). Therewere small dose-related decreases in stroke volumeand in LV dp/dt. Echocardiographic LV dimensionsat end-diastole, and at end-systole, increased slightly.Ethanol infusion during autonomic blockade resultedin an absolute decrease in HR and a less significantdrop in stroke volume.
In our study, we used the noninvasive techniques ofechocardiography and phonocardiography. The reli-ability of deriving information from the LV minordimensions (e.g. Vcf, ventricular volumes) in diseasedventricles with abnormal shapes has beenquestioned.38' 53' 54 However, in normal subjects, par-ticularly when serial studies on the same person arecompared, most investigators are satisfied with thereproducibility of LV minor axis dimensions34 37 andwith the correlation of Vcf with LV perfor-
3234,37 4mance, provided BP and HR are considered.48The PEP/LVET value correlates well with LV per-
formance, and is relatively unrelated to changes in HRup to 110 beats/min.39 40 4 We used this ratio as themost useful indicator of the systolic intervals ofchanges in LV function. Increases in PEP/LVET to0.44 or greater usually denote decreased LV perfor-mance.37 38 48 It is not clear why our clinically andechocardiographically normal subjects had a controlbaseline PEP/LVET of 0.39 ± 0.05 that was justabove I SD for reported normals of 0.35 ± 0.04. Anincrease in PEP/LVET may occur in normal individ-uals with assumption of the upright posture. This isnot germane to our study. However, there is a normaldiurnal decrease in LVET without a change in PEP inthe afternoon hours.47 This may be a partial explana-tion for the PEP/LVET values in our patients.
Ethanol alone (tables 1 and 2) resulted in no signifi-cant change in HR or Vcf, and in a slight (+4%) butsignificant increase in PEP/LVET (p < 0.02). Thismight suggest a mild decrease in LV function, but it isnot convincing. Autonomic blockade (tables 1 and 2)resulted in an increase of 54% (p < 0.001) in HR tolevels equivalent to the predicted IHR of Jose.28 29There was a 20% increase in Vcf (p < 0.01), propor-tionate to the increase in HR. The 10% increase inPEP/LVET (p < 0.01) is probably related to thewithdrawal of sympathetic stimulation of the heart inthat the Vcf and IHR were normal. Thus, this mayrepresent basal myocardial contractility.
Beta blockade with propranolol is associated with aslight lengthening of the PEP and shortening ofLVET,47 5 with a resultant increase in PEP/LVET. Itis unclear what the effect of atropine alone will be onthis ratio, but our study reveals that full autonomicblockade results in a significant increase inPEP/LVET in otherwise normal hearts. That such afinding could represent LV dysfunction is doubtful be-cause there was a concomitant increase in Vcf.
123
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

VOL 59, No 1, JANUARY 1979
When the effects of combined ethanol andautonomic blockade were studied, the PEP/LVETrose further to 0.45 (± 0.05 SD), an increase of 12%(p < 0.01). However, Vcf only rose 7% compared tothe 20% increase with autonomic blockade alone.Thus, the Vcf did not rise as much as expected, in rela-tion to an increase in HR, when autonomic blockadeand ethanol were combined. In essence, there was anincrease in PEP/LVET (p < 0.01) and a relativedecrease in Vcf, (p < 0.05), when ethanol plusautonomic blockade were compared to autonomicblockade as the baseline. In addition, the HR was de-creased by 10% (p < 0.001) by ethanol and autonomicblockade compared with autonomic blockade alone.This IHR of 95.8 (mean) with ethanol would be con-sidered by Jose28" 29 as evidence for a decrease in myo-cardial function when compared with the IHR of105.8 (mean) without ethanol. This was statisticallysignificant when each person was compared withhimself or herself. These findings (upon combiningethanol and autonomic blockade) of decreased IHR,increased PEP/LVET, and relative decrease in Vcf,suggest a decrease in LV performance. Therefore,autonomic blockade "unmasked" myocardial depres-sion due to ethanol.
Potential criticisms of our study include the smallnumber of subjects, the narrow age range, and thepossibility that the subjects were less than truthfulabout their true alcohol usage. Timmis et al.'6 studiedsystolic time intervals in normal subjects subdividedon the basis of their average daily consumption ofethanol. The greater the average daily consumption,the higher were the initial control values and the lesswas the change in each systolic time interval afteracute ethanol ingestion. Their results suggesttolerance as well as progressive degreees of chroniccardiac malfunction proportionate to the amount ofchronic ethanol exposure.We took our measurements at only one isolated
moment after the ingestion of ethanol: at 60 minutes,with a mean blood ethanol of 10 mg/dl. This 60-min-ute blood level was equivalent to that of Ahmed15 andDelgado2' in normal human subjects, and of Regan"3in dogs. Higher blood levels and multiple time periodsof measurement might have shown depression of LVperformance by ethanol alone, or might have moreclearly defined such depression after the withdrawal ofadrenergic effect by autonomic blockade. However,similar and even higher ethanol blood levels have in-consistently affected cardiac function in otherreports.8' 14-16, 20, 21 Our subjects drank Scotch whiskeywhich was not mixed with any other substance (e.g.,sugars), and osmolarity changes have previously beenshown not to be responsible for alterations in cardiacinotropy.2' 56 We did not study the effects of varioustemperatures of the orally ingested ethanol on theparameters measured, nor did we study the effects ofan equivalent amount of non-alcohol calories.From our study, we conclude that in normal human
subjects: 1) pharmacologic autonomic blockade aloneresults in no detectable myocardial dysfunction; 2) noimportant acute effects of ethanol alone could be
demonstrated; and 3) ethanol produces a significantdecrease in contractility in the autonomic blockadedheart, with a mild negative chronotropic effect. Thus,autonomic blockade apparently "unmasked" myo-cardial depression due to ethanol per se at bloodethanol levels comparable to other reported studies.This is also in agreement with the animal studies.These findings cannot necessarily be extrapolated tothe chronic cardiac patient, or to the patient withalcoholic cardiomyopathy. However, application ofthe technique of autonomic blockade provides furtherinsight into the relationship between ethanol and car-diac dysfunction.
AcknowledgmentsThe authors express their gratitude to Dr. Joseph K. Perloff for
his editorial comments and to Gail S. Asato and Roxane D. Davisfor their assistance in preparing the manuscript.
References
I. Alexander CS: Idiopathic heart disease. I. Analysis of 100cases, with special reference to alcoholism. II. Electronmicroscopic examination of myocardial biopsy specimens inalcoholic heart disease. Am J Med 41: 213, 1966
2. Perloff JK: The cardiomyopathies - current perspectives. Cir-culation 44: 942, 1971
3. Regan TJ, Levinson GE, Oldewurtel HA, Frank MJ, WeisseAB, Moschos CB: Ventricular function in noncardiacs withalcoholic fatty liver: role of ethanol in the production of cardio-myopathy. J Clin Invest 48: 387, 1969
4. Burch GE, DePasquale NP: Alcoholic cardiomyopathy. Am JCardiol 23: 723, 1969
5. Gould L, Zahir M, Shariff M, Dilieto M: Cardiachemodynamics in alcoholic heart disease. Ann Intern Med 71:543, 1969
6. Spodick DH, Piggot VM, Chirife R: Preclinical cardiacmalfunction in chronic alcoholism. N Engl J Med 287: 677,1972
7. Conway N: Effects of ethyl alcohol in patients with coronaryheart disease. Br Heart J 30: 638, 1968
8. Gould L, Zahir M, DeMartino A, Gomprecht RF: Cardiaceffects of a cocktail. JAMA 218: 1799, 1971
9. Orlando J, Aronow WS, Cassidy J, Prakash R: Effect ofethanol on angina pectoris. Ann Intern Med 84: 652, 1976
10. Webb WR, Degerli IU: Ethyl alcohol and the cardiovascularsystem. JAMA 191: 1055, 1965
11. Mitchell JH, Cohen LS: Alcohol and the heart. Mod Conc Car-diovasc Dis 39: 103, 1970
12. Wong M: Depression of cardiac performance by ethanol un-masked during autonomic blockade. Am Heart J 86: 508, 1973
13. Regan TJ, Koroxenidis G, Moschos CB, Oldewurtel HA,Tehan PH, Hellems HK: The acute metabolic and hemo-dynamic responses of the left ventricle to ethanol. J Clin Invest45: 270, 1966
14. Webb WR, Gupta DN, Cook WA, Sugg WL, Bashour FA,Unal MO: Effects of alcohol on myocardial contractility. DisChest 52: 602, 1967
15. Ahmed SS, Levinson GE, Regan TJ: Depression of myo-cardial contractility with low doses of ethanol in normal man.Circulation 48: 378, 1973
16. Timmis GC, Ramos RC, Gordon S, Gangadharan V: The basisfor differences in ethanol induced myocardial depression in nor-mal subjects. Circulation 51: 1144, 1975
17. Riff DP, Jain AC, Doyle JT: Acute hemodynamic effects ofethanol on normal human volunteers. Am Heart J 78: 592, 1969
18. Blomqvist G, Saltin B, Mitchell JH: Acute effects of ethanol in-gestion on the response to submaximal and maximal exercise inman. Circulation 42: 463, 1970
19. Wendt VE, Aljuni R, Bruce TA, Prasad AS, Bing RJ: Acute
124 CIRCULATION
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

ETHANOL AND AUTONOMIC BLOCKADE/Child et al.
effects of alcohol on the human myocardium. Am J Cardiol 17:804, 1966
20. Juchems R, Klobe R: Hemodynamic effects of ethyl alcohol inman. Am Heart J 78: 133, 1969
21. Delgado CE, Fortuin NJ, Ross RS: Acute effects of low dosesof alcohol on left ventricular function by echocardiography.Circulation 51: 535, 1975
22. Horowitz LD, Atkins JM: Acute effects of ethanol on left ven-tricular performance. Circulation 49: 124, 1974
23. Masserman JH, Beal H, Sanders R: Stimulant effects of ethylalcohol in corticohypothalamic functions. J Pharmacol ExpTher 70: 450, 1940
24. Klingman GI, Goodall MC: Urinary epinephrine andlevarterenol excretion during acute sublethal alcohol ad-ministration in dogs. J Pharmacol Exp Ther 12: 313, 1957
25. Perman ES: The effect of ethyl alcohol on the secretion fromthe adrenal medulla in man. Acta Physiol Scand 44: 241, 1958
26. Siegel JH: The effect of enteric ethanol on arterial and portalvenous catecholamines (abstr) Clin Res 12: 213, 1964
27. Nayler WG: Some factors involved in the maintenance andregulation of cardiac contractility. Circ Res 21 (suppl III): III-213, 1967
28. Jose AD, Stitt F: Cardiac function after combined beta-adrenergic and cholingeric blockade. Relationship of intrinsicrate to contractile force in dogs. Circ Res 21 (suppl III): III-231, 1967
29. Jose AD, Taylor RR: Autonomic blockade by propranolol andatropine to study intrinsic myocardial function in man. J ClinInvest 48: 2019, 1969
30. Murray JA, Johnston W, Reid JM: Echocardiographic deter-mination of left ventricular dimensions, volumes and per-formance. Am J Cardiol 30: 252, 1972
31. Belenkie I, Nutter DO, Clark DW, McGraw DB, Raizner AE:Assessment of left ventricular dimensions and functions byechocardiography. Am J Cardiol 31: 755, 1973
32. Ludbrook P, Karliner JS, Peterson K, Leopold G, O'RourkeRA: Comparison of ultrasound and cineangiographic mea-surements of left ventricular performance in patients with andwithout wall motion abnormalities. Br Heart J 35: 1026, 1973
33. Quinones MA, Gaasch WH, Alexander JK: Echocardiographicassessment of left ventricular function: with special reference tonormalized velocities. Circulation 50: 42, 1974
34. Redwood DR, Henry WL, Epstein SE: Evaluation of the abilityof echocardiography to measure acute alterations in left ven-tricular volume. Circulation 50: 901, 1974
35. Cooper RH, O'Rourke RA, Karliner JS, Peterson KL,Leopold GR: Comparison of ultrasound and cineangiographicmeasurements of the mean rate of circumferential shortening inman. Circulation 46: 914, 1972
36. Fortuin NJ, Pawsey CGK: The evaluation of the left ven-tricular function by echocardiography. Am J Med 63: 1, 1977
37. Stefadouros MA, Canedo MI: Reproducibility of echocardio-graphic estimates of left ventricular dimensions. Br Heart J 39:390, 1977
38. Feigenbaum H: Echocardiography, 2nd ed. Philadelphia, Lea
and Febiger, 1976, p 309-31339. Martin CE, Shaver JA, Thompson ME, Reddy PS, Leonard
JJ: Direct correlation of external systolic time intervals with in-ternal indices on left ventricular function in man. Circulation44: 419, 1971
40. Lewis RP, Rittgers SE, Forester WF, Boudoulas H: A criticalreview of the systolic time intervals. Circulation 56: 146, 1977
41. Bassette R, Ozeris S, Whitnak CH: Gas chromatographicanalysis of head space gas of dilute aqueous solutions. AnalChem 34: 1540, 1962
42. Solon J, Watkins J, Mikkelsen L: Automated analysis ofalcohols in blood. J Forensic Sci 17: 447, 1972
43. Popp RL, Filly K, Brown OR, Harrison DC: Effect oftransducer placement on echocardiographic measurement ofleft ventricular dimensions. Am J Cardiol 35: 537, 1975
44. Abbasi AS, MacAlpin RN, Eber LM, Pearce ML: Echocar-diographic diagnosis of idiopathic hypertrophic car-diomyopathy without outflow tract obstruction. Circulation 46:897, 1972
45. Child JS, Levisman JA, Abbasi AS, MacAlpin RN: Echocar-diographic manifestations of infiltrative cardiomyopathy. Areport of seven cases due to amyloid. Chest 70: 726, 1976
46. Dixon WJ, Massey FJ Jr: Introduction to statistical analysis,3rd ed. New York, McGraw-Hill Co, 1969, p 109-123, 264
47. Weissler AM, Garrard CL Jr: Systolic time intervals in cardiacdisease (I and II). Mod Conc Cardiovasc Dis 40: 1, 1971
48. Hirshleifer J, Crawford M, O'Rourke RA, Karliner JS:Influence of acute alterations in heart rate and systemic arterialpressure on echocardiographic measures of left ventricular per-formance in normal human subjects. Circulation 52: 835, 1975
49. Mendelsohn JH: Alcohol abuse and alcohol related illness. InTextbook of Medicine, 14th ed, edited by Beeson PB, McDer-mott W. Philadelphia, WB Saunders, 1975, p 598
50. Ritchie JM: The aliphatic alcohols. In the Pharmacologic Basisof Therapeutics, 3rd ed, edited by Goodman LS, Gilman A.New York, MacMillan, 1965, p 148-150
51. Segal LD, Miller RR, Mason DT: Depressive effects of acuteethanol exposure on function of isolated working rat hearts.Cardiovasc Med 3: 211, 1978
52. Nakano J, Prancan AV: Effects of adrenergic blockade on car-diovascular responses to ethanol and acetaldehyde. Arch IntPharmacodyn Ther 1%: 259, 1972
53. Teichholz LE, Kreulen T, Herman MV, Gorlin R: Problems inechocardiographic-angiographic correlations in the presence orabsence of asynergy. Am J Cardiol 37: 7, 1976
54. Johnson AD, Alpert JS, Francis GS, Vieweg WVR, Ockene J,Hagan AD: Assessment of left ventricular function in severeaortic insufficiency. Circulation 54: 975, 1976
55. Harris WS, Schoenfeld CD, Weissler AM: Effects ofadrenergic receptor activation and blockade on the systolicpreejection period, heart rate, and arterial pressure in man.J Clin Invest 46: 1704, 1967
56. Nakano J, Moore SE: Effect of different alcohols on the con-tractile force of the isolated guinea-pig myocardium. Eur JPharmacol 20: 266, 1972
125
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

J S Child, R B Kovick, J A Levisman and M L PearceCardiac effects of acute ethanol ingestion unmasked by autonomic blockade.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1979 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.59.1.120
1979;59:120-125Circulation.
http://circ.ahajournals.org/content/59/1/120the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from