Embed Size (px)
Citation preview

This copy is for personal use only. To order printed copies, contact [email protected]
This copy is for personal use only. To order printed copies, contact [email protected] ORIGINAL RESEARCH • CARDIAC IMAGING
Although a timely and correct diagnosis of myocarditis should represent the first step toward a tailored thera-
peutic strategy to reduce the risk of progression to chronic active inflammation and/or dilated cardiomyopathy (1,2), the diagnosis of myocarditis remains one of the most chal-lenging in clinical cardiology (3).
With its unique capability for tissue characterization, cardiac MRI has become the primary tool for noninvasive diagnosis of myocarditis for clinicians, if it is available to them. Current diagnostic Lake Louise criteria (LLC) aim to visualize the hallmarks of myocardial inflammation by means of T2-weighted edema imaging, assessment of vasodilatatory response and/or capillary leak based on early gadolinium-enhanced imaging, and visualization of myocardial fibrosis and/or necrosis with late gadolinium-enhanced imaging (4). Nevertheless, many studies have reported considerable variations in sensitivity (66%–92%) and specificity (47%–80%) of LLC (5–7).
One potential explanation for this phenomenon is the existence of different types of myocarditis based on the
predominant clinical presentation. Growing clinical evi-dence suggests that myocarditis with acute infarctlike pre-sentation might need a different diagnostic approach than does myocarditis manifesting as new-onset heart failure or in its chronic stage (2,6–8).
Recently, T1 and T2 mapping techniques have been introduced as quantitative and thus more objective and reliable approaches to the detection of myocardial in-flammation. However, the routine clinical use of mapping techniques is still hindered by several major limitations, the most important one being the large overlap of myocardial T1 and T2 times between health and disease (9–12). Recently proposed approaches that aim to detect inflammation- induced tissue changes by quantifying the heterogeneity of T2 relaxation times in the myocardium (10,13) require an elaborated off-line calculation of the derived parameters and thus cannot be easily applied during the mapping postprocessing workflow. Consequently, faster methods to assess inflammatory tissue changes that can be applied di-rectly during the routine postprocessing of cardiac T1 and
Cardiac MRI Texture Analysis of T1 and T2 Maps in Patients with Infarctlike Acute Myocarditis
Bettina Baessler, MD • Christian Luecke, MD • Julia Lurz, MD • Karin Klingel, MD • Maximilian von Roeder, MD • Suzanne de Waha, MD • Christian Besler, MD • David Maintz, MD • Matthias Gutberlet, MD • Holger Thiele, MD • Philipp Lurz, MD, PhD
From the Department of Radiology, University Hospital of Cologne, Kerpener Str 62, 50937 Cologne, Germany (B.B., D.M.); Department of Diagnostic and Interven-tional Radiology, Heart Center Leipzig, Leipzig, Germany (C.L., M.G.); Department of Internal Medicine/Cardiology, Heart Center Leipzig-University Hospital, Leipzig, Germany (J.L., M.v.R., C.B., H.T., P.L.); Department of Cardiopathology, Institute for Pathology and Neuropathology, University Hospital Tuebingen, Tuebingen, Germany (K.K.); Department of Cardiology, Angiology, and Intensive Care Medicine, University Heart Center Luebeck, Luebeck, Germany (S.d.W.); German Center for Cardiovascular Research (DZHK), partner site Hamburg/Kiel/Luebeck, Luebeck, Germany (S.d.W.); and Leipzig Heart Institute, Leipzig, Germany (M.G., H.T., P.L.). Received February 16, 2018; revision requested March 14; final revision received June 5; accepted June 8. Address correspondence to B.B. (e-mail: [email protected]).
Conflicts of interest are listed at the end of this article.
Radiology 2018; 00:1–9 • https://doi.org/10.1148/radiol.2018180411 • Content code:
Purpose: To assess the diagnostic potential of texture analysis applied to T1 and T2 maps obtained with cardiac MRI for the diag-nosis of acute infarctlike myocarditis.
Materials and Methods: This prospective study from August 2012 to May 2015 included 39 participants (overall mean age 6 stan-dard deviation, 34.7 years 6 12.2 [range, 18–63 years]; mean age of women, 46.1 years 6 10.8 [range, 24–63 years]; mean age of men, 29.8 years 6 9.2 [range, 18–56 years]) from the Magnetic Resonance Imaging in Myocarditis (MyoRacer) trial with clinical suspicion of acute myocarditis and infarctlike presentation. Participants underwent biventricular endomyocardial biopsy, cardiac catheterization, and cardiac MRI at 1.5 T, in which native T1 and T2 mapping as well as Lake Louise criteria (LLC) were assessed. Texture analysis was applied on T1 and T2 maps by using a freely available software package. Stepwise dimension reduction and texture feature selection was performed for selecting features enabling the diagnosis of myocarditis by using endomyocardial biopsy as the reference standard.
Results: Endomyocardial biopsy confirmed the diagnosis of acute myocarditis in 26 patients, whereas 13 participants had no signs of acute inflammation. Mean T1 and T2 values and LLC showed a low diagnostic performance, with area under the curve in receiver operating curve analyses as follows: 0.65 (95% confidence interval [CI]: 0.45, 0.85) for T1, 0.67 (95% CI: 0.49, 0.85) for T2, and 0.62 (95% CI: 0.42, 0.79) for LLC. Combining the texture features T2 run-length nonuniformity and gray-level non-uniformity resulted in higher diagnostic performance with an area under the curve of 0.88 (95% CI: 0.73, 1.00) (P , .001) and a sensitivity and specificity of 89% [95% CI: 81%, 93%] and 92% [95% CI: 77%, 93%], respectively.
Conclusion: Texture analysis of T2 maps shows high sensitivity and specificity for the diagnosis of acute infarctlike myocarditis.
© RSNA, 2018
Online supplemental material is available for this article.

Cardiac MRI Texture Analysis of T1 and T2 Maps in Infarctlike Acute Myocarditis
2 radiology.rsna.org n Radiology: Volume 00: Number 0—2018
Study DesignAmong all participants enrolled in the MyoRacer trial from August 2012 to May 2015, only participants with clinical sus-picion of acute myocarditis and infarctlike presentation were included. Additionally, 10 healthy volunteers underwent car-diac MRI for comparison. Inclusion and exclusion criteria for participants and healthy control participants are illustrated in Figure 1.
Biopsy and ImmunohistochemistryBiventricular endomyocardial biopsy (EMB) sampling was performed via femoral venous and arterial access by using myo-cardial biopsy forceps (Teleflex Medical Tuttlingen, Tuttlingen, Germany); six to seven EMB samples were taken from different locations within the left ventricle by using fluoroscopic guid-ance. Right ventricular biopsies (five to seven samples) were taken exclusively from the septal or apical regions.
Histologic, immunohistologic, and molecular pathologic analyses were performed by an experienced observer (K.K., with 15 years of experience in cardiovascular pathology) as previously described (6,7), in accordance with consensus recommendations (18). A detailed description of EMB analysis is provided in Ap-pendix E1 (online).
In addition, standard blood parameters (troponin, creatine kinase-MB, N-terminal pro b-type Natriuretic Peptide) were re-corded for each participant.
Cardiac MRICardiac MRI was performed with a clinical 1.5-T system (In-tera CV; Philips Healthcare, Best, the Netherlands) by using a dedicated five-element cardiac coil. For T2 short inversion time inversion-recovery and T1-weighted spin-echo sequences, a body coil was used. The entire cardiac MRI protocol is shown in Figure E1 (online). A detailed description of the protocol parameters and cardiac MRI data analysis is provided in Ap-pendix E1 (Tables E1 and E2 [online]).
Image analysis of LLC was performed with a standard post-processing platform (cmr42, version 5.1.0; Circle Cardiovascu-lar Imaging, Calgary, Alberta, Canada) by two experienced ob-servers in consensus (C.L. and B.B., with 8 years and 6 years of experience in cardiovascular imaging, respectively). The myocar-dium was evaluated visually for presence of myocardial edema at T2-weighted black-blood imaging, as well as by calculating the T2-ratio as previously described (4). Briefly, a myocardial region of interest and a skeletal muscle region of interest were drawn and the subsequent signal intensity of the myocardium was di-vided by the signal intensity of the skeletal muscle. Edema was diagnosed if T2 ratio was greater than 1.9.
For calculation of the early gadolinium enhancement ratio, standardized myocardial and skeletal muscle regions of interest were drawn on one axial section before and after contrast ma-terial administration. Early gadolinium enhancement ratio was calculated as previously described and deemed pathologic when greater than or equal to 4 (4).
The myocardium was visually assessed on late gadolinium-enhanced images and considered suspicious for myocarditis in cases of focal signal intensity alterations with a subepicardial or
AbbreviationsAUC = area under the curve, CI = confidence interval, EMB = endo-myocardial biopsy, LLC = Lake Louise criteria, ROC = receiver operat-ing curve, TA = texture analysis
SummaryTexture analysis of T2 maps obtained with cardiac MRI shows excel-lent diagnostic performance in detecting a positive endomyocardial biopsy result for infarctlike myocarditis.
Implications for Patient Care n In patients with biopsy-proven acute infarctlike myocarditis, the
diagnostic performance of Lake Louise criteria, as well as global native T1 and T2, is only moderate when compared against endo-myocardial biopsy as a reference standard.
n Two T2 mapping–derived texture features (T2 run-length non-uniformity and T2 gray-level nonuniformity), both represent-ing measures of tissue inhomogeneity, yield superior diagnostic performance (sensitivity of 89% and specificity of 92%) for acute infarctlike myocarditis compared with Lake Louise criteria and na-tive T1 and T2 mapping.
n Combination of texture features with blood parameters (troponin, creatine kinase-MB, N-terminal pro b-type Natriuretic Peptide) resulted in increased diagnostic performance (sensitivity and speci-ficity of 100%) for detection of acute infarctlike myocarditis.
T2 maps are desirable for further improvement of diagnostic ac-curacy of cardiac MRI in myocarditis.
The increasing use of texture analysis (TA) allows the assess-ment of the underlying texture of a tissue. TA also detects tissue changes that remain imperceptible to the human eye (14) by quantifying gray-level patterns and pixel interrelationships in an image (14). Recently, applications of TA in cardiac MRI have been described in the setting of myocardial infarction, demon-strating the potential of TA for detecting small myocardial scars at cine imaging (15) and for differentiating acute versus chronic myocardial infarction (16).
The hypothesis for our study was that TA applied on myo-cardial T1 and T2 maps delivers diagnostic parameters reflecting inflammatory myocardial tissue changes with high diagnostic ac-curacy, especially when combined with clinical (blood) param-eters. Thus, the purpose of our proof-of-principle study was to assess the diagnostic potential of TA applied to T1 and T2 maps obtained with cardiac MRI with and without combination of blood parameters for the diagnosis of biopsy-proven acute in-farctlike myocarditis.
Materials and MethodsOur prospective single-center study represents a substudy from the Magnetic Resonance Imaging in Myocarditis (MyoRacer) trial (ClincialTrials.gov registration no. NCT02177630), includ-ing 44 of 129 originally reported consecutive participants (7,17). This prior article evaluated patients with acute and chronic myo-carditis by using LLC and T1 and T2 mapping, whereas the present article reports the application of TA on T1 and T2 map-ping not reported previously. Our study had institutional review board and local ethics committee approval. All participants and healthy control participants gave written informed consent.

Baessler et al
Radiology: Volume 00: Number 0— 2018 n radiology.rsna.org 3
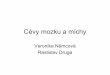
Technical University of Lodz, Lodz, Poland) (21) as previously described (15,22). T1 and T2 maps (midventricular short axis and horizontal long axis) were ex-ported as single Digital Imaging and Communications in Medicine images for further analysis, and re-gions of interest encompassing the entire left ventriclar myocardium were drawn by an experienced observer (B.B.) who was blinded to participant data (Fig 2). The trabeculated layer and epicardial border were carefully excluded to avoid partial volume effects. Visu-ally appreciable artifacts were ex-cluded from the region of interest. Drawing of regions of interest and computation of the TA features by the software took about 30 sec-onds per participant.
For testing the reproducibility of texture features, region-of-inter-est delineation was repeated twice after a pause of 2 weeks in a sub-set of 20 participants by the same reader for intraobserver analysis and by another reader (C.L.) for in-terobserver analysis. Results of the first reading were blinded for both coreadings.
Gray-level normalization was performed with the TA software by rescaling the histogram data to fit within m-gray-level mean 6 3s (s-gray-level standard deviation) to minimize the effect of brightness and contrast variations at TA (23). Five subset texture feature sets were
extracted separately (Table E3 [online]), resulting in a total of 271 texture features.
Texture Feature Selection and Dimension ReductionBecause of the high number of texture features, a stepwise fea-ture selection and dimension reduction was necessary to reduce the feature set to those that contributed most to accuracy of classification (24). The complete texture feature reduction and selection strategy is described in Appendix E1 (online).
Statistical AnalysisStatistical analysis was performed in R (version 3.4.0; R Foundation for Statistical Computing, Vienna, Austria) (25) with RStudio (version 1.0.136; RStudio, Boston, Mass) (26). R packages used for further statistical analyses are de-scribed in Appendix E1 (online). All continuous data are given as means 6 standard deviations or medians with interquartile
intramyocardial pattern typical for myocarditis (4). LLC were deemed positive for myocarditis with the presence of at least two of three LLC (4).
TA of ImagesTA represents different statistical image analysis techniques that quantify the texture of an image based on pixel signal intensity distributions and relationships of values between neighboring pixels (19). Unlike means and standard devia-tions that often assess more global characteristics, TA ana-lyzes more locally to small neighborhoods in the images (20). Computing texture features thus allows for the recognition and quantification of the intrinsic heterogeneity of different tissues and lesions, which are usually imperceptible to the hu-man eye (14).
In short, TA was performed by using a freely available soft-ware package (MaZda, version 4.6; Institute of Electronics,
Figure 1: Flowchart shows study design, including inclusion and exclusion criteria and reasons for participant dropout for comparison of endomyocardial biopsy (EMB) results with 1.5-T cardiac MRI. CAD = coronary artery disease, CMR = cardiac magnetic resonance, ECG = electrocardio-gram, EMB+ = EMB-positive, EMB2 = EMB-negative, LV-EF = left ventricular ejection fraction, RV = right ventricle.

Cardiac MRI Texture Analysis of T1 and T2 Maps in Infarctlike Acute Myocarditis
4 radiology.rsna.org n Radiology: Volume 00: Number 0—2018
For selecting variables that allow classification of participants with posi-tive findings for acute myocarditis at EMB from control participants and for participant subgroup analyses, multiple and multinomial logistic regression models were fitted and compared with the Akaike information criterion. The misclassification rate of these models was assessed by using 10-fold cross-validation (ie, data were split at random into 10 subsets, where each subset was used once as a test data set, with the remaining part being used for refitting the model). The presented proportions of correct classification were aggregated over the 10 subsets. To define optimal cutoff values for the current data, sin-gle classification trees (also known as recursive partitioning) were fitted by using the Gini index as a measure for impurity (27). The diagnostic accuracy of optimal predictive parameters was evaluated from the area under the curve (AUC) from receiver operating charac-teristic (ROC) analyses, and diagnostic sensitivity and specificity were calcu-lated. Optimal diagnostic performance was chosen at the point where highest specificity was achieved. 95% confi-dence intervals (CIs) were calculated for all AUCs, sensitivities, and specificities. Again, misclassification rates were as-sessed by 10-fold cross-validation. ROC curves were compared according to the DeLong method. Intra- and interob-server agreement was tested by using intraclass correlation coefficients.
Results
Study PopulationOur study flow and reasons for partici-pant dropout for comparison of EMB results with cardiac MRI are illustrated in Figure 1. Participant characteristics are shown in Table E4 (online).
Results of EMB and Cardiac MRIIn two participants, only left ven-tricular specimens could be obtained during EMB. Among 39 participants
included in our final study population, 26 had positive find-ings at EMB and 13 had negative findings. Diagnoses based on EMB findings are shown in Table E5 (online).
Similarly, edema ratio, early gadolinium enhancement, and presence of late gadolinium enhancement did not differ
ranges, where appropriate. Testing for group differences was performed by using Wilcoxon sum-rank test or Welch inde-pendent t test after assessing normality distribution of data by using the Shapiro-Wilk test. A two-tailed P value of , .05 was regarded to indicate statistical significance.
Figure 2: Image shows cardiac MRI findings in one exemplary healthy control participant, one participant with positive findings for myocarditis at endomyocardial biopsy (EMB, or EMB+), and one participant with negative findings at EMB (or EMB2). For better display, only short-axis images are shown. From top to bottom, numbers within panels indicate native T1 times, T2 times, T2 run-length nonuniformity, and T2 gray-level nonuniformity. Healthy control participant was a 38-year-old woman with low native T1 and T2, as well as low values for two texture features. Participant with positive findings at EMB was a 42-year-old woman with high native T1 and T2, as well as high values for two texture features but demonstrating negative Lake Louise criteria (LLC). Participant with negative findings at EMB was a 54-year-old woman demonstrating positive LLC and similarly high native T1 and T2, but considerably lower values for two texture features when compared with participant with positive findings at EMB, allow-ing discrimination of noninflammatory myocardium from myocardial inflammation.

Baessler et al
Radiology: Volume 00: Number 0— 2018 n radiology.rsna.org 5
TA for Differentiating Participants with Positive Findings for Acute Myocarditis at EMB from Healthy Control ParticipantsAt the end of the multistep dimension reduction and texture fea-ture selection process described in Appendix E1 (online), the six most important and independent texture features derived from T1 and T2 mapping were selected for further statistical analyses, including three second-order features from the co-occurrence matrix (T2 sum average, T2 invasive different moment, and T1 angular second moment), two second-order features from the run-length matrix (T2 run-length nonuniformity [T2_RLNon-Uni] and T2 short run emphasis), and one higher-order feature from the autoregressive model (T1 sigma).
All six texture features showed significant differences between participants with positive findings for myocarditis at EMB and healthy control participants, except for T1 angular second moment (Table 1). In single and multiple logistic regression analyses, the five significantly different texture features showed a similar diagnostic performance when used as a single parameter in a model accord-ing to their Akaike information criterion with AUCs in ROC analyses ranging from 0.78 to 0.90, except for T1 sigma with an AUC of 0.72 (95% CI: 0.57, 0.88) (Table 2). The combination of global myocardial T2 and T2_RLNonUni in a model finally resulted in highest diagnostic performance with an AUC of 1.00 (95% CI: 0.77, 1.00), a sensitivity of 26 of 26 (100% [95% CI: 87%, 100%]), and a specificity of 10 of 10 (96% [95% CI: 82%, 100%]), respectively (Fig 3, Table 2). Ten-fold cross-validation
between participants with positive findings at EMB and those with negative findings at EMB (Table 1). Consequently, the diagnosis of EMB-positive myocarditis was established with a sensitivity of 16 of 26 (63% [95% CI: 42%, 78%]) and a specificity of eight of 13 (62% [95% CI: 40%, 77%]) by using standard LLC (AUC in ROC analysis, 0.62 [95% CI: 0.42, 0.79]) compared with a sensitivity of 21 of 26 (80% [95% CI: 64%, 95%]) and specificity of seven of 10 (73% [95% CI: 53%, 86%]) for differentiating participants with positive findings at EMB from healthy control participants (AUC, 0.82 [95% CI: 0.68, 0.95]).
Similar observations were made for global myocardial T1 and T2, which showed a moderate and significant correla-tion (Pearson r = 0.44; P , .001). While demonstrating significant differences between participants with positive findings at EMB and control participants, no significant dif-ferences were observed for participants with positive find-ings at EMB versus those with negative findings (Table 1). In logistic regression and ROC analysis, global T1 had a slightly inferior AUC compared with global T2 (0.80 [95% CI: 0.65, 0.94] vs 0.90 [95% CI: 0.81, 0.99]; P = .164) for differentiating participants with positive findings at EMB from control participants, whereas their ability to differen-tiate participants with positive findings at EMB from those with negative findings was far inferior and similar to LLC with AUCs of 0.65 (95% CI: 0.45, 0.85) and 0.67 (95% CI: 0.49, 0.85) (P = .877), respectively.
Table 1: Results of Cardiac MRI and Texture Analysis
ParameterHealthy Control Participants (n = 10)
Participants with Positive Findings at EMB (n = 26) P Value*
Participants with Negative Findings at EMB (n = 13) P Value†
Edema ratio … 1.9 6 0.5 … 1.8 6 0.5 .48Early enhancement … 4.7 6 2.5 … 5.7 6 4.2 .73Presence of late gadolinium enhancement
… 20 (74) … 7 (54) .43
Lake Louise criteria … 17 (63) … 5 (39) .26Mean T1 (msec) 962 6 80 1053 6 76 .001‡ 1012 6 75 .14Mean T2 (msec) 55.8 6 1.8 62.1 6 4.8 ,.001‡ 59.0 6 4.4 .09T2 run-length nonuniformity§ 737 6 132 1024 6 230 ,.001‡ 739 6 236 ,.001‡
T2 gray-level nonuniformity 142 6 38 233 6 49 ,.001‡ 161 6 48 ,.001‡
T2 sum average 16.5 6 0.2 16.8 6 0.2 ,.001‡ 16.8 6 0.2 .78T2 sum entropy 1.17 6 0.03 1.19 6 0.03 .002‡ 1.15 6 0.04 .002‡
T2 invasive different moment 0.44 6 0.05 0.49 6 0.05 .003‡ 0.48 6 0.10 .05‡
T1 angular second moment 0.014 6 0.004 0.023 6 0.006 .53 0.036 6 0.001 .01‡
T2 short run emphasis 0.83 6 0.04 0.76 6 0.05 ,.001‡ 0.79 6 0.07 .02‡
T1 sigma 0.44 6 0.11 0.57 6 0.17 .02‡ 0.59 6 0.15 .75
Note.—Data are means 6 standard deviations. Whereas mean T1 and T2 relaxation times show significant differences between participants with positive findings for acute myocarditis at endomyocardial biopsy (EMB) and control participants, no significant differences can be observed when comparing participants with positive findings and those with negative findings. In contrast, several texture features show significant differences in both subgroup comparisons, the most distinct differences being observed for T2 run-length nonuniformity and T2 gray-level nonuniformity.* Control participants versus participants with positive findings at EMB.† Participants with positive findings at EMB versus those with negative findings.‡ Indicates significant P values.§ Texture features are dimensionless.

Cardiac MRI Texture Analysis of T1 and T2 Maps in Infarctlike Acute Myocarditis
6 radiology.rsna.org n Radiology: Volume 00: Number 0—2018
Tab
le 2
: D
iag
no
stic
Perf
orm
an
ce o
f C
on
ven
tio
na
l C
ard
iac
MR
I a
nd
Text
ure
Fea
ture
s
Part
icip
ants
with
Pos
itive
Fin
ding
s at E
MB
vs C
ontro
l Par
ticip
ants
Part
icip
ants
with
Pos
itive
Fin
ding
s at E
MB
vs P
artic
ipan
ts w
ith
Neg
ativ
e Fi
ndin
gs
Para
met
erAU
CSe
nsiti
vity
(%)
Spec
ifici
ty (%
)AU
CSe
nsiti
vity
(%)
Spec
ifici
ty (%
)La
ke L
ouise
crit
eria
0.82
(0.6
8, 0
.95)
21/2
6 (8
0) [6
4, 9
5]7/
10 (7
3) [5
3, 8
6]0.
62 (0
.42,
0.7
9)16
/26
(63)
[34,
89]
8/13
(62)
[32,
83]
Mea
n T
10.
80 (0
.65,
0.9
4)23
/26
(87)
[67,
100
]6/
10 (6
3) [5
9, 1
00]
0.65
(0.4
5, 0
.85)
21/2
6 (8
2) [3
8, 9
6]6/
13 (4
6) [3
1, 9
2]M
ean
T2
0.90
(0.8
1, 0
.99)
24/2
6 (9
3) [7
3, 1
00]
7/10
(74)
[67,
100
]0.
67 (0
.49,
0.8
5)15
/26
(56)
[44,
89]
10/1
3 (7
7) [5
4, 9
2]T
2 ru
n-le
ngth
non
unifo
rmity
0.87
(0.7
6, 0
.98)
24/2
6 (9
3) [8
7, 1
00]
8/10
(78)
[74,
100
]0.
86 (0
.71,
1.0
0)20
/26
(78)
[77,
100
]12
/13
(92)
[77,
100
]T
2 gr
ay-le
vel n
onun
iform
ity0.
90 (0
.83,
1.0
0)21
/26
(80)
[73,
100
]9/
10 (9
3) [8
5, 1
00]
0.86
(0.7
2, 1
.00)
23/2
6 (8
9) [8
5, 1
00]
11/1
3 (8
5) [6
9, 1
00]
T2
sum
ave
rage
0.85
(0.7
1, 0
.99)
24/2
6 (9
3) [8
0, 1
00]
8/10
(82)
[78,
100
]0.
53 (0
.33,
0.7
3)15
/26
(56)
[15,
85]
8/13
(62)
[23,
85]
T2
sum
ent
ropy
0.79
(0.6
4, 0
.93)
24/2
6 (9
3) [7
3, 1
00]
6/10
(63)
[59,
96]
0.80
(0.6
3, 0
.97)
21/2
6 (8
2) [7
0, 1
00]
11/1
3 (8
5) [7
7, 1
00]
T2
inva
sive
diffe
rent
mom
ent
0.78
(0.6
0, 0
.94)
19/2
6 (7
3) [5
3, 9
3]9/
10 (9
3) [8
5, 1
00]
0.70
(0.5
0, 0
.90)
24/2
6 (9
3) [5
9, 1
00]
7/13
(54)
[56,
92]
T2
shor
t run
em
phas
is0.
86 (0
.74,
0.9
8)17
/26
(67)
[73,
100
]9/
10 (9
3) [8
1, 1
00]
0.73
(0.5
4, 0
.92)
22/2
6 (8
5) [4
1, 1
00]
8/13
(62)
[38,
100
]T
1 sig
ma
0.72
(0.5
7, 0
.88)
24/2
6 (9
3) [8
0, 1
00]
6/10
(59)
[44,
93]
0.53
(0.2
8, 0
.66)
9/26
(33)
[19,
70]
11/1
3 (8
5) [2
3, 9
2]T
2 ru
n-le
ngth
non
unifo
rmity
+
T
2 m
ean
1.00
(0.7
7, 1
.00)
26/2
6 (1
00) [
87, 1
00]
10/1
0 (9
6) [8
2, 1
00]
0.87
(0.7
0, 1
.00)
25/2
6 (9
6) [7
8, 1
00]
10/1
3 (7
7) [7
4, 1
00]
T2
run-
leng
th n
onun
iform
ity +
T2
gray
-leve
l non
unifo
rmity
0.92
(0.8
0, 1
.00)
21/2
6 (8
0) [8
0, 1
00]
9/10
(93)
[81,
100
]0.
88 (0
.73,
1.0
0)23
/26
(89)
[81,
93]
12/1
3 (9
2) [7
7, 9
3]
Not
e.—
Unl
ess o
ther
wise
spec
ified
, dat
a ar
e nu
mer
ator
s and
den
omin
ator
s, w
ith p
erce
ntag
es in
par
enth
eses
and
95%
con
fiden
ce in
terv
als i
n br
acke
ts. W
here
as L
ake
Loui
se c
riter
ia a
s wel
l as
mea
n T
1 an
d T
2 sh
ow g
ood
diag
nosti
c pe
rform
ance
for d
iffer
entia
ting
part
icip
ants
with
pos
itive
find
ings
for a
cute
myo
card
itis a
t end
omyo
card
ial b
iops
y (E
MB)
from
con
trol p
artic
ipan
ts,
diag
nosti
c pe
rform
ance
is p
oor f
or d
iffer
entia
ting
part
icip
ants
with
pos
itive
find
ings
from
thos
e w
ith n
egat
ive
findi
ngs.
Seve
ral t
extu
re fe
atur
es sh
ow su
perio
r dia
gnos
tic p
erfo
rman
ce to
con
-ve
ntio
nal c
ardi
ac M
RI p
aram
eter
s whe
n us
ed a
s sin
gle
para
met
ers i
n re
ceiv
er o
pera
ting
curv
e an
alys
is. C
ombi
ning
T2
run-
leng
th n
onun
iform
ity a
nd m
ean
T2
in a
mod
el re
sults
in th
e be
st di
agno
stic
perfo
rman
ce fo
r diff
eren
tiatin
g pa
rtic
ipan
ts w
ith p
ositi
ve fi
ndin
gs fr
om c
ontro
l par
ticip
ants.
The
com
bina
tion
of T
2 ru
n-le
ngth
non
unifo
rmity
and
T2
gray
-leve
l non
unifo
rmity
in a
m
odel
fina
lly re
sults
in su
perio
r dia
gnos
tic p
erfo
rman
ce fo
r diff
eren
tiatin
g pa
rtic
ipan
ts w
ith p
ositi
ve fi
ndin
gs a
nd th
ose
with
neg
ativ
e fin
ding
s. AU
C =
are
a un
der t
he c
urve
.
resulted in an internal estimate of accuracy of 0.80 and a cross-validation estimate of accuracy of 0.78.
TA for Differentiating Participants with Positive Findings for Acute Myocarditis at EMB from Participants with Negative Findings at EMBBy repeating the stepwise dimension reduction and feature selection process, a similar set of three texture features was identified as impor-tant for the differentiation of participants with positive and negative findings. Again, T2_RL-NonUni was identified as a most important variable. In addition, another second-order fea-ture from the T2 co-occurrence matrix (T2 sum entropy) and one additional feature from the T2 run-length matrix (T2 gray-level nonuniformity [T2_GLevNonU]) were deemed important.
All three texture features showed significant differences between participants with positive findings at EMB and those with negative findings (Table 1). The selected texture features showed a superior diagnostic performance compared with LLC as well as global T1 and T2 when used as single parameters in a model, with AUCs rang-ing from 0.80 to 0.86 (Table 2). Combining the two run-length matrix features (T2_RLNon-Uni and T2_GLevNonU) in the model finally showed the best diagnostic performance, with an AUC of 0.88 (95% CI: 0.73, 1.00), a sensitivity of 23 of 26 (89% [95% CI: 81%, 93%]), and a specificity of 12 of 13 (92% [95% CI: 77%, 93%]), respectively (Fig 4a, Table 2). Ten-fold cross-validation resulted in an internal estimate of accuracy of 0.80 and a cross-validation esti-mate of accuracy of 0.80.
When combining blood parameters (tropo-nin, creatine kinase-MB, N-terminal pro b-type Natriuretic Peptide) with the two texture fea-tures in a model, diagnostic performance was even better and superior to a combination of blood parameters with LLC (AUC, 1.00 [95% CI: 0.80, 1.00] vs 0.78 [95% CI: 0.57, 0.89]; P , .001; sensitivity, 26 of 26 [100%; 95% CI: 90%, 100%] vs 16 of 26 [60%; 95% CI: 43%, 75%]; and specificity, 13 of 13 [100%; 95% CI: 83%, 100%] vs 13 of 13 [100%; 95% CI: 79%, 100%]) (Fig 4b).
DiscussionIn our study, we assessed the potential of TA for confirming or rejecting the clinical diagno-sis of myocarditis while comparing the results of cardiac MRI to EMB, rather than to those of healthy control participants. The main find-ings of our study can be summarized as follows:

Baessler et al
Radiology: Volume 00: Number 0— 2018 n radiology.rsna.org 7
acute infarctlike symptoms. In most of these studies, the di-agnostic sensitivity and specificity of LLC was in the range of 80%–92% and 80%–100%, respectively (5,28–30). No-tably, all these studies compared the diagnostic potential of LLC to a group of healthy control participants by using the clinical suspicion of myocarditis as the reference stan-dard. The diagnostic performance of LLC for differentiating between participants with positive findings for myocardi-tis at EMB and healthy control participants in our study is in line with these previous results. The lower diagnostic
In a selected participant cohort with biopsy-proven acute infarctlike myocarditis, the diagnostic performance of LLC and global myocardial T1 and T2 is only moderate when compared against EMB as the reference standard. In ad-dition, TA parameters yield better diagnostic performance compared with conventional LLC as well as to global myo-cardial T1 and T2, especially when adding clinical (blood) parameters to the model.
Only a small set of previous studies (5,28–30) focused in a similar fashion on a homogeneous participant cohort with
Figure 4: (a, b) Graphs show receiver operating characteristics (ROC) analyses for participants with positive findings for acute infarctlike myocarditis at endomyocardial biopsy (EMB, or EMB+) versus those with negative findings at EMB (or EMB2). ROC analysis indicates accuracy of Lake Louise criteria (LLC), as well as of single and combined texture analysis (TA) features (a) and for combination of blood parameters (troponin, creatine kinase-MB, N-terminal pro b-type Natriuretic Peptide) with LLC and texture features for diagnosing positive findings for acute infarctlike myocarditis at EMB compared with negative findings at EMB. 95% confidence intervals for area under the curves (AUCs) are shown for LLC (0.42, 0.79), mean T1 (0.45, 0.85), mean T2 (0.49, 0.85), T2_RLNonUni (0.71, 1.00), 0.73–1.00), T2_RLNonUni and T2_GLevNonU, positive LLC and blood paramters (0.57, 0.89), and T2_RLNonUni, T2_GLevNonU, and blood parameters (0.80, 1.00).
Figure 3: Graph shows receiver operating characteristics (ROC) analyses for participants with positive findings for acute infarctlike myo-carditis at endomyocardial biopsy (EMB, or EMB+) versus healthy control participants. ROC analysis indicates accuracy of Lake Louise criteria (LLC), as well as of single and combined texture analysis (TA) features for diagnosing participants with positive findings compared with healthy control participants. 95% confidence intervals for area under the curves (AUCs) are shown for LLC (0.68, 0.95), mean T1 (0.65, 0.94), mean T2 (0.81, 0.99), T2_RLNonUni (0.76, 0.98), and mean T2 and T2_RLNon-Uni (0.77, 1.00).

Cardiac MRI Texture Analysis of T1 and T2 Maps in Infarctlike Acute Myocarditis
8 radiology.rsna.org n Radiology: Volume 00: Number 0—2018
In conclusion, our findings show that the utility of global T1 or T2 times in participants suspected of having infarctlike myocarditis is limited because signal averaging over the entire myocardium might miss focal spots of disease and thus reduce sensitivity. In contrast, combining two parameters derived from T2 mapping (T2_RLNonUni and T2_GLevNonU) in a pre-dictive model resulted in excellent diagnostic performance and detected participants with positive findings for myocarditis at EMB with high sensitivity and specificity.
Author contributions: Guarantors of integrity of entire study, B.B., C.B.; study concepts/study design or data acquisition or data analysis/interpretation, all authors; manuscript drafting or manuscript revision for important intellectual content, all authors; approval of final version of submitted manuscript, all authors; agrees to ensure any questions related to the work are appropriately resolved, all authors; literature research, B.B., C.B., D.M., M.G., H.T., P.L.; clinical studies, J.L., K.K., M.v.R., S.d.W., C.B., D.M., M.G., H.T., P.L.; statistical analysis, B.B., C.B. and manuscript editing, B.B., C.L., J.L., C.B., D.M., M.G., H.T., P.L.
Disclosures of Conflicts of Interest: B.B. disclosed no relevant relationships. C.L. disclosed no relevant relationships. J.L. disclosed no relevant relationships. K.K. disclosed no relevant relationships. M.v.R. disclosed no relevant relation-ships. S.d.W. disclosed no relevant relationships. C.B. disclosed no relevant rela-tionships. D.M. disclosed no relevant relationships. M.G. disclosed no relevant relationships. H.T. disclosed no relevant relationships. P.L. disclosed no relevant relationships.
References 1. Dennert R, Crijns HJ, Heymans S. Acute viral myocarditis. Eur Heart J
2008;29(17):2073–2082. 2. Francone M, Chimenti C, Galea N, et al. CMR sensitivity varies with clinical pre-
sentation and extent of cell necrosis in biopsy-proven acute myocarditis. JACC Car-diovasc Imaging 2014;7(3):254–263.
3. Biesbroek PS, Beek AM, Germans T, Niessen HW, van Rossum AC. Diagnosis of myocarditis: current state and future perspectives. Int J Cardiol 2015;191:211–219.
4. Friedrich MG, Sechtem U, Schulz-Menger J, et al. Cardiovascular magnetic reso-nance in myocarditis: a JACC white paper. J Am Coll Cardiol 2009;53(17):1475–1487.
5. Luetkens JA, Doerner J, Thomas DK, et al. Acute myocarditis: multiparametric car-diac MR imaging. Radiology 2014;273(2):383–392.
6. Lurz P, Eitel I, Adam J, et al. Diagnostic performance of CMR imaging compared with EMB in patients with suspected myocarditis. JACC Cardiovasc Imaging 2012;5(5):513–524.
7. Lurz P, Luecke C, Eitel I, et al. Comprehensive cardiac magnetic resonance imag-ing in patients with suspected myocarditis: the MyoRacer-trial. J Am Coll Cardiol 2016;67(15):1800–1811.
8. Gutberlet M, Spors B, Thoma T, et al. Suspected chronic myocarditis at cardiac MR: diagnostic accuracy and association with immunohistologically detected inflamma-tion and viral persistence. Radiology 2008;246(2):401–409.
9. Baeßler B, Schaarschmidt F, Stehning C, Schnackenburg B, Maintz D, Bunck AC. A systematic evaluation of three different cardiac T2-mapping sequences at 1.5 and 3T in healthy volunteers. Eur J Radiol 2015;84(11):2161–2170.
10. Baeßler B, Schaarschmidt F, Dick A, et al. Mapping tissue inhomogeneity in acute myocarditis: a novel analytical approach to quantitative myocardial edema imaging by T2-mapping. J Cardiovasc Magn Reson 2015;17(1):115.
11. Wassmuth R, Prothmann M, Utz W, et al. Variability and homogeneity of cardio-vascular magnetic resonance myocardial T2-mapping in volunteers compared to pa-tients with edema. J Cardiovasc Magn Reson 2013;15(1):27.
12. von Knobelsdorff-Brenkenhoff F, Prothmann M, Dieringer MA, et al. Myocardial T1 and T2 mapping at 3 T: reference values, influencing factors and implications. J Cardiovasc Magn Reson 2013;15(1):53.
13. Baeßler B, Schaarschmidt F, Treutlein M, et al. Re-evaluation of a novel approach for quantitative myocardial oedema detection by analysing tissue inhomogeneity in acute myocarditis using T2-mapping. Eur Radiol 2017;27(12):5169–5178.
14. Larroza A, Bodí V, Moratal D. Texture analysis in magnetic resonance imaging: re-view and considerations for future applications. In: Constantinides C, ed. Assess-ment of Cellular and Organ Function and Dysfunction using Direct and Derived MRI Methodologies. InTech, 2016.
15. Baessler B, Mannil M, Oebel S, Maintz D, Alkadhi H, Manka R. Subacute and chronic left ventricular myocardial scar: accuracy of texture analysis on nonenhanced cine MR images. Radiology 2018;286(1):103–112.
16. Larroza A, Materka A, López-Lereu MP, Monmeneu JV, Bodí V, Moratal D. Dif-ferentiation between acute and chronic myocardial infarction by means of texture analysis of late gadolinium enhancement and cine cardiac magnetic resonance imag-ing. Eur J Radiol 2017;92:78–83.
17. Lurz JA, Luecke C, Lang D, et al. CMR-derived extracellular volume fraction as a marker for myocardial fibrosis: the importance of coexisting myocardial inflamma-tion. JACC Cardiovasc Imaging 2018;11(1):38–45.
performance of LLC and global myocardial T1 and T2 for differentiating participants with positive findings at EMB from those with negative findings in our study compared with previous reports (4,6,7,28,29) needs further explana-tion. One important difference between acute infarctlike myocarditis and other clinical presentations of myocarditis could be the focal versus diffuse nature of the pathologic condition. Although difficult to prove, myocarditis at an early stage is believed to cause more patchy and inhomo-geneous myocardial pathologic condition than participants with heart failure–like presentation and chronic symptoms, resulting in a homogeneously diffuse myocardial pathologic condition. T1 or T2 time averaged over the entire myocar-dium might miss focal spots of disease and thus lead to false-negative results, reducing sensitivity (10,13). The problem of high interindividual variability of myocardial T1 and T2 times can further reduce sensitivity and—even more so—specificity when using an averaging approach alone (9,10).
Although previous reports have shown a high sensitivity and specificity for native T1 in detecting myocardial edema (5,28,31), no parameter derived from T1 mapping was among the most powerful discriminators when assessing predictive models and a significant correlation was observed between mean T1 and T2. Thus, our results show that no significant additional effect can be achieved by combining T1 and T2 parameters, in-cluding those derived from TA in a multiparametric imaging ap-proach for detecting acute infarctlike myocarditis.
Both texture features (T2_RLNonUni and T2_GLevNonU) are derived from the higher-order run-length feature matrix, which is based on computing the number of gray-level runs of various lengths. A gray-level run represents a set of linearly adjacent picture points having the same gray-level value (14), and the length of the run is the number of picture points within it. The run-length matrix elements de-fine how often a particular gray-level value is met in a par-ticular run length (14). Thus, the two features T2_RLNon-Uni and T2_GLevNonU are a measure for the homogeneity of the pixel gray-level distribution of the underlying tissue, where higher values represent more inhomogeneity within the gray-levels of the run-length matrix. Although the two features were highly collinear in our study, they showed a sig-nificant additive value when used in combination.
We acknowledge several limitations of our study. Although EMB is widely accepted as the reference standard for diagnos-ing myocarditis, a sampling error leading to false-negative re-sults cannot be excluded. We performed biventricular EMB acquiring a high number of samples as suggested previously (32) to acquire a reliable reference standard, but some minor uncertainty remains. The mapping techniques used in our study represented the methodology available in mid-2012. In the meantime, techniques with potentially more robust estimation of T1 and T2 relaxation times have been reported (33). Thus, additional studies using these techniques should be performed to further elucidate the application of TA on T1 and T2 mapping and the influence of technical factors, such as field strength or sequence type, on derived markers for tissue inhomogeneity.

Baessler et al
Radiology: Volume 00: Number 0— 2018 n radiology.rsna.org 9
18. Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiol-ogy, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2013;34(33):2636–2648, 2648a–2648d.
19. MacKay JW, Murray PJ, Kasmai B, Johnson G, Donell ST, Toms AP. MRI texture analysis of subchondral bone at the tibial plateau. Eur Radiol 2016;26(9):3034–3045.
20. Summers RM. Texture analysis in radiology: does the emperor have no clothes? Ab-dom Radiol (NY) 2017;42(2):342–345.
21. Szczypiński PM, Strzelecki M, Materka A, Klepaczko A. MaZda: a software pack-age for image texture analysis. Comput Methods Programs Biomed 2009;94(1): 66–76.
22. Baeßler B, Mannil M, Maintz D, Alkadhi H, Manka R. Texture analysis and ma-chine learning of non-contrast T1-weighted MR images in patients with hypertro-phic cardiomyopathy: preliminary results. Eur J Radiol 2018;102:61–67.
23. Collewet G, Strzelecki M, Mariette F. Influence of MRI acquisition protocols and image intensity normalization methods on texture classification. Magn Reson Imag-ing 2004;22(1):81–91.
24. Xu JW, Suzuki K. Max-AUC feature selection in computer-aided detection of polyps in CT colonography. IEEE J Biomed Health Inform 2014;18(2):585–593.
25. R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing, 2017.
26. RStudio Team. RStudio: integrated development for R. Boston, Mass: RStudio, 2016.
27. Breiman L. Random forests. Mach Learn 2001;45(1):5–32. 28. Ferreira VM, Piechnik SK, Dall’Armellina E, et al. T(1) mapping for the diagnosis
of acute myocarditis using CMR: comparison to T2-weighted and late gadolinium enhanced imaging. JACC Cardiovasc Imaging 2013;6(10):1048–1058.
29. Luetkens JA, Homsi R, Sprinkart AM, et al. Incremental value of quantitative CMR including parametric mapping for the diagnosis of acute myocarditis. Eur Heart J Cardiovasc Imaging 2016;17(2):154–161.
30. Schwab J, Rogg HJ, Pauschinger M, et al. Functional and morphological parameters with tissue characterization of cardiovascular magnetic imaging in clinically verified “infarct-like myocarditis”. Rofo 2016;188(4):365–373.
31. Messroghli DR, Moon JC, Ferreira VM, et al. Correction to: Clinical recommenda-tions for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellu-lar volume: a consensus statement by the Society for Cardiovascular Magnetic Reso-nance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2018;20(1):9.
32. Yilmaz A, Kindermann I, Kindermann M, et al. Comparative evaluation of left and right ventricular endomyocardial biopsy: differences in complication rate and diag-nostic performance. Circulation 2010;122(9):900–909.
33. Baeßler B, Schaarschmidt F, Stehning C, Schnackenburg B, Maintz D, Bunck AC. Cardiac T2-mapping using a fast gradient echo spin echo sequence: first in vitro and in vivo experience. J Cardiovasc Magn Reson 2015;17(1):67.